Embed Size (px)
Citation preview

Rhinosinusitis: Current Rhinosinusitis: Current ConceptsConcepts
Frederick S. Rosen, MDFrederick S. Rosen, MDMatthew Ryan, MDMatthew Ryan, MD

2
Introduction

3
Introduction•The medical condition most commonly reported by US Census Department•Major Factors: Facial pain/pressure, congestion, nao, discolored discharge, hyposmia, pus, fever•Minor Factors: H/A, fever, halitosis, fatigue, dental pain, cough, ear pain/fullness

4
Topical Intranasal Medications
5
Topical Intranasal Medications••3% NaCl more effective than 0.9% NaCl 3% NaCl more effective than 0.9% NaCl in vivo in vivo (Talbot, 1997)(Talbot, 1997)••Lactated Ringers only solution that does NOT Lactated Ringers only solution that does NOT affect Mucociliary clearance affect Mucociliary clearance in vitroin vitro; 7% NaCl ; 7% NaCl causes complete, partially reversible ciliostasiscauses complete, partially reversible ciliostasis(Boek, 1999)(Boek, 1999)••Alkaline milieu thought to lend to “sol” state; no Alkaline milieu thought to lend to “sol” state; no supporting datasupporting data••Bactroban only FDABactroban only FDA--approved intranasal approved intranasal antimicrobial; safety of others not establishedantimicrobial; safety of others not established

6
Immunodeficiency•• When to suspectWhen to suspect
–– Recurrent acute RS not attributable to other causeRecurrent acute RS not attributable to other cause–– Persistent infection unresponsive to antibioticsPersistent infection unresponsive to antibiotics–– Infections at other sites (pneumonia, sepsis, meningitis)Infections at other sites (pneumonia, sepsis, meningitis)–– Unusual sinus pathogens or severe infectionsUnusual sinus pathogens or severe infections–– Family h/o immunodeficiencyFamily h/o immunodeficiency
•• IgG subclass deficiency (4 subclasses)IgG subclass deficiency (4 subclasses)–– IgG1 IgG1 –– bacterial protein, 67% (Tetanus, DPT)bacterial protein, 67% (Tetanus, DPT)–– IgG2 IgG2 –– bacterial polysaccharide, 23% (bacterial polysaccharide, 23% (H. flu, S. pneumoH. flu, S. pneumo))–– IgG3 IgG3 –– M. CatarrhalisM. Catarrhalis, , S. PyogenesS. Pyogenes

7
Immunodeficiency
8
Immunodeficiency
•• WorkupWorkup–– CBC w/ Dif, HIVCBC w/ Dif, HIV–– Ig concentrations, IgG subclass concentrationsIg concentrations, IgG subclass concentrations–– Test response to DPT, Pneumococcal vaccineTest response to DPT, Pneumococcal vaccine–– +/+/-- TT--cell function (cell function (in vitro > in vivo)in vitro > in vivo)–– +/+/-- CHCH--5050
•• 53.3% abnormal T53.3% abnormal T--cell function (Cheep, 2001)cell function (Cheep, 2001)•• IgA deficiency (40%),CVID (25%)(Sethi, 1995)IgA deficiency (40%),CVID (25%)(Sethi, 1995)
9
Immunodeficiency
•• TreatmentTreatment–– IVIG: CVID, Total IgG deficiency, IgG subclass IVIG: CVID, Total IgG deficiency, IgG subclass
deficiency WITH decreased response to vaccinedeficiency WITH decreased response to vaccine–– LongLong--term antibiotic prophylaxis (Augmentin 500 mg term antibiotic prophylaxis (Augmentin 500 mg
QD)QD)–– Genetic counseling/testing of familyGenetic counseling/testing of family

