Embed Size (px)
Citation preview

THYROID THYROID GLANDGLAND
THYROIDITISTHYROIDITIS

THYROIDITISTHYROIDITISIIt is a heterogeneous group of t is a heterogeneous group of
inflammatory disorders inflammatory disorders involving the thyroid gland, of involving the thyroid gland, of which the etiologies range from which the etiologies range from
autoimmune to infectious autoimmune to infectious origins. origins.
The clinical course may be The clinical course may be
acute, subacute, or chronic.acute, subacute, or chronic.

A classification of A classification of thyroiditis:thyroiditis:
Acute thyroiditisAcute thyroiditis
infectious infectious
non-infectiousnon-infectious
Subacute thyroiditisSubacute thyroiditis
Autoimmune thyroiditisAutoimmune thyroiditis
Chronic autoimmune Chronic autoimmune thyroiditis :thyroiditis :
Hashimoto’s thyroiditisHashimoto’s thyroiditis
Atrophic thyroiditisAtrophic thyroiditis
Focal thyroiditis Focal thyroiditis
Juvenile thyroiditisJuvenile thyroiditis
Silent thyroiditisSilent thyroiditis
Postpartum thyroiditisPostpartum thyroiditis
IV. Riedel’s thyroiditisIV. Riedel’s thyroiditis

ACUTE INFECTIOUS ACUTE INFECTIOUS
THYROIDITISTHYROIDITIS
RRare, serious, bacterial are, serious, bacterial
inflammatory disease of the inflammatory disease of the
thyroid.thyroid.

Protective mechanisms of Protective mechanisms of
the thyroid gland:the thyroid gland:
very good perfusionvery good perfusionefficient lymphatic drainageefficient lymphatic drainagecapsulation of the thyroidcapsulation of the thyroid
high concentration of iodinehigh concentration of iodine

Etiologic agents:Etiologic agents:Streptococcus pyogenes, Streptococcus pyogenes,
Streptococcus pneumoniae, Streptococcus pneumoniae, Escherichia coli, Escherichia coli,
Pseudomonas aeruginosa, Pseudomonas aeruginosa, Salmonella typhi, Salmonella typhi,
anaerobes of the oropharyngeal anaerobes of the oropharyngeal cavity.cavity.

RARE FORMS OF RARE FORMS OF INFECTIOUS THYROIDITIS:INFECTIOUS THYROIDITIS:
the thyroid is rarely the seat of the thyroid is rarely the seat of
tuberculosis, syphilis, fungal tuberculosis, syphilis, fungal
infections (Aspergillus species), or infections (Aspergillus species), or
parasites; parasites;
Pneumocystis carinii infection of Pneumocystis carinii infection of
the thyroid has been reported in the thyroid has been reported in
patients with AIDS.patients with AIDS.

hematogenous seedinghematogenous seeding
from distant focifrom distant foci
extension from extension from adjacent infected structuresadjacent infected structures
direct direct
traumatrauma through through a persistenta persistent
thyroglossal ductthyroglossal duct
Infection to theInfection to the thyroid occurs bythyroid occurs by::

CLINICAL PICTURECLINICAL PICTUREOF OF ACUTE INFECTIOUS ACUTE INFECTIOUS
THYROIDITISTHYROIDITIS
severe anterior neck pain of abrupt severe anterior neck pain of abrupt onset, pain may radiate to the ear, onset, pain may radiate to the ear, mandible, or occiput; dysphagia, mandible, or occiput; dysphagia,
dysphonia, fever, rigor, diaphoresisdysphonia, fever, rigor, diaphoresis
palpation shows a unilateral or less-palpation shows a unilateral or less-frequently bilateral tender swelling of the frequently bilateral tender swelling of the thyroid which is associated with cervical thyroid which is associated with cervical
lymphadenopathylymphadenopathy

CLINICAL PICTURECLINICAL PICTUREOF OF ACUTE INFECTIOUS ACUTE INFECTIOUS
THYROIDITISTHYROIDITISthe skin over the infected area is the skin over the infected area is
erythematous and warmerythematous and warm
the white cell count and erythrocyte the white cell count and erythrocyte
sedimentation rate are elevatedsedimentation rate are elevated
thyroid antibodies are absentthyroid antibodies are absent
serum Tserum T44 and T and T33 levels are usually levels are usually
normal as well as thyroid RAIUnormal as well as thyroid RAIU

