Embed Size (px)
Citation preview

Roberson et al. BMC Public Health 2014, 14:14http://www.biomedcentral.com/1471-2458/14/14
RESEARCH ARTICLE Open Access
Beyond BMI: The “Metabolically healthy obese”phenotype & its association with clinical/subclinical cardiovascular disease and all-causemortality – a systematic reviewLara L Roberson1, Ehimen C Aneni1, Wasim Maziak3, Arthur Agatston1, Theodore Feldman1, Maribeth Rouseff2,Thinh Tran2, Michael J Blaha4, Raul D Santos5, Andrei Sposito6, Mouaz H Al-Mallah7, Ron Blankstein8,Matthew J Budoff9 and Khurram Nasir1,3,4,10*
Abstract
Background: A subgroup has emerged within the obese that do not display the typical metabolic disordersassociated with obesity and are hypothesized to have lower risk of complications. The purpose of this review wasto analyze the literature which has examined the burden of cardiovascular disease (CVD) and all-cause mortality inthe metabolically healthy obese (MHO) population.
Methods: Pubmed, Cochrane Library, and Web of Science were searched from their inception until December2012. Studies were included which clearly defined the MHO group (using either insulin sensitivity and/orcomponents of metabolic syndrome AND obesity) and its association with either all cause mortality, CVD mortality,incident CVD, and/or subclinical CVD.
Results: A total of 20 studies were identified; 15 cohort and 5 cross-sectional. Eight studies used the NCEP AdultTreatment Panel III definition of metabolic syndrome to define “metabolically healthy”, while another nine usedinsulin resistance. Seven studies assessed all-cause mortality, seven assessed CVD mortality, and nine assessed incidentCVD. MHO was found to be significantly associated with all-cause mortality in two studies (30%), CVD mortality in onestudy (14%), and incident CVD in three studies (33%). Of the six studies which examined subclinical disease, four (67%)showed significantly higher mean common carotid artery intima media thickness (CCA-IMT), coronary artery calcium(CAC), or other subclinical CVD markers in the MHO as compared to their MHNW counterparts.
Conclusions: MHO is an important, emerging phenotype with a CVD risk between healthy, normal weight andunhealthy, obese individuals. Successful work towards a universally accepted definition of MHO would improve(and simplify) future studies and aid inter-study comparisons. Usefulness of a definition inclusive of insulin sensitivityand stricter criteria for metabolic syndrome components as well as the potential addition of markers of fatty liver andinflammation should be explored. Clinicians should be hesitant to reassure patients that the metabolically benignphenotype is safe, as increased risk cardiovascular disease and death have been shown.
* Correspondence: [email protected] for Prevention and Wellness Research, Baptist Health Medical Group,Michigan Ave Suite 500, Miami Beach, Florida3Department of Epidemiology, Robert Stempel College of Public Health,Florida International University, Miami, FloridaFull list of author information is available at the end of the article
© 2014 Roberson et al.; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.

Roberson et al. BMC Public Health 2014, 14:14 Page 2 of 12http://www.biomedcentral.com/1471-2458/14/14
BackgroundIt is well established that obesity continues to rise inprevalence, nearly doubling between the years of 1980 and2008 worldwide [1]. In the United States between 2009–2010, the rate of obesity was 35.7% in adults and 17% inchildren [2], which translates into about 78 million adultsand 12.5 million children. In literature review, obesity hasbeen shown to be predictive of all-cause, cardiovasculardisease (CVD), and cancer mortality [3,4]. Economically,obesity is costly due to its direct association with morbid-ity and mortality, with the medical costs of treating obesityand its sequelae estimated to be $147 billion in 2009 [5].From a clinical perspective, the question remains how tobest identify those who are at the lowest risk of developingthese obesity-related complications, and monitor them ina cost effective way, while allocating the most resources tothose in the highest risk group.A subgroup has been identified within the obese popula-
tion, who do not display the typical metabolic disordersassociated with obesity and are hypothesized to have lowerrisk of obesity-related complications. Metabolically healthyobesity (MHO), as it will be referred to in this review, hasbeen previously defined as a subgroup of obese individualswho do not have insulin resistance, lipid disorders, orhypertension [6]. Multiple studies indicate 10-25% of theobese can be categorized as MHO [6,7]. Wildman et al.used NHANES, a nationally representative sample ofadults living in the US, to examine the MHO phenotypeand found a prevalence of 32% among obese adults overthe age of 20 [8].In this review, we aim to evaluate the MHO phenotype
in context of cardiovascular disease risk and all-causemortality. By conducting a systematic literature searchwhich selected studies assessing the association of theMHO phenotype with all-cause mortality, CVD outcomesand subclinical CVD, we sought to summarize the risks inthis group, and discuss the challenges faced by studies inexamining this unique population.
MethodsA systematic literature search was conducted usingPubmed, Web of Science, and Cochrane Library. InPubmed, the following medical subject headings (MESH)and free text terms were used: (“metabolically healthy” OR“metabolically normal” OR “metabolically benign” OR “in-sulin sensitive”) AND (“obese” OR “overweight”). Thesame text word search was used in Web of Science andCochrane Library as in Pubmed. No restrictions were usedfor publication status or date, but studies had to be peer-reviewed to be selected. Libraries were searched untilDecember 2012. Studies were selected if they were writtenin English, included human subjects over the age of 18, de-fined a metabolically healthy obese/overweight group andcontained either a measure of subclinical cardiovascular
disease or a hard outcome such as death or cardiovasculardisease. Studies were excluded if they failed to include acomparison group to the MHO, the abstract and full textwas unavailable, or were reviews, letters, and case-reports.Studies were also excluded if they failed to define metabol-ically healthy using either insulin sensitivity or componentsof metabolic syndrome or failed to define obesity usingBMI, body fat percentage, or waist circumference. Two re-viewers independently selected articles, and then jointlyagreed on the final studies to be included.
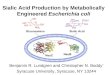
ResultsEligible studiesOur search identified a total of 340 studies fromPubmed, 156 from Web of Science, and 20 fromCochrane library. Six more studies were identified bysearching the reference lists of all full-text papers in-cluded from the initial database search. Twenty articlesmet the final inclusion criteria (Figure 1).
Cohort studiesA total of 14 cohort studies were identified which exam-ined the MHO phenotype and mortality or cardiovascularoutcomes [9-22] (Tables 1 and 2). These studies reportedan average follow-up time of 11 years. In total, the 14studies examined 359,137 participants, 9,865 fitting theMHO phenotype, or 2.7% of the total population studied.One study examined the MHO phenotype and progres-sion of subclinical cardiovascular disease at three-yearfollow-up [23]. The majority of studies examined risksin Caucasian subjects or subjects of European descent(n = 12). One study used an Iranian cohort [12] and onestudy did not report ethnicity [13]. On average, participantswere over the age of 50 (n = 9), while a small segment ofstudies reported younger average age (n = 4), or did notreport age [13]. One cohort study examined the MHOphenotype and subclinical CVD [23] (Tables 3 and 4).
i. Definitions of MHOStudies were examined in reference to their definition ofMHO (Table 1). In 13 of the studies, obesity was definedas BMI ≥ 30 kg/m2. The remaining study defined obesityas either BMI ≥ 30 kg/m2 or body fat > 25% in men and30% in women [16]. Three studies included measures ofinflammation (either C-Reactive protein [CRP] or whiteblood cell [WBC] count) in the definition of MHO[11,15,17]. Two studies defined “metabolically healthy” asabsence of metabolic syndrome (MetS) based on theNCEP ATP III definition of MetS without any modifica-tion [18,19]. Five studies defined “metabolically healthy” asabsence of MetS with study specific modifications to theMetS criteria [11,12,16,20,21]. One study used only insulinsensitivity (IS) to define “metabolically healthy” [10]. Twostudies created a unique definition using a combination of

Records identified through database searching
(n = 516)
Additional records identified through other sources
(n = 6 )
Records after duplicates removed (n = 469)
Records screened (n = 469)
Records excluded (n = 358)
Full-text articles assessed for eligibility
(n = 111 )
Studies excluded (N=91)No hard outcome or subclinical CVD marker (56)No comparison group to MHO (18)Case reports, not written in English, review articles, letters (17)
Studies included (n = 20)
Figure 1 Search flow chart.
