Embed Size (px)
Citation preview

Copyright © 2011 Accenture All Rights Reserved. Accenture, its logo, and High Performance Delivered are trademarks of Accenture.
aIPAM Educational Conference
September 29, 2011
John Woerly, MSA, RHIA, CHAM, FHAM
(317)590-3067 [email protected]
"Revenue Cycle Health Check-Up: Learning & Performance Support at its
Finest"

Agenda for today’s discussion
2
Define trends and implications in today’s Provider marketplace
Identify Opportunities for the astute Revenue Cycle Manager
Review Learning & Performance Support Strategy as one way to cultivate self and staff,
and to differentiate oneself
Review the 3 main ingredients and how to set-up each:
o Performance Metrics and Monitors
o Learning Program
o Quality Assurance Program
Solicit participant ideas and best practices

2011 Trends & Implications in the Provider marketplace
Trend (Accenture analysis) Implication
“Cost is king” • Sub trends: Cost Reduction & Utilization Management, Business Model Shifts: Risk Sharing &
Population Management, and Consolidation
• Opportunity to cut cost and improve quality with “sourcing” and labor arbitrage
Connected Health • Opportunity to design and/or implement systems to coordinate patient care in a way that
improves overall productivity, lowers costs and empowers patients
• mHealth or Mobile provider solutions is also an opportunity for sourcing
Electronic Medical Record
(EMR)
• Opportunity to design and/or implement systems that offer providers clinical quality and
strong analytics capabilities value promised by their EMR investments
• Also -- an opportunity for sourcing
Accountable Care Orgs
(ACOs)
• Sub-trend: there is an opportunity to develop and/or implement the next generation of primary
care --that makes use of technology and is more consumer/retail based
Continued decline in paying
patients
• Opportunity to make IT more pervasive to cut operating cost and make care more patient -as -
consumer oriented
• Opportunity for sourcing
Retail Clinics and Online
diagnostics/Telehealth
• Opportunity to develop and /or implement systems that are consumer oriented, convenient
and can be available online
Interoperability • Consumerism and the Patient Experience
• Opportunity to design &/or implement systems that strategically communicate with each other
• Opportunity --for sourcing
Physician Integration &
Clinical Process Improvement
• Opportunity: Coordinate Physician/Ambulatory services, develop financial incentives, cultivate
and leverage physician leaders, collaboration & Clinical Process Improvement
Changing Role of IT & the
Value of Data
• Impact: Increased transparency which can lead to a change in physician behavior/care.
• Opportunity for sourcing 3

Healthcare reimbursement is migrating from a quantity-based
system to a quality-based system
4
Beginning October 1, 2012, CMS will base hospital reimbursement on a system of quality
outcomes, efficiency and patient satisfaction with their healthcare services, referred to as
Value Based Purchasing (VBP).
Reimbursements will be tied to a baseline score or improvements against that baseline.
The better the information gathered up front, the better the end result of the financial
transaction and the resulting patient satisfaction.
The key factors will be:
• Quality, including CMS's Core Measures, patient safety, and readmission and mortality
rates
• Efficiency, including the relative measure of the cost to the hospital for providing services
• Affordability, a relative comparison of prices charged for inpatient and outpatient services
• Patient satisfaction, as measured by the Hospital Consumer Assessment of Healthcare
Providers and Systems (HCAHPS)
Resource: “Don't Forget the Revenue Cycle: The First and Final Impression”. Stephen M. Stewart, MBA, FACHE, CPHIMS,
CHCIO. Advance, September 2011.

