Embed Size (px)
Citation preview

Hindawi Publishing CorporationBiochemistry Research InternationalVolume 2013, Article ID 189430, 6 pageshttp://dx.doi.org/10.1155/2013/189430
Research ArticleRisk of Cardiovascular Diseases in Diabetes Mellitus and SerumConcentration of Asymmetrical Dimethylarginine
Seema L. Jawalekar,1 Aarti Karnik,2 and Anil Bhutey3
1 Department of Biochemistry, Sree Narayana Institute of Medical Sciences, Chalakka, Ernakulam, Kerala, India2Department of Biochemistry, ACPMMedical College, Dhule, Maharashtra, India3 Department of Biochemistry, Panjabrao Deshmukh Medical College, Amravati, Maharashtra, India
Correspondence should be addressed to Seema L. Jawalekar; [email protected]
Received 2 July 2013; Revised 25 August 2013; Accepted 25 August 2013
Academic Editor: R. J. Linhardt
Copyright © 2013 Seema L. Jawalekar et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Introduction. Asymmetric dimethylarginine (ADMA) is a nonselective nitric oxide (NO) synthase inhibitor associated withcardiovascular and metabolic disorders. ADMA plays an important role in the regulation of vascular tone by acting as anendogenous inhibitor of NO synthesis. Objectives. This study aimed to investigate ADMA with respect to diabetes and its clinicalrelevance as an independent predictor of CAD (Coronary Artery Disease). Methodology. The present case control study includestwo hundred and forty patients selected randomly. SerumADMAwas analyzed by using enzyme immunoassay for the quantitativedetermination of endogenous ADMA, and serum nitric oxide was estimated by the method of Cortes. Results. Elevated NO levellevels was a strong predictor and significantly (𝑡: 9.86, 𝑃 < 0.001) associated with occurrence of CAD. Increased ADMA levelwas found to be another strong predictor and associated significantly (𝑡: 8.02, 𝑃 < 0.001) with CAD. On intra group analysis,the relationship between ADMA and NO in diseased group, is significant negative correlation (𝑟 = −0.743). 𝑃 (0.001) was foundbetween ADMA and NO. Conclusion. ADMA level was found to be one of the strong predictors for CAD. ADMA is an emergingindependent risk marker for future CVD (cardiovascular disease) events.
1. Introduction
Cardiovascular disease (CVD) is the major cause of mor-bidity and mortality in patients with diabetes mellitus(DM). Diabetes is at high risk for several cardiovasculardisorders: coronary heart disease, stroke, peripheral arterialdisease, cardiomyopathy, and congestive heart failure [1–3].Endothelial dysfunction is a common feature in diabeticpatients and may contribute to cardiovascular morbidity [4–6]. Mechanisms of diabetes-induced endothelial dysfunctioninclude the production of prostanoid vasoconstrictors andthe increased oxidative degradation of NO [7, 8]. Deficiencyof NO increases vascular resistance and promotes atherogen-esis [9].
Nitric oxide (NO) is a very active but short lived, amolecule that is released into the circulation from endothe-lial cells. It is a potent vasodilator that regulates vascularresistance and tissue blood flow. In addition, NO inhibits
key processes of atherosclerosis, such as monocyte endo-thelial adhesion, platelet aggregation, and vascular smoothmuscle cell proliferation. Hence, endothelial dysfunction dueto reduced NO availability is an early step in the course ofatherosclerotic vascular disease [10]. NO is synthesized bystereospecific oxidation of the terminal guanidino nitrogen ofthe amino acid, L-arginine, by the action of a family of NOS.Since NOhas tremendous biological activity, its blood and/ortissue concentration must be kept within narrow limits inorder to prevent harmful effects on cell activity.The synthesisof NO can be blocked, however, by inhibition of the NOSactive site with guanidino-substituted analogs of L-arginine,such as asymmetrical dimethylarginine (ADMA) [10].
ADMA is a naturally occurring amino acid that has theinteresting property of competitively inhibiting the activityof nitric oxide synthase (NOS). ADMA is produced bymethylation of arginine residues in intracellular proteins viaprotein arginine N-methyltransferases (PRMT).

2 Biochemistry Research International
After hydrolyzation of proteins, results into release ofADMA.ADMA is excreted in the urine, and, not surprisingly,there is an increase in plasma ADMA in patients with end-stage renal disease [11]. Parenthetically, patients with renaldisease have an increased risk of cardiovascular morbidityand mortality, and in these patient’s plasma ADMA concen-trations carry prognostic information [12].
The primary route of ADMA clearance, however, is byenzymatic degradation. Dimethylamine dimethylaminohy-drolase (DDAH) converts ADMA to citrulline and dimethy-lamine. By regulating the plasma and tissue concentrations ofADMA, NOS activity is protected by DDAH [13].
Recently, it has been demonstrated that plasma levelsof ADMA are elevated in patients with diabetes mellitus[7]. These findings suggest that the elevated ADMA indiabetes could contribute to accelerated atherosclerosis inthis population. Further, as ADMA is mainly metabolizedby dimethylarginine dimethylaminohydrolase (DDAH), it isconceivable that the inhibition of ADMA via upregulation ofDDAH may be a novel therapeutic target for the preventionof CVD in patients with diabetes.
Under experimental conditions that lead to suboptimal L-arginine concentrations or to a relative deficiency of essentialcofactors for NO synthase, the activity of this enzyme is“uncoupled.” This means that the oxidation of L-arginine toNO is not complete [14–16]. Normally, five electrons are beingtransferred in two steps of a coupled reduction-oxidationreaction by the two domains of NO synthase frommolecularoxygen to L-arginine, resulting in the release of L-citrullineand NO.
ADMA is elevated to a level that can significantly inhibitNOS activity in individuals with hypercholesterolemia,hypertension, and hyperhomocysteinemia, tobacco expo-sure, and hyperglycemia [17–19] in each of these condi-tions; the elevation in ADMA level is a result of oxidativestress. Further oxidative stress impairs the ability of DDAHto metabolize ADMA [17, 20]. Hyperglycemia can elevateintracellular oxidative stress through multiple mechanisms[21, 22].
Under suboptimal conditions like those mentionedabove, the electron flow within the two domains of NOsynthase is disturbed, and molecular oxygen acts as anelectron acceptor. This makes NO synthases a superoxide(O2
−) radical-producing enzyme.The endothelium-derived relaxation factor, nitric oxide,
provides a unifyingmechanism for the action ofmany cardio-vascular disease risk factors. Nitric oxide cannot bemeasureddirectly, but the inhibitor of its formation and asymmetricdimethylarginine (ADMA) can be measured. The functionof ADMA in modulating nitric oxide production has asignificant impact on cardiovascular endothelial function.
2. Objectives
Asymmetric dimethylarginine (ADMA) is a nonselectivenitric oxide (NO) synthase inhibitor associated with car-diovascular and metabolic disorders. This study aimed toinvestigate ADMA with respect to diabetes and its clinicalrelevance as an independent predictor of CAD.
3. Materials and Methods
The present case control study includes two hundred andforty patients, selected randomly. After careful clinical exami-nation and confirmed diagnosis, they are further divided intothree groups. Group I, patients presenting CVD (𝑛 = 80);Group II, patients with type II diabetes mellitus (𝑛 = 80);Group III, patients with type II DM with CVD; and a controlgroup (𝑛 = 80).
All patients selectedunderwent medical examination bya physician. A careful medical history was taken to obtaininformation about other diseases (particularly hypertension,coronary heart disease, myocardial infarction, stroke, periph-eral vascular disease and endocrine disorders). Inclusioncriteria, and patients clinically diagnosed having angiograph-ically proven CVD with/without type II DM. Prevalence ofdiabetes was assessed either by fasting blood glucose level≥126.0mg/DL or HbA1C levels more than 6%. Exclusioncriteria—patients with a history of prior coronary arterybypass grafting and patients with kidney and acute liverdiseases were excluded.
Patients matched 80 subjects as control, and group IIwas randomly selected from patients attending diabetic OPD(Outpatient department). Controls have a negative historyof CVD, Type II DM and had a normal resting ECG(Electrocardiogram).
Patients in group I and III were recruited from inpatientand outpatients departments of the hospital.The diagnosis ofCVD was made on the basis of the clinical history (typicalangina, history of myocardial infarction) and 12—lead stan-dard ECG before subjecting them to coronary angiography.The presence of any stenosis >30% according to coronaryangiography by visual assessment of coronary artery wasincluded in the study.
The study was approved by the ethical committee of ourinstitute. Fully informed consent was obtained from patients.Blood samples were drawn into vacutainer tubes. SerumADMA was analyzed by using enzyme immunoassay for thequantitative determination of endogenous ADMA, [23] andserum nitric oxide was estimated by the method of Cortes[24].
ADMAwas analysed by enzyme linked immunoassay forthe quantitative determination of endogenous asymmetricdimethylarginine in serum, manufactured by DLD diagnos-tics GMBH, which is based on principal, the competitiveADMA-ELISA uses the microtiter plate format. ADMA isbound to the solid phase of the microtiter plate. ADMAin the samples is acetylated and competes with solid phasebound ADMA for a fixed number of rabbit anti-ADMAantiserum binding sites. When the system is in equilib-rium, free antigen and free antigen antiserum complexes areremoved by washing. The antibody bounded to the solidphase ADMA is detected by the anti-rabbit/peroxidase. Thesubstrate TMB/peroxidase reaction is monitored at 450 nm.The amount of antibody bound to the solid phase ADMAis inversely proportional to the ADMA concentration of thesample.
Statistical analysis was carried by student’s 𝑡-test and chi-square test. Results were expressed as mean ± SD. Probability

Biochemistry Research International 3
Table 1: Baseline characteristics of the study population.
Control Diseased 𝑃 valueAge (years) 47.29 ± 10.21 56.21 ± 6.73 <0.10Family history 13 24 —Smoker 4 22 —BMI 21 (>25) 31 (>25) —BP systolic (mm/Hg) 122.84 ± 3.45 132.53 ± 7.62 <0.01BP diastolic (mm/Hg) 80.14 ± 5.53 86.23 ± 6.54 <0.20F BSL (mg/dL) 95.60 ± 18.38 132.80 ± 32 <0.01HbA1C 6.0 ± 1.27 7.32 ± 2.46 <0.50Total cholesterol 159.86 ± 26.98 282.36 ± 28 <0.01HDL (mg/dL) 44.21 ± 8.35 28.67 ± 8.89 <0.01LDL (mg/dL) 102.02 ± 25.78 159.69 ± 29.65 <0.05VLDL (mg/dL) 32.98 ± 10.43 45.31 ± 14.30 <0.02TG (mg/dL) 172.67 ± 56.87 227.38 ± 68.79 <0.01
values of 0.05were considered statistically significant. Associ-ations between two categorical variables were tested bymeansof the 𝜒2 or Fisher exact tests. All baseline characteristics,presented in Table 1, were evaluated as potential confounders,using univariate Cox regression analysis. All tests were twotailed, and 𝑃 < 0.05 was considered statistically significant.Statistical analysis was performed with SPSS statistical soft-ware (V.13.0).
4. Results
Patients who had no diabetes mellitus and cardiovasculardisease were grouped as control; diabetes with CVD andnondiabetes with CVD are categorized as diseased group andothers are categorized as nondiseased group.
Baseline characteristics of the participants are presentedin Table 1.The overallmean age for control was 47.0 years, anddiseased groupwas 56.0 years; 74.7%weremen.DiabeteswithCVD had higher systolic blood pressure and hyperlipidemiathan normal healthy subjects. Table 2 shows that type IIdiabetes with CAD patients have significantly higher ADMAconcentration than normal healthy subjects and other studygroups𝑃 < 0.001. NO concentrationwas lower lowest 26.71±3.41 in DM with CAD patients than the other study groupsand normal healthy subjects.
In a multiple logistic regression analysis adjusting forhypertension, hypercholesterolemia, low HDL cholesteroland diabetes or fasting glucose, ADMA remained a strongand independent predictor for the presence of CAD. ElevatedNo level levels was a strong predictor and significantly (𝑡:9.86,P < 0.001) associatedwith occurrence of CAD. IncreasedADMA level was found to be another strong predictor andassociated significantly (𝑡: 8.02, 𝑃 < 0.001) with CAD.
The univariate logistic regression analysis for risk factorsversus CVD (as a dependent variable) was done to assessrelative risk of development of CVD with each risk factorin the entire study population that includes diseased andnondiseased subjects. Age, family history, obesity, and SBPand DBP are highly significant and associated with CADpathogenesis (Tables 2, 3, and 4).
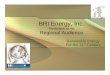
ADMA/NO10.90.80.7
ADMA/NO
ADMA 0.6
0.5
Linear
0.4
(ADMA/NO)
0.30.20.100 20 40 60
NO
R2= 0.6593
y = −0.0135x + 1.0454
Figure 1: Correlation between ADMA and NO in diseased group.
NO cut-off level was 30 𝜇mol/L. All study groups indicatepresence of disease. Our data supports NO which is also oneof the independent risk factors and significantly (𝜒2: 40.65,𝑃 < 0.001) associated with pathogenesis of CAD. The cut-off level for ADMA was 0.60𝜇mol/L (𝜒2: 36.46, 𝑃 < 0.001),which is another independent risk factor for CAD.
Diagnostic validity was done for assessing a good andbetter novel predictor for CAD. Sensitivity (presence ofthe disease if ≤30 𝜇mol/L) of NO was found to be 53.20%and specificity (absence of the disease if ≤30 𝜇mol/L) was95.40%. PPN (positive predictor value) of NO was 90.0%,and NPV (negative predictor value) was 68.10%. Overallaccuracy or diagnostic efficiency of NO was found to be76.0%. Sensitivity (presence of the disease if ≤30 𝜇mol/L) ofADMAwas found to be 74.40%and specificity (absence of thedisease if ≤30 𝜇mol/L) was 82.80%. PPN (positive predictorvalue) of ADMA was 91.10%, and NPV (negative predictorvalue) was 68.10%. Overall accuracy or diagnostic efficiencyof NOwas found to be 79.20%. Odds ratios for NOwere 19.10and 7.11 for ADMA (Table 5).
Figure 1 reports the relationship between ADMA andNOin diseased group, on intra group analysis there is significantnegative correlation (𝑟 = −0.743); 𝑃 (0.001) was foundbetween ADMA and NO. It suggests that increase in ADMAassociated with decrease is in NO activity or concentration.
5. Discussion
Associations between increased levels of ADMA and manycardiovascular risk factors such as age, hypertension, dia-betes, insulin resistance, hypercholesterolemia, hypertriglyc-eridemia, and hyperhomocysteinemia have been docu-mented [25–27]. Evidence for a causal relationship betweenincreased ADMA levels and endothelial vasodilator dysfunc-tion has been demonstrated in many of these conditions.Hyperglycaemia is associated with endothelial dysfunctionboth in vivo [28] and in vitro [29], therefore, endothelialdysfunction is an early feature in the development of vascular

4 Biochemistry Research International
Table 2: Risk factors.
Variables Control Group I Group II Group III 𝐹 𝑃 valueNO 𝜇mol/L 52.36 ± 6.09 32.01 ± 5.005 43 ± 8.62 26.71 ± 3.41 120.8 0.001ADMA 𝜇mol/L 0.36 ± 0.30 0.66 ± 0.76 0.49 ± 0.28 0.78 ± 0.83 7.633 0.001
Table 3: Parameters taking CAD as dependent variable.
Variable Diseasedgroup
Nondiseasedgroup 𝜒
2𝑃 value
NO<30.00 𝜇mol/L
52.6 ± 7.79
51%27.38 ± 4.06
6% 80.44 <0.0001
ADMA>0.60 𝜇mol/L
0.40 ± 0.65
72% 0.69 ± 0.85 135.1 <0.0001
complications in people with diabetes [30]. Patients withdiabetes have an adverse cardiovascular risk profile. ElevatedADMA concentration has been described in patients withtype 2 And type 1 diabetes [25]. Hyperglycemia probablymay increaseADMAconcentration.One invite study demon-strated that elevated glucose levels are capable of inhibitingDDAH activity in cultured endothelial cells [31]. Clinicalinvestigations in patients also indicate that ADMA is directlyrelated to blood glucose levels [25, 32]. As demonstrated ina recent study, strict glycemic control may exert antiathero-genic effects by reducing ADMA levels in patients with type 2diabetes [33]. Consistent with these studies, the present studyprovide evidence that elevated serum ADMA and reducedNO independently associated with cardiovascular risk in dia-betes patients with coronary artery disease. ADMAmight actas pathophysiologically relevant factor for diabetes associatedcomplications. Nevertheless, hyperglycemia remains a majorcause for both increased ADMA and the development ofdiabetic complications which makes the interpretation of thedata more complex.
ADMA was that atherosclerosis is marked by impairedvasodilation in response to normal physiological stimuli,and the impairment can be relieved by intravenous L-arginine [34]. A number of standard heart disease riskfactors (smoking, hypertension, hyperlipidemias) are relatedto vasodilatory impairment, but the strongest correlationmaybe the ADMA in plasma [35]. Elaboration of endothelium-derived nitric oxide affects the behaviour of circulating Tlymphocytes and monocytes. Mononuclear cell adhesivenessis inversely correlated with the plasma ADMA, and theeffect is reversed by restoration of the ratio-to-control levelswith oral administration of 14–21 grams of arginine [36].These changes lead to lower rates of atherosclerotic plaqueformation and lower risk of heart disease. In addition, theassociation of elevated LDL cholesterol with increased risk ofheart disease may be a covariable in the oxidative activationof ADMA synthesis. Oxidized LDL particles stimulate theexpression of enzymes that generate ADMA [37].
ADMAmay contribute to abnormal blood flow responsesand to atherogenesis in type 2 diabetics [38]. In hypertensives,the urinary excretion rate of nitrite plus nitrate (NOx), anindex of endogenous NO production, was lowered from77 to 56 micromol/mmol creatinine, while plasma levels of
ADMA were increased from 1.1 to 2.4, indicating ADMAinhibition of NO production [39]. ADMAplays an importantrole in the pathogenesis of hypertension associated with theexperimental focal and segmental glomerulosclerosis [40].
ADMA is released after posttranslational methylationfrom nuclear proteins involved in RNA processing andtranscriptional control.The enzyme protein arginine methyl-transferase type I (PRMT I) forms ADMA, whereas PRMTII forms symmetric dimethylarginine (SDMA) (i.e., thestereoisomer of ADMA with no known effect on NOS).Other data suggests that human endothelial cell PRMTactivity is upregulated by LDL cholesterol, due in part tothe enhanced gene expression of PRMTs [37]. Thus, we findADMA intermeshed with both cholesterol, and homocys-teine cardiovascular risk factors. Hyperglycemia is anotherfactor related to ADMA. Human endothelial cells exposed tohigh glucose concentrations show impairment of DDAH andaccumulation of ADMA that may contribute to endothelialvasodilator dysfunction in diabetes mellitus [31]. Improvedglycemic control in patients with type 2 diabetes results inlowering of plasma ADMA levels.
As ADMA directly impairs the physiological NO-dependent functions of the endothelial lining, its primarypathophysiological mechanism of action is different from allother known risk factors like hypertension (pressure overloadof the arterial wall and reduced arterial elasticity), hyperc-holesterolemia (uptake of (oxidized) LDL into the intimallayer, generation of foam cells, and local inflammation),smoking (induction and potentiation of oxidative damage ofcellular structures within the arterial wall). Accordingly, itcan be expected that the deleterious effects of ADMA areindependent of other risk factors and add to their effects.
In our study, ADMA level was found to be one of thestrong predictors for CAD. Another group of investigatorsfromThe Netherlands studied the survival of patients under-going intensive care unit treatment and aimed to identifynovel risk factors for survival during ICU treatment [41].Among all biochemical markers of organ function anddisease risk that were measured in this study, ADMA wasthe factor with the highest predictive power. Patients withelevated ADMA levels had a 17-fold increased risk of fatalityduring ICU treatment [41].
Understanding of the pathophysiological role of ADMAfor the development of cardiovascular diseases, this moleculehas become a novel goal for therapeutic intervention. ADMAplays an important role in the regulation of vascular toneby acting as an endogenous inhibitor of NO synthesis. Byinhibiting NO synthesis, plasma ADMAmay reduce vascularcompliance, increase vascular resistance, and limit bloodflow. Furthermore, plasma ADMA may promote atheroge-nesis as it opposes the vasoprotective effects of NO. Thus,elevations in plasma ADMA may accelerate the progression

Biochemistry Research International 5
Table 4: Univariate analysis of cofounding factors.
Variable Particular Diseased group Nondiseased group 95% CI 𝑃 valueNO <30.0 𝜇mol/L 54.34 6.2 38.18–42.67 <0.0001ADMA >0.60 𝜇mol/L 0.81 0.63 0.62–1.16 <0.0001
Table 5: Prognostic value of novel markers.
Variable Specificity Sensitivity Positive predictive value Negative predictive value Diagnostic accuracy Odd ratioNO 53.20% 95.40% 90.0% 68.10% 76.0% 19.10ADMA 74.40% 82.80% 91.10% 79.20% 84.00% 7.11
of atherosclerosis and increase the risk of cardiovascularevents.
In conclusion, ADMA is an emerging independent riskmarker for future CVD events. The clinical acceptance ofthis parameter will depend on the availability of a therapyto directly decrease ADMA, which could then confirm therole of ADMA as a causal risk factor. Further studies arewarranted in patients with diabetes, especially regarding thepossible effects of ADMA on diabetes associated complica-tions.
Abbreviations
ADMA: Asymmetric dimethylarginineCAD: Coronary artery diseaseCVD: Cardiovascular diseaseDM: Diabetes mellitusDDAH: Dimethylamine dimethylaminohydrolaseECG: ElectrocardiogramNO: Nitric oxideNOS: Nitric oxide synthaseOPD: Outpatient departmentPRMT: Protein arginine N-methyltransferases.
References
[1] R. Candido, P. Srivastava, M. E. Cooper, and L. M. Burrell,“Diabetes mellitus: a cardiovascular disease,” Current Opinionin Investigational Drugs, vol. 4, no. 9, pp. 1088–1094, 2003.
[2] Expert Committee on the Diagnosis and Classification ofDiabetes Mellitus, “Report of the expert committee on thediagnosis and classification of diabetes mellitus,”Diabetes Care,vol. 22, supplement 1, pp. S5–S19, 1999.
[3] A. D. Mooradian, “Cardiovascular disease in type 2 diabetesmellitus: current management guidelines,” Archives of InternalMedicine, vol. 163, no. 1, pp. 33–40, 2003.
[4] H.Miyazaki, H.Matsuoka, J. P. Cooke et al., “Endogenous nitricoxide synthase inhibitor: a novel marker of atherosclerosis,”Circulation, vol. 99, no. 9, pp. 1141–1146, 1999.
[5] V. Schachinger, M. B. Britten, and A. M. Zeiher, “Prognosticimpact of coronary vasodilator dysfunction on adverse long-term outcome of coronary heart disease,” Circulation, vol. 101,no. 16, pp. 1899–1906, 2000.
[6] J. A. Suwaidi, S. Hamasaki, S. T. Higano, R. A. Nishimura, D. R.Holmes Jr., and A. Lerman, “Long-term follow-up of patientswithmild coronary artery disease and endothelial dysfunction,”Circulation, vol. 101, no. 9, pp. 948–954, 2000.
[7] C. Nielson and T. Lange, “Blood glucose and heart failure innondiabetic patients,” Diabetes Care, vol. 28, no. 3, pp. 607–611,2005.
[8] B. Tesfamariam, M. L. Brown, and R. A. Cohen, “15-Hydro-xyeicosatetraenoic acid and diabetic endothelial dysfunction inrabbit aorta,” Journal of Cardiovascular Pharmacology, vol. 25,no. 5, pp. 748–755, 1995.
[9] J. P. Cooke and V. J. Dzau, “Nitric oxide synthase: role in thegenesis of vascular disease,” Annual Review of Medicine, vol. 48,pp. 489–509, 1997.
[10] J. P. Cooke, “DoesADMAcause endothelial dysfunction?”Arte-riosclerosis, Thrombosis, and Vascular Biology, vol. 20, no. 9, pp.2032–2037, 2000.
[11] J. T. Kielstein, R. H. Boger, S.M. Bode-Boger et al., “Asymmetricdimethylarginine plasma concentrations differ in patients withend-stage renal disease: relationship to treatment method andatherosclerotic disease,” Journal of the American Society ofNephrology, vol. 10, no. 3, pp. 594–600, 1999.
[12] C. Zoccali, S. M. Bode-Boger, F. Mallamaci et al., “Plasma con-centration of asymmetrical dimethylarginine and mortality inpatients with end-stage renal disease: a prospective study,”Lancet, vol. 358, no. 9299, pp. 2113–2117, 2001.
[13] H. Dayoub, V. Achan, S. Adimoolam et al., “Dimethylargininedimethylaminohydrolase regulates nitric oxide synthesis:genetic and physiological evidence,” Circulation, vol. 108, no.24, pp. 3042–3047, 2003.
[14] P. Klatt, K. Schmidt, G. Uray, and B. Mayer, “Multiple catalyticfunctions of brain nitric oxide synthase,” Journal of BiologicalChemistry, vol. 268, no. 20, pp. 14781–14787, 1993.
[15] J. Vasquez-Vivar, B. Kalyanaraman, P. Martasek et al., “Super-oxide generation by endothelial nitric oxide synthase: theinfluence of cofactors,” Proceedings of the National Academy ofSciences of the United States of America, vol. 95, no. 16, pp. 9220–9225, 1998.
[16] K. A. Pritchard Jr., L. Groszek, D.M. Smalley et al., “Native low-density lipoprotein increases endothelial cell nitric oxide syn-thase generation of superoxide anion,”Circulation Research, vol.77, no. 3, pp. 510–518, 1995.
[17] R. H. Boger, S. M. Bode-Boger, A. Szuba et al., “Asymmetric di-methylarginine (ADMA): a novel risk factor for endothelialdysfunction: its role in hypercholesterolemia,” Circulation, vol.98, no. 18, pp. 1842–1847, 1998.
[18] M. C. Stuhlinger, P. S. Tsao, J. H. Her, M. Kimoto, R. F. Balint,and J. P. Cooke, “Homocysteine impairs the nitric oxide syn-thase pathway role of asymmetric dimethylarginine,” Circula-tion, vol. 104, no. 21, pp. 2569–2575, 2001.
[19] A. Fard, C. H. Tuck, J. A. Donis et al., “Acute elevations ofplasma asymmetric dimethylarginine and impaired endothelial

6 Biochemistry Research International
function in response to a high-fat meal in patients with type2 diabetes,” Arteriosclerosis, Thrombosis, and Vascular Biology,vol. 20, no. 9, pp. 2039–2044, 2000.
[20] A. Ito, P. S. Tsao, S. Adimoolam, M. Kimoto, T. Ogawa, and J. P.Cooke, “Novel mechanism for endothelial dysfunction: dysreg-ulation of dimethylarginine dimethylaminohydrolase,” Circula-tion, vol. 99, no. 24, pp. 3092–3095, 1999.
[21] L. A. Powell, S. M. Nally, D. McMaster, M. A. Catherwood, andE. R. Trimble, “Restoration of glutathione levels in vascularsmooth muscle cells exposed to high glucose conditions,” FreeRadical Biology andMedicine, vol. 31, no. 10, pp. 1149–1155, 2001.
[22] W. C. Duckworth, “Hyperglycemia and cardiovascular disease,”Current Atherosclerosis Reports, vol. 3, no. 5, pp. 383–391, 2001.
[23] F. Schulze, R.Wesemann, E. Schwedhelm et al., “Determinationof asymmetric dimethylarginine (ADMA) using a novel ELISAassay,” Clinical Chemistry and Laboratory Medicine, vol. 42, no.12, pp. 1377–1383, 2004.
[24] N. K. Cortas andN.W.Wakid, “Determination of inorganic nit-rate in serum and urine by a kinetic cadmium-reductionmethod,” Clinical Chemistry, vol. 36, no. 8, pp. 1440–1443, 1990.
[25] F. Abbasi, T. Asagmi, J. P. Cooke et al., “Plasma concentrations ofasymmetric dimethylarginine are increased in patients withtype 2 diabetes mellitus,” American Journal of Cardiology, vol.88, no. 10, pp. 1201–1203, 2001.
[26] M. C. Stuhlinger, F. Abbasi, J. W. Chu et al., “Relationship bet-ween insulin resistance and an endogenous nitric oxide syn-thase inhibitor,” Journal of the American Medical Association,vol. 287, no. 11, pp. 1420–1426, 2002.
[27] M. C. Stuhlinger, R. K. Oka, E. E. Graf et al., “Endothelial dys-function induced by hyperhomocyst(e)inemia: role of asym-metric dimethylarginine,” Circulation, vol. 108, no. 8, pp. 933–938, 2003.
[28] H. Kawano, T. Motoyama, O. Hirashima et al., “Hyperglycemiarapidly suppresses flow-mediated endothelium-dependentvasodilation of brachial artery,” Journal of the American Collegeof Cardiology, vol. 34, no. 1, pp. 146–154, 1999.
[29] F. Cosentino, K. Hishikawa, Z. S. Katusic, and T. F. Luscher,“High glucose increases nitric oxide synthase expression andsuperoxide anion generation in human aortic endothelial cells,”Circulation, vol. 96, no. 1, pp. 25–28, 1997.
[30] N. N. Chan, P. Vallance, and H.M. Colhoun, “Endothelium-de-pendent and -independent vascular dysfunction in type 1diabetes: role of conventional risk factors, sex, and glycemiccontrol,” Arteriosclerosis, Thrombosis, and Vascular Biology, vol.23, no. 6, pp. 1048–1054, 2003.
[31] K. Y. Lin, A. Ito, T. Asagami et al., “Impaired nitric oxide syn-thase pathway in diabetesmellitus: role of asymmetric dimethy-larginine and dimethylarginine dimethylaminohydrolase,” Cir-culation, vol. 106, no. 8, pp. 987–992, 2002.
[32] M. I. Worthley, A. S. Holmes, S. R. Willoughby et al., “The dele-terious effects of hyperglycemia on platelet function in diabeticpatients with acute coronary syndromes mediation by super-oxide production, resolution with intensive insulin administra-tion,” Journal of the American College of Cardiology, vol. 49, no.3, pp. 304–310, 2007.
[33] S. Yasuda, S. Miyazaki, M. Kanda et al., “Intensive treatment ofrisk factors in patients with type-2 diabetes mellitus is associ-ated with improvement of endothelial function coupled with areduction in the levels of plasma asymmetric dimethylarginineand endogenous inhibitor of nitric oxide synthase,” EuropeanHeart Journal, vol. 27, no. 10, pp. 1159–1165, 2006.
[34] M. A. Creager, S. J. Gallagher, X. J. Girerd, S. M. Coleman, V. J.Dzau, and J. P. Cooke, “L-Arginine improves endothelium-dependent vasodilation in hypercholesterolemic humans,” Jour-nal of Clinical Investigation, vol. 90, no. 4, pp. 1248–1253, 1992.
[35] R. H. Boger and S. M. Bode-Boger, “Asymmetric dimethylargi-nine, derangements of the endothelial nitric oxide synthasepathway, and cardiovascular diseases,” Seminars in Thrombosisand Hemostasis, vol. 26, no. 5, pp. 539–545, 2000.
[36] J. R. Chan, R. H. Boger, S. M. Bode-Boger et al., “Asymmetricdimethylarginine increases mononuclear cell adhesiveness inhypercholesterolemic humans,” Arteriosclerosis, Thrombosis,and Vascular Biology, vol. 20, no. 4, pp. 1040–1046, 2000.
[37] R. H. Boger, K. Sydow, J. Borlak et al., “LDL cholesterol upregu-lates synthesis of asymmetrical dimethylarginine in humanendothelial cells: involvement of S-adenosylmethionine-dependent methyltransferases,” Circulation Research, vol. 87,no. 2, pp. 99–105, 2000.
[38] A. Fard, C. H. Tuck, J. A. Donis et al., “Acute elevations of plas-ma asymmetric dimethylarginine and impaired endothelialfunction in response to a high-fat meal in patients with type2 diabetes,” Arteriosclerosis, Thrombosis, and Vascular Biology,vol. 20, no. 9, pp. 2039–2044, 2000.
[39] A. Surdacki, M. Nowicki, J. Sandmann et al., “Reduced urinaryexcretion of nitric oxide metabolites and increased plasmalevels of asymmetric dimethylarginine in men with essentialhypertension,” Journal of Cardiovascular Pharmacology, vol. 33,no. 4, pp. 652–658, 1999.
[40] J. Sato,H.Masuda, S. Tamaoki et al., “Endogenous asymmetricaldimethylarginine and hypertension associated with puromycinnephrosis in the rat,” British Journal of Pharmacology, vol. 125,no. 3, pp. 469–476, 1998.
[41] R. J. Nijveldt, T. Teerlink, M. P. C. Siroen, A. A. Van Lambalgen,J. A. Rauwerda, and P. A. M. Van Leeuwen, “The liver is an im-portant organ in themetabolism of asymmetrical dimethylargi-nine (ADMA),”Clinical Nutrition, vol. 22, no. 1, pp. 17–22, 2003.

Submit your manuscripts athttp://www.hindawi.com
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Anatomy Research International
PeptidesInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporation http://www.hindawi.com
International Journal of
Volume 2014
Zoology
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Molecular Biology International
GenomicsInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Signal TransductionJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Evolutionary BiologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Biochemistry Research International
ArchaeaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Genetics Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Advances in
Virolog y
Hindawi Publishing Corporationhttp://www.hindawi.com
Nucleic AcidsJournal of
Volume 2014
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Enzyme Research
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
International Journal of
Microbiology