Roberson et al. BMC Public Health 2014, 14:14 Page 3 of 12http://www.biomedcentral.com/1471-2458/14/14
insulin sensitivity (IS) and MetS [17,23]. Lastly, four stud-ies examined both the IS and MetS definitions of “meta-bolically healthy” within the same study [9,13-15].
ii. Outcomes measured
a. All-cause mortality. Seven studies reported all-causemortality [9-11,13,16,19,23]. MHO was found to besignificantly associated with all-cause mortality intwo studies (30% of studies). Five studies used meta-bolically healthy, normal weight (MHNW) as thecomparison group [9,13,16,19,23] of which the twosignificant studies were included. Two used metabol-ically normal, “not obese, BMI <30 kg/m2” [10,11] asthe comparison and both reported null results.Finally, four studies controlled for physical fitness(either reported exercise or measured cardio-respiratory fitness) of which all reported nullresults [11,16,19,24].
b. CVD mortality. Seven studies separately analyzedCVD mortality [9-11,16,19,20,23]. Five studiesshowed no statistically significant associationbetween MHO and CVD mortality, but pointedtowards higher CVD mortality in the MHO[9,11,16,19,20]. Only one study (14% of reviewed
studies) found the metabolically healthy obese tohave significantly higher risk of CVD mortality [23].The studies using “metabolically normal, not obese”rather than “normal weight” as their comparisongroup found no association between MHO andCVD mortality [10,11].
c. Incident CVD. Nine studies examined incident CVDevents [9,12,14-19,21,23]. Incident CVD was definedas stroke, coronary heart disease (CHD), and/orheart failure. Three studies (33%) reportedsignificant increase in risk of CVD events among theMHO [9,15,23]. Five studies showed no statisticallysignificant association between incident CVD andMHO, but consistently pointed towards anincidence of CVD in the MHO approximately 1.5times that of the comparison group [11,12,14,17,21].The single study which was non-significant and didnot point towards an increase in risk had a follow upof 6 years, small sample size of 550, and measuredonly incident heart failure [18].
d. Subclinical measures of CVD. Bobbioni-Harsch et al.examined the three year progression of commoncarotid intima medial thickness (CCA-IMT), ameasure of arterial wall thickness and indicator ofatherosclerotic disease progression, in a cohort of

Table 1 MHO definition; cohort studies
Study Definition of metabolically healthy obese (MHO) Definition of metabolically healthy, normal weight(MHNW)
Katzmarzyk [19] • <3 MetS • ≤ 2 MetS criteria, normal weight (BMI 18.5-24.9 kg/m2)
• BMI ≥30 kg/m2
• Diabetics included
St-Pierre [17] • ≤2 insulin resistance syndromeA (IRS) criteria • ≤2 IRSA criteria, normal weight (BMI <25 kg/m2)
• BMI≥ 30 kg/m2
• Diabetics excluded
Meigs [14] • < 3 MetS criteria and/or IS by HOMA-IR < 75th percentile • <3 MetS criteria, normal weight (BMI < 25 kg/m2)and/or IS, normal weight (BMI < 25 kg/m2)
• BMI≥ 30 kg/m2
• Diabetics excluded
Daly [20] • <3 MetSB • <3 MetSB , normal weight (BMI <25 kg/m2)
• BMI > 30 kg/m2
• Diabetics included
Song [21] • < 3 MetSC criteria • <3 MetSC , normal weight (BMI <25 kg/m2)
• BMI ≥30 kg/m2
• Diabetics included
Kuk [13] • ≤1 MetS criteria and/or IS by HOMA < 2.5 • ≤1 MetS criteria, normal weight (BMI < 25 kg/m2)and/or IS, normal weight (BMI < 25 kg/m2)
• BMI≥ 30 kg/m2
• Diabetics included
Arnlov [9] • <3 MetSD criteria and/or IS by HOMA-IR <75th percentile • <3 MetSD criteria, normal weight (BMI < 25 kg/m2)and/or IS, normal weight (BMI < 25 kg/m2)
• BMI > 30 kg/m2
• Diabetics excluded
Calori [10] •IS by HOMA-IR < 2.5 • IS, not obese (BMI < 30 kg/m2)
• BMI≥ 30 kg/m2
• Diabetics included
Voulgari [18] • < 3 MetS criteria • <3 MetS criteria, normal weight (BMI <24.9 kg/m2)
• BMI≥ 30 kg/m2
• Diabetics excluded
Hosseinpanah [12] • <3 MetSE criteria • <3 MetSE criteria, normal weight (BMI 18.5-24.9 kg/m2)
• BMI ≥30 kg/m2
• Diabetics included
Bobbioni-Harsch [23] • 0 MetS criteria • 0 MetS criteria, normal weight (BMI < 25 kg/m2)
• BMI ≥25 kg/m2
Ogorodnikova [15] •≤ 2 MetSC criteria; ≤1 of any MetSC criteria, IR by HOMA-IR >75th percentile of all participants, or systemic inflammationby WBC >75th percentile for all participants; or IS byHOMA-IR ≤25th percentile among non-diabetic obese,sex-specific
•≤ 2 MetSC criteria, normal weight (BMI 18.5-24.9 kg/m2)or≤ 1 MetSC criteria, IR by HOMA-IR > 75th percentile ofall participants, or systemic inflammation by WBC >75thpercentile for all participants, normal weight(BMI 18.5-24.9 kg/m2) or IS, normal weight(BMI 18.5-24.9 kg/m2)
• BMI≥ 30 kg/m2
• Diabetics included
Hamer [11] • <2 MetSF criteria (including CRP ≥3.0 mg/L) • <2 MetSF criteria, not obese (BMI 18–29.9 kg/m2) or <2 MetSF
criteria, normal waist (≤102 cm in men, ≤88 cm in women)• BMI ≥30 kg/m2 or waist circumference >102cm men, >88 cm women
• Diabetics included
Roberson et al. BMC Public Health 2014, 14:14 Page 4 of 12http://www.biomedcentral.com/1471-2458/14/14

Table 1 MHO definition; cohort studies (Continued)
Bo [22] • < IS by HOMA < 2.5 AND <3 MetSG criteria • IS, normal weight (BMI <25 kg/m2)
• BMI > 30 kg/m2
• Diabetics included
Ortega [16] • ≤1 MetSC criteria • ≤1 MetSC criteria, normal weight (BMI 18.5-24.9 kg/m2)or • ≤1 MetSC criteria, normal body fat(<25% men/<30% women)• Body Fat%≥ 25/30 (M/F) ORBMI≥ 30 kg/m2
• Diabetics includedATG ≥150 mg/dL, HDL <50 mg/dL, ≥54.5% of LDL particles with diameter <255A, Apo lipoprotein B level ≥1.36 g/L, fasting insulin level ≥ 85.2 pmol/L, blood pressure ≥135/85 mmHg, CRP ≥3.0 mg/L; BTG and waist circumference excluded, added BMI > 30 kg/m2 into criteria;CWaist circumference excluded; DWaist circumferenceexcluded, added BMI ≥ 29.4 kg/m2 cut-point into criteria; EWaist circumference ≥89 cm for men and ≥91 cm for women, blood pressure ≥ 140/85 mmHg; FTG excluded,added CRP ≥ 3 mg/L into criteria; GWaist circumference ≥94 cm for men and ≥80 cm for women, fasting plasma glucose ≥ 100 mg/dl or use of hypoglycemic therapy.
