Embed Size (px)
Citation preview

Proc. Natl. Acad. Sci. USAVol. 86, pp. 2103-2106, March 1989Neurobiology
Resistance to axonal degeneration after nerve compression inexperimental diabetes
(fiber injury/streptozotocin-induced diabetes/nerve myo-inositol, sorbitol, and fructose)
PETER JAMES DYCK, JANEAN K. ENGELSTAD, CATERINA GIANNINI, ALFRED C. LAIS,SHARON R. MINNERATH, AND JEANNINE L. KARNESPeripheral Neuropathy Research Laboratory, Mayo Clinic and Mayo Foundation, Rochester, MN 55905
Communicated by Ralph T. Holman, December 19, 1988 (received for review August 8, 1988)
ABSTRACT To determine the effect of diabetes on thedevelopment of axonal degeneration after acute nerve com-pression, the mobilized peroneal nerves of rats with strepto-zotocin-induced diabetes and of control rats were compressedat 150 mmHg (1 mmHg = 133 Pa) for 30 min by using speciallydevised cuffs. At three intervals after compression-3 days,rats diabetic for 31 wk; 14 days, diabetic for 6 wk; and 24 days,diabetic for 31 wk-groups of nerves were studied to assessnumbers and sizes of fibers above, at, and below the cuff andto assess frequency of fiber degeneration in teased fibers fromnerve distal to the cuff. Teased fibers with pathologic abnor-malities were more frequent in nerves from controls than innerves from diabetic rats in all three groups but the differencewas statistically significant only at 3 and 14 days after com-pression. The lack of significant difference at 24 days may beexplained by higher rates of disappearance of degeneratingproducts and of fiber regeneration at 24 than at 3 and 14 days.This study provides evidence that in addition to delaying thereported functional deficit of vibratory detection threshold andconduction block during nerve compression, diabetes also maypartially prevent axonal injury. Low nerve myo-inositol con-centration did not predispose diabetic nerve to acute compres-sion injury. If these results also apply to human diabetes andif repeated acute compression is involved in the genesis of fiberdegeneration in entrapment, then a higher frequency of en-trapment neuropathy among diabetics might be due to mech-anisms other than increased susceptibility of fibers to acutecompression-e.g., possibly to greater constriction of nervedue to pathologic alterations of the carpal ligament.
Chronic entrapment neuropathies, such as the carpal tunnelsyndrome, are said to be more common among diabetics (1,2) than among nondiabetics. An epidemiologic population-based review of medical records in Olmsted County seems toindicate that the carpal tunnel syndrome is two to three timesmore frequent in diabetics than it is in the general population(J. C. Stevens, personal communication). Assuming entrap-ment neuropathy to be more common in diabetes, excessivefiber vulnerability, decreased reparative capacity, or in-creased external constriction may be involved. On the otherhand, vibratory perception (3, 4) and nerve conduction (5, 6)fail earlier during cuff compression in controls than indiabetics, suggesting that diabetes inhibits the developmentof functional deficits.The present studies assess whether standard cuffcompres-
sions of the peroneal nerve cause a significantly lowerfrequency of fiber degeneration in controls than in strepto-zotocin-induced diabetic rats.
MATERIALS AND METHODSCuff Design. The cuff used in study 1 consisted of two
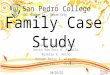
balloons each fitted over rectangular box-like metal frameswith the open side (bottom or top) of each frame facing thenerve (Fig. 1). The necks of the balloons were tied and gluedto a short tube that was soldered into the sides of each frameconnecting an aneroid manometer with the inside ofthe frameand balloon. The inner surfaces of the balloons were glued tothe outer surfaces of the sides and closed (top or bottom) sideof the metal frames facing away from the nerve. At varioustimes (see Results) after the rats became diabetic the deflatedballoons and frames were positioned so that one balloon andits frame were under a mobilized 1-cm segment of theperoneal nerve and the other balloon and frame were over it.When the two apposing balloons were inflated, the nerve wassqueezed between them. The pressure used in an experimentwas the pressure desired on the nerve plus the pressureneeded to just appose the balloons in air for the width of thecuff.
