Embed Size (px)
DESCRIPTION
Clinical news for nephrologists and urologists.
Citation preview

CME FEATURE
IN THIS ISSUE
3 Pulmonary hypertension in HD patients hikes death risk
8 Renal decline associated with TNF receptors
9 HD patients are at higher risk for herpes zoster
13 Heavy alcohol use may raise prostate cancer risk
13 Empiric antibiotics for elevated PSA not warranted
24 Men with ED more likely to have atopic dermatitis
27 Web-based tools are enhancing donor screening
Adrenal CT scan showing adenoma
PAGE 23
Earn 1 CME credit in this issue
Clinical Challenges and Renal Considerations in Managing GoutPAGE 28
CKD Incidence Higher in BlacksRESEARCHERS WHO analyzed 20-year follow-up data from a prospec-tive study found that African Americans have a higher incidence of chronic kid-ney disease (CKD) than whites in part because of albuminuria.
“This fi nding provides an important contrast to cross-sectional studies reporting a higher CKD prevalence
among whites compared with African Americans,” the authors concluded in a paper published in the Clinical Journal of the American Society of Nephrology (2012;7:101-107).
The study compared the incidence of CKD among young African-American and white adults who participated in
BY JODY A. CHARNOWSAN FRANCISCO—Two studies com-paring various treatment modalities for prostate cancer (PCa) could help doc-tors and patients make more informed treatment decisions, according to pre-sentations at the 2012 Genitourinary Cancers Symposium.
In one study, investigators led by Ronald C. Chen, MD, Assistant Professor of Radiation Oncology at the University of North Carolina in Chapel Hill, found that proton therapy is no better than intensity modulated radiotherapy (IMRT) as a treatment for localized PCa, and it is associated with greater gastrointes-tinal (GI) toxicities. The other study, led by Jay P. Ciezki, MD, a staff mem-ber of the Department of Radiation Oncology at Cleveland Clinic, dem-onstrated that brachytherapy is less toxic and less costly than either external beam radiotherapy (EBRT) or radical prostatectomy (RP).
continued on page 10
Proton Beam Superiority Questioned
© S
PL /
PHO
TO R
ESEA
RCHE
RS, I
NC.
BY JODY A. CHARNOWSAN FRANCISCO—A novel medication may provide a new standard of care for the treatment of patients with castration-resistant prostate cancer (CRPC) and bone metastases, researchers conclud-ed in a presentation here at the annual Genitourinary Cancers Symposium.
In a phase 3 study, radium-223 chlo-ride (Alpharadin)—a first-in-class drug—signifi cantly prolonged overall survival and time to fi rst skeletal event (SRE) in CRPC patients with bone metastases, according to lead investi-gator Chris Parker, MD, of The Royal Marsden NHS Foundation Trust in Sutton, U.K. The drug was well toler-ated and associated with a low inci-dence of bone toxicities.
“Radium-223 is, chemically-speaking, like calcium, so it localizes to bone, and specifi cally to bone metastases,” Dr. Parker said. “And radium-223 is an alpha emitter, so once in the bone it emits alpha particles, which are highly lethal and highly localized because they are very, very short range.”
Researchers analyzed data from 809 patients randomized to receive radium-223 (541 men) or placebo (268 men). The primary endpoint was overall survival.
The median overall survival was 14 months in the radium-223 group com-pared with 11.2 months in the placebo recipients, which translated into a 30% decreased death risk. The median time to fi rst SRE was 13.5 months in the
Radium Drug Called ‘A Big Deal’ for PCaRadium-223 is much less toxic to bone than other radioactive bone-targeting drugs
M A R C H 2 0 1 2 ■ ■ ■ V O L U M E 1 1 , I S S U E N U M B E R 3 ■ ■ ■ www.renalandurologynews.com
continued on page 10
continued on page 10
A NEW DRUG for PCa bone metastases (shown above) prolonged overall survival.

www.renalandurologynews.com MARCH 2012 Renal & Urology News 3
PULMONARY hypertension is com-mon in hemodialysis (HD) patients and it is associated with an increased death risk, a study found.
In a study led by Rajiv Agarwal, MD, of the Indiana University School of Medicine in Indianapolis, pulmonary hypertension was present in 110 (38%)
of 288 HD patients, according to a report in Nephrology Dialysis Transplantation (published online ahead of print). Dr. Agarwal defi ned pulmonary hyperten-sion as an estimated systolic pulmonary artery pressure greater than 35 mm Hg using echocardiograms performed with-in an hour after the end of dialysis.
Over a median follow-up period of 2.1 years, 97 patients (34%) died, for a crude mortality rate of 114.2 per 1,000 patient-years. Of these, 58 deaths occurred among the 110 patients with pulmonary hyper-tension and 39 occurred among subjects without it. After adjusting for multiple variables, pulmonary hypertension sig-
nifi cantly and independently predicted a twofold increased risk of all-cause mortal-ity. Pulmonary hypertension was strongly associated with an enlarged left atrium.
“Reducing left atrial size such as through volume control may be an attractive target to improve pulmonary hypertension,” Dr. Agarwal concluded. ■
Pulmonary Hypertension Common in HD Patients
PROVENGE® (sipuleucel-T)Suspension for Intravenous Infusion Rx Only
BRIEF SUMMARY — See full Prescribing Information for complete product information
INDICATIONS AND USAGE: PROVENGE® (sipuleucel-T) is an autologous cellular immunotherapy indicated for the treatment of asymptomatic or minimally symptomatic metastatic castrate resistant (hormone refractory) prostate cancer.
DOSAGE AND ADMINISTRATION For Autologous Use Only.
diphenhydramine.
the infusion bag.Do Not Initiate Infusion of Expired Product.
Do Not Use a Cell Filter.
(See Dosage and Administration [2] of full Prescribing Information.)
CONTRAINDICATIONS: None.
WARNINGS AND PRECAUTIONS
PROVENGE is intended solely for autologous use.
Acute infusion reactions
following the third infusion. Some (1.2%) patients in the PROVENGE group were
PROVENGE group.
administered as needed.
Handling Precautions for Control of Infectious Disease. PROVENGE is notleukapheresis material and PROVENGE may carry the risk of transmitting infectious
should be followed.
Concomitant Chemotherapy or Immunosuppressive Therapy. Use of either
with PROVENGE.
Product Safety Testing. PROVENGE is released for infusion based on the microbial
Dendreon will notify the treating physician. Dendreon will attempt to identify the
and communicate the results to the treating physician. Dendreon may request additional information from the physician in order to determine the source of contamination.
(See Warnings and Precautions [5] of full Prescribing Information.)
ADVERSE REACTIONS
mononuclear cells.
included acute infusion reactions (see Warnings and Precautions)
tumor flare.
number of these patients discontinued treatment as a result. Monitoring for infectious
were Caucasian.
Table 1 Incidence of Adverse Events Occurring in ≥5% of Patients Randomized to PROVENGE
Any Adverse EventChillsFatigue
NauseaJoint acheHeadacheCitrate toxicityParesthesiaVomiting
ConstipationPainParesthesia oralPain in extremity
Muscle ache
Diarrhea
Musculoskeletal painDyspneaEdema peripheralHot flushHematuriaMuscle spasms
591 (98.3)
247 (41.1)
186 (30.9)
7 (1.2)
291 (96.0) 97 (32.0)
All Gradesn (%)
All Gradesn (%)
Grade 3-5n (%)
Grade 3-5n (%)
PROVENGE (N = 601) Control* (N = 303)
(Table 1 continued on next page.)

4 Renal & Urology News MARCH 2012 www.renalandurologynews.com
Stents May Benefit Renal Transplant PatientsUreteral stents in recipients of deceased donor organs lower the risk of ureteral complications
RECIPIENTS OF deceased donor kid-neys who have ureteral stents implanted are at lower risk of ureteral complica-tions, but are more likely to experience urinary tract infection (UTI), according to researchers.
In a study of 961 renal transplant recipients—310 with ureteral stents and 651 without the stents—investiga-tors found that the ureteral complica-tion rate was 1.9% in stent recipients compared with 5.8% of those without
stents. After adjusting for confounders, the stent group overall had a signifi cant 60% decreased risk of ureteral compli-cations. Further analysis revealed that stents benefi ted primarily recipients of deceased donor kidneys, who had
a 66% decreased risk of ureteral com-plications compared with non-stented recipients, investigators reported online ahead of print in Transplantation.
“Routine stenting in deceased donor transplants is recommended as its protective effect was observed in this group,” the authors concluded.
The protective effect of stents was related primarily to a significant reduction in stricture but not leak. “We speculate that the stent affects the healing process in the early post-operative period in such a way that stricture is less likely to occur at a later time point,” Sameh A. Fayek, MD, and colleagues at the University of Maryland School of Medicine in Baltimore, stated.
Deceased donor kidneys are more prone to ischemic insult secondary to long cold ischemia time and as cer-tain donor characteristics, such as age and diabetes mellitus with possible microvasculature disease. This insult is manifested by the higher delayed graft
function rate in the stent group than in the no-stent group (46% vs. 28.6%), the authors noted.
The UTI rate was 14.2% in the stent group compared with 7.9% in the no-stent group, a difference that translated into a signifi cant 79% increased risk of UTI in the stent group, after adjusting for potential confounders. The fi nd-ing of an increased UTI risk in renal transplant patients who had ureteral stents implanted is consistent with fi nd-ings from previous studies, Dr. Fayek’s group observed.
A major strength of the study was its relatively large cohort of both deceased and living donor recipients, the researchers said. However, the study is limited by its retrospective design and the fact that patients were operated on by different surgeons with variable practices and thresholds for stenting. According to the authors, the value of stents in recipients of living donor kidneys remains to be determined given the low rate of stent utilization in this group. ■
Ureteral stents, however, are linked to an increased risk of UTI.
Cerebrovascular Events.
(See Adverse Reactions [6] of full Prescribing Information.)
To report SUSPECTED ADVERSE REACTIONS, contact Dendreon Corporation at 1-877-336-3736 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Table 1 Incidence of Adverse Events Occurring in ≥5% of Patients Randomized to PROVENGE
Hypertension
Upper respiratory tract infection
Musculoskeletal chest painCoughNeck painWeight decreasedUrinary tract infectionRashSweatingTremor
All Gradesn (%)
All Gradesn (%)
Grade 3-5n (%)
Grade 3-5n (%)
PROVENGE (N = 601) Control* (N = 303)
Dendreon Corporation Seattle, Washington 98101
PROVENGE are registered trademarks of Dendreon Corporation.P-A-11.10-073.02(a)
References: 1. Kantoff PW, Higano CS, Shore ND, et al; for the IMPACT Study Investigators. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411-422. 2. PROVENGE [package insert]. Dendreon Corporation; June 2011.