Roberson et al. BMC Public Health 2014, 14:14 Page 5 of 12http://www.biomedcentral.com/1471-2458/14/14
376 metabolically healthy adults aged 30 to 60 years[23] (Tables 1 and 2). At baseline and three years,cardio-metabolic risk factors were measured. Partici-pants were grouped by weight class and according totheir metabolic status at follow up. They were con-sidered at-risk if they had developed one or morecardio-metabolic risk factors. At baseline, there wasno significant difference in mean CCA-IMT betweenweight classes. Among the metabolically normal atfollow-up, mean CCA-IMT was significantly higherin obese women as compared to normal body weightwomen. In regression, BMI was significantly associ-ated with the occurrence of ≥1 cardio-metabolic riskfactors in all subgroups at follow-up. The incidenceof one or more cardio-metabolic risk factors was57.2% in overweight and obese participants whowere metabolically normal at baseline, comparedwith 31.7% of normal weight participants. Also, theyfound independent of metabolic abnormalities, theCCA-IMT was thicker in the obese and overweight,than in the normal weight.
iii.Other considerations
a. Inflammation. A total of 5 of the 14 included studiesreported any measure of inflammation. Four studiesdocumented C-reactive protein (CRP) levels[11,17,21,22]. One study used white blood cell count >75th percentile as a marker of inflammation [15].Hamer, Ogorodokniva and St Pierre included vascularinflammation in the definition of metabolic health[11,15,17]. Only one study adjusted for the presence ofvascular inflammation in predicting CVD [21]. None ofthese studies reported the association of vascular in-flammation with CVD outcomes.
b. Risk-reducing behaviors. Eight of 14 studies includedmeasures of exercise or fitness[11-13,16,18,19,21,23]. One study measured cardio-respiratory fitness by treadmill test and found thatincreased physical activity offset the increased CVDmortality seen in the MHO [19]. Seven studies uti-lized self-reported measures of physical activity and
found that the MHO had higher physical activitylevels as compared to the MUHO. However, thesestudies did not assess the effect of physical activityalone on CVD outcomes in the metabolically healthyobese. Only three studies documented dietary behav-iors in the study populations [13,21,23]. All threeutilized self reported methods. Out of these, onestudy found that in subjects with BMI < 30, insulinsensitive individuals had significantly higher meandaily fiber consumption as compared to insulin re-sistant subjects. No significant difference was foundin fiber consumption between insulin sensitive orresistant subjects with BMI > 30 [23].
Cross sectional studiesA total of five cross sectional studies met inclusion cri-teria, [25-29] (Tables 3 and 4). In total 5,234 participantswere examined for prevalence of subclinical CVD in re-lation to the MHO phenotype.
i. Definitions of MHOAll studies included diabetics. Two studies definedobese/overweight as BMI ≥ 25 kg/m2 [27,28]. Theremaining studies used BMI > or ≥ 30 kg/m2. Two stud-ies defined MHO using IS [25,26]. Of the remainingthree studies, one used the standard NCEP ATP III def-inition of MetS [29], and the other two used a modifiedversion of the MetS definition [27,28]. One study in-cluded CRP < 3 mg/L in the definition of “metabolicallyhealthy” [27].
ii Outcomes measured
a. Common carotid artery-intima medial thickness. Allfive of the studies measured CCA-IMT as a markerof atherosclerosis. Of the four studies reportingmean difference in CCA-IMT between MHO andMHNW individuals [25-28], two reported signifi-cantly higher levels in the MHO [25,27]. However,in the two studies that did not attain statisticalsignificance, the mean CCA-IMT tended to behigher in the MHO group as compared to the

Table 2 Results; cohort studies
Study Subjects(age , male)
Median follow-uptime (yrs)
Outcome Results
Katzmarzyk [19] N = 19,173 10 All-cause mortalityCVD mortality
MHO = All cause: 25 (3%); CVD: 12 (1%);MHNW = All-cause: 160 (2%); CVD: 38 (1%);
MHO = 1,019 (43, 100%) •Unadjusted HR for MHO vs.MHNW= NR (All-cause); NR (CVD)
MHNW= 7,153 (41, 100%) •AdjustedA HR for MHO vs.MHNW= 0.88 (0.57-1.36) [All-cause];1.59 (0.81-3.12) [CVD]
St-Pierre [17] N = 1,824 13 Incident CVD Total = 284 (16%); MHO = NR; MHNW = NR
MHO = 54 (NR, 100%) •Unadjusted HR for MHO vs. MHNW= NR
MHNW= 512 (NR, 100%) •AdjustedB HR for MHO vs. MHNW= 1.53 (0.79-3.00)
Meigs [14] N = 2,902 11 Incident CVD MHO = CVD: 19 (8%); MHNW = CVD: 19 (5%);
MHO = 236 (52, 51%) •Unadjusted RR for MHO vs. MHNW= NR
MHNW= 981 (52, 27%) • AdjustedC RR for MHO (MetS)vs. MHNW= 1.48 (0.87-2.55)[CVD]
•AdjustedC RR for MHO (IS) vs.MHNW= 1.42 (0.87-2.33) [CVD]
Daly [20] N = 8,397 (60, 87%) 4 CVD mortality MHO = NR (3%); MHNW = NR (2%)
MHO = 839 (NR,NR) •Unadjusted RR for MHO vs. MHNW= 1.42 (0.76-2.63)
MHNW= NR •Adjusted RR for MHO vs. MHNW= NR
Song [21] N = 25,626 10 Incident CVD MHO = CVD: 77 (3%); MHNW = CVD: 278 (2%)
MHO = 2,925 (54, 0%) •Unadjusted RR for MHO vs. MHNW= NR
MHNW= 12,943 (54, 0%) •AdjustedD RR for MHO vs. MHNW= 1.05 (0.66-1.66)
•AdjustedE RR for MHO vs. MHNW= 1.07 (0.68-1.70)
Kuk [13] N = 6,011 9 All-cause mortality Total = 292 (5%); MHO = NR; MHNW = NR
MHO = 78 (NR, NR) •Unadjusted RR for MHO (MetS) vs. MHNW= NR
MHNW= 1,461 (NR, NR) •AdjustedF RR for MHO (MetS) vs. MHNW= 2.80 (1.18-6.65)
•Unadjusted RR for MHO (IS) vs. MHNW= NR
•AdjustedF RR for MHO (IS) vs. MHNW= 2.58 (1.00-6.65)
Arnlov [9] N = 1,758 30 All-cause mortality MHO = All-cause: 18 (60%); CVD mortality: 5 (17%)MHNW = All-cause: 391 (44%); CVD mortality: 155 (17%)
MHO = 30 (50, 100%) CVD mortality •Unadjusted RR for MHO (MetS) vs. MHNW= NR
MHNW= 891 (50, 100%) Incident CVD • AdjustedG RR for MHO (MetS) vs. MHNW= 1.65(1.03-2.66) [All-cause]; 1.20 (0.49-2.93) [CVD mortality];1.95 (1.14-3.34) [Incident CVD]
• AdjustedG RR for MHO (IS) vs. MHNW= 2.04 (1.25-3.32)[All-cause]; 1.80 (0.79-4.08) [CVD mortality]; 1.91 (1.07-3.41)[Incident CVD]
