Embed Size (px)
Citation preview
RHEUMATIC FEVERNUREEN FATIN SYAFIQA ADNAN
110201045
ACUTE RHEUMATIC FEVERINCIDENCE-Children (most common b/w 5&15 years)-Young adults-Geographical distribution : very RARE in Western Europe & Northern America-Remains ENDEMIC in parts of Asia, Africa & South America-Annual Incidence : >100 per 100,000-Most common cause of ACQUIRED heart disease in childhood & adolescence
ACUTE RHEUMATIC FEVERPATHOGENESIS
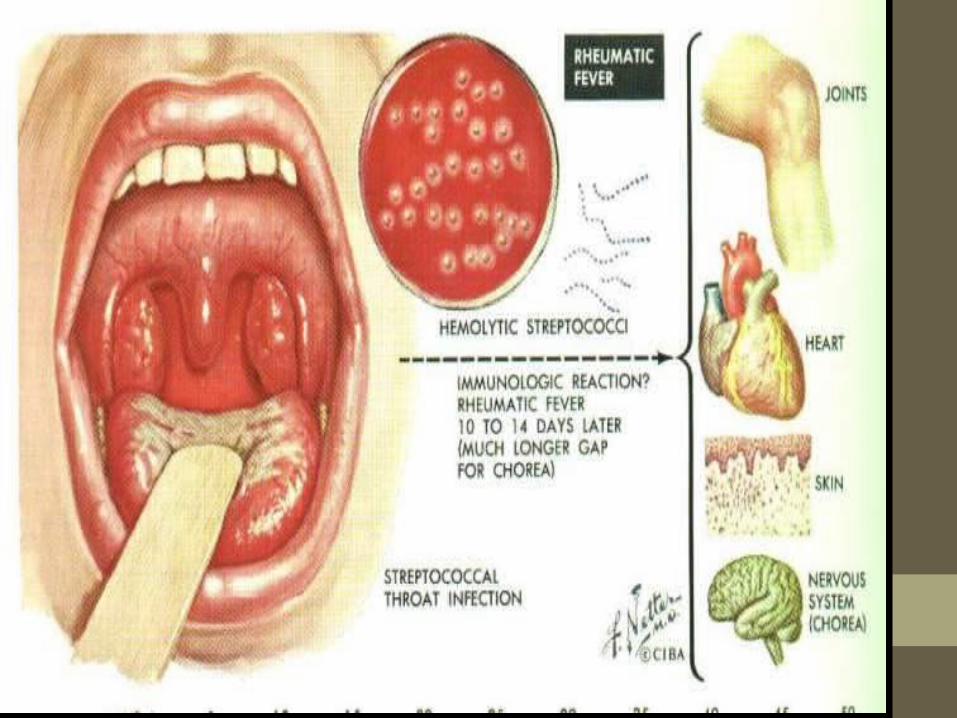
immune-mediated delayed response to infection with specific strain of group A Streptococci (have Ags that may cross-react with CARDIAC MYOSIN & SARCOLEMMAL MEMBRANE PROTEIN)
Abs produced against the streptococcal Ags
Inflammation in the endocardium, myocardium, pericardium, joints & skin

Immuneresponse
M-Protein
Molecular mimicry
Heart, Brain, Skin, Connective tissue
ACUTE RHEUMATIC FEVERHISTOLOGY-FIBRINOID degeneration in the COLLAGEN of connective tissue-ASCHOFF nodules are pathognomonic, occur only in the HEART (multinucleated giant cells surrounded by macrophages & T lymphocytes, seen in sub acute & chronic phases of rheumatic carditis)