In study 2, the balloons were made of nondistensiblesilastic sheeting with subdermal implants (no. 501-1, Dow)(cuff 2), but in other respects the cuffwas exactly like the firstcuff. The balloons were fashioned so that when just inflatedbut at 0 pressure, their apposing surfaces would just meet forthe width of the cuff. The pressure exerted on the nervetherefore should be the same as that recorded on themanometer.Both cuffs were 8 mm wide.Histologic Processing. At 3, 14, and 24 days after cuff
compression [150 mmHg (1 mmHg = 133 Pa) for 30 min], theperoneal nerve was fixed in situ for 15 min with 4% glutar-aldehyde in 0.025 M sodium cacodylate buffer at pH 7.38(body temperature). After fixation, the nerve was removedand immersed in 2.5% glutaraldehyde in buffer for 24 hr forepoxy embedding and for 1 hr for teased fiber preparation.The further histologic processing and method of teasing toprovide representative samples were as outlined elsewhere(7).Morphometric and Teased Fiber Assessment. Transverse
0.75-,um epoxy-embedded sections of the fixed nerves werestained with phenylenediamine, and the number of myelin-ated fibers (MFs) per nerve and the size distribution of MFdiameters (diameter of a circle of equivalent area) wereobtained by using previously described techniques and ourimaging system for nerve morphometry (ISNM) (7). MFprofiles considered to represent degenerating fibers were notincluded.One hundred teased fibers from each peroneal nerve were
graded according to our published criteria (7): A = normal;B = myelin irregularities; C= demyelination; D = demyelin-
Abbreviation: MF, myelinated fiber.
2103
The publication costs of this article were defrayed in part by page chargepayment. This article must therefore be hereby marked "advertisement"in accordance with 18 U.S.C. §1734 solely to indicate this fact.
Dow
nloa
ded
by g
uest
on
June
4, 2
020

Proc. Natl. Acad. Sci. USA 86 (1989)
>air pressure
- Inflated cuff over metalframe compressingperoneal nerve
FIG. 1. Mobilized peroneal nerve ofrat was compressed between two inflated balloons, one positioned beneath and the other above the nerve.The cuffs are balloons (solid lines and hatching) held in place by underlying metal frames (broken lines) whose edges in the inflated positiondid not contact nerve. For study 1, the balloon was Silastic; for study 2, an improved design was used (see text).
ation and remyelination; E = axonal degeneration; F =remyelination; and G = focal myelin reduplication. To ensurethat a fiber was undergoing axonal degeneration and notsimply demyelination of consecutive internodes, myelinovoids and balls at the same stage of degeneration had toextend for a distance judged to be at least four internodes.
Studies. Study 1. Male 250-g Sprague-Dawley rats were eartagged and randomly assigned to diabetic and control groups.Diabetes was present (fasting plasma glucose > 16 mmol/liter) by the third day after an intraperitoneal injection ofstreptozotocin (60 mg/kg). Controls were pair-fed.Under pentobarbital anesthesia, peroneal nerves were
exposed by blunt dissection without interruption of the bloodsupply and were undercut for a distance of 1 cm. The cuffwaspositioned, inflated to 150mmHg for 30 min, and thendeflated. The nerve was kept moist with Ringer's saline. Thewound was closed by surgical clips. The same procedure thenwas performed on the contralateral side. On day 4, the leftwound was reopened, and the peroneal nerve was exposedand fixed in situ with glutaraldehyde. After removal of thenerve, this limb was amputated at the upper thigh, because insitu fixation prevented wound healing. Collars of nerve tissuewere taken from the nerve above, at, and below the cuff,osmicated, and embedded in epoxy. An 8-mm length ofnervedistal to the distal tissue collar was used for the preparationofteased fibers. On the 25th day, the right peroneal nerve wasfixed and processed by the same methods. Four nerves wereused from each of the 3-day and 24-day diabetic groups andsix nerves were used from each of the 3-day and 24-daycontrol groups.
Study 2. The second study was performed because (i) theresults that were obtained in study 1 needed confirmationbased on a larger study, (ii) an improved cuff was designedto deliver more exact pressures, and (iii) glucose, fructose,sorbitol, and myo-inositol concentrations were to be studied.The selection and feeding of groups, the position of the cuff,the pressure and duration of cuff compression, and themethods of nerve processing were like those in study 1. Thecompression was performed at 6 wk after induction of thediabetic state, and the tissue was harvested 14 days later. The
right unfixed peroneal nerve was frozen in isopentane at-800C until analysis, and the endoneurial glucose, fructose,sorbitol, and myo-inositol concentrations were measured asdescribed (8).
RESULTSStudy 1. The rats had been diabetic for 31 wk before the
nerves were compressed.Experiment 1: 3 days after cuff compression. Teased Fi-
bers. Many teased fibers were undergoing changes typical,but not diagnostic, of early axonal degeneration. The fre-quency (mean ± SD) of all teased fiber abnormalities, mainlymyelin irregularities (condition B) and paranodal demyelina-tion (condition C), was significantly higher in controls (27.1%± 12.4%) than in diabetics (8.0% ± 4.3%; 0.025 > P > 0.01)(Fig. 2).Morphometry. The numbers of MFs per nerve were not
significantly different between diabetics and controls above,at, and below the cuff. MF diameter and In(axonal area) weresmaller in the diabetic nerves than in control nerves. Thesedecreases cannot be attributed to the compression injurybecause they also were found in proximal nerve and aretypical of nerve in untreated streptozotocin-induced diabetes(9, 10). For this reason, we compared differences betweencontrols and diabetics in MF diameter, In(axonal area), andIn(myelin area) at and distal to the cuff relative to valuesproximal to it at the 2.5th, 50th, and 97.5th percentiles. Nostatistically significant difference was found (table onrequest).Experiment 2: 24 days after cuff compression. Teased
Fibers. The frequency (mean ± SD) of all abnormalities ofteased fibers was higher in controls (42.7% ± 11.7%) than indiabetics (34.7% ± 19.5%), but this difference was notstatistically significant (P > 0.05).Morphometry. No statistically significant differences be-
tween diabetics and controls were found for MF diameter,In(axonal area), or ln(myelin area).
Study 2. The mean body weights of the diabetic and controlrats were not significantly different at the time of sacrifice;
2104 Neurobiology: Dyck et A
Dow
nloa
ded
by g
uest
on
June
4, 2
020

Proc. Natl. Acad. Sci. USA 86 (1989) 2105
605 Control SD
50-Streptozotocindiabetes
40 -
% 30
20
10
00.01<P<0.025 0.01<P<0.025 P >0.05
3 14 24
Days after cuff application (30 min, 150 mm Hg)* Most abnormal fibers showed B and C change
Most abnormal fibers showed E change
FIG. 2. Percentage of teased MFs of peroneal nerve of strepto-zotocin-induced diabetic rats and control rats showing pathologicabnormalities at 3, 14, and 24 days after cuff application. The rats forthe 3- and 24-day studies (study 1) had been diabetic for 31 wk,whereas the rats for the 14-day studies (study 2) had been diabetic for6 wk. For all groups of nerves, average mean frequency of pathologicabnormality was higher in control nerves than in diabetic nerves. Thedifference was statistically significant (0.01 < P < 0.025) in the 3- and14-day groups.
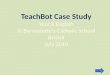
the rats had lost -50 g in weight in both groups since theinduction of diabetes. Mean fasting plasma glucose was 4.3mmol/liter in controls and 19.8 mmol/liter in diabetics (P <0.001). There was a manyfold increase of endoneurial glu-cose, fructose, and sorbital in the endoneurium of diabeticnerves (P < 0.001, Fig. 3). By contrast, endoneurial myo-inositol was decreased to less than one-half of that in controls(P < 0.015, Fig. 3).Teased Fibers. The frequency of abnormality was signifi-
cantly higher in controls (38.2% ± 13.4%) than in diabetics(25.4% ± 10.1%, 0.01 < P < 0.025) (Fig. 2). Axonal degen-eration was almost the only pathologic abnormality encoun-tered. Less than 1% of the abnormalities were demyelinationor remyelination changes.Morphometry. In previous studies we have established
that the number of MFs in peroneal nerve of control rats isnot significantly different between the proximal and distal (tothe cuff) levels but that the fiber diameters are slightly
5 505._
a 400
@ 30
0)
._
0 20
\ 10
0
myo-inositolFI
0
.0
A
I 1.
0
0
fructose[ W51
20[
15 [
10
5
0
C D C D C Dp=.015 p<.001 p<.OO0
smaller, due to tapering, in the distal level (data on request).Streptozotocin diabetes in rats does not induce a change innumber of MFs per nerve but prevents development orreduces axon caliber (9). Direct comparison of numbers andsize distribution of MFs per nerve in the distal segment ofcontrols and diabetics might reflect loss of fibers fromdegeneration or gain offibers from regeneration. The diabeticcondition might affect the size of fibers. To minimize theeffect of the diabetic condition, we normalized the morpho-metric results of distal nerve to that of proximal nerve. Rateof fiber degeneration was estimated separately by analysis ofteased fiber conditions (previous section).The mean transverse fascicular area of the distal nerve was
increased by -70%o in controls and by =30% in diabetics (P< 0.001) relative to the proximal nerve (Fig. 4). For controlsand diabetics, the number of MFs per nerve was =20% lessdistal to the cuffthan proximal to it. The difference in numberof MFs per nerve of distal from proximal nerve was greaterin controls than in diabetics but this did not reach statisticalsignificance (Fig. 4). Similarly, differences in median MFdiameter, myelin area, and axon area below as compared toabove the cuff in controls and diabetics did not reachstatistical significance.
DISCUSSIONIn the present study we show that cuff compression of themobilized peroneal nerve of rat at 150 mmHg for 30 mininduces axonal degeneration of approximately one-third ofMFs below the level of the cuff. In an earlier study, using thesame cuff employed in study 1, we had found that nervecompression also induces demyelination and remyelinationof a proportion of the MFs at the level of the cuff (11).Among the times tested, 14 days appeared to be the most
appropriate time because the pathologic abnormalities werebetter expressed than at 3 days or at 24 days. At 3 days thecharacteristic pathologic abnormalities of axonal degenera-tion in teased fibers were not yet fully expressed and by 21days the characteristic changes had partially disappeared. At3 days, myelin ovoids may have been included spuriously inmorphometric results, thus overestimating the numbers ofintact fibers. At 24 days, myelin ovoids and balls in degen-erating fibers were small and widely spaced or nonexistent.At this time, regenerated fibers are well developed andappear as normal fibers. Our studies suggest that grading ofteased fibers was more sensitive for detection of fiberdegeneration than was estimating the numbers and sizes ofMFs.
200
Li~0
.)
£D Q0 E
0o'
C Dp=.003
FIG. 3. Endoneurial myo-inositol was significantly decreased,whereas endoneurial glucose, fructose, and sorbitol were signifi-cantly increased in diabetic as compared to pair-fed rats (C and D).According to one viewpoint, the lower concentration of myo-inositolmight predispose diabetic nerves to higher rates of injury, but despitelower myo-inositol levels diabetic nerve fibers were less vulnerableto compression injury than were control nerves.
160
120
80
40
0
IT
P -: 0.00.1 P :>0.05TFA MF,
no. nerve
P :>.05MF diam
P >0.05 P 0 05Myelin Axon area
area (med) (med)
FIG. 4. Morphometric results shown as differences (%) betweendistal and proximal measurements. TFA, transverse fascicular area;MF, number of MFs per nerve; MF diam, MF diameters; med,median. Nerve was from controls and diabetics at 14 days after cuffcompression. Except for TFA, no statistically significant differenceswere found.
Neurobiology: Dyck et al.
I
I
I
I
Dow
nloa
ded
by g
uest
on
June
4, 2
020

Proc. Natl. Acad. Sci. USA 86 (1989)
A statistically significant higher frequency of fiber abnor-mality distal to the cuff in controls than in rats with strepto-zotocin-induced diabetes was found at 3 and 14 days after cuffcompression. The frequency of abnormality was also higherin controls than in diabetics at 24 days, but statisticalsignificance was not attained possibly because myelin de-generative products had disappeared from some nervestrands and regenerating fibers had developed that coulddilute the differential effect. The frequency of fiber regener-ation was not evaluated because it would be expected to bedecreased in the diabetics as a result of fewer fibers havingdegenerated.Why was a statistically significant difference of number of
MFs per nerve in the distal as compared to proximal nervenot demonstrated in control as compared to diabetic nervewhen a statistically significant increase in teased fibersundergoing degeneration was demonstrated? First, in teasedfibers one estimates directly the rate of degenerating fibers,whereas in morphometric assessment nondegenerated andregenerating MFs are estimated-an indirect measure of fiberdegeneration. Second, even by 14 days considerable axonalregeneration into the distal nerve segment is expected andwas observed. The frequency of regeneration would beexpected to be higher in nerves with higher frequency ofdegeneration, since regeneration follows degeneration, thusdiminishing differences between controls and diabetics.
It has been stated that nerves in diabetics are morevulnerable to acute compression (1, 2), but there is evidenceto the contrary. Paresthesia and increase of the vibratorydetection threshold and development of nerve conductionblock fail sooner during compression in controls than indiabetics (3-6). The present study extends previous studiesto show that diabetes not only retards the development offunctional alterations of nerve fibers but also inhibits degen-eration of fibers.How can resistance to compression axonal degeneration in
experimental diabetes be explained? It seems unlikely that itcould be due to alterations in the amount of endoneurial fluidor in its constituents because the endoneurial fluid is assumedto be displaced from beneath the cuff in controls anddiabetics. The difference also cannot be explained by differ-ences in numbers of fibers in control and in diabetic ratsbecause these were not different. The fiber attenuation thatoccurs in untreated diabetes might predispose diabetics, andnot controls, to fiber degeneration. The low endoneurialcontent of myo-inositol found in this study also mightpredispose diabetic nerves to fiber degeneration (12-14), butthe converse was found arguing against a role of myo-inositoldeficiency in predisposing nerve to fiber injury from acutecompression. It may be that the bases for resistance toischemic conduction block and for resistance to compressionaxonal degeneration are the same-a greater store of energy-producing substrate or a decrease in metabolic requirementof nerve fibers in diabetics (15, 16).The present study may have implications for understanding
nerve vulnerability to compression and entrapment. Gilliattand Harrison (17) made a distinction between acute com-pression and entrapment nerve injuries, with increased pres-sure known to be involved in the former but not known to beinvolved in the latter. On the other hand, repeated minordegrees of compression of the nerve, particularly duringunusual joint activity or position, may be involved along withother mechanisms in entrapment nerve injury. The relative
contributions of mechanical displacement of axoplasm, isch-emia, stretch, tethering, and other tissue alterations to nerveinjury in acute compression and entrapment are still unre-solved (18-23).Assuming that compression neuropathy is more common
in diabetics than in controls, mechanisms other than in-creased vulnerability of diabetic nerve fibers must be impli-cated. The present studies strongly imply that diabetic nervefibers are less vulnerable to compression injury. Pathologicalterations of the connective sheaths of nerve or of theligaments overlying nerves-e.g., alteration of the amountand flexibility of connective tissue as a consequence ofprotein glycation-might be a basis for increased compres-sion of the median nerve by the carpal ligaments (24).
1. Mulder, D. W., Lambert, E. H., Bastron, J. A. & Sprague,R. G. (1961) Neurology 11, 275-284.
2. Phalen, S. G. (1970) J. Am. Med. Assoc. 212, 1365-1368.3. Steiness, I. B. (1959) Acta Med. Scand. 163, 195.4. Steiness, I. B. (1961) Acta Med. Scand. 170, 319.5. Jaramillo, J., Simard-Duquesne, N. & Dvornik, D. (1984) Can.
J. Physiol. Pharmacol. 63, 733.6. Seneviratne, K. N. & Peiris, 0. W. (1969) J. Neurol. Neuro-
surg. Psychiatry 32, 462.7. Dyck, P. J., Karnes, J., Lais, A., Lofgren, E. P. & Stevens,
J. C. (1984) in Peripheral Neuropathy, eds. Dyck, P. J., Tho-mas, P. K., Lambert, E. H. & Bunge, R. (Saunders, Philadel-phia), pp. 760-870.
8. Dyck, P. J., Zimmerman, B. R., Vilen, T. H., Minnerath,S. R., Karnes, J. L., Yao, J. K. & Poduslo, J. F. (1988) NewEngl. J. Med. 319, 542.
9. Jacobsen, J. (1976) Diabetologia 12, 539.10. Sugimura, K., Windebank, A., Natarajan, V., Lambert, E. H.,
Schmid, H. H. 0. & Dyck, P. J. (1980) J. Neuropathol. Exp.Neurol. 39, 710.
11. Dyck, P. J. (1969) Arch. Neurol. 21, 73.12. Greene, D. A. & Lattimer, S. A. (1987) in Diabetic Neuropa-
thy, eds. Dyck, P. J., Thomas, P. K., Asbury, A. K., Wine-grad, A. I. & Porte, D., Jr. (Saunders, Philadelphia), pp. 289-298.
13. Sima, A. A. F., Brismar, T. & Yagihashi, S. (1987) in DiabeticNeuropathy, eds. Dyck, P. J., Thomas, P. K., Asbury, A. K.,Winegrad, A. I. & Porte, D., Jr. (Saunders, Philadelphia), pp.253-259.
14. Winegrad, A. I. & Simmons, D. A. (1987) in Diabetic Neu-ropathy, eds. Dyck, P. J., Thomas, P. K., Asbury, A. K.,Winegrad, A. I. & Porte, D., Jr. (Saunders, Philadelphia), pp.279-288.
15. Low, P. A., Ward, K., Schmelzer, J. D. & Brimijoin, S. (1985)Am. J. Physiol. 248, E457-E462.
16. Low, P. A., Schmelzer, J. D. & Ward, K. K. (1986) Am. J.Physiol. 250, E94-E99.
17. Gilliatt, R. W. & Harrison, M. J. G. (1984) in Peripheral NerveDisorders, eds. Asbury, A. K. & Gilliatt, R. W. (Butterworth,London), pp. 243-286.
18. Weiss, P. & Hiscoe, H. B. (1948) J. Exp. Zool. 107, 315.19. Denny-Brown, D. & Brenner, C. (1944) Arch. Neurol. Psychi-
atry 52, 1.20. Ochoa, J., Fowler, T. J. & Gilliatt, R. W. (1972) J. Anat. 113,
433.21. Aguayo, A., Nair, C. P. V. & Midgley, R. (1971) Arch. Neurol.
24, 358.22. Richardson, P. M. & Thomas, P. K. (1979) J. Neurosurg. 51,
178.23. Lundborg, G., Myers, R. & Powell, H. (1983) J. Neurol.
Neurosurg. Psychiatry 46, 1119.24. Brownlee, M., Vlassara, H. & Cerami, A. (1984) Ann. Intern.
Med. 101, 527-537.
2106 Neurobiology: Dyck et A
Dow
nloa
ded
by g
uest
on
June
4, 2
020