Calori [10] N = 2,011 15 All-cause mortality MHO = All-cause: 7 (16%); CVD: 2 (5%) MHNW = All-cause:141 (20%); CVD: 58 (8%)
MHO = 43 (55, 28%) CVD mortality •Unadjusted HR for MHO vs. MHNW= NR
MHNW= 708 (55, 45%) •AdjustedH HR for MHO vs. MHNW= 0.99(0.46-2.11) [All-cause]; 0.73 (0.18-3.00) [CVD]
Voulgari [18] N = 550 (60, NR) Incident heartfailure
MHO = 43 (9%); MHNW = 17 (16%)
MHO = 96 (NR, NR) 6 •Unadjusted HR for MHO vs. MHNW= 0.26 (NR)
MHNW= 109 (NR, NR) •AdjustedI HR for MHO vs. MHNW= 0.41 (0.10-1.31)
Roberson et al. BMC Public Health 2014, 14:14 Page 6 of 12http://www.biomedcentral.com/1471-2458/14/14

Table 2 Results; cohort studies (Continued)
Hosseinpanah [12] N = 6,215 8 Incident CVD MHO = 13 (3%); MHNW = 64 (4%)
MHO = 408 (45, 20%) •Unadjusted HR for MHO vs. MHNW= NR
MHNW= 1,555 (45, 57%) •AdjustedJ HR for MHO vs. MHNW= 1.07 (0.59-1.96)
BobbioniHarsch [23]
N = 436 3 CCA-IMT Male Subjects Mean CCA-IMT at Baseline:MHO = 0.63 (0.07) vs. MHNW= 0.59 (0.08) p = NS
MHO = 65 (45, 42%) Mean CCA-IMT at 3 years: MHO = 0.62 (0.10)vs. MHNW= 0.60 (0.07) p = NS
MHNW= 194 (43, 23%) Female Subjects Mean CCA-IMT at Baseline:MHO = 0.57 (0.06) vs. MHNW= 0.56 (0.06) p = NS
Mean CCA-IMT at 3 years: MHO = 0.61 (0.08) vs.MHNW= 0.58 (0.06) p < 0.05
Ogorodnikova [15] N = 17,544 12 Incident CVD Total = 2,439 (14%); MHO = NR; MHNW = NR
MHO = 1,167 (56, 32%) •Unadjusted HR for MHO vs. MHNW= NR
MHNW= 4,036 (58, 33%) •AdjustedK HR for MHO (using various definitions)vs. MHNW= 1.30 (1.03-1.66) [ATP III definition];1.17 (0.87-1.57) [ATP-III Expanded];1.52 (1.19-1.95) [IS definition]
Hamer [11] N = 22,203 7 All-cause mortality MHO = All-cause: 38 (3%); CVD: 18 (2%);
MHO = 1,160 (51.3, 53%) CVD mortality MHNW = All-cause: 777 (6%); CVD: 225 (2%)
MHNW= 12,716 (51.9, 45%) •Unadjusted HR for MHO vs. MHNW= NR
•AdjustedL HR for MHO v. MHNW= 0.91(0.64-1.29) [All-cause]; 1.26 (0.74-2.13) [CVD]
Bo [22] N = 1,658 9 All-cause mortality MHO = All-cause: 15 (21%); CVD mortality:8 (11%); Incident CVD: NR (8%)
MHO = 72 (55, 33%) CVD mortality MHNW = All-cause: 28 (5%); CVD mortality:7 (1%);Incident CVD: NR (3%)
MHNW= 540 (54, 38%) Incident CVD •Unadjusted HR for MHO vs. MHNW= NR
•AdjustedM HR for MHO vs. MHNW= 1.36(0.64-2.08) [All-cause]; 2.48(1.35-3.61) [CVD mortality];2.76 (1.05-7.28) [Incident CVD]
Ortega [16] N = 43,265 14 All-cause mortality MHO = All-cause: 52 (3%); CVD mortality:17 (1%); Incident CVD: 30 (6%)
MHO = 1,738 (NR, 80%) CVD mortality MHNW = All-cause: 449 (3%); CVD mortality:98 (1%); Incident CVD: 261 (4%)
MHNW= 16,002 (NR,NR) Incident CVD •Unadjusted HR for MHO(referent) vs. MHNW= NR
•AdjustedN HR for MHO(referent) vs. MHNW= 0.91(0.67-1.24) [All-cause]; 0.73 (0.42-1.28) [ CVD mortality];0.78 (0.52-1.18) [Incident CVD]
AAdjusted for age, year of exam, smoking, alcohol use, possible existence of CVD, parental history or premature CVD, cardio-respiratory fitness; BAdjusted for age,smoking, and medication use at baseline; CAdjusted for age, sex, LDL, smoking; DAdjusted for age, treatment assignment, smoking, exercise, alcohol use, totalcalorie intake, postmenopausal hormone use, multivitamin use, parental history of myocardial infarction before 60 years, BMI; EAdjusted for age, treatment assignment,smoking, exercise, alcohol use, total calorie intake, postmenopausal hormone use, multivitamin use, parental history of myocardial infarction before 60 years, CRP;FAdjusted for age, sex, income, smoking, ethnicity, alcohol use; GAdjusted for age, smoking, and LDL; HAdjusted for age, sex; IAdjusted for age, sex, impaired glucosetolerance, dyslipidemia, hypertension, smoking, physical inactivity, left ventricular hypertrophy, and function on echocardiography; JAdjusted for age, gender, exercise,smoking, family history of premature CAD, high total cholesterol; KAdjusted for age, gender, race, smoking, education, alcohol use, and study cohort; LAdjusted for age,sex, smoking physical activity, socioeconomic group, and BMI; MAdjusted for age, sex, fiber intake, exercise, waist circumference; NAdjusted for age, sex, examination year,smoking, alcohol, parental history of CVD, fitness.
Roberson et al. BMC Public Health 2014, 14:14 Page 7 of 12http://www.biomedcentral.com/1471-2458/14/14
MHNW group [26,28]. The final study determinedthat carotid atherosclerosis was similar among nor-mal weight, overweight, and obese participants whenstratified by presence or absence of MetS,
b. Other subclinical measures of CVD. One studyassessed coronary artery calcium (CAC), which is anearly indicator of atherosclerotic disease measuring
the degree of calcification in the coronary arteries[27]. Khan et al. reported higher mean levels of CACand increased frequency of higher CAC in themetabolically healthy obese as compared to controls.One study assessed liver fat, and found that thefrequency of MHO participants with fatty liver wassignificantly higher than that of normal weight, but

Table 3 MHO Definition; Cross Sectional Studies
Study Definition of metabolically healthy obese (MHO) Definition of metabolically healthy, normal weight (MHNW)
Marini [25] • IS by OGTT & euglycemic clamp ≥75th percentile of all obese participants • Not obese (BMI < 27 kg/mg2)
• BMI >30
• Diabetics included
Stefan [26] • IS by OGTT ≥75th percentile of all obese participants • IS, normal weight (BMI < 25 kg/m2)
• BMI≥ 30
• Diabetics included
Irace [29] • <3 MetS criteria • <3 MetS, normal weight (BMI 18.5-25 kg/m2)
• BMI > 29.9
• Diabetics included
Khan [27] • <3 MetSA Criteria (including CRP ≥3.0 mg/L) • <3 MetSA criteria, normal weight (BMI < 25 kg/m2)
• BMI≥ 25
• Diabetics included
Park [28] • 0 MetSB criteria • 0 MetSB criteria, normal weight (BMI <23 kg/m2)
• BMI≥ 25
• Diabetics includedAWaist circumference excluded, added CRP ≥3.0 mg/L; BWaist circumference ≥90 cm for men and ≥80 cm for women, fasting glucose at least 100 mg/dL.