So what does this mean for Revenue Cycle operations &
Patient Access more specifically?
Opportunities for YOU and your TEAM . . .
• Demonstrate ability to be trend-setter by gaining new knowledge and fully accepting change
• Know your customers (internal and external): What do they REALLY want?
• Dream in the “future”
• Strive to improve what you are doing today: Little steps are OK!
• Measure outcomes
• Inspire others to achieve great levels of success! Celebrate successes!
• Communicate – to learn, to share, to inspire and to reward!
5

High PerformingRevenue Cycle Model
Accenture’s High Performing Revenue Cycle Vision
What does it take to be a High Performer?
6
Customer
Satisfaction
Financial
Integrity
Operational
Effectiveness
Standardization of Like Functions
Optimized Staffing & Training
Key Performance Metrics
Learning & Performance Support (Performance Metrics & Monitors, Learning & QA)
Core Operational Requirements Core Technology Requirements
Process Automation & Integration
Technology Enabled Work Flow
Enhanced Data Integrity
The Customer Comes First
Collect the Right Amount,
At the Right Time,
From the Right Source
Train & Communicate Effectively
Do it the Right Way
Assign Accountabilities & Reward

One way to get there . . .
Learning & Performance Support Program
Curriculum &
Course Content
Outcome
Management
Performance
Support
Learning
Environment
Learning
Management
• Position Descriptions
• Policies / Procedures
• Job Aids
• Online Repository
• Performance Metrics / SLAs /
KPIs
• User Network
• User Help Desk
• Bulletin Board Assistance /
Chat Room
• Course Scheduling &
Registration
• Logistics
• Competency Testing
• Course Evaluation
• Training History
• Classoom Interaction and Role Play
• Computer-Based Training
• Virtual Business Simulation (Online Practice)
• Coaching & Mentoring
• Newsletters & Other Communications
• Performance-Based
Evaluation Criterion
• Performance Standards
& Metrics
• Performance Monitors,
Reporting & Feedback
• Quality Assurance Audits /
Reviews
• Process Improvement Initiatives
• Orientation, Refresher & Continuing Education:
– Process & Technical Training
– Customer Excellence & Culture
Transformation Training
– Career & Leadership Training
Performance
Improvement &
Sustainability
7

Learning & Performance Support programs deliver
value by . . .
• Aligning senior management team around the organization’s strategy, as well as
alignment up and down the organization
• Communicating strategic objectives to associates and the rest of the organization
• Promoting associate engagement and a culture of accountability & follow-up
• Providing a mechanism for associate learning and feedback
• Serving as a management tool for decision-making and continuous process improvement
8

• Curriculum based upon leading practice processes, as well as materials from various business partners
• Multiple modes of learning utilized, including self-study, classroom style and coaching
• Courses developed by Instructional Curriculum Designers, focused on adult learning and competency measurement
• Various learning tracks (i.e. Beginner, Intermediate, Advanced, etc.) developed, in addition to Certification and Career Laddering programs
• Performance standards, monitors and feedback mechanisms incorporated and utilized to drive performance and outcomes
• Learning strategy and design developed at the Corporate level with training deployed locally
Key Attributes of the Learning & Performance
Support Strategy
Learning & Performance
SupportStrategy
9

Learning & Performance Support Operational Model
Policy / Procedure Development, Competency & Performance Standards,
Certification, and Compliance
Oversight & Coordination
Local Deployment:
• Learning Solution Delivery
• Performance Management Quality
Assurance Audits / Reviews
• Service Level Agreement Coordination
• Process Improvement Initiatives
Centralized Design & Development:
• Learning Solution Design & Development
• Learning Solution Support
• Outcome Management Design,
Development & Support
• Timely maintenance of program materials
Learning Mgt.
System(HealthStream)
Central Data
Repository(QuickBase)
Reporting
Metrics
Blended
Learning Solution
10

What steps do I take to get there?
Operational Foundations (Task 2)
Operational Enhancements (Task 3)
Project Set-Up (Task 1)
Deliverables and Milestones
(Task A) (Task B) (Task C) (Task D) (Task E)
11
Develop Organizational
Structure

What are some required Key Deliverables?
Project Set-Up:
Project Charter
Detailed Project Plan developed and approved
Project Status and Issue Tracking Database
developed
Project Strategy
Organizational Model
Communication Plan (Newsletters, Updates)
Analyze:
Learning and Performance Support Needs
Assessment
Design:
Learning Program Conceptual Design
Management Development Program Approach and
Design
Requirements Matrix
Training Environment Strategy
System Change Request
Training Style Sheet
Training Prototype (Course outline)
Detailed Course Design
Learning Plan template
Build:
Learning and Performance Support (L&PS)
Maintenance Plan
Initial / Pilot Learning and Performance Support
Materials (Training Content, Job Aids, Competency
Tests)
Job Descriptions (related to Learning and
Performance Support team & incorporation of key
components of L&PS within all staff’s job
descriptions)
Policies/Procedures
Test:
Test Protocols / Scenario’s
Pilot Guidelines
Pilot Evaluation and Gap Analysis Report
Post-Implementation Materials (Updates)
Training Environment designed
Final Training Materials (multi-modes of learning)
Final Performance Support Materials
Help Desk Guide
Deploy:
Perform Training and deliver Performance Support
Job Shadow
Update / Refine, as required12

Key Ingredients of a Learning & Performance
Support Program
13
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
Setting up the Action Plan – Phased Approach
SLAs
KPIs
Quality Assurance & Productivity
Phase 3
Phase 2
Phase 1
Performance Standards provide the employee with specific performance
expectations for each major duty. They provide guidance to the employee as
to the results that are expected for satisfactory job performance. They tell the
employee what a good job looks like. The primary purpose of performance
standards is to communicate expectations.
‒ Examples: Staff productivity, process compliance, and data integrity /
quality
Effective Key Performance Indicators measure the department's key activities and
performance, and support a range of stakeholder needs (patients, physicians, internal
customers, etc.). Selected metrics are financial and production based, as well as inwardly
focused on meeting customer requirements and value. These metrics are used to assess
the health of the organization and measure six criteria: time, cost, resources, scope,
quality, and actions.
‒ Examples: Number of days out, cost-to-collect, realization table (projected cost vs.
projected revenue), FTE & staff productivity, incomplete / missing data, etc.
Performance Monitors & ReportsPerformance Monitors & Reports provide a visual display of performance
outcomes. The departmental dashboard provides monthly trended
outcomes on KPIs, helping to monitor, assess and improve performance.
‒ Examples: Reports documenting baselines and benchmarks to actual
performance
Service Level Agreements help define the expectations for service between a department and its
customers and form a critical component to understanding how effective the department is. A
thoughtfully designed SLA operates as a “contract” between the department and its customers, defining
the roles, responsibilities, and expected behaviors for each group. They create a means to develop a
spirit of shared responsibility which is required to create successful end-to-end processes.
‒ Examples: Hours of Operation, Service Offerings, Roles/Responsibilities, Performance
Measurement, Performance Reporting, Customer Support, Escalation Processes, Service
Recovery, Change Orders, Chargeback Approach.
14
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
How To Guide
• Define what to measure. Ensure that data is timely, well-defined, understandable, easily accessible & “true”:‒ Personnel productivity
‒ Registration accuracy rates‒ Front-end impact on claim edits, denials and write-offs, duplicate medical record assignments, and returned mail
‒ Collection rates
‒ Customer satisfaction / service standards (Patients, Physicians, Ancillary Departments, Staff)
• Define how to display– the look and feel:‒ Service line, site, department, individual reporting
‒ Monthly data & trend charts for all levels
‒ Summary information with detail data available upon request
‒ Summary & trending data available for patient access & education staff
‒ Distribution of data via email shared folders
• Develop the plan:‒ Identify available data and data sources
‒ Understand current data issues - work on resolving those issues
‒ Identify resources responsible for reporting
‒ Benchmarking data availability
‒ Determine implementation approach -- “Big-bang” vs. pilot/phase-in
• Start the implementation:‒ Solicit feedback from users in the design (those performing data entry and those receiving the Scorecard)
‒ Draft the Scorecard
‒ Educate users (those performing data entry and those receiving Scorecard)
‒ Test results – Is data measurable, understandable, correct?
‒ Distribute first draft
‒ Receive Feedback on draft Scorecard and make updates
‒ Re-educate, as needed15
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
Metrics Definition Template (SAMPLE)
16
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
Metrics Definition Grid (SAMPLE)
#
E D S Hosp SS
Enterprise Patient Access
# of registrations
Track and trend volumes to
understand staffing and capacity
needs
Weekly, Monthly x x x x x
Average completed visits per day
Track and trend volumes to
understand staffing and capacity
needs
Monthly x x x x
Incomplete registrations by end-
user
Track productivity and accuracy of
registrarsMonthly x x x x
Open Encounter Reports Weekly x x x x
Scheduling
% of patients with complete and
accurate data elements collected
at time of scheduling
Measure productivity and
compliance of schedulers to
complete necessary tasks
Weekly, Monthly x x x x x
Elective. IP/SDS Booked with <2
days Prior to Svc (%)
Trend by physicians to determine
the need and ability to adequately
pre-register the visit prior to service
Weekly, Monthly x x
Medical Screening Completed
(Applicable Services)
Track compliance of registrars /
office staff with use of ABN /
Medical necessity software
Weekly, Monthly x
Scheduling of Service not
meeting medical necessity
guidelines
Evaluate appropriateness /
necessity of scheduled service and
determine if ABN was obtained /
signed
Weekly, Monthly x x x
Calls received from non-Epic
providers
Track the amount of non-TH owned
calls / referrals that Trinity receivesMonthly x
Pre-Admission / Pre-Registration
% of scheduled patients pre-
admitted/pre-registered by
service date
Measure of patients both scheduled
and pre-registered within select
time frames (w/in 24 hours, same
day, etc.)
Weekly, Monthly x x x
% of required registration data
elements complete and
accurate at time of pre-
admission /pre-registration
Measure accuracy and performance
of scheduling staffWeekly, Monthly x x
Outgoing Call Made to
Verify/Complete Pre-admission
Track volume of calls placed to
ensure appropriate staffing is in
place to accommodate volumes
Weekly, Monthly x x
Insurance Verification
Percent of scheduled services
with insurance verified within 24
hours prior to the visit
Measure to ensure that all add-on
visits are receiving appropriate
financial clearance prior to service
Weekly, Monthly x x x
Percent of emergency
admissions with insurance
verified within 24 hours after
admission
Measure to ensure that all ED
admits are receiving appropriate
financial clearance
Weekly, Monthly x x x
Data Required /
Source of Data
Type of Report
(Executive,
Departmental,
Supervisory)
Entity
Indicator Indicator DescriptionFrequency of
Reporting
17
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
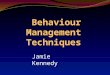
How do High Performers measure success?
High Level Measures
PATIENT ACCESS
Key Performance Indicators
Target
Benchmarks
Scheduled Outpatient Cases (by Centralized
Scheduling) * > 80%
Pre-Registration of Scheduled Outpatients > 95%
Pre-Registration of all Outpatients* > 75%
Registration Accuracy > 98%
% of Duplicate Medical Records < 1%
POS Collections as a % of Net Revenue 3 - 4%
CLINICAL DOCUMENTATION
Key Performance Indicators
Target
Benchmarks
Review Coverage > 70%
Severity of Illness Performance 1.3953 (Ohio)
Mortality Rate *** 2.96%
Query Response Rate 90% Response
Key DRG Pairs
> 80% of Pairs meet
benchmarks
Medical and Surgical CC Categories > 75% meet benchmarks
PATIENT FINANCIAL SERVICES
Key Performance Indicators
Target
Benchmarks
AR Days < 45 Days
Clean Claims > 80%
Discharged Not Final Billed Holds < 5 Days
Aged AR > 90 Days < 20%
Denials as % of Gross Revenue (Initial Claim
Rejections) < 2%
Write-Offs as a % of Net Revenue < 1%
CODING
Key Performance Indicators
Target
Benchmarks
DNFC (IP) < 3 Days
DNFC (ED) < 3 Days
DNFC (SDS) < 3 Days
DNFC (Other Ops) < 3 Days
DNFC (OBV) < 3 Days
Coding Accuracy Rate > 98%
DRG Accuracy Rate > 97%
• Metrics help us understand more about our products, processes, and services.
• Metrics evaluate these products, processes, and services against established standards and goals.
• Metrics provide the information needed to control resources and processes used to produce our capabilities.
• Metrics predict attributes of entities in the future.
18
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
Department Dashboard (SAMPLE)
Performance Metrics Leading
Practice
Patient Scheduling Processing for Central Scheduling Areas
Total New Cases Scheduled Annually (Central Scheduling)
Appointments made via Fax / Web 20-25%
Turnaround time for Fax / Web Appointment Response < 8 hrs
Average % Appointments Cancelled (by facility & department) < 10%
Average % Appointments Rescheduled (by reason & appointment
date)
< 15%
% “No Show” Cases (by cancel date, appt date and reason) < 10%
Total Stat Cases
Total Add-on Cases
% Cases Scheduled by Central Scheduling > 80%
Unfilled / Same Day Appointments Utilized (Open Access)
Success Rate in Accommodating Same Day Appointment
Requests (Note: Must consider impact to 3rd party requirements)
≥ 90%
Next 3rd Available Appointment < 72 hours
Accuracy Rate (Data Integrity) > 98%
LMRP / LCD Review at point of Scheduling 100%
Utilization of Genesis Standard Physician Order form > 75%
# of New Cases scheduled per FTE 70 per day
Performance Metrics Leading
Practice
Call Handling
Call volume (Operator /Switchboard level)
Overall
Overall % of call volume triaged to Central
scheduling
Call Volume (Incoming and Outgoing) – By day,
week, month, year
Average Call Response Time < 20 secs
Average Calls Answered within 20 seconds > 80%
Average Call Abandonment Rate < 4%
Average Talk Time (Scheduling Only) < 180 secs
Average Call Hold Time (Queue Time) < 30 secs
Average Maximum Call Hold Time < 180 secs
Agent Availability to Schedule > 90%
19
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
Department Metrics (SAMPLE)
20
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Performance Metrics & Monitors
Visual Management Techniques
Display Results – Communicate!
Other Methods: E-Mail Updates, ShareDrive Access
21
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Basic
Intermediate
Advanced
World Class
Learning Program
Levels of Maturity
As learning programs progress they are more
comprehensive and strategic versus tactical.
• Informal; On the job
• No Policies and
Procedures
• Training conducted by
peers
• No line of sight to strategy
• No individual
development plans
• Training part of staff function
• Some Policies and
Procedures
• Minimal formal training
• More formal systems training
• No line of sight to strategy
• No individual development
plans
• No measurement of
learning effectiveness
• Dedicated Training Staff
• Formal Policies and
Procedures
• Defined Learning Objectives
• Formal Training Materials
• Some Audit and Review
• Some proficiency testing
• Limited manager/
leadership involvement.
• Some measurement of
learning effectiveness
• Use of Learning
Management Systems
• Fully Implemented Learning
Strategy and Deployment
• Performance Improvement
Based Learning
• Defined Learning Plan for
each associate
• Learning Objectives tied to
Performance Outcomes
• Training materials designed
by Instructional Designers
• Fully integrated proficiency
and certification programs
with staff performance
reviews
• High level of manager and
leadership support and
involvement
• Associates take
accountability for learning
Traditional Training High Impact Learning & Development
Good to Great
22
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Learning Program
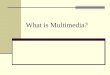
The ROI of Associate Training and Development
• Organizations that invest in more training
days and dollars per associate may
produce greater revenue per employee
than those that invest less in this
important human capital process. 1
• Investing in improving the associate
experience to improve the customer
experience results in greater associate
and customer loyalty and lower costs to
serve customers. 2
• A firm’s investment in associate training is
the single most powerful predictor of stock
price. 3
Median Revenue Per Employee
$137,931
$210,380
$-
$50,000
$100,000
$150,000
$200,000
$250,000
Equal to or Less than 5
Days
Greater than 5 Days
Average Learning Day Per Employee
Sources: 1) APQC, Open Standards Benchmarking Collaborative,
data retrieved June 2008
2) APQC, Managing the Total Customer Experience, 2004
3) Media Communications Association International, “Finally, Proof that Training Works!,” May 2005
34% increase
23
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Learning Program
Training Guide by Job Role (Sample)
Role
Education Tools & Methods Assessment Tools & Methods Related Job AidsRelated Policies and
Procedures
Bring in payor rep Online testing Payor Inventory List Pre-Service/Financial Clearance
Screen shot of insurance card with
interactive info index on intranet QA/Denial Management
Observation
Screen shots Observation/On the job
Keystroke emulation Online testing
CMS Learning Tools Mystery observers
Role-playing Demonstration
Instructor lead tests based on
scenarios Report cards
Role playing Error tracking
Coaching & counseling Denial data
Skills Lab - multpile stations with
hands on learning, make it fun!
Required for all staff to do yearly.
Test at each station, either
verbal or written. Must pass all
subsections
Online assessment test via intranet;
helps management determine weak
areas in training
Job
Competencies
Registrar
Performance Objectives & Required
Skills
Selecting correct insurance plan
(Obtaining eligibility) differentiating
different insurance programs off card
Financial (Math) Skills
Hospitality
Understand insurance benefits -
effectively read, interpret, & explain
benefits to patients
98% accuracy rate on all accounts
registered
Screening - Financial
Performing a CPI Search
Interpreting insurance plans/cards
Medicare MSPs, ABNs
Verify demographic information on each and every occurrence
Communication skills - effectively and courtesly explain registratation and health care reimbursement issues and financial obligations
Interviewing skills
POS Collections
24
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Learning Program
Training Curriculum Planning Guide (Sample)
25
Financial Clearance / Registration & Check-in
- Financial Clearance Overview
- Financial Clearance WorkflowClass Kim, Denise PA, FC, Decn ~ 95 4 Sessions
- Pre-Registration & Registration/Check-in CBL PA, FC, Decn
- Insurance Eligibility & Benefit Verification
- Referral Management
- Authorization Management
Class w/ yearly
CBL
Amanda, Donita,
Karen, DenisePA, FC, Decn, RC ~ 120 5 sessions
- Patient Liability Calculation & Collection
- Patient Notification / CommunicationCBL PA, FC, Decn, RC
- EscalationSection may be removed as majority of the information contained in this section is now within the Delay Postpone training module. A
review with section managers will help determine the final outcome,
Training Module(s)
Delivery Method
(Class, CBL,
Hybrid)
Presenter
Applicable Staffing
Groups (CS, FC, PA,
RC, Decn)
Approx.
number of
participants
Total SessionsTime Frame (in
hours)
Future State Overview
- Future State Operating Model Overview Complete: Overview provided to staff in late July and early August
- New Job Descriptions & Org StructurePatient Access Managers/Supervisors will provide and communicate new job descriptions and org chart with staff during the week of
August 22nd
Scheduling
- Overall Scheduling Process (PPT) Class Norma/Tina
Phase I – All Tempus
Users
Phase II – All
schedulers from
decentralized areas
Phase I: ~20
Phase II: ~40
(lots of cross
trained staff in
Decn areas)
2-3 Sessions
- Medical Necessity for Medicare
• Part I – Passport for Medical Necessity (PPT)
• Part II – ABN Process (PPT)
• Part III – CBL on using system
Part I & II: Class
Part III: CBL
Part I & II:
Denise I: CBL
CS, PA, FC,
Decentralized
Part I, II, III: All
Scheduling (CS,
Decn), FC, PA
4 sessions (25
per)
Part I: 0.5
Part II: 0.5
Part III: 0.25
CS – Central Scheduling; FC – Financial Clearance; PA – Patient Access (Registration); RC – Resource Counseling, Decn - Decentralized
Performance Metrics & Monitors
Learning Program
Quality Assurance Program

Quality Assurance Program
Areas of Focus
26
Performance Metrics & Monitors
Learning Program
Quality Assurance Program
• POS Registration Errors – Missing and Incorrect Data
• Pre-Bill Edits / DNFB
• Duplicate Medical Record / Account Assignment
• Returned Mail
• Denials
Outcomes
Associate accountability & engagement
Robust feedback and communication
Effective education & training
Continuous quality & performance improvement

Quality Assurance Program
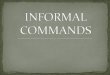
Review Methods
27
Performance Metrics & Monitors
Learning Program
Quality Assurance Program
Automated Process - Real-Time /
POS or Post-Service
↑ Highly accurate
↑ Provides quick response time (to fix
and to communicate issue)
↑ Provides detailed trends
↓ Complex rules to set-up & maintain
↓ Only as good as the rules
↓ Expensive to purchase & maintain
Reg. Audit Sheet
Facility: _______________
Account Number: _____________ Service Date: ______/______/______
User: _______________ Patient Type: IP OP OBV EC DSU Recurring
Data Elements Wt. Error TOTAL
Patient Type AuditedPatient Data
Name 2 0
Gender/Sex 1 0
SS# 2 0
DOB 2 0
Address/Zip Code 2 0
Telephone Number 2 0
Guarantor Data
Guarantor Name 2 0
Relationship 1 0
Guarantor SS# 1 0
Guarantor Phone Number 2 0
Employer's Name 2 0
Employer's Address/Zip Code 2 0
Employer's Phone Number 1 0
Visit Specific Data
Physician-Primary/Referring/PCP/IPA 2 0
Financial Class 1 0
Insurance Data
Insurance Company Name/Code 2 0
Insured Name 2 0
Contract Code 2 0
Relationship 2 0
Insured SS# 1 0
Policy # 2 0
Group Name/# 2 0
Effective Date 2 0
Pre-cert # / PCP Authorization # 2 0
InsuranceAddress/Zip Code 2 0
Insurance Telephone Number 2 0
Workers' Compensation
Occurrence Code / Injury/Illness Code *** 2 0
Accident/Illness Date/Time *** 1 0
W/C Name/Code *** 2 0
W/C Carrier Address *** 2 0
W/C Carrier Phone Number *** 1 0
Attachments/Signatures
Insurance Card Copies 1 0
ID/Driver's License Copy 1 0
Financial Agreement 1 0
Consent for Treatment 1 0
Co-pays/Deductibles $ Collected 1 0
Past Accts $ Collected 1 0
MSP Form/Data Entered*ALL 1 0
Important Msg (Medicare/Champus)*IP Only 1 0
Non-Coverage Waivers/ABN** 1 0
POSSIBLE ERRORS 63
TOTAL ERRORS (Wtd.) 0
ACCURACY RATE (%) 100%
1. Medicare *IP - or - Medicare*ALL
2. ABN Required **
3. Workers' Comp ***
Error Checker enters:
1. Facility (hospital name), Account #,
User/Registrar's Initials, Service Date,
Patient Type (SEE ABOVE)
3 Categories (Only count the above astericked data fields, if the Error
Checker indicates one of the below categories)
Manual Process - Post-Service
↑ Quick deployment
↑ Provides a level of awareness to issues
and trends
↑ Relatively inexpensive, other than time
↓ Varied accuracy
↓ Slower response time
↓ Time consuming to conduct & to monitor
trends

Conclusion
• Sound leadership and associate development has quantifiable returns to the organization
• Incorporating the leading practice Learning and Performance Support Strategy in
operational design and delivery ensures higher “payoffs” and ensures sustained process
improvements
• World Class Learning is attainable and when actualized will differentiate the organization in
the marketplace
28

Questions & Participant Input