Embed Size (px)
Citation preview
Otolaryngology–Head and Neck Surgery (2007) 136, 252-257
ORIGINAL RESEARCH
Systemic corticosteroids for allergic fungal
rhinosinusitis and chronic rhinosinusitis with nasal
polyposis: A comparative study
Roee Landsberg, MD, Yoram Segev, MD, Ari DeRowe, MD,
Tali Landau, MD, Avi Khafif, MD, and Dan M. Fliss, MD, Tel-Aviv, IsraelOBJECTIVES: To compare the effect of preoperative high-dosesystemic corticosteroids on the radiographic and endoscopic ap-pearance of allergic fungal rhinosinusitis (AFRS) and chronicrhinosinusitis with nasal polyposis (CRSwNP).STUDY DESIGN AND SETTING: Eight AFRS and 10CRSwNP patients underwent computed tomographic (CT) scansand then received preoperative 1 mg/kg prednisone for 10 days.CT scans were repeated 1 day before surgery and compared withpretreatment scans (Lund-MacKay radiologic scoring system). Theendoscopic appearance was recorded intraoperatively.RESULTS: The score dropped from 16 (66.4%) to 4.75 in theAFRS group and from 18.4 (23%) to 14.1 in the CRSwNP group(P � 0.0064). Intraoperatively, most sinus mucosal surfaces ap-peared normal in the AFRS patients but were markedly edematousin the CRSwNP patients.CONCLUSION: Radiographic response of AFRS to systemiccorticosteroids is significantly greater compared with CRSwNP.This finding is supported by endoscopic observation.© 2007 American Academy of Otolaryngology–Head and NeckSurgery Foundation. All rights reserved.
Systemic corticosteroids (steroids) are an important partof the medical arsenal used for the treatment of chronic
rhinosinusitis with nasal polyposis (CRSwNP).1 It is wellrecognized that these potent anti-inflammatory agents in-duce a reduction in the polyps’ volume and consequentlysignificantly improve the patients’ nasal breathing and senseof smell. Systemic steroids also have an important role inthe treatment of allergic fungal rhinosinusitis (AFRS) and,as an adjuvant to surgery, steroids have been established as
From the Departments of Otolaryngology–Head and Neck Surgery (DrsLandsberg, DeRowe, Khafif, and Fliss) and Radiology (Dr Segev), Tel-AvivSourasky Medical Center, and the Department of Otolaryngology–Head andNeck Surgery (Dr Landau), Sapir Medical Center, Kfar Sava, affiliated with
the Sackler Faculty of Medicine, Tel-Aviv University.0194-5998/$32.00 © 2007 American Academy of Otolaryngology–Head and Necdoi:10.1016/j.otohns.2006.09.010
an essential medical remedy as a result of their strong effecton the extent of inflammation.2
AFRS has evolved into a distinct entity with its owndiagnostic criteria that have clearly differentiated it fromCRSwNP.3-5 Recent studies, however, have claimed that thevast majority of chronic rhinosinusitis (CRS) represent animmune-mediated response to the presence of fungi.6,7
These new views hold that the term allergic fungal rhino-sinusitis is a misnomer and that patients thought to have thisdisorder are merely a part of the larger group of patientswith CRS. It was proposed to eliminate the term allergicand instead to use the term eosinophilic fungal rhinosinus-itis (EFRS) to describe most patients who have CRS.8
We will attempt to challenge this new trend in the currentstudy. It is our experience that patients with CRS do notrepresent a homogenous group whereas the traditional di-agnostic criteria for AFRS define a very distinct group ofpatients. We were impressed by the extent of the radio-graphic and endoscopic response of AFRS to systemic ste-roids. Our literature search failed to retrieve any studies thatquantify this response.
We now compare the objective effects of preoperativehigh-dose systemic steroids on the radiographic and endo-scopic appearance of AFRS and CRSwNP.
MATERIALS AND METHODS
This prospective study was conducted by the Otolaryngol-ogy Head and Neck Surgery and Radiology Departments of
Reprint requests: Roee Landsberg, MD, Department of Otolaryngology–Head and Neck Surgery, Tel-Aviv Sourasky Medical Center, 6 WeizmanStreet, Tel-Aviv 64239, Israel.