CLINICAL PICTURECLINICAL PICTUREOF OF ACUTE INFECTIOUS ACUTE INFECTIOUS
THYROIDITISTHYROIDITISthe isotope scans reveal a “cold” defect the isotope scans reveal a “cold” defect
in the involved lobein the involved lobe
ultrasonography shows an enlarged ultrasonography shows an enlarged
irregular mass of mixed echogenicityirregular mass of mixed echogenicity
the presence at fine-needle aspiration of the presence at fine-needle aspiration of
purulent material is confirmatory of purulent material is confirmatory of
suppurative thyroiditis and allows for suppurative thyroiditis and allows for
the identification of the causative agentthe identification of the causative agent

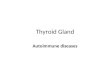
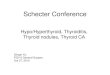
Ultrasonography of acute Ultrasonography of acute bacterial thyroiditisbacterial thyroiditis

Ultrasonography of acute Ultrasonography of acute bacterial thyroiditisbacterial thyroiditis

TREATMENTTREATMENT OF INFECTIOUS OF INFECTIOUS THYROIDITISTHYROIDITIS
this type of thyroiditis requires this type of thyroiditis requires
the administration of the administration of
appropriate antibiotics based appropriate antibiotics based
on the findings of the culture on the findings of the culture
from a fine-needle aspirate, from a fine-needle aspirate,
and surgical drainage (or and surgical drainage (or
excision) of any area of excision) of any area of
fluctuance or abscess. fluctuance or abscess.

Before the results of the cultureBefore the results of the culture
a combined regimen of a combined regimen of nafcilin and nafcilin and
gentamicin or a third generation gentamicin or a third generation
cephalosporincephalosporin would be would be
appropriate treatment.appropriate treatment.

NON-INFECTIOUS NON-INFECTIOUS THYROIDITISTHYROIDITIS
clinical picture depends clinical picture depends
on causative agentson causative agents

NON-INFECTIOUS NON-INFECTIOUS THYROIDITISTHYROIDITIS
AFTER AFTER 131131J THERAPYJ THERAPY
(hyperthyroidism, thyroid cancer):(hyperthyroidism, thyroid cancer):
tender swelling of the thyroid, tender swelling of the thyroid,
itching of the skin over thyroid, itching of the skin over thyroid,
subfebrile body temperaturesubfebrile body temperature

NON-INFECTIOUS NON-INFECTIOUS THYROIDITISTHYROIDITIS
AFTER RADIOTHERAPYAFTER RADIOTHERAPY
(external radiotherapy of the thyroid cancer, (external radiotherapy of the thyroid cancer,
complementary external radiotherapy in complementary external radiotherapy in
patients with breast cancer):patients with breast cancer):
symptomatic or oligosymptomatic symptomatic or oligosymptomatic
course, leading into hypothyroidismcourse, leading into hypothyroidism

NON-INFECTIOUS NON-INFECTIOUS THYROIDITISTHYROIDITIS
AFTER TRAUMA OF THE NECKAFTER TRAUMA OF THE NECK
(bleeding to thyroid parenchyma (bleeding to thyroid parenchyma
or thyroid cystor thyroid cyst))
severe anterior neck pain of abrupt severe anterior neck pain of abrupt
onset, onset,
swelling of the thyroid, swelling of the thyroid,
fluctuationfluctuation

NON-INFECTIOUS THYROIDITISNON-INFECTIOUS THYROIDITISTREATMENTTREATMENT
In milder cases disappear In milder cases disappear spontaneouslyspontaneously
In some casesIn some cases::
salicylates or salicylates or
non steroidal anti-inflammatory drugs non steroidal anti-inflammatory drugs (Polopiryni S 2-3 g/day, (Polopiryni S 2-3 g/day,
Paracetamol 1.5-2.0g/day)Paracetamol 1.5-2.0g/day) ExceptionallyExceptionally::
corticosteroids corticosteroids (Prednisone 20-30mg/day)(Prednisone 20-30mg/day)