Highlights of the GU Cancers Symposium
This issue features coverage of the 2012 Genitourinary (GU) Cancers Symposium, which was
held in San Francisco. On the cover are two news articles, one of which reports on two studies comparing prostate can-cer (PCa) treatment modalities. Among the chief fi ndings: Brachytherapy is less toxic and less costly than either external beam radiotherapy or radical prosta-tectomy, and proton beam therapy—the most expensive PCa treatment of all—is no better than intensity-modulated radiotherapy.
Although clinicians may be averse to letting cost be an overriding issue in the treatment they recommend, they might have no choice in the future. These data could be considered by public and private health insurers as they develop reimbursement policies aimed at cut-ting health care spending. They could formulate payment guidelines that encourage the use of one treatment over another.
Symposium news coverage continues on pages 12 and 13, where you will fi nd a report on a large study showing that clinicians are not following the U.S. Preventive Services Task Force recommendation against PSA screening for men aged 75 years and older. The study did not look at why, but the lead investigator suspects that one reason may be that clinicians do not believe that the controversy surrounding the value of PSA screening in this subpopulation has been resolved.
And be sure to read about the study showing that 11% of men with metastatic PCa receive no anticancer treatment. The study found that Medicaid, Medicare, and uninsured patients were more likely than the privately insured to go without treatment. I thought it was particularly interesting that Medicare patients were more likely than Medicaid patients to be untreated. I would have thought the reverse given that the Medicaid population tends to be more disadvantaged socioeconomically.
Lastly, we have a report on a study suggesting that everolimus may be the fi rst effective pharmacologic treatment for angiomyolipoma (AML). Nearly 42% of patients with this benign tumor had an AML response compared with none of the placebo recipients.
For additional news reports from the symposium, I invite you to visit our web site (www.renalandurologynews.com), where you can view video podcasts of colleagues providing details of their studies.
Yours sincerely,
Jody A. CharnowEditor
FROM THE EDITOR
EDITORIAL ADVISORY BOARD
Renal & Urology News (ISSN 1550-9478) Volume 11, Number 3. Published monthly by Haymarket Media, Inc., 114 West 26th Street, 4th Floor, New York, NY 10001. Periodicals postage paid at New York, NY, and an additional mailing offi ce. The subscription rates for one year are, in the U.S., $75.00; in Canada, $85.00; all other foreign countries, $110.00. Single issues, $20.00. www.renalandurologynews.com. Postmaster: Send address changes to Renal & Urology News, c/o DMD Data Inc., 2340 River Road, Des Plaines, IL 60018. For reprints, contact Wright’s Reprints at 1.877.652.5295. Copyright: All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means (electronic, mechanical, photocopying, recording, or otherwise) without the prior written permission of Haymarket Media, Inc. Copyright © 2012.
Renal & Urology News Staff
Editor Jody A. Charnow Executive editor Marina Galanakis Senior editor Delicia Honen Yard Web editor Stephan Cho Editorial coordinator Candy Iemma Group art director, Haymarket Medical Jennifer Dvoretz VP, audience development and operations John Crewe Production manager Kathleen Millea Product manager, digital products Chris Bubeck Circulation manager Paul Silver Assistant circulation manager Monica Bond National accounts manager William Canning Editorial director Tanya Gregory Publisher Dominic Barone VP medical magazines and digital products Jim Burke CEO, Haymarket Media Inc. Lee Maniscalco
Medical Director, Urology
Robert G. Uzzo, MD, FACSG. Willing “Wing” Pepper Chair in Cancer ResearchProfessor and ChairmanDepartment of Surgery Fox Chase Cancer Center Temple University School of MedicinePhiladelphia
Urologists
Frank R. Cerniglia Jr, MDAttending Pediatric UrologistChildren’s Urology of VirginiaRichmond, Va.Christopher S. Cooper, MDDirector, Pediatric UrologyChildren’s Hospital of IowaIowa CityR. John Honey, MDHead, Division of Urology,Endourology/Kidney Stone DiseasesSt. Michael’s HospitalUniversity of TorontoStanton Honig, MDAssociate Clinical Professor of Surgery/UrologyUniversity of Connecticut School of Medicine, Urology CenterNew HavenJ. Stephen Jones, MD, FACSChairmanDepartment of Regional UrologyCleveland ClinicGlickman Urological & Kidney InstituteProfessor of SurgeryCleveland ClinicLerner College of Medicineof Case Western Reserve UniversityJames M. McKiernan, MDAssistant Professor of UrologyColumbia University Collegeof Physicians and SurgeonsNew York CityKenneth Pace, MD, MSc, FRCSCAssistant ProfessorDivision of UrologySt. Michael’s HospitalUniversity of TorontoRyan F. Paterson, MD, FRCSCAssistant ProfessorDivision of Urologic SciencesUniversity of British ColumbiaVancouver, Canada
Medical Director, Nephrology
Kamyar Kalantar-Zadeh, MD, PhD, MPHProfessor of Medicine and Pediatrics, and Director, Dialysis Expansion & Epidemiology Harbor-UCLA Division of Nephrology & Hypertension Los Angeles BioMedical Research Institute, The David Geffen School of Medicine at UCLA
Nephrologists
Anthony J. Bleyer, MD, MSProfessor of Internal Medicine/NephrologyWake Forest University School of MedicineWinston-Salem, N.C.
Suphamai Bunnapradist, MDDirector of ResearchDepartment of NephrologyKidney Transplant Research CenterThe David Geffen School of Medicine at UCLA
R. Michael Hofmann, MDAssociate Professor and Medical Director, Living Kidney Donor Program University of Wisconsin School of Medicine and Public Health, Madison
Csaba P. Kovesdy, MDAssociate Professor of Clinical Medicine University of Virginia, CharlottesvilleChief of NephrologySalem VA Medical CenterSalem, Va.
Edgar V. Lerma, MD, FACP, FASN, FAHA Clinical Associate Professor of Medicine Section of Nephrology Department of Medicine University of Illinois at Chicago College of Medicine, Chicago
Allen Nissenson, MD Emeritus Professor of Medicine The David Geffen School of Medicine at UCLA, Chief Medical Offi cer, DaVita Inc.
Rulan Parekh, MD, MSAssociate ProfessorJohns Hopkins Children’s Center, BaltimoreRobert Provenzano, MDChief, Section of NephrologySt. John Hospital and Medical Center, DetroitRobert S. Rigolosi, MDDirector, Regional Hemodialysis CenterHoly Name Hospital, Teaneck, N.J.
Lynda Anne Szczech, MD, MSCEAssociate Professor of NephrologyDuke University School of MedicineDurham, N.C.
Renal & Urology News welcomes letters to the editor. Send to:Jody A. Charnow, 114 West 26th Street, 4th Floor, New York, NY 10001or e-mail [email protected]
www.renalandurologynews.com MARCH 2012 Renal & Urology News 5

““
ContentsNephrology 3 Pulmonary Hypertension Common in HD
Patients In a study, 38% of hemodialysis patients had
the condition, and it was associated with an increased death risk.
4 Stents May Benefi t Renal Transplant Patients The devices lower the risk of ureteral
complications in recipients of deceased donor kidneys
9 Infl ammatory Markers, CKD Linked Chronic kidney disease is more likely to
develop in patients with elevated levels of tumor necrosis factor alpha receptor 2 and interleukin-6.
11 Not ALL ESRD Patients May Want Dialysis Some patients would accept a shorter
life expectancy in exchange for a better quality of life.
Urology
9 Non-Cancer Death Less Likely with PN Patients who undergo partial nephrectomy
for localized renal cell carcinoma are more likely to die from causes other than their cancer compared with patients treated with radical nephrectomy.
12 No Change in PSA Testing for Men 75+ Prostate cancer screening using PSA tests has
not declined despite a 2008 U.S. Preventive Services Task Force recommendation against such screening in this age group.
13 Empiric Antibiotic Use May Be Unjustifi ed New fi ndings challenge the widespread prac-
tice of placing men on an empiric course of antibiotics for a newly elevated PSA level.
24 PSMs Predict PCa Recurrence in Some Men Positive surgical margins are a risk factor for
biochemical recurrence in men who have undergone radical prostatectomy for inter-mediate-risk disease.
Departments 5 From the Editor Genitourinary Cancers
Symposium highlights
8 News in Brief Biomarkers identify AKI
18 Renal Nutrition Update Salt reduction should be
promoted
23 On the Forefront A puzzling case of primary
aldosteronism
26 Malpractice News A $9 million Wyoming
verdict
34 Your Money Weighing the benefi ts of
target-date funds
28 CME FeatureClinical Challenges and Renal Considerations When Managing GoutWilliam F. Finn, MD, Professor of Medicine in the Division of Nephrology and Hypertension at the University of North Carolina School of Medicine at Chapel Hill, discusses the etiology of gout, the pathogenesis of hyperuricemia, risk factors in renal transplant recipients, patient workup, and other aspects of care.
18
At this time, we cannot recommend the addition of rituximab to MMF for the initial therapy of proliferative lupus nephritis.
See our story on page 24
Expert Q&ARenal & Urology News talks with a leading authority on brachytherapy
Clinical QuizTake our latest quiz at renalandurologynews.com/clinical-quiz/. Answer correctly and you will be entered to win a $50 American Express gift card. Congratulations to our January winner:Randy Chudler, MD
The Medical MinuteVisit renalandurologynews.com/the-medical-minute to hear podcast reports on new studies. Our latest include:• Prostate Health Supplement No Better than Placebo
• Stroke Risk Signifi cant Higher in Hemodialysis Patients
• A New Radiotherapy Option for Prostate Cancer
News CoverageVisit our website for on-site coverage of the 27th Annual Congress of the European Association of Urology in Paris, Feb. 24-28.
M A R C H 2 0 1 2 ■ V O L U M E 1 1 , I S S U E N U M B E R 3
ONLINE this month atrenalandurologynews.com

8 Renal & Urology News MARCH 2012 www.renalandurologynews.com
News in Brief Please visit us at www.renalandurologynews.com for the latest news updates from the fi elds of urology and nephrology
Nephrologist Earnings RiseFrom 2009 to 2010, median annual income rose by 5.1% for nephrologists and fell by 4.6% for urologists, according to data from the Medical Group Management Association. Median income rose by 9.5% for all specialists combined.
Source: Medical Group Management Association. Physician Compensation and Production Survey (2010 and 2011).
Adverse RP Effects Not Lessened with RoboticsPatients undergoing prostate cancer surgery face similar risks for incontinence
and sexual problems whether they undergo robotic-assisted laparoscopic radical prostectomy (RP) or open RP.
Michael J. Barry, MD, and colleagues studied 406 Medicare patients who had undergone robotic-assisted laparoscopic RP and 220 who had undergone open RP. Of those who responded to questions on a mail survey, 31.1% reported a moderate or big problem with incontinence and 88% reported a moderate or big problem with sexual function, according to an online report in the Journal of Clinical Oncology. Adjusted analyses showed that robotic and open surgery were associated with similar likelihoods of greater problems with urinary and sexual function.
“Medicare-age men should not expect fewer adverse effects following robotic prostatectomy,” the authors concluded.
Biomarkers Identify AKI in Emergency Patients
In an international study of 1,635 emergency-department patients, urinary neutrophil gelatinase-associated lipocalin (uNGAL) was the most useful of
fi ve urinary biomarkers in predicting the severity and duration of acute kidney injury (AKI) at the time of hospital admission, with 81% specifi city and 68% sensitivity at a cutoff of 104 ng/mL.
In the study by Thomas L. Nickolas, MD, MS, and colleagues, which was pub-lished in the Journal of the American College of Cardiology (2012;59:246-255), uNGAL and another biomarker, urinary kidney injury molecule 1, predicted a composite outcome of dialysis initiation or death during hospitalization, improved the net risk classifi cation compared with conventional assessments, and identifi ed a substantial subpopulation of patients who had low serum creatinine at hospital admission but were at risk of adverse events.
Study: Form of Bladder Cancer Increased by 56%
A lthough a detailed trend analysis of 127,614 U.S. cases of fi rst primary blad-der cancer demonstrated a 9% overall drop in disease occurrence between
1973 and 2007, papillary transitional cell carcinoma (PTCC)—one of two main subtypes—increased by 56% over that period.
In contrast, the other main subtype, non-papillary transitional cell carcinoma (NPTCC), fell by about 53%. The results suggest that external and internal blad-der tumors are two disease entities with separate causes, according to a report in BJU International (2012;109:52-56).
Lead investigator Yawei Zhang, MD, of the School of Public Health and School of Medicine at Yale University, in New Haven, Conn.,observed that “no epidemiologi-cal studies have investigated the risk factors for these two subtypes separately. Our study suggests that future research must make clear distinctions between PTCC and NPTCC and not just treat them as subtypes of transitional cell carcinoma.”
Vytorin Label WillInclude Kidney DataThe FDA has approved new labeling for the cardiovascular agent Vyto-rin (ezetimibe/simvastatin) that will include data from the Study of Heart and Renal Protection (SHARP), in which Vytorin 10/20 mg reduced the risk for major vascular events in patients with moderate-to-severe chronic kidney dis-ease. The FDA did not approve a new related indication for Vytorin because SHARP did not assess the independent contributions of ezetimibe and simvas-tatin to the observed effect.
Dietary Calcium MayDecrease PCa RiskDietary calcium is associated with lower risk for prostate cancer (PCa), particularly among black men, and with a lower risk for high-grade PCa among all men, according to a study involving 108 U.S. veterans with biopsy-positive prostate cancer, 161 biopsy-negative controls, and 237 healthy controls.
The highest tertile of calcium
from food was associated with a 63% decreased risk of high-grade PCa in a comparison of high-grade cases and biopsy-negative con-trols and a 62% decreased risk in a comparison of high-grade cases and healthy controls, according to a report in Preventing Chronic Disease (2012;9:110125).
Renal Decline Linkedto TNF Receptors High levels of tumor necrosis factor (TNF) receptors 1 and 2 are associated with an increased risk of kidney disease in patients with type 1 diabetes, according to fi nd-ings published online ahead of print in the Journal of the American Society of Nephrology. In a study by Andrzej S. Krolewski, MD, and colleagues, patients with TNF receptor 2 levels in the highest quartile were three times more likely to experience renal decline than patients in other quartiles. The risk associated with TNF receptor 1 was slightly less than that associated with TNF receptor 2 values.
Short Takes
0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
20092010
All specialists (excludes primary
care doctors)
UrologistsNephrologists
$306,046
$372,455$356,885
$290,986
$390,678
$325,916

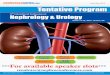
Non-Cancer Death Less Likely with PN Partial nephrectomy should be offered for RCC whenever technically feasible, researchers conclude
PATIENTS WHO UNDERGO par-tial nephrectomy (PN) for localized renal cell carcinoma (RCC) are more likely to die from causes other than their cancer compared with patients treated with radical nephrectomy (RN), data show.
Maxine Sun, MD, of the University of Montreal Health Center, and colleagues compared other-cause mortality (OCM) among 1,068 PN patients and 1,068 RN patients, adjusting for cancer-specifi c mortality (CSM), age, baseline Charlson comorbidity index (CCI), race, gender, socioeconomic status, tumor grade, and year of surgery. Subjected were propensity matched.
The two- and fi ve-year OCM rates were 5% and 16%, respectively, for the PN group compared with 6.9% and 18.1% for the RN group. In mul-tivariate analyses, PN patients had a signifi cant 17% decreased likelihood of OCM compared with RN patients, the investigators reported online ahead of print in European Urology.
Additionally, higher CCI, increasing age, female gender, and baseline hyper-calcemia and baseline hyperlipidemia were independent predictors of OSM.
As a result of their findings, the researchers concluded that PN should be offered as a treatment for localized RCC whenever technically feasible.
The authors noted that previous stud-ies have suggested that PN may not be associated with a survival benefi t and in fact may be associated with increased overall mortality compared with RN. In a randomized, prospective study of 541 patients with small solitary renal tumors, Hendrik Van Popple, MD, and colleagues (Eur Urol 2011;59:543-552) found no signifi cant difference in sur-vival between PN and RN. A study by William C. Huang, MD, and colleagues (J Urol 2009;181:55-61) showed that RN was associated with a signifi cant 38% increased risk of overall mortality com-pared with PN, and a study by Laurent Zini, MD, PhD, and colleagues (Cancer 2009;115:1465-1471) demonstrated a
signifi cant 23% increased risk of overall mortality associated with RN compared with PN. Dr. Sun’s group pointed out, however, that previous studies have either failed to account for inherent patient and sociodemographic differ-
ences between PN and RN patients, did not consider baseline conditions, or did not account for the effect of CSM.
In their discussion of limitations of their study, Dr. Sun’s group noted that their study sample was restricted to Medicare beneficiaries, which have an age of 65 years and older. “This restriction may have compromised the generalizability of the results and may represent a major difference relative to previous studies that did not have an age restriction applicable to their analyses,” the authors wrote.
In addition, the investigators pointed out, “the lack of information on baseline kidney functions and serum creatinine levels to identify patients with preex-isting and treatment-induced chronic kidney disease may have infl uenced the rates of OCM events. As such, the observed effect between treatment type and OCM cannot be inferred as a direct causal relationship but only as a mere correlation, which would need to be confi rmed in future studies.” ■
Inflammatory Markers, CKD LinkedELEVATED LEVELS OF certain infl ammatory markers are associated with an increased risk of develop-ing chronic kidney disease, a study found.
The population-based study, which included a cohort of 4,926 individuals, divided subjects into tertiles based on their baseline serum levels of C-reactive protein (CRP), tumor necrosis factor-alpha receptor 2 (TNF-αR2), inter-leukin-6 (IL-6), and serum white blood cell (WBC) count, all markers of infl ammation.
After adjusting for multiple vari-ables, including diabetes and hyper-tension, subjects in the highest tertile
of TNF-αR2 and WBC count had a twofold increased risk of developing CKD over a 15-year follow-up period compared with subjects in the lowest tertile, according to a research team led by Anoop Shankar, MD, of the West Virginia School of Medicine in Morgantown. Patients in the highest tertile of interleukin-6 levels had a 45% increased risk. CRP level was not associ-ated with CKD risk.
“Results from our study further extend the current understanding of the role of infl ammatory markers in the pathogenesis of CKD,” Dr. Shankar’s team wrote in Kidney International (2011;80:1231-1238).
In addition, the authors concluded: “A practical application of our fi ndings is that, if replicated in other studies, these markers may be a potential future way of assessing subjects who are more likely to develop CKD.”
Strengths of the study, the researchers noted, include its population-based sample, high participation rate, the availability of specifi c markers of infl am-mation, and the use of standardized protocols for exposure and outcome measurement. Lack of information on a marker of kidney injury, such as 24-hour urine protein or urinary albu-min/creatinine ratio, was a main study limitation, they wrote. ■
PATIENTS ON long-term hemodialy-sis (HD) are at increased risk of herpes zoster compared with the general popu-lation, according to researchers.
Chien-Chun Kuo, MD, and colleagues at Kaohsiung Medical University in Kaohsiung, Taiwan, studied 843 patients who began HD in 1999-2003 and a com-
parison group of 3,372 patients without end-stage renal disease matched for age and gender. Mean follow-up was 4.73 and 5.49 years for the HD and com-parison groups, respectively. The inci-dence rate of herpes zoster was 73.34 events per 1,000 person-years in the HD group, which was signifi cantly greater
than that of the 31.03 events/1,000 per-son-years in the comparison group, the investigators reported online ahead of print in the American Journal of Kidney Diseases. After adjusting for confound-ers, herpes zoster was twice as likely to develop in the HD patients than the comparison group. ■
HD Patients at Higher Risk for Herpes Zoster
PSMs Rare After Partial NephrectomyPOSITIVE SURGICAL margins (PSMs) are rare in patients undergoing partial nephrectomy (PN) for kidney cancer, researchers found.
A nonsystematic literature review by Martin Marszalek, MD, of Donaus-pital, Vienna, Austria, and colleagues revealed that PSMs are present in 0%-7% of patients following open PN, 0.7%-4% after laparoscopic PN, and 3.9%-5.7% after robot-assisted PN, according to a report in European Urology (published online ahead of print).
Intermediate follow-up data show that the vast majority of patients with PSMs after PN remain without local or distant tumor recurrence. “Therefore,” the authors concluded, “a surveillance strategy with adher-ence to a vigilant follow-up protocol seems to be preferable over surgical reintervention.” ■
www.renalandurologynews.com MARCH 2012 Renal & Urology News 9
Partial vs. Radical Nephrectomy
0
5
10
15
20 Radical nephrectomyPartial nephrectomy
Two-year Five-yearOther-cause mortality rates
Partial nephrectomy for renal cell carci-noma is associated with a lower risk of death from non-cancer causes compared with radical nephrectomy, a study found.
Source: Sun M, Trinh Q-D, Bianchi M, et al. A non-cancer-related survival benefi t is associated with partial nephrectomy. Eur Urol. 2011 [Epub ahead of print]

10 Renal & Urology News MARCH 2012 www.renalandurologynews.com
the community-based Coronary Artery Risk Development in Young Adults (CARDIA) study. The study popula-tion included 4,119 subjects aged 18-30 years with an estimated glomerular fi l-tration rate (eGFR) of 60 mL/min/1.73 m2 or higher. The researchers, led by Paul Munter, PhD, of the University of Alabama in Birmingham, defi ned devel-opment of CKD as a decrease in eGFR to below 60 and a 25% or greater decline in eGFR at study visits conducted 10, 15, and 20 years after baseline.
Forty-three CKD cases developed dur-ing follow-up: 29 (1.4%) among African Americans and 14 (0.7%) among whites, a signifi cant difference between the races. After adjusting for age, gender, body mass index, systolic blood pressure, fasting plasma glucose, and high-density lipo-protein cholesterol, researchers found that CKD was 2.5 times more likely to
develop in African Americans than in whites, Dr. Munter’s group reported. In a multivariable analysis that accounted for albuminuria at year 10, however, CKD was only 12% more likely to develop in African Americans than in whites at year 15 or 20.
At the year 10 visit, the geometric mean albuminuria level was 8.2 mg/g among African Americans compared with 6.6 mg/g among whites.
It is well established that African Americans have a higher incidence of end-stage renal disease than whites, the researchers noted. Recent data from the U.S. Renal Data System shows that ESRD is four times more likely to develop in African Americans than in whites, they pointed out.
It is possible that African Americans have more severe kidney disease that progresses more rapidly to ESRD. It is noteworthy that six of the seven par-ticipants with ESRD in their study were African American, researchers stated. ■
“Today, proton radiation is receiv-ing a lot of attention as a new way to treat prostate cancer and it is the most expensive radiation technique to date,” Dr. Chen said. The number of proton radiation centers has been increasing rapidly in the United States despite no evidence of proton therapy superiority over IMRT, he added.
The study also showed that IMRT is superior to conformal radiation therapy (CRT) in terms of adverse effects and cancer control.
Less bowel morbidity with IMRT“To compare treatment-related toxici-ties and cancer control among the three radiotherapy modalities, the researchers analyzed data from the Surveillance, Epidemiology, and End Results (SEER)-Medicare linked database for patients with non-metastatic PCa. Using pros-pensity-score analysis to adjust for patient characteristics, the researchers found that IMRT patients had a 34% decreased risk for bowel morbidity than
patients who underwent proton therapy. The study revealed no signifi cant differ-ence in the need for additional cancer treatment, which the investigators used as a surrogate for cancer recurrence.
In a propensity-score adjusted analysis, IMRT patients had a signifi cant 9% decreased risk of bowel morbidity and a 22% decreased risk of hip fractures com-pared with CRT patients, Dr. Chen said. IMRT, however, was associated with a signifi cant 12% increased risk of erectile dysfunction (ED). IMRT patients had a signifi cant 19% decreased risk of receiv-ing additional cancer treatments.
Dr. Chen concluded that the study “supports the use of IMRT as the current standard radiation technique for prostate cancer.” He also stated that,“IMRT causes fewer side effects and achieves better cancer control com-pared to the older conformal radiation technique. Currently, there is no clear evidence that proton therapy is better than IMRT.” Additionally, Dr. Chen noted that more comparative effec-tiveness studies are needed to directly compare patient outcomes of proton therapy versus IMRT.
In the other study, Dr. Ciezki’s team used the Surveillance, Epidemiology, and End Results (SEER)-Medicare database to identify patients aged 65 years and older treated for PCa from 1991 to 2007. Of 137,427 patients identifi ed, 60,806 (44.2%) received EBRT, 59,559 (43.3%) underwent RP, and 17,062 (12.4%) were treated with brachytherapy.
Brachytherapy the safestGI toxicity occurred in 1.7%, 0.1%, and 0.3% of patients treated with EBRT, RP, and brachytherapy, respectively, after a median follow-up of 71 months. Genitourinary toxicity occurred in 7.1%, 6.7%, and 3.4% of these groups, respec-tively. Within treatment modalities, the percentages receiving toxicity-related intervention were 8.8% for EBRT, 6.9% for RP, and 3.7% for brachytherapy.
The average cost per patient per year was $2,557 for brachytherapy, $6,412
for EBRT, and $3,205 for open pros-tatectomy, investigators found.
Prostate cancer specialist Leonard G. Gomella, MD, who headed the sympo-sium’s program committee, noted that “many times, there’s an assumption that the newest or perhaps the most expensive modalities that we have to offer are the best for our patients. These two studies suggest from a side effect standpoint that the more expensive technologies, be they proton therapy or external beam radiation therapy, may in fact be associated with a higher risk of side effects.”
Treat patients as individualsDr. Gomella, who is Chair of the Department of Urology at Thomas Jefferson University’s Kimmel Cancer Center in Philadelphia, stressed that “at the end of the day we really need to look at each patient as an individual and pick for that individual patient what may be the best for them looking at both cancer control and quality of life.”
Although brachytherapy turned out to be the lowest cost option in the study by Dr. Ciezki and colleagues, men who might choose this treatment may not be a good candidate for it, Dr. Gomella observed. For example, brachytherapy probably is not good for men who have a lot of urinary symptoms. “If they choose brachytherapy, those symptoms may actually get much worse. So we have to be very careful in that we can’t paint a broad brush stroke here on all of the competing treatment options for prostate cancer.” ■
Proton Beamcontinued from page 1
radium-223 group versus 8.4 months in the placebo arm, a 39% reduction in SRE risk.
Radium-223 significantly reduced time to three of four SRE components: time to fi rst use of external beam radio-therapy to relieve skeletal symptoms; time to fi rst spinal cord compression; and time to fi rst symptomatic patho-logic bone fracture.
With respect to adverse events (AEs), grade 3 or 4 neutropenia was observed in only 2% of patients in the radium-223 arm and 1% of placebo recipients. Grade 3 or 4 thrombocytopenia was observed in 4% and 2% of these groups, respectively.
Sixty-eight patients (13%) in the radium-223 arm and 51 (20%) in the placebo group dropped out of the study because of AEs.
Leonard G. Gomella, MD, a pros-tate cancer specialist who headed the
symposium’s program committee and is Chair of the Department of Urology at Thomas Jefferson University’s Kimmel Cancer Center in Philadelphia, said the new agent “is a big deal in pros-tate cancer and probably will be a big deal in other cancers that tend to go to the bone.”
Existing radiation-based treatments that target bone are so-called beta emitters, Dr. Gomella said. Although these agents helped to control pain and limit fractures, they were very toxic to bone marrow.
“What is very exciting and very important about radium-223 is that it’s an alpha emitter, so it does not have the same effect on the bone marrow that some of these earlier radiation-based treatments have on the bone,” Dr. Gomella told Renal & Urology News. “So this is going to be a very important step forward not only for the potential for the survival, as we saw in the study, but also from the potential quality of life in controlling SRE.” ■
Radium Drugcontinued from page 1
Prostate Cancer Treatment Costs
A study found that brachytherapy is the least costly of the common treatments for prostate cancer. The average cost per patient per year by treatment modality is shown here.
Brachytherapy EBRT Open Prostatectomy
$2,557 $6,412 $3,205
Source: Ciezki JC et al. Long-term toxicity and associated cost of initial treatment and subsequent toxicity-related intervention for patients treated with prostatectomy, external beam radiotherapy, or brachytherapy: A SEER/Medicare database study. Data presented at the 2012 Genitourinary Cancers Symposium in San Francisco. Abstract 4.
Jay P. Ciezki, MD
CKD Incidence Higher
continued from page 1