E-mail address: [email protected].
k Surgery Foundation. All rights reserved.
253Landsberg et al Systemic corticosteroids for allergic fungal . . .
the Tel-Aviv Sourasky Medical Center (Israel) during 2001through 2004. The study protocol was approved by the localIRB committee.
AFRS Patients’ CharacteristicsThe diagnosis of AFRS was based on Bent and Kuhn’scriteria3: 1) type 1 hypersensitivity, 2) nasal polyposis, 3)characteristic computed tomography (CT) scans, 4) eosino-philic mucus without fungal invasion into sinus tissue, and5) positive fungal stain or sinus contents removed duringsurgery. Unilateral predominance, radiographic bone ero-sion, and positive fungal culture were not necessary butserved to support the diagnosis of AFRS. A total of 14patients met these criteria and 8 of them (5 males, 3 females;mean age, 23 years; range, 14 to 38 years) were treatedaccording to the study protocol and comprise the AFRSgroup. Two patients had been previously operated; 1 patienthad undergone an external frontotomy and radical ethmoid-ectomy with a coronal flap, and the other had undergone 3operations in another institution (endoscopic sinus surgery[ESS] twice and a frontal osteoplastic flap surgery). All 8patients had nasal polyps, characteristic CT findings (hy-perdensities, expansion, remodeling, bone erosion) and IgEhypersensitivity (mean total, IgE 1690 IU/mL; range, 428 to8331). Allergic mucin (histologically containing fungal hy-phae and degranulating eosinophils) was harvested duringsurgery and identified in 7 patients but not in the 8th patientbecause of complete resolution after high-dose systemicsteroid treatment. Six patients had unilateral disease; 2 pa-tients had asthma.
CRSwNP Patients’ CharacteristicsThe criteria for selecting CRSwNP patients were: 1) bilat-eral complete or near complete nasal obstruction by polypsas verified by rhinoscopy or endoscopy, 2) bilateral nasalcavity and sinus complete or near-complete opacification byCT scan, 3) absence of CT findings characteristic for AFRS, 4)absence of IgE hypersensitivity (mean total IgE 70 IU/mL,range 30-105), and 5) absence of Samter‘s triade (nasalpolyposis, asthma, aspirin sensitivity). Ten consecutive pa-tients who fulfilled these criteria (6 males, 4 females; meanage, 47 years; range, 38 to 65 years) comprised theCRSwNP group. Three patients had asthma. Four patientshad previously undergone between 1 and 3 nasal operations,including nasal polypectomies and ESS.
Study ProtocolAll 18 patients were scheduled for ESS after CTs of theparanasal sinuses. They all had been treated preoperativelyby oral prednisone 1 mg/kg (50 to 80 mg/day) and oralantacids for 10 days. Topical steroids were not used. CTscans were repeated 1 day before surgery and comparedwith pretreatment scans by an experienced neuroradiologist(YS) with the use of the Lund-MacKay radiologic scoringsystem.9 All the ESS procedures included middle antros-
tomy and total ethmoidectomy. Seven of the AFRS patientsand 7 of the CRSwNP patients underwent frontal sinusot-omy; 5 AFRS patients and 7 CRSwNP patients underwentsphenoidectomy. The endoscopic appearance was recordedintraoperatively for each patient. Recorded features in-cluded mucosa (normal or edematous), polyps (absent,present, diffuse), frontal and sphenoethmoidal recesses(normal, narrow or wide), ostium diameter (normal, narrow,or wide), sinus volume (normal or expanded), sinus shape(normal or remodeled), dura (hidden or exposed) and mac-roscopic allergic mucin (present or absent). After taperingthe dose, systemic steroids were halted 6 to 9 days postop-eratively.
Statistic AnalysisComparison between the percentage changes in poststeroidLund-MacKay scores for the CRSwNP and AFRS groupswas performed with the Mann-Whitney nonparametric test.A sample of 9 CT studies (108 sinuses) was analyzed forinterobserver agreement (YS, RL), and the strength ofagreement was evaluated by the Kappa value.