SUBACUTE (GRANULOMATOUS) SUBACUTE (GRANULOMATOUS) THYROIDITIS THYROIDITIS
(DE QUERVAIN’S DISEASE)(DE QUERVAIN’S DISEASE) AA spontaneously remitting, painful, spontaneously remitting, painful, inflammatory disease of the thyroid, inflammatory disease of the thyroid,
probably of viral origin. probably of viral origin. It is the most frequent cause of It is the most frequent cause of
anterior neck pain. anterior neck pain. Most prevalent in the temperate zone. Most prevalent in the temperate zone.
Afflicts more frequently women Afflicts more frequently women between the third and sixth decades between the third and sixth decades
of life.of life.

SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS ETIOLOGYETIOLOGY
PPROBABLY VIRAL, ROBABLY VIRAL,
THERE ARE SOME EVIDENCES:THERE ARE SOME EVIDENCES:Often preceded by an upper Often preceded by an upper
respiratory tract viral respiratory tract viral infectioninfection
Prodromal viral symptomsProdromal viral symptomsSeasonal distribution Seasonal distribution
(summer and fall)(summer and fall)

SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS ETIOLOGYETIOLOGY
Occurs in coincidence with Occurs in coincidence with outbreaks of viral diseases outbreaks of viral diseases
(mumps, measles, influenza)(mumps, measles, influenza)Elevated titers of viral Elevated titers of viral
antibodies antibodies (coxsackievirus, (coxsackievirus, adenovirus, mumps)adenovirus, mumps) have have
been found in convalescent been found in convalescent sera of patients with subacute sera of patients with subacute
thyroiditisthyroiditis

infiltration with neutrophils and infiltration with neutrophils and mononuclear cells, mononuclear cells,
disruption of follicles, disruption of follicles, typical lesion characterized by a typical lesion characterized by a central core of colloid surrounded central core of colloid surrounded
by a large number of individual by a large number of individual histiocytes histiocytes
(giant multinucleated cells).(giant multinucleated cells).
SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS HISTOPATHOLOGICAL HISTOPATHOLOGICAL
CHANGESCHANGES

There is usually a viral There is usually a viral prodrome withprodrome with:: myalgias, myalgias,
low-grade fever, low-grade fever, sore-throat sore-throat dysphagiadysphagia
SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS CLINICAL PICTURECLINICAL PICTURE

Anterior neck pain occurs abruptly, Anterior neck pain occurs abruptly, is sometimes unilateral, and is sometimes unilateral, and
may radiate to the ear, mandible may radiate to the ear, mandible or occiput, pain may shift to the or occiput, pain may shift to the
contralateral lobe contralateral lobe (creeping thyroiditis);(creeping thyroiditis);
moving the head, swallowing, or moving the head, swallowing, or coughing aggravate the paincoughing aggravate the pain..
SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS CLINICAL PICTURECLINICAL PICTURE

Symptoms of thyrotoxicosis Symptoms of thyrotoxicosis
may occurmay occur
the release of performed the release of performed
thyroid hormones from thyroid hormones from disrupted folliclesdisrupted follicles
SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS CLINICAL PICTURECLINICAL PICTURE

On palpationOn palpation:: the thyroid is slightly to the thyroid is slightly to
moderately enlarged, moderately enlarged, sometimes asymmetrical or sometimes asymmetrical or
even nodular, even nodular, firm, firm,
tender tender and painfuland painful
SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS CLINICAL PICTURECLINICAL PICTURE

elevated erythrocyte sedimentation elevated erythrocyte sedimentation rate rate (>55mm/h),(>55mm/h),
normal or slightly elevated leukocyte normal or slightly elevated leukocyte counts, counts,
increased serum IL-6 and Tg increased serum IL-6 and Tg concentrations during the thyrotoxic concentrations during the thyrotoxic
phasephase,, thyroid antibodies are transiently thyroid antibodies are transiently detectable at low titers in a minority of detectable at low titers in a minority of
patientspatients
SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS LABORATORY FINDINGSLABORATORY FINDINGS

