Embed Size (px)
DESCRIPTION
Clinical news for nephrologists and urologists.
Citation preview

J U N E 2 0 1 2 ■ ■ ■ V O L U M E 1 1 , I S S U E N U M B E R 6 ■ ■ ■ www.renalandurologynews.com
BY JODY A. CHARNOWATLANTA—Radical prostatectomy (RP) is associated with better overall and disease-specifi c survival compared with external beam radiation therapy (EBRT) for localized prostate cancer (PCa), according to fi ndings presented at the American Urological Association 2012 annual meeting.
In a study of 1,655 men with localized PCa—including 1,164 (70.3%) who underwent RP and 491 (29.7%) who had EBRT—researchers found that RP was associated with a 40% and 65% decreased likelihood of overall and
disease-specifi c mortality, respectively, compared with EBRT, after adjusting for multiple confounders.
“The poorer overall survival with radiotherapy is largely due to selec-tion bias—healthier men are more likely to get surgery,” said lead inves-tigator Richard M. Hoffman, MD, MPH, Professor of Internal Medicine at the University of New Mexico in Albuquerque. He and his colleagues obtained information on medical condi-tions at the time of diagnosis based on well-accepted comorbidity scales, and they used multivariate statistical tech-
niques to adjust for comorbidity differ-ences between treatment groups. These measures are relatively crude, however, Dr. Hoffman said.
As for why radiotherapy patients had worse disease-specific survival com-pared with RP patients, Dr. Hoffman
observed that in the mid 1990s, radia-tion dosages were lower and data had yet to be published showing that men with high-risk PCa (based on high PSA levels and high Gleason scores) benefited from receiving
RP Bests EBRT for PCa SurvivalPatient selection bias could be a factor
Higher 25D Levels Needed to Lower PTH
DISEASE-SPECIFIC mortality is greater with external beam radiation than RP.
© D
R. P
. MAR
AZZI
/ P
HOTO
RES
EARC
HERS
, IN
C
Dipstick Test for Sepsis-Related AKI
NATIONAL HARBOR, Md.—New-onset dipstick proteinuria may be a useful and inexpensive biomarker for predicting development of acute kid-ney injury (AKI) in critically ill septic patients, researchers reported at the National Kidney Foundation 2012 Spring Clinical Meetings.
AKI develops in nearly 30% of patients with severe sepsis, and microalbuminuria has been described in up to 87% of septic patients, the investigators noted.
Resident physician Javier Neyra, MD, and collaborators at Henry Ford Hospital in Detroit enrolled 470 pa-tients hospitalized with severe sepsis.
Of these, 328 underwent dipstick test-ing at admission. Serum creatinine increased by at least 0.3 mg/dL in 210 subjects (64%) within the fi rst 72 hours of admission. In this group, the researchers observed new-onset dipstick proteinuria in 114 patients (54%), which translated into a 75% positive predictive value for AKI, and in 91 of 166 subjects (55%) with AKI by Acute Kidney Injury Network (AKIN) criteria, for a PPV of 60%. New-onset dipstick proteinuria at the time of ad -mission was independently asso-ciated with a 2.3 times increased likelihood of AKI, after adjusting for
BY JODY A. CHARNOWNATIONAL HARBOR, Md.—Levels of 25-hydroxyvitamin D (25D) higher than 20 ng/mL would be required to normalize intact parathyroid hormone (iPTH) levels in patients with stages 3 and 4 chronic kidney disease (CKD) as well as vitamin D insuffi ciency and sec-ondary hyperparathyroidism, research-ers concluded in a study presented at the National Kidney Foundation 2012 Spring Clinical Meetings.
Amit Sharma, MD, Chief Medical Offi cer at Pacifi c Renal Research Institute in Meridian, Idaho, and colleagues noted that a 2010 Institute of Medicine report CME FEATURES Earn 2 CME credits
in this issue
Lupus: an update on • management p.15
Part III of our series on• gout management p.35
IN THIS ISSUE
8 Escherichia coli resistance to ciprofl oxacin on the rise
12 Oral calcitriol as effective as vitamin D for treating SHPT
14 Q&A: With ESAs, should weindividualize treatment?
23 PD patients are at higher risk for infections
30 Neoadjuvant chemotherapy for small cell urothelial carcinoma
Doctors haunted by catastrophic
errors in surgery
PAGE 33
continued on page 10
continued on page 10
continued on page 10
PAGE 35

Put Women Back on the Research Agenda
Should a nephrologist start an osteoporotic post-menopausal transplant patient on hormone
replacement therapy? What is the risk of breast cancer in a woman on chronic dialysis? Should she get a yearly mammogram? Does a 35-year-old woman with chronic kidney disease (CKD) have the same car-diovascular risk as a man? Why are women referred less frequently for fi stula placement and kidney trans-plantation? No answers? I don’t have them either. Unfortunately, in the past few years, very few studies have looked at issues relating to gender and CKD, including response to therapy, which is of great-est concern.
In almost all studies and in recommendations for care, including guidelines from the Kidney Disease: Improving Global Outcomes (KDIGO) foundation and the Kidney Disease Outcomes Quality Initiative (KDOQI), there are no specifi c recommendations made based on gender. At the National Kidney Foundation (NKF) Spring Clinical Meetings, Mitton et al from State University of New York Downstate Medical Center in Brooklyn and the NKF of Greater NY, reported the fi ndings of a survey of 300 kidney disease professionals from throughout the United States, Canada, and the Caribbean, show-ing a universal self-perceived lack of knowledge regarding women’s health issues in CKD, including the use of hormone replacement therapy, treatment of osteoporosis and menstrual disorders, and gender disparities in care.
In addition, a review of the 394 posters presented at the same meeting revealed only four (1%) addressing any issue related to gen-der, including the observation by Molnar et al from Harbor-UCLA Medical Center that women are referred later for initiation of dialysis after failed transplant.
It is time for the NKF and the International Society of Nephrology to focus on gender difference in CKD, dialysis, and transplantation, and develop guidelines for care, following in the footsteps of the American Heart Association, that has published specifi c guidelines on the prevention of cardiovascular disease in women (Circulation 2011:123:1243-1262). Women make up at least half, if not more, of patients with CKD. It is time for us to put gender back on the agenda, both in research and in patient care.
Mariana Markell, MDAssociate Professor of MedicineState University of New York Downstate Medical Center, Brooklyn
GUEST EDITORIAL
EDITORIAL ADVISORY BOARD
Renal & Urology News (ISSN 1550-9478) Volume 11, Number 6. Published monthly by Haymarket Media, Inc., 114 West 26th Street, 4th Floor, New York, NY 10001. Periodicals postage paid at New York, NY, and an additional mailing offi ce. The subscription rates for one year are, in the U.S., $75.00; in Canada, $85.00; all other foreign countries, $110.00. Single issues, $20.00. www.renalandurologynews.com. Postmaster: Send address changes to Renal & Urology News, c/o DMD Data Inc., 2340 River Road, Des Plaines, IL 60018. For reprints, contact Wright’s Reprints at 1.877.652.5295. Copyright: All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means (electronic, mechanical, photocopying, recording, or otherwise) without the prior written permission of Haymarket Media, Inc. Copyright © 2012.
Renal & Urology News Staff
Editor Jody A. Charnow Executive editor Marina Galanakis Senior editor Delicia Honen Yard Web editor Stephan Cho Editorial coordinator Candy Iemma Art director Andrew Bass Group art director, Haymarket Medical Jennifer Dvoretz VP, audience development and operations John Crewe Production manager Kathleen Millea Product manager, digital products Chris Bubeck Circulation manager Paul Silver National accounts manager William Canning Publisher Dominic Barone VP medical magazines and digital products Jim Burke CEO, Haymarket Media Inc. Lee Maniscalco
Medical Director, Urology
Robert G. Uzzo, MD, FACSG. Willing “Wing” Pepper Chair in Cancer ResearchProfessor and ChairmanDepartment of Surgery Fox Chase Cancer Center Temple University School of MedicinePhiladelphia
Urologists
Frank R. Cerniglia Jr, MDAttending Pediatric UrologistChildren’s Urology of VirginiaRichmond, Va.Christopher S. Cooper, MDDirector, Pediatric UrologyChildren’s Hospital of IowaIowa CityR. John Honey, MDHead, Division of Urology,Endourology/Kidney Stone DiseasesSt. Michael’s HospitalUniversity of TorontoStanton Honig, MDAssociate Clinical Professor of Surgery/UrologyUniversity of Connecticut School of Medicine, Urology CenterNew HavenJ. Stephen Jones, MD, FACSChairmanDepartment of Regional UrologyCleveland ClinicGlickman Urological & Kidney InstituteProfessor of SurgeryCleveland ClinicLerner College of Medicineof Case Western Reserve UniversityJames M. McKiernan, MDAssistant Professor of UrologyColumbia University Collegeof Physicians and SurgeonsNew York CityKenneth Pace, MD, MSc, FRCSCAssistant ProfessorDivision of UrologySt. Michael’s HospitalUniversity of TorontoRyan F. Paterson, MD, FRCSCAssistant ProfessorDivision of Urologic SciencesUniversity of British ColumbiaVancouver, Canada
Medical Director, Nephrology
Kamyar Kalantar-Zadeh, MD, PhD, MPHProfessor of Medicine and Pediatrics, and Director, Dialysis Expansion & Epidemiology Harbor-UCLA Division of Nephrology & Hypertension Los Angeles BioMedical Research Institute, The David Geffen School of Medicine at UCLA
Nephrologists
Anthony J. Bleyer, MD, MSProfessor of Internal Medicine/NephrologyWake Forest University School of MedicineWinston-Salem, N.C.
Suphamai Bunnapradist, MDDirector of ResearchDepartment of NephrologyKidney Transplant Research CenterThe David Geffen School of Medicine at UCLA
R. Michael Hofmann, MDAssociate Professor and Medical Director, Living Kidney Donor Program University of Wisconsin School of Medicine and Public Health, Madison
Csaba P. Kovesdy, MDAssociate Professor of Clinical Medicine University of Virginia, CharlottesvilleChief of NephrologySalem VA Medical CenterSalem, Va.
Edgar V. Lerma, MD, FACP, FASN, FAHA Clinical Associate Professor of Medicine Section of Nephrology Department of Medicine University of Illinois at Chicago College of Medicine, Chicago
Allen Nissenson, MD Emeritus Professor of Medicine The David Geffen School of Medicine at UCLA, Chief Medical Offi cer, DaVita Inc.
Rulan Parekh, MD, MSAssociate ProfessorJohns Hopkins Children’s Center, BaltimoreRobert Provenzano, MDChief, Section of NephrologySt. John Hospital and Medical Center, DetroitRobert S. Rigolosi, MDDirector, Regional Hemodialysis CenterHoly Name Hospital, Teaneck, N.J.
Lynda Anne Szczech, MD, MSCEAssociate Professor of NephrologyDuke University School of MedicineDurham, N.C.
www.renalandurologynews.com JUNE 2012 Renal & Urology News 5
Renal & Urology News welcomes letters to the editor. Send to:Jody A. Charnow, 114 West 26th Street, 4th Floor, New York, NY 10001or e-mail [email protected]

““
ContentsUrology
10 Baldness Increases PCa Risk Male pattern baldness is signifi cantly
associated with an elevated risk for prostate cancer.
30 Partial Nephrectomy Is An Option for Larger Tumors
Partial nephrectomy can be safely performed in patients with renal tumors 7 cm or more in diameter with acceptable technical, oncologic and functional outcomes.
31 HIFU Focal Therapy Feasible for PCa In a small study, 90% of men had erections
satisfactory for intercourse at 12 months post-treatment and all men who were pad-free at baseline were pad-free three months post-op.
32 Perineural Invasion Predicts PSA Relapse After Brachytherapy
Perineural invasion and post-treatment PSA levels at 12 months strongly predict long-term PSA relapse-free survival after defi ni-tive brachytherapy for prostate cancer.
Nephrology 13 Phosphate Binder Noncompliance Underreported Dialysis patient underreporting of noncom-
pliance with phosphate binder therapy may contribute to poor phosphorus control.
22 Early Dialysis Starts May Be Unwise This approach is associated with deleterious
consequences, such as an increased likelihood of withdrawal from treatment.
23 Death Risk Is Highest With CVCs Central venous catheters are associated
with the highest mortality risk among hemodialysis vascular access options.
32 A Down Side to Antimicrobial Locks They may result in more dangerous
or harder-to-treat catheter-related bloodstream infections.
Departments 5 Guest Editorial Put women on the
nephrology research agenda
8 News in Brief Retransplanted kidney
regains function
19 On the Forefront Teaming up to show
“meaningful use”
24 Renal Nutrition Update DASH-style diet may
benefi t CKD patients
33 Malpractice News Catastrophic medical
errors can haunt docs
34 Practice Management The pros and cons
of telemedicine
CME Features 15 Update on the Management
of Lupus Nephritis The authors discuss the
pathogenesis, disease course, and treatment.
35 Part 3: Clinical Challenges and Renal Considerations in Managing Gout
Our ongoing series on gout management with particular emphasis on renal complications.
24
16
The art of medicine is the skill of reconciling the risks and benefi ts of any treatment when the data are incomplete and those risks are, in part, unknown.
See our Expert Q&A on page 14
Expert Q&ARenal & Urology News speaks with Oliver Khakmahd, MD, a member of a large nephrology practice in Oakland, Calif., about implementing an electronic health record system.
Clinical QuizTake our latest quiz at renalandurologynews.com/clinical-quiz/. Answer correctly and you will be entered to win a $50 American Express gift card. Congratulations to our April winner:Geoffrey Lee, MD
The Medical MinuteVisit renalandurologynews.com/the-medical-minute/ to hear podcast reports on new studies. Our latest include:Metformin May Improve Prostate•
Cancer Surgery OutcomesAspirin Found to Protect Against•
Kidney CancerStem Cells May Lower Infection •
Risk in Transplant Recipients
News CoverageVisit our web site for comprehensive coverage of the American Transplant Congress in Boston, June 2-6.
J U N E 2 0 1 2 ■ V O L U M E 1 1 , I S S U E N U M B E R 6
ONLINE this month atrenalandurologynews.com

8 Renal & Urology News JUNE 2012 www.renalandurologynews.com
News in Brief Please visit us at www.renalandurologynews.com for the latest news updates from the fi elds of urology and nephrology
Failing Donor Kidney Regains Function in Second RecipientA renal allograft was removed from a 27-year-old man on posttransplant
day 14 and donated to a 66-year-old man on the waiting list after the fi rst patient suffered persistent proteinuria, worsening hypoalbuminemia, rising creatinine, and the development of intraabdominal hematoma beginning on posttransplant day 2.
Both patients and the hospital ethics committee and internal review board consented to the transfer. The allograft, originally donated by the younger man’s sister, regained function immediately after retransplantation, with serum creatinine levels declining from 5.27 to 1.84 mg/dL and proteinuria falling from 25 g to 1.2 g per 24 hours, according to a report in the New England Journal of Medicine (2012;366:1648-1649). Biopsies performed on days 8 and 25 after retransplantation showed a reversal of the histopathologic lesions seen developing in the fi rst recipient. Eight months after retransplantation, the second recipient’s glomerular fi ltration rate remained above 90 mL/min/1.73m2 in the setting of mild proteinuria (0.27 g per 24 hours).
Fish Oil Capsules Taken After AV Graft Creation Benefi cialF ish oil supplementation is associated with cardiovascular benefi ts in patients
with stage 5 chronic kidney disease following creation of a synthetic arterio-venous graft for hemodialysis access, according to study fi ndings published in the Journal of the American Medical Association (2012;307:1809-1816).
In the study, 99 patients took four 1 gram capsules of fi sh oil and 97 took placebo on the seventh day following graft creation. After 12 months, compared with the placebo group, the fi sh-oil group experienced a lower rate of graft failure (3.43 vs. 5.95 per 1,000 access-days), half as many thromboses (1.71 vs. 3.41 per 1,000 access-days), fewer corrective interventions (2.89 vs. 4.92 per 1,000 access-days), improved cardiovascular-event-free survival, and lower mean systolic blood pressure. Loss of native patency did not differ signifi cantly between the groups, however.
New Medication Approvedfor Erectile DysfunctionThe FDA has approved avanafi l (Stendra) for the treatment of erectile dys-
function (ED), making it the fi rst drug to be approved for the condition in nearly 10 years.
Manufactured by Vivus, of Mountain View, Calif., avanafi l met all primary effi cacy endpoints in more than 1,200 men with ED who participated in clinical studies, according to a press release issued by the company. Signifi cant improvements in erectile function were observed for all doses (50 mg, 100 mg, and 200 mg) com-pared with placebo.
“Patients and treating physicians continue to report signifi cant dissatisfaction with current treatments of ED,” Vivus President Peter Tam said.
It is recommended that avanafi l be taken about 30 minutes before sexual activ-ity. It should not be taken more than once per day.
Study Demonstrates RARP AdvantagesAn analysis comparing 11,889 men who underwent robot-assisted radical prostatectomy (RARP) with 7,389 open radical prostatectomy (RP) patients demonstrated that the RARP patients were 66% less likely to receive a blood transfusion, 53% and 14% less likely to experience an intra-operative or postoperative complica-tion, respectively, and 72% less likely to experience a prolonged length of stay compared with open RP patients. researchers reported in European Urology (2012;61:679-685).
Aliskiren Warnings Being UpdatedLabels for the aliskiren-containing drugs Amturnide, Tekturna, Tekturna HCT, Tekamlo, and Valturna are being updated to warn against the use of the drug with angiotensin receptor block-ers (ARBs) or ACE inhibitors in patients with diabetes because of a risk of renal impairment, hypotension, and hyper-kalemia. Also being added is a warning to avoid the use of aliskiren with ARBs or ACE inhibitors in patients with moderate-to-severe renal impairment.
E. coli Ciprofl oxacin Resistance RisingU.S. outpatient urine samples contain-ing Escherichia coli isolates showed that the bacterium’s resistance to cip-rofl oxacin rose from 3% to 17.1% and its resistance to trimethoprim-sulfame-thoxazole increased from 17.9% to 24.2%, from 2000 to 2010, according to a report in Antimicrobial Agents and Chemotherapy (2012;56:2181-2183). During the same period, however, minimal change was observed in E. coli resistance to nitrofurantoin (0.8% to 1.6%) and ceftriaxone (0.2% to 2.3%).
Transdermal Gel for OAB LaunchedWatson Pharmaceuticals of Parsippany, N.J., and Antares Pharma. Inc. of Ewing, N.J., have announced the launch of Gelnique (oxybutynin), a transdermal gel for the treatment of overactive bladder (OAB) with symptoms of urge urinary incon-tinence, urgency and frequency. Gelnique is applied once-daily to the thigh, abdomen, upper arm, or shoulder, and delivers a consistent dose of oxybutynin through the skin over a 24-hour period.
Short Takes
A recent Renal & Urology News online poll asked urologists: “Should percent free PSA be incorporated into the decision to perform an initial prostate biopsy in men with moderately elevated PSA levels?” Here are the results based upon 175 responses.
Straight
from
the W
eb The Value of Percent Free PSA
57.7%33.7%
8.6%