BY ROSEMARY FREI, MScSOME INDIVIDUALS with end-stage renal disease (ESRD) are willing to give up a few months of life rather than live with the logistical diffi culties that can be associated with dialysis, according to a survey.
The survey findings, which were published online in the Canadian Medical Association Journal, showed that patients would be willing to forgo seven months of life expectancy in exchange for having fewer hospital visits for dialysis and forgo 15 months of life expectancy so they could travel more. It is the fi rst study of its kind to examine the choices pre-dialysis patients make between dialysis and no dialysis.
“Our research has shown that patients are particularly interested in knowing their expected survival, the number of visits to a dialysis facility that they would have to make, the resultant restrictions on their ability to travel for work or vacation, and the time of day dialysis can be performed,” noted lead investigator Rachael Morton, PhD, of the Sydney School of Public Health at the University of Sydney in Australia. “In addition, patients have the right to know that a pathway of care is avail-able should they choose not to initiate dialysis.”
The survey was completed by 105 subjects, all of whom had stage 3-5 chronic kidney disease. Their average age was 63 years, 56% were men, and 44% had private health insurance.
The study is what is known as a dis-crete choice experiment in which par-ticipants are asked to choose between several hypothetical scenarios. The participants were presented with 12 choice sets (scenarios) involving trade-offs between life expectancy, number of visits to hospital per week for dialysis, travel restrictions, number of hours on treatment and whether subsidized transportation was available for hospital visits. The alternative to dialysis was presented as supportive non-dialysis medical management.
The patients chose dialysis as their preferred option 90% of the time. Six patients chose conservative care with every scenario. Some of the reasons the patients gave, when fi lling in the optional comments section at the end of the survey, were—in this case, from a 67-year-old man—“I think dialysis would be very restrictive to my quality of life. I am very active in my commu-nity and also love to travel and head bush whenever I like. At the moment I have a very unrestrictive lifestyle and want to keep it that way.”
As the investigators expected, higher
average estimated life expectancy was associated with an 84% greater likeli-hood that the patients would choose dialysis. Subjects were nearly nine times as likely to opt for dialysis if it was avail-able during the day or evening, versus only during the day or overnight and 55% more likely if subsidized trans-portation was available.
The researchers also used the survey responses to calculate the trade-offs between life expectancy and other characteristics. They found patients were willing to forgo seven months of life expectancy in exchange for reducing the number of hospital visits for dialysis from four to three. They were willing to forgo 15 months of
life expectancy to decrease their travel restrictions by one level, for example, from “very restricted” to “somewhat restricted.”
The investigators concluded that dialysis should not be the presumed treatment for all patients approach - ing ESRD.
“We acknowledge that instigating such conversations [about non-dialysis options] with patients and their fami-lies may be diffi cult. However, further support is available for nephrologists through the ‘shared decision making’ clinical practice guideline (2010) issued by the Renal Physicians Association,” said Dr. Morton, referring to the Rockville, Md.-based organization. ■
Not All ESRD Patients May Want DialysisFor some, freedom from the hassles of treatment is worth a shorter life expectancy, study fi nds
BY NAYANAH SIVALONDON—Cryotherapy can be used to treat small renal tumors or masses successfully with relatively low rates of complications and recurrence, a urolo-gist skilled in the technique told attend-ees at the Renal and Bladder Cancer 3rd National conference here.
Neil Barber, FRCS, Consultant Urological Surgeon at Frimley Park Hospital, Surrey, UK, spoke about his experience with cryotherapy for renal cancer. Since 2008, he has used this modality to treat 52 patients, 75% of whom had a small malignant mass (4 cm or less). Patients had an average age of 70 years. The typical procedure time was two hours and 20 minutes and no blood transfusions were required. The average hospital stay was one night. Three patients experienced complica-tions: two patients had bleeding, which
was managed conservatively, and one had a ureteric injury.
With the incidence of small renal masses (2-4 cm) rising in both men and women, particularly in elderly patients, Dr. Barber said he believes treatment
options other than surveillance could reasonably be considered when manag-ing this group of patients.
“Surveillence is the talk of the town [at the moment] when we talk about how to manage small renal masses, and there is increasing evidence that surveil-
lance is a safe option although there are no randomised trials to confi rm this.” Data have shown that most of these tumors grow very slowly.
Dr. Barber cited data from the Surveillance, Epidemiology, and End Results (SEER) database showing that up to 75% of patients with small renal masses had malignant small renal masses. Of those that were malignant, about 55% had low-grade malignancy. However, up to 20% of patients had high-grade tumors, with some smaller tumors were already metastatic at presentation.
Treatment options for small renal tumors or masses include nephron-sparing surgery or partial nephrectomy, but these, too, are not without their complications, Dr. Barber said.
Dr. Barber’s cryotherapy involves freezing and thawing the renal mass.
By using hollow needles, he uses argon to freeze the mass. Ice crystals form inside and outside of cells as well as in the surrounding blood supply. During the thawing stage, helium is placed into the mass. Extracellular fl uid re-enters cells, further damaging the mass and causing necrosis in the entire tumor.
Overfreezing can be an issue, and there may be complications with bleed-ing, he noted. The overall complication rate is 9.4%, but this appears to be less than with radiofrequency ablation. Dr. Barber said he thinks cryotherapy is an important option for patients, particularly elderly patients who have a high incidence of small renal tumors. Cryotherapy is minimally invasive and is associated with rapid hospital dis-charge, and low complication rates, he said. In addition, it is not very techni-cally demanding for surgeons. ■
Cryotherapy Is An Option for Small Renal Masses
Patients have a right to know dialysis is not the only option, according to researchers.
It is associated with low rates of complications and recurrence.
www.renalandurologynews.com MARCH 2012 Renal & Urology News 11
© L
ARRY
MUL
VEHI
LL /
PHO
TO R
ESEA
RCHE
RS, I
NC.

■ 2012 Genitourinary Cancers Symposium, San Francisco
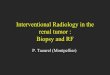
No Change in PSA Testing for Men 75+
PROSTATE CANCER screening using PSA tests has not declined among men aged 75 years and older despite a 2008 U.S. Preventive Services Task Force (USPSTF) recommendation against such screening in this age group.
Using data from the 2005 and 2010 National Health Interview Survey, a cross-sectional household survey pro-viding a representative sample of the U.S. population, investigators found that PSA tests were ordered for 40.6% of men aged 75 years and older in 2010 compared with 40.4% in 2005.
In addition, the study, led by Michael W. Drazer, a fourth-year medical stu-dent at the University of Chicago, found that PSA testing in 2010 was signifi -cantly more common in men aged 75 and older than in men aged 40 to 49
(9.2%) and 50-59 (26.2%). “Despite the USPSTF recommendation against prostate cancer screening in men aged 75 or older, there was no decrease in PSA testing rates in these men,” the researchers concluded in a poster pre-sentation. “A signifi cant proportion of elderly men continue to receive PSA screening despite a very low likelihood of benefi t.”
Speculating as to why PSA testing has not waned for men aged 75 and older, Drazer said physicians may believe “the controversy hasn’t really been resolved yet” regarding the value of PSA testing in elderly men. “They’re more likely to err on the side of caution,” Drazer added. He observed that sometimes men want to continue with their screen-ing past age 75.
Commenting on the study’s fi ndings, Leonard G. Gomella, MD, chairman of the symposium’s program committee, said the task force chose 75 years as the cutoff because that is when the average man in the United States reaches his 10-year life expectancy.
Caution should be exercised, however, in making broad determinations about men who have 10-year life expectan-cies, said Dr. Gomella, chairman of the Department of Urology and Associate Director of the Kimmel Cancer Center at Thomas Jefferson University in Philadelphia.
“They’re not all the same,” Dr. Gomella said. “Older men do die from aggressive prostate cancer. While we can’t say that screening will eliminate the risk of death in these men, certainly to ignore the men in that older age group who may ultimately suffer from prostate cancer at this point in time seems a little bit premature. Having said that, the 10-year life expectancy and looking at patients’ overall health is very important in deciding when you stop screening.”
He pointed out that the life expec-tancy of men in the United States is going up dramatically in part because improvements in cardiovascular care have reduced their risk of dying from heart attacks and strokes.
Dr. Gomella said he thinks that in the next couple of years PSA screening will used more thoughtfully and providers and patients will be engaged in more dialogue in deciding whether screening is the right thing to do given a patient’s age and health status. ■
ELDERLY MEN who receive defi ni-tive local treatment for prostate cancer (PCa) are much more likely to die from causes other than their cancer, a fi nding that could inform doctor-patient dis-cussions about treatment for localized PCa, according to researchers.
Investigators who studied 4,237 men aged 65 years or older who were treated with radical prostatectomy (1,634 men), external beam radiotherapy (1,570 men), or brachytherapy (1,033 men) found that the risk of PCa-specifi c mor-tality (PCSM) compared with compet-ing causes of mortality (CCM) is low, especially for patients with moderate-to-severe comorbidity.
“Even if you had high-risk prostate cancer and no comorbidities, you were
still much more likely to die of other causes than you were from prostate cancer,” observed investigator Joseph C. Klink, MD, a urologic oncology fel-
low at Cleveland Clinic, who presented study fi ndings.
Over a median follow-up of 72 months, investigators observed 88 and 748 PCSM and CCM events, respec-tively. Among healthy men with low-
risk PCa, 10-year PCSM was 2% and CCM was 19%. Among healthy men with high-risk PCa, PCSM was 11% and CCM was 27%.
In a group of patients with moder-ate-to-severe comorbidities, PCSM was 1%, 3%, and 21% for men with low-, intermediate-, and high-risk PCa, respectively, whereas CCM was 49%, 59%, and 58%, respectively.
The investigators noted that current evidence suggests that local treatment for PCa is associated with a 25% reduction in PCSM at best. Therefore, they observed, with active surveillance, it is unlikely that PCSM would exceed 5%-7% in patients with low- and intermediate-risk PCa.
The study by Dr. Klink and colleagues is not the fi rst to show that men treated
for localized PCa are more likely to die from non-PCa causes than from their cancer. In a study of 120,392 men who underwent radical prostatectomy for localized PCa, Sergey Shikanov, MD, and colleagues at the University of Chicago showed that 15-year PCa-specifi c mortality was 5.3% and the 15-year non-PCa mortality was 30.6%, according to recent report published online ahead of print in Prostate Cancer and Prostatic Diseases.
In addition, 15 years after surgery, mortality related to cardiovascular dis-ease was 11%, other cancers, 9.1%, and other causes, 10.5%. Among men aged 65 years and older, 15-year PCSM was 6% and 15-year non-PCa mortality was 40.8%. ■
PCa-Related Deaths Uncommon Post-Treatment
12 Renal & Urology News MARCH 2012 www.renalandurologynews.com
Patients are much more likely to die from causes other than prostate cancer.
PSA Testing in the Very OldPSA testing remained unchanged among men aged 75 and older despite recom-mendations against such screening from the U.S. Preventive Services Task Force, a study found. Shown here are the testing rates by age group for 2005 compared with 2010.
Source: Drazer MW et al. Impact of U.S. Preventive Services Task Force recommendation on screening for prostate cancer in men aged 75 or older. Data presented at the 2012 Genitourinary Cancers Symposium in San Francisco. Abstract 216.
0
10
20
30
40
5020102005
40-4950-5960-7475+
40.4% 40.6%43.9%
46.7%
27.8% 26.2%
9.8% 9.2%
The articles on these pages report on studies presented at the 2012 Genitourinary Cancers Symposium in San Francisco, which was sponsored by the American Society of Clinical Oncology, the American Society of Radiation Oncology, and the Society of Urologic Oncology. Renal & Urology News editor Jody A. Charnow provided news coverage.