THYROTOXIC:THYROTOXIC: high Thigh T44 and/or T and/or T33 level, level,
low TSH level, low TSH level, RAIU value <5% RAIU value <5%
(isotope scans show a cold area in the (isotope scans show a cold area in the involved section of the gland or no involved section of the gland or no
uptake at all)uptake at all)
THE PHASES OF THE PHASES OF SUBACUTE SUBACUTE THYROIDITIS THYROIDITIS

HYPOTHYROID: HYPOTHYROID: low Tlow T44, ,
high TSH level, high TSH level, normal RAIU valuenormal RAIU value
THE PHASES OF THE PHASES OF SUBACUTE SUBACUTE THYROIDITIS THYROIDITIS

RECOVERY:RECOVERY: normal Tnormal T44 and T and T33 level, level,
normal TSH level, normal TSH level, normal RAIU valuenormal RAIU value
THE PHASES OF THE PHASES OF SUBACUTE SUBACUTE THYROIDITIS THYROIDITIS

SUBACUTE THYROIDITIS SUBACUTE THYROIDITIS
The course of the disease may last 2 The course of the disease may last 2 to 6 months without treatment. to 6 months without treatment. Recurrences of the subacute Recurrences of the subacute thyroiditis are reported in about thyroiditis are reported in about
one-fifth of the patients. one-fifth of the patients. Permanent hypothyroidism is rare Permanent hypothyroidism is rare
(1-5%).(1-5%). The disease may evolve into chronic The disease may evolve into chronic
autoimmune thyroiditis.autoimmune thyroiditis.

SUBACUTE THYROIDITISSUBACUTE THYROIDITISTREATMENTTREATMENT
In milder casesIn milder cases:: salicylates or non steroidal salicylates or non steroidal
anti-inflammatory drugs anti-inflammatory drugs
provide some relief of pain provide some relief of pain
and tenderneesand tendernees..

SUBACUTE THYROIDITISSUBACUTE THYROIDITISTREATMENTTREATMENT
In more severe casesIn more severe cases:: corticosteroids corticosteroids
(prednisone 40-60mg/day)(prednisone 40-60mg/day) have a more dramatic and rapid have a more dramatic and rapid
effect; effect; the corticosteroid is slowly the corticosteroid is slowly tapered over the next 6 to 8 tapered over the next 6 to 8
weeks and then discontinuedweeks and then discontinued..

SUBACUTE THYROIDITISSUBACUTE THYROIDITISTREATMENTTREATMENT
Symptoms of thyrotoxicosisSymptoms of thyrotoxicosis should be managed with B-should be managed with B-adrenergic blocking agents adrenergic blocking agents
(Propranolol 20-40mg, (Propranolol 20-40mg,
3 to 4 times daily)3 to 4 times daily) In patients with In patients with hypothyroidism hypothyroidism L-TL-T44
replacement is needed.replacement is needed.

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITIS
CHRONIC AUTOIMMUNE CHRONIC AUTOIMMUNE THYROIDITIS PRESENTS WITH THYROIDITIS PRESENTS WITH
TWO CLINICAL ENTITIES:TWO CLINICAL ENTITIES:
a goitrous a goitrous formform
(Hashimoto (Hashimoto thyroiditis)thyroiditis)
an atrophic forman atrophic form (atrophic (atrophic
thyroiditis or thyroiditis or primary primary
myxedema)myxedema)

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITIS
Treatment with Treatment with immunosuppressive agents immunosuppressive agents
(corticosteroids) is not (corticosteroids) is not recommended in autoimmune recommended in autoimmune
thyroiditis. thyroiditis. Lifelong substitution therapy Lifelong substitution therapy
with L-thyroxine is indicated with L-thyroxine is indicated in hypothyroid patientsin hypothyroid patients..

