Embed Size (px)
Citation preview

RHEUMATIC HEART DlSEASE
II. INCIDENCE AND DISTRIBUTION OF THE AGE OF DEATH*
DAYID DAVIS, KD., AND SOMA VEISS, M.D. BOSTON, MASS.
T HE r81e of rheumatic heart disease in the causation of death was discussed in a previous communication.1 The absolute frequency
of rheumatic heart disease was estimated. and an attempt made to differ- entiate between the frequency of death from rheumatic heart disease, the frequency of death in which rheumatic heart disease is a contributing factor, and of death in which rheumatic heart disease is present as a non- contributing and incident,al finding.
Two sets of data are essential to a study of the natural history of rheumatic heart disease : the age distribution and incidence of (a) the first infection, (b) the death of the patients. The determination of the occurrence of t,he first rheumatic infection, particularly of the heart, is difficult. The distribution of the age of death, however. can be determined accurately, and this knowledge is pertinent to clinical and public health problems. The present discussion is therefore concerned with that phase of the subject.
DISTRIBUTION OF TITE BGE OF DEATH IN RHEUMATIC HEART DISEASE
Fig. 1 shows the age distribution in 161 of the total 164 instances of death caused directly by rheumatic heart disease and occurring in a series of 5215 consecutive necropsies performed in the Boston City Hospital between the years 1905 and 1929, inclusive. But fpw deaths occurred in the first decade. The death rate was distributed mainly over t,he second to the seventh decades. The largest number of deaths occurred in the fourth and fifth decades; but as many as 37 cases, or 23 per cent, of the total number of deaths occurred in the sixth and seventh decades. In the third decade t.here was a comparative but perhaps not significant decrease. This fact, that not infrequently rheu- matic heart, disease may be responsible for cleatah as late as the sixth and seventh decades of life, is often not appreciated in clinical medicine.
The age of death in patients dying from rheumatic heart disease was studied in 68 additional cases in which necropsy was not performed. The diagnosis in this group of cases was based on clinical and labora- tory findings. The patients were observed in the Boston City Hospital during the years 1920 to 1929. The clistribntion of the age of deat,h in this group is shown in Fig. 2, and the curve is not significantly different, from that of the 161 necropsied cases. These 68 cases, how- ever, cannot be consiclered as representative as the necropsy series, for
*From the Thorndike Memorial Laboratory, Second and Fourth Medical Services (Harvard), Boston City Hospital and the Department of Medicine, Harvard Medical
School, Boston, Mass. 18‘)

DAVIS ASD WEISS: RHEUMBTIC HEART DISEASE 183
undoubtedly some cases of death from rheumatic heart disease are unrecognized in the absence of postmortem studies. Fig. 3 represents the two groups combined. The combined group, comprising 229 cases, is large enough to permit certain general conclusions concerning the distribution of the age of death in rheumatic heart disease.
Willius’ reported the age distribution of death in 160 cases without necropsy examination, and Coombs3 in 95 cases with necropsy. As
AGE ‘AOU P
Fig. 1. Fig. 2.
Fig. l.--4ge distribution of 161 deaths caused directly by rheumatic heart dis- ease.
Fig. Z.--Age distribution of 68 additional cases of death from rheumatic heart disease in which necropsy was not performed.
Fig. %-Age distribution of 161 autopsied cases of death caused directly by rheu- matic heart disease and of 6S additional cases of death in which autopsy was not performed.
these authors apparently did not determine whether or not death in the respective groups was directly due to rheumatic heart disease, their fig- ures are not comparable to those of Fig. 3.
THE AGE OF DE-\TII TN RHEUMATIC HEART DISEASE COMPLTCATED BY
SUBACUTE BACTERIAL ENDOCARDITIS AND ACUTE
MALIGNANT ESDOC’ARDITIS
A discussion of the incidence of the age distribution of death due to rheumatic heart disease should include those eases which are compli- cated by subacute bacterial endocarditis and acute bacterial endocarditis.

184 THE AMERICAN HENiT JOURNAL
These may be regarded as complications which ordinarily occur on the basis of an old rheumatic infection of the heart. Fig. 4 shows the age variation in the grotrp of deaths from subacute bacterial endocarditjis. This group comprises 47 cases, 35 of which gave morphological or clini- cal and morphological evidence of a rheumatic basis. The remaining 12 cases may also have occurred on a basis of rheumatic heart disease, but this was not noted in the postmortem records. In 6 of these cases
o-9 IO-19 20-29 m-39 40
AGE GROUP AGE GROUP Fig. 4. Fig. 5.
Fig. 4.-Age distribution of 47 deaths caused by subacute bacterial endocarditis. Fig. B.-Age distribution of 18 deaths caused by primary malignant endocarditis.
AGE GROVP
Fig. 6. Fig. 7.
Fig. B.-Age distribution of 236 deaths caused by rheumatic heart disease and by rheumatic heart disease combined with subacute and acute bacterial endocar- ditis.
Fig. ‘I.--Age distribution of all 467 cases in which rheumatic heart disease was present as a contributing or noncontributing factor to death.
a history of rheumatic pains and fever was obtained. Subacute bac- terial endocarditis occurred at all ages from fifteen to seventy-five years. A relatively large number of cases (40 out of 47) occurred before the age of fifty years. This is somewhat in contrast to the small group of cases with acute malignant endocarditis (Fig. 5) in which all deaths occurred before the age of fort,y years.
Fig. 6 represents the age distribution in the group of deaths from rheumatic heart disease and rheumatic heart disease combined with subacute and acute bacterial endocarditis. Ages were available in 223 of a total of 232 of these cases. A definite accentuation of the curve occurs again between the ages of thirty and forty-nine years.

DAVIS AND WEISS: RHEUMATIC HEART DISEASE 185
Fig. 7 shows the age distribution of all cases in which rheumatic heart disease was present, regardless of whether or not rheumatic heart disease caused death directly, contributed to it! or was present as a mere accidental finding. The character of this distribution curve is essentially the same ,as that representing the group of cases in which rheumatic heart disease was the cause of death (Fig. 1).
A COMPARISON OF THE AGE DISTRIBUTION IN CASES WITH RHEU-
MATIC HEART DISEASE WITH THAT OF THE ENTIRE NECROPSY
SER,IES OF 5215 CONSECUTIVE CASES
Fig. 8 shows the age distribution, expressed in percentage of the total numbers, of the 5060 available cases of the 5215 necropsy series. Curves
?
\
h b o-*
\
\
\ \ 22 iO-”
Fig. S.--A, Percentage age distribution of 5060 consecutive deaths, Boston City Hospital (1905-1929). B, Percentage age distribution of total deaths in urban popu- lation of Massachusetts (average for years 1910, 1916, 1922, 1928). C, Percentage age distribution of 161 deaths caused directly by rheumatic heart disease. D, Percentage age distribution of all deaths (467) in which rheumatic heart disease was present.
of the age distribution of all cases with rheumatic cardiac manifestations and all cases with rheumatic cardiac death are shown on the same chart for comparison. Fig. 9 represents the same data espressed in absolute numbers. The distribution of the age of death in these 5060 cases taken from the Boston City Hospital and the average distribution reported by the United States Department of Commerce for the urban population of Massachusetts for 1910, 1916, 1922 and 1928, are indicated in Figs. 8 and 9. Although the two curves are not strictly parallel, there is a fair de- gree of similarity between them. The most outstanding difference is that in the hospital population the deaths predominate between the fourth and seventh decades and are relatively scarce after the seventh decade as corn-

186 THE AMERICAN HEART JOURNAL
pared with the urban population. The probable explanation of this dif- ference lies in the fact that adult, and middle aged people with ailments are likely to enter the hospital for relief, while very old people are in- clined to stay at home until the time of death. Notwithstanding these differences in the age distribution oi the population of the Boston City Hospital and the urban population of Massachusetts, it is felt that with reservations the incidence of rheumatic heart disease in the postmortem series of the Boston City Hospital is roughly applicable to the commn- nity as a whole. The application of the age distribution in these 5060 cases to the population at, large is further warranted by a comparison of the incidence of a disease such as cancer in the necropsy series with that reported by public health statistics for the entire community. The aver-
Fig. 9.-A, Age distribution of 5060 consecutive deaths, Boston City Hospital (1905- 1920). B, Age distribution of total deaths in urban population of Massachusetts (average for years 1910, 1916, 1922, 1928). directly by rheumatic heart disease.
CI Age distribution of 161 deaths caused D, Age distribution of all deaths (467) in which
rheumatic heart disease was present.
age incidence of cancer in the cases on which necropsy examination was performed was 10.4 per cent between the years 1910 and 1928.l The average incidence of cancer in t,he urban population of Massachusetts was 5.58 per cent in 1910, 7.05 per cent in 1916, 9.12 per cent in 1922, and 10.72 per cent in 1928, with an average of 8.12 per cent for the four years. The gradual increase in the incidence of cancer is attributed to the increasing recognition of the disease rather than to its greater inci- dence. Hence the figures for the past decade, with an average of be- tween 9 and 10 per cent, are comparable to the average incidence of cancer in 10.4 per cent of t,hr population of the Boston City Hospital.
A comparative examination of the curves (Fig. 9) reveals that ap- proximately 20 per cent of the total necropsied deaths occurring in the

DAVIS AXD WEISS: RHEUMATIC HEART DIHEbSE 187
second decade show some earmarks of rheumatic heart disease and that 15 per cent of all deaths in this decade are caused by rheumatic heart disease.
This strikingly high percentage is explained by the relatively small number of deat,hs from various causes in the second decade of life and the high incidence of the rheumatic infection in the first and second decades. Thus in 114 cases of rheumatic heart deaths (93 with necrop- sies and 31 without) with a positive rheumatic history, the first symptoms of the infection occurred before the age of twenty-one years in 76 cases (68 per cent). A further contributing factor is the fact that a vast ma- jority of patients with a rheumatic infection occurring in the first decade survive to be exposed to intercurrent disease or die of rheumatic heart disease in the second decade. As indicated before, Fig. 1 shows very few rheumatic deaths in the first decade. The progressive decrease in the percentage of deaths due directly to rheumatic heart disease and the percentage of deaths associated with any degree of rheumatic heart dis- ease is caused mainly by the progressive rise of the incidence of death of the hospital population at large during these decades. There is an apparent rise or stagnation in the seventh decades.
THE PROBABLE DISTRIBUTION OF RHEUMATIC HEART DISEASE AND
RHEUMATIC HEART DEATHS IN BOSTON AND ITS VICINITY
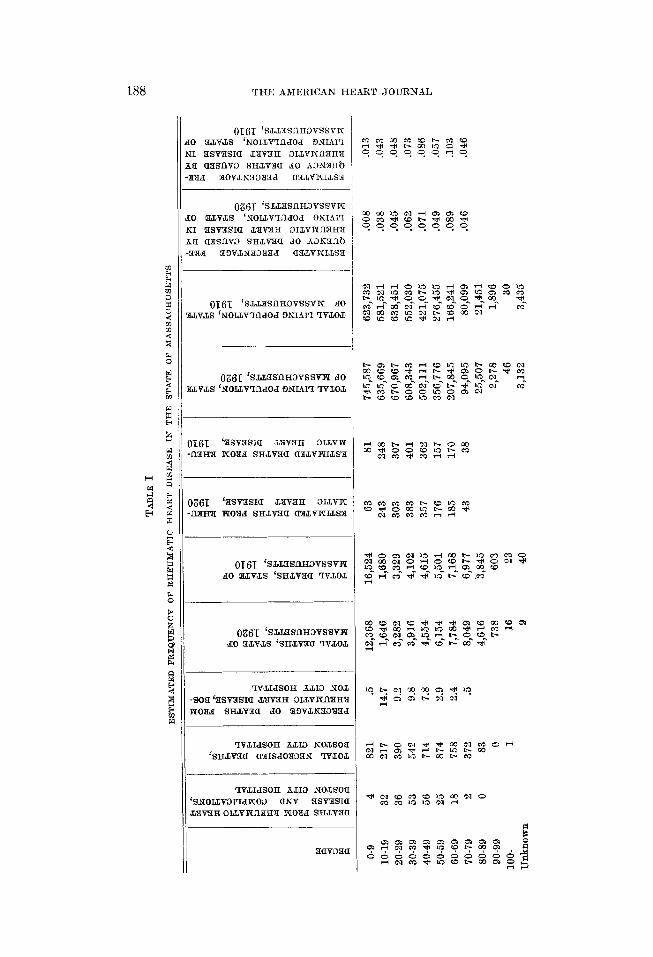
Since the age distribution curve of the cases autopsied in the Boston City Hospital is roughly parallel to that of deaths in the population at large, the percentage of deaths from rheumatic heart, disease in any given decade should be approximately the same in these two groups. By ap- plying the percentages obtained from the Boston City Hospital figures to the vital and mortality statistics for the State of Massachusetts, one may estimate (1) what number of deaths in the population at large in any given decade may be expected to occur from rheumatic heart disease, and (2) what percentage of the total living population for that decade these probable deaths represent. Table I gives the result of such a calcula- tion. The estimated frequency of fatal rheumatic heart disease varied between 10 to 100 per 100,000 population in 1910 and 10 to 900 in 1920 in various decades.
The frequency of rheumatic heart disease which contributed partially to death, and of that which was present only as an accidental, noncon- tributing finding at death cannot be estimated for the living population, since the figures representing this type of case cannot be applied statis- tically from the dead population of the hospital to the living community. In general, however, the statistics suggest that these milder types of rheumatic heart disease must be expected to occur among the living population many times more frequently t,llan that degree of the disease which leads to death.
THE AMERICAN HEART JOURNAL
()I(jr 'S&,L3SflHDVSSvK 0 3cLvm ‘NOIJFIfidOd ONIAI'I I 3SVXSIa DWOH 3LLvNfl3HX B CI3SnVD SH&vM JO hLlN3fltl [IL5 3Ov,LN3D!JIId a3mmm3
Oz6T kLL3SIlH3VSSVW 0 3,LvJA ‘NOLLV?fldOd 3NIAI'I :I 3SVXSIa JAWiIH 3IdVWflZH71 B a3SYlv,D SH.LvIa d0 AtlN3Jlti GM 33VtLN33H3d a3.mmrs3
0~6~ ‘S&L3SlIHDVSSvX 80 ,&V&S lNOLLV'XldOdONIAI'ITvJ.O&
13361 ‘SJZ3SIlH3VSSvR JO LV~S'NO~V?~dOdONIAl??B~O~
1‘161 ‘asvasxa ~VPH OIJAVPI n3m ~039 smv3a aryzmmLs3
lZ61 fSv3SIa JXV3H DLLVN 113H3 NO?ld SHAv3a a3d,VNLLS3
()Tf5T. ‘SiiX3SflH3VSSVN do 3kLvd‘s %H&v3a 1vnzhx
0$33‘c %.mmmvssvm do r.Lv%Ls ‘SH&v3(I 1v&xkI
?V&IdSOH h&ID NOJ .SOtl‘3SV3SIa dXV3H 3LIXNA3H't mOEd SHtLVBIa d0 3f)vtLN3iXT3d
?VJddSOH h&Ill NO&SOE ‘SHdXita a3ISdOW3N W&O3
'IVJddSOH hJJ3 NO&SOS k'NOIJXWId~O0 aNV 3SV,3SI< L?D"3HOILvPUlIH'd NOXd SHAV3C
3av33c
-I
-/
-
I [ I -
I

DAVIS AND WEISS: RHEUMATIC HFART DISEASE 189
SUMMARY
The incidence and distribution by decades of the age of death of 5060 consecutive necropsy examinations performed in the Boston City Hos- pital have been analyzed. Deaths from rheumatic heart disease in 229 cases were distributed widely from the second to the fifth decades of life inclusive, the largest number of deaths occurring in the fourth or fifth dec- ades. Of 4’7 cases in which subacute bacterial endocarditis was superim- posed on an old rheumatic heart disease, 40 cases died before the age of fifty years. In all the 19 cases with malignant endocarditis superimposed on rheumatic heart disease death occurred before t,he age of forty years.
It is to be emphasized that as late as the sixth and seventh decades of life rheumatic heart disease is frequently present in paGents wit,h cardiac symptoms and signs. The evidence presented suggests that the age dis- tribution of death of the hospital population studied is roughly parallel to that of the population at large. An estimate of the expected fre- quency of fatal rheumatic heart disease among the living population of the State of Massachusetts is presented. This estimated frequency of the fatal rheumatic heart disease must, however, represent but a small portion of the total prevalence of rheumatic heart disease in the living population.
REFERENCES
1. Davis, David, and Weiss, Soma: Rheumatic Heart Disease: I. Incidence and R61e in the Causation of Death. A Study of 5215 Consecutive Necropsies. AM. HEART J. 7: 146, 1931.
2. Willius, F. A.: A Study of the Course of Rheumatic Heart Disease. AM. HEART J. 3: 139, 1927.
3. Coombs, Cary F.: Ltd.
R,heumatic Heart Disease, Bristol, 1924, John Wright & Sons,