Possible First Drug Therapy for AML
HEAVY ALCOHOL use is associated with an increased risk of prostate can-cer (PCa) among low-risk men with at least one prior negative prostate biopsy, according to researchers. It also is asso-ciated with an elevated risk for high-grade PCa.
The fi ndings emerged from a study of data from 6,729 men who had at least one on-study biopsy while participat-ing in the REDUCE (Reduction by Dutasteride of Prostate Cancer Events) trial. Of these, 49% were moderate drinkers and 26% were heavy drink-ers. The researchers, led by Lionel L. Bañez, MD, of Duke University Medical Center in Durham, N.C., found that as ethanol intake increased, so did the risk
for PCa overall and for high-grade dis-ease. Dutasteride decreased overall PCa risk signifi cantly by 27% and alcohol did not interfere with the protective effect of dutasteride.
Compared with non-drinkers, heavy drinkers had a 21% greater risk of PCa overall and a 34% greater risk of high-grade PCa (Gleason score of 7 or higher).
For the study, the investigators defi ned alcohol intake in terms of units (half pint of beer, glass of wine, for example). They classifi ed subjects as nondrinkers, mod-erate drinkers (seven units or less per week), and heavy drinkers (more than seven units per week). The study is not the fi rst to fi nd a link between alcohol
use and prostate cancer risk. In a pro-spective study published recently in the American Journal of Epidemiology (2011;174:1044-1053), researchers found that higher-frequency drinking (three or
more days per week compared with less than one day per week) was associated with a signifi cant 55% increased risk of prostate cancer.
In another prospective study published in the same journal (2010;172:773-780), researchers who studied 294,707 U.S. men found that those who consumed six or more drinks per day had a 25% higher risk of nonadvanced PCa than nondrink-ers. The authors observed no asso-ciation between alcohol intake and advanced prostate cancer among heavy drinkers.
However, based on a meta-analysis published online in the European Journal of Cancer Prevention, research-ers concluded that there is no evidence of a material association between alco-hol drinking and prostate cancer, even at high doses. The meta-analysis con-sidered data from 50 case-control and 22 cohort studies that included a total of 52,899 PCa cases. ■
Drinking too much may hike PCa risk.
EVEROLIMUS IS the fi rst potential pharmacologic treatment option for patients with angiomyolipoma (AML), a benign tumor that usually occurs in the kidney.
John J. Bissler, MD, of the Cincinnati Children’s Hospital Medical Center, and colleagues conducted a pro-spective, double-blind study of 118 patients with AML randomized to receive everolimus 10 mg daily (79 patients) or placebo (39 patients). The study population included patients who had tuberous sclerosis complex or lymphangioleiomyomatosis. The
primary efficacy endpoint was the proportion of patients with an AML response, defi ned as a 50% or greater reduction in the sum of volumes of all target AML relative to baseline.
The mean duration of treatment 38.1 weeks for the everolimus group and 34 weeks fo the placebo group. Results showed that 41.8% of everolimus-treated patients had an AML response compared with none of the placebo recipients. Additionally, the mean time to AML progression was 11.4 months for placebo and was not reached in the everolimus group. Everolimus-treated
subjects also had signifi cantly higher best overall skin lesion response rate (complete or partial response) than placebo (26% vs. 0%), according to the investigators.
The drug was associated with an acceptable safety profile consistent with previous reports in tuberous sclerosis complex. Most adverse effects (AEs) were grade 1 or 2. The incidence of AEs was similar in both groups.
Angiomyolipomas rarely cause symptoms, but they can bleed or grow large enough to cause pain or renal failure, the study noted. ■
Empiric Antibiotic Use May Be Unjustifi edNEW FINDINGS challenge the wide-spread practice of placing men on an empiric course of antibiotics for a newly elevated PSA level.
Scott E. Eggener, MD, of the University of Chicago, and colleagues studied 77 men with a newly elevated PSA level. Of these, 38 were random-ized to receive ciprofl oxacin 500 mg twice daily for two weeks or no antibi-otic (control group). PSA was measured 21-45 days following randomization and immediately prior to prostate biopsy.
Prostate biopsy revealed prostate cancer in 36 men (47%). Detection rates did not differ significantly between patients with an increas-ing PSA or decreasing PSA between the two measurements, said Michael Christopher Large, MD, a urologic oncology fellow at the University of Chicago, who presented study fi nd-ings. Mean PSA levels at random ization into the study were 7.6 ng/mL in the antibiotic group and 6.5 ng/mL in the control arm. The mean PSA lev-
els at biopsy were 8.5 and 6.9 ng/mL, respectively.
In the antibiotic group, cancer was found after a PSA increase in seven (44%) of 16 patients after a PSA decrease in fi ve (24%) of 21 patients. In the control arm, cancer was found after a PSA increase in 12 (60%) of 20 patients and after a PSA decrease in 11 (58%) of 19 patients. “Prescription of empiric antibiotics in asymptomatic men with ele-vated PSA is not of any clinical benefi t,” Dr. Large said. ■
Metastatic PCa Often Goes UntreatedMANY PATIENTS with metastatic pros-tate cancer (PCa) never receive anti-cancer treatment. “This is an important observation because these patients are basically falling through the cracks,” said Alexander C. Small, a fourth-year medical student at Mount Sinai School of Medicine in New York, one of the in-vestigators. The National Cancer Data-base was used to identify patients diag-nosed with stage IV PCa between 2000 and 2008. Of 1,201,732 patients with PCa diagnosed during this period, 59,074 (4.8%) had metastatic disease. Among these, 6,582 (11.1%) received no anticancer treatment. With each 10-year increment in age, the prevalence of untreated metastatic PCa increased by 43%. Blacks and Hispanics were, respectively, 32% and 41% more likely than whites to have untreated meta-static PCa. Medicaid patients, Medicare patients, and uninsured patients were, respectively, 57%, 82%, and 96% more likely to be untreated compared with privately insured patients. ■
■ 2012 Genitourinary Cancers Symposium, San Francisco
© IO
FOTO
/ S
HUTT
ERST
OCK
www.renalandurologynews.com MARCH 2012 Renal & Urology News 13
Prostate Cancer Linked to Heavy Alcohol Use

18 Renal & Urology News MARCH 2012 www.renalandurologynews.com
Renal Nutrition UpdateHealth care workers should promote dietary salt reduction, an inexpensive, practical way to impact health BY ALISON L. STEIBER, PhD, RD, LD
H ow important is it for the average person to limit salt? Worldwide, more than one billion adults
have hypertension, and, in 17%-30% of cases, the hypertension is related to excess dietary intake of salt. Historically, salt has been a commodity, a preservative, and a fl avor enhancer. The salt shaker has a special place in most kitchens or dining room tables. Therefore, when dietitians or other health-care providers suggest to patients that they should reduce or limit salt intake to lower blood pressure (BP) and prevent fl uid retention, they are often very resistant. However, it is not just patient resistance that makes salt reduction diffi cult.
Salt, or sodium chloride, is used by food manufacturers in all types of food products. This means that much of the sodium patients consume comes from processed or restaurant food items. In fact, 77% of sodium intake is from pro-cessed foods in most developed coun-tries (J Am Coll Nutr 1991;10:383-393). Through these food items, Americans may consume double the recommended intake of sodium, potentially contributing to more than 7.6 million premature deaths and billions of dollars in health care costs (CMAJ 2009;181:605-609).
It has been well documented that salt-sensitive patients benefit from a reduction in sodium, but in patients who are not salt sensitive, one may question whether reductions in salt or sodium should be recommended for hypertension.
A 2011 meta-analysis found that reduc-tions in salt intake result in decreased
urinary sodium excretion and decreased systolic BP in normotensive individuals and those with hypertension or heart failure. This reduction in urinary sodi-um excretion and BP did not appear to translate into decreased cardiovascular or all-cause mortality (Am J Hypertens2011;24:843-853). A limitation of this meta-analysis was the lack of end points; therefore, while large effects could be detected, small or moderate effects may not be found.
It is these small effects, which over a lifetime, may cumulatively impact qual-ity of life, mortality, and health care costs for a nation. In fact, Frohlich and Susic (Circulation 2011;124:1882-1885) sug-gest that more attention needs to be paid to the “subtle adverse end points of dietary salt excess.” Within this review, the authors outline the organs impacted by excessive salt intake (heart, arteries, and kidneys) and highlight experimen-tal studies conducted in animal models demonstrating that salt loading results in local pathophysiological changes. Years of continuous excessive salt consumption may lead to elevated BP and multi-organ structural and functional damage.
Due to this potential organ damage and subsequent impact on health care costs and mortality, communities and countries have begun instituting public policy regarding salt reductions. It has been estimated that a “population-wide decrease of 2 mm Hg diastolic blood pressure could lower the prevalence of hypertension by 17%, coronary artery disease by 6%, and the risk of stroke by 15%” (CMAJ 2009;181:605-609).
A recent analysis by Asaria et al (Lancet 2007; 370:2044-2053) demonstrated that 8.5 million deaths worldwide could be avoided (2006-2015) with public policies directed at reducing salt intake.
It has been suggested, and exempli-fi ed by Finland, that for a population-based sodium reduction to occur there must be a partnership formed with the food industry. Finland began to have a countrywide sodium reduction in the 1970’s that resulted in a 40% decrease in sodium intake and a 70% reduction in mortality from stroke and coronary artery disease (Prog Cardiovasc Dis 2006;49:59-75). Other countries such as the United Kingdom, France, and Canada have begun similar programs.
In the new Affordable Care Act, a key indicator of the National Prevention Strategy is to reduce the average daily sodium intake in the United States pop-ulation from the current 3,641 mg to 2,300 mg within 10 years. This goal is in line with the Institute of Medicine, which set the “upper tolerable intake”
for adults at 2,300 mg, the World Health Organization goal of 2000 mg or less daily, and the United Kingdom goal of 2,400 mg daily. As health care provid-ers we must work with our patients to identify foods (both processed and fresh) that are lower in sodium; support food manufacturers that lower sodium without raising other potentially harmful additives (potassium or phosphorus); and advocate for government controlled food labeling that gives clear and accurate nutrient information.
Lowering salt is an inexpensive, practical way to have a major impact on population health, mortality and overall health care costs. It behooves the health care com-munity to stand up and loudly applaud this initiative within the Affordable Care Act, but even more so to engage in activi-ties which will ensure its success. ■
Dr. Steiber is Coordinator of the Dietetic Internship/Master’s Degree Program at Case Western Reserve University in Cleveland.
Sodium in American diets comes mainly from restaurant food and from the large amount of processed foods we eat.
© IS
TOCK
PHO
TO.C
OM
/ L
AURI
PAT
TERS
ON
Salt Intake in the U.S.• The 2010 Dietary Guidelines for Americans recommend limiting sodium
intake to 1,500 mg per day for individuals aged 51 year or older.• Most Americans consume more than twice the recommended sodium limit
each day.• 77% of an individual’s salt intake comes from restaurant or processed food;
only 6% is added to food at the table and 5% during cooking.
Sources: Mattes RD, Donnelly D. Relative contributions of dietary sodium sources. J Am Coll Nutr 1991;10:383–93 and the Centers for Disease Control and Prevention.