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITIS
Among children living in areas of Among children living in areas of iodine sufficiency, juvenile iodine sufficiency, juvenile
lymphocytic thyroiditis is the cause lymphocytic thyroiditis is the cause of euthyroid goiter in about one-of euthyroid goiter in about one-
half to two-thirds of patientshalf to two-thirds of patients.. Silent thyroiditis is characterized by Silent thyroiditis is characterized by
transient thyrotoxicosistransient thyrotoxicosis with low with low thyroid radioiodone uptake and a thyroid radioiodone uptake and a small, painless, nontender goitersmall, painless, nontender goiter..

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITIS
The postpartum rebound of The postpartum rebound of immunity may be accompanied immunity may be accompanied
by destructive thyroiditis by destructive thyroiditis (postpartum thyroiditis),(postpartum thyroiditis),
resulting in transient resulting in transient thyrotoxicosis evolving to thyrotoxicosis evolving to
hypothyroidism, or hypothyroidism, or hypothyroidism alone, followed hypothyroidism alone, followed
by gradual recoveryby gradual recovery..

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISETIOLOGYETIOLOGY
OOrgan-specific autoimmunity is rgan-specific autoimmunity is the cause of the disease, the cause of the disease,
the thyroid is infiltrated by the thyroid is infiltrated by lymphocytes, lymphocytes,
thyroid antibodies are present thyroid antibodies are present in serum, in serum,
and there is a clinical or and there is a clinical or immunological overlap with immunological overlap with other autoimmune diseasesother autoimmune diseases..

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISETIOLOGYETIOLOGY
AActivated, autoreactive T-helper ctivated, autoreactive T-helper recruit in the recruit in the thyroid cytotoxic T thyroid cytotoxic T
cells cells
(T cells may kill directly thyroid cells (T cells may kill directly thyroid cells or also cause tissue injury by or also cause tissue injury by
release of cytokines)release of cytokines) and B cellsand B cells
(are transformed into plasmacytes (are transformed into plasmacytes which produce antithyroid which produce antithyroid
antibodieantibodies)s)

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISETIOLOGYETIOLOGY
ANTITHYROID ANTIBODIEANTITHYROID ANTIBODIESS::
thyroid peroxidase thyroid peroxidase antibodies antibodies (TPOAb),(TPOAb),
thyroglobulin antibodies thyroglobulin antibodies (TgAb),(TgAb),
TSH-blocking TSH-blocking antibodiesantibodies

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISETIOLOGYETIOLOGY
EEnvironmental factorsnvironmental factors
(infectious agents, (infectious agents, therapeutically administered therapeutically administered interferon alpha, physical and interferon alpha, physical and
emotional stress, and emotional stress, and increased iodine intake)increased iodine intake)
may be important for the may be important for the development of autoimmune development of autoimmune
thyroiditisthyroiditis..

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISEPIDEMIOLOGYEPIDEMIOLOGY
the disease is most often diagnosed the disease is most often diagnosed between the ages of 50 - 60 years, between the ages of 50 - 60 years,
5 to 7 times more frequently in women 5 to 7 times more frequently in women than in men; than in men;
the prevalence of thyroid antibodies the prevalence of thyroid antibodies
(which correlates with autoimmune (which correlates with autoimmune thyroiditis)thyroiditis)
is higher in communities with sufficient is higher in communities with sufficient iodine intake and increases from 6% to iodine intake and increases from 6% to
27% in the second to sixth decades of life 27% in the second to sixth decades of life in women.in women.

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISCLINICAL PICTURECLINICAL PICTURE
Patients may present a goiter Patients may present a goiter
with or without hypothyroidism.with or without hypothyroidism.
A feeling of tightnees in the A feeling of tightnees in the
neck may occur, but neck may occur, but
compression of the trachea is compression of the trachea is
uncommon.uncommon.

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISCLINICAL PICTURECLINICAL PICTURE
On physical examinationOn physical examination most Hashimoto’s glands are most Hashimoto’s glands are
diffusely enlarged, diffusely enlarged, but one lobe may be larger than but one lobe may be larger than
the other, the other, and the pyramidal lobe may be and the pyramidal lobe may be
palpable; palpable; the goiter is generally moderate the goiter is generally moderate
in size, though massive in size, though massive enlargements may occur; enlargements may occur;

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISCLINICAL PICTURECLINICAL PICTURE
On physical examinationOn physical examination the gland is nontender, firm or the gland is nontender, firm or
rubbery in consistency, with a rubbery in consistency, with a bosselated surface;bosselated surface;
the thyroid gland is reduced in the thyroid gland is reduced in size in atrophic thyroiditis.size in atrophic thyroiditis.

AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISCLINICAL PICTURECLINICAL PICTURE
Thyrotoxicosis Thyrotoxicosis (Hashitoxicosis)(Hashitoxicosis) rarely occurs, rarely occurs,
due to a combination of due to a combination of Hashimoto’s thyroiditis with Hashimoto’s thyroiditis with Graves’ disease in the same Graves’ disease in the same patient or to the transient patient or to the transient
discharge of performed discharge of performed thyroid hormones as a result thyroid hormones as a result of the inflammatory process.of the inflammatory process.

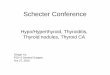
TSH, FTTSH, FT44 and FT and FT33 serum levels serum levels
AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISDIAGNOSTIC PROCEDURESDIAGNOSTIC PROCEDURES
HA
SH
ITO
XIC
OS
IH
AS
HIT
OX
ICO
SI
SS
FTFT44 FT FT33
TSHTSH
HY
PO
TH
YR
OID
ISH
YP
OTH
YR
OID
ISMM
FTFT44 FT FT33
TSH TSH

AAntithyroid antibodiesntithyroid antibodies are positive: are positive: TPOAbTPOAb 95% patients95% patients
TgAbTgAb 60-80% patients60-80% patients
IIn a few patients antithyroid n a few patients antithyroid antibodies are in low or antibodies are in low or
undetectable titers undetectable titers
(seronegative Hashimoto’s thyroiditis)(seronegative Hashimoto’s thyroiditis)
AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISDIAGNOSTIC PROCEDURESDIAGNOSTIC PROCEDURES

Thyroid radionuclide scan and Thyroid radionuclide scan and radioactive iodine uptake (RAIU) radioactive iodine uptake (RAIU) are not crucial to the diagnosis are not crucial to the diagnosis
(normal, low, or high)(normal, low, or high)..
An ultrasound pattern of the An ultrasound pattern of the thyroidthyroid::
diffusely reduced echogenicitydiffusely reduced echogenicity
AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISDIAGNOSTIC PROCEDURESDIAGNOSTIC PROCEDURES

FNAB- cytological smears of FNAB- cytological smears of Hashimoto’s thyroiditis are rich Hashimoto’s thyroiditis are rich in lymphocytes and oxyphil cells in lymphocytes and oxyphil cells
(it is advisable in patients with (it is advisable in patients with suspicious nodules or a rapidly suspicious nodules or a rapidly enlarging goiter in order to rule enlarging goiter in order to rule
out malignancyout malignancy).).
AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISDIAGNOSTIC PROCEDURESDIAGNOSTIC PROCEDURES

Chronic autoimmune thyroiditis is a Chronic autoimmune thyroiditis is a component of type 2 autoimmune component of type 2 autoimmune
polyglandular syndrome, a polyglandular syndrome, a condition characterized by a condition characterized by a
coexistence of two or more of the coexistence of two or more of the following disorders:following disorders:
Addison’s disease, autoimmune Addison’s disease, autoimmune thyroiditis, insulin dependent thyroiditis, insulin dependent
diabetes mellitus, atrophic gastritis diabetes mellitus, atrophic gastritis with or without pernicious anemia, with or without pernicious anemia,
vitiligo, alopecia, myasthenia vitiligo, alopecia, myasthenia gravis, and hypophysitis.gravis, and hypophysitis.