RESULTS
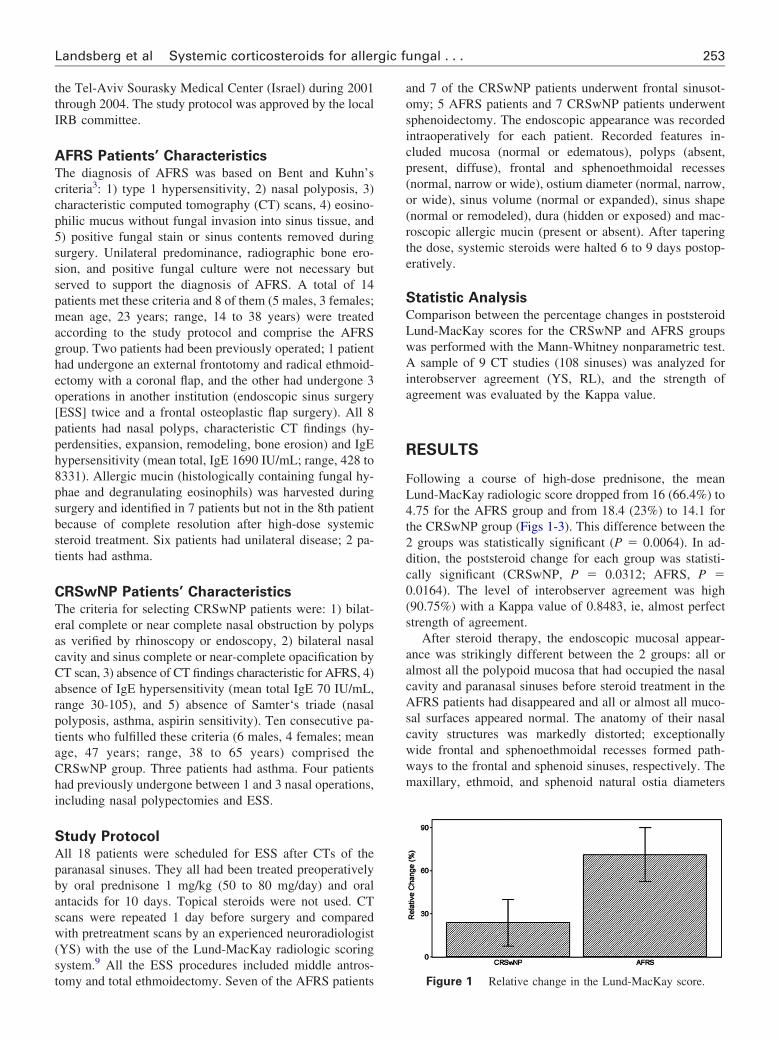
Following a course of high-dose prednisone, the meanLund-MacKay radiologic score dropped from 16 (66.4%) to4.75 for the AFRS group and from 18.4 (23%) to 14.1 forthe CRSwNP group (Figs 1-3). This difference between the2 groups was statistically significant (P � 0.0064). In ad-dition, the poststeroid change for each group was statisti-cally significant (CRSwNP, P � 0.0312; AFRS, P �0.0164). The level of interobserver agreement was high(90.75%) with a Kappa value of 0.8483, ie, almost perfectstrength of agreement.
After steroid therapy, the endoscopic mucosal appear-ance was strikingly different between the 2 groups: all oralmost all the polypoid mucosa that had occupied the nasalcavity and paranasal sinuses before steroid treatment in theAFRS patients had disappeared and all or almost all muco-sal surfaces appeared normal. The anatomy of their nasalcavity structures was markedly distorted; exceptionallywide frontal and sphenoethmoidal recesses formed path-ways to the frontal and sphenoid sinuses, respectively. Themaxillary, ethmoid, and sphenoid natural ostia diameters
Figure 1 Relative change in the Lund-MacKay score.