10
Cystic Fibrosis•• Most common lethal Auto Recessive disease in Most common lethal Auto Recessive disease in
CaucasiansCaucasians•• 1:2,000 live births; carrier rate 1:201:2,000 live births; carrier rate 1:20--2525•• Thick, exocrine mucus causing mucostasisThick, exocrine mucus causing mucostasis•• CFTR gene on 7q31 affecting chloride channel; CFTR gene on 7q31 affecting chloride channel;
DeltaDelta--F508 F508 –– 70% of CF mutations70% of CF mutations•• Chronic endobronchial infections, progressive Chronic endobronchial infections, progressive
COPD, pancreatic insufficiency, male infertility, and COPD, pancreatic insufficiency, male infertility, and CRS +/CRS +/-- polyposis (up to ½)polyposis (up to ½)

11
Cystic Fibrosis
•• <10% report troubling nasal sx; 12% vs 71% anosmia<10% report troubling nasal sx; 12% vs 71% anosmia•• Dx: 2 + sweat tests (>60 mmol/L), or 1 + sweat test Dx: 2 + sweat tests (>60 mmol/L), or 1 + sweat test
and 2 CF mutations and 2 CF mutations •• False positives: AI, Anorexia, Hypothyroidism, Low False positives: AI, Anorexia, Hypothyroidism, Low
IgIg
12
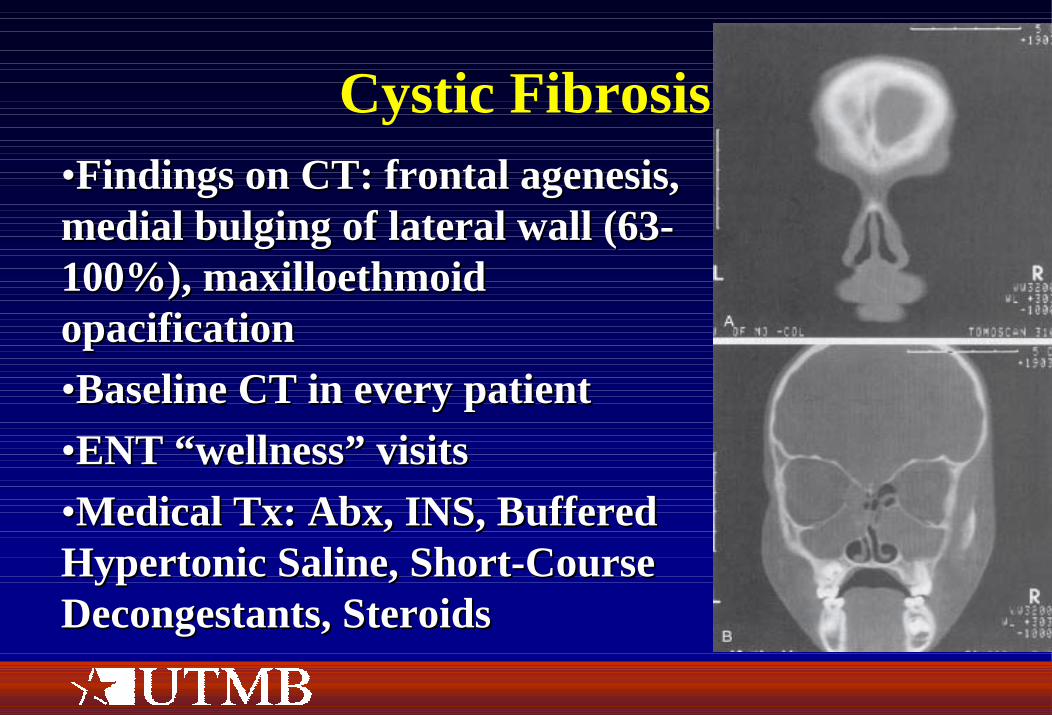
Cystic Fibrosis••Findings on CT: frontal agenesis, Findings on CT: frontal agenesis, medial bulging of lateral wall (63medial bulging of lateral wall (63--100%), maxilloethmoid 100%), maxilloethmoid opacificationopacification••Baseline CT in every patientBaseline CT in every patient••ENT “wellness” visitsENT “wellness” visits••Medical Tx: Abx, INS, Buffered Medical Tx: Abx, INS, Buffered Hypertonic Saline, ShortHypertonic Saline, Short--Course Course Decongestants, SteroidsDecongestants, Steroids
13
Cystic Fibrosis•• Indications for Surgery:Indications for Surgery:
–– Persistent NAO despite medsPersistent NAO despite meds–– Medialized lateral nasal wallMedialized lateral nasal wall–– Worsening pulmonary status or lung problems Worsening pulmonary status or lung problems
associated with sinonasal problemsassociated with sinonasal problems–– Facial pain or H/A affecting QOLFacial pain or H/A affecting QOL
•• Double CFTR mutations associated w/ CRS in nonDouble CFTR mutations associated w/ CRS in non--CF patients (Wang, 2000)CF patients (Wang, 2000)
•• CFTR mistrafficking associated w/ CRS in children CFTR mistrafficking associated w/ CRS in children (Coltrera, 1999)(Coltrera, 1999)

14
Allergic Fungal Rhinosinusitis••First described by First described by Safirstein, 1976Safirstein, 1976••Analogous to Allergic Analogous to Allergic Bronchopulmonary Bronchopulmonary Aspergillosis (ABPA)Aspergillosis (ABPA)••Molds=Hyphae, Molds=Hyphae, Yeasts=Spores, Yeasts=Spores, Pseudohyphae=Chain of Pseudohyphae=Chain of sporesspores
••Dematiaceous fungi: Bipolaris, Alternaria, Dematiaceous fungi: Bipolaris, Alternaria, Cladosporium, Curvularia, Drechslera, ExserohilumCladosporium, Curvularia, Drechslera, Exserohilum

15
Allergic Fungal Rhinosinusitis
•• 55--10% of CRS cases, though marked 10% of CRS cases, though marked geographical variation; common in warm, humid geographical variation; common in warm, humid climatesclimates
•• AR (67%), Asthma (50%)AR (67%), Asthma (50%)•• Early=gradual NAO, semisolid nasal crusts; Early=gradual NAO, semisolid nasal crusts;
Late=extensive nasal polyposis, CRS (1/2 unilat)Late=extensive nasal polyposis, CRS (1/2 unilat)•• Pain is uncommon (suggests bacterial infection)Pain is uncommon (suggests bacterial infection)
16
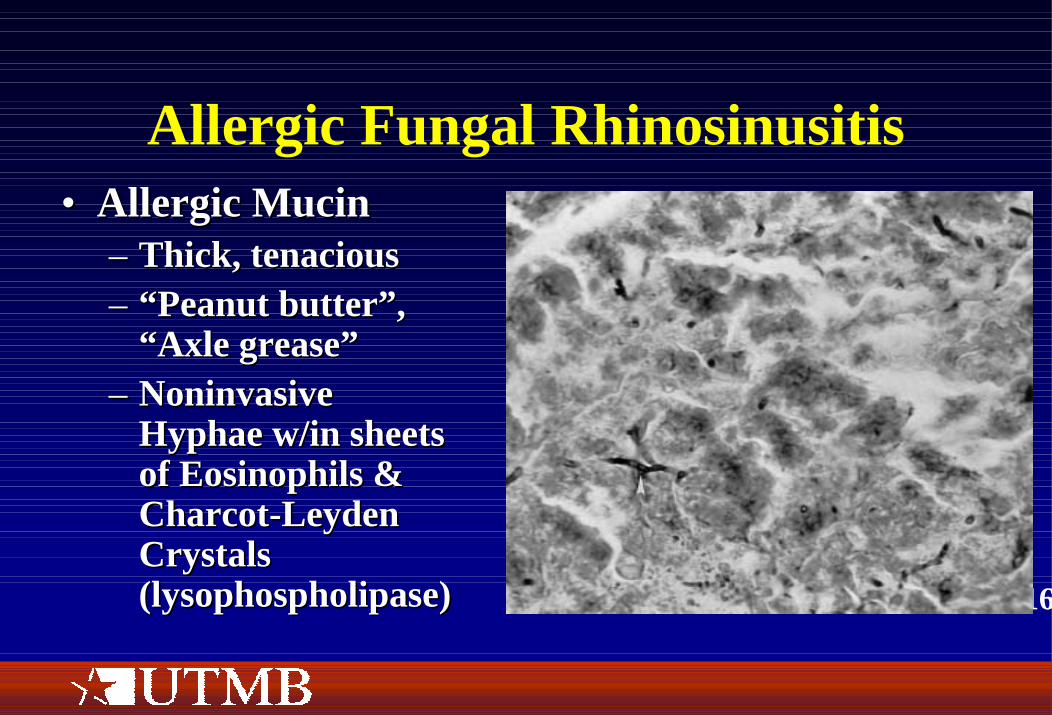
Allergic Fungal Rhinosinusitis•• Allergic MucinAllergic Mucin
–– Thick, tenaciousThick, tenacious–– “Peanut butter”, “Peanut butter”,
“Axle grease”“Axle grease”–– Noninvasive Noninvasive
Hyphae w/in sheets Hyphae w/in sheets of Eosinophils & of Eosinophils & CharcotCharcot--Leyden Leyden Crystals Crystals (lysophospholipase)(lysophospholipase)
17
Allergic Fungal Rhinosinusitis
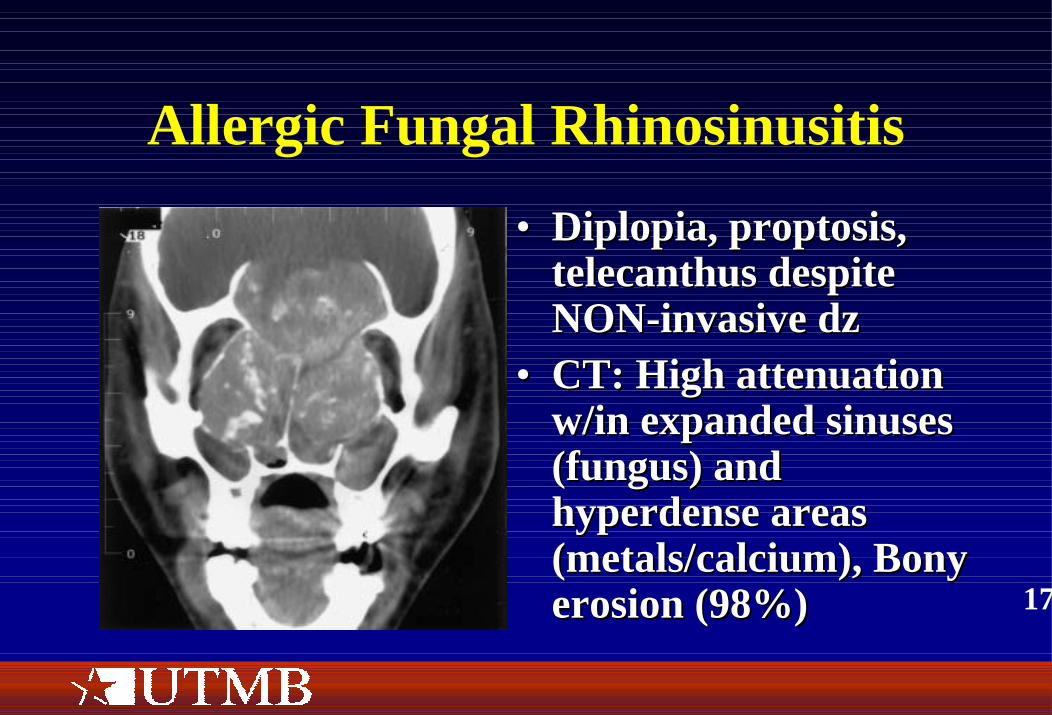
•• Diplopia, proptosis, Diplopia, proptosis, telecanthus despite telecanthus despite NONNON--invasive dzinvasive dz