Roberson et al. BMC Public Health 2014, 14:14 Page 8 of 12http://www.biomedcentral.com/1471-2458/14/14
lower than metabolically unhealthy obeseparticipants [26]. Finally, one study also examinedmultiple measures of cardiovascular changesincluding left ventricular mass index(LVMI), mitralE/A ratio, E/Ea ratio, TDI and Ea velocity [28]. Parket al. found the MHO had significantly increasedLVMI and decreased mitral E/A ratio as comparedto the metabolically normal, normal weightparticipants; indicating changes in heart structureand function in this group [28].
iii.Other considerations
a. Inflammation. CRP was measured in two studies[27,28] neither of which reported the association ofCRP and CVD outcomes in the context of metabolichealth and obesity. Khan et al. included vascularinflammation (VI) in the definition of metabolicsyndrome [27]. Park adjusted for VI in predictingsubclinical CVD outcomes studied [28].
DiscussionThe purpose of the present study was to review the lit-erature that has examined the relationship between themetabolically healthy obese phenotype and cardiovascu-lar disease. The most common definition of MHO usedwas having a BMI ≥ 30 kg/m2 and less than 3 MetS cri-teria (8 studies). Nine studies also included insulin sensi-tivity in the definition of MHO. The most commonlyused comparison group was MHNW defined as having aBMI < 25 kg/m2 and meeting < 3 MetS criteria (9 stud-ies). Of the fourteen studies identified examining CVD
outcomes or all-cause mortality, most were not able todemonstrate a significant association between MHO andincreased risk of CVD and mortality. However, a trendtowards a slight increase in risk in all but one study wasobserved, which was supported by increased subclinicaldisease burden observed in the cross-sectional studies.In the six studies measuring subclinical CVD, the MHOphenotype was associated with increased subclinicalCVD burden in four, and this association achieved statis-tical significance. It appears that MHO individuals havea slightly increased CVD risk as compared to their nor-mal weight counterparts, but the results are mixed ascan be seen from the studies reviewed here. It is difficultto determine whether the mixed findings are a result ofmethodological issues (such as variable follow-up dur-ation, small sample size, non-standardized comparisongroups, outcome measurement, etc.) or due to a trulyweak effect. Therefore, there is a pressing need for estab-lishing a streamlined, central definition of “metabolicallyhealthy obese” in future studies.
Defining “metabolically healthy obese”As mentioned previously, the definitions of MHO arequite heterogeneous and make quantitative synthesis ofthe reviewed studies difficult. One of the first to identifyand review this phenotype in 2001, was Sims [30], whohighlighted visceral adiposity and insulin resistance as keydeterminants of MHO. In the literature analyzed for thisreview, the most commonly applied definition was the ab-sence or presence of MetS in conjunction with obesity(measured via BMI). IR was often ignored and replacedwith fasting glucose. BMI, though a useful tool for

Table 4 Results; Cross Sectional Studies
Study Subjects (Age, Male) Outcome Results
Marini [25] N = 153 CCA-IMT Mean CCA-IMT: MHO = 0.79 (0.08) vs. MHNW= 0.61 (0.11) p < 0.001
MHO = NR (35, 0%)
MHNW= 73 (34, 0%)
Stefan [26] N = 314 CCA-IMT Mean CCA-IMT: MHO = 0.54 (0.02) vs. MHNW= 0.51 (0.02) p = NS
MHO = 31 (47, 39%)
MHNW= 54 (45, 17%)
Irace [29] N = 1842 (30–80 years old, 55%) MHO = NR CCA-IMT Mean CCA-IMT: MHO = NR vs. MHNW= NR
MHNW=NR • AdjustedA OR of CCA-IMT MetS: 1.42 (1.10-1.83) p = 0.01BMI: p = NS
Khan [27] N = 475 CCA-IMT Mean CCA- IMT: MHO = 0.68 (0.09) vs. MHNW =0.64 (0.08) p < 0.001
MHO = 260 (51, 0%) aPWV Mean aPWV: MHO = 809.9 (182.3) vs. MHNW =731 (176.4) p < 0.001
MHNW= 145 (51, 0%) CAC Frequency (%) with increased CAC: MHO = 53 (20%) vs.MHNW =13 (9%) p < 0.001
AC Frequency (%) with increased AC: MHO = 130 (50%) vs.MHNW =47 (32%) p < 0.001
•AdjustedB OR's of CAC and AC associated with MHO vs.MHNW CAC: 2.38 (1.20,4.70) p = 0.01; AC: 2.37 (1.49.3.80) p < 0.001
•AdjustedB regression coefficients associated with MHO vs.MHNW CCA-IMT: 0.034 p < 0.001; aPWV: 59.7 p = 0.001
Park [28] N = 2540 MHO = 71 (52, 45%) CCA-IMT Mean CCA IMT: MHO = 0.72 (0.06) vs. MHNW= 0.70 (0.06) p = NS
MHNW= 286 (52, 52%) aPWV Mean aPWV: MHO = 12.8 (1.1) vs. MHNW= 12.9 (1.6) p = NS
LVMI Mean LVMI: MHO = 42.4 (7.4) vs. MHNW= 35.4 (6.6) p < 0.01
E/A ratio Mean E/A ratio: MHO = 1.17 (0.34) vs. MHNW= 1.34 (0.41) p < 0.05AAdjusted for age, sex, smoking, metabolic syndrome, BMI, LDL; BAdjusted for age, site of recruitment, education, race, smoking; CAdjusted for age, sex, heart rate,CRP, medication for hypertension, treatment for diabetes mellitus.