22 Renal & Urology News MARCH 2012 www.renalandurologynews.com
ED Highly Prevalent Among Men on HemodialysisMOST MEN ON hemodialysis (HD) have erectile dysfunction (ED) and do not receive treatment for the condition, a multinational study found.
Of 946 male HD patients who pro-vided complete data on ED, 83% reported ED and 47% reported severe ED, according to a report published
online ahead of print in Nephrology Dialysis Transplantation. The preva-lence of ED was highest among unmar-ried men (94%). Compared with unmarried men, married men had a 51% lower risk of ED. Each one-year increment in age was associated with a 6% and 10% increased risk of ED
and severe ED, respectively, according to the researchers.
The strongest predictor of ED was depressive symptoms. ED was 2.4 times more likely to occur in men with depressive symptoms than in those without these symptoms. Additionally, compared with employed men, those
receiving a pension or who were unemployed had a 2.0 and 1.8 times increased risk of ED, respectively.
The study also revealed that only 3% of those with ED and 2% of those with severe ED reported receiving pharmacologic treatment. “The rea-sons behind such a lower intervention rate are that we still have suboptimal evidence about the benefi ts and harms of drugs used to treat ED in people on hemodialysis, there is low awareness from treating clinicians, patient embar-rassment and the importance of symp-toms relative to the patients’ overall health concerns,” said lead investigator Prof. Giovanni F. M. Strippoli, MD, PhD, Senior Vice President Scientifi c Affairs of Diaverum AB, a provider of renal services.
The researchers observed that the ED prevalence in men on HD is mark-edly higher than that of the general population, in which 10%-40% of
men report one or more features of sexual dysfunction. The authors pro-posed that men receiving HD should be routinely asked about ED using existing and easily accessible validated instruments.
Dr. Strippoli and his colleagues reported that they were not able to confi rm previous observations that anemia, hypertension, or dyslipidemia were associated with ED risk.
They noted that their study of ED in HD patients is the largest of its kind to date and included men from several HD centers and countries, “facili-tating our ability to identify the key correlates of erectile dysfunction by adjusting for important confounding variables that have not previously been accounted for, particularly depressive symptoms.” Of particular importance, the researchers noted, they collected data on ED and depression using vali-dated instruments.
The researchers evaluated ED using the erectile function domain of the International Index of Erectile Function questionnaire and evalu-ated depressive symptoms using the Center for Epidemiological Studies-Depression Scale. ■
Erectile dysfunction was most strongly associated with depressive symptoms.
Brief Summary: Consult package insert for complete Prescribing Information
INDICATIONS AND USAGE:Bone Metastasis from Solid Tumors. Xgeva is indicated for the prevention of skeletal-related events in patients with bone metastases from solid tumors.
Important Limitation of Use. Xgeva is not indicated for the prevention of skeletal-related events in patients with multiple myeloma (see Clinical Trials [14] in Full Prescribing Information).
DOSAGE AND ADMINISTRATION:Recommended Dosage. The recommended dose of Xgeva is 120 mg administered as a subcutaneous injection every 4 weeks in the upper arm, upper thigh, or abdomen. Administer calcium and vitamin D as necessary to treat or prevent hypocalcemia (see Warnings and Precautions).
Preparation and Administration. Visually inspect Xgeva for particulate matter and discoloration prior to administration. Xgeva is a clear, colorless to pale yellow solution that may contain trace amounts of translucent to white proteinaceous particles. Do not use if the solution is discolored or cloudy or if the solution contains many particles or foreign particulate matter. Prior to administration, Xgeva may be removed from the refrigerator and brought to room temperature (up to 25°C/77°F) by standing in the original container. This generally takes 15 to 30 minutes. Do not warm Xgeva in any other way (see How Supplied/Storage and Handling). Use a 27-gauge needle to withdraw and inject the entire contents of the vial. Do not re-enter the vial. Discard vial after single-use or entry.
HOW SUPPLIED/STORAGE AND HANDLING: Xgeva is supplied in a single-use vial. Store Xgeva in a refrigerator at 2°C to 8°C (36°F to 46°F) in the original carton. Do not freeze. Once removed from the refrigerator, Xgeva must not be exposed to temperatures above 25°C/77°F or direct light and must be used within 14 days. Discard Xgeva if not used within the 14 days. Do not use Xgeva after the expiry date printed on the label. Protect Xgeva from direct light and heat. Avoid vigorous shaking of Xgeva.
CONTRAINDICATIONS: None.
WARNINGS AND PRECAUTIONS: Hypocalcemia. Xgeva can cause severe hypocalcemia. Correct pre-existing hypocalcemia prior to Xgeva treatment. Monitor calcium levels and administer calcium, magnesium, and vitamin D as necessary. Monitor levels more frequently when Xgeva is administered with other drugs that can also lower calcium levels. Advise patients to contact a healthcare professional for symptoms of hypocalcemia (see Adverse Reactions and Patient Counseling Information [17] in full Prescribing Information). Based on clinical trials using a lower dose of denosumab, patients with a creatinine clearance less than 30 mL/min or receiving dialysis are at greater risk of severe hypocalcemia compared to patients with normal renal function. In a trial of 55 patients, without cancer and with varying degrees of renal impairment, who received a single dose of 60 mg denosumab, 8 of 17 patients with a creatinine clearance less than 30 mL/min or receiving dialysis experienced corrected serum calcium levels less than 8.0 mg/dL as compared to 0 of 12 patients with normal renal function. The risk of hypocalcemia at the recommended dosing schedule of 120 mg every 4 weeks has not been evaluated in patients with a creatinine clearance less than 30 mL/min or receiving dialysis.
Osteonecrosis of the Jaw (ONJ). Osteonecrosis of the jaw (ONJ) can occur in patients receiving Xgeva, manifesting as jaw pain, osteomyelitis, osteitis, bone erosion, tooth or periodontal infection, toothache, gingival ulceration, or gingival erosion. Persistent pain or slow healing of the mouth or jaw after dental surgery may also be manifestations of ONJ. In clinical trials, 2.2% of patients receiving Xgeva developed ONJ; of these patients, 79% had a history of tooth extraction, poor oral hygiene, or use of a dental appliance (see Adverse Reactions). Perform an oral examination and appropriate preventive dentistry prior to the initiation of Xgeva and periodically during Xgeva therapy. Advise patients regarding oral hygiene practices. Avoid invasive dental procedures during treatment with Xgeva. Patients who are suspected of having or who develop ONJ while on Xgeva should receive care by a dentist or an oral surgeon. In these patients, extensive dental surgery to treat ONJ may exacerbate the condition.
ADVERSE REACTIONS: The following adverse reactions are discussed below and elsewhere in the labeling:
(see Warnings and Precautions)(see Warnings and Precautions)
The most common adverse reactions in patients receiving Xgeva (per-patient incidence greater than or equal to 25%) were fatigue/asthenia, hypophosphatemia, and nausea (see Table 1). The most common serious adverse reaction in patients receiving Xgeva was dyspnea. The most common adverse reactions resulting in discontinuation of Xgeva were osteonecrosis and hypocalcemia.
Clinical Trials Experience. Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in other clinical trials and may not reflect the rates observed in practice. The safety of Xgeva was evaluated in three randomized, double-blind, double-dummy trials (see Clinical Trials [14] in full Prescribing Information) in which a total of 2841 patients with bone metastasis from prostate cancer, breast cancer, or other solid tumors, or lytic bony lesions from multiple myeloma received at least one dose of Xgeva. In Trials 1, 2, and 3, patients were randomized to receive either 120 mg of Xgeva every 4 weeks as a subcutaneous injection or 4 mg (dose adjusted for reduced renal function) of zoledronic acid every 4 weeks by intravenous (IV) infusion.
Entry criteria included serum calcium (corrected) from 8 to 11.5 mg/dL (2 to 2.9 mmol/L) and creatinine clearance 30 mL/min or greater. Patients who had received IV bisphosphonates were excluded, as were patients with prior history of ONJ or osteomyelitis of the jaw, an active dental or jaw condition requiring oral surgery, non-healed dental/oral surgery, or any planned invasive dental procedure. During the study, serum chemistries including calcium and phosphorus were monitored every 4 weeks. Calcium and vitamin D supplementation was recommended but not required. The median duration of exposure to Xgeva was 12 months (range: 0.1 – 41) and median duration on-study was 13 months (range: 0.1 – 41). Of patients who received Xgeva, 46%
and 3% Black. The median age was 63 years (range: 18 – 93). Seventy-five percent of patients who received Xgeva received concomitant chemotherapy.
Table 1. Per-patient Incidence of Selecteda Adverse Reactions of Any Severity (Trials 1, 2, and 3)
a Adverse reactions reported in at least 10% of patients receiving Xgeva in Trials 1, 2, and 3, and meeting one of the following criteria:
5% greater incidence in patients treated with zoledronic acid compared to placebo (US Prescribing Information for zoledronic acid)
b Laboratory-derived and below the central laboratory lower limit of normal [8.3 – 8.5 mg/dL (2.075 – 2.125 mmol/L) for calcium and 2.2 – 2.8 mg/dL (0.71 – 0.9 mmol/L) for phosphorus]
Severe Mineral/Electrolyte Abnormalities
1.75 mmol/L) occurred in 3.1% of patients treated with Xgeva and 1.3% of patients treated with zoledronic acid. Of patients who experienced severe hypocalcemia, 33% experienced 2 or more episodes of severe hypocalcemia and 16% experienced 3 or more episodes (see Warnings and Precautions and Use in Specific Populations).
than 0.6 mmol/L) occurred in 15.4% of patients treated with Xgeva and 7.4% of patients treated with zoledronic acid.
Osteonecrosis of the JawIn the primary treatment phases of Trials 1, 2, and 3, ONJ was confirmed in 1.8% of patients in the Xgeva group and 1.3% of patients in the zoledronic acid group (see Warnings and Precautions). When events occurring during an extended treatment phase of approximately 4 months in each trial are included, the incidence of confirmed ONJ was 2.2% in patients who received Xgeva. The median time to ONJ was 14 months (range: 4 – 25).
Immunogenicity. As with all therapeutic proteins, there is potential for immunogenicity. Using an electrochemiluminescent bridging immunoassay, less than 1% (7/2758) of patients with osseous metastases treated with denosumab doses ranging from 30 – 180 mg every 4 weeks or every 12 weeks for up to 3 years tested positive for binding antibodies. No patient with positive binding antibodies tested positive for neutralizing antibodies as assessed using a chemiluminescent cell-based in vitro biological assay. There was no evidence of altered pharmacokinetic profile, toxicity profile, or clinical response associated with binding antibody development. The incidence of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of a positive antibody (including neutralizing antibody) test result may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of antibodies to denosumab with the incidence of antibodies to other products may be misleading.
DRUG INTERACTIONS: No formal drug-drug interaction trials have been conducted with Xgeva. In clinical trials in patients with breast cancer metastatic to bone, Xgeva was administered in combination with standard anticancer treatment. Serum denosumab concentrations at 1 and 3 months and reductions in the bone turnover marker uNTx/Cr (urinary N-terminal telopeptide corrected for creatinine) at 3 months were similar in patients with and without prior intravenous bisphosphonate therapy. There was no evidence that various
anticancer treatments affected denosumab systemic exposure and pharmacodynamic effect. Serum denosumab concentrations at 1 and 3 months were not altered by concomitant chemotherapy and/or hormone therapy. The median reduction in uNTx/Cr from baseline to month 3 was similar between patients receiving concomitant chemotherapy and/or hormone therapy (see Clinical Pharmacology [12.2] in full Prescribing Information).
USE IN SPECIFIC POPULATIONS:Pregnancy: Category C. There are no adequate and well-controlled trials of Xgeva in pregnant women. Use Xgeva during pregnancy only if the potential benefit justifies the potential risk to the fetus. Encourage women who become pregnant during Xgeva treatment to enroll in Amgen’s Pregnancy SurveillanceProgram. Patients or their physicians should call 1-800-77-AMGEN (1-800-772-6436) to enroll. In an embryofetal developmental study, cynomolgus monkeys received subcutaneous denosumab weekly during organogenesis atdoses up to 6.5-fold higher than the recommended human dose of 120 mg every 4 weeks, based on body weight (mg/kg). No evidence of maternal toxicity
during the first trimester, and fetal lymph nodes were not examined. Potential adverse developmental effects resulting from exposures during the second and third trimesters have not been assessed in animals (see Nonclinical Toxicology [13.2] in full Prescribing Information). In genetically engineered mice in which the gene for RANK ligand (RANKL) has been deleted (a “knockout mouse”), the absence of RANKL caused fetal lymph node agenesis and led to postnatal impairment of dentition and bone growth. Pregnant RANKL knockout mice also showed altered maturation of the maternal mammary gland, leading to impaired lactation postpartum (see Use in Nursing Mothers).
Nursing Mothers. It is not known whether Xgeva is excreted into human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from Xgeva, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother. Maternal exposure to Xgeva during pregnancy may impair mammary gland development and lactation based on animal studies in pregnant mice lacking the RANK/RANKL signaling pathway that have shown altered maturation of the maternal mammary gland,leading to impaired lactation postpartum (see Nonclinical Toxicology [13.2] infull Prescribing Information).
Pediatric Use. The safety and effectiveness of Xgeva in pediatric patients have not been established. Treatment with Xgeva may impair bone growth inchildren with open growth plates and may inhibit eruption of dentition. In neonatal rats, inhibition of RANKL with a construct of osteoprotegerin bound toFc (OPG-Fc) at doses less than or equal to 10 mg/kg was associated with inhibition of bone growth and tooth eruption. Adolescent monkeys dosed with denosumab at 5 and 25 times (10 and 50 mg/kg dose) higher than therecommended human dose of 120 mg subcutaneously every 4 weeks (based on body weight mg/kg) had abnormal growth plates (see Nonclinical Toxicology [13.2] in full Prescribing Information).
Geriatric Use. Of patients who received Xgeva in Trials 1, 2, and 3, 1260 (44%) were 65 years of age or older. No overall differences in safety or efficacywere observed between these patients and younger patients.
Renal Impairment. In a trial of 55 patients without cancer and with varying degrees of renal function who received a single dose of 60 mg denosumab, patients with a creatinine clearance of less than 30 mL/min or receiving dialysis were at greater risk of severe hypocalcemia with denosumab compared to patients with normal renal function. The risk of hypocalcemia at the recommended dosing schedule of 120 mg every 4 weeks has not been evaluated in patients with a creatinine clearance of less than 30 mL/min or receiving dialysis (see Warnings and Precautions, Adverse Reactions, and Clinical Pharmacology [12.3] in full Prescribing Information).
OVERDOSAGE: There is no experience with overdosage of Xgeva.
PATIENT COUNSELING INFORMATION:Advise patients to contact a healthcare professional for any of the following:
twitching, spasms, or cramps (see Warnings and Precautions and Adverse Reactions)
the jaw, mouth, or teeth (see Warnings and Precautions and Adverse Reactions)
(see Warnings and Precautions)
(see Use in Specific Populations)Advise patients of the need for:
Advise patients that denosumab is also marketed as Prolia®. Patients should inform their healthcare provider if they are taking Prolia®.
Body SystemXgeva
n = 2841 %
Zoledronic Acid n = 2836
%
GA STROINTESTINAL Nausea Diarrhea
31 20
32 19
GE NERAL Fatigue/ Asthenia
45
46
IN VESTIGATIONS b
b
18 32
9
20
NE UROLOGICAL 13
14
RE SPIRATORY Dyspnea Cough
21 15
18 15
Amgen Manufacturing Limited, a subsidiary of Amgen Inc.One Amgen Center Drive
Thousand Oaks, California 91320-1799©2011 Amgen Inc.
All rights reserved. Printed in USA.
©2011 Amgen Inc. All rights reserved. 63850-R1-V1 12/11 www.XGEVA.com
REFERENCES: 1. Saad F, Gleason DM, Murray R, et al, for the Zoledronic Acid Prostate Cancer Study Group. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with
metastatic hormone-refractory prostate cancer. J Natl Cancer Inst. 2004;96:879-882. 2. Ibrahim A, Scher N, Williams G, et al. Approval summary for zoledronic acid for treatment of multiple myeloma and cancer
bone metastases. Clin Cancer Res. 2003;9:2394-2399. 3. Yu EY, Nathan FE, Higano CS. Role of detection of metastatic disease as a leading cause of screening failure in an ongoing phase III trial of zibotentan
versus placebo in patients with nonmetastatic castration-resistant prostate cancer (CRPC). J Clin Oncol. 2011;29(suppl 7). Abstract 135. 4. Scher HI, Morris MJ, Kelly WK, Schwartz LH, Heller G. Prostate cancer clinical
trial end points: “RECIST”ing a step backwards. Clin Cancer Res. 2005;11:5223-5232. 5. Tannock IF, de Wit R, Berry WR, et al, for the TAX 327 Investigators. Docetaxel plus prednisone or mitoxantrone plus prednisone for
advanced prostate cancer. N Engl J Med. 2004;351:1502-1512. 6. Petrylak DP, Tangen CM, Hussain MHA, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate
cancer. N Engl J Med. 2004;351:1513-1520. 7. XGEVA® (denosumab) prescribing information, Amgen. 8. Saad F, Gleason DM, Murray R, et al, for the Zoledronic Acid Prostate Cancer Study Group. A randomized, placebo-
controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94:1458-1468.