254 Otolaryngology–Head and Neck Surgery, Vol 136, No 2, February 2007
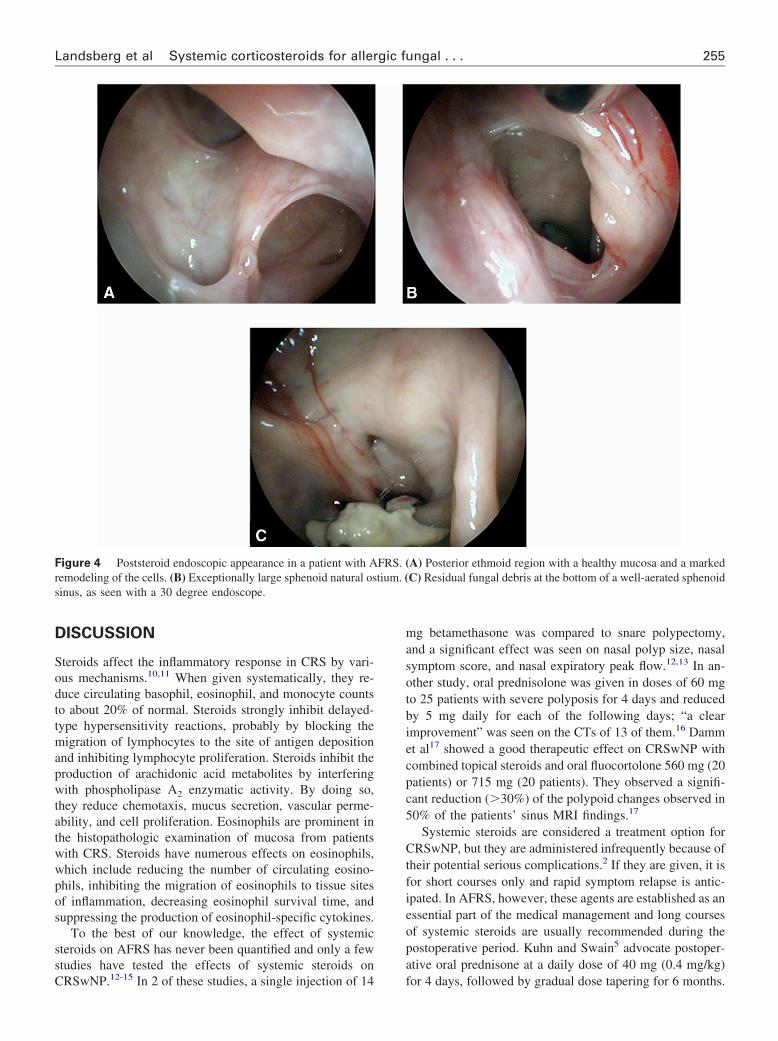
were abnormally larger. All patients had sinus expansion.The ethmoid intersinus septae had vanished and appeared tobe replaced by unusual cavity formations (remodeling).Structures that are usually hidden were found freely ex-posed to sinuses lumen in 4 cases; they included the duraposterior to the frontal sinus posterior table, the dura pos-terior to the dorsum sella, the dura above the posteriorethmoid, and the posterior ethmoid artery. Limited amountsof polypoid or edematous mucosa were found in remotesinuses adjacent to small foci of yellowish inspissated ma-terial that was later confirmed to have hyphae and abundanteosinophils, ie, allergic mucin (Fig 4).