Corticosteroids are not recommendedCorticosteroids are not recommended Substitution therapy with L-TSubstitution therapy with L-T44 at a at a
dose that normalizes serum TSH dose that normalizes serum TSH levels : levels :
the average daily replacement dose of L-Tthe average daily replacement dose of L-T44 in adults is 1.6ug/kg body weight in adults is 1.6ug/kg body weight
=75-100ug/day in women and =75-100ug/day in women and 100-150ug/day in men.100-150ug/day in men.
AUTOIMMUNE THYROIDITISAUTOIMMUNE THYROIDITISTREATMENTTREATMENT

SILENT (PAINLESS) SILENT (PAINLESS) THYROIDITISTHYROIDITIS
it is cit is chharacterized by aracterized by transient thyrotoxicosis transient thyrotoxicosis
with low RAIU, and a small, with low RAIU, and a small, painless, nondender goiter. painless, nondender goiter.
TThyrotoxicosis results from damage hyrotoxicosis results from damage of follicular cells by the of follicular cells by the
inflammatory process, with inflammatory process, with leakage of performed thyroid leakage of performed thyroid hormones in the bloodstream.hormones in the bloodstream.

SILENT (PAINLESS) SILENT (PAINLESS) THYROIDITISTHYROIDITIS
The overall prevalence of silent The overall prevalence of silent thyroiditis as a cause of thyroiditis as a cause of
thyrotoxicosis ranges from 4 to thyrotoxicosis ranges from 4 to 15%; 15%;
greater prevalence in previously greater prevalence in previously iodine-deficient areas, but iodine-deficient areas, but
recently exposed to sufficient recently exposed to sufficient iodine; iodine;
the female/male ratio isthe female/male ratio is ~ ~ 2:1; 2:1;

Silent thyroiditis presents with Silent thyroiditis presents with a relatively abrupt onset of a relatively abrupt onset of
symptoms of mild symptoms of mild thyrotoxicosisthyrotoxicosis::
tachycardia, tachycardia, heat intolerance, heat intolerance, sweating, sweating, nervousness, nervousness,
weight loss.weight loss.
Serum TgSerum Tg and urinary iodine and urinary iodine concentrations are increasedconcentrations are increased
SILENT THYROIDITISSILENT THYROIDITISCLINICAL PICTURECLINICAL PICTURE

THERE ARE 3 PHASES:THERE ARE 3 PHASES: thyrotoxicosis, thyrotoxicosis,
hypothyroidism, hypothyroidism, recoveryrecovery..
PPersistent hypothyroidism ersistent hypothyroidism may also develop in about may also develop in about
5%5%..
SILENT THYROIDITISSILENT THYROIDITISCLINICAL PICTURECLINICAL PICTURE

Differentiation from Graves’ Differentiation from Graves’ hyperthyroidism is importanthyperthyroidism is important..
IIn silent thyroiditisn silent thyroiditis abrupt onset, abrupt onset,
thyrotoxicosis less severe, thyrotoxicosis less severe, duration of thyrotoxicosis < 3 months,duration of thyrotoxicosis < 3 months,
thyroid bruit, ophthalmopathy and thyroid bruit, ophthalmopathy and dermopathy absent, dermopathy absent, TT33/T/T44 ratio < 20/1, ratio < 20/1,
RAIU low, RAIU low, TSH-R antibodies usually negative, TSH-R antibodies usually negative,
thyrotoxicosis transientthyrotoxicosis transient..
SILENT THYROIDITISSILENT THYROIDITISCLINICAL PICTURECLINICAL PICTURE

Anti-thyroid drugs or radioiodine Anti-thyroid drugs or radioiodine are inappropriate for treatment of are inappropriate for treatment of
silent thyroiditissilent thyroiditis..
In thyrotoxic phaseIn thyrotoxic phase::
ββ-adrenergic blocking agents-adrenergic blocking agentsIn hypothyroid phaseIn hypothyroid phase::
L-TL-T44 replacement therapy replacement therapy
SILENT THYROIDITISSILENT THYROIDITISTREATMENTTREATMENT

POSTPARTUM THYROIDITISPOSTPARTUM THYROIDITIS
DDuring pregnancy all autoimmune uring pregnancy all autoimmune
reactions are inhibited by a reactions are inhibited by a
number of physiologic factors, number of physiologic factors,
and following delivery there is a and following delivery there is a
reversal of these alterations reversal of these alterations
with rebound of autoimmune with rebound of autoimmune
phenomena.phenomena.