ACUTE RHEUMATIC FEVERCLINICAL FEATURES
-fever, anorexia, lethargy, joint pain, 2-3 weeks after an episode of streptococcal pharyngitis-Diagnosis is made using the Revised Jones criteria
ACUTE RHEUMATIC FEVERJONES CRITERIA for diagnosis of Rheumatic Fever
MAJOR manifestations
1.Carditis
2.Polyarthritis
3.Chorea
4.Erythema marginatum
5.Subcutaneous nodules
ACUTE RHEUMATIC FEVERJONES CRITERIA for diagnosis of Rheumatic Fever
MINOR manifestations1.Fever2.Arthralgia3.Previous RF4.Raised ESR or CRP5.Leukocytosis6.First-degree AV block
PLUS Supporting evidence of preceding streptococcal infection;1.Recent scarlet fever2.Raised ASO or other strep Ab titre3.Positive throat culture
ACUTE RHEUMATIC FEVERDIAGNOSTIC CRITERIA
1.2 or more major manifestations2.1 major or 2 or more minor manifestations1&2 along with evidence of preceding streptococcal infection
PRESUMPTIVE DIAGNOSIS-Isolated chorea or pancarditis, if other causes for these hv been excluded
ESTABLISHED RHD or PRIOR RF-Diagnosis of acute RF can be made based only on the presence of MULTIPLE MINOR criteria & evidence of PRECEDING group A streptococcal pharyngitis.
ACUTE RHEUMATIC FEVERCLINICAL FEATURES
1.Carditis
2.Arthritis
3.Skin lesions
4.Sydenham’s chorea (St. Vitus dance)
ACUTE RHEUMATIC FEVERCARDITIS-Pancarditis-Breathlessness ( heart failure, pericardial effusion)-Palpitations-Chest pain-Tachycardia-New / changed cardiac murmurs•Soft mid-diastolic murmur (Carey-Coombs murmur) – due to valvulitis, nodules on mitral valve leaflets-Aortic regurgitation-Pericarditis (chest pain, pericardial friction rub, precordial tenderness)-Cardiac failure (myocardial dysfunction, valvular regurgitation)-Syncope ( conduction defects)
ACUTE RHEUMATIC FEVER- ECG; ST & T wave changes
ACUTE RHEUMATIC FEVERARTHRITIS-Most common major manifestation-Occurs early when streptococcal Ab titres are high-Acute PAINFUL-ASYMMETRICAL-MIGRATORY-Inflammation of LARGE joints (knees, ankles, elbows, wrists)-QUICK succession-RED, SWOLLEN, TENDER-Between 1 day to 4 weeks-RESPONDS to ASPIRIN

ACUTE RHEUMATIC FEVERSKIN LESIONS
1.ERYTHEMA MARGINATUM-<5% pts-Red macules (blotches)-Fades in centre, RED at the EDGES-TRUNK, PROXIMAL extremities-NOT the face-Red rings or margins may coalesce or overlap

ACUTE RHEUMATIC FEVERSKIN LESIONS
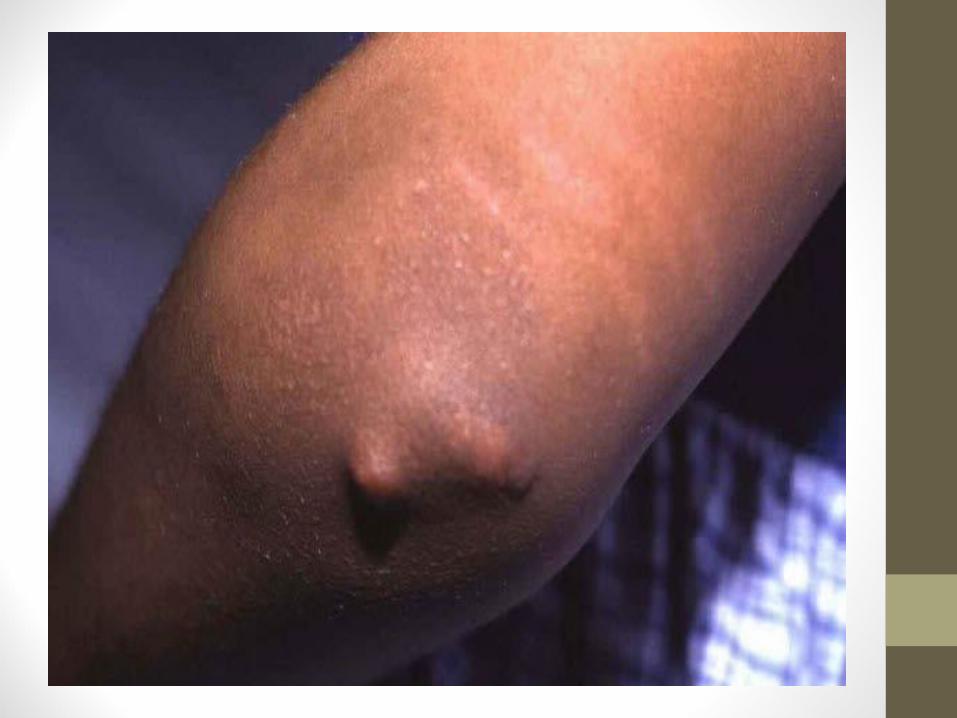
2. SUBCUTANEOUS NODULES-5-7% pts-Small (0.5-2.0 cm), firm, PAINLESS-EXTENSOR surfaces of bone or tendons-Appear >3 weeks AFTER onset of other manifestations

ACUTE RHEUMATIC FEVERSYDENHAM’S CHOREA ( ST. VITUS DANCE )-Appears at least 3 months AFTER episode of acute RF-1/3 of cases-> females-1st feature; EMOTIONAL LIABILITY-Purposeless involuntary choreiform movements of HANDS< FEET or FACE-EXPLOSIVE or HALTING speech-Spontaneous recovery within few months-Approx. ¼ develop chronic rheumatic valve disease
ACUTE RHEUMATIC FEVEROTHER SYSTEMIC MANIFESTATIONS-Rare-Pleurisy, pleural effusion, pneumonia
ACUTE RHEUMATIC FEVERINVESTIGATIONS
1.Evidence of a systemic illness ( non-specific )-Leukocytosis-Raised ESR & CRP (monitor disease progression)
2. Evidence of preceding streptococcal infection ( specific )-Throat swab culture ; GABHS ( family members, contacts )•+ve in only 10-25% cases-ASO titres ; RISING titres OR >200 U (adults), >300 U (children)•Normal in 1/5 of adult cases of RF & most cases of chorea
ACUTE RHEUMATIC FEVER3. Evidence of carditis-CXR ; cardiomegaly, pulmonary congestion-ECG ; 1st & rarely 2nd degree heart block, features of pericarditis, T-wave insertion, reduction in QRS voltages-ECHO ; cardiac dilatation, valve abnormalities•ECHO typically shows
i)MITRAL regurgitation with dilatation of mitral annulus & prolapse of ant. mitral leaflet
ii)Aortic regurgitation
iii)Pericardial effusion
ACUTE RHEUMATIC FEVERMANAGEMENT OF ACUTE ATTACK
1.SINGLE DOSE of BENZYL penicillin 1.2 million U IM or
2.PHENOXYMETHYLpenicillin 250mg 6-hourly for 10 days
Should be given ON DIAGNOSIS, to eliminate any residual streptococcal infection
•Erythromycin or cephalosporin in penicillin-allergic pts
ACUTE RHEUMATIC FEVERBED REST & SUPPORTIVE THERAPY
Bed rest – lessens joint pain, reduces cardiac workload
Valve replacement – heart failure not responding to medical Rx
ACUTE RHEUMATIC FEVERASPIRIN
Rapid relief of arthritis within 24 hours, confirm the Dx
Starting dose – 60mg/kg/day divided into 6 doses
Adults – 100mg/kg/day may be needed up to limits of tolerance OR max of 8grams/day
Continued until ESR has fallen & tapered gradually
Toxic effects; nausea, tinnitus, deafness, vomiting, tachypnoea, acidosis
ACUTE RHEUMATIC FEVERCORTICOSTEROIDS
More rapid relief
Indications; cases with carditis, severe arthritis
Prednisolone 1.0-2.0 mg/kg/day in divided doses, until ESR is normal & tapered.
ACUTE RHEUMATIC FEVERSECONDARY PREVENTION1.Benzathine penicillin 1.2 MU IM monthly or2.Oral phenoxymethylpenicillin 250mg 12-hourly•Sulfadiazine or erythromycin (pts allergic to penicillin)•Sulfonamides prevent infection, but not eradication of GAS
-Further attacks of RF, unusual after 21 yrs, Rx may be stopped
-Extension of Rx •i) if attack occurred in last 5 yrs •ii) Pts live in area of high prevalence, occupational exposure•iii) Residual heart disease, •Prophylaxis until 10 yrs after last episode OR until 40 yrs of age, whichever longer
THANK YOU.






