In the CRSwNP group, although it had significantly shrunk,most of the polypoid mucosa that had occupied the nasal cavityand paranasal sinuses before steroid treatment was still present.The polyps appeared denser and felt firmer than their prester-oid state. The mucosa of the maxillary, frontal, and sphenoid
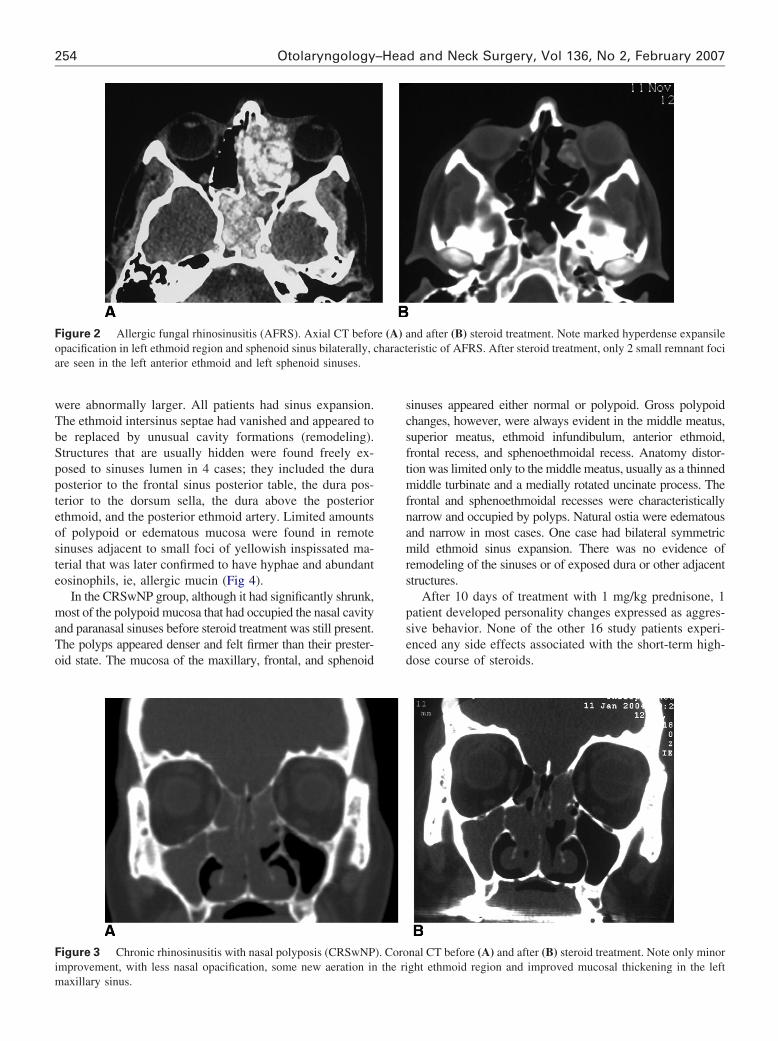
Figure 2 Allergic fungal rhinosinusitis (AFRS). Axial CT beforopacification in left ethmoid region and sphenoid sinus bilaterally, care seen in the left anterior ethmoid and left sphenoid sinuses.
Figure 3 Chronic rhinosinusitis with nasal polyposis (CRSwNPimprovement, with less nasal opacification, some new aeration in
maxillary sinus.sinuses appeared either normal or polypoid. Gross polypoidchanges, however, were always evident in the middle meatus,superior meatus, ethmoid infundibulum, anterior ethmoid,frontal recess, and sphenoethmoidal recess. Anatomy distor-tion was limited only to the middle meatus, usually as a thinnedmiddle turbinate and a medially rotated uncinate process. Thefrontal and sphenoethmoidal recesses were characteristicallynarrow and occupied by polyps. Natural ostia were edematousand narrow in most cases. One case had bilateral symmetricmild ethmoid sinus expansion. There was no evidence ofremodeling of the sinuses or of exposed dura or other adjacentstructures.
After 10 days of treatment with 1 mg/kg prednisone, 1patient developed personality changes expressed as aggres-sive behavior. None of the other 16 study patients experi-enced any side effects associated with the short-term high-dose course of steroids.
nd after (B) steroid treatment. Note marked hyperdense expansileeristic of AFRS. After steroid treatment, only 2 small remnant foci
nal CT before (A) and after (B) steroid treatment. Note only minorght ethmoid region and improved mucosal thickening in the left
e (A) aharact
). Corothe ri
255Landsberg et al Systemic corticosteroids for allergic fungal . . .
DISCUSSION
Steroids affect the inflammatory response in CRS by vari-ous mechanisms.10,11 When given systematically, they re-duce circulating basophil, eosinophil, and monocyte countsto about 20% of normal. Steroids strongly inhibit delayed-type hypersensitivity reactions, probably by blocking themigration of lymphocytes to the site of antigen depositionand inhibiting lymphocyte proliferation. Steroids inhibit theproduction of arachidonic acid metabolites by interferingwith phospholipase A2 enzymatic activity. By doing so,they reduce chemotaxis, mucus secretion, vascular perme-ability, and cell proliferation. Eosinophils are prominent inthe histopathologic examination of mucosa from patientswith CRS. Steroids have numerous effects on eosinophils,which include reducing the number of circulating eosino-phils, inhibiting the migration of eosinophils to tissue sitesof inflammation, decreasing eosinophil survival time, andsuppressing the production of eosinophil-specific cytokines.