The incidenThe incidencce of PPT e of PPT
ranges from 1% toranges from 1% to 16% of women16% of women
during the first year after during the first year after
deliverydelivery..
POSTPARTUM THYROIDITISPOSTPARTUM THYROIDITIS

Risk factors for the development Risk factors for the development of PPT include:of PPT include:
positive TPOAb in the first positive TPOAb in the first trimester of pregnancy,trimester of pregnancy,
type 1 diabetes mellitus, type 1 diabetes mellitus, a history of chronic autoimmune a history of chronic autoimmune thyroiditis or Graves’ disease, or a thyroiditis or Graves’ disease, or a previous episode of PPT during a previous episode of PPT during a
preceding pregnancypreceding pregnancy..
POSTPARTUM THYROIDITISPOSTPARTUM THYROIDITIS

The clinical course and The clinical course and
treatment are the same as treatment are the same as
described above for silent described above for silent
thyroiditisthyroiditis
POSTPARTUM THYROIDITISPOSTPARTUM THYROIDITIS

RIEDEL’S THYROIDITIS RIEDEL’S THYROIDITIS (SCLEROSING THYROIDITIS, (SCLEROSING THYROIDITIS,
INVASIVE FIBROUS THYROIDITIS)INVASIVE FIBROUS THYROIDITIS)
IIt is a rare, chronic inflammatory disorder t is a rare, chronic inflammatory disorder of unknown etiology, characterized by of unknown etiology, characterized by
dense fibrosis involving the thyroid and dense fibrosis involving the thyroid and adjacent tissues, and extracervical areas adjacent tissues, and extracervical areas
(fibrous mediastinitis, retroperitoneal (fibrous mediastinitis, retroperitoneal fibrosis, retro-orbital fibrosis, sclerosing fibrosis, retro-orbital fibrosis, sclerosing
cholangitis, and pancreatitis).cholangitis, and pancreatitis).
It occurs mainly in middle-age or elderly It occurs mainly in middle-age or elderly women.women.

RIEDEL’S THYROIDITIS RIEDEL’S THYROIDITIS CLINICAL PICTURECLINICAL PICTURE
A patient will present with a long A patient will present with a long history of a painless, history of a painless,
progressively increasing anterior progressively increasing anterior neck mass.neck mass.
Pressure symptomsPressure symptoms:: dysphagia, cough, hoarseness, dysphagia, cough, hoarseness,
stridor, attacks of suffocation)stridor, attacks of suffocation)may appear.may appear.
Most patients are euthyroidMost patients are euthyroid

RIEDEL’S THYROIDITIS RIEDEL’S THYROIDITIS CLINICAL PICTURECLINICAL PICTURE
On physical examination:On physical examination:
a stony-hard or woody thyroid mass a stony-hard or woody thyroid mass
that varies in size from small to that varies in size from small to
very large, may involve one or very large, may involve one or
both lobes, and is fixed to both lobes, and is fixed to
surrounding structuressurrounding structures..

RIEDEL’S THYROIDITIS RIEDEL’S THYROIDITIS CLINICAL PICTURECLINICAL PICTURE
Thyroid antibodies are present in Thyroid antibodies are present in up to 45% of patientsup to 45% of patients..
Serum calcium may be low due to Serum calcium may be low due to parathyroid invasionparathyroid invasion..
Differentiation from thyroid Differentiation from thyroid carcinoma or lymphoma of the carcinoma or lymphoma of the thyroid requires open biopsy, thyroid requires open biopsy, since FNAB may be difficult to since FNAB may be difficult to
interpretinterpret..

RIEDEL’S THYROIDITIS RIEDEL’S THYROIDITIS CLINICAL PICTURECLINICAL PICTURE
Surgical treatment is necessary to Surgical treatment is necessary to relieve pressure on the trachea and to relieve pressure on the trachea and to
establish diagnosisestablish diagnosis.. Corticosteroids are of little or no Corticosteroids are of little or no
valuevalue.. The course of the lesion may be The course of the lesion may be slowly progressive, may stabilize, or slowly progressive, may stabilize, or
remit.remit. Extrathyroidal fibrotic lesions may Extrathyroidal fibrotic lesions may
complicate the prognosis.complicate the prognosis.