•• CT: High attenuation CT: High attenuation w/in expanded sinuses w/in expanded sinuses (fungus) and (fungus) and hyperdense areas hyperdense areas (metals/calcium), Bony (metals/calcium), Bony erosion (98%)erosion (98%)
18
Allergic Fungal Rhinosinusitis
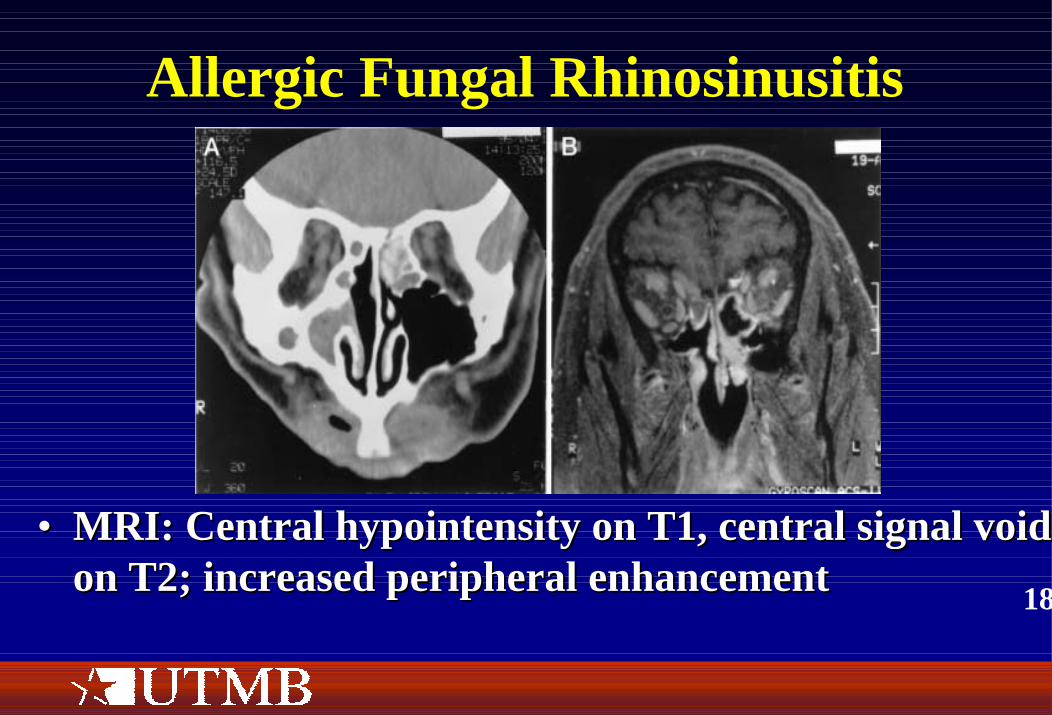
•• MRI: Central hypointensity on T1, central signal voidMRI: Central hypointensity on T1, central signal void on T2; increased peripheral enhancementon T2; increased peripheral enhancement
19
Allergic Fungal Rhinosinusitis
•• Diagnosis (Bent and Kuhn Criteria, 1994):Diagnosis (Bent and Kuhn Criteria, 1994):–– TypeType--I HypersensitivityI Hypersensitivity–– Nasal PolyposisNasal Polyposis–– Characteristic CT signsCharacteristic CT signs–– Eosinophilic mucus without fungal invasion Eosinophilic mucus without fungal invasion –– Positive fungal stain and/or fungal culturePositive fungal stain and/or fungal culture