To the best of our knowledge, the effect of systemicsteroids on AFRS has never been quantified and only a fewstudies have tested the effects of systemic steroids on
Figure 4 Poststeroid endoscopic appearance in a patient with Aremodeling of the cells. (B) Exceptionally large sphenoid natural ossinus, as seen with a 30 degree endoscope.
CRSwNP.12-15 In 2 of these studies, a single injection of 14
mg betamethasone was compared to snare polypectomy,and a significant effect was seen on nasal polyp size, nasalsymptom score, and nasal expiratory peak flow.12,13 In an-other study, oral prednisolone was given in doses of 60 mgto 25 patients with severe polyposis for 4 days and reducedby 5 mg daily for each of the following days; “a clearimprovement” was seen on the CTs of 13 of them.16 Dammet al17 showed a good therapeutic effect on CRSwNP withcombined topical steroids and oral fluocortolone 560 mg (20patients) or 715 mg (20 patients). They observed a signifi-cant reduction (�30%) of the polypoid changes observed in50% of the patients’ sinus MRI findings.17
Systemic steroids are considered a treatment option forCRSwNP, but they are administered infrequently because oftheir potential serious complications.2 If they are given, it isfor short courses only and rapid symptom relapse is antic-ipated. In AFRS, however, these agents are established as anessential part of the medical management and long coursesof systemic steroids are usually recommended during thepostoperative period. Kuhn and Swain5 advocate postoper-ative oral prednisone at a daily dose of 40 mg (0.4 mg/kg)
A) Posterior ethmoid region with a healthy mucosa and a markedC) Residual fungal debris at the bottom of a well-aerated sphenoid
FRS. (tium. (
for 4 days, followed by gradual dose tapering for 6 months.

256 Otolaryngology–Head and Neck Surgery, Vol 136, No 2, February 2007
The purpose in maintaining the patients on prednisone for along period was to allow the mucous clearance mechanismstime to completely clear the sinuses from remnants of fun-gal hyphae not removed by surgery. The use of systemicsteroid therapy 1 to 2 weeks before surgery to shrink thenasal polyps, reduce mucosal inflammation, and decreaseblood loss is less often recommended.18 The common prac-tice to administer systemic steroids only postoperatively isbased on the assumption that preoperative steroids mayconfuse the diagnosis of AFRS and cause resolution of thetypical allergic mucin required for histopathologic diagnosisof the disease.19
In 1999, a hypothesis of CRS was proposed by Ponikauet al6 who suggested that colonizing fungi in sinus mucusplay a much broader role in the pathogenesis of CRS. Withthe use of an innovative culture technique, 93% of 101consecutive patients with CRS demonstrated positive fungalcultures from nasal lavage. Examination of surgically ob-tained specimens from these patients also revealed eosino-phils and fungal hyphae in the sinus mucus of nearly allpatients. It was also observed that 100% of a group ofhealthy control subjects had positive fungal cultures fromnasal lavage. Conventional IgE-mediated allergy to fungiwas not consistently observed in the patients with CRS. Theauthors proposed that CRS was associated with sensitizationto colonizing fungi in virtually all patients. It was furthersuggested that the term allergic fungal sinusitis be replacedwith eosinophilic fungal rhinosinusitis.8 Part of the consid-erable controversy that these new views created seems tostem from the fact that an inflammatory process stimulatedby fungal hyphae had previously been implicated in only asmall subset of cases defined as AFRS. The proposal byPonikau et al6 to redefine CRS as eosinophilic fungal rhi-nosinusitis seems to dismiss the importance of defining aunique group of patients.
Our study shows that the radiographic response ofAFRS to systemic steroids is much greater comparedwith CRSwNP. Our endoscopic observation, albeit subjec-tive, supports this finding. With the knowledge that steroidshave a major effect on the production, migration, and acti-vation of eosinophils, we speculate that eosinophils mayplay a key role in that response. In CRSwNP, nasal polypsare characterized by eosinophilic inflammation within themucosa.20 In AFRS, however, as demonstrated by imagingand observed during surgery, large amounts of allergic mu-cin occupying the sinuses lumen and containing numerouseosinophils are the hallmark of the disease. It is possible thatedema and polyps subside under steroid treatment and aninflux of malfunctioning eosinophils exits the sinusesthrough the typically widened ostia and recesses. Theseenlarged pathways, caused by the expansible nature of theaccumulating mucin, probably serve as a key factor in thealmost complete recovery of sinus cavities under steroidinfluence. Only sparse foci of allergic mucin and fungaldebris are trapped within blocked sinus cells and are left for
surgical extirpation.Preoperative treatment with high-dose steroids providedthe endoscopic surgeon a surgical field that was much easierto control. In addition, it was now possible to performendoscopic surgery targeted to allergic mucin foci remnantsaccording to their precise location, as seen on the post-steroid CT scan. As initial observation, it appears that thismanagement improves the outcome of these patients whencompared with the outcome of alternative approaches de-scribed in published data. Targeted surgery reduces opera-tion time and can obviate unnecessary extensive surgerywith the potential associated complications. Long-term ef-ficiency of this treatment protocol awaits future studies.
The exclusion of aspirin-sensitive patients and allergicpatients from the control group was done for the sake ofcomparing 2 relatively homogenous groups. Individualswith aspirin sensitivity comprise a well-known subgroup ofpatients that represents only about 2% to 7% of the patientswith nasal polyposis.21,22 The goal of this study was to com-pare AFRS with the vast majority of patients with nasal pol-yposis who do not have aspirin sensitivity. In a recent study,Alobid et al23 demonstrated that no significant differences innasal symptoms, polyp size, and quality of life between aspi-rin-tolerant and aspirin-sensitive patients with asthma werefound before and after a short course of oral steroids or long-term intranasal steroid treatment. As such, it is not likely thatadding aspirin-sensitive patients to the control group wouldhave changed our study results significantly.
Similarly, since type 1 hypersensitivity is a criterion inthe “classic AFRS” criteria, we excluded patients with type1 hypersensitivity from the NP control group. In his 2002study, Kirtsreesakul24 demonstrated that nasal polyps withpositive allergen skin test showed less improvement com-pared with nasal polyps with negative allergen skin test.Again, it is unlikely that adding patients with allergy and NPwould have reduced the significance of our findings.
The results of this study do not support the concept thatAFRS is a misnomer and that patients with AFRS merelyconstitute a part of the large group of CRS or eosinophilicrhinosinusitis patients. Besides the well-defined AFRS clas-sical criteria, our findings add radiographic and mucosalresponse to systemic steroids as distinctive characteristics ofthis unique disease. While newer studies contend that apositive fungal smear and degranulating eosinophils are notspecific to AFRS, we find our observation a useful clinicaladdition to its diagnosis.
CONCLUSIONS
Radiographic and mucosal responses of AFRS to systemicsteroids are significantly greater compared with CRSwNP.Targeting surgery to the location of residual disease afterhigh-dose steroids makes possible a minimally invasiveESS approach.
We thank Esther Eshkol for editorial assistance.

257Landsberg et al Systemic corticosteroids for allergic fungal . . .
REFERENCES
1. Settipane GA. Nasal polyps: epidemiology, pathology, immunology,and treatment. Am J Rhinol 1987;1:119–26. (Grade D).
2. Ferguson BJ. What role do systemic corticosteroids, immunotherapy,and antifungal drugs play in the therapy of allergic fungal sinusitis?Arch Otolaryngol Head Neck Surg 1998;124:1174–7. (Grade D).
3. Bent JP, Kuhn FA. Diagnosis of allergic fungal sinusitis. OtolaryngolHead Neck Surg 1994;111:580–8. (Grade D).
4. Kuhn FA, Javer AR. Allergic fungal sinusitis: our experience. ArchOtolaryngol Head Neck Surg 1998;124:1179–80. (Grade D).