10 Renal & Urology News JUNE 2012 www.renalandurologynews.com
both radiation and androgen depri-vation therapy. “Current radiation modalities and treatment regimens could provide better outcomes for patients,” Dr. Hoffman added. “However, another explanation could be that surgery is a better treatment.”
The study, which was presented at the meeting by David F. Penson,
MD, MPH, of Vanderbilt University in Nashville, Tenn., included partici-pants in the Prostate Cancer Outcomes Study, which enrolled subjects diag-nosed with PCa between October 1994 and October 1995.
Dr. Hoffman noted that no random-ized controlled trials have compared survival outcomes among men with localized PCa treated with RP versus radiotherapy. The study by his group provides the fi rst long-term survival
results comparing the two treatments for localized PCa. Previous observa-tional studies have focused either on just one type of treatment, used sur-rogate endpoints such as PSA rises, or were single-center investigations.
“Our results, based on a large-pop-ulation-based cohort, are much more generalizable, though we recognize that patient selection and treatments have changed since we enrolled patients in the mid 1990s,” Dr. Hoffman said. ■
recommended 20 ng/mL as the lower limit of the normal range for 25D for healthy individuals, but recent studies sug-gest that this limit may be too low for patients with stage 3 or 4 CKD and high iPTH levels.
Existing therapies, he noted, such as over-the-counter vitamin D sup-plements, have diffi culty raising 25D levels effectively or consistently.
“Despite the widely held belief that a serum 25D level of 30 ng/mL is sufficient, our research suggests that we need to target much high-er levels of 25D in stage 3 and 4 CKD patients, possibly as high as 60 ng/mL,” Dr. Sharma told Renal & Urology News.
Dr. Sharma’s team examined the relationship between iPTH and 25D in patients with stages 3 and 4 CKD in a doubled-blind study of CTAP101 Capsules, a modifi ed-release formulation of calcifediol, poised to enter Phase 3 development shortly. Seventy-eight patients aged 18-80
years were randomized to receive the capsules (30, 60, or 90 µg of the drug) or matching placebo for six weeks. At baseline, subjects had a mean eGFR of 39.4 mL/min/1.73 m2, iPTH of 136 pg/mL, 25D level of 22.4 ng/mL, serum calcium level, 9.3 mg/dL, and serum phosphorus level of 3.7 mg/dL.
Throughout treatment, serum 25D values increased progressively in a dose-proportional manner up to about 100 ng/mL at the 90 µg dose, the researchers reported. After six weeks of treatment, the first iPTH lowering threshold occurred at a 25D value of about 40 ng/mL, which is sub-stantially higher than the iPTH reduc-tion threshold (12 ng/mL) observed in non-CKD patients.
In the active drug group, a 25D level of 84 ng/mL was associated with the upper limit of normal for iPTH (72 pg/mL). Some patients had 25D increases exceeding 100 ng/mL, but investiga-tors reported observing no signifi cant change in calcium or phosphorus.
Data from this clinical study sug-gest that stage 3 and 4 CKD patients require much higher levels of 25D to lower iPTH effectively, “certainly much higher than we can achieve through existing therapies,” Dr. Sharma said.
Bone and mineral metabolism guide-lines from both the Kidney Disease Outcomes Quality Initiative (K/DOQI) and Kidney Disease: Improving Global Outcomes (KDIGO) foundation, rec-ommend fi rst correcting 25D levels in Stage 3 and 4 CKD patients with elevat-ed iPTH levels. “We know from practi-cal experience that existing therapies to correct 25D are used off-label and are ineffective for the majority of patients,” Dr. Sharma said. “A new therapy that has the ability to signifi cantly raise 25D levels and lower iPTH in this patient population would be of signifi cant ben-efi t for our practice.” ■
Levels of 25D higher than 20 ng/mL needed to normalize iPTH.
PCa survival bettercontinued from page 1
Higher 25D levels
continued from page 1
Baldness Increases PCa RiskATLANTA—Androgenic alopecia, also known as male pattern baldness, is signifi cantly associated with an elevated risk for prostate cancer (PCa), researchers reported at the American Urological Association 2012 annual meeting.
In a prospective study of 196 consecutive patients referred for prostate biopsy, Neil E. Fleshner, MD, and colleagues at the University of Toronto, and colleagues found that the more severe the pattern baldness, the greater the risk for PCa. Frontal balding was associated with a 1.3 times increased risk, whereas mild, moderate, and severe vortex balding was associ-ated with a 1.9, 2.4, and 2.5 times increased risk. Balding remained a signifi cant predictor even after adjusting for age, digital rectal exami-nation (normal vs. abnormal), and PSA level.
The study also looked at whether the ratio of the lengths of the index and ring fi ngers predicted PCa and found no association. Previous retrospective studies have suggested that a low ratio, which indicates high prenatal androgen exposure, is associated with PCa.
Androgens play a role in the devel-opment of both androgenic alopecia and PCa. Previous retrospective studies have shown a relationship between male pattern baldness and PCa. For example, French research-ers reported in Annals of Oncology (2011;22:1824-1827) that patients with PCa were twice as likely to have androgenic alopecia at age 20 com-pared with non-PCa patients.
Dr. Fleshner said the fi ndings of the new study are preliminary, so at this point they should not alter clini-cal decision making. “However, our next step is to test whether adding patterns of hair loss may augment current prediction models for prostate biopsies,” he said. “This should be done on a larger cohort and prefer-ably in the primary care setting.” ■
age, race, gender, comorbidities, and other factors.
Dr. Neyra, who presented study fi ndings, explained that sepsis results in increased urinary excretion of albumin. Evidence suggests that this could be related to decreased tubular reabsorption of albumin and upregu-lation of the kidney albumin gene in response to AKI. “So the appearance of proteinuria is expected in these patients,” Dr. Neyra said.
Production of creatinine from mus-cle is reduced in septic patients, so relying on changes in serum creati-nine to diagnose AKI in such settings could delay the diagnosis of AKI, Dr. Neyra and his colleagues stated. Conse - quently, they observed, it is important
to identify sensitive and specifi c bio-markers that provide timely diagnosis of AKI before substantial damage is done. The investigators concluded that new-onset dipstick proteinuria represents a simple, inexpensive bio-marker in sepsis with predictive power for AKI.
The study by Dr. Neyra’s group adds to a growing literature on the topic of predicting development of AKI. Last year, researchers at Mayo Clinic reported in the Clinical Journal of the American Society of Nephrology (2011;6:1744-1751) that delayed initia-tion of adequate antibiotic treatment and transfusion of blood products are among the risk factors associated with development AKI in patients with septic shock. Other predictors include intra-abdominal sepsis, use of an ACE inhibitor or angiotensin
receptor blocker (ARB), and body mass index (BMI).
The study included 390 patients admitted to a medical intensive care unit. After adjusting for confounders, the researchers found that each hour of delay in initiation of adequate antibiot-ics was associated with a signifi cant 3% increased risk of AKI. Each 1 kg/m2
increment in BMI was associated with a 2% increased risk. Use of an ACE inhibitor or ARB was associated with a signifi cant 88% increased risk. Intra-abdominal sepsis and blood product transfusion increased AKI risk twofold and fi vefold, respectively.
Additionally, each 1 mL/min/1.73 m2 increment in baseline GFR was associated with a 1% decreased risk of AKI. Adequate goal-directed resus-citation was associated with a 47% decreased risk. ■
Dipstick test for AKI continued from page 1

12 Renal & Urology News JUNE 2012 www.renalandurologynews.com
NATIONAL HARBOR, Md.—Oral calcitriol is as effective as vitamin D analogues for treating secondary hyper-parathyroidism (SHPT) in hemodialy-sis patients but is more cost effective, according to a study presented at the National Kidney Foundation 2012 Spring Clinical Meetings.
Sandeep Aggarwal, MD, and collabo-rators at Drexel University College of Medicine in Philadelphia retrospectively studied 52 dialysis patients with SHPT who were converted from intravenous vitamin D analogues (paricalcitol or doxercalciferol) to oral calcitriol. The researchers observed no significant
differences in calcium and phospho-rus levels at three months after switch-ing to calcitriol and at the end of the study at nine months. After switching from vitamin D analogues to calcitriol, mean intact parathyroid hormone lev-els increased from 360 to 418 pmol/L and mean calcium levels rose from 9.19
to 9.50 mg/dL, but the increases were not statistically signifi cant and values remained within guideline targets rec-ommended by the Kidney Disease: Improving Global Outcomes (KDIGO) foundation. The cost per patient per week was $116.40 with vitamin D com-pared with $6.60 with calcitriol. ■
Calcitriol is as Effective as Vitamin D Analogues
Brief Summary of Prescribing Information for:OMONTYS (peginesatide) Injection for intravenous or subcutaneous use
WARNING: ESAs INCREASE THE RISK OF DEATH, MYOCARDIAL INFARCTION, STROKE, VENOUS THROMBOEMBOLISM, THROMBOSIS OF VASCULAR ACCESS AND TUMOR PROGRESSION OR RECURRENCE. See full prescribing information for complete boxed warning.
Chronic Kidney Disease:• In controlled trials, patients experienced greater risks for death,
serious adverse cardiovascular reactions, and stroke when administered erythropoiesis-stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL.
• No trial has identified a hemoglobin target level, ESA dose, or dosing strategy that does not increase these risks [see Warnings and Precautions].
• Use the lowest OMONTYS dose sufficient to reduce the need for red blood cell (RBC) transfusions [see Warnings and Precautions].
INDICATIONS AND USAGEAnemia Due to Chronic Kidney DiseaseOMONTYS is indicated for the treatment of anemia due to chronic kidney disease (CKD) in adult patients on dialysis.Limitations of UseOMONTYS is not indicated and is not recommended for use:• In patients with CKD not on dialysis because of safety concerns in this
population [see Warnings and Precautions].• In patients receiving treatment for cancer and whose anemia is not due to
CKD, because ESAs have shown harm in some settings and the benefit-risk factors for OMONTYS in this setting have not been evaluated [see Warnings and Precautions].
• As a substitute for RBC transfusions in patients who require immediate correction of anemia.
• OMONTYS has not been shown to improve symptoms, physical functioning or health-related quality of life.
CONTRAINDICATIONSOMONTYS is contraindicated in patients with:• Uncontrolled hypertension [see Warnings and Precautions].WARNINGS AND PRECAUTIONSIncreased Mortality, Myocardial Infarction, Stroke, and Thromboembolism• In controlled clinical trials of other ESAs in patients with CKD comparing
higher hemoglobin targets (13 – 14 g/dL) to lower targets (9 - 11.3 g/dL)(see Table 2), increased risk of death, myocardial infarction, stroke, congestive heart failure, thrombosis of hemodialysis vascular access, and other thromboembolic events was observed in the higher target groups.
• Using ESAs to target a hemoglobin level of greater than 11 g/dL increases the risk of serious adverse cardiovascular reactions and has not been shown to provide additional benefit. Use caution in patients with coexistent cardiovascular disease and stroke. Patients with CKD and an insufficient hemoglobin response to ESA therapy may be at even greater risk for cardiovascular reactions and mortality than other patients. A rate of hemoglobin rise of greater than 1 g/dL over 2 weeks may contribute to these risks.
• In controlled clinical trials of ESAs in patients with cancer, increased risk for death and serious adverse cardiovascular reactions was observed. These adverse reactions included myocardial infarction and stroke.
• In controlled clinical trials, ESAs increased the risk of death in patients undergoing coronary artery bypass graft surgery (CABG) and deep venous thrombosis (DVT) was observed in patients undergoing orthopedic procedures.
The design and overall results of 3 large trials comparing higher and lower hemoglobin targets are shown in Table 2 (Normal Hematocrit Study (NHS), Correction of Hemoglobin Outcomes in Renal Insufficiency (CHOIR) and Trial to Reduce Cardiovascular Events with Aranesp® Therapy (TREAT)).
Table 2 Adverse Cardiovascular Outcomes in Randomized Controlled Trials Comparing Higher and Lower Hemoglobin Targets in Patients with CKD
NHS(N = 1265)
CHOIR(N = 1432)
TREAT(N = 4038)
Time Period of Trial 1993 to 1996 2003 to 2006 2004 to 2009
Population
Patients with CKD on hemodialysis
with coexisting CHF or CAD, hematocrit
30 ± 3% onepoetin alfa
Patients with CKD not on dialysis with
hemoglobin< 11 g/dL
not previously administeredepoetin alfa
Patients withCKD not on dialysis with
type II diabetes, hemoglobin≤ 11 g/dL
Hemoglobin Target; Higher vs. Lower (g/dL)
14.0 vs. 10.0 13.5 vs. 11.3 13.0 vs. ≥ 9.0
Median (Q1, Q3)Achieved Hemoglobin level (g/dL)
12.6 (11.6, 13.3)vs.
10.3 (10.0, 10.7)
13.0 (12.2, 13.4)vs.
11.4 (11.1, 11.6)
12.5 (12.0, 12.8) vs.
10.6 (9.9, 11.3)
Primary Endpoint All-cause mortalityor non-fatal MI
All-cause mortality, MI, hospitalizationfor CHF, or stroke
All-cause mortality, MI, myocardial ischemia, heart
failure, and strokeHazard Ratio or Relative Risk(95% CI)
1.28 (1.06 – 1.56) 1.34 (1.03 – 1.74) 1.05 (0.94 – 1.17)
Adverse Outcome for Higher Target Group All-cause mortality All-cause mortality Stroke
Hazard Ratio or Relative Risk (95% CI)
1.27 (1.04 – 1.54) 1.48 (0.97 – 2.27) 1.92 (1.38 – 2.68)
Patients with Chronic Kidney Disease Not on DialysisOMONTYS is not indicated and is not recommended for the treatment of anemia in patients with CKD who are not on dialysis.A higher percentage of patients (22%) who received OMONTYS experienced a composite cardiovascular safety endpoint event compared to 17% who received darbepoetin alfa in two randomized, active-controlled, open-label, multi-center trials of 983 patients with anemia due to CKD who were not on dialysis. The trials had a pre-specified, prospective analysis of a composite safety endpoint consisting of death, myocardial infarction, stroke, or serious adverse events of congestive heart failure, unstable angina or arrhythmia (hazard ratio 1.32, 95% CI: 0.97, 1.81).Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence in Patients with Cancer receiving ESAsOMONTYS is not indicated and is not recommended for reduction of RBC transfusions in patients receiving treatment for cancer and whose anemia is not due to CKD because ESAs have shown harm in some settings and the benefit-risk factors for OMONTYS in this setting have not been evaluated.The safety and efficacy of OMONTYS have not been established for use in patients with anemia due to cancer chemotherapy. Results from clinical trials of ESAs in patients with anemia due to cancer therapy showed decreased locoregional control, progression-free survival and/or decreased overall survival. The findings were observed in clinical trials of other ESAs administered to patients with: breast cancer receiving chemotherapy, advanced head and neck cancer receiving radiation therapy, lymphoid malignancy, cervical cancer, non-small cell lung cancer, and with various malignancies who were not receiving chemotherapy or radiotherapy.HypertensionOMONTYS is contraindicated in patients with uncontrolled hypertension.Appropriately control hypertension prior to initiation of and during treatment with OMONTYS. Reduce or withhold OMONTYS if blood pressure becomes difficult to control. Advise patients of the importance of compliance with antihypertensive therapy and dietary restrictions.Lack or Loss of Response to OMONTYSFor lack or loss of hemoglobin response to OMONTYS, initiate a search for causative factors (e.g., iron deficiency, infection, inflammation, bleeding). If typical causes of lack or loss of hemoglobin response are excluded, evaluate the patient for the presence of antibodies to peginesatide. In the absence of antibodies to peginesatide, follow dosing recommendations for management of patients with an insufficient hemoglobin response to OMONTYS therapy.Contact Affymax, Inc. (1-855-466-6689) to perform assays for binding and neutralizing antibodies.Dialysis ManagementPatients may require adjustments in their dialysis prescriptions after initiation of OMONTYS. Patients receiving OMONTYS may require increased anticoagulation with heparin to prevent clotting of the extracorporeal circuit during hemodialysis.Laboratory MonitoringEvaluate transferrin saturation and serum ferritin prior to and during OMONTYS treatment. Administer supplemental iron therapy when serum ferritin is less than 100 mcg/L or when serum transferrin saturation is less than 20%. The majority of patients with CKD will require supplemental iron during the course

NATIONAL HARBOR, Md.—Dialysis patient underreporting of noncompli-ance with phosphate binder therapy may contribute to poor phosphorus control, investigators reported at the National Kidney Foundation 2012 Spring Clinical Meetings. Nischala Dhanekula, MD, and collaborators at
Unity Health System in Rochester, N.Y., interviewed 60 adult dialysis patients with uncontrolled phosphorus levels (mean levels of 5.5 mg/dL or above) using a questionnaire. They compared these patients with a control group of 40 dialysis patients with mean phosphorus levels below 5.5 mg/dL.
Results showed that 25.4% of the uncontrolled patients reported that they missed taking their binders on a daily basis, which was a signifi cantly greater percentage than the 2.5% observed in the control group. However, pharmacy records indicated that 41.7% of the uncontrolled patients were not fi lling
their prescriptions regularly, “indicating that about 16% of this group under-reported their noncompliance,” the researchers stated.
In addition, the study showed that patient knowledge about high phos-phorus diets did not differ signifi cant between the groups. Interestingly, the investigators noted, the uncontrolled patients were better able to identify the health risks associated with high phosphorus.
Dr. Dhanekula’s group concluded that drug dispensing information from pharmacies may play a role in control-ling hyperphosphatemia. ■
Phosphate Binder Noncompliance Underreported
Renal US Use Unchanged in CKD PatientsNATIONAL HARBOR, Md.—Renal ultrasound use for patients with chronic kidney disease (CKD) has not changed signifi cantly since the release of guide-lines in 2002 recommending imaging studies for patients with CKD or who are at risk for it as a result of urinary stones, infections, and other factors, according to a study of U.S. veterans presented at the National Kidney Foun-dation 2012 Spring Clinical Meetings.
Nadia Chaudhri, MD, and Stephen Seliger, MD, of the University of Mary-land Medical Center and Baltimore VA Medical Center in Baltimore, studied 127,155 active outpatients with CKD who had renal ultrasound studies performed from October 1, 2002 to September 30, 2006. This group represented 12% of veterans with CKD receiving care during that period. The researchers observed no signifi cant change in renal ultrasound usage during the study period.
Patients with an estimated glo -merular fi ltration rate (eGFR) of 15-30 mL/min/1.73 m2 had the highest rate of renal ultrasound studies. Com-pared with patients who had an eGFR of 45-60, those with an eGFR of 30-45 were 41% more likely to have had a renal ultrasound. Those with an eGFR of 15-30 and below 15 were 19% and 88% less likely to have had a renal ultrasound. ■
of ESA therapy. Following initiation of therapy and after each dose adjustment, monitor hemoglobin every 2 weeks until the hemoglobin is stable and sufficient to minimize the need for RBC transfusion. Thereafter, hemoglobin should be monitored at least monthly provided hemoglobin levels remain stable.ADVERSE REACTIONSThe following serious adverse reactions observed during clinical trials with OMONTYS are discussed in greater detail in other sections of the labeling:• Increased Mortality, Myocardial Infarction, Stroke, and Thromboembolism
[see Warnings and Precautions]• Hypertension [see Warnings and Precautions]Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of OMONTYS cannot be directly compared to rates in the clinical trials of other drugs and may not reflect the rates observed in practice.Patients with Chronic Kidney DiseaseAdverse reactions were determined based on pooled data from two active controlled studies of 1066 dialysis patients treated with OMONTYS and542 treated with epoetin, including 938 exposed for at least 6 months and825 exposed for greater than one year to OMONTYS. The population for OMONTYS was 20 to 93 years of age, 58.5% male, and the percentages of Caucasian, Black (including African Americans), and Asian patients were 57.9%, 37.4%, and 3.1%, respectively. The median weight adjusted dose of OMONTYS was 0.07mg/kg and 113 U/week/kg of epoetin.Table 3 summarizes the most frequent adverse reactions (≥ 10%) in dialysis patients treated with OMONTYS.
Table 3 Adverse Reactions Occurring in ≥10% of Dialysis Patients treated with OMONTYS
Adverse Reactions
Dialysis Patients Treated with OMONTYS(N = 1066)
Dialysis Patients Treated with
Epoetin(N = 542)
Gastrointestinal DisordersDiarrhea 18.4% 15.9%Nausea 17.4% 19.6%Vomiting 15.3% 13.3%
Respiratory, Thoracic and Mediastinal DisordersDyspnea 18.4% 19.4%Cough 15.9% 16.6%
Injury, Poisoning and Procedural ComplicationsArteriovenous FistulaSite Complication 16.1% 16.6%
Procedural Hypotension 10.9% 12.5%Nervous System Disorders
Headache 15.4% 15.9%Musculoskeletal and Connective Tissue Disorders
Muscle Spasms 15.3% 17.2%Pain in Extremity 10.9% 12.7%Back Pain 10.9% 11.3%Arthralgia 10.7% 9.8%
Vascular DisordersHypotension 14.2% 14.6%Hypertension 13.2% 11.4%
General Disorders and Administration Site ConditionsPyrexia 12.2% 14.0%
Metabolism and Nutrition DisordersHyperkalemia 11.4% 11.8%
Infections and InfestationsUpper Respiratory Tract Infection 11.0% 12.4%
Seizures have occurred in patients participating in OMONTYS clinical studies. During the first several months following initiation of OMONTYS, blood pressure and the presence of premonitory neurologic symptoms should be monitored closely.Advise patients to contact their healthcare practitioner for new-onset seizures, premonitory symptoms, or change in seizure frequency.Al lergic react ions have been reported in pat ients treated with OMONTYS. Discontinue OMONTYS and administer appropriate therapy if a serious allergic, anaphylactic or infusion-related reaction occurs.ImmunogenicityOf the 2357 patients tested, 29 (1.2%) had detectable levels of peginesatide-specific binding antibodies. There was a higher incidence of peginesatide-specific
binding antibodies in patients dosed subcutaneously (1.9%) as compared to those dosed intravenously (0.7%). Peginesatide neutralizing antibodies were detected in vitro using a cell-based functional assay in 21 of these patients (0.9%). In approximately half of all antibody-positive patients, the presence of antibodies was associated with declining hemoglobin levels, the requirement for increased doses of OMONTYS to maintain hemoglobin levels, and/or transfusion for anemia of CKD. No cases of pure red cell aplasia (PRCA) developed in patients receiving OMONTYS during clinical trials.DRUG INTERACTIONSNo formal drug/drug interaction studies have been performed. Peginesatide does not bind to serum albumin or lipoproteins as demonstrated in in vitro protein binding studies in rat, monkey and human sera. In vitro studies conducted with human hepatocytes or microsomes have shown no potential for peginesatide to induce or inhibit CYP450 enzymes.USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category CThere are no adequate and well-controlled studies in pregnant women. Peginesatide was teratogenic and caused embryofetal lethality when administered to pregnant animals at doses and/or exposures that resulted in polycythemia. OMONTYS should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.Administration of peginesatide by intravenous injection to rats and rabbits during organogenesis was associated with embryofetal toxicity and malformations. Dosing was every third day in rats for a total of 5 doses and every fifth day in rabbits for a total of 3 doses (0.01 to 50 mg/kg/dose). In rats and rabbits, adverse embryofetal effects included reduced fetal weight, increased resorption, embryofetal lethality, cleft palate (rats only), sternum anomalies, unossification of sternebrae and metatarsals, and reduced ossification of some bones. Embryofetal toxicity was evident in rats at peginesatide doses of ≥ 1 mg/kg and the malformations (cleft palate and sternoschisis, and variations in blood vessels) were mostly evident at doses of ≥ 10 mg/kg. The dose of 1 mg/kg results in exposures (AUC) comparable to those in humans after intravenous administration at a dose of 0.35 mg/kg in patients on dialysis. In a separate embryofetal developmental study in rats, reduced fetal weight and reduced ossification were seen at a lower dose of 0.25 mg/kg. Reduced fetal weight and delayed ossification in rabbits were observed at ≥ 0.5 mg/kg/dose of peginesatide. In a separate embryofetal developmental study in rabbits, adverse findings were observed at lower doses and included increased incidence of fused sternebrae at 0.25 mg/kg. The effects in rabbits were observed at doses lower (5% - 50%) than the dose of 0.35 mg/kg in patients.Nursing MothersIt is not known whether peginesatide is excreted in human milk. Because many drugs are excreted into human milk, caution should be exercised when OMONTYS is administered to a nursing woman.Pediatric UseThe safety and efficacy of OMONTYS in pediatric patients have notbeen established.Geriatric UseOf the total number of dialysis patients in Phase 3 clinical studies of OMONTYS, 32.5% were age 65 and over, while 13% were age 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects.OVERDOSAGEOMONTYS overdosage can elevate hemoglobin levels above the desired level, which should be managed with discontinuation or reduction of OMONTYS dosage and/or with phlebotomy, as clinically indicated. Cases of severe hypertension have been observed following overdose with ESAs [see Warnings and Precautions].PATIENT COUNSELING INFORMATIONSee FDA-approved patient labeling (Medication Guide).
Marketed by:Affymax, Inc.Palo Alto, CA 94304
Distributed and Marketed by:Takeda Pharmaceuticals America, Inc.Deerfield, IL 60015
For more detailed information, see the full prescribing information for OMONTYS at www.omontys.com or contact Takeda Pharmaceuticals America, Inc.
OMONTYS is a trademark of Affymax, Inc. registered in the U.S. Patent and Trademark Office and used under license by Takeda Pharmaceuticals America, Inc.
All other trademarks are the property of their respective owners.
©2012 Takeda Pharmaceuticals America, Inc.
March 2012PEG096 R1 L-DSG-0312-1
03-12-00027-A.; DSG-00057.
www.renalandurologynews.com JUNE 2012 Renal & Urology News 13

14 Renal & Urology News JUNE 2012 www.renalandurologynews.com
In a recent editorial (Clin J Am Soc Nephrol 2012;7:354-357), you contend that physicians should tailor the use of ESAs within the context of the patient’s perceived quality of life. What experiences brought you to this conclusion?Dr. Kliger: Several studies of patients with CKD and those on dialysis have shown the dangers of treating anemia of CKD to goal hemoglobin (Hb) of 13 g/dL or higher. For decades, we have prescribed ESAs to achieve goal Hb levels, as if the Hb level itself is the important outcome. However, our patients tell us a different story. For some, the Hb level appears to make no difference to their health, as long as they do not have profound anemia. For others, symptoms develop and change lives at different Hb levels. Since each of our patients is different, a single goal Hb level does not work, particularly when we know that there is potential harm to set goal Hb at 13 or higher, and we do not know if that harm extends to goals below 13.
Do you endorse this QOL practice for specifi c subgroups—for example, in those patients who are more likely to succumb to end-stage renal disease than to the cardiovascular side effects of ESAs—or would you like to see it applied across the spectrum of all CKD patients with anemia?Dr. Kliger: I believe the practice of indi-vidualizing anemia treatment should be done for all patients. For each patient,
we must consider the balance between the benefi ts and the risks of ESA treat-ment. That balance will not be the same for all. For example, a minority of patients with ischemic heart disease develop increased angina and other symptoms when they become more anemic. For these patients, the benefi ts of ESAs, iron, or blood transfusions likely outweigh the risks, even if their achieved Hb levels to eliminate angina are in the range of 13 g/dL. For other patients, anemia appears to have no effect on their health, even when Hb levels are below 10 g/dL. For these patients, the risks of treating anemia outweigh the benefi ts, and ESAs should not be used.
What do you think of the FDA’s modifi ed dosing recommendation to consider starting ESA treatment when Hb level is less than 10 g/dL—without defi ning how far below 10 g/dL is appropriate for initiation and without recommending a goal of 10 g/dL or higher (www.fda.gov/Drugs/DrugSafety/ucm259639.htm).Dr. Kliger: Since several studies in recent years have shown increased incidence of complications—some life-threat-ening—associated with using ESAs to goal Hb at 13 g/dL or higher, the FDA has responded appropriately to change the label for ESA use to refl ect these dangers. The challenge is that there are no studies that show what the danger is when Hb goals are less than 13 g/dL. Is it safe to set goal Hb at 10 or 9 g/dL
or higher? We do not know. If a single goal Hb level is not appro-
priate for all patients, I think it is wiser to craft individualized therapy rather than seeking to fi nd the single goal best for all. This does mean that each patient and his or her doctor must consider the relative risks and benefi ts of treatment to the best of their ability, and not sim-ply depend on the FDA “black box” warning to prescribe a dose of ESA.
Another editorial in the same issue of CJASN (pp. 348-353) argued that the FDA should have been even more specifi c about ESA use. Instead of advising nephrologists to individualize dosing and reduce it when Hb exceeds 11 g/dL in dialysis patients and 10 g/dL in nondialysis-dependent CKD patients, should the agency have recommended targeting Hb ranges of 9 to 11 g/dL in dialysis patients and 9 to 10 g/dL in nondialysis patients. Is there any benefi t to giving target ranges, or would such recommendations restrict the inclination to customize treatment?Dr. Kliger: In the absence of clear studies showing the risks of targeting Hb at 9 or 10 g/dL, I think the FDA becomes a fortune teller rather than a re -spon sible scientific body should
they recommend targeting Hb levels to 9 or 10. I believe the FDA should say we have insufficient data to determine the risk of targeting Hb less than 13, and direct patients and their physicians to consider the risks and benefi ts as best the data allow on an individual basis.
How can nephrologists reconcile the cardiovascular risks of ESAs with following your approachif it means bringing the patient into a high hemoglobin range, perhaps above 11 g/dL or even above 13 g/dL?Dr. Kliger: The art of medicine is the skill of reconciling the risks and bene -fi ts of any treatment when the data are incomplete and those risks are, in part, unknown. The dilemma posed by ESA treatment urges us all to step back and examine carefully the model of care we have used. We have treated anemia to goal Hb levels, with little evidence that this model improves patients’ health. We believe that indi-vidualizing anemia care by using patient-reported outcomes, within the context of monitoring their Hb levels, may prove to be a more effective model of care.
Do you have any experiences to share about patients you have maintained at particularly high or particularly low hemoglobin levels through ESA use?Dr. Kliger: I cared for a 50-year-old man with stage IV CKD whose life was affected profoundly whenever his Hb level fell below 12 g/dL. In truth, I did not need to get a laboratory test to measure his Hb level; he came to the offi ce and said, “I feel fi ne,” or at other times said, “I can’t walk up stairs,” or, “I get breathless walking more than a block, and I know my anemia needs better treatment.” At these times, his Hb level was always less than 12.
When we treated his anemia based on his symptoms, he did well. I discussed with him the risks of ESA treatment to higher Hb goals, and he understood those risks, but for him the ESA treat-ments were life-changing. He was anx-ious and angry when we discussed the possibility that I might not be able to treat him with ESAs to an arbitrary Hb level. He felt it was his decision to determine the risks and receive the best treatment for him. ■
With ESAs, Let the Patient Be Your GuideWhen using erythropoiesis-stimulating
agents (ESAs) to correct anemia in
patients with chronic kidney disease
(CKD), focus less on hitting a given hemoglobin target
and more on improving patient-perceived quality of
life (QOL) in such areas as fatigue, weakness, and
shortness of breath, advises Alan S. Kliger, MD, Chief Medical Offi cer and Chief Quality Offi cer for the
Saint Raphael Healthcare System in New Haven, Conn.
Dr. Kliger spoke to Renal & Urology News senior editor
Delicia Honen Yard on the subject.
We should individualize anemia treatment for all patients.
—Alan S. Kliger, MD
QA&

www.renalandurologynews.com JUNE 2012 Renal & Urology News 15
BY GERALD B. APPEL, MD, AND ALICE SUE APPEL, PHD
Renal involvement is a frequent and potentially serious mani-festation of systemic lupus erythematosus (SLE).1-4 It
contributes to both morbidity and mortality, in part directly and in part through complications of therapy. There has been recent progress in treat-ing patients with SLE and renal involve-ment. This treatment is based on the use of a uniform histologic classifi cation system (the International Society of Nephrology [ISN] classifi cation), better understanding of the clinical course of different patterns of renal involvement, and through the use of information obtained from large randomized trials to treat lupus nephropathy.
LN epidemiology and pathogenesis
While the incidence of SLE and lupus nephritis (LN) varies considerably among studies,5 in general, females outnumber males approximately 10:1, and the peak average age is 15-45 years. Renal disease may be more severe in
children and males and affects 25%-50% of SLE patients at onset and up to 60% during their disease course. LN is more common and more severe in minorities— including African Americans and Hispanic Americans—than in Caucasians, and in those with lower socioeconomic status regardless of racial background.
Genetics and environmental, and hormonal factors all play a role in the predilection to lupus and perhaps to LN.3,5-7 A number of spontaneous and inducible models of SLE and LN have been well studied in mice, including the NZB B/W F1 hybrid, the BXSB/yaa, and the MRL/lpr mod-els.3,6 Autoimmunity is important in the pathogenesis of SLE,6-9 the dis-ease process, including a breakdown in self tolerance, polyclonal hyperac-tivity of B cells along with defective auto-regulation of T cells that leads to autoantibody production, and deposi-tion of immune deposits with a subse-quent infl ammatory responses.3,6-9 The failure of apoptotic mechanisms to delete or silence autoreactive cells (tol-erance) may allow clonal expansion of such cells later in life, leading to auto-reactive cells and auto-antibody production. The deposition of circu-
CME FEATURE
An Update on the Management of Lupus NephritisApproximately 30%-50% of SLE patients have clinically evident renal disease at presentation, but renal involvement occurs in up to 60% of patients overall.
Release Date: June 2012Expiration Date: June 2013Estimated time to complete the educational activity: 1 hour
This activity is jointly sponsored by Medical Education Resources and Haymarket Media, Inc.
STATEMENT OF NEED: Renal involvement is a frequent and potential serious manifestation of system lupus erythematosus (SLE). Studies in recent years have led to improved understanding of the pathogenesis and disease course of SLE-related lupus nephritis as well as new approaches to treating the condition. Clinicians involved in the care of patients with SLE-related lupus nephritis need to be aware of these advancements.
TARGET AUDIENCE: This activity has been designed to meet the educational needs of nephrologists and others clinicians involved in the care of patients with lupus nephritis.
EDUCATIONAL OBJECTIVES: After completing the activity, the participant should be better able to:
Describe the clinical course of different patterns of renal involvement in patients with SLE.• Distinguish among the different lupus nephritis classes.• Choose therapies appropriate to lupus nephritis class.•
ACCREDITATION STATEMENT: This activity has been planned and implemented in accor-dance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Medical Education Resources (MER) and Haymarket Media, Inc. MER is accredited by the ACCME to provide continuing medical education for physicians.
CREDIT DESIGNATION: Medical Education Resources designates this enduring material for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit com-mensurate with the extent of their participation in the activity.
DISCLOSURE OF CONFLICTS OF INTEREST: Medical Education Resources ensures balance, independence, objectivity, and scientifi c rigor in all its educational programs. In accordance with this policy, MER identifi es confl icts of interest with its instructors, content managers, and other individuals who are in a position to control the content of an activity. Confl icts are resolved by MER to ensure all scientifi c research referred to, reported, or used in a CME activity conforms to the generally accepted standards of experimental design, data collection, and analysis. MER is committed to providing its learners with high-quality CME activities that promote improvements or quality in health care and not a commercial interest.
The faculty reported the following fi nancial relationships with commercial interests whose products or services may be mentioned in this CME activity:
Name of Faculty Reported Financial Relationship• Gerard B. Appel, MD
• Alice Sue Appel, PhD
Grants/Research Support: Aspreva-Vifor, Genentech, Centacor. Consultant: Genentech, Centacor, Amgen, Pfi zerSpeakers’ Bureau: Genentech, Merck, Takeda, GenzymeRoyalty: Up-To-Date
No fi nancial relationships to disclose
The content managers, Jody A. Charnow and Marina Galanakis, of Haymarket Media, Inc., and Victoria C. Smith, MD, of Medical Education Resources, have disclosed that they have no relevant fi nancial relationships or confl icts of interest.
METHOD OF PARTICIPATION: There are no fees for participating in and receiving CME credit for this activity. During the period June 2012 through June 2013, participants must: 1) read the learning objectives and faculty disclosures, 2) study the educational activity, 3) complete the posttest and submit it online. Physicians may register at www.myCME.com/renalandurologynews, and 4) complete the evaluation form online.
A statement of credit will be issued only upon receipt of a completed activity evaluation form and a completed post-test with a score of 70% or better.
Gerald B. Appel, MD, is Professor of Clinical Medicine at Columbia University College of Physicians & Surgeons,
and Director of Clinical Nephrology at the Glomerular Institute, a part of Columbia University Medical Center in New York City.
Alice Sue Appel, PhD, is an Adjunct Associate Research Scientist in the Division of Nephrology
at Columbia University College of Physicians & Surgeons in New York City.

16 Renal & Urology News JUNE 2012 www.renalandurologynews.com
lating immune complexes, the in situ formation of others and the activa-tion of complement are major com-ponents of glomerular involvement in LN. Although most investigators believe mesangial and subendothelial immune complex deposits are derived from deposition of circulating immune complexes while subepithelial com-plexes found in membranous LN are often formed in situ, many factors infl uence the localization of glomerular immune complexes. These include the size, charge, and avidity of the immune complexes, as well as the clearing ability by the mesangium and local hemo-dynamics.3,4 The glomerular localiza-tion of immune complexes activates complement-mediated damage, pro-coagulant factors, leukocyte chemoat-traction, and release of cytokines associated with cellular proliferation and matrix formation. In some patients, vascular and tubulointerstitial damage are prominent.
Clinical manifestations
Both the course of SLE and LN is char-acterized by episodes of illness (fl ares) followed by episodes of relative quies-cence (remissions). From 30%-50% of SLE patients have clinically evident renal disease at presentation,1-4 but renal involvement occurs in as many as 60% of patients during the disease course. LN is manifested by proteinuria, microhe-maturia with dysmorphic erythrocytes, erythrocyte casts, and hypertension. In some, development of nephritic syn-drome is associated with proliferative glomerulonephritis and a decline in glomerular fi ltration rate (GFR). Other patients, including those with prolif-erative disease and some with membra-nous lupus nephropathy, develop the nephrotic syndrome. Clinical features generally correlate well with histologic fi ndings on renal biopsy.
Pathology
Glomerular disease in LN is a dynamic process with the potential for glom-erular lesions to transform from one pattern to another. 1-4 Adjacent glom-eruli may show different degrees of involvement. The widely accepted 2004 ISN/Renal Pathology Society (RPS) Classifi cation of LN is highly reproducible, and predicts disease course and outcome.10 (Table 1). ISN
Class I denotes normal glomeruli by light microscopy but with mesan -gial immune deposits by immuno-fl uorescence and electron microsco-py. ISN CLASS II, which is mesan-gial proliferative LN, is characterized by mesangial hypercellularity dem-onstrated by LM, with greater than three mesangial cells in areas away from the vascular pole by LM as well as mesangial immune deposits. ISN CLASS III is focal LN, defined as focal segmental and/or global endo -capillary and/or extracapillary glom-erulonephritis affecting less than 50% of the glomeruli. ISN Class IV is diffuse LN. It is characterized by segmental and/or global endocapil-lary and/or extracapillary glomeru-lonephritis affecting more than 50% of glomeruli. Both Class III and IV have subendothelial immune deposits. LN Class IV is subdivided into dif-fuse segmental versus diffuse global proliferation, and both Class III and IV may have active A (proliferative), and inactive chronic C (sclerosing) lesions. ISN Class V is membranous LN defi ned by subepithelial immune depos-its. SLE Patients may have combined lesions noted as Class III + V or IV + V. Class VI is defi ned as advanced scle-rosing LN with more than 90% global glomerular sclerosis.
In LN, IgG staining on IF is almost always present and C1q is particularly common. “Full house staining” (the
presence of IgG, IgA, IgM, and C3 and C1q – three of one kind and two of the other) is very suggestive of LN, as is IF deposition along the tubular basement membranes and the glomerular base-ment membranes. Likewise by EM, tubulo-reticular inclusions (TRI)—24 nm interanastomosing tubular struc-tures in the glomerular endothelial cells—are commonly found only in biopsies of patients with LN or in those with HIV infection.
With treatment or over time, serial biopsies often show transformation from one histologic class to another.4 In general, clinical renal manifesta-tions correlate well with ISN biopsy class. Nephrotic patients with mem-branous lupus and lupus patients with antiphospholipid antibodies are par-ticularly predisposed to thrombotic complications such as deep vein throm-bophlebitis, renal vein thrombosis, and pulmonary emboli.20
Treatment protocol
Patients with ISN Classes I and II need no attention directed at their renal lesions. Some patients with very mild class III lesions can be treated with a short course of increased corticoster-oids, which typically results in a good clinical and histologic response. For most patients with active prolifera-tive LN, Class III and IV, it is useful to divide treatment into an induction
phase and a maintenance phase. The induction phase typically is used for uncontrolled, active renal disease that at times may be acutely life- or organ-threatening, whereas the maintenance phase focuses on the long-term man-agement of chronic, relatively indolent disease, where avoidance of the adverse effects of therapy and prevention of fl ares become very important.
Induction phase treatment of proliferative LN
Most clinicians initially treat active proliferative LN with high doses of corticosteroids in conjunction with other immunosuppressive medications. High dose oral regimens include start-ing doses of predisone or predniso-lone 1 mg/kg/day or 60 mg/day and/or “pulse” intravenous (IV) methyl-prednisolone infusions (0.5-1.0 g daily for one to three days followed by lower doses of oral corticosteroids.
Steroid doses have usually been tapered to 0.5mg/kg/day or less by the third month of treatment to avoid such adverse effects as cosmetic alterations, gastrointestinal ulceration, hyperten-sion, psychoses, and enhanced risk of infectious complications.
Cytotoxic agents in conjunction with corticosteroids have long been a mainstay of many induction regimens for the treatment of LN.11-14 While it remains uncertain whether oral therapy or IV pulses of cyclophosphamide is more effective,15 clearly IV therapy involves a lower cumulative dose with the likelihood of fewer side effects and problems with adherence. Through a series of trials at the National Institute of Health (NIH), IV monthly pulses of cyclophosphamide ( 0.5-1 g/m2) for six consecutive months followed by pulses every third month were established as an effective therapy that is supe-rior to corticosteroids in preventing renal failure.33 Subsequent studies have focused on achieving equal effi cacy but less long-term morbidity through use of shorter or modifi ed induction and maintenance regimens.13,14
A trial by the EuroLupus Group14 randomized 90 patients with diffuse or focal proliferative LN or membranous plus proliferative disease to receive either the standard six monthly pulses of cyclophosphamide (0.5-1 g/m2/month) followed by infusions every third month or to a shorter treatment course consist-
CME FEATURE
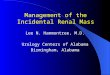
Micrograph of diffuse proliferative lupus nephritis showing increased mesangial matrix and mesangeal hypercellularity.
COUR
TESY
OF
DR. G
ERAL
D B.
APP
EL

www.renalandurologynews.com JUNE 2012 Renal & Urology News 17
ing of 500 mg of IV cyclophosphamide every two weeks for six doses (total dose 3g) and then switching to azathioprine maintenance therapy (2mg/kg/day). Both regimens were equally effective in achieving various renal and extra-renal outcomes. The shorter regimen had less toxicity with signifi cantly fewer severe 0and total infections. This trial was largely performed in Caucasians and may not be applicable to other popu-lations. Reports after fi ve and 10 years continued to fi nd no differences in the risk of renal failure between treatment groups15 and no differences in serum creatinine values and 24-hour urinary protein excretion at 10 years. The cumu-lative dose of cyclophosphamide using the older NIH regimen was almost double that of the newer low-dose regi-men. Although there are limitations to the Euro-Lupus data (small numbers of patients, mainly Caucasian subjects, and exclusion of patients with severe renal insuffi ciency), this regimen has largely replaced the older NIH regimen and is widely accepted as a fi rst-line induction therapy for severe LN.
Controlled trials, and subsequent meta-analyses, have also examined the role of mycophenolate mofetil (MMF) as a fi rst-line induction agent for severe LN 12-14,16 One Chinese study randomized 42 patients to receive either 12 months of oral MMF (2g/d for six months followed by 1 g daily for six months) or six months of oral cyclophosphamide (2.5 mg/kg/day)
followed by oral azathioprine (1.5 mg/kg/day) for six months,17 both along with concomitant corticosteroids. At 12 months, the number of complete or partial remissions and relapses was similar in both treatment arms, but with fewer infections and deaths in the MMF arm. Longer follow-up confi rmed these benefi ts.18 A second Chinese trial also compared treatment with pulse IV cyclophosphamide to MMF and found that MMF -treated patients had greater reductions in proteinuria and hematuria and improved histology on repeat biopsy.1
A U.S. induction trial including 140 patients mostly with proliferative lupus nephritis compared the results of six IV cyclophosphamide monthly pulses to oral MMF up to 3 g daily with a simi-lar tapering dose of corticosteroids.19 In both treatment arms, more than 50% of subjects were African American. At six months, complete remissions and complete and partial remission com-bined were signifi cantly more common in the MMF arm. Moreover, adverse effects were less severe with MMF, with no signifi cant differences at three years in the numbers of patients with renal failure, end-stage renal disease (ESRD), or mortality.
The Aspreva Lupus Management Study (ALMS), a 370-patient interna-tional multicenter trial of induction therapy with either MMF, 3g/day, or monthly IV cyclophosphamide showed equivalent complete and partial remis-
sions at six months as well as resolution or stability of all renal and extra-renal parameters in both study arms.20 In the small subgroup of patients with initial GFR less than 30mL/min/1.73 m2, there was no indication that MMF was less effective than cyclophosphamide.21 The adverse effects of each regimen were as expected, with diarrhea the most common adverse effect with MMF and nausea/vomiting and alopecia the most common adverse effects with cyclo-phosphamide therapy. Mortality in both treatment arms was similar, with only 14 deaths, mostly infection-related, out of the 370 patients. With the results of these two large randomized trials , MMF has become well accepted as a fi rst-line induction therapy for severe LN.
Other induction agents
Other agents studied as induction therapy for severe LN include aza-thioprine, cyclosporine, tacrolimus, plasmapheresis, IV gamma globulin, rituximab, and CTLA4IG , a co-stim-ulatory blocker. None has achieved the success of the EuroLupus or MMF regimens. Although a trial compar-ing azathioprine to cyclophosphamide found no difference in eventual out-come, there were more relapses and more doublings of serum creatinine values with azathioprine.22
Maintenance therapy for proliferative LN
For most patients with active LN, six months of modern effective therapy will improve markers of disease activity, including anti-DNA antibody levels, serum complement, GFR, and degree of hematuria and proteinuria. However, some proteinuria and urinary sediment abnormalities are often still present at this time. Regimens of maintenance therapy have been devised to avoid relapses and fl ares of disease activity. Although low-dose daily or alternate day corticosteroids (equivalent of 5-10 mg/day prednisone) are commonly used as part of most maintenance regimens, there are no controlled studies to verify their necessity. Both controlled trials and meta-analyses clearly document the important role of continuing immu-nosuppressive medications during the maintenance phase of LN therapy.
Although both oral and IV cyclophos-phamide have been effectively used
for induction therapy of LN, their use should be limited to three to six months to avoid toxic side effects (e.g., alopecia, bladder toxicity, infertility, increased risk of long-term neoplasms). A study of 59 patients with severe LN who responded to six to eight monthly pulses of IV cyclophosphamide as induction therapy clearly showed the superiority of main-tenance regimens with either oral MMF or oral azathioprine compared with IV cyclophosphamide administered every third month.13 Azathioprine and MMF both proved superior at maintaining remissions and preventing mortality or ESRD, with fewer adverse effects, including fewer days of hospitalization, fewer episodes of amenorrhea, and fewer severe infections. Two more recent trials compared these two oral agents in the maintenance phase of severe LN. The ALMS maintenance trial looked at 227 patients who had responded to a regi-men of either six months of oral MMF or to IV monthly cyclophosphamide as induction therapy for severe LN.23 MMF maintenance (1g twice daily) proved superior to that with azathio-prine maintenance (2 mg/kg/day). At three years, MMF proved superior to azathioprine in terms of total renal end-points, relapse rate, doubling of serum creatinine, ESRD, and requirement for new additional immunosuppres-sive agents, regardless of which initial therapy the patients received, their racial background, or in what country they were treated. In the MAINTAIN Nephritis Trial, patients starting with six months of the Euro-Lupus regi-men of IV cyclophosphamide and steroids were randomized to MMF or azathioprine for four years.24 Although neither drug proved statistically supe-rior, there were fewer relapses with the MMF in this smaller, largely Caucasian population. In both studies, researchers observed excellent patient and renal survival rates, supporting the longer use of maintenance immunosuppres-sive drugs. There are only limited data on the use of other immunosuppressive drugs such as cyclosporine and tacroli-mus as maintenance agents in LN.25,26 Likewise, repeated dosing of rituximab either every six months or when the CD19-20 B cell count rises has been used in a number of patients.
A number of adjunctive agents have proved helpful in treating LN patients, including renoprotective measures such as blockade of the renin angiotensin
CME FEATURE
Table 1. Classifi cation of Glomerulonephritis in Systemic Lupus Erythematosus
Class Defi nition
IMinimal mesangial LN• Normal glomeruli by LM, but mesangial immune deposits by IF•
IIMesangial proliferative LN• Mesangial hypercellularity with mesangial immune deposits.•
III
Focal LN • III (A): Purely active lesions: focal proliferative LN• III (A/C): Active and chronic lesions: focal proliferative and sclerosing LN• III (C): Chronic inactive with glomerular scars: focal sclerosing LN•
IV
Diffuse LN • IV-S (A) or IV-G (A): Purely active lesions: diffuse segmental (S) or•
global (G) proliferative LNIV-S (A/C) or IV-G (A/C): Active and chronic lesions: diffuse segmental •
or global proliferative and sclerosing LNIV-S (C) or IV-G (C): inactive with glomerular scars: diffuse segmental •
or global sclerosing LN
V Membranous LN•
VIAdvanced sclerosing LN• ≥• 90% of glomeruli globally sclerosed without residual activity

18 Renal & Urology News JUNE 2012 www.renalandurologynews.com
system in proteinuric patients, optimal blood pressure control, and the use of statins for both their lipid lowering and pleiotropic effects. Use of antimalarials may help with extrarenal symptoms, but there are only limited data on their effect in renal involvement.
Measures to prevent cardiovascular disease and future coagulation events in patients who are antiphospholipid posi-tive with a previous clotting event are also recommended. As osteoporosis and avascular necrosis of bone have become important long-term health issues for many LN patients, it is important to minimize the use of corticosteroids and encourage the use of vitamin D and calcium supplements along with other agents to reduce bone loss.
Membranous lupus nephropathy
Patients with membranous lupus and subnephrotic proteinuria do extremely well regardless of treatment. There is no consensus on management with immu-nosuppressive agents. In membranous LN patients with nephrotic syndrome, both monthly pulse IV cyclophosph-amide and oral cyclosporine have prov-en superior to oral prednisone therapy in inducing complete and partial remis-sions.26 In the two large recent trials of MMF versus IV cyclophophamide induction in LN, 84 of the 510 patients had pure membranous lupus nephropa-thy.27 Both drugs proved equivalent in inducing partial and complete remis-sions of the nephrotic syndrome. ■
REFERENCES
1. Bomback AS, Appel GB. Updates on the treatment of lupus nephritis. J Am Soc Nephrol 2010;21:2028-2035.
2. Appel GB, Jayne D. Lupus Nephritis. In: Johnson R, Floege J, Feehaly J, eds. Comprehensive Clinical Nephrology, 4th Edition. Philadelphia, Pa. Elsevier, 2010:308-321.
3. D’Agati V, Appel GB. Lupus Nephritis: Pathology and Pathogenesis. In: Wallace DJ and Hahn BH, eds. Dubois’ Lupus Erythematosus 7th Edition. Philadelphia, Pa. Lippincott Williams & Wilkins, 2007:1094-1111.
4. Appel GB, Radhakrishnan J, D’Agati V. Secondary Glomerular Diseases. In: Taal MW, Chertow GM, Marsden PA, Skorecki K, Yu ASL, Brenner BM, eds. The Kidney. 9th Edition, Philadelphia, Pa. Elsevier, 2011:1192-1202.
5. Rus V, Maury EE, Hochberg MC. The Epidemiology of Systemic Lupus Erythematosus. In: Wallace DJ and Hahn BH, eds. Dubois’ Lupus Erythematosus
7th Edition. Philadelphia. Lippincott Williams & Wilkins, 2007:34-45.
6. Harley JB, Alarcon-Riquelme ME, Criswell LA, et al. Genome-wide association scan in women with systemic lupus erythematosus identifi es susceptibil-ity variants in ITGAM, PXK, KIAA1542 and other loci. Nat Genet. 2008;40:204-210.
7. Appel GB. New and future therapies for lupus nephritis. Cleve Clin J Med 2012;79:134-140.
8. Clatworthy MR, Smith KGC. Systemic lupus erythe-matosus: Mechanism. In Mason J, Pusey C, ed. The Kidney in Systemic Autoimmune Disease. Amster-dam, the Netherlands. Elsevier, 2008:285-309.
9. Tsokos GC. Systemic lupus erythrematosus. N Eng J Med 2011;365:2110-2121.
10. Weening JJ, D’Agati VD, Schwartz MM, et al. The classifi cation of glomerulonephritis in systemic lupus nephritis revisited. Kidney Int 2004; 65:521-530.
11. Gourley MF, Austin HA 3rd, Scott D, et al. Meth-ylprednisolone and cyclophosphamide, alone or in combination, in patients with lupus nephritis. A randomized, controlled trial. Ann Intern Med 1996;125:549-557.
12. Illei GG, Austin HA, Crane M, et al.: Combination therapy with pulse cyclophosphamide plus pulse methylprednisolone improves long-term renal out-come without adding toxicity in patients with lupus nephritis. Ann Intern Med 2001;135:248-257.
13. Contreras G, Pardo V, Leclercq B, et al. Sequential therapies for proliferative lupus nephritis. N Engl J Med 2004;350: 971-980.
14. Houssiau FA, Vasconcelos C, D’Cruz D, et al.: Immunosuppressive therapy in lupus nephritis: the Euro-Lupus Nephritis Trial, a randomized trial of low-dose versus high-dose intravenous cyclophosph-amide. Arthritis Rheum 2002;46:2121-2131.
15. Houssiau FA, Vasconcelos C, D’Cruz D et al. The 10-year follow-up data of the Euro-Lupus Nephritis Trial comparing low-dose versus high-dose intravenous
cyclophosphamide. Ann Rheum Dis 2010;69:61-64. 16. Walsh M, James M, Jayne D, et al. Mycophenolate
mofetil for induction therapy of lupus nephritis: a systematic review and meta-analysis. Clin J Am Soc Nephrol 2007;2:968-975.
17. Chan TM, Li FK, Tang CS, et al.: Effi cacy of myco-phenolate mofetil in patients with diffuse proliferative lupus nephritis. Hong Kong-Guangzhou Nephrology Study Group. N Engl J Med 2000;343:1156-1162.
18. Chan TM, Tse KC, Tang CS, Mok MY, Li FK: Long-term study of mycophenolate mofetil as continuous induction and maintenance treatment for diffuse proliferative lupus nephritis. J Am Soc Nephrol 2005;16:1076-1084.
19. Ginzler EM, Dooley MA, Aranow C, et al. Mycophe-nolate mofetil or intravenous cyclophosphamide for lupus nephritis. N Engl J Med 2005;353:2219-2228.
20. Appel GB, Contreras G, Dooley MA, et al. Mycophe-nolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J Amer Soc Nephrol 2009;20:1103-1112.
21. Walsh M, Solomons N, Jayne D. Mycophenolate mofetil in patients with lupus nephritis and poor renal function: Results from a randomized controlled trial. Data presented at Renal Week 2008. Abstract SA-PO2953.
22. Grootscholten C, Ligtenberg G, Hagen EC et al. Aza-thioprine/methylprednisolone versus cyclophosph-amide in proliferative lupus nephritis. A randomized controlled trial. Kidney Int 2006;70:732-742.
23. Dooley MA, Jayne D, Ginzler EM, et al. Mycopheno-late versus azathioprine as maintenance therapy for lupus nephritis. N Engl J Med 2011;36:1886-1895.
24. Houssiau FA, D’Cruz D Sangles S, et al. Azathio-prine versus mycophenolate mofetil for long-term immunosuppression in lupus nephritis. Results from the MAINTAIN Nephritis Trial. Ann Rheum Dis 2010;69:2083-2089.
25. Moroni G, Doria A, Mosca M, et al. A randomized, pilot trial comparing cyclosporine and azathioprine for maintenance therapy in diffuse lupus nephritis over four years. Clin J Am Soc Nephrol 2006;1:925-932.
26. Austin H, Ilei GG, Braun MJ, Balow JE. Randomized controlled trial of prednisone, cyclophosphamide, and cyclosporine in lupus membranous nephropathy. J Am Soc Nephrol 2009;20:901-911.
27. Radhakrishnan J, Moutzouris DA, Ginzler E, et al. Mycophenolate mofetil and intravenous cyclophos-phamide are similar as induction therapy for class V lupus nephritis. Kidney Int 2010;77:152-160.
CME FEATURE
DISCLAIMER: The content and views presented in this educational activity are those of the authors and do not neces-sarily refl ect those of Medical Education Resources or Haymarket Media, Inc. The authors have disclosed if there is any discussion of published and/or investigational uses of agents that are not indicated by the FDA in their presenta-tions. The opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of Medical Education Resources, or Haymarket Media, Inc. Before prescribing any medicine, primary references and full prescribing information should be consulted. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications on dangers in use, review of any applicable manufacturer’s product informa-tion, and comparison with recommendations of other authorities. The information presented in this activity is not meant to serve as a guideline for patient management.
CME Post-testExpiration Date: June 2013Medical Education Resources designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Participants should claim only the credit commensurate with the extent of their participation in the activity. Physician post-tests must be completed and submitted online. Physicians may register at no charge at www.myCME.com/renalandurologynews. You must receive a score of 70% or better to receive credit.
1. In general, the incidence of systemic lupus erythematosus (SLE) and lupus nephritis (LN) is:
Higher in men than womena. Higher in women than menb. The same for both gendersc.
2. What proportion of SLE patients have clinically evident renal disease at presentation:
10%-20%a. 20%-30%b. 30%-50%c. None of the aboved.
3. SLE patients with LN in which ISN class(es) need attention directed at their renal lesions:
Class Ia. Class IIb. Class IIIc. Class IVd. All of the abovee. Both c and df.
4. High-dose oral regimens for the initial treatment of active proliferative LN may include:
Starting dose of prednisone or prednisolone 1 mg/kg/daya. Starting dose of prednisone or prednisolone 60 mg/dayb. Both a and bc. None of the aboved.
5. Which of the following agents have been studied as induction therapy for severe LN:
Azathioprinea. Cyclosporineb. Tacrolimusc. Plasmapheresisd. All of the abovee.
6. For inducing complete or partial remission in membranous LN patients with nephrotic syndrome, which of the following is true:
Monthly pulse intravenous (IV) cyclophosphamide is superior to a. oral prednisoneOral cyclosporine is superior to oral prednisoneb. Oral prednisone is superior to both IV cyclophosphamide and c. oral cyclospsorineBoth a and bd. None of the abovee.

BY J. STEPHEN JONES, MD, WENDY O’CONNELL, AND COURTNEY ELLIS, RN
T he federal Health Information Technology for Economic and Clinical Health Act (HITECH)
is the component of health care reform that provides federal incentive pay-ments to doctors and hospitals when they adopt electronic health records (EHRs) and demonstrate their use in ways that can improve quality, safety, and effectiveness of care. Incentive payments began in 2011 and will con-tinue at diminishing levels for up to six years, ending once the incentive pool is depleted. After that, penalties will be assessed for non-qualifi cation, resulting in reduced provider payments for services.
Defi ning ‘meaningful use’The term “meaningful use” implies that clinicians not simply use the EHR, but that it must play a meaningful role in care delivery. The Centers for Medicare and Medicaid Services devel-oped metrics that were designed to signify that the EHR is used to improve patient care. For year 1 (2011), qualify-
ing clinicians had to use e-prescribing to: 1) directly deliver at least 40% of prescriptions from the EHR to the patient’s chosen pharmacy, 2) print an after visit summary (AVS) docu-menting the diagnosis and care plan for more than 80% of patients, and 3) maintain an active problem list that must be reviewed or updated in 80% of ambulatory visits.
Despite external pressure, clinicians may delay adoption of EHRs if they perceive the meaningful use processes as contributing to decreased effi ciency for most encounters. However, the Glickman Urological and Kidney Institute adopted the EHR almost a
decade ago both for documentation and e-billing as part of an enterprise effort. As a result of this early adoption,
we were prepared to combine energies towards achieving the meaningful use qualifi cation for institute physicians.
New workfl ow: smart setsThe first step was to identify the measures and to build them into the workfl ow of the Epic EHR on an insti-tute basis. A clinical support analyst (CSA) was hired to educate, assist, and bridge the urologists and nephrologists into a combined program to have every staff member qualifi ed within the fi rst year. “Smart sets” were developed to facilitate documentation, diagnosis entry, and computerized physician order entry in one or two motions.
This allowed standardization where appropriate and decreased duplication of data entry. Finally, pharmacy data were entered and confi rmed for each patient by the employee staff prior to all visits.
The next step was to educate both nephrologists and urologists in build-ing the three meaningful use measures (e-prescribing, AVS, and problem list maintenance) into standard workfl ows. Early experience was challenging, as many physicians had diffi culty follow-ing all three, but starting months before the measures became offi cial allowed us to have most physicians qualifi ed as the program began in the fall of 2011. Monthly reports were supplied to all physicians letting them know how close they were to achieving meaningful use status. Stragglers received one-on-one assistance with the CSA until all were qualifi ed.
Lessons learnedAcross all three departments (Neph-rology, Urology, Regional Urology), a total of 98% of physicians quali-fi ed by the fi rst quarter of 2012.
One major lesson learned was that physicians were slowest to adopt e-prescribing, one of the common features made available in the decade of EHR adoption. But once physi-cians used it for just short spans of time, few considered returning to paper prescriptions based on the effi ciency, accuracy, and legibility of e-prescribing. Notably, most physicians perceived that patients would resist letting go of paper prescriptions, but fewer than 5% of patients requested written versions.
Paid incentives and outcomesEven more remarkable was the positive impact on the organization. Providers were awarded on average $16,498, and the institute expects a slightly higher amount in 2012. This success was mirrored across Cleveland Clinic. Notably, Cleveland Clinic employs only 0.35% of all eligible providers, but 7.7% of all qualifying funds in the United States went to Cleveland Clinic, demonstrating dedication to qualifi cation across the organization. Fully 12% of all qualifying urologists in the United States were from the Glickman Institute.
The major lesson was that infrastruc-ture was critical to this success. This took time and labor investment up front, but at this point all the steps in each encounter are quick and our prescribing process is incomparably improved, including the accuracy of medication reconciliation throughout the enterprise. As more measures are introduced, we will build on this infra-structure to further harness the evolving EHR, with the hope that it will be able to improve population outcomes as well as those for individuals. ■
The authors are affi liated with Cleve-land Clinic’s Glickman Urological and Kidney Institute.
On the Forefront Urologists and nephrologists working together: an emerging model of patient care
Urologists and Nephrologists Team Up to Adopt EHR ‘Meaningful Use’
Screenshot showing the single click required to prescribe tamsulosin. Physicians deter-mine beforehand the default settings for commonly used medications in their Preference Lists. For this test patient, the dose, number to be dispensed, and number of refi lls is automated, and the prescription automatically transmits as “normal”, meaning it goes directly to the patient’s personal pharmacy. All choices can be overridden, but for the overwhelming majority of medications these pre-sets save tremendous time and eliminate much of the risk for error.
On the webFor more on cutting-edge models of patient care,
please visit us at renalandurologynews.com/forefront
Few physicians considered returning to paper prescriptions based on the effi ciency, accuracy, and legibility of e-prescribing.
www.renalandurologynews.com JUNE 2012 Renal & Urology News 19

22 Renal & Urology News JUNE 2012 www.renalandurologynews.com
RECENT STUDY findings add to mounting evidence of the deleterious consequences of early dialysis initia-tion, prompting researchers to ques-tion this approach, especially among older patients.
Investigators documented a doubling of the withdrawal rate from 1.5 to 3.0 per 100 patient-years of dialysis in the Canadian Organ Replacement Registry (CORR) from 2001 and 2009. Each 10-year increase in age was associated with an 84% greater likelihood of with-drawal, and early-start dialysis is associ-ated with a 15% greater probability of withdrawal than late starts. Meanwhile, the researchers observed a sharp rise in the proportion of deaths due to with-drawal among deceased dialysis patients, from 7.9% in 2001 to 19.5% in 2009.
“More patients are starting dialysis early, especially elderly patients, with higher eGFRs [estimated glomerular fi ltration rates], and it is this same popu-lation that goes on to just withdraw,” said Amanda Ellwood, MD, who led the study while she was completing her nephrology fellowship at the University
of Western Ontario in London. “So the question is, should we be starting them on dialysis or should we be considering another approach, such as multidisci-plinary conservative management?”
Working under Louise Moist, MD, Associate Professor of Nephrology at the university, and in conjunction with other researchers, Dr. Ellwood examined CORR data from 2001-2009. They focused on patients who started dialysis in that period. For the study, the researchers defi ned early dialysis start as initiating dialysis at an estimated glomerular fi ltration (eGFR) of 10.5 mL/min/1.73 m2 or higher and late start as an eGFR below 10.5.
The 3,339 patients who withdrew from dialysis and the 42,842 who did not had divergent demographic and medical characteristics. For example, the mean age of those who stopped dialysis was 73.2 years compared with 63 years for those who remained on dialy-sis, with 51.5% and 26.9% of the two groups, respectively, aged 75 or older. Furthermore, 39.8% of the withdrawal subjects had early dialysis initiation com-
pared with 34.4% in the no-withdrawal group. The only statistically signifi cant similarities between the two groups were their rates of hypertension and diabetes, at about 80% and 45%, respectively.
Overall, the median time to withdrawal was 15.9 months and 15.6 months for patients aged 75 and older and those with early-start dialysis, respectively. The respective median times for patients with late-start dialysis and those younger than 75 years were 20.2 and 21.6 months.
Dr. Ellwood’s group found that the
factors most significantly associated with withdrawal were increased age, early versus late dialysis initiation, late versus early referral to a nephrologist, initiating dialysis from 2006-2009 rather than 2001-2005, and starting dialysis in Nova Scotia (compared with Ontario, the reference province).
Factors associated with not withdraw-ing from dialysis were being male, being black or native Indian rather than white, and starting dialysis in Alberta, British Columbia, or New Brunswick. ■
Early Dialysis Starts May Be UnwiseThis approach is associated with an increased likelihood of withdrawal from treatment, study fi nds
High Pre-Transplant iPTH Predicts Worse OutcomesRENAL TRANSPLANT recipients who have elevated pre-transplant levels of intact parathyroid hormone (iPTH) are at increased risk of post-transplant hypercalcemia and graft failure, according to new study fi ndings.
“The association of pre-transplant iPTH level with outcome is interesting and clearly suggests mineral metabolism is important in post-transplant outcome,” lead investigator John Gill, MD, told Renal & Urology News. “The mechanisms which underlie this association need fur-ther study.”
Dr. Gill, a transplant nephrologist at St. Paul’s Hospital in Vancouver, B.C., and his co-investigators made this dis-covery when gathering information about the increasingly common phenomena of hyperparathyroidism and hypercalce-mia in kidney transplant patients. The researchers reviewed information from 1,352 consecutive adults who received kidneys alone between January 2000 an
August 2007 in two of Canada’s largest transplant centers, St. Paul’s Hospital and the Toronto General Hospital.
A “striking” 40% of the patients had at least one episode of hypercalcemia—defi ned as albumin-corrected serum calci-um level of 2.6 mmol/L or greater—within
a year of transplantation. Furthermore, 162 patients (12%) had hypercalcemia throughout the fi rst post-transplant year. Hypercalcemia resolved within two years in 25% of patients with this condition, and it resolved within three and fi ve years post-transplant in 36% and 54%, respec-tively, of the affected cohort. Twenty-one
(13%) of hypercalcemic patients required surgical parathyroidectomy.
Patients with post-transplant hyper-calcemia experienced an average 1.81 mL/min/1.73 m2/year drop in esti-mated glomerular fi ltration rate, com-pared with a 0.22 mL/min/1.73 m2/year increase among those who did not develop post-op hypercalcemia.
Post-transplant hypercalcemia was significantly associated with age. Compared with individuals younger than 40 years, those aged 40-49, 50-59, and aged 60 and older had an 89%, 75%, and 114% increased risk of post-transplant hypercalcemia, respectively.
A pre-transplant iPTH level of 10.6-53 pmol/L was associated with a fourfold higher risk of hypercalcemia compared with a level below 10.6 pmol/L, whereas an iPTH level above 53 pmol/L was asso-ciated with an 11-fold higher risk.
Duration of dialysis prior to transplanta-tion was another factor associated with
post-transplant hypercalcemia. Compared with patients who were on dialysis for less than one year prior to transplanta-tion, those on pre-transplant dialysis for more than fi ve years had a 2.7 times increased risk.
Additionally, patients with pre-transplant calcium levels greater than 2.6 mmol/L had a 5.7 times increased risk of post-transplant hypercalcemia compared with patients who had normal serum calcium levels.
Post-transplant hypercalcemia was not associated with graft failure, but researchers observed an 80% higher probability of graft failure among patients with pre-transplant iPTH levels above 53 pmol/L compared with patients whose pre-transplant levels were below 10.6 pmol/L. The researchers could not determine whether post-transplant iPTH levels are associated with graft failures because these levels are not rou-tinely measured. ■
Study reveals increased risk of hypercalcemia and graft failure.
Rosemary Frei, MSc, provided news coverage of the Canadian Society of Nephrology’s 2012 meeting ■ CSN annual meeting, St. John’s, Newfoundland
Dialysis Withdrawal Factors
In a study, patients who started on dialysis early and those aged 75 and older had a shorter median time to dialysis withdrawal than those who started dialysis late and patients younger than 75.
Source: Ellwood A, et al. Data presented at the Canadian Society of Nephrology annual meeting, St. John’s, Newfoundland.
0 5 10 15 20 25
20.2 months
15.6 monthsEarly dialysis start (eGFR 10.5 or higher)
Late dialysis start (eGFR �10.5)
Age 75 and older
Younger than 75
15.9 months
Median time to dialysis withdrawal in months
21.6 months

www.renalandurologynews.com JUNE 2012 Renal & Urology News 23
OLDER PEOPLE who have cor-onary angiography and then experience acute kidney injury (AKI) are signifi -cantly less likely to receive cardiovascu-lar medications than their counterparts who do not develop AKI, a new study shows.
An analysis of Alberta residents over age 65 who received coronary angiography for an acute coronary syndrome between November 1, 2002 and March 31, 2008 demonstrated that those who developed AKI during their hospitalization were 23% less likely than those without AKI to receive an ACE inhibitor or angiotensin recep-tor blocker (ARB). They were also 22% less likely to receive anti-platelet medication, 19% less likely to receive a statin, and 15% less likely to be prescribed a beta-blocker.
The results are independent of base-line renal function and whether the patients had received the medications prior to hospitalization.
“A possible explanation for this could be concern on the part of clini-cians that use of the cardiovascular medications could affect renal function and worsen outcomes. So the patients
were substituted to other classes of medications—but were not switched back prior to discharge,” lead investi-gator Kelvin Leung, MD, a nephrology fellow at the University of Calgary, told Renal & Urology News.
Dr. Leung and other members of the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease and the Alberta Kidney Disease Network excluded from their database analysis individuals who were
on dialysis or who had received a kidney transplant. They included 5,991 patients who did not develop AKI and another 898 who did.
The team also determined that AKI patients had a significantly lower cumulative incidence of the use of statins, beta-blockers, ACE inhibitors/ARBs, and anti-platelet agents.
An analysis of cardiovascular-medication-naïve patients who developed AKI showed that they also were signifi cantly less likely than their medication-naïve non-AKI counter-parts to receive the potentially life-saving agents.
Additionally, the investigators found that the lower rates of heart medica-tion use among AKI patients generally was not related to the presence of dia-betes, heart failure, baseline estimated glomerular fi ltration rate, or overall medication use. The only exception was a signifi cantly decreased use of ACE inhibitors among patients with pre-existing heart failure who devel-oped AKI.
Dr. Leung said he and his co-inves-tigators are “unsure if this translates into an effect on mortality.” ■
AKI After Coronary AngiographyDeters Cardiovascular Drug Use
Kelvin Leung, MD
Risk of Serious Infections Greater with PDPATIENTS ON peritoneal dialysis (PD) are at 51% higher risk of being hospitalized for infections than those receiving hemodialysis (HD), new fi nd-ings suggest.
“Higher risk of infection-related hospitalization among peritoneal dialysis patients is mostly explained by dialysis-related infections, which are for the most part peritonitis,” said primary investigator Jean-Philippe Lafrance, MD, of the University of Montreal.
He and his colleagues analyzed data from the Quebec health care insur-ance plan, Quebec hospital discharge summary databases, and the Canadian Organ Replacement Register. They ana-lyzed information on all adults (except those who had already had a kidney transplant or fewer than three months’ of follow-up data) with information in
all three sets of databases who initiated chronic dialysis between January 2001 and December 2007. The investigators compared the characteristics of 915 PD patients in the resultant cohort of 5,858 patients to 915 matched HD patients.
Twenty-one percent of the PD patients had been hospitalized once in the previous year (not counting the hospitalization during which dialysis was initiated) compared with 16% of the matched HD patients. PD patients were also more likely than HD patients to have two or more and three or more hospitalizations (8% vs. 5% and 8% vs. 3%, respectively).
Compared with HD, PD was associ-ated with a nearly 2.9-fold higher risk of hospitalization due to dialysis-related infections and a twofold increased risk of hospitalizations due to other infec-tions, including a 1.6-fold higher risk of
hospitalization due to abdominal infec-tions. However, PD also was associated with 70% and 40% lower probabilities of being hospitalized for septicemia or pneumonia, respectively.
In a previous retrospective cohort study of 168 patients initiating out-patient dialysis (71 on PD and 97 on HD), researchers at Sunnybrook Health Sciences Centre in Toronto found that patients who initiate outpatient PD do not have a signifi cantly increased risk of infection-related hospitaliza-tion compared with patients who ini-tiate outpatient HD, according to a report published in Peritoneal Dialysis International (2011;31:440-449). The study, however, showed that patients starting outpatient treatment on PD were significantly more likely than those starting on HD to be hospitalized for peritonitis. ■
Death Risk Is Highest With CVCsCENTRAL VENOUS catheters (CVCs) are associated with the highest mor-tality risk among hemodialysis (HD) vascular access options, according to a systematic literature review.
Arteriovenous grafts confer the second-highest risk for mortality, followed by native arteriovenous fi s-tulas (AVFs). Although these fi ndings are congruent with clinical practice guidelines, which tout AVFs as the preferred form of vascular access in HD patients, lead investigator Pietro Ravani, MD, told Renal & Urology News that solid evidence to back this recommendation is lacking.
“The surprise is the low level of quality of the available studies and the huge variation of the point estimates from those studies,” said Dr. Ravini, of the Department of Community Health at the University of Calgary in Alberta. “Better-quality data are needed, but not from studies with the same design as those already available.”
The researchers analyzed 59 stud-ies, 68% of which were conducted in North America. The mean ages of the combined 315,960 subjects ranged from 16-80 years. Dr. Ravani’s team found the risk of participation bias was high—that is, there was a signifi -cant likelihood that the study subjects were not representative of most hemodialysis patients—in 50 (89%) of the studies. The team identifi ed other defi cits as well. During follow-up, in 51 (86.4%) of studies, investigators did not record a switch from the initial vascular-access type to a newer one. Moreover, in only 18 (30.5%) of stud-ies did investigators adjust the mortal-ity risk for age, sex, and presence of diabetes and cardiovascular disease
Overall, compared with patients who had AVFs, those with arteriovenous grafts had a 45% increased mortal-ity risk. Furthermore, compared with arteriovenous grafts, CVCs conferred a 25% higher death risk. ■
Rosemary Frei, MSc, provided news coverage of the Canadian Society of Nephrology’s 2012 meeting ■ CSN annual meeting, St. John’s, Newfoundland

24 Renal & Urology News JUNE 2012 www.renalandurologynews.com
M ore than 60 million Americans are in some stage of chron-ic kidney disease (CKD).
Therefore, it makes a lot of sense to direct nutrition interventions toward prevention or delay of progression. A key modifi able characteristic that contributes to CKD is hypertension. Use of a multi-disciplinary approach, with a strong emphasis on nutrition by a registered dietitian, to reduce blood pressure (BP) could be very cost effi cient for the health care system as a whole.
DASH dietThe Dietary Approaches to Stop Hypertension (DASH) diet concept may be an excellent way to do this. Both the DASH and Premier studies were positive trials that demonstrated the effectiveness of dietary changes on BP control (N Engl J Med 1997;336:1117-1124 and JAMA 2003;289:2083-2093). The difference between the DASH and Premier trials is that DASH was a con-trolled feeding trial whereas Premier was a comprehensive lifestyle behav-ior trial. In the DASH study, Appel and colleagues executed an eight-week clinical trial in which individuals with prehypertension or stage I hypertension were placed on a diet rich in fruits, vegetables, and low-fat dairy products. This type of diet is rich in calcium, mag-nesium, and potassium. Meat products
were also low in fat, and grains were whole wheat. Subjects in the DASH diet were provided food and thus did not have to make major behavioral changes. While this study demonstrated that the diet was effective, it did not show whether individuals who were taught the concepts could in turn be successful in lowering BP. The sub-
sequent Premier study did show that individuals could be taught the DASH principles and experience signifi cant reductions in blood pressure.
Potassium concernsInitially, one might be hesitant to adopt the DASH concept in individuals with CKD because a diet rich in fruits, vegetables, and dairy products would contain a lot of potassium and phos-phorus. However, in the early stages of CKD, potassium content is not an issue per se, as it is not usually restricted until stages 3 and 4. It is worth noting that individuals on ACE inhibitors for hypertension should have their serum potassium monitored systematically as these drugs are potassium sparing. Furthermore, there are benefi ts to diets rich in fruits, vegetables, and whole grains besides BP lowering, includ-ing reduction in the albumin excre-tion rate (AER) and decreased risk of kidney stones.
Jacobs et al. (Am J Kidney Dis 2009 53:638-646) used frozen urine from sub-jects who participated in the DASH diet study to determine whether AER could benefi t from a DASH diet even though protein was not reduced. The study looked at three groups: the DASH diet group with 18% of energy from pro-tein, 57% from carbohydrate, and 25% from fat; the fruit and vegetable group with 15% of energy from protein, 49%
from carbohydrate, and 36% from fat; and the control diet with 14% of energy from protein, 51% from carbohydrate, and 36% from fat. The fruit and vegeta-ble group was rich in fruits, vegetables, whole grains, and nuts and reduced in refi ned grain but otherwise similar to the control. The DASH diet was even richer in vegetables, whole grains, and nuts,
had decreased meat, poultry, and fi sh, and eliminated whole milk and added low-fat dairy foods. After eight weeks, the researchers observed no signifi cant changes in AER; however, a signifi cant interaction was found in subjects with an AER of 7 mg/24 hour or greater. In subjects with the higher AER at baseline, AER at eight weeks was lower in partici-pants eating the fruit and vegetable diet compared with those on the DASH or control diets. The results of this study may indicate that for patients further along in the progression of CKD, pro-tein control in addition to greater intake of fruits, vegetables, and whole grains may be benefi cial.
Another study investigated the impact of a DASH-style diet on kidney stones. The theory was that diets high in fruits and vegetables increases urinary citrate. Citrate is an inhibitor of calcium stone formation. Furthermore, diets with moderate to high calcium content in conjunction with low animal protein and sodium can decrease the risk of calcium oxalate stone recurrence by 51% (N Engl J Med 2002; 346:77-84). However, the DASH diet is high in both vitamin C and oxalate, both of which contribute to kidney stone formation. A study by Taylor et al. (J Am Soc Nephrol
2009;20:2253-2259) demonstrated the positive benefi ts of the DASH-style diet by creating a DASH score. The DASH score is based on eight components (high intake of fruits, vegetables, nuts, legumes, low-fat dairy products, and whole grains, and low intake of sodium, sweetened beverages, and red and pro-cessed meats). Results of their analysis showed that people with higher DASH scores had higher intake of calcium, potassium, magnesium, oxalate, and vitamin C and lower intakes of sodium. Higher DASH scores were associated with lower risk of kidney stone devel-opment even with the higher intake of calcium and vitamin C. (See the article in the November 2009 issue or go to www.renalandurologynews/DASH.)
The DASH-style diet rich in vegetables, fruit, and whole grains is a nutrition intervention shown to lower BP, reduce AER in patients with AER greater than 7 mg/24 hours, and reduce the risk of kidney stones, all important factors when trying to prevent or delay the progression of CKD in at-risk individuals. ■
Dr. Steiber is Coordinator of the Dietetic Internship/Master’s Degree Program at Case Western Reserve University in Cleveland.
Renal Nutrition UpdateDASH-style diet may provide an effective way to prevent or delay progression of chronic kidney disease BY ALISON L. STEIBER, PhD, RD, LD
A diet stressing fruits, vegetables, and whole grains can lower BP, decrease the albumin excretion rate, and reduce the risk of kidney stones.
Increased intake of fruits and vegetables may have renal benefi ts in CKD patients.
© IS
TOCK
PHO
TO.C
OM
/ A
LUXU
M

28 Renal & Urology News JUNE 2012 www.renalandurologynews.com
BY ROSEMERY FREI, MSC
A NEW study suggests that vitamin D may protect against prostate cancer (PCa), but some PCa specialists remain unconvinced.
The non-randomized trial was pub-lished online April 16 in The Journal of Clinical Endocrinology and Metabolism.
Fifty-two men with an average age of 65 years took 4,000 IU/day of vitamin D3 in soft-gel capsules. Forty-four of the subjects took it for a full year and had both safety and effi cacy data avail - able for analysis. Fifty-five percent of the men had a decrease in the num-ber of positive cores or in Gleason
score at repeat biopsy, according to researchers. No significant adverse events were observed.
The investigators compared with these patients with 19 control subjects with PCa who were similar to the test sub-jects but did not take vitamin D. Of these, 63% progressed compared with
only 34% of vitamin D supplementa-tion group. In addition, only 21% of control subjects had improved on repeat biopsy (experienced a decrease in the number of positive cores or no increase in Gleason score at repeat biopsy).
“We are now performing a random-ized study, which will take another two to three years to complete, but in the meantime our open-label study showed that the supplement seems to benefi t subjects,” said lead investi-gator Sebastiano Gattoni-Celli, MD, Professor of Radiation Oncology at the Medical University of South Carolina in Charleston. “We are not claiming this is the end of the story, but it certainly is hopeful.”
However, Eric A. Klein, MD, Chairman of the Glickman Urological and Kidney Institute at Cleveland Clinic and Professor of Surgery at Cleveland Clinic Lerner College of Medicine, said the Selenium and Vitamin E Cancer
Prevention Trial, which showed a signifi cant increase in PCa incidence with vitamin E over the longer term, is a reminder of deleterious effects that can eventually be uncovered from “seemingly innocuous substances such as vitamins.”
He added that the lack of placebo control group in the new trial “makes the conclusion of this study tenuous.” In addition, “fewer positive cores after a year of supplementation is not evi-dence of disease stabilization, regres-sion, or lack of progression in biological aggressiveness,” Dr. Klein told Renal & Urology News. “Consumers should be wary of claims of benefi ts from dietary supplementation unless they are rigor-ously demonstrated in large-scale, pla-cebo-controlled, randomized trials.”
Eric J. Jacobs, PhD, Strategic Director, Pharmacoepidemiology, National Home Offi ce, American Cancer Society, Inc., Atlanta, agrees.
“Results of small studies such as this are interesting but preliminary, Dr. Jacobs said. There is not adequate evidence for physicians to suggest to their prostate cancer patients that vita-min D supplements may be useful in treating their disease.” ■
Vitamin D May Benefit Prostate Cancer Patients
Brief Summary: Consult package insert for complete Prescribing Information
INDICATIONS AND USAGE:Bone Metastasis from Solid Tumors. Xgeva is indicated for the prevention of skeletal-related events in patients with bone metastases from solid tumors.
Important Limitation of Use. Xgeva is not indicated for the prevention of skeletal-related events in patients with multiple myeloma (see Clinical Trials [14] in Full Prescribing Information).
DOSAGE AND ADMINISTRATION:Recommended Dosage. The recommended dose of Xgeva is 120 mg administered as a subcutaneous injection every 4 weeks in the upper arm, upper thigh, or abdomen. Administer calcium and vitamin D as necessary to treat or prevent hypocalcemia (see Warnings and Precautions).
Preparation and Administration. Visually inspect Xgeva for particulate matter and discoloration prior to administration. Xgeva is a clear, colorless to pale yellow solution that may contain trace amounts of translucent to white proteinaceous particles. Do not use if the solution is discolored or cloudy or if the solution contains many particles or foreign particulate matter. Prior to administration, Xgeva may be removed from the refrigerator and brought to room temperature (up to 25°C/77°F) by standing in the original container. This generally takes 15 to 30 minutes. Do not warm Xgeva in any other way (see How Supplied/Storage and Handling). Use a 27-gauge needle to withdraw and inject the entire contents of the vial. Do not re-enter the vial. Discard vial after single-use or entry.
HOW SUPPLIED/STORAGE AND HANDLING: Xgeva is supplied in a single-use vial. Store Xgeva in a refrigerator at 2°C to 8°C (36°F to 46°F) in the original carton. Do not freeze. Once removed from the refrigerator, Xgeva must not be exposed to temperatures above 25°C/77°F or direct light and must be used within 14 days. Discard Xgeva if not used within the 14 days. Do not use Xgeva after the expiry date printed on the label. Protect Xgeva from direct light and heat. Avoid vigorous shaking of Xgeva.
CONTRAINDICATIONS: None.
WARNINGS AND PRECAUTIONS: Hypocalcemia. Xgeva can cause severe hypocalcemia. Correct pre-existing hypocalcemia prior to Xgeva treatment. Monitor calcium levels and administer calcium, magnesium, and vitamin D as necessary. Monitor levels more frequently when Xgeva is administered with other drugs that can also lower calcium levels. Advise patients to contact a healthcare professional for symptoms of hypocalcemia (see Adverse Reactions and Patient Counseling Information [17] in full Prescribing Information). Based on clinical trials using a lower dose of denosumab, patients with a creatinine clearance less than 30 mL/min or receiving dialysis are at greater risk of severe hypocalcemia compared to patients with normal renal function. In a trial of 55 patients, without cancer and with varying degrees of renal impairment, who received a single dose of 60 mg denosumab, 8 of 17 patients with a creatinine clearance less than 30 mL/min or receiving dialysis experienced corrected serum calcium levels less than 8.0 mg/dL as compared to 0 of 12 patients with normal renal function. The risk of hypocalcemia at the recommended dosing schedule of 120 mg every 4 weeks has not been evaluated in patients with a creatinine clearance less than 30 mL/min or receiving dialysis.
Osteonecrosis of the Jaw (ONJ). Osteonecrosis of the jaw (ONJ) can occur in patients receiving Xgeva, manifesting as jaw pain, osteomyelitis, osteitis, bone erosion, tooth or periodontal infection, toothache, gingival ulceration, or gingival erosion. Persistent pain or slow healing of the mouth or jaw after dental surgery may also be manifestations of ONJ. In clinical trials, 2.2% of patients receiving Xgeva developed ONJ; of these patients, 79% had a history of tooth extraction, poor oral hygiene, or use of a dental appliance (see Adverse Reactions). Perform an oral examination and appropriate preventive dentistry prior to the initiation of Xgeva and periodically during Xgeva therapy. Advise patients regarding oral hygiene practices. Avoid invasive dental procedures during treatment with Xgeva. Patients who are suspected of having or who develop ONJ while on Xgeva should receive care by a dentist or an oral surgeon. In these patients, extensive dental surgery to treat ONJ may exacerbate the condition.
ADVERSE REACTIONS: The following adverse reactions are discussed below and elsewhere in the labeling:
(see Warnings and Precautions)(see Warnings and Precautions)
The most common adverse reactions in patients receiving Xgeva (per-patient incidence greater than or equal to 25%) were fatigue/asthenia, hypophosphatemia, and nausea (see Table 1). The most common serious adverse reaction in patients receiving Xgeva was dyspnea. The most common adverse reactions resulting in discontinuation of Xgeva were osteonecrosis and hypocalcemia.
Clinical Trials Experience. Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in other clinical trials and may not reflect the rates observed in practice. The safety of Xgeva was evaluated in three randomized, double-blind, double-dummy trials (see Clinical Trials [14] in full Prescribing Information) in which a total of 2841 patients with bone metastasis from prostate cancer, breast cancer, or other solid tumors, or lytic bony lesions from multiple myeloma received at least one dose of Xgeva. In Trials 1, 2, and 3, patients were randomized to receive either 120 mg of Xgeva every 4 weeks as a subcutaneous injection or 4 mg (dose adjusted for reduced renal function) of zoledronic acid every 4 weeks by intravenous (IV) infusion.
Entry criteria included serum calcium (corrected) from 8 to 11.5 mg/dL (2 to 2.9 mmol/L) and creatinine clearance 30 mL/min or greater. Patients who had received IV bisphosphonates were excluded, as were patients with prior history of ONJ or osteomyelitis of the jaw, an active dental or jaw condition requiring oral surgery, non-healed dental/oral surgery, or any planned invasive dental procedure. During the study, serum chemistries including calcium and phosphorus were monitored every 4 weeks. Calcium and vitamin D supplementation was recommended but not required. The median duration of exposure to Xgeva was 12 months (range: 0.1 – 41) and median duration on-study was 13 months (range: 0.1 – 41). Of patients who received Xgeva, 46%
and 3% Black. The median age was 63 years (range: 18 – 93). Seventy-five percent of patients who received Xgeva received concomitant chemotherapy.
Table 1. Per-patient Incidence of Selecteda Adverse Reactions of Any Severity (Trials 1, 2, and 3)
a Adverse reactions reported in at least 10% of patients receiving Xgeva in Trials 1, 2, and 3, and meeting one of the following criteria:
5% greater incidence in patients treated with zoledronic acid compared to placebo (US Prescribing Information for zoledronic acid)
b Laboratory-derived and below the central laboratory lower limit of normal [8.3 – 8.5 mg/dL (2.075 – 2.125 mmol/L) for calcium and 2.2 – 2.8 mg/dL (0.71 – 0.9 mmol/L) for phosphorus]
Severe Mineral/Electrolyte Abnormalities
1.75 mmol/L) occurred in 3.1% of patients treated with Xgeva and 1.3% of patients treated with zoledronic acid. Of patients who experienced severe hypocalcemia, 33% experienced 2 or more episodes of severe hypocalcemia and 16% experienced 3 or more episodes (see Warnings and Precautions and Use in Specific Populations).
than 0.6 mmol/L) occurred in 15.4% of patients treated with Xgeva and 7.4% of patients treated with zoledronic acid.
Osteonecrosis of the JawIn the primary treatment phases of Trials 1, 2, and 3, ONJ was confirmed in 1.8% of patients in the Xgeva group and 1.3% of patients in the zoledronic acid group (see Warnings and Precautions). When events occurring during an extended treatment phase of approximately 4 months in each trial are included, the incidence of confirmed ONJ was 2.2% in patients who received Xgeva. The median time to ONJ was 14 months (range: 4 – 25).
Immunogenicity. As with all therapeutic proteins, there is potential for immunogenicity. Using an electrochemiluminescent bridging immunoassay, less than 1% (7/2758) of patients with osseous metastases treated with denosumab doses ranging from 30 – 180 mg every 4 weeks or every 12 weeks for up to 3 years tested positive for binding antibodies. No patient with positive binding antibodies tested positive for neutralizing antibodies as assessed using a chemiluminescent cell-based in vitro biological assay. There was no evidence of altered pharmacokinetic profile, toxicity profile, or clinical response associated with binding antibody development. The incidence of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of a positive antibody (including neutralizing antibody) test result may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of antibodies to denosumab with the incidence of antibodies to other products may be misleading.
DRUG INTERACTIONS: No formal drug-drug interaction trials have been conducted with Xgeva. In clinical trials in patients with breast cancer metastatic to bone, Xgeva was administered in combination with standard anticancer treatment. Serum denosumab concentrations at 1 and 3 months and reductions in the bone turnover marker uNTx/Cr (urinary N-terminal telopeptide corrected for creatinine) at 3 months were similar in patients with and without prior intravenous bisphosphonate therapy. There was no evidence that various
anticancer treatments affected denosumab systemic exposure andpharmacodynamic effect. Serum denosumab concentrations at 1 and 3 months were not altered by concomitant chemotherapy and/or hormone therapy. The median reduction in uNTx/Cr from baseline to month 3 was similar between patients receiving concomitant chemotherapy and/or hormonetherapy (see Clinical Pharmacology [12.2] in full Prescribing Information).
USE IN SPECIFIC POPULATIONS:Pregnancy: Category C. There are no adequate and well-controlled trials ofXgeva in pregnant women. Use Xgeva during pregnancy only if the potential benefit justifies the potential risk to the fetus. Encourage women who become pregnant during Xgeva treatment to enroll in Amgen’s Pregnancy SurveillanceProgram. Patients or their physicians should call 1-800-77-AMGEN (1-800-772-6436) to enroll. In an embryofetal developmental study, cynomolgusmonkeys received subcutaneous denosumab weekly during organogenesis atdoses up to 6.5-fold higher than the recommended human dose of 120 mgevery 4 weeks, based on body weight (mg/kg). No evidence of maternal toxicity
during the first trimester, and fetal lymph nodes were not examined. Potential adverse developmental effects resulting from exposures during the second and third trimesters have not been assessed in animals (see Nonclinical Toxicology [13.2] in full Prescribing Information). In genetically engineered mice in which the gene for RANK ligand (RANKL) has been deleted (a “knockout mouse”), the absence of RANKL caused fetal lymph node agenesis and led to postnatal impairment of dentition and bone growth. Pregnant RANKL knockout mice alsoshowed altered maturation of the maternal mammary gland, leading to impaired lactation postpartum (see Use in Nursing Mothers).
Nursing Mothers. It is not known whether Xgeva is excreted into human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from Xgeva, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother. Maternal exposure to Xgevaduring pregnancy may impair mammary gland development and lactationbased on animal studies in pregnant mice lacking the RANK/RANKL signalingpathway that have shown altered maturation of the maternal mammary gland,leading to impaired lactation postpartum (see Nonclinical Toxicology [13.2] infull Prescribing Information).
Pediatric Use. The safety and effectiveness of Xgeva in pediatric patients have not been established. Treatment with Xgeva may impair bone growth inchildren with open growth plates and may inhibit eruption of dentition. In neonatal rats, inhibition of RANKL with a construct of osteoprotegerin bound toFc (OPG-Fc) at doses less than or equal to 10 mg/kg was associated withinhibition of bone growth and tooth eruption. Adolescent monkeys dosed with denosumab at 5 and 25 times (10 and 50 mg/kg dose) higher than therecommended human dose of 120 mg subcutaneously every 4 weeks (based on body weight mg/kg) had abnormal growth plates (see Nonclinical Toxicology [13.2] in full Prescribing Information).
Geriatric Use. Of patients who received Xgeva in Trials 1, 2, and 3, 1260 (44%) were 65 years of age or older. No overall differences in safety or efficacywere observed between these patients and younger patients.
Renal Impairment. In a trial of 55 patients without cancer and with varying degrees of renal function who received a single dose of 60 mg denosumab, patients with acreatinine clearance of less than 30 mL/min or receiving dialysis were at greater risk of severe hypocalcemia with denosumab compared to patients with normal renal function. The risk of hypocalcemia at the recommended dosing schedule of 120 mg every 4 weeks has not been evaluated in patients with a creatinine clearance of less than 30 mL/min or receiving dialysis (see Warnings and Precautions, Adverse Reactions, and Clinical Pharmacology [12.3] in full Prescribing Information).
OVERDOSAGE: There is no experience with overdosage of Xgeva.
PATIENT COUNSELING INFORMATION:Advise patients to contact a healthcare professional for any of the following:
twitching, spasms, or cramps (see Warnings and Precautions and Adverse Reactions)
the jaw, mouth, or teeth (see Warnings and Precautions and Adverse Reactions)
(see Warnings and Precautions)
(see Use in Specific Populations)Advise patients of the need for:
Advise patients that denosumab is also marketed as Prolia®. Patients shouldinform their healthcare provider if they are taking Prolia®.
Body SystemXgeva
n = 2841 %
Zoledronic Acid n = 2836
%
GA STROINTESTINAL Nausea Diarrhea
31 20
32 19
GE NERAL Fatigue/ Asthenia
45
46
IN VESTIGATIONS b
b
18 32
9
20
NE UROLOGICAL 13
14
RE SPIRATORY Dyspnea Cough
21 15
18 15
Amgen Manufacturing Limited, a subsidiary of Amgen Inc.One Amgen Center Drive
Thousand Oaks, California 91320-1799©2011 Amgen Inc.
All rights reserved. Printed in USA.
©2011 Amgen Inc. All rights reserved. 63850-R1-V1 12/11 www.XGEVA.com
REFERENCES: 1. Saad F, Gleason DM, Murray R, et al, for the Zoledronic Acid Prostate Cancer Study Group. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with
metastatic hormone-refractory prostate cancer. J Natl Cancer Inst. 2004;96:879-882. 2. Ibrahim A, Scher N, Williams G, et al. Approval summary for zoledronic acid for treatment of multiple myeloma and cancer
bone metastases. Clin Cancer Res. 2003;9:2394-2399. 3. Yu EY, Nathan FE, Higano CS. Role of detection of metastatic disease as a leading cause of screening failure in an ongoing phase III trial of zibotentan
versus placebo in patients with nonmetastatic castration-resistant prostate cancer (CRPC). J Clin Oncol. 2011;29(suppl 7). Abstract 135. 4. Scher HI, Morris MJ, Kelly WK, Schwartz LH, Heller G. Prostate cancer clinical
trial end points: “RECIST”ing a step backwards. Clin Cancer Res. 2005;11:5223-5232. 5. Tannock IF, de Wit R, Berry WR, et al, for the TAX 327 Investigators. Docetaxel plus prednisone or mitoxantrone plus prednisone for
advanced prostate cancer. N Engl J Med. 2004;351:1502-1512. 6. Petrylak DP, Tangen CM, Hussain MHA, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate
cancer. N Engl J Med. 2004;351:1513-1520. 7. XGEVA® (denosumab) prescribing information, Amgen. 8. Saad F, Gleason DM, Murray R, et al, for the Zoledronic Acid Prostate Cancer Study Group. A randomized, placebo-
controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94:1458-1468.
Reduced number of positive cores found on repeat prostate biopsy.

www.renalandurologynews.com JUNE 2012 Renal & Urology News 29
Despite advances in the treat-ment of hypertension, the majority of patients with chronic kidney disease
(CKD) remain above current blood pres-sure (BP) targets. Improved BP control is expected to slow progression of loss of kidney function and reduce the incidence of cardiovascular events and death. Data from NHANES 1999-2004 show adults with CKD are less likely to have control of BP than those without evidence of CKD.1 The inability to achieve goal BP despite three or more antihypertensive drugs is defi ned as resistant hypertension, and this is more common in CKD patients.
Practice guidelines
The National Heart, Lung and Blood Institute’s Joint National Committee
(JNC) 72 and National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) clinical practice guidelines3 currently recom-mend targets lower than 130/80 mm Hg in CKD patients.
However, updated BP guidelines from KDIGO to be published this year suggest the level of evidence to support this target varies by the pres-ence or absence of diabetes and the level of albuminuria in this patient population. In fact, a recent systematic review of the literature revealed only three randomized controlled trials in which patients with CKD achieved a BP lower than 130/80 mm Hg.4 None of these trials included patients with diabetes, and two of the three trials showed a benefi t in terms of slowing CKD progression only in the sub-groups with more than one gram of proteinuria with minor increases in both the number of anti-hypertensive drugs used and adverse effects.
Data from more than 16,000 par-ticipants in the National Kidney Foundation’s Kidney Early Evaluation Program (KEEP) show associations between BP levels and end-stage renal disease (ESRD), or chronic kidney fail-ure, in patients with stage 3 and stage 4 CKD. A higher risk for developing ESRD was observed among people with BP measurements of 140/90 or higher, but those who had BP mea-surements of 150/90 and above were at highest risk.
Additionally, the study found that that more than 30% of people with CKD
had BP measurements above 150/90. This study highlights the importance of BP control in CKD patients, suggesting that a target of 140/90 may suffi ce at least in terms of delaying progression to chronic kidney failure.5
Innovative strategies are needed to lower BP in patients with CKD. Novel approaches to hypertension treat-ment reviewed subsequently include: baroreceptor sensitization and renal nerve ablation.
Baroreceptor modulation for refractory hypertension
The Rheos Barorefl ex Hypertension Therapy System is an implantable device that can treat patients with resistant hypertension. It activates the carotid barorefl ex through electrical stimulation of the carotid sinus wall. The Rheos Pivotal Trial is a random-ized, double-blind, parallel-design, phase 3 trial of barorefl ex activation
therapy (BAT) on systolic blood pres-sure (SBP) in 265 patients with resistant hypertension.6 Subjects received either BAT (Group A) for the fi rst six months or delayed BAT initiation following the six-month visit (Group B).
The fi ve coprimary endpoints were:acute SBP responder rate at • six months sustained responder rate at • 12 months procedure safety • BAT safety • device safety • The trial showed signifi cant benefi t
for the endpoints of sustained effi cacy, BAT safety, and device safety. However, it did not meet the endpoints for acute responders or procedural safety. A protocol-specifi ed ancillary analysis showed 42% of patients in Group A achieved an SBP of 140 mm Hg or less at six months compared with 24% of Group B, a statistically signifi cant
Providing Renal Protection Through BP Control Innovative strategies are needed to lower blood pressure in patients with chronic kidney disease BY GEORGE L. BAKRIS, MD, AND JOSEPH A. VASSALOTTI, MD
George L. Bakris, MD Joseph A. Vassalotti, MD
■ FEATURE
continued on page 30
Editor’s note: The National Kidney Foundation sponsored a session on this topic at its 2012 Spring Clinical Meetings in National Harbor, Md. The moderators were George L. Bakris, MD, Professor of Medicine and Director, ASH Comprehensive Hypertension Center, The University of Chicago Medicine, and Joseph A. Vassalotti, MD, Chief Medical Offi cer, NKF, and Associate Clinical Professor of Medicine, Mount Sinai School of Medicine. What follows is a summation of the presentations given during the session.

30 Renal & Urology News JUNE 2012 www.renalandurologynews.com
difference between the groups. Both groups achieved an SBP of 140 mm Hg or higher at 12 months.
A non-randomized unblinded follow up of the Rheos Pivotal Trial revealed that 76% of subjects qualified as clinically signifi cant responders, and an additional 10% were indetermi-nate.7 Among long-term responders receiving BAT, the mean BP drop was 35/16 mm Hg. Medication use was reduced by the end of the randomized phase and remained lower through the follow-up period. Among responders, 55% achieved goal BP (less than 140 or less than 130 mm Hg in patients with diabetes or kidney disease). BP measurements of all active patients remained stable from completion of the randomized phase through long-term follow-up. BAT substantially reduced arterial pressure for most patients par-ticipating in the Rheos Pivotal Trial, which was maintained over long-term follow-up of 22 to 53 months.
Renal denervation
Nephrologists are well aware that stimulation of the renal sympathetic nerves causes increased renin release, increased sodium reabsorption, and a reduction of renal blood fl ow. These elements of the neural homeostatic regulation of kidney function may be
overstimulated, resulting in chronically heightened sympathetic tone in hyper-tensive patients. Therapeutic denerva-tion may also become an option for refractory hypertension.
The “Symplicity” technique uses a catheter inserted into the renal artery via the femoral artery to deliver radio-frequency energy to ablate the renal sympathetic nerve. The Symplicity HTN-1 study included 153 patients treated with this technique at 19 cen ters in Australia, Europe, and the United States.8,9
At baseline, the study population had a mean age of 57 years; 39% of subjects were women, 31% were diabetic, and 22% had coronary artery disease. They had a mean offi ce BP of 176/98 mm Hg and were on a mean of fi ve antihy-pertensive medications. Subjects had a mean estimated glomerular fi ltration rate of 83 mL/min/1.73 m2.
The median time from fi rst to last radiofrequency energy ablation was 38 minutes. The procedure was with-out complication in 97% of patients (149 of 153). Four acute procedural complications occurred, including three groin pseudoaneurysms and one renal artery dissection, all managed without further sequelae. Automated clinic pressure with printout (the pri-mary trial endpoint) was reduced by 20/10, 24/11, 25/11, 23/11, 26/14, and 32/14 mm Hg at 1, 3, 6, 12, 18, and 24 months, respectively. These
fi ndings support the short-term safe-ty and effi cacy treatment of resistant hypertension with catheter-based renal sympathetic denervation.
The Symplicity HTN-2 random-ized unblinded trial of renal sympa -thetic denervation versus usual care for medication-resistant hyperten -sion show a significant reduction in systolic and diastolic blood pres-sure at six months compared with age-matched, equally hypertensive controls. Although offi ce-based BP measurements provided the sole assess-ment of BP as a primary endpoint, this intragroup variability of BP assess-ment requires further explanation, particularly because 35% of controls enjoyed a 10 mm Hg or more decrease in systolic pressure at six months. The major limitations of Symplicity HTN 1 and 2 studies are the absence of data beyond 36 months. There is specula-tion that functional renal sympathetic reinervation may occur, but there is no evidence of this up to three years post procedure.
The Symplicity HTN-3 is a random-ized blinded trial of renal sympa thetic denervation versus usual care for medi-cation-resistant hypertension. This will be the largest of the 3 trials recruiting 542 patients in the United States and recruit-ment is ongoing. Results from this trial should be available early next year.
The overall evidence suggests that both BAT and renal denervation can
safely reduce SBP in patients with resistant hypertension. Unfortunately, most of the clinical trials with both approaches have avoided patients with Stages 3b or higher CKD. Future clini-cal trials will address the limitations and long-term outcomes of these therapies to further defi ne their potential thera-peutic roles. ■
REFERENCES
1. Snyder JJ, Collins AJ. KDOQI hypertension, dyslipi-demia, and diabetes care guidelines and current care patterns in the United States CKD population: National Health and Nutrition Examination Survey 1999-2004. Am J Nephrol 2009;30:44-54.
2. Chobanian AV, Bakris GL, Black HR, et al, The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003;289:2560-2572.
3. National Kidney Foundation, K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease. Am J Kidney Dis 2004;43(suppl 1):S1-S290.
4. Upadhyay A, Earley A, Haynes SM, et al. Systematic review: blood pressure target in chronic kidney disease and proteinuria as an effect modifi er. Ann Intern Med 2011;154:541-548.
5. Peralta CA, Norris KC, Li S, et al. Blood pressure components and end-stage renal disease in persons with chronic kidney disease: The Kidney Early Evaluation Program (KEEP). Arch Intern Med 2012;172:41-47.
6. Bisognano JD, Bakris G, Nadim MK, et al. Barorefl ex activation therapy lowers blood pressure in patients with resistant hypertension: results from the double-blind, randomized, placebo-controlled rheos pivotal trial. J Am Coll Cardiol 2011;58:765-73.
7. Bakris GL, Nadim MK, Haller H, et al. Barorefl ex Activation Therapy provides durable benefi t in patients with resistant hypertension: results of long-term follow-up in the Rheos Pivotal Trial. J Am Soc Hypertens 2012 Feb 14; published online ahead of print.
8. Symplicity HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 months. Hypertension 2011;57:911-917.
9. Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hyper-tension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet 2010;376:1903-1909.
BP control continued from page 29
PARTIAL NEPHRECTOMY (PN) can be safely performed in patients with renal tumors 7 cm or more in diameter with acceptable technical, oncologic and functional outcomes, according to researchers.
Consequently, they concluded, PN should be a surgical option when fea-sible regardless of tumor size.
Christopher J. Long, MD, of Fox Chase Cancer Center in Philadelphia, and colleagues used a prospectively maintained institutional kidney can-cer database to identify 46 patients undergoing PN for 49 renal tumors 7 cm or more in diameter. The patient population included 33 men and 13 women. The patients had a median age of 58 years (range 21-83) and a median tumor size of 8.7 cm. Thirteen patients (25.5%) had 7.0-7.9 cm tumors, 11 (22.5%) had 8.0-8.9 cm tumors, and fi ve (10.2%) had 9.0-9.9 cm tumors.
Twenty patients (40.8%) had tumors larger than 10 cm. Approximately 80% of tumors were malignant.
The five- and 10-year overall and renal cell carcinoma-specifi c surviv-als were 94.5% and 70.9%, respec-tively, the researchers reported in BJU International (2012;109:1450-1456). The fi ve- and 10-year recurrence-free survival rates were 88.7% and 66.5%, respectively. Five patients (10.9%) had an upward migration in their chronic kidney disease status after PN. Sixteen complications occurred after a median follow-up of 13.1 months (range 0.2–170.0 months), including four (8.2%) blood transfusions and six (12.2%) urinary fi stulae.
The researchers noted that their results compare favorably with those of published reports of similarly stage-matched tumors treated with radical nephrectomy. ■
Partial Nephrectomy Is An Option for Larger Tumors
NEOADJUVANT CHEMOTHERAPY for patients with small cell urothelial carci-noma (SCUC) improves their likelihood of survival compared with a historical cohort of patients treated with initial cystectomy, a study found.
Researchers concluded that neoadju-vant chemotherapy should be con-sidered for all patients with surgically resectable SCUC.
“With neoadjuvant chemotherapy, we are now seeing a large number of patients who are cancer-free for more than fi ve years and are essentially cured of their small cell urothelial can-cer,” lead investigator Arlene Siefker-Radtke, MD, told Renal & Urology News. “It is important for physicians to recognize the presence of this vari-ant histology before cystectomy and
refer patients to a medical oncologist.” Dr. Siefker-Radtke and her colleagues at M.D. Anderson Cancer Center in Houston led studied 95 SCUC pa-tients who were surgical candidates. Of these, 48 received neoadjuvant chemotherapy and 47 underwent initial surgery. The median overall and disease-specifi c survival were signifi -cantly greater in the adjuvant chemo-therapy recipients than those who had initial surgery (159.5 vs. 18.3 months and 79% vs. 20%, respectively), ac-cording to a report in European Urology (published online ahead of print).
Adjuvant chemotherapy had no im-pact on overall survival among patients treated with initial cystectomy, although the small number of patients limits the impact of this fi nding. ■
Neoadjuvant Chemo Urged For Rare Bladder Tumor

PROSTATE CANCER (PCa) patients found to have a positive surgical margin (PSM) in their radical prostatectomy specimen have a low long-term risk of systemic progression and cancer-related death, data show.
In a study of 2,895 PCa patients with a PSM, researchers at Mayo Clinic in Rochester, Minn., led by Stephen A. Boorjian, MD, found that the 15-year systemic- progression-free survival and cancer-specifi c survival was 90% and 93%, respectively, according to a report in Prostate Cancer and Prostatic Diseases (2012;15:56-62). Greater tumor volume, higher pathological Gleason score, and advanced pathological tumor stage were associated with significantly increased risks of systemic progres-sion and death from prostate cancer, but the number and location of positive margins were not.
In multivariate analysis, patients with pT3 or more advanced stage had a twofold increased risk of systemic pro-gression and cancer-related death com-pared with patients who had pT2 stage
cancer. Compared with patients with Gleason score 6, those with Gleason 7 or higher disease had a nearly fourfold increased risk of systemic progression and cancer-related death.
Receipt of adjuvant radiotherapy (RT) was associated with a 66% decreased likelihood of receiving salvage therapy or progression.
When the researchers excluded patients who received postoperative adjuvant RT from multivariate analysis, the variables of tumor volume, patho-logical tumor stage, and pathological Gleason score remained signifi cantly associated with systemic progression and cancer-related death.
In their discussion of study limita-tions, the authors noted that the study was retrospective and nonrandomized. “As such, decisions to treat with adju-vant and salvage therapies were based on patient preference and physician counseling, and were thereby subject to inherent selection bias,” they wrote.
Following surgery, 439 patients (15%) received adjuvant RT, includ-ing 88 who were treated with concur-rent adjuvant androgen deprivation therapy. The recipients of adjuvant RT had a signifi cantly higher median preoperative PSA level and mean tumor volume than those who did not, the study showed. ■
www.renalandurologynews.com JUNE 2012 Renal & Urology News 31
FOCAL THERAPY for localized pros-tate cancer is associated with a low rate of erectile problems and urinary incon-tinence a year after treatment, accord-ing to a small prospective study.
In the study, 42 men underwent focal ablation with high-intensity focused ultrasound (HIFU). Investigators used multiparametric magnetic resonance imaging (MRI) to identify cancerous areas. Almost 90% of men reported having erections satisfactory for inter-course at 12 months post-treatment. All 40 men who were pad-free at baseline were pad-free by three months and maintained pad-free continence at 12 months, according to an online report in The Lancet.
In addition, investigators found no biopsy evidence of cancer in the treated regions in 30 of 39 men who were biop-sied at six months; 36 of the 39 were free of clinically signifi cant cancer.
Of 31 men with good baseline func-tion, 26 (84%) “achieved the trifecta
status” of having leak-free and pad-free continence, erections suffi cient for intercourse, and no evidence of clinically signifi cant disease on multi-parametric MRI at 12 months.
“Focal therapy of discrete areas of cancer, whether unifocal or multi-focal, is feasible, safe, and can be delivered in an ambulatory setting,” the researchers, led by Hashim U. Ahmed, MD, of University College London, noted.
With HIFU, tissue destruction occurs as a result of thermal, mechan-ical, and cavitation effects to pro-duce a clearly demarcated region of coagulative necrosis surrounded by normal tissue on microscopic examina-tion, the authors explained.
The researchers standardized the focal therapy process by setting three broad guidelines: a maximum of 60% of the prostate could be ablated; the edge of the ablation zone had to be at least 10 mm from a neurovascular
bundle (the ablation zone had to be at least 5 mm from both neurovascular bundles if disease was bilateral); and untreated areas could not have any histologic evidence of cancer. High-grade prostate intraepithelial neoplasia and atypical small acinar proliferation were permitted.
“Focal therapy could hold promise in mitigating the harms that result from current therapeutic strategies,” the authors wrote.
In an accompanying editorial, Matvey Tsivian, MD, Michael R. Abern, MD, and Thomas J. Polascik, MD, of Duke University Medical Center in
Durham, N.C., noted that the new study “represents the fi rst rigorously designed study of the early outcomes of focal therapy.”
Still, they noted that the study by Dr. Ahmed and colleagues should be considered as an early report “in view of the constant development of both imag-ing and ablative technology.” In fact, in the new study, ablation was guided not by MRI imaging but by conventional ultrasound, they observed.
Focal therapy, they added, needs standardization, defi nition of consen-sual treatment schemes and nomencla-ture, as well as optimization of patient selection criteria. “With these issues addressed,” they wrote, “focal therapy could potentially become a mainstream therapy for localized prostate cancer that would offer personalized treat-ment tailored to the patient and his disease characteristics as opposed to conventional, stereotypes, whole-gland treatment.” ■
HIFU Focal Therapy Feasible for PCaIn a small study, 90% of men had erections satisfactory for intercourse at 12 months post-treatment
PCa Death Risk Low Despite PSM DIALYSIS MAY improve outcomes in pa-
tients suffering from treatment-resistant congestive heart failure (CHF) accompa-nied by severe renal insuffi ciency, new fi ndings suggest.
Trijntje T. Cnossen, MD, PhD, of the Maastricht University Medical Center in Maastricht, The Netherlands, prospec-tively studied 23 hypervolemic patients with CHF complicated by progressive and permanent chronic renal insuffi -ciency. The patients were classifi ed as having cardiorenal syndrome (CRS) Type 2. All subjects had failed treatment with high-dose intravenous diuretics.
Twelve patients were treated with peri-toneal dialysis (PD) and 11 were treated with intermittent hemodialysis (IHD). The median survival time after the start of dialysis was 16 months. Hospitalizations for cardiovascular causes decreased signifi cantly from 1.4 days/patient/month pre-dialysis to 0.4 days/patient/month post-dialysis, the research-ers reported online ahead of print in Nephrology Dialysis Transplantation. The
investigators observed no signifi cant change in hospitalizations for all causes. The authors noted that “hospitaliza -tions for non-cardiovascular causes appeared to be especially pronounced in patients who were already hospital-ized at the start of dialysis and were in general not related to complications of the treatment.”
In addition, New York Heart Associa-tion class improved signifi cantly from 3.8 at the start of dialysis to 2.4 after eight months. Dr. Cnossen’s team observed no signifi cant change in left ventricular ejection fraction. The investi-gators reported a relatively high number of technical complications associated with dialysis.
The cohort had a mean age of 66 years. Seventeen subjects (74%) were men and 12 (52%) had diabetes. The cohort’s mean glomerular fi ltration rate at baseline was 14.6 mL/min/1.73 m2. Fourteen patients had chronic kidney disease (CKD) stage 5, seven had CKD stage 4, and two had CKD stage 3. ■
Dialysis Helps Some Patientswith Treatment-Resistant CHF
All men who were pad-free at baseline were pad-free three months post-op.

HYPERTENSION RISK among indi-viduals living in rural areas may depend on the distance of their residence from population centers, according to a study conducted in Japan.
The study included 1,348 individuals in a rural mountainous region in the eastern part of Shimane prefecture who were interviewed face to face by trained staff and had sitting blood pressure measurements taken at a public center. Individuals who lived a moderate and far distance from a population center (Matsue city) had a signifi cant 44% and 78% increased risk of self-report-ed hypertension (patients reporting that they were taking antihypertensive medication or were under treatment for hypertension without medication) compared with those who lived close to the population center, after adjusting for potential confounders.
However, the association between distance and hypertension risk became nonsignificant when hyper-tension defi ned by BP measurement (140/90 mm Hg or higher) was taken
into account, Tsuyoshi Hamano, MA, an Associate Professor at Shimane University in Izumo, and colleagues reported online ahead of print in the American Journal of Hypertension.
For the study, the researchers esti-mated distance from subjects’ actual home addresses to the population center based on road network data and did not use straight-line distance. “This is because a road network is more complicated in a mountainous region compared with an urban region; there-fore, the straight-line distance might be less effective in this kind of research design,” the authors noted.
The researchers noted that they used self-reported hypertension to defi ne the presence of the condition because a BP measurement taken at a public center might increase bias towards a higher BP.
As for why remoteness from a popula-tion center might increase hypertension risk, the authors noted that Japanese liv-ing in rural areas might consume more traditional Japanese food, which has a higher salt content than the food of people living in urban areas. In discussing study limitations, the authors noted that their data did not allow for the assessment of other important risk factors for hyperten-sion, such as diet, education, income, and family history. ■
32 Renal & Urology News JUNE 2012 www.renalandurologynews.com
ANTIMICROBIAL LOCKS (AML) decrease the incidence of catheter-relat-ed bloodstream infections in hemo-dialysis (HD) patients, but they may result in the emergence of problematic pathogens, data show.
In a retrospective study, John J. Dixon, MD, and colleagues at St. Helier Hospital in Carshalton, Surrey, found that AML containing vancomycin and gentamicin significantly decreased the incidence of catheter-related bloodstream infections from 8.50 to 3.80/1,000 catheter-days. However, the proportion of Gram-positive bacteria, notably Staphylococcus aureus, increased signifi cantly with AML use, although the proportion of methicillin-resistant S. aureus and vancomycin resistance did not, the researchers reported online ahead of print in Nephrology Dialysis Transplantation.
Although their study demonstrates no increased risk of developing sub-sequent catheter-related bloodstream
infections with resistant organisms fol-lowing AML treatment, the risk is not eliminated completely, the investiga-tors observed. The most important predictor of early treatment failure of catheter-related bloodstream infections, they pointed out, appears to be the causative pathogen.
The study found that AML use was lined to increased gentamicin and cipro-fl oxacin resistance among Enterobacter species, but not among Pseudomonas species or Escherichia coli.
Dr. Dixon’s team noted that catheter-related bloodstream infections caused by S. aureus are highly pathogenic, with studies showing that it associated with 22% in-hospital mortality, rising to 32% at 90 days. Enterobacter bacter-emia has a mortality rate of 5%-20%, increasing to 44% in patients who develop endocarditis. “It seems logi-cal that resistant Enterobacter will be harder to treat with consequent higher mortality,” the authors stated.
“Given the prevalence of S. aureus and resistant Enterobacter, there is a need for a trial directly comparing the effective-ness of AML with non-antibiotic locks (e.g. citrate) in reducing CR-BSI,” they wrote. Non-antibiotic locks do not pro-mote antimicrobial resistance and may be more cost-effective, they noted.
The study included 927 HD patients, of whom 662 received vancomycin and gentamicin systemically as well as in an AML. The other 265 patients received only systemic vancomycin and gentami-cin and served as a control group.
The proportion of S. aureus cultures was 37.7% in the AML group com-
pared with only 28.6% of the control arm. In the AML group, 29.4% of Enterobacter isolates were resistant to gentamicin, 23.5% were resistant to ciprofl oxacin, and 15.7% were resistant to both drugs. In the control group, none of the Enterobacter isolates were resistant to gentamicin and 2.9% were resistant to ciprofl oxacin. None of the isolates was resistant to both drugs.
In addition, the researchers calculated that three patients needed to be treated with AML to prevent one catheter-related bloodstream infection.
The proportion of patients with acute kidney injury who developed catheter-related bloodstream infections in tun-neled hemodialysis catheters was lower than expected in both study arms.
Although the retrospective design of the study was its major limitation, the authors pointed out that the data collection method and contemporary analysis were robust enough to have not missed any data. ■
A Down Side to Antimicrobial LocksThey may result in more dangerous or harder-to-treat catheter-related bloodstream infections
Hypertension Risk Tied to Remoteness Perineural invasion (PNI) and post-treat-
ment PSA levels at 12 months strongly predict long-term PSA relapse-free surviv-al (PRFS) after defi nitive brachytherapy seed implantation for prostate cancer (PCa), according to a study.
William Ding, MD, of California Pacifi c Medical Center in San Francisco, and colleaguges studied 204 patients with localized PCa not previously treated with hormonal therapy. Of these pa-tients, 60%, 35%, and 2% had low-, intermediate-, and high-risk disease according to the National Comprehen-sive Cancer Network risk classifi cation system. Subjects had a median age of 69 years. They underwent I-125 or Pd-103 brachytherapy seed implanta-tion. The primary clinical outcome measure was PSA relapse according to the Phoenix defi nition (PSA nadir plus 2 ng/mL). The median follow-up was 80 months.
The fi ve-year PRFS for patients with PSA levels of 1 or less, 1.01-2.00, 2.01-3.00, and greater than 3.00 ng/
mL at 12 months was 98.5%, 85.7%, 61.5%, and 22.2%, respectively, the in-vestigators reported in the International Journal of Radiology, Biology, Physics (published online ahead of print). The 10-year PRFS for patients with PSA levels of 1.00 or less and 1.01-2.00 at 12 months was 90.5% and 85.7%, respectively.
In multivariate analyses, patients with a PSA level of 1.01-2.00, 2.01-3.00, and greater than 3.00 at 12 months had a 4.96, 27.57, and 65 times increased likelihood of long-term PSA relapse compared with men whose 12-month post-treatment PSA level was 1.00 or less. PNI was present in 5% of patients and it was associated with a 6.1 times increased risk of long-term PSA relapse compared with the absence of PNI.
Dr. Ding and his colleagues propose that in addition to traditional high-risk features, “the presence of positive PNI may play an important role in the standard risk assessment.” ■
Perineural Invasion Shows PSA Relapse Post-Brachytherapy
Researchers observe a greater likelihood of Staphylococcus aureus infections.

www.renalandurologynews.com JUNE 2012 Renal & Urology News 33
Anesthesiologists Surveyed About Catastrophic Errors
Results of a recent survey indicate that catastrophic medical errors can haunt practitioners for years.
The study, published in the journal Anesthesia & Analgesia, looked at the results of surveys sent to 1,200 randomly selected members of the American Society of Anesthesiologists to determine how physicians handle the emotional impact of surgical catastrophes. A total of 659 physicians (56%) completed the survey. Results indicated that most respondents (84%) had been involved in at least one unanticipated death or serious patient injury during surgery.
Alarmingly, although 67% of respond-ing physicians reported that their ability to provide patient care was impaired in the fi rst four hours following the event, and only 7% were given time off. Results also showed that 12% of respondents considered a career change after a surgical catastrophe. The authors concluded that surgical catastrophes can have a profound and lasting emotional impact on anes-thesiologists and may affect a physician’s ability to provide patient care following such an incident.
Six State Alone Payout Over 50% of Malpractice Claims
Diederich Healthcare, a medical mal-practice insurance company, recently released an analysis of medical mal-practice payments made in 2011, as recorded by the National Practitioner
Data Bank. By far, the state with the highest malpractice payout was New York, at $677,866,050, followed by Pennsylvania ($319,710,250), Illinois ($242,108,800), New Jersey ($221,170,750), Florida ($218,123,050) and California ($215,519,200). These six states together represent 51.4% of total payouts for 2011. States with the lowest payouts included South Dakota ($3,033,750), Vermont ($3,938,250), Wyoming ($4,235,000), North Dakota ($4,852,500), and Alaska ($6,347,500).
The majority of payments were made for patients between the ages of 40 and 59 ($1,351,743,100) followed by those between the ages of 20 and 30 ($786,317,650). Fifty-eight percent of the total payouts were for female patients. In more positive news, med-ical malpractice payouts have been dropping since they reached a high of $4,822,485,800 in 2003. The numbers for 2011 were slightly less than those in 2010.
Former Airman Sues U.S. for Medical Malpractice
In the most recent challenge to the Feres Doctrine, a former airman who lost his legs due to a botched gallbladder surgery is suing the U.S. government, the Air Force, and the David Grant Medical Center for medical malpractice.
The Feres Doctrine, based on a 1950 case, Feres v. United States, states that the federal government cannot be held liable for injuries arising from activities incident to military service. Basically, the doctrine is an extension of the com-mon law concept of sovereign immu-nity. Numerous challenges have tried to overturn the Feres precedent, but the Supreme Court has yet to overrule the verdict.
A 23-year-old airman who went in for a routine laparoscopic cholecys-tectomy just prior to being deployed overseas is bringing suit. He was treated at a local air force base medical cen-ter. During surgery, one of the operat-ing physicians lacerated the airman’s aorta, which caused a massive bleed in the retroperitoneal area. The surgi-cal team did not initially realize that
the patient’s aorta had been lacerated. Later in the operation as the airman’s blood pressure dropped precipitously, the operating team opened up the air-man’s abdomen to ascertain if there was an internal bleed. At that point, the doctors’ tried to repair the aortic tear with sutures, but by then more than two-thirds of the airman’s blood supply was gone.
After surgery, the airman was remanded to the intensive care unit. After several hours, the ischemia in both his legs was apparent—they were cold, pale, and mot-tled. The airman was then transferred to the University of California-Davis Medical Center. A vascular surgeon at the hospital determined that the aorta supplying blood to his legs had been blocked for too long and that necrosis had set in. The airman’s legs were subsequently amputated.
The airman and his wife are suing for at least $34.3 million in damages for pain, loss-of-earning capacity, physi-cal impairment, mental anguish, and disfigurement. The suit also seeks an
additional $20.5 million for the airman’s wife for loss of consortium and capacity to enjoy life.
Indemnity Payments Jack Up Malpractice Defense Costs
Defense costs for malpractice cases range widely among specialties, but invariably are higher for claims result-ing in indemnity payments, a recently published letter in The New England Journal of Medicine states.
Researchers at leading academic and medical institutions, and the RAND Corporation analyzed the defense costs associated with 26,853 malpractice claims closed between 1995 and 2005. Each claim contained information on whether or not a payment was made to a patient, the specialty of the physician involved, and the defense costs associ-ated with the claim. The defense costs analyzed included only items directly associated with the defense of the indi-vidual claim—expert-witness fees and fi ling costs. The mean defense cost was about $23,000. However, claims where an indemnity payment was made were associated with higher mean defense costs than those where no payment was made ($45,070 vs. $17,130).
Mean defense costs varied widely among specialties, the researchers found. Cardiologists had the highest defense costs: claims against cardi-ologists that resulted in an indemnity payment had a mean defense cost of $83,056. Oncologists had the sec-ond highest defense costs on record, with a mean of $78,890 for cases involving indemnity payments. Neurology, family general practice, psychiatry, obstetrics, internal medi-cine, and pediatrics were other special-ties typically associated with higher than average defense costs. The spe-cialties with the lowest defense costs were gynecology ($25,073), derma-tology ($24,007), and ophthalmol-ogy ($23,780). To see the full report on mean defense costs for paid and unpaid claims, according to physi-cian specialty, go to www.nejm.org/doi/full/10.1056/NEJMc1114805 Accessed May 10, 2012).
The authors of the study are careful to point out that though there is a sub -stantive variation in costs among spe-cialties, this variation is not necessarily the same as the difference in the fre-quency or size of claims. They conclude that “lowering the costs of dispute resolution could lead to considerable savings for physicians and insurers, particularly in specialties with high mean defense costs.” ■
Ms. Latner, a former criminal defense attorney, is a freelance medical writer in Port Washington, N.Y.
Malpractice News BY ANN W. LATNER, JD
© P
HOTO
TAKE
USA.
COM
/ C
ANAD
IAN
PRE
SS
© T
HIN
KSTO
CK.C
OM
/ S
TOCK
BYTE
A mistake made during routine surgery
led to this offi cer losing both his legs.
Many physicians consider a career
change after a surgical catastrophe.

34 Renal & Urology News JUNE 2012 www.renalandurologynews.com
T elemedicine, the use of electronic communication to provide health care, has been relatively slow
to catch on in some places, but many physicians who have incorporated tele-medicine into their practice believe it can be advantageous. It helps provide regular care to patients in remote areas, saves time for patients and providers, and increases effi ciency.
In interviews with Renal & Urology News, Larry Greenbaum, MD, PhD, Chief of Pediatric Nephrology at Children’s Healthcare in Atlanta, and Tejas Desai, MD, Assistant Program Director of the Internal Medicine Residency Program at the Brody School of Medicine at East Carolina University in Greenville share their experiences with telemedicine.
Extended reachChildren’s Healthcare of Atlanta (CHOA) has had enough success using telemedi-cine that it is continuously expanding the service, Dr. Greenbaum said. The hospital has an internal “hub” that con-nects to a network of sites funded and equipped by the Georgia Partnership of Telehealth. These sites are set up in rural areas, allowing patients to connect with distant doctors. Nephrologists affi li-ated with CHOA use the technology for outpatients. At each remote site, there is a “presenter,” which might be a nurse or physician assistant, who performs a routine physical exam that the physician can see and hear with specially equipped
stethoscopes, otoscopes, and ophthal-moscopes. The only part of the physical exam that cannot be easily transmitted is palpation of the abdomen.
Dr. Greenbaum said the technology provides access for families that might not be able to travel to Atlanta. Patients and parents do not need to miss a full day of school and work, respectively. It also allows them to monitor rural patients more frequently. “We can communicate by phone, but it’s just not the same as this kind of interaction,” he said.
Accessing a doctor when there is not one on hand is the main reason the Brody School of Medicine at East Carolina University in Greenville uses the technol-ogy said Dr. Desai. It allows doctors to be “in different places at the same time.”
Physicians, pharmacists, and residents all have either iPhones or iPads with cam-eras. If clinicians are with a patient and they need to connect with Dr. Desai or another senior-level physician, they log into the program FaceTime, which con-nects the two parties via video.
“We don’t use it as a way to eliminate us from the room. We use it so when someone junior is there, he can talk with me,” he said. “We can see more people in a faster amount of time and give them the feeling they have been taken care of.”
He uses it for talking with patients in a dialysis unit, lab follow ups, seeing a patient prior to discharge, summarizing information for family members, and to see a patient who cannot easily be moved.
He also communicates with patients via e-mail so they use an offi ce visit for things like lab results.
Reimbursement is one of the biggest challenges of telemedicine. A handful of states including California, Louisiana, Texas, Oklahoma, and Kentucky mandate reimbursement by private insurance for telehealth services. The reimbursement rates may vary and aren’t always equiva-lent to an in-person meeting.
Medicaid reimburses for telemedicine in many states. Medicare reimburses for ser-vices such as outpatient visits, nutritional counseling, kidney disease education, medication management and end-stage renal disease-related services—but only for rural patients.
Another disadvantage, according to Dr. Greenbaum, is the imperfect physi-cal exam. If clinicians suspect problems, they have to make sure the patient gets a hands-on exam by another physician.
Telemedicine should be avoided when patients have emergency needs, Dr. Desai said. It also should not be used for “really bad news” or as a replace-ment for a daily face-to-face visit with hospitalized patients.
Telemedicine tipsSpeak with someone experienced in using telemedicine prior to implementing
a program, said Dr. Desai, who offers the following advice:
Document all e-mails in a patient’s • health record. Video conferences can also be recorded, saved, and uploaded into their record. Only allow video conferencing from • 9 a.m. to 5 p.m. Require patients to initiate communi-• cation and agree to check it afterward for his response. Patients should be informed that serious issues should be handled by telephone and if their e-mail will not be answered weekends. Drs. Desai and Greenbaum do
not recommend using programs like Skype for patient visits. The image quality isn’t exactly great, and there is no reimbursement for a consult here (because there is no physical exam), Dr. Greenbaum said.
Dr. Greenbaum noted that he and his colleagues are fortunate to have the infrastructure they do. “I think it obviously makes sense with what I’m doing—outpatient visits with patients coming from a signifi cant distance,” he said. “For people who have a practice that has a wide geographic coverage area it works really nicely.” ■
Tammy Worth is a freelance medical jour-nalist based out of Blue Springs, Mo.
Practice ManagementTelemedicine can offer a number of distinct advantages, but its use is not appropriate in certain circumstances BY TAMMY WORTH
Telemedicine allows doctors to consult with other experts across a wide geographic area.
© T
HIN
KSTO
CK /
HEM
ERA
Resources for TelehealthThe Telehealth Resources Center provides a wealth of information on every-thing from training to staffi ng and legal issues to reimbursement information on its site at www.telehealthresourcecenter.org/operations-tools.
A Medicare reimbursement checklist for telehealth professional fees can be found online at www.nrtrc.org/wp-content/uploads/CMSTelehealthProfessionalFees2011.pdf. The document highlights requirements for Medicare reimbursement, the services that are covered and their codes.

www.renalandurologynews.com JUNE 2012 Renal & Urology News 35
BY ANTHONY J. BLEYER, MD
CASE INTRODUCTION:hypertension, high blood cholesterol, and gout
Mr. F, a 58-year-old man, presents for evaluation of gout. The patient fi rst devel-oped gout attacks approximately 10 years ago. Mr. F has a history of hypertension and hypercholesterolemia treated with atorvastatin. He also has a history of cal-cium oxalate renal calculi.
Physical examination shows the patient is obese (body mass index, 33.5 kg/m2). His blood pressure is 130/85 mm Hg. Mr. F’s pulmonary and cardiac exami-nations are normal. He has no edema. He has tophi, approximately 0.5 cm in diameter, on several fi ngers, and a 2 cm tophus on both the right and left elbows. Mr. F has seen several physicians over the years who told him that he “just had to live with” his condition, and that his unhealthy diet was contributing to his gout.
For the past 3 years, the gout attacks had become more frequent and the patient had developed worsening tophi that occa-sionally drain. Mr. F has been treated with colchicine and frequent courses of predni-sone. He would like to stay on prednisone long-term for his condition. He says he was on allopurinol in the past, but cannot remember why it was stopped.
Discussion: addressing lifestyle and medical issues Gout is often perceived as a lifestyle disease, primarily the result of overeating purine-rich foods. While the clinician needs to evaluate dietary factors, it is also important to look at both lifestyle and medical issues that contribute to the disorder. The clinician should view gout as an opportunity to infl uence lifestyle choices and also to uncover any hidden medical conditions that may contribute to hyperuricemia.
CME FEATURE
Part III: Clinical Challenges and Renal Considerations in Managing GoutA case study involving a 58-year-old man with acute gout attacks and multiple comorbidities, including hypertension and hypercholesterolemia
Anthony J. Bleyer, MD is Professor of Medicine in the
Section of Nephrology at Wake Forest University School of Medicine in
Winston-Salem, N.C. Dr. Bleyer’s clinical interests include the management of
gout in patients with CKD.
This is the third part of an ongoing series profi ling case-based challenges in gout management with particular emphasis on renal considerations therein. To see parts I and II, please visit us online at www.mycme.com/marchgout and www.mycme.com/aprilgout or look at our March and April 2012 issues.
Release Date: June 2012Expiration Date: June 2013Estimated time to complete the educational activity: 1 hourThis activity is jointly sponsored by Medical Education Resources and Haymarket Medical Education and is supported by an educational grant from Savient Pharmaceuticals.STATEMENT OF NEED: Clinicians today face an increasing number of patients with gout. Nephrologists in particular must contend with complex cases in patients with varying degrees and stages of renal dysfunction in addition to other comorbidities and individual characteristics that affect treatment decisions and, ultimately, treatment success. As gout occurs in tandem with renal disorders, nephrologists must be able to appropriately identify and treat these patients.TARGET AUDIENCE: This activity has been designed to meet the educational needs of nephrologists and other clinicians involved in the treatment of patients with gout. EDUCATIONAL OBJECTIVES: After completing the activity, the participant should be better able to:
Describe how renal function affects the management of gout.• Evaluate current and emerging options for urate-lowering therapy with regard to their benefi ts • and limitations in patients with varying degrees of renal impairment.Discuss ways to motivate patient adherence to a long-term treatment plan that incorporates • lifestyle considerations and pharmacotherapy.
ACCREDITATION STATEMENT: This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Medical Education Resources (MER) and Haymarket Medical Education. MER is accredited by the ACCME to provide continuing medical education for physicians.CREDIT DESIGNATION: Medical Education Resources designates this enduring material for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.DISCLOSURE OF CONFLICTS OF INTEREST: Medical Education Resources ensures balance, independence, objectivity, and scientifi c rigor in all our educational programs. In accordance with this policy, MER identifi es confl icts of interest with its instructors, content managers, and other individuals who are in a position to control the content of an activity. Confl icts are resolved by MER to ensure all scientifi c research referred to, reported, or used in a CME activity conforms to the generally accepted standards of experimental design, data collection, and analysis. MER is committed to providing its learners with high-quality CME activities that promote improvements or quality in health care and not a commercial interest.
The faculty reported the following fi nancial relationships with commercial interests whose products or services may be mentioned in this CME activity:
Name of Faculty Reported Financial Relationship • Anthony J. Bleyer, MD Consultant: Takeda Pharmaceuticals, Savient Pharmaceuticals
The content managers, Krista Sierra, Susan Basilico, Jody A. Charnow, and Marina Galanakis of Haymarket Medical Education, and Victoria C. Smith, MD, of Medical Education Resources, have disclosed that they have no relevant fi nancial relationships or confl icts of interest.METHOD OF PARTICIPATION: There are no fees for participating in and receiving CME credit for this activity. During the period June 2012 through June 2013, participants must: 1) read the learning objectives and faculty disclosures, 2) study the educational activity, 3) complete the posttest and submit it online. Physicians may register at www.myCME.com/junegout (June 2012), and 4) complete the evaluation form online.A statement of credit will be issued only upon receipt of a completed activity evaluation form and a completed post-test with a score of 70% or better.

36 Renal & Urology News JUNE 2012 www.renalandurologynews.com
While asking patients about their habits, particular attention should be paid to alcohol intake. Consumption of alcohol, especially beer, may be excessive and the patient may require counseling in this regard.
CASE: assessing dietary factors
Mr. F drinks four to fi ve beers per week. He eats out frequently at fast-food restau-rants and does enjoy beef and seafood. However, he states that avoiding these foods in the past failed to decrease the frequency of his gout attacks.
Discussion: purine-rich foods and metabolismBeer has a high content of guanosine, a purine that is converted to uric acid. In addition, alcohol increases the degrada-tion of adenosine triphosphate (ATP) to adenosine monophosphate (AMP), resulting in increased uric acid produc-tion.1 Thus, beer is associated with a much higher incidence of hyperuricemia; liquor has only a modest effect, and wine is neu-tral. It would seem prudent to probe into the individual’s history and risk for alco-holism rather than suggesting a change from beer to hard liquor or wine.
All forms of meat—especially beef and organ meats—are high in purine content and can contribute to gout. Sandwich meat and hot dogs also have a high purine content. Men who are in the highest quintile of meat intake have a 41% increased chance of developing gout.2 Seafood—especially shellfi sh—also has a high purine content. Vegetables with a high purine content—for example, spinach, mushrooms, and peas—do not increase the risk of gout for reasons that are not clearly understood.
The dietary history may uncover causes of overproduction of uric acid; however, the medical and family histories are more likely to identify reasons for underex-cretion of uric acid. Underexcretion of uric acid, as defi ned by a low fractional excretion, is present in most individuals with gout.
Urate is freely fi ltered at the glomeru-lus. Urate reabsorption occurs in the proximal tubule. A number of organic anion transporters participate in proximal tubular urate reabsorption. How these transporters function together is not com-pletely understood, but there are several aspects of proximal urate transport that are known and of importance to clinical nephrologists.
One important consideration is that there are slight variations at the DNA level in the genes for urate transporters in the population. For example, large population studies have identifi ed poly-morphisms in the gene ABCG2 as a cause of hyperuricemia.3 The function of this gene had previously been unidentifi ed, but this study led to further investigations identifying ABCG2 as a high effl ux urate transporter. Polymorphisms in this gene may be responsible for up to 10% of gout cases.3 These small changes can affect the ability of the urate transporters to reabsorb urate. Such genetic differences between individuals are likely to explain why some individuals are underexcreters of urate vs. other individuals with normal urate excretion.
Another important clinical aspect of urate tubular transport is that urate reabsorption is tightly linked to sodium reabsorption. Factors that increase sodium reabsorption will increase urate reabsorption. These factors include volume depletion, the use of diuretics, and congestive heart failure. Similarly, patients with decreased proximal tubular absorption of sodium will have low serum uric acid levels. For example, in hyponatremia due to volume deple-tion, the serum urate level will tend to be high. In patients with hyponatremia due to the syndrome of inappropriate antidiuretic hormone excess, patients are mildly volume-expanded, with decreased proximal sodium reabsorption resulting in lower serum urate levels.
CASE: patient history
Mr. F has a 5-year history of hypertension, for which he has been receiving hydro-
chlorothiazide. He was on a low-sodium diet. He has also suffered from nephro-lithiasis with several calcium oxalate renal calculi in the last fi ve years. Mr. F has no history of kidney disease. His father and two uncles also suffered from gout but they did not have kidney disease.
Discussion: comorbidities affecting hyperuricemiaThe medical history has revealed sev-eral conditions associated with gout. An association between hypertension and gout has long been documented. The use of hydrochlorothiazide increases distal tubular sodium excretion, which leads to a secondary increase in proximal tubu-lar sodium reabsorption. The increased proximal tubular sodium reabsorption secondarily leads to increased urate reab-sorption and hyperuricemia.4
Nephrolithiasis is also highly asso-ciated with gout. Patients who expe -rience urate overproduction excrete increased levels of urate in the urine. While a high urinary urate excretion is a risk factor for uric acid calculi, an even more important determinant is urinary pH owing to the solubility of urate vs. uric acid and the pKA of uric acid. There is a signifi cant difference in the solubility of urate vs uric acid, with urate having a solubility of 158 mg/dL, and uric acid having a solubility of only 8 mg/dL. The pKA of uric acid is 5.7. This means that at a pH of 7, 95% is present as urate (very soluble), and at a pH of 5, about 80% is present as uric acid (very insoluble).
Shifting pH can change uric acid solu-bility by almost a factor of 20.5 Dietary factors such as excess meat in the diet will not only increase uric acid produc-
tion but will also decrease urinary pH, resulting in an increased potential for uric acid calculi.5,6
In addition, there is an increased risk of calcium oxalate calculi in patients with hyperuricosuria, as uric acid acts as a pro-moter for calcium oxalate stone formation, with approximately 20% of patients with calcium oxalate nephrolithiasis having urinary urate excretions of >800 mg/d (men) and >750 mg/d (women).5 Excess consumption of meat causes increased uric acid production as well as increased urinary acidity, thereby increasing the risk of calcium oxalate calculi.
In a double-blind randomized study,6 60 patients suffering from recurrent cal-cium oxalate calculi, hyperuricosuria, and normocalciuria were randomized to allopurinol (300 mg/d) vs. placebo. In this study, the mean rate of subsequent calculous events was 0.26 per patient-year in the placebo group and 0.12 in the allopurinol group (P<0.02). While allopurinol is currently only indicated in the treatment of symptomatic gout, one needs to consider this possible benefi t in patients with the disease.
While 24-hour urine collections are not necessary in the management of most patients with gout, in diffi cult cases such as this, it is important to understand the pathophysiology of urate excretion. Random spot urine uric acid:creatinine ratios have been found to be unreliable in predicting 24-hour urinary uric acid excretion due to diurnal variation. For this reason, one must consider obtaining a 24-hour collection for uric acid and creatinine with a simultaneous measure-ment of uric acid excretion. A 24-hour excretion of greater than 700 mg of uric acid is the diagnostic threshold for urate overproduction.7
CASE: identifying urate overproduction
In 24 hours, the patient produces one liter of urine containing 800 mg of uric acid and 1500 mg of creatinine. The serum uric acid level is 9.5 mg/dL, and the serum creatinine is 0.9 mg/dL.
Discussion: understanding high serum urate levels The results indicate that the patient has a high daily uric acid excretion of 800 mg. As he is in a relatively steady state, the amount produced will be equal to the amount excreted. The fractional excretion of uric acid in this patient is
CME FEATURE
The x-ray above shows pronounced tophi (in red) affecting several proximal- and distal-interphalangeal joints in each hand.
© B
IOPH
OTO
ASS
OCI
ATES
/ P
HOTO
RES
EARC
HERS
, IN
C.

www.renalandurologynews.com JUNE 2012 Renal & Urology News 37
(800/9.5) / (1500/0.9) = 0.05%, which is low.
Thus, there are two factors that are contributing to the high serum uric acid levels observed in this patient. He pro-duces excessive uric acid (800 mg/dL; at the same time, he reabsorbs more uric acid than normal, leading to a low frac-tional excretion of urate.
Uric acid excretion is very high in infancy and about 8% to 20% during childhood. With puberty, there is a decline in the fractional excretion of uric acid in men, but not in women, resulting in an increase in serum uric acid relative to women. After meno-pause, the fractional excretion of uric acid is similar between men and women. The low fractional excretion of uric acid, in addition to the relative increased dietary protein intake in men, results in an increased incidence of gout in men vs. women. In an observational study of 100 patients with gout vs. 72 controls,7 the mean fractional excretion of urate was 4.6 ± 1.2 mg/dL in gout patients and 7.6 ± 1.9% in controls.
For unclear reasons, patients with increased urinary uric acid excretion frequently have low fractional excre-tions of uric acid as well.7
An interesting note in this patient is the low urinary output. This low urinary excretion places the patient at increased risk of kidney stones, as decreased urinary output has consistently been associated with an increased risk of renal calculi. In addition, increased water intake has been associated with a decreased risk of development of gouty attacks.
There are two important condi -tions that the nephrologist should con-sider in patients with chronic kidney disease, hyperuricemia, and decreased fractional excretion of uric acid. First, lead poisoning has been well associated with both gout and chronic kidney disease. Lead poisoning can be due to lead exposure to paint that was produced many years ago or from occupational exposure. This is less com-mon today.
Another important consideration is mutation in the UMOD gene encoding uromodulin (Tamm-Horsfall protein) as a cause of gout and chronic kidney disease.8 In this condition, production of abnormal uromodulin in the thick ascending limb results in defective func-tion of the thick ascending limb and impaired sodium reabsorption. The
impaired sodium reabsorption leads to increased proximal tubular sodium (and secondarily urate) reabsorption. Patients usually present with gout in the teenage years, but attacks can begin at any age.
Chronic kidney disease with a bland urinary sediment and absence of protei-nuria occurs during the third through seventh decades of life. Clues to the diagnosis include a very strong family history of gout and kidney disease. Mutational analysis is available in many clinical genetics laboratories.
At this point, the clinician had a good understanding of the pathophysiol-ogy of the patient’s gout and initiated prolonged discussion with the patient about potential treatments.
CASE: chronic debility
Mr. F stated that he had suffered from gout for about 10 years. Over the last fi ve years, he has become increas-ingly debilitated with the development of tophi on the feet and both hands. Mr. F, an accountant, has acknowledged that the pain from the tophi now sub-stantially hinders his job performance. The patient was tearful in his discussion about how the progressive gout has not only affected his professional life but decreased his ability to do many things outside of the home.
Discussion: indications and options for treatmentIndications for the treatment of chronic gout are based on attack frequency and severity, uric acid burden, and prognosis. Gout attacks occurring less than once per year may respond well to symptomatic care. Many patients would opt for symptomatic treatment of acute events together with lifestyle modifi cation rather than chronic medi-cation. On the other hand, individuals who are very active may fi nd even infre-quent gout attacks a burden and desire preventive treatment. Patients with more frequent attacks are more likely to favor preventive care; the decision is a personal one that must be discussed between the patient and clinician. The risk of developing another gout attack is also associated with higher serum urate levels; this should be taken into account when discussing therapy. For a patient with mild gout and a mildly elevated serum urate level, preventive therapy may not be required.
In this patient with severe tophaceous gout, it is likely that the uric acid burden will increase over time and that attacks will become more frequent. Prevention with attempts to signifi cantly lower serum urate levels are required in this case, since an increased body burden of uric acid will result in an increased risk of gout in the future.
Mr. F has been treated chronically with colchicine and prednisone. These two medications decrease infl amma-tion and prevent gout attacks; in the meantime, however, the body’s uric acid burden will increase, and tophi can increase in size.
Prednisone is an unacceptable agent for long-term gout management,
because of the potential for toxicities over time. Colchicine, which is no lon-ger generic, is now quite expensive, and chronic therapy with this agent may result in myopathy and other adverse effects. For this reason, treatment should focus on decreasing the body’s burden of urate.
In patients whose hyperuricemia is solely due to underexcretion of urate, probenecid is a possible alternative to lower serum urate levels. This agent is not used as frequently in the United States as in other countries. A 24-hour urine collection should be obtained prior to usage to rule out uric acid overproduction. Urine output must remain high, and urine pH should be monitored to prevent the development of uric acid stones. For this patient, probenecid would not be a good choice because he is overproducing uric acid, has renal calculi, and produces low urinary volume.
There are three agents that are of potential benefi t in the treatment of this patient’s gout: allopurinol, febuxostat, and pegloticase.
Allopurinol and febuxostat are both xanthine oxidase inhibitors. They pre-vent hypoxanthine and xanthine metab-olism to uric acid, and as such function to decrease serum uric acid levels.
Allopurinol should be given primary consideration in the treatment of gout
because it is inexpensive and has been used for many years. Dosage usually starts at 100 mg/d and is titrated up to 300 mg/d. The initial lowering of serum urate levels that accompanies the administration of allopurinol and febuxostat has been associated with the development of acute gout attacks. Patients are at risk for these attacks after allopurinol or febuxostat initiation for up to 6 months. Educating the patient about the potential for acute attacks and the prescribing of a glucocorticoid dose pack may be indicated.
Prophylaxis with colchicine or non-steroidal agents may also be consid-ered, though these agents may not be appropriate in patients with a decreased
glomerular fi ltration rate. Prophylaxis with prednisone is not recommended but in an extreme case such as this patient’s, it may be considered for a short period of time.
At usual doses, allopurinol does not lower serum uric acid levels as much as febuxostat. Some physicians, especially rheumatologists, are more comfortable prescribing doses of allopurinol up to 800 mg/d in individuals with “normal” kidney function.9 It is unclear if this places patients at increased risk of toxicity or the severe allergic reactions that have been documented with allopurinol.
Febuxostat appears to be more potent and at routine doses has been found to be more effective than allopurinol. Febuxostat is not a purine analogue; as such, patients may not be at risk of developing the severe hypersensitiv-ity reactions that have been seen with allopurinol. In a study of 762 hyperu-ricemic patients10 assigned to febuxo-stat (80 mg or 120 mg) or allopurinol (300 mg) daily for one year, the primary end point of a serum urate level less than 6 mg/dL was reached in 53% of patients receiving 80 mg of febuxostat, 62% of patients receiving 120 mg of febuxostat, and in 21% of individuals receiving 300 mg of allopurinol (P<.001).
Pegloticase is a pegylated uric acid- specifi c enzyme that is indicated for chronic gout in adult patients who are
CME FEATURE
Indications for the treatment of chronic gout are based on the frequency and severity of fl are-ups, uric acid burden, and prognosis.

38 Renal & Urology News JUNE 2012 www.renalandurologynews.com
CME FEATURE
DISCLAIMER: The content and views presented in this educational activity are those of the authors and do not neces-sarily refl ect those of Savient Pharmaceuticals, Medical Education Resources, or Haymarket Medical Education. The authors have disclosed if there is any discussion of published and/or investigational uses of agents that are not indicated by the FDA in their presentations. The opinions expressed in this educational activity are those of the faculty and do not necessarily represent the views of Savient Pharmaceuticals, Medical Education Resources, or Haymarket Medical Education. Before prescribing any medicine, primary references and full prescribing information should be consulted. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications on dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities. The information presented in this activity is not meant to serve as a guideline for patient management.
CME Post-testExpiration Date: June 2013Medical Education Resources designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Participants should claim only the credit commensurate with the extent of their participation in the activity. Physician post-tests must be com -pleted and submitted online. Physicians may register at no charge at www.myCME.com/junegout. You must receive a score of 70% or better to receive credit.
1. Pegloticase:Is a form of uricase used to treat tumor lysis syndromea. Is an oral medication that rapidly decreases serum urate levelsb. Is an intravenous formulation that rapidly decreases serum urate levelsc. Has the same mechanism of action as allopurinold.
2. The primary cause of gout in the general population is:Consumption of high-purine-content foodsa. Underexcretion of uric acidb. Overproduction of uric acidc. Both under-excretion and over-production of uric acidd.
3. In a patient with renal calculi containing calcium oxalate:Increased consumption of meat increases urinary acid secretion, a. increasing the risk of calculi.In one study, treatment with allopurinol decreased hyperuricosuria b. and decreased stone formation in calcium oxalate stone formers with hyperuricosuria.Increased fl uid intake will decrease the risk of stone formation.c. All of the aboved.
4. In individuals receiving pegloticase infusions:Decreased effi cacy of pegloticase in lowering serum uric acid levels is a. associated with the development of allergic reactions with infusion.Allergic reactions usually develop only after many months of therapy.b. It usually takes 4 to 6 weeks to see a decline in serum urate levels.c. As uric acid levels drop so quickly, an exacerbation of gout fl ares does d. not occur.
5. Which of the following is the best dietary recommendation to lower serum urate levels?
Stop drinking liquor and switch to red winea. Stop drinking beer and switch to milkb. Stop eating hamburgers and switch to seafood and shellfi shc. Decrease sodium in the dietd.
6. Patients with a mutation in the gene encoding uromodulin:Often develop gout in middle age and kidney failure in their 80sa. Often develop gout in their teenage years and 20s and proceed to dialysis b. in their 40sDo not have gout, but develop kidney failure in their 40sc. Develop both gout and kidney failure in childhoodd.
7. Which of the following conditions does NOT result in hyperuricemia?Congestive heart failurea. Volume depletionb. Lead poisoningc. Syndrome of inappropriate antidiuretic hormone excessd.
refractory to conventional therapy. Most animal species have the enzyme uricase, which converts uric acid to allantoin, which is benign and soluble. Humans do not produce this enzyme.11
Administering uricase to humans is immunogenic and results in the rapid production of antibody. Therefore, investigators developed a porcine uricase enzyme that was surrounded by methoxy polyethylene-glycol.
Due to the need for intravenous admin-istration every two weeks and the rate of anaphylactic reactions, pegloticase is reserved for more severe, refractory cases of gout or in individuals who cannot tol-erate other treatments. When antibodies do not render pegloticase inactive, it dramatically lowers serum urate levels and is extremely effective in tophaceous gout in patients in whom allopurinol or febuxostat cannot be given.12
Two replicated randomized prospective studies have been done with pegloticase.13 These studies enrolled 225 patients with serum urate levels ≥8 mg/dL with chron-ic gout refractory to other medications. Patients were randomized to placebo, a pegloticase dose of 8 mg every two weeks, or a pegloticase dose of 8 mg every four weeks. All patients received colchicine or nonsteroidal prophylaxis and received fexofenadine on the night prior and the morning of infusion, as well as 200 mg of hydrocortisone immediately before treatment. Serum uric acid levels fell to less than 6 mg/dL in 42%, 35%, and 0% of individuals in the two-week, monthly, and placebo groups. Serum uric acid levels fell precipitously within 24 hours of the fi rst infusion. Resolution of at least one tophus occurred in 40% of those receiving pegloticase every two weeks. Unfortunately, antibodies devel-oped in nearly 90% of those receiv-ing active drug, and 41% developed an inability to respond to pegloticase. The patients who sustained a loss of the urate-lowering effect of pegloticase were especially at high risk of developing infusion reactions. The loss of response to pegloticase usually occurred within the fi rst four months of therapy.
Thus, pegloticase represents a new therapeutic agent that can be dramati-
cally effective in reducing tophus size and treating gout; however, development of antibodies may reduce its effi cacy in a substantial proportion of patients. Instead of prescribing this medication infrequently, it is probably better to refer patients to a physician with expertise in its use.
CASE: patient summary
As Mr. F had previously been on allopurinol and developed a question-able rash, he opted to receive febuxostat. In conjunction, he is changing his diet and has been placed on losartan (which decreases proximal tubular reabsorption of urate) instead of hydrochlorothiazide for gout. He is considering starting peg-loticase if he does not notice a decrease in the size of his tophi.
Due to the severe nature of his gout and the risk of future gout attacks, Mr. F was also referred to a rheuma-tologist for help in management of his arthritis and the potential use of pegloticase. ■
REFERENCES
1. Choi HK, Mount DB, Reginato AM. Pathogenesis of gout. Ann Intern Med 2005;143:499-516.
2. Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N Engl J Med 2004;350:1093-1103.
3. Woodward OM, Kottgen A, Coresh J, Boerwinkle E, Guggino WB, Kottgen M. Identifi cation of a urate transporter, ABCG2, with a common functional polymorphism causing gout. Proc Natl Acad Sci U S A 2009;106:10338-10342.
4. Iwaki K, Yonetani Y. Decreased renal excretion of uric acid following diuretic administration in rats. Jpn J Pharmacol 1984;34:389-396.
5. Coe FL, Parks JH. Nephrolithiasis: Pathogenesis and Treatment. 2nd ed. Chicago: Yearbook Medical Publishers; 1988.
6. Ettinger B, Tang A, Citron JT, Livermore B, Williams T. Randomized trial of allopurinol in the prevention of calcium oxalate calculi. N Engl J Med 1986;315:1386-1389.
7. Perez-Ruiz F, Calabozo M, Erauskin GG, Ruibal A, Herrero-Beites AM. Renal underexcretion of uric acid is present in patients with apparent high urinary uric acid output. Arthritis Rheum 2002;47:610-613.
8. Hart TC, Gorry MC, Hart PS, et al. Mutations of the UMOD gene are responsible for medullary cystic kidney disease 2 and familial juvenile hyperuricaemic nephropathy. J Med Genet 2002;39:882-892.
9. Neogi T. Gout. N Engl J Med 2011;364:443-452. 10. Becker MA, Schumacher HR, Jr., Wortmann RL
et al. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. N Engl J Med 2005;353:2450-2461.
11. Johnson RJ, Titte S, Cade JR, Rideout BA, Oliver WJ. Uric acid, evolution and primitive cultures. Semin Nephrol 2005;25:3-8.
12. Sundy JS, Baraf HS, Yood RA, et al. Effi cacy and tolerability of pegloticase for the treatment of chronic gout in patients refractory to conventional treatment: two randomized controlled trials JAMA 2011;306:711-720.

Hundreds of activities.
Dozens of therapeutic areas.
Take a closer look at myCME, the fastest growing online CME/CE resource, now available on your mobile device.
For more information go to myCME.com/app.
© Haymarket Medical Education, LP 2012. All rights reserved.
myCME.com
myCME my App
Download it today!