20
Allergic Fungal Rhinosinusitis
•• Treatment (3 points of attack)Treatment (3 points of attack)–– Atopy: Immunotherapy (must be initiated POSTAtopy: Immunotherapy (must be initiated POST--
operatively)operatively)–– Remove antigenic burden: FESS, antifungal meds Remove antigenic burden: FESS, antifungal meds
(Itraconazole(Itraconazole--$$$$$$$$$$$)$$$$$$$$$$$)–– Halt inflammatory cascade: Topical and systemic Halt inflammatory cascade: Topical and systemic
corticosteroidscorticosteroids
•• Total serum IgE used to monitor dzTotal serum IgE used to monitor dz
21
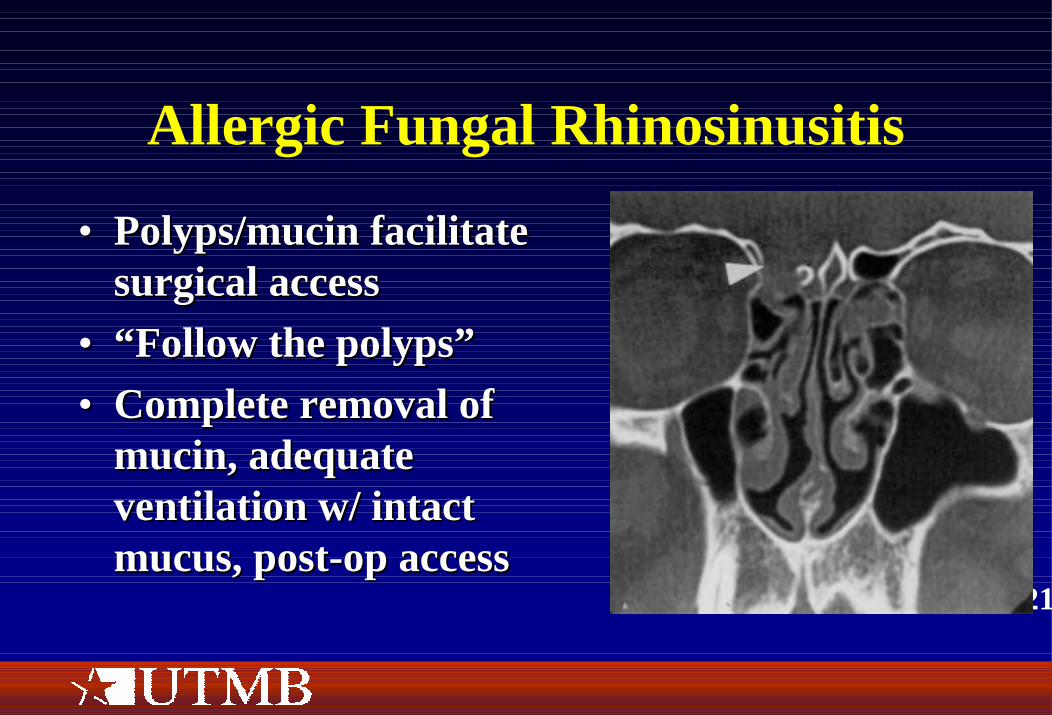
Allergic Fungal Rhinosinusitis
•• Polyps/mucin facilitate Polyps/mucin facilitate surgical accesssurgical access
•• “Follow the polyps”“Follow the polyps”•• Complete removal of Complete removal of
mucin, adequate mucin, adequate ventilation w/ intact ventilation w/ intact mucus, postmucus, post--op accessop access

22
Allergic Fungal Rhinosinusitis
23
Allergic Fungal Rhinosinusitis•• Fungal panFungal pan--antigen?antigen?•• THE CONTROVERSYTHE CONTROVERSY
–– Ponikau, 1999: 96% of CRS patients grew out fungus; Ponikau, 1999: 96% of CRS patients grew out fungus; 100% of healthy controls grew out fungus; 93% of surgical 100% of healthy controls grew out fungus; 93% of surgical pt’s met their criteria for AFRS (excluded atopy)pt’s met their criteria for AFRS (excluded atopy)
–– If IgEIf IgE--mediated, then why unilateral?mediated, then why unilateral?–– Immunotherapy works, but not by changing fungalImmunotherapy works, but not by changing fungal--specific specific
IgEIgE–– IgG immune complexes have not been foundIgG immune complexes have not been found–– TH2 CDTH2 CD--4 cells4 cells

24
Allergic Fungal Rhinosinusitis
Schubert, 2001

25
Case Study
•• 12 yo female with chronic 12 yo female with chronic cough, referred by PCPcough, referred by PCP
26
Case Study
•• History: No sinonasal complaints, denies History: No sinonasal complaints, denies allergic rhinitis. Previous hospitalization for allergic rhinitis. Previous hospitalization for pneumonia. pneumonia.
•• Family hx: Maternal grandfather died from Family hx: Maternal grandfather died from “pneumonia” at age 32“pneumonia” at age 32
•• PMH/PSH: Asthma, No prior surgeriesPMH/PSH: Asthma, No prior surgeries•• Physical exam: Small for age, widened nasal Physical exam: Small for age, widened nasal
bridgebridge
27
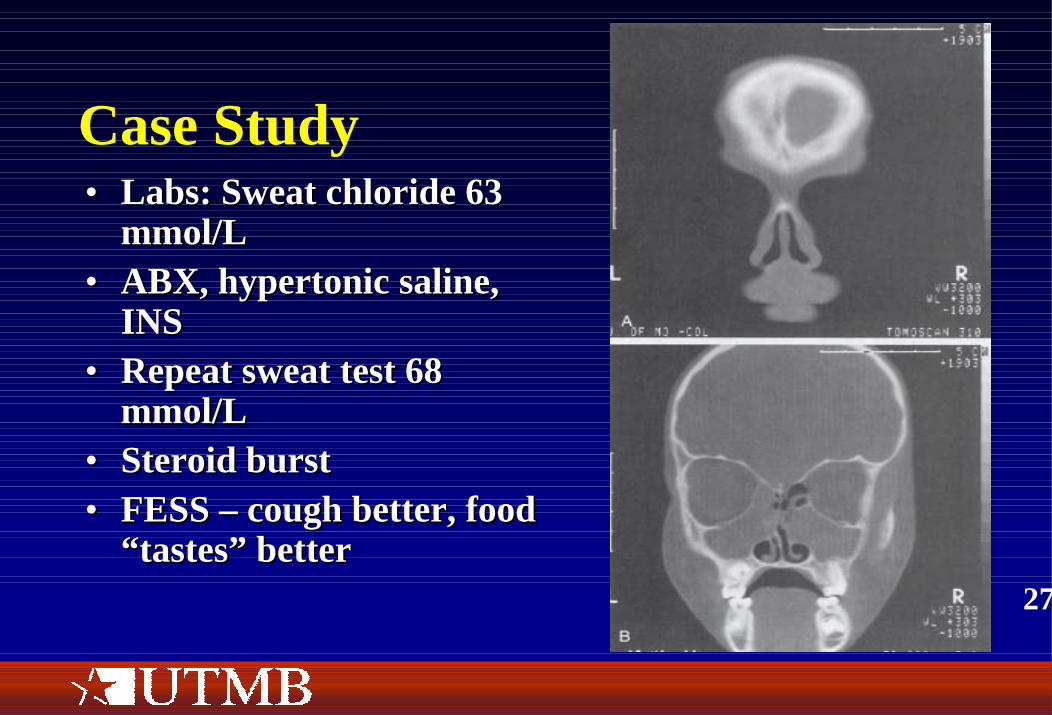
Case Study•• Labs: Sweat chloride 63 Labs: Sweat chloride 63
mmol/Lmmol/L•• ABX, hypertonic saline, ABX, hypertonic saline,
INSINS•• Repeat sweat test 68 Repeat sweat test 68
mmol/Lmmol/L•• Steroid burstSteroid burst•• FESS FESS –– cough better, food cough better, food
“tastes” better“tastes” better