5. Kuhn FA, Swain R. Allergic fungal sinusitis: diagnosis and treatment.Curr Opin Otolaryngol Head Neck Surg 2003;11:1–5. (Grade D).
6. Ponikau JU, Sherris DA, Kern EB, et al. The diagnosis and inci-dence of allergic fungal sinusitis. Mayo Clin Proc 1999;74:877– 84.(Grade B).
7. Sasama J, Sheris DA, Shin SH, et al. New paradigm for the roles offungi and eosinophils in chronic rhinosinusitis. Curr Opin OtolaryngolHead Neck Surg 2005;13:2–8. (Grade D).
8. Braun H, Buzina W, Freudenschuss K, et al. Eosinophilic fungalrhinosinusitis: a common disorder in Europe? Laryngoscope 2003;113:264–9. (Grade B).
9. Lund VJ, Kennedy DW. Quantification for staging sinusitis. Ann OtolRhinol Laryngol Suppl 1995;167:17–21. (Grade D).
10. Schleimer RP. Glucocorticosteroids: their mechanism of action anduse in allergic diseases. In: Middelton E, Reed CE, Ellis EF, et al,editors. Allergy: principles and practice, 4th ed. St Louis: CV Mosby;1993. p. 898. (Grade D).
11. Schleimer RP, Bochner BS. The effect of glucocorticosteroids on humaneosinophils. J Allergy Clin Immunol 1994;94:1202–13. (Grade D).
12. Lildholt T, Rudcrantz H, Bende M, et al. Glucocorticoid treatment fornasal polyps: the use of topical budesonide powder, intramuscularbetamethasone, and surgical treatment. Arch Otolaryngol Head Neck
Surg 1997;123:595–600.13. Lildholt T, Fogstrup J, Gammelgaard N, et al. Surgical versusmedical treatment of nasal polyps. Acta Otolaryngol 1988;105:140 –3. (Grade B).
14. Tuncer U, Soylu L, Aydogan B, et al. The effectiveness of steroidtreatment in nasal polyposis. Auris Nasus Larynx 2003;30(3):263–8.(Grade D).
15. Bonfils P, Avan P. Nonspecific bronchial hyperresponsiveness is a riskfactor for steroid insensitivity in nasal polyposis. Acta Otolaryngol2004;124(3):290–6. (Grade B).
16. Van Camp C, Clement PA. Results of oral steroid treatment in nasalpolyposis. Rhinology 1994;32:5–9. (Grade B).
17. Damm M, Jungehusing M, Eckel HE, et al. Effects of systemic steroidtreatment in chronic polypoid rhinosinusitis evaluated with magneticresonance imaging. Otolaryngol Head Neck Surg 1999;120:517–23.(Grade B).
18. Marple BF. Allergic fungal sinusitis: current theories and managementstrategies. Laryngoscope 2001;111:1006–19. (Grade D).
19. Graham SM, Ballas ZK. Preoperative steroids confuse the diagnosis ofallergic fungal sinusitis. J Allergy Clin Immunol 1998;101:139–40.(Grade D).
20. Jankowski R, Bouchoua F, Coffinet L, et al. Clinical factors influenc-ing the eosinophil infiltration of nasal polyps. Rhinology 2002;40:173–8. (Grade D).
21. Moloney JR. Nasal polyps, nasal polypectomy, asthma, and aspirinsensitivity: their association in 445 cases of nasal polyps. J LaryngolOtol 1977;91:837–46. (Grade C).
22. Kennedy DW. Prognostic factors, outcomes and staging in ethmoidsinus surgery. Laryngoscope 1992;102(suppl 57):1–18. (Grade C).
23. Alobid I, Benitez P, Pujols L, et al. Severe nasal polyposis and itsimpact on quality of life: the effect of a short course of oral steroidsfollowed by long-term intranasal steroid treatment. Rhinology 2006;44:8–13. (Grade B).
24. Kirtsreesakul V. Role of allergy in therapeutic response of nasal
polyps. Asian Pac J Allergy Immunol 2002;20(3):141–6. (Grade B).