BY JIWAN K. THAPA, MD, GEORGE THOMAS, MD, ROBERT STEIN, MD, AND EMMANUEL L. BRAVO, MD
A 43-year-old man was evaluated for uncontrolled hypertension (HTN) despite multiple drug
therapy, which included amlodipine 10 mg daily, clonidine 0.3 mg BID, and metoprolol XL 200 mg BID. He had several episodes of hypokalemia (2.7-3.0 mmol/L) over the years that persist-ed despite oral potassium supplementa-tion and discontinuing diuretics.
On examination, he had elevated blood pressure (BP) in both arms (160/110 mm Hg) with a heart rate of 60 beats/minute. Physical examination was otherwise unre-markable. His laboratory tests showed serum potassium (K) of 2.8 mmol/L, serum bicarbonate of 33 mmol/L, and serum creatinine of 1.48 mg/dL with esti-mated GFR of 55 mL/min/1.73 m2.
Plasma aldosterone (PAC) was 33 ng/dL and plasma renin activity (PRA) was less than 0.1 µg/L/hour. A 24-hour urine collection with salt load-ing showed urinary potassium wasting (60 mmol) and high aldosterone excre-tion (42 µg). An adrenal computed tomography scan revealed a low-density 1.5 × 1.2 cm nodule in the left adrenal gland (Figure 1). He was started on eplerenone 100 mg BID, which con-trolled his BP (123/78 mm Hg on sit-ting and 122/70 mm Hg on standing). Serum K normalized (4.0 mmol/L) without need for supplementation.
The patient wished to undergo sur-gery. Adrenal venous sampling showed lateralization to the left (See table).
Surgical pathology after laparoscop-ic unilateral left adrenalectomy con-fi rmed the diagnosis of adrenocortical adenoma. Eplerenone was stopped post-operatively. Plasma aldosterone
decreased to 3.3 ng/dL with a PRA of 0.8 µg/L/hour. Over the next year, his serum potassium remained normal (4.0-5.0 mmol/L) without supplemen-tation and his BP was well-controlled (below 120/80 mm Hg) on amlodipine 10 mg alone.
DiscussionResistant HTN is defi ned as persistent elevation of BP above goal in spite of concurrent use of three anti-hyper-tensive agents, each of unique class, including a diuretic, with all drugs at maximally tolerated doses. HTN that is controlled with the use of four or more medications is also considered resistant to treatment. It is so defi ned to identify patients who are more like-ly to have reversible causes of HTN. Consultation with a HTN specialist should be considered if goal BP cannot be achieved. Evaluation for secondary causes should be done in patients with resistant HTN, and a high suspicion of primary aldosteronism (1°A) should be entertained in patients with the follow-ing clinical history: 1) spontaneous or unprovoked hypokalemia with renal potassium wasting, 2) severe diuretic-induced hypokalemia (potassium 3.0 mEq/L or less), which does not normal-
ize after discontinuation of diuretics for at least four weeks and is unresponsive to angiotensin blockers, 3) hypertension with adrenal adenoma, and 4) family history of 1°A. ■
The authors are affi liated with the Cleveland Clinic’s Glickman Urologi-cal and Kidney Institute
REFERENCES
1. Bravo EL. Primary aldosteronism. Issues in diagnosis and management. Endocrinol Metab Clin North Am. 1994;23:271-283. Review.
2. Thomas G, Bravo EL. Outpatient evaluation of secondary causes of resistant hypertension. US Cardiology 2011;8:102–107. Review
3. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientifi c statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hyperten-sion 2008;51:1403-1419.
On the Forefront Urologists and nephrologists working together: an emerging model of patient care
Resistant Hypertension Secondary to Primary Aldosteronism
BY SURAFEL GEBRESELASSIE, MD,EMMANUEL BRAVO, MD, AND JIHAD KAOUK, MD
P rimary aldosteronism was first described by Jerome Conn in 1955 in a patient with an aldosterone-
producing adrenal adenoma. It’s now a widely recognized cause of secondary hypertension. The following case illus-trates the challenges of making clini-cal diagnosis of aldosterone producing adrenal adenoma.
A middle-aged woman with medullary sponge kidney and nephrocalcinosis was fi rst diagnosed with adrenal mass on a computed tomography scan performed for kidney stone evaluation about 10 years previously (Figure 2). She had normal
serum potassium and serum bicarbonate levels. Subsequently, she was found to have elevated blood pressure and was referred to the Department of Nephrology and Hypertension for further evalua-tion. Her serum aldosterone level was 475.5 ng/dL. Despite achieving 290 mmol/day of urinary sodium, she had no kaliuresis following an oral salt loading test. The urinary aldosterone level was 231 µg/day. After further discussion with colleagues in the Department of Urology, the patient successfully underwent robotic-assisted lapara-scopic adrenalectomy. She became normotensive requiring no further antihypertensive medication.
Aldosterone is a potent mineralocor-ticoid secreted by the zona glomerulosa
of the adrenal cortex. Unlike cortisol, which is inactivated to cortisone by 11-β hydroxysteroid dehydrogenase, aldoster-one avidly binds to the mineralocorticoid receptor in the distal nephrone leading to sodium retention resulting in anti-natri-
uresis, volume expansion, hypertension, metabolic alkalosis and renal potassium wasting. The patient had a very high levels of circulating serum aldosterone (475.5 ng/dL) but did not present with hypokalemia or metabolic alkalosis, and did not have resistant hyperten-sion, which delayed the diagnosis of aldosterone-producing adenoma. We thought that the renal tubular disease resulting from nephrocalcinosis caused the distal tubule to be resistant to the action of aldosterone even in the pres-ence of high distal sodium delivery and high aldosterone levels. ■
The authors are affi liated with the Cleveland Clinic’s Glickman Urologi-cal and Kidney Institute
Unusual Manifestation of an Aldosterone-Producing Adenoma
Figure 2. Adrenal CT showing left adrenal adenoma and bilateral nephrocalcinosis.
Aldosterone Versus Cortisol LevelsAldosterone ng/dL Cortisol ug/dL A/C ratio
Left Adrenal 15,230 545 27.9
Right Adrenal 426.3 615 0.69
Low IVC 64.6 16.5 3.9Left adrenal vein A/C ratio divided by Right adrenal vein A/C ratio (value >4 indicates lateralization to left adrenal) Right adrenal vein A/C ratio divided by low Inferior Vena Cava (IVC) A/C ratio (value <1.0 indicates suppression of aldosterone secretion from the right adrenal)
Figure 1. CT scan showing left adrenal adenoma
www.renalandurologynews.com MARCH 2012 Renal & Urology News 23

Rituximab Ineffective as an LN Add-OnUsed with MMF and corticosteriods, the drug did not boost partial renal response rates
BY ROSEMARY FREI, MScADDING RITUXIMAB to mycophe-nolate mofetil (MMF) and corticos-teroids does not improve outcomes in patients with lupus nephritis (LN), data show.
As part of the Lupus Nephritis Assessment with Rituximab (LUNAR) trial, American and Mexican investiga-tors led by Brad H. Rovin, MD, Director of Nephrology at the Ohio State College of Medicine in Columbus, Ohio, studied 144 patients (aged 16-75 years) with class III or IV LN who were taking MMF and corticosteroids. They randomized 72 subjects to receive add-on therapy with 1000 mg rituximab on days 1, 15, 168, and 182, and 72 to receive placebo on the same schedule.
Rituximab treatment was not associ-ated with a higher rate of complete or partial renal responses at the end of the study, with a 56.9% rate compared to 45.8% for placebo, the research-ers reported online ahead of print in Arthritis & Rheumatism.
“At this time, we cannot recommend the addition of rituximab to MMF for
the initial therapy of proliferative lupus nephritis,” Dr. Rovin concluded. “We suspect that there are patients who may benefi t from rituximab, but we still need to develop methods to identify who they are.”
LN can occur in up to 50% of patients with systemic lupus erythematosus and is not associated with a good prog-nosis. Furthermore, standard prolif-erative treatment of LN achieves renal response rates of only 50%-80%, and many patients achieve partial rather than full remission. Because B cells have been shown to play a key role in LN, and because rituximab depletes CD20-positive B cells while sparing stem cells and plasma cells, Dr. Rovin’s team opted to study rituximab as add-on LN therapy.
Treatment protocolMMF was fi rst given at 1.5 g/day in three divided doses and increased, as tolerated, to 3 g/day by week 4 and continued until at least week 52. In addition, patients received oral pred-nisone 0.75 mg/kg/day up to a maxi-
mum of 60 mg until day 16, and were tapered to 10 mg/day or less by week 16. Other immunosuppressive agents were not permitted.
Rituximab depleted peripheral CD19+ B cells in 98.6% of ritux-imab-treated patients (71/72). The
study, however, demonstrated no significant difference in the rate of the primary endpoint—complete and partial renal responses—between the two groups. Moreover, the small differ-ence in the rate was primarily due to more partial responses with rituximab, according to the investigators.
Rates of serious adverse events, including infections, were similar in both groups. Neutropenia, leucopenia, and hypotension were more frequent in the rituximab group.
“Further randomized trials with rituximab can help clarify the role of rituximab in LN treatment, includ - ing whether rituximab should be used in place of MMF or cyclo -phosphamide instead of as add-on therapy, and whether rituximab has a role in salvaging patients with refrac - tory LN,” Dr. Rovin stated. “These studies remain to be set up, but the results of an ongoing U.K. investigation of rituximab as a primary therapy will be reported soon; results presented in abstract form at scientifi c meetings indi-cate this approach has promise.” ■
Brad H. Rovin, MD
Deceased Donor Tx Rates DecliningDIALYSIS PATIENTS waiting for a deceased donor kidney transplant face a declining likelihood of receiving one, according to a recent study.
The study, by researchers at the Medical College of Wisconsin in Milwaukee, examined data from 70,891 patients receiving dialysis and who were waitlisted for their fi rst deceased donor renal transplant between January 1996 and December 2005. Patients waitlisted in 1998, 2000, 2002, and 2004 were, respectively, 15%, 27%, 37%, and 42% less likely than patients
waitlisted in 1996 to receive a kidney within 12 months, researchers reported in The American Journal of Medicine (2012;125:57-65).
“It is apparent that current efforts are not enough and creative strategies are needed to improve transplanta-tion rates,” the authors wrote. “These should include enhancing organ dona-tion from both living and deceased donors. Increased effort to enhance public education that might result in increasing deceased donor donation is an important consideration.”
Investigators also observed that certain subgroups receiving long-term dialysis have a greater likelihood of dying before receiving a kidney transplant. These include the elderly and blacks and those with diabetic end-stage renal disease. In addition, although the transplantation ratio is nearly equal for male and female patients, women have a higher death ratio than men. “As a result, women are disadvantaged such that the chance of dying before receiving the benefi t of a transplant is greater compared with men,” the researchers observed. ■
PSMs Predict PCa Recurrence in Some MenPOSITIVE SURGICAL margins (PSMs) are a risk factor for biochemi-cal recurrence of prostate cancer (PCa) in patients who have undergone radical prostatectomy for intermediate-risk disease, researchers reported online in BJU International.
Niall Corcoran, MD, of the Leslie and Gordon Diamond Health Care
Centre in Vancouver, British Columbia, and colleagues studied 1,514 patients who underwent radical prostatectomy for PCa. Of these, 276 (18.2%), 761 (50.3%), and 477 (31.5%) had low-, intermediate-, and high-risk disease, respectively. Investigators identifi ed PSMs in 370 men (24.4%). The PSM rate rose from 11% in men with low-
risk disease to 43% in those with high-risk disease.
After a median follow-up of 22.2 months, 165 (7%) experienced bio-chemical recurrence. Multivariate analysis revealed that PSMs were a signifi cant predictor of biochemical recurrence only men with intermediate-risk disease. ■
ED Linked to Atopic DermatitisMEN WITH ERECTILE dysfunction (ED) are more likely to have had prior atopic dermatitis than men without ED, according to study fi ndings pub-lished online in the Journal of Sexual Medicine.
Investigators led by Herng-Ching Lin, PhD, of Taipei Medical University in Taiwan, compared 3,997 men with newly diagnosed ED and 19,985 men without a history of ED (controls). Of the 23,982 subjects, 1,758 had been previously diagnosed with atopic der-matitis: 425 (10.6%) in the ED group versus 1,333 (6.7%) in the control group. Men with ED were 60% more likely to have prior atopic dermatitis than controls, after adjusting for hy-pertension, diabetes, coronary heart disease, and other potential confound-ing factors. ■
24 Renal & Urology News MARCH 2012 www.renalandurologynews.com

