Embed Size (px)
Citation preview

Heat Stress and Sudden Infant Death Syndrome Incidence:A United States Population Epidemiologic Study
Joshua R. Scheers-Masters, BA*; Mario Schootman, PhD*‡; and Bradley T. Thach, MD*
ABSTRACT. Objectives. To determine the role of heatstress in sudden infant death syndrome (SIDS) by exam-ining the SIDS rates during periods of extreme environ-mental temperatures in a period when most infants wereplaced prone for sleep.
Design. A retrospective study of SIDS rates and mor-tality rates attributable to excessive environmental heatin relationship to climatologic temperature was per-formed. Data were collected for each of 454 counties in 4states (Arkansas, Georgia, Kansas, and Missouri) fromMay 1 to September 30, 1980, and were then summed toyield the mortality rates for each 5°F (2.8°C) temperaturerange.
Results. �2 analyses revealed significant relation-ships for heat-related mortality rates and both the maxi-mal daily temperature and mean daily temperature butdemonstrated no such relationships for SIDS rates. Noassociation between SIDS rates and heat-related mortal-ity rates was found with Spearman’s ranked correlation,for either the maximal daily temperature or the meandaily temperature.
Conclusions. On the basis of our findings of no sig-nificant association between SIDS and either measure oftemperature during periods of high heat stress-relateddeath rates, it seems unlikely that the heat stress associ-ated with the combination of prone sleep positions andelevated environmental temperatures has a significantrole in the development of SIDS. Pediatrics 2004;113:e586 –e592. URL: http://www.pediatrics.org/cgi/content/full/113/6/e586; SIDS, thermal stress, bedding,overwrapping, sleep position.
ABBREVIATIONS. SIDS, sudden infant death syndrome; Tmax,maximal daily temperature; Tavg, average daily temperature.
The thermal stress theory for sudden infantdeath syndrome (SIDS) states that many SIDSdeaths occur as a result of increased demands
on thermoregulatory mechanisms attributable to aprone sleep position, increased ambient temperature,and/or a decreased ability to eliminate body heat asa result of excessive clothing covering the infant.1Although the relationship between climatic temper-ature and SIDS incidence has been examined care-fully, the studies were performed predominantly in
nations without extreme temperature variations,such as Great Britain, Tasmania, and New Zea-land.2–5 Such research has consistently associated in-creased SIDS incidence with colder outdoor temper-atures. It has been suggested that some parents mayrespond to such cold waves by overwrapping infantsor excessively increasing room temperatures.3 Incontrast, a cross-cultural study found comparativelyweak relationships between climatic temperatureand SIDS incidence in communities in the UnitedStates.6 Therefore, it is possible that seasonal over-wrapping of infants may not be a major cause ofSIDS in the United States.
Sections of the United States, particularly the Mid-west, are subject to periodic heat waves, which canlead to severe epidemics of deaths attributable toexposure to excessive heat.7 Such conditions presentan opportunity to examine the effect of increasedenvironmental temperature on SIDS incidence. Wereasoned that, if thermal stress increases the risk ofSIDS, then an increase in the number of SIDS deathsshould be observed when there is an increase in thenumber of heat-related deaths in the general popu-lation.
METHODS
PopulationThis study concentrated on the heat waves of the summer of
1980. In that year, excessive heat from all sources was listed as theunderlying cause of death for a total of 1700 deaths across theUnited States,8 which was notably greater than the median of 274deaths per year from 1979 to 1998 and was the largest number ofheat-related deaths during that period.9 To avoid a false-negativefinding attributable to seasonal variations in the SIDS rate, theperiod was restricted to May 1 through September 30, 1980. Alldeaths attributable to SIDS and exposure to excessive heat result-ing from weather conditions in each of the counties of the 4 stateswith the greatest numbers of heat-related deaths, namely, Arkan-sas, Georgia, Kansas, and Missouri, during this period were con-sidered.
Data SourcesSIDS mortality data were defined as all records from the Mor-
tality Detail Files, 1979–1980,10 that fit the aforementioned criteriaand for which an International Classification of Diseases, 9th revision,code of 798.0 was assigned for the underlying cause of death.Heat-mortality data were defined as all records for which anInternational Classification of Diseases, 9th revision, code of 900.0(“death due to excessive heat due to weather conditions”) wasassigned. Population data for each county were obtained from theCensus of Population and Housing, 1980 (United States): County Pop-ulation by Age, Sex, Race, and Spanish Origin,11 with the populationsbeing defined as the entire population of the county for heat-related deaths and the population �1 year of age for SIDS deaths.
Data on the maximal daily temperature (Tmax) and minimaldaily temperature were determined for each county of the 4 states
From the *Edward Mallinckrodt Department of Pediatrics and ‡Departmentof Internal Medicine, Washington University School of Medicine, St Louis,Missouri.Received for publication Sep 25, 2002; accepted Dec 29, 2003.Reprint requests to (B.T.T.) Washington University School of Medicine, 660S Euclid, Campus Box 8208, St Louis, MO 63110. E-mail: [email protected] (ISSN 0031 4005). Copyright © 2004 by the American Acad-emy of Pediatrics.
e586 PEDIATRICS Vol. 113 No. 6 June 2004 http://www.pediatrics.org/cgi/content/full/113/6/e586 by guest on April 4, 2019www.aappublications.org/newsDownloaded from

studied from the Record of Climatological Observations.12 Tempera-tures for the counties were recorded from a single weather stationwithin each county. For counties that were missing data, temper-ature data were calculated as the average of values from 2 weatherstations in 2 bordering counties. If original data were missing forall bordering counties, then data for the next closest counties wereused. Average daily temperatures (Tavg) in each location thenwere calculated as the average of Tmax and the minimal dailytemperature. All temperature data were rounded to the nearestinteger.
Statistical AnalysesFor each 5°F temperature range (for example, 60–64°F [15.6–
17.8°C]), the population of each county was multiplied by thenumber of days the county experienced that temperature range.These values then were summed for all counties, to yield the totalpopulation at risk for each temperature range. The total number ofdeaths that occurred in that temperature range then was dividedby the total population at risk to yield the mortality rate for eachtemperature range.
�2 tests for trend were performed to determine the associationbetween the SIDS rate and the heat-related death rate for Tavg andTmax. To determine the association between the SIDS rate and theheat-related death rate, Spearman’s rank correlation coefficientwas used. A P value of �.05 was considered statistically signifi-cant. These analyses were repeated after recoding of any infantdeaths attributable to exposure to excessive heat as deaths attrib-utable to SIDS. In these cases, the population associated withheat-related deaths was equal to the entire population of thecounty minus the population �1 year of age.
Because of the relatively few cases (111) of SIDS recordedduring the study period, we used a simulation to calculate theempirical power to detect a linear increase in the SIDS rate withincreasing temperature. With the available SIDS deaths, the powerwas calculated to be 0.78 if the SIDS rate at the highest tempera-ture was 2.7 times that at the lowest temperature. The power was0.70 if the SIDS rate at the highest temperature was 1.8 times thatat the lowest temperature. If the SIDS rate at the highest temper-ature was 1.5 times that at the lowest temperature, then the powerwas calculated to be 0.63 (Table 1).
RESULTSBetween May 1 and September 30, 1980, in the
states of Arkansas, Georgia, Kansas, and Missouri, atotal of 111 SIDS deaths and 402 deaths attributableto excessive heat resulting from weather conditionswere recorded. �2 tests demonstrated increased heat-related mortality rates with increasing Tmax values (P� .0001) but indicated no such relationship for SIDSrates (P � .362) (Fig 1). Also, there was a strongassociation between heat-related mortality rates andTavg values (P � .0001); however, there was no linearassociation for SIDS rates and Tavg (P � .713) (Fig 2).
Furthermore, analysis of the relationship betweenSIDS rates and heat-related mortality rates withSpearman’s ranked correlation indicated no associa-tion for either Tmax (P � .2080) or Tavg (P � .8979).
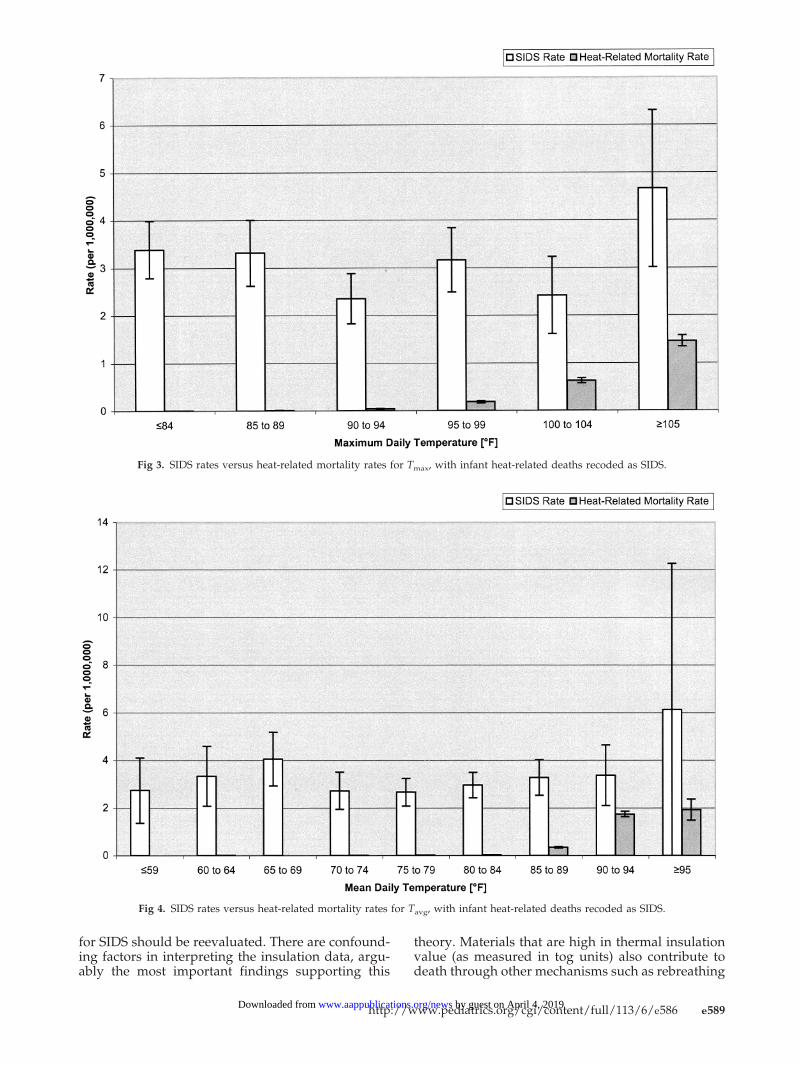
The 3 infant deaths were diagnosed as being at-tributable to environmental heat. The analysis wasrepeated after these deaths had been removed fromthe heat-related category and entered as SIDS deaths.Again, �2 tests demonstrated increases in heat-re-lated mortality rates with increasing Tmax values (P� .0001) but indicated no such relationship for SIDSrates (P � .605) (Fig 3). Heat-related mortality ratesincreased with Tavg values (P � .0001), but againthere was no association between SIDS rates and Tavg(P � .945) (Fig 4). In addition, analysis of the recodeddata with Spearman’s ranked correlation indicatedno association for either Tmax (P � .9572) or Tavg (P �.4175). Finally, we considered the possibility thatthere could be a threshold for heat stress, increasingSIDS risks at higher temperature ranges. Therefore,we analyzed the dichotomized Tavg variable. The ratefor Tavg of �85°F was 3.0 cases per 1 000 000 popu-lation, whereas the rate for �85°F was 3.4 cases per1 000 000. This difference was not statistically signif-icant (P � .568).
DISCUSSIONIn this study, we failed to find a relationship be-
tween elevated environmental temperatures and theincidence of SIDS during a period in which deathsattributable to excessive environmental temperaturesin the general population were increased to epidemiclevels. Physiologic and epidemiologic research sug-gests increased risks attributable to heat stressamong prone-sleeping infants, because their abilityto eliminate heat may be reduced in this position.13,14
During the period of our study, �72% to 77% ofinfants slept prone.15 Therefore, US infants as agroup should have been unusually susceptible toheat stress.
The power calculation indicated that the numberof SIDS deaths studied was sufficient to allow detec-tion of an increase in SIDS rates of 1.8-fold betweenthe highest and lowest temperatures. Smaller in-creases would have been undetectable. Increases ofthis magnitude are relatively small, considering thatthe differences between summer and winter SIDSrates during the 1980s in New Zealand, for example,were five- to sevenfold.3 Therefore, if the large sea-sonal variations in SIDS rates observed in the pastwere primarily attributable to heat stress, as sug-gested previously,1,16 then we would expect to haveobserved changes of this magnitude among heat-stressed infants. Furthermore, the present study in-dicated that heat-related death rates in the generalpopulation we studied were much higher at thehighest temperature, compared with the lowest. IfSIDS infants are to be considered at high risk fordeath attributable to heat stress, then an increase indeath rates of a magnitude comparable to that fordeaths attributable to heat stress in the general pop-ulation would be expected. The statistical power wasmore than adequate to detect such an increase.
These findings suggest that the heat stress theory
TABLE 1. Empirical Power Calculations*
Increase in SIDSRate at HighestVersus LowestTemperature
Power
Linear IncreaseWith Increasing
Temperature
Stepwise IncreaseWith Increasing
Temperature
6.0 0.89 0.953.5 0.83 0.932.7 0.78 0.881.8 0.70 0.731.5 0.63 0.641.2 0.56 0.60
* For example; the Power is 0.78 if the SIDS rate at the highesttemperature is 2.7 times that at the lowest temperature, with alinear increase in the SIDS rate with increasing temperature. Thepower is 0.70 if the SIDS rate at the highest temperature is 1.8times that at the lowest temperature, with a linear increase in theSIDS rate with increasing temperature.
http://www.pediatrics.org/cgi/content/full/113/6/e586 e587 by guest on April 4, 2019www.aappublications.org/newsDownloaded from
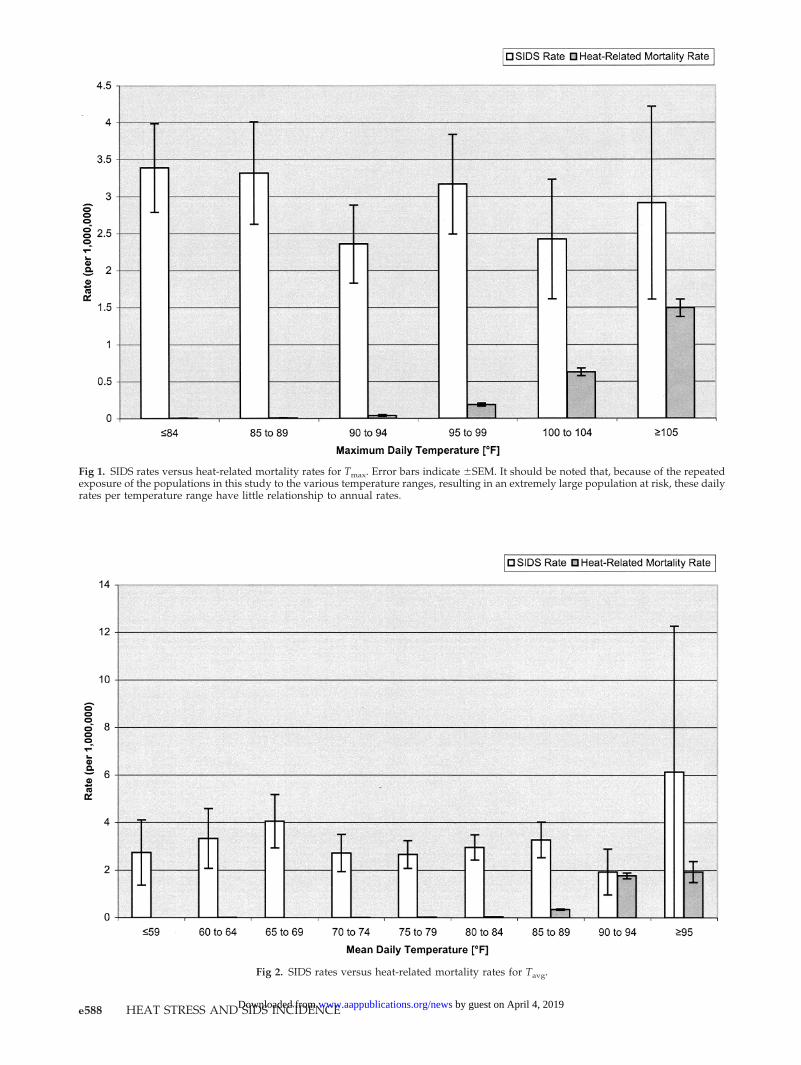
Fig 1. SIDS rates versus heat-related mortality rates for Tmax. Error bars indicate �SEM. It should be noted that, because of the repeatedexposure of the populations in this study to the various temperature ranges, resulting in an extremely large population at risk, these dailyrates per temperature range have little relationship to annual rates.
Fig 2. SIDS rates versus heat-related mortality rates for Tavg.
e588 HEAT STRESS AND SIDS INCIDENCE by guest on April 4, 2019www.aappublications.org/newsDownloaded from
for SIDS should be reevaluated. There are confound-ing factors in interpreting the insulation data, argu-ably the most important findings supporting this
theory. Materials that are high in thermal insulationvalue (as measured in tog units) also contribute todeath through other mechanisms such as rebreathing
Fig 3. SIDS rates versus heat-related mortality rates for Tmax, with infant heat-related deaths recoded as SIDS.
Fig 4. SIDS rates versus heat-related mortality rates for Tavg, with infant heat-related deaths recoded as SIDS.
http://www.pediatrics.org/cgi/content/full/113/6/e586 e589 by guest on April 4, 2019www.aappublications.org/newsDownloaded from

of expired air causing asphyxiation. Studies havefound that infant bedding items such as quilts, com-forters, and blankets have a high potential for caus-ing rebreathing.17,18 Fleming et al16 found that in-fants who died as a result of SIDS were wrapped inclothing or covered by bedding with a significantlygreater tog value than were control infants. Theincreased SIDS risk associated with increased bodyinsulation was highest among prone-sleeping in-fants. Because prone sleeping and increased insula-tion can interact to reduce an infant’s ability to elim-inate heat, the investigators attributed the increasedSIDS risk in the prone position to thermal stress.However, those investigators did not include bulkybedding items (such as duvets, quilts, or comforters)covering infants in their multivariate analysis. Theseitems not only are very substantial components ofthe tog estimate but also place infants at increasedrisk for rebreathing. In fact, Ponsonby et al19 foundthat the increase in the risk of SIDS resulting fromquilt or comforter use was evident only for supine-sleeping infants, suggesting that heat stress may notbe the primary mechanism for the increased riskassociated with these items.
The thermal stress theory of SIDS originated withpremortem and postmortem observations of ele-vated body temperature or excessive sweatingamong infants with SIDS.20,21 The observations ofoverwrapping or elevated room temperature on theday of death provided additional support for thistheory.16,20,22,23 It is important to note that the ther-mal stress theory draws a sharp distinction betweenSIDS resulting from heat stress and death attribut-able to extreme hyperthermia leading to heatstroke.22,24 Therefore, it has been suggested that ther-mal stress, with or without moderate increases inbody temperature, can result in fatal disruption ofvital systems among infants predisposed to SIDS.1,25
It has been proposed that congenital or acquiredanatomic abnormalities in brainstem centers regu-lating respiratory or cardiovascular stability couldrepresent the underlying defects that render SIDSinfants susceptible to death resulting from heatstress.26
Our reasoning in assuming that a substantial num-ber of infants at risk for SIDS experienced significantheat stress is as follows. First, several factors indicatethat young infants can be expected to experiencemore heat stress than older children or adults whenenvironmental temperatures increase. The full spec-trum of heat-related illnesses among infants must beconsidered, because more cases of nonlethal environ-mental heat-related illnesses (eg, heat prostrationand water-deficiency heat exhaustion) than actualheat stroke occur among infants.27 The actual deathrates for infants, compared with the elderly, duringheat waves are less likely to reflect the true incidenceof heat stress, because death seems to be less fre-quent among infants diagnosed with heat strokethan in the older population.27 The risk for all heat-related illnesses is thought to be increased amonginfants, compared with older children or adults.28–30
This is attributed to increased metabolic rate, in-creased surface area/body mass ratio, and increased
tendency for emesis as well as refusal to accept orallyadministered fluids when overheated, which makeinfants more susceptible to heat stress and relateddehydration.27,31 Therefore, for any given thermalexposure, infants may be expected to experiencesymptoms of heat stress more rapidly than other agegroups.
Second, it might be expected that most parentswould pay particular attention to keeping infantscool in hot weather. Evidence suggests that this is notthe case. A study of heat-stressed infants hospital-ized for treatment found that 68% of the infants’caretakers were unaware of the need for increasedfluid intake by their infants during hot weather andhad seriously underestimated the seriousness of theinfants’ initial symptoms.27 Other studies also indi-cated a lack of parental perception regarding infantheat stress. It has been reported that the practice ofleaving sleeping infants in parked cars while parentsrun errands is a frequent cause of heat-related mor-bidity and death.31–34 It is noteworthy that 24% ofmothers admit to this practice, again indicating seri-ous underestimation by caretakers of their infants’ability to cope with increased environmental temper-atures.32
Third, it is unlikely that many infants kept indoorsduring the 1980 heat wave received adequate protec-tion as a result of access to home air conditioning orfans. A government-sponsored study of the avail-ability of home air conditioners in the 4 states westudied, spanning 1980 to 1984, indicated that mosthouseholds (51%) had inadequate access to air con-ditioners sufficient to reduce the risk of heat stroke.35
Even more relevant were the findings of a 1980 studythat found that �80% of the households in the lowerone-third socioeconomic group did not have air con-ditioning.36 Fans in the home were not found todecrease the risk of heat stroke.37 Therefore, it can beinferred that the majority of the infants, includingthose at highest risk for SIDS (ie, infants in low-income households), did not have access to environ-ments adequate to eliminate heat stress.
Fourth, any consideration of the possible relation-ship of heat stress to SIDS in the United States mustalso take into account the fact that the population athighest risk for one is also that at highest risk for theother. It has been well established in several studies,including an analysis of the 1980 heat wave in Mis-souri, that low-income, urban, and African Americanpopulations are at highest risk for heat stroke be-cause of the combination of an urban “heat-island”effect that increases both indoor and outdoor tem-peratures, substandard housing, poor ventilation,and decreased access to air conditioning.38–41 Wheninfant physiologic factors, the failure of caregivers toperform appropriate interventions, and populationsat greatest risk for both heat stress and SIDS aretaken into account, it might reasonably be predictedthat, if heat stress per se is a significant cause of SIDS,SIDS incidence should increase significantly duringsummer heat waves, when the number of deathsattributable to overheating in the general populationincreases.
Heat stress can be defined as a deviation from a
e590 HEAT STRESS AND SIDS INCIDENCE by guest on April 4, 2019www.aappublications.org/newsDownloaded from

thermoneutral environment that requires increaseduse of the body’s mechanisms for cooling. In con-trast, heat stroke, defined as a body temperature of�105°F (�40.6°C) and altered mental status,42 leadsto cardiac arrhythmias, seizures, or hypovolemicshock, with tachycardia and eventual circulatory col-lapse.43 Depression of central nervous system ther-moregulatory mechanisms is thought to be involvedin such deaths.43,44 Because it is difficult to diagnoseheat stroke after death among both infants andadults, because of the lack of specific pathologic find-ings, the most important information for the post-mortem diagnosis comes from body-temperaturemeasurements and death-scene investigations.45–47
In this study, there were 3 infant deaths among the402 deaths attributable to excessive heat exposure.Two of those deaths occurred on consecutive days inJackson County, Missouri (which includes KansasCity). During the summer heat wave, 5 deaths diag-nosed as SIDS occurred in Jackson County, whichsuggests that the medical examiner for that jurisdic-tion was accustomed to distinguishing infant deathsattributable to SIDS from heat stroke deaths. Even ifall 3 heat-related deaths had been attributed to SIDS,the relationship of SIDS incidence to environmentaltemperature would have remained insignificant.
Finally, it must be noted that either genetic oracquired abnormalities involving sweat gland func-tion or the thermoregulatory centers of the brain mayrender individuals vulnerable to heat stress, whichcan be fatal.48,49 It is also clear that the numbers ofdeaths primarily attributable to respiratory or car-diovascular disease increase during periods of envi-ronmental heat stress.8,50 This has been attributed tothe fact that accommodation to increased environ-mental temperatures results in increased demandson the heart and lungs. Accordingly, it would beexpected that, if infants with SIDS have congenital oracquired abnormalities of thermoregulation or of re-spiratory or cardiovascular function, then the num-bers of SIDS deaths would increase during periods ofdangerously elevated environmental temperatures.This did not occur; therefore, it seems unlikely that acongenital or acquired defect in thermoregulation isan underlying cause of a significant number of infantdeaths attributed to SIDS.
The present findings do not exclude the possibilitythat a combination of factors, including increasedbody insulation or febrile illnesses associated withthe winter months, are causal in certain SIDS cases.More research is needed on potential interactionsbetween these factors. However, given that the largemajority of infants were placed prone for sleep dur-ing the period of this study, it seems that heat stressproduced by increased environmental temperaturesand prone positions alone does not have a substan-tial causal role in SIDS.
ACKNOWLEDGMENTSThis research was funded by National Institute of Child Health
and Human Development grant HD-10993.The data used in this study were made available in part by the
Inter-University Consortium for Political and Social Research. Thedata for the Mortality Detail Files, 1979–1980, were originally col-lected by the National Center for Health Statistics. The data for
Census of Population and Housing, 1980 (United States): County Pop-ulation by Age, Sex, Race, and Spanish Origin were originally col-lected by the US Department of Commerce, Bureau of the Census.Neither the collectors of the original data nor the Consortium bearany responsibility for the analyses or interpretations presentedhere.
REFERENCES1. Harper RM, Kinney HC, Fleming PJ, Thach BT. Sleep influences on
homeostatic functions: implications for sudden infant death syndrome.Respir Physiol. 2000;119:123–132
2. Schluter PJ, Ford RP, Brown J, Ryan AP. Weather temperatures andsudden infant death syndrome: a regional study over 22 years in NewZealand. J Epidemiol Community Health. 1998;52:27–33
3. Mitchell EA, Stewart AW, Cowan SF. Sudden infant death syndromeand weather temperature. Paediatr Perinat Epidemiol. 1992;6:19–28
4. Campbell MJ, Rodrigues L, Macfarlane AJ, Murphy MF. Sudden infantdeaths and cold weather: was the rise in infant mortality in 1986 inEngland and Wales due to weather? Paediatr Perinat Epidemiol. 1991;5:93–100
5. Jones ME, Ponsonby AL, Dwyer T, Gilbert N. The relation betweenclimactic temperature and sudden infant death syndrome differs amongcommunities: results from an ecologic analysis. Epidemiology. 1994;5:332–336
6. Murphy MF, Campbell MJ. Sudden infant death syndrome and envi-ronmental temperature: an analysis using vital statistics. J EpidemiolCommunity Health. 1987;41:63–71
7. National Oceanic and Atmospheric Administration (United States).Heat Wave: A Major Summer Killer. Washington, DC: United StatesDepartment of Commerce; 1985. Available at: www.nws.noaa.gov/om/brochures/heatwave.pdf
8. Centers for Disease Control and Prevention. Heat-related illnesses anddeaths: United States, 1994–1995. MMWR Morb Mortal Wkly Rep. 1995;44:465–468
9. Centers for Disease Control and Prevention. Heat-related deaths: LosAngeles County, California, 1999–2000, and United States, 1979–1998.MMWR Morb Mortal Wkly Rep. 2001;50:623–626
10. United States Department of Health and Human Services, NationalCenter for Health Statistics. Mortality Detail Files, 1979–1980 (computerfile). Hyattsville, MD: United States Department of Health and HumanServices, National Center for Health Statistics; 1985
11. United States Department of Commerce, Bureau of the Census. Censusof Population and Housing, 1980 (United States): County Population by Age,Sex, Race, and Spanish Origin (computer file). Washington, DC: UnitedStates Department of Commerce, Bureau of the Census; 1982
12. National Climatic Data Center. Record of climatological observations,October 3, 2001, to January 2, 2002. Available at: http://nndc.noaa.gov/?subscriptions.shtml
13. Nelson EA, Taylor BJ, Weatherall IL. Sleeping position and infantbedding may predispose to hyperthermia and the sudden infant deathsyndrome. Lancet. 1989;1:199–201
14. Ponsonby AL, Dwyer T, Gibbons LE, Cochrane JA, Wang YG. Factorspotentiating the risk of sudden infant death syndrome associate withthe prone position. N Engl J Med. 1993;329:377–382
15. Hoffman HJ, Hillman LS. Epidemiology of the sudden infant deathsyndrome: maternal, neonatal, and postneonatal risk factors. Clin Peri-natol. 1992;19:717–737
16. Fleming PJ, Gilbert R, Azaz Y, et al. Interaction between bedding andsleeping position in the sudden infant death syndrome: a populationbased case-control study. BMJ. 1990;301:858–859
17. Kemp JS, Thach BT. Quantifying the potential of infant bedding to limitCO2 dispersal and factors affecting rebreathing in bedding. J ApplPhysiol. 1995;78:740–745
18. Carleton JN, Donoghue AM, Porter WK. Mechanical model testing ofrebreathing potential in infant bedding materials. Arch Dis Child. 1998;78:323–328
19. Ponsonby AL, Dwyer T, Couper D, Cochrane J. Association betweenuse of a quilt and sudden infant death syndrome: case-control study.BMJ. 1998;316:195–196
20. Stanton AN, Scott DJ, Downham MA. Is overheating a factor in someunexpected infant deaths? Lancet. 1980;1:1054–1057
21. Beal S, Porter C. Sudden infant death syndrome related to climate. ActaPaediatr Scand. 1991;80:278–287
22. Bass M, Kravath RE, Glass L. Death-scene investigation in suddeninfant death. N Engl J Med. 1986;315:100–105
http://www.pediatrics.org/cgi/content/full/113/6/e586 e591 by guest on April 4, 2019www.aappublications.org/newsDownloaded from

23. Williams SM, Taylor BJ, Mitchell EA, et al. Sudden infant deathsyndrome: insulation from bedding and clothing and its effect modifi-ers. Int J Epidemiol. 1996;25:366–375
24. Krous HF, Nadeau JM, Fukumoto RI, Blackbourne BD, Byard RW.Environmental hyperthermic infant and early childhood death: circum-stances, pathologic changes, and manner of death. Am J Forensic MedPathol. 2001;22:374–382
25. Fleming PJ, Levine MR, Azaz Y, Wigfield R, Stewart AJ. Interactionsbetween thermoregulation and the control of respiration in infants:possible relationship to sudden infant death. Acta Paediatr Suppl. 1993;389:57–59
26. Kinney HC, Filiano JJ, White WF. Medullary serotonergic networkdeficiency in the sudden infant death syndrome: review of a 15-yearstudy of a single dataset. J Neuropathol Exp Neurol. 2001;60:228–247
27. Danks DM, Webb DW, Allen S. Heat illness in infants and youngchildren. BMJ. 1962;2:287–293
28. Kilbourne EM. Heat waves and hot environments. In: Noji EK, ed. ThePublic Health Consequences of Disasters. New York, NY: Oxford Univer-sity Press; 1997:245–269
29. Henschel A, Burton LL, Margolies L, Smith JE. An analysis of the heatdeaths in St. Louis during July, 1966. J Am Public Health. 1969;59:2232–2241
30. Centers for Disease Control and Prevention. Heat-related deaths: Dal-las, Wichita and Cooke counties, Texas, and United States. JAMA.1997;278:462–463
31. Wadlington WB, Tucker AL Jr, Fly F, Green HL. Heat stoke in infancy.Am J Dis Child. 1978;130:1250–1251
32. Roberts KB, Roberts EC. The automobile and heat stress. Pediatrics.1976;58:101–104
33. Krous HF, Nadeau JM, Fukumoto RI, Blackbourne BD, Byard RW.Environmental hyperthermic infant and early childhood death. Am JForensic Med Pathol. 2001;22:374–382
34. King K, Negus K, Vance JC. Heat stress in motor vehicles: a problem ininfancy. Pediatrics. 1981;68:579–582
35. Rogot E, Sorlie PD, Backlund E. Air-conditioning and mortality in hotweather. Am J Epidemiol. 1992;136:106–116
36. Jones TS, Liang AP, Kilbourne EM, Griffin MR. Morbidity and mortalityassociated with the July 1980 heat wave in St. Louis and Kansas City,MO. JAMA. 1982;247:3327–3331
37. Kilbourne EM, Choi K, Jones TS, Thacker SB; Field Investigation Team.Risk factors for heatstroke. JAMA. 1982;247:3332–3336
38. Klingenberg E. Heatwave: A Social Autopsy of Disaster in Chicago. Chicago,IL: University of Chicago Press; 2002:81–84
39. Smoyer K. Putting risk in its place: methodological considerations forinvestigating extreme event health risk. Soc Sci Med. 1998;47:1809–1824
40. Lowery W. The climate of cities. Sci Am. 1967;217(2):15–2341. Kalkstein L. Lessons from a very hot summer. Lancet. 1995;346:857–85942. Centers for Disease Control and Prevention. Heat-related deaths:
United States, 1993. MMWR Morb Mortal Wkly Rep. 1993;42:558–56043. Simon HB. Hyperthermia. N Engl J Med. 1993;329:483–48744. Guyton AC, Hall JE. Textbook of Medical Physiology. 9th ed. Philadelphia,
PA: W.B. Saunders Co; 1996:92145. Spitz WU, ed. Spitz and Fisher’s Medicolegal Investigation of Death: Guide-
lines for the Application of Pathology to Crime Investigation. 3rd ed. Spring-field, IL: Charles C. Thomas; 1993:181
46. Schuliar Y, Savourey G, Besnard Y, Launey JC. Diagnosis of heat strokein forensic medicine: contribution of thermophysiology. Forensic Sci Int.2001;124:205–208
47. Byard RW, Cohle SD. Sudden Death in Infancy, Childhood, and Adolescence.Cambridge, United Kingdom: Cambridge University Press; 1994:42
48. Darmstadt GL, Lane A. Ectodermal dysplasias. In: Behrman RE, Klieg-man RM, Arvin AM, eds. Nelson Textbook of Pediatrics. 15th ed. Phila-delphia, PA: W. B. Saunders Co; 1996:1837
49. Foster KG, Hey EN, O’Connell B. Sweat function in babies with defectsof the central nervous system. Arch Dis Child. 1971;46:444–451
50. McGeehin MA, Mirabelli M. The potential impacts of climate variabilityand change on temperature-related morbidity and mortality in theUnited States. Environ Health Perspect. 2001;109(suppl 2):185–189
e592 HEAT STRESS AND SIDS INCIDENCE by guest on April 4, 2019www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.113.6.e5862004;113;e586Pediatrics
Joshua R. Scheers-Masters, Mario Schootman and Bradley T. ThachPopulation Epidemiologic Study
Heat Stress and Sudden Infant Death Syndrome Incidence: A United States
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/113/6/e586including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/113/6/e586#BIBLThis article cites 40 articles, 8 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/sids_subSIDShttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_subFetus/Newborn Infantcollection(s): This article, along with others on similar topics, appears in the following
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlits entirety can be found online at: Information about reproducing this article in parts (figures, tables) or in
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on April 4, 2019www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.113.6.e5862004;113;e586Pediatrics
Joshua R. Scheers-Masters, Mario Schootman and Bradley T. ThachPopulation Epidemiologic Study
Heat Stress and Sudden Infant Death Syndrome Incidence: A United States
http://pediatrics.aappublications.org/content/113/6/e586on the World Wide Web at:
The online version of this article, along with updated information and services, is located
1073-0397. Copyright © 2004 by the American Academy of Pediatrics. All rights reserved. Print ISSN: American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.been published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
by guest on April 4, 2019www.aappublications.org/newsDownloaded from





