Roberson et al. BMC Public Health 2014, 14:14 Page 9 of 12http://www.biomedcentral.com/1471-2458/14/14
estimating body fatness, has limitations in that it does notdiscriminate between lean muscle and fat, or fat distribu-tion. Waist circumference, however, provides an estimateof visceral adiposity which many studies have shown to besignificantly associated with IR, type 2 diabetes, and car-diovascular events [31]. Fasting glucose, used in the diag-nosis of MetS, has limitations in that in only provides asnap-shot of glucose regulation [32]. Ideally, IR should bemeasured using the gold standard diagnostic test, thehyperinsulinemic euglycemic glucose clamp (HEGC) [33].However, this procedure is costly, labor intensive for theinvestigator, and largely uncomfortable for the patient. Lessinvasive, but still labor intensive tests such as HOMA-IR orthe quantitative insulin sensitivity check index (QUICKI)have been shown to produce similar results and may beuseful substitutes for HEGC.Two often-discussed points in MHO are inflammation
as measured by C-reactive protein (CRP) and fatty liveror non-alcoholic fatty liver disease (NAFLD). Inflamma-tion has been shown to promote IR [34]. CRP is thoughtto be the best biomarker of vascular inflammation andhas been shown to be predictive of CVD events [34,35].In the studies reviewed here, 4 studies included CRP inthe definition of MHO, but none of them assessed therelationship of VI and CVD risk. Therefore, the usefulness
of CRP as part of the definition of MHO, or as a predictorof CVD events in the metabolically healthy obese remainsuncertain in the studies reviewed here. It is difficult todraw conclusions regarding the usefulness of including VIin the definition of metabolic health or its role as a pre-dictor of CVD from the studies included in this review.Absence of NAFLD has also been explored as a potentialidentifier of MHO. Fatty liver has been implicated as con-tributing to IR, and has been associated with increasedrisk of incident cardiovascular disease even when control-ling for metabolic syndrome and obesity [36,37]. Messieret al. found that the MHO had lower liver fat content thantheir “at-risk” obese equivalents [38]. One study reviewedexamined fatty liver in the MHO and found them to havea prevalence of NAFLD similar to overweight participantsand greater than those in the normal weight category [26].Going forward, liver fat could prove a useful tool to diag-nose and assess metabolic health of the obese, especiallywhen other metabolic abnormalities are absent. NAFLDcan be assessed non-invasively using ultrasound, and pro-vides an early diagnostic marker for cardiovascular diseaserisk. More long-term studies are needed to confirm itsusefulness in the MHO population.Future studies would be well served to use an increas-
ingly strict definition of MHO which requires measures of

Roberson et al. BMC Public Health 2014, 14:14 Page 10 of 12http://www.biomedcentral.com/1471-2458/14/14
the most significant features (visceral adiposity and IR)while still including information on blood pressure, fastingglucose, cholesterol, triglycerides, liver fat, and inflamma-tion. To show a greater difference in risk, defining MHOas having none of the components may have greater util-ity. St-Pierre et al. found the relative risk of ischemic heartdisease increased linearly with increasing number of meta-bolic abnormalities [17]. No study reviewed used 0 MetScomponents to define MHO. However, among the threecohort studies which used ≤1 MetS criteria in the defin-ition of MHO, only one showed statistically significant dif-ference in the MHO as compared to MHNW [13].Equally important as defining MHO is the need to de-
termine appropriate comparison groups. In this review,we chose to look at only the comparison between MHOand the “healthiest” group. This was defined as themetabolically healthy, normal weight participants (BMI< 25 kg/m2) in most studies; however, some studieschose to use only normal weight individuals with no re-port of metabolic health, or included overweight individ-uals in the comparison group. Using these parameters,“unhealthy” traits may have leaked into the “healthiest”groups, leading to crossover bias in analysis which wouldmake true differences between these groups more diffi-cult to detect. No study has compared CVD risks in theMHO by class of obesity. Soverini et al. examined theprevalence of metabolic syndrome and insulin resistancein morbidly obese patients, and found a small percent-age maintained insulin sensitivity even at BMI > 40 kg/m2 [39]. When comparing MHO to the healthiest, thesickest, or even an intermediary (metabolically unhealthyand normal weight), this review stresses the importanceof a well defined comparison group in order to make in-ferences relevant to the general population.
Subclinical disease measuresWhen assessing intermediate risk populations such as theobese, the usefulness of traditional risk factor assessment(such as Framingham) diminishes. Measures of subclinicaldisease are increasingly important as they provide a viewof actual disease progression and more accurate event pre-diction than traditional CVD risk factors. The most com-mon subclinical disease measures used are CCA-IMT,CAC, ankle-brachial index (ABI), and endothelial func-tion. CCA-IMT was the most commonly studied measureof subclinical disease in the studies reviewed. A majorityof the studies documented a significant trend towards in-creased IMT in MHO versus controls. The rising goldstandard for measuring degree of atherosclerosis is CAC.Only one study in our analysis measured CAC and foundit was significantly increased in the MHO. No study todate has examined whether the differences in outcome(incident CVD and CVD mortality) can be explainedby differences in subclinical CVD. In the studies which
examined subclinical disease, all except one were cross-sectional in design, which gives us a snapshot of subclin-ical disease in the MHO, but does not allow us to examinethe progression of disease. The prospective study byBobbioni-Harsh et al. gave important insights into the de-velopment and progression of subclinical disease amongthe metabolically healthy obese, showing faster progres-sion of subclinical CVD, independent of metabolic abnor-malities [23]. Cohort studies allow us to see the timesensitive component of obesity, and the progressive devel-opment of cardiovascular risk factors. Future follow-upstudies are needed which include multiple measures ofsubclinical CVD at baseline and follow-up and examineMHO in context of increased burden as compared to theirnormal weight counterparts.
Expanding the subject populationCardiovascular disease prevalence, morbidity, and mortal-ity difference are well established across racial/ethnic andsocioeconomic lines [40,41]. Surveillance data fromNHANES and BRFSS indicate African Americans experi-ence higher death rates due to both heart disease andstroke [40]. Likewise, Hispanics and Non-Hispanic blackshave higher levels of obesity as compared to Non-Hispanicwhites [2]. Of the current studies reviewed, all but oneassessed CVD risk in the MHO phenotype in participantsof mainly Caucasian or European descent. Surveillancedata likewise indicates the prevalence of heart disease,hypertension, and stroke in those persons with incomesbelow the poverty threshold, is significantly greater thanthose at or above the poverty threshold [41]. We did notidentify any study which examined the prevalence of theMHO phenotype in association with CVD risk in theMHO across racial or socioeconomic lines. Thus, there isan urgent need for longitudinal studies with socioeconomi-cally diverse, multi-ethnic populations in order to correctlyidentify the CVD risk of the MHO group.
Mechanisms of MHOBehavioral and lifestyle factors may play a large role inwhy a subset of the obese do not present with metabolicabnormalities or present them at a slower pace. However,this is a topic which has not been studied at length andpresents mixed findings. Seven of the eight studies meas-uring physical activity found increased activity in themetabolically healthy obese, when compared to the meta-bolically unhealthy obese. In addition, several studiesfound that increased physical activity offset the increasedrisk of CVD in the MHO. This suggests that all studiesexamining the MHO phenotype should also assess phys-ical activity, as physical activity appears to nullify the effectof MHO on CVD risk. Hankinson et al. found no differ-ence between diet factors, and physical activity reportedbetween MHO and unhealthy obese participants [42].

Roberson et al. BMC Public Health 2014, 14:14 Page 11 of 12http://www.biomedcentral.com/1471-2458/14/14
However, Messier and colleagues found engaging in phys-ical activity increased the odds of presenting with theMHO phenotype among obese participants [38]. A reviewby Gill found that increasing physical activity reduced IR,a key factor in defining MHO [43]. While most studiesmeasured physical activity by self report, more accurateresults are obtained when physical fitness is directly mea-sured. Ortega et al. measured cardio-respiratory fitness bytreadmill test and found MHO participants had signifi-cantly higher VO2 max when compared to the metabolic-ally unhealthy obese [16]. Recent research on sedentarybehavior, independent of physical activity, has shown thatincreased sedentary time is associated with increased riskof diabetes, cardiovascular events, and cardiovascular aswell as all-cause mortality [44]. This is in agreement withthe belief that the natural tendency of the MHO is to pro-gress to MUHO when physical activity is stopped or re-duced [45]. To date, no study has examined sedentarytime in the MHO phenotype.Future research should also target genetic studies to illu-
minate why some obese individuals do not develop or ex-perience delayed development of metabolic syndrome. Forexample, one study in mice found that extremely obesemice with a mutation in the Brd2 gene are protected fromdeveloping type 2 diabetes mellitus [46]. This could providea clue as to why certain obese individuals do not seem todevelop the metabolic abnormalities associated with obes-ity. However, the search for relevant genes in humanmodels continues. It is likely that a gene-environment inter-action is at play, similar to the model suggested for the de-velopment of obesity [47]. More follow-up studies areneeded to examine the transition between MHO and meta-bolically unhealthy and obese, and whether genetics andlifestyle factors play a role in both development and reversalof such. Likewise, studies conducted in aging cohorts wouldgive insight into the prevalence of this phenotype in theelderly, clarifying the time-dependent relationship of obesityand metabolic abnormality presentation.