Adherence to diet, medicine, scheduling, and follow-up helped Ed Strudwick survive 39 years on hemodialysisBY ROBERT S. RIGOLOSI, MD
What the ‘HD Marathon Man’ Teaches Us
■ FROM THE EDITORIAL ADVISORY BOARD
As Ed Strudwick’s neph-rologist for every day of his remarkable 39 years and nine months on dial-
ysis (Renal & Urology News, “The Hemodialysis Marathon Man,” October 2007; (www.renalandurologynews.com/search/marathon+man/) until his recent death from septicemia at age 71, I would like to revisit some of the valuable lessons that this experience has reinforced for me.
Remind your dialysis patients that adherence is key. Ed’s longevity was due to his full adherence to diet, medi-cine, scheduling, and follow-up. If you have a compliant patient like this, you can expect long-term survival. We have about 200 patients on dialysis in our center, and I would guess that 10% or 15% of them have been on dialysis for more than 35 years. We may have another 10% that have been on 20 to 30 years. Patients do best when they embrace their new disease-driven life-style and accept what they have to do. Be sure they understand that they can’t be too careful. For example, if they go off their diet by eating a high-potassi-um-containing food and then become hyperkalemic, all the work they have done during the course of their dialysis time—whether months or years—is wasted because they’re hyperkalemic, and that can be fatal. So these things have to be avoided.
Staff diligence matters. Dialysis patients don’t have much leeway in terms of how much they can cheat. We’ve had patients gain 15 pounds kin the 48 hours between sessions. They can’t do that repeatedly and survive a long time. They might be able to get away with it once or twice,
or maybe even fi ve or six times, but the staff has to be very attentive and get right on top of them, pointing out why they can’t do what they’re doing, educating them, and encourag-ing them. Nutritionists are key, as are the nurses getting involved with the care. Certainly Ed was down in the dumps on many occasions. The staff would bring it to the doctors’ atten-tion and would try to help him work through those issues, which I believe
contributed to his longevity. Patients really have two supportive teams: One is their family and friends, and the other is their professional team—the nephrologist, the nurse, the dietitian, the social worker.
Don’t lose the patient relationship. Today, we’re being encouraged to use electronic systems to record our patients’ visits. And what’s happening is, physicians are losing that personal contact. For example, I’ve seen young doctors take a patient’s history while keeping their eyes on their computer as they input the data, only occasion-ally glancing at the patient. In this age of computerization, I hope we don’t lose that personal eye-to-eye contact
with the patient. Talk to your patients and their families regularly, and try to stay engaged with them. Let the patient know that he or she can call you to discuss a problem. You have a social worker who can always help them through personal issues and fam-ily issues. Ed Strudwick had a personal rapport with the staff that made it less of a chore for him to come in three times a week, 156 times a year, for 39 years. His nurse, Karen, could tell you
everything that was going on with his family, down to his grandchildren. And when Ed reached his 30th or 35th year on dialysis, we even marked the occasion by buying him and his wife tickets to a Broadway show and a nice dinner.
Encourage home dialysis. I think home dialysis treatment is preferable. Ed had a cadaver transplant in 1977, only about four years into his dialysis treatment. The testing between the donor and the recipient wasn’t as good as it is now, and Ed had a very bad experience: His body rejected the kidney before he ever got out of the hospital. We tried to send him back for another transplant, but he refused.
But at the time, we had a large home hemodialysis program. We taught his wife how to do his home hemodialysis, and he was happy with that. He was able to get back to work and dialyze at home. He stayed on that for about 15 years after the failed transplant. We don’t have many home hemodialysis patients anymore, but now we have a large peritoneal dialysis program here, and the patients love doing home peri-toneal dialysis because they can eat more, they can drink more, they’re more independent, they can dialyze around their own schedule; everything is much more fl exible. And home peri-toneal dialysis is more rehabilitative and less expensive for the government than in-center hemodialysis.
Give patients hope. I share the example of Ed Strudwick with pre-dialysis patients, because when you’re telling these people that they’re about to start a treatment that requires them to come in three times a week to sur-vive, and that they have to do that for the rest of their lives if they don’t get a kidney transplant, you do have to give them hope. I can tell them, “You can do well with this treatment as long as you follow certain instructions and listen to your staff members; I had a patient who lived 39 years that way.” Ed saw two daughters get mar-ried and four or fi ve grandchildren born during his time on dialysis, some-thing many people would not expect could happen. ■
Dr. Rigolosi is Director of the Regional Hemodialysis Center at Holy Name Hospital in Teaneck, N.J. He is a mem-ber of the Renal & Urology News Edi-torial Advisory Board.
www.renalandurologynews.com MARCH 2012 Renal & Urology News 25
Dialysis in the U.S.• As of December 31, 2009, the U.S. had 370,274 patients on hemodialysis
and 22,522 on peritoneal dialysis• The adjusted rates of all-cause mortality for dialysis patients in the 2009
were 6.5-7.4 times greater than those of the general population• In 2004, the adjusted survival fi ve-year survival probability for hemodialysis
patients was 34%.
Source: U.S Renal Data System 2011 Annual Data Report

26 Renal & Urology News MARCH 2012 www.renalandurologynews.com
Malpractice News BY ANN W. LATNER, JD
Distracted Care Can Lead To Increase in Malpractice
While the innovation of such things as cell phones, iPads, social network-ing sites, and the Internet can often be a boon when it comes to gaining or sharing clinical information on the go, they can also be a distraction to health care professionals. A recent New York Times report highlighted this issue, which was termed “distracted doctoring.” According to the report, clinicians have been found to use their smart phones and tablet computers for personal reasons—social networking, checking news, airfare prices, and the like—while engaging in patient care, and not simply to access drug infor-mation or patient data. When used to obtain clinical information, these devices can be strong support tools, but individual browsing (while on the job) can compromise patient safety and has led to errors.
A recent study of 439 perfusionists and supporting technicians illuminates this problem (Perfusion 2011;26:375-380). This survey of clinicians who perform car-diopulmonary bypass (CPB) showed that more than 55% of respondents admitted to using a cell phone while performing CPB. In addition, 49% reported send-ing text messages during the procedure. For those who had smart phone features, 21% admitted to checking e-mail, 15% used the Internet, and 3% posted on social networking sites during surgery. And yet more than 78% of the sur-veyed participants stated that cell phone use in the operating room (OR) could introduce a signifi cant safety risk to patients.
The New York Times case cited above prolifes an incident where a patient was left partially paralyzed after surgery, during which a distracted neurosurgeon used a wireless headset to make at least 10 personal calls. This case was settled out of court.
Many hospitals are addressing this new safety issue by instituting policies
that restrict the use of cell phones, smart phones, and other electronic devices in hospital. The Oregon Health and Science University (OHSU) Hospital in Portland instituted a policy establishing operating rooms as “quiet zones,” after complaints that staff cli-nicians were using smart phones (to check or send e-mails) while intu-bating patients. After the policy was fi rmly in place, an OHSU nurse was formally reprimanded for checking airline prices (on an OR computer) during a spinal operation.
Younger clinicians are more apt to use these new devices, so medical schools are starting to incorporate policy edicts during training, stress-ing the importance of using technol-ogy only for garnering patient-related information.
Malpractice Attorney Charged with Theft
A New York attorney is charged with stealing $70,000 from his cli-ents, according to Rockland County District Attorney, Thomas P. Zugibe. The clients, a husband and wife, were plaintiffs in a medical malpractice case. The defendant sent a $70,000 check directly to the couple in an effort to settle the case. The plaintiffs did not want to settle for less than $350,000 and told their attorney this when they
handed the check over to him. The prosecutor allegedly told his clients that he would return the check to the other party in the lawsuit, but instead deposited the money into his personal bank account. The attorney in question then falsely fi led an agree-ment and release to settle the case for $70,000—without the knowledge or consent of his clients.
The counselor was subsequently charged with grand larceny in the sec-ond degree, criminal possession of a forged instrument, and offering a false instrument for fi ling. He faces up to 15 years in prison.
In a press release, Zugibe said the defendant in this case “is accused of betraying his clients. Having already been injured by the negligent acts of others, this unsuspecting couple was again victimized by their lawyer. This arrest should serve as a warning to unscrupulous professionals who seek to prey on their clients.”
$9 Million Wyoming Verdict Is Largest on Record
A jury recently found in favor of a Wyoming man, the plaintiff in a mal-practice lawsuit, and awarded a record-breaking $9 million in damages.
The plaintiff was a 51-year old oilfi eld worker whose truck slid off an icy road and rolled over several times before landing upside down. Emergency medi-cal service (EMS) workers arrived on the scene, freed the man from the truck and immediately immobilized him with a backboard. The EMS team then put a brace on the man’s neck. The plain-tiff was conscious when he arrived at Campbell County Memorial Hospital in Gillette and was complaining of neck pain. The attending ER physician immediately ordered X-rays and CT scans of the accident victim’s head, thoracic spine, and facial bones—but not of his neck.
The physician ultimately released the patient without a cervical collar and without performing a full physi-cal exam.
The patient returned to the hospital four days later with extreme pain in his left shoulder and neck and weakness
in his left arm. Further tests revealed that the man had a broken neck and he then underwent emergency neck-fusion surgery. Because of the initial failure to diagnose the fracture, the plaintiff suffered permanent C5 nerve root injuries and had to undergo a sec-ond neck fusion.
In fact, the plaintiff will need addi-tional surgeries, including the implanta-tion of a spinal cord stimulator in hopes of reducing intense, chronic pain.
At trial date, the plaintiff was still not back at work due to disability, and, because of chronic pain, was largely confi ned to his home.
At trial, the doctor denied that he had failed to perform a physical exam; however, on cross-examination, his own defense expert testifi ed that if the exam
had actually been performed, the plain-tiff’s obvious and intense pain should have prompted would have indicated that X-rays were required.
The jury found the physician and the hospital negligent and awarded the plaintiff damages in the amount of $7 million plus an additional $2 million to the plaintiff’s wife for loss of con-sortium. Prior to this, the record-high malpractice award in Wyoming had been $1.5 million. ■
Ms. Latner, a former criminal defense attorney, is a freelance medical writer in Port Washington, N.Y.
© M
ICHA
EL D
ON
NE
/ PH
OTO
RES
EARC
HERS
, IN
C.
© IS
TOCK
PHO
TO.C
OM
/ S
VARI
OPH
OTO
Many clinicians admit to using social media sites during surgical procedures.
An ER physician missed an injured worker’s broken neck.
For more Malpractice News articles, please visit
renalandurologynews.com

www.renalandurologynews.com MARCH 2012 Renal & Urology News 27
Web-Based Tools Speed Donor ScreeningPotential kidney donors fi ll out an online form that helps transplant centers evaluate eligibility
BY ROSEMARY FREI, MScMIAMI BEACH, FLA.—Web-based preliminary screening of potential kidney donors has resulