Embed Size (px)
Citation preview

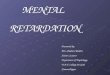
Contribution of twin pregnancyto perinatal mortality and fetal growth retardation;reversal of growth retardation after birth
0 24 4S 72 W 123 144 1.AGEATDEAII4'lhws4

25
20
15
1000
2001-2500 2501-3000
501 1000 1001 1501 2000BIRTHWEIGHT grams

Gestational Age (ink)
(cm (cm)
Gestationa) Age (wk)

For the OptimumManagement of
Iron Deficiency
Sb.v-Fe(ferrous sulfate) hematinicINDICATIONS:The management of iron deficiencystates and anemia.CONTRAINDICATIONS:Iron therapy is contraindicated in thepresence of hemochromatosis,hemosiderosis and hemolytic anemia.
WARNING:Keep out of reach of children.
ADVERSE REACTIONS:Gastro-intestinal side effects such asnausea and gastro-intestinal irritationare rare. Other side effects whichhave been rarely reported are:vomiting, constipation, diarrhea,abdominal pain and skin rash.
PRECAUTIONS:Slow-Fe, like all oral ironpreparations, may aggravate existingpeptic ulcer, regional enteritis andulcerative colitis. Iron when givenwith tetracyclines, binds inequimolecular ratio thus lowering theabsorption of tetracyclines.
DOSAGE:Prophylaxis: One tablet daily issufficient to maintain an adequateiron intake during pregnancy and inpatients with simple iron deficiency.Iron Deficiency: Depending on theseverity, one or two tablets ofSlow-Fe daily, usually in one dose.In mild anemias, one tablet daily willusually suffice. For moderate orsevere anemias, two tablets dailyshould be given until hemoglobinlevels return to normal.* In severecases, up to a maximum of 4 tabletsdaily may be given.In the case of children, one tablet ofSlow-Fe daily is a suitable dose forchildren able to swallow a smalltablet.*This physiological process mayrequire a period of up to eight weeks.Once the desired hemoglobin level isattained, the dose can then bereduced to one tablet daily formaintenance to build up the ironreserves over a further 12 to 16weeks.
Supplied:Each off-white, film-coated Slow-Fetablet contains 160 mg of driedferrous sulfate (=50 mg elementaliron) in a specially formulated matrix.Packaged in push-through packscontaining 30 tablets per sheet andare available in units of 30, 120 and4,800.References:1. Product Monograph.Full information available on request.
CIBADORVAL, OU.BEC.H951B1 C7066
See outside back cover
(slow-release potmlum chloride tablets.)
indications - All circumstances in whichpotassium supplementation is necessary andparticularly during prolonged or intensivediuretic therapy.Patients at special risk are those with advancedhepatic cirrhosis or chronic renal disease,patients with considerable edema (particularlyif urinary output is large) and patients receivingdigitalis (a lack of potassium sensitizes themyocardium to the toxic effects of digitalis).The range of indications for SLOW-K may besummarized as follows:As a supplement to Ulcerative colitisdiuretics Steatorrhea
Hypochloremic Chronic diarrheaalkalosis Regional ileitis
Cushing's Syndrome IleostomyCorticosteroid therapyLiver cirrhosisDigitalis therapy
SLOW-K is also indicated during convalescenceof patients following 'diseases characterized bypersistent vomiting" and of surgical patients inwhom prolonged withdrawal of fluids had takenplace.
Contraindications - Renal impairment witholiguria or azotemia, untreated Addison'sDisease, myotonia congenita, hyperadrenalismassociated with adrenogenital syndrome, acutedehydration, heat cramps and hyperkalemia ofany etiology: conditions associated with stasisof the GI. tract; esophageal compression dueto an enlarged left atrium; patients undergoingheart surgery.Warnings - A probable association existsbetween the use of coated tablets containingpotassium salts, with or without thiazidediuretics and the incidence of serious smallbowel ulceration. Such preparations should beused only when adequate dietarysupplementation is not practical and should bediscontinued if abdominal pain, distension,nausea, vomiting or gastrointestinal bleedingoccurs.Precautions - Administer cautiously topatients in advanced renal failure to avoidpossible hyperkalemia. SLOW-K should be usedwith caution in diseases associated with heartblock since increased serum potassium mayincrease the degree of block.Adverse reactions - Small bowel ulcerationhas been very rarely reported.Dosage - The dosage is determined accordingto the needs of the individual patient. Whenadministered as a potassium supplement duringdiuretic therapy, a dose ration of one SLOW-Ktablet with each diuretic tablet will usuallysuffice but may be increased as necessary. Ingeneral, a dosage range between 2-6 SLOW-Ktablets (approximately 16-48 mEq K) daily oron alternate days, will provide adequatesupplementary potassium in most cases.Preferably, administer after meals.Overdosage - Symptoms found inhyperpotassemia closely resemble those ofhypopotassemia; these include asthenia,hypotension, mental confusion, paresthesias,pallor, bradycardia and cardiac arrhythmias.Hyperpotassemia may be treated by i.v.administration of sodium chloride, calciumchloride or calcium gluconate (10-20 ml of a10 percent solution), dextrose (1 DO ml. of a 50percent solution or 1,000 ml of a 10 percentsolution with 30 units of unmodified insulininjection), or by administration of acation-exchange resin which removespotassium, given orally or as a retention enema.Supplied - Tablets (pale orange, coated), eachcontaining 600 mg (8 mEq) of potassiumchloride in a slow-release, inert wax core.References1. ODriscoll, B.J.: Potassium chloride with
diuretics, Brit. Med. J. 11:348, 1966.
Full information available on request
CIBADORVAL, QUEBECH9S iBi 5442R
See page 342
mortality and morbidity in twin preg-nancy:
1. Screening of all pregnant wom-en at 16 to 20 weeks of gestationfor early diagnosis of twin pregnancyby ultrasonography or electrocardio-graphy.
2. Bed rest from time of diagnosisto 34 weeks of gestation.
3. Good maternal nutrition, with aweight gain adequate for two fetuses.
4. No smoking.225. Ultrasonography every 2nd week
to assess fetal growth.6. Management of very early onset
of premature labour with uterine re-laxants.
7. Induction of labour in selectedcases for irreversible fetal growth re-tardation, preceded by determinationof pulmonary maturity.
8. Monitoring of all twins duringlabour.
9. High-energy feeding postnatallyuntil growth retardation is reversed.
References1. BABSON SG, PHILLIPS DS: Growth and de-
velopment of twins dissimilar in size atbirth. N Engi J Med 289: 937, 1973
2. HOHENAUER L: Prenatal nutrition and subse-quent development (C). Lancet 1: 644, 1971
3. POWERS WF: Twin pregnancy: complicationsand treatment. Obstet Gynecol 42: 795, 1973
4. DAvIEs PA, DAVIS JP: Very low birth-weightand subsequent head growth. Lancet 2: 1216,1970
5. WONG KS, SCoTT KE: Fetal growth at sealevel. Biol Neonate 20: 175, 1972
6. USHER R, MCLEAN F, Scorr KE: Judgementof fetal age: II. Clinical significance ofgestational age and an objective method forits assessment. Pediatr Gun North Am 13:835, 1966
7. BENIRSCHKE K, CHUNG K: Multiple pregnancy(first of two parts). N Engi J Med 288: 1276,1973
8. FAItOOQUI MO, GROSSMAN JH I., SHANNONRA: A review of twin pregnancy and pen-natal mortality. Obstet Gynecol Surv 28:144, 1973
9. MORAND G, GUIMONo P: Grossesse multiple:G.A.R.E. et F.A.R.E. Union Med Can 103:296, 1974
10. NYLANOER PPS: Twinning in Nigeria. AdaGenet Med Gemellol 19: 457, 1970
11. GRUENWALD P: Stillbirth and early neonataldeath, in Perinatal Problems: the SecondReport ol the British Perinatal MortalitySurvei', BUTLER NR, ALBERMAN ED (eds),Edinburgh, Livingstone, 1969, p 163
12. KLEIN J: Perinatal mortality in twin preg-nancy. Obstet Gynecol 23: 738, 1964
13. The editorial team: The multiple births, inPerinatal Problems: the Second Report olthe British Perinatal Mortality Survey, opcit, pp 72-140
14. ANDERSON WJR: Stillbirth and neonatalmortality in twin pregnancy. J Obstet Gynae-col Br Emp 63: 205, 1956
15. HENDRICKS CH: Twinning in relation to birthweight, mortality, and congenital anomalies.Obstet Gynecol 27: 47, 1966
16. BARTER RH, Hsu 1, ERKENBECK RV, et al:The prevention of prematurity in multiplepregnancy. Am .1 Obstet Gynecol 91: 787,1965
17. JONAS EG: The value of prenatal bed-restin multiple pregnancy. J Obstet Gynaecol BrCommonw 70: 461, 1963
18. ROBERTSON JG: Twin pregnancy: influence ofearly admission on fetal survival. ObstetGynecol 23: 854, 1964
19. FERGUSON WF: Perinatal mortality in mul-tiple gestations: a review of perinatal deathfrom 1609 multiple gestations. Obstet Gynecol23: 861, 1964
20. CAMPBELL 5, DEWHURST CJ: Quintuplet preg-nancy diagnosed and assessed by ultrasoniccompound scanning. Lancet 1: 101, 1970
21. SUNDEN B: Ultrasound in the diagnosis oftwins and hydramnios. J Obstet Gynaecol BrCommonw 72: 952, 1965
22. FAsIA J: Cigarettes pendant la grossesse,poids de nalssance et mortalit6 p.rinatale.Can Med Assoc J 109: 1104, 1973