ConclusionMHO is an important, emerging phenotype with riskssomewhere intermediate between healthy, normal weightand unhealthy, obese individuals. Successful work towardsa universally accepted definition of MHO would improve(and simplify) future studies and strengthen inter-studycomparisons. Usefulness of a definition inclusive of insulinsensitivity in concert with stricter criteria for metabolicsyndrome components should be explored, as well as thepotential inclusion of fatty liver. As obesity continues torise, this phenotype will become increasingly important.Clinicians exercise caution in reassuring patients that themetabolically benign phenotype is safe, as increased risk ofcardiovascular events and death remains a possibilitybased on the limited data reviewed.
AbbreviationsABI: Ankle-brachial index; AC: Aortic calcium; aPWV: Aortic pulse wavevelocity; BMI: Body mass index; CAC: Coronary artery calcium; CCA-IMT: Common carotid artery intima media thickness; CRP: C-reactive protein;E/A: Early/Late; IR: Insulin resistance; IS: Insulin sensitive; LVMI: Left ventricularmass index; MetS: Metabolic syndrome based on the NCEP ATP III Definition:waist circumference ≥ 102 cm (male), ≥ 88 cm (female), TG ≥ 150 mg/dL oruse of lipid lowering medications HDL-C < 40 mg/dL (male) < 50 mg/dL(female) or use of lipid lowering medications, blood pressure ≥ 130/85 mmHgor use of antihypertensive medications fasting plasma glucose ≥ 110 mg/dlor use of antidiabetic medications.; MHNW: Metabolically healthy, normalweight; MHO: Metabolically healthy obese; MUHO: Metabolically unhealthyobese; MUNW: Metabolically unhealthy, normal weight; NAFLD: Non-alcoholicfatty liver disease; NR: Not reported; VI: Vascular inflammation; WBC: Whiteblood cell.
Competing interestsThe authors have no competing interests. Please send reprint requests [email protected]
Authors’ contributionsLR and EA carried out the literature review and data extraction. LR, WM, MB(Blaha), RD, and AS participated in table construction. LR, AA, TF, and MAdrafted the manuscript. RB and MB(Budoff) contributed to subclinical CVDsection. MR and TT assisted with discussion section. KN conceived of themanuscript concept and oversaw all aspects of manuscript preparation. Allauthors read and approved the final manuscript.
Author details1Center for Prevention and Wellness Research, Baptist Health Medical Group,Michigan Ave Suite 500, Miami Beach, Florida. 2Baptist Health South Florida,Miami, Florida. 3Department of Epidemiology, Robert Stempel College ofPublic Health, Florida International University, Miami, Florida. 4The JohnsHopkins Ciccarone Center for the Prevention of Heart Disease, Baltimore,Maryland. 5Lipid Clinic Heart Institute, University of Sao Paulo Medical SchoolHospital, Sao Paulo, Brazil. 6Department of Cardiology, Faculty of MedicalSciences, State University of Campinas (Unicamp), Campinas, São Paulo,Brazil. 7King Abdul Aziz Cardiac Center, Riyadh, Saudi Arabia. 8Brigham andWomen’s Hospital, Harvard School of Medicine, Boston, Massachusetts, USA.9Los Angeles Biomedical Research Institute, Torrance, California, USA.10Department of Medicine, Herbert Wertheim College of Medicine, FloridaInternational University, Miami, Florida.
Received: 25 June 2013 Accepted: 10 December 2013Published: 8 January 2014
References1. World Health Statistics 2012: World Health Organization. 20 Avenue Appia, 1211
Geneva 27, Switzerland: WHO Press; 2012. Retrieved February 12, 2013 fromhttp://www.who.int/gho/publications/world_health_statistics/2012/en/.
2. Ogden CL, Carroll MD, Kit BK, Flegal KM: Prevalence of obesity in theUnited States, 2009–2010. NCHS data brief 2012, 82:1–8.
3. Solomon CG, Manson JE: Obesity and mortality: a review of theepidemiologic data. Am J Clin Nutr 1997, 66(4 Suppl):1044S–1050S.
4. Flegal KM, Kit BK, Orpana H, Graubard BI: Association of all-cause mortalitywith overweight and obesity using standard body mass index categor-ies: a systematic review and meta-analysis. JAMA 2013, 309(1):71–82.
5. Finkelstein EA, Trogdon JG, Cohen JW, Dietz W: Annual medical spendingattributable to obesity: payer-and service-specific estimates. Health Aff(Millwood) 2009, 28(5):w822–w831.
6. Bluher M: The distinction of metabolically 'healthy' from 'unhealthy'obese individuals. Curr Opin Lipidol 2010, 21(1):38–43.
7. Karelis AD: To be obese–does it matter if you are metabolically healthy?Nat Rev Endocrinol 2011, 7(12):699–700.
8. Wildman RP, Muntner P, Reynolds K, et al: The obese withoutcardiometabolic risk factor clustering and the normal weight withcardiometabolic risk factor clustering: Prevalence and correlates of 2phenotypes among the us population (nhanes 1999–2004). Arch InternMed 2008, 168(15):1617–1624.

Roberson et al. BMC Public Health 2014, 14:14 Page 12 of 12http://www.biomedcentral.com/1471-2458/14/14
9. Arnlov J, Ingelsson E, Sundstrom J, Lind L: Impact of body mass index andthe metabolic syndrome on the risk of cardiovascular disease and deathin middle-aged men. Circulation 2010, 121(2):230–236.
10. Calori G, Lattuada G, Piemonti L, Garancini MP, Ragogna F, Villa M, Mannino S,Crosignani P, Bosi E, Luzi L, et al: Prevalence, metabolic features, andprognosis of metabolically healthy obese Italian individuals: the CremonaStudy. Diabetes Care 2011, 34(1):210–215.
11. Hamer M, Stamatakis E: Metabolically healthy obesity and risk of all-causeand cardiovascular disease mortality. J Clin Endocrinol Metab 2012,97(7):2482–2488.
12. Hosseinpanah F, Barzin M, Sheikholeslami F, Azizi F: Effect of differentobesity phenotypes on cardiovascular events in Tehran Lipid andGlucose Study (TLGS). Am J Cardiol 2011, 107(3):412–416.
13. Kuk JL, Ardern CI: Are metabolically normal but obese individuals atlower risk for all-cause mortality? Diabetes Care 2009, 32(12):2297–2299.
14. Meigs JB, Wilson PW, Fox CS, Vasan RS, Nathan DM, Sullivan LM, D'AgostinoRB: Body mass index, metabolic syndrome, and risk of type 2 diabetes orcardiovascular disease. J Clin Endocrinol Metab 2006, 91(8):2906–2912.
15. Ogorodnikova AD, Kim M, McGinn AP, Muntner P, Khan U, Wildman RP:Incident cardiovascular disease events in metabolically benign obeseindividuals. Obesity (Silver Spring) 2012, 20(3):651–659.
16. Ortega FB, Lee DC, Katzmarzyk PT, Ruiz JR, Sui X, Church TS, Blair SN: Theintriguing metabolically healthy but obese phenotype: cardiovascularprognosis and role of fitness. Eur Heart J 2013, 34(5):389–397.
17. St-Pierre AC, Cantin B, Mauriege P, Bergeron J, Dagenais GR, Despres JP,Lamarche B: Insulin resistance syndrome, body mass index and the riskof ischemic heart disease. CMAJ 2005, 172(10):1301–1305.
18. Voulgari C, Tentolouris N, Dilaveris P, Tousoulis D, Katsilambros N, StefanadisC: Increased heart failure risk in normal-weight people with metabolicsyndrome compared with metabolically healthy obese individuals. J AmColl Cardiol 2011, 58(13):1343–1350.
19. Katzmarzyk PT, Church TS, Janssen I, Ross R, Blair SN: Metabolic syndrome,obesity, and mortality: impact of cardiorespiratory fitness. Diabetes Care2005, 28(2):391–397.
20. Daly CA, Hildebrandt P, Bertrand M, Ferrari R, Remme W, Simoons M, Fox KM:Adverse prognosis associated with the metabolic syndrome in establishedcoronary artery disease: data from the EUROPA trial.Heart 2007, 93(11):1406–1411.
21. Song Y, Manson JE, Meigs JB, Ridker PM, Buring JE, Liu S: Comparison ofusefulness of body mass index versus metabolic risk factors inpredicting 10-year risk of cardiovascular events in women. Am J Cardiol2007, 100(11):1654–1658.
22. Bo S, Musso G, Gambino R, Villois P, Gentile L, Durazzo M, Cavallo-Perin P,Cassader M: Prognostic implications for insulin-sensitive and insulin-resistant normal-weight and obese individuals from a population-basedcohort. Am J Clin Nutr 2012, 96(5):962–969.
23. Bobbioni-Harsch E, Pataky Z, Makoundou V, Laville M, Disse E, Anderwald C,Konrad T, Golay A: From metabolic normality to cardiometabolic risk factorsin subjects with obesity. Obesity (Silver Spring) 2012, 20(10):2063–2069.
24. Alam I, Ng TP, Larbi A: Does inflammation determine whether obesity ismetabolically healthy or unhealthy? Aging Perspect Mediat Inflamm 2012,2012:14.
25. Marini MA, Succurro E, Frontoni S, Hribal ML, Andreozzi F, Lauro R, PerticoneF, Sesti G: Metabolically healthy but obese women have an intermediatecardiovascular risk profile between healthy nonobese women and obeseinsulin-resistant women. Diabetes Care 2007, 30(8):2145–2147.
26. Stefan N, Kantartzis K, Machann J, Schick F, Thamer C, Rittig K,Balletshofer B, Machicao F, Fritsche A, Haring HU: Identification andcharacterization of metabolically benign obesity in humans.Arch Intern Med 2008, 168(15):1609–1616.
27. Khan UI, Wang D, Thurston RC, Sowers M, Sutton-Tyrrell K, Matthews KA,Barinas-Mitchell E, Wildman RP: Burden of subclinical cardiovasculardisease in "metabolically benign" and "at-risk" overweight and obesewomen: the Study of Women's Health Across the Nation (SWAN).Atherosclerosis 2011, 217(1):179–186.
28. Park J, Kim SH, Cho GY, Baik I, Kim NH, Lim HE, Kim EJ, Park CG, Lim SY,Kim YH, et al: Obesity phenotype and cardiovascular changes.J Hypertens 2011, 29(9):1765–1772.
29. Irace C, Scavelli F, Carallo C, Serra R, Cortese C, Gnasso A: Body mass index,metabolic syndrome and carotid atherosclerosis. Coron Artery Dis 2009,20(2):94–99.
30. Sims EA: Are there persons who are obese, but metabolically healthy?Metabolism 2001, 50(12):1499–1504.
31. Lebovitz HE, Banerji MA: Point: visceral adiposity is causally related toinsulin resistance. Diabetes Care 2005, 28(9):2322–2325.
32. Bonora E, Tuomilehto J: The pros and cons of diagnosing diabetes withA1C. Diabetes Care 2011, 34(Suppl 2):S184–S190.
33. Muniyappa R, Lee S, Chen H, Quon MJ: Current approaches for assessinginsulin sensitivity and resistance in vivo: advantages, limitations, andappropriate usage. Am J Physiol Endocrinol Metab 2008, 294(1):E15–E26.
34. Bastard JP, Maachi M, Lagathu C, Kim MJ, Caron M, Vidal H, Capeau J, Feve B:Recent advances in the relationship between obesity, inflammation, andinsulin resistance. Eur Cytokine Netw 2006, 17(1):4–12.
35. Nordestgaard BG, Zacho J: Lipids, atherosclerosis and CVD risk: is CRP aninnocent bystander? Nutr Metab Cardiovasc Dis 2009, 19(8):521–524.
36. Moore JB: Non-alcoholic fatty liver disease: the hepatic consequence ofobesity and the metabolic syndrome. Proc Nutr Soc 2010, 69(2):211–220.
37. Targher G, Day CP, Bonora E: Risk of cardiovascular disease in patients withnonalcoholic fatty liver disease. N Engl J Med 2010, 363(14):1341–1350.
38. Messier V, Karelis AD, Robillard ME, Bellefeuille P, Brochu M, Lavoie JM,Rabasa-Lhoret R: Metabolically healthy but obese individuals: relationshipwith hepatic enzymes. Metabolism 2010, 59(1):20–24.
39. Soverini V, Moscatiello S, Villanova N, Ragni E, Di Domizio S, Marchesini G:Metabolic syndrome and insulin resistance in subjects with morbidobesity. Obes Surg 2010, 20(3):295–301.
40. Romero CX, Romero TE, Shlay JC, Ogden LG, Dabelea D: Changing trendsin the prevalence and disparities of obesity and other cardiovasculardisease risk factors in three racial/ethnic groups of USA adults. Adv PrevMed 2012, 2012:172423.
41. Mensah GA, Mokdad AH, Ford ES, Greenlund KJ, Croft JB: State ofdisparities in cardiovascular health in the United States. Circulation 2005,111(10):1233–1241.
42. Hankinson AL, Daviglus ML, Van Horn L, Chan Q, Brown I, Holmes E, Elliott P,Stamler J: Diet composition and activity level of at risk and metabolicallyhealthy obese American adults. Obesity (Silver Spring) 2012, 21(3):637–643.
43. Gill JM, Malkova D: Physical activity, fitness and cardiovascular diseaserisk in adults: interactions with insulin resistance and obesity. Clin Sci(Lond) 2006, 110(4):409–425.
44. Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, Khunti K,Yates T, Biddle SJ: Sedentary time in adults and the association withdiabetes, cardiovascular disease and death: systematic review andmeta-analysis. Diabetologia 2012, 55(11):2895–2905.
45. Nesto RW: Obesity: a major component of the metabolic syndrome.Texas Heart Institute journal / from the Texas Heart Institute of St Luke'sEpiscopal Hospital, Texas Children's Hospital 2005, 32(3):387–389.
46. Wang F, Deeney JT, Denis GV: Brd2 Gene disruption causes "metabolicallyhealthy" obesity: epigenetic and chromatin-based mechanisms thatuncouple obesity from type 2 diabetes. Vitam Horm 2013, 91:49–75.
47. Speakman JR: Obesity: the integrated roles of environment and genetics.J Nutr 2004, 134(8 Suppl):2090S–2105S.
doi:10.1186/1471-2458-14-14Cite this article as: Roberson et al.: Beyond BMI: The “Metabolicallyhealthy obese” phenotype & its association with clinical/subclinicalcardiovascular disease and all-cause mortality – a systematic review.BMC Public Health 2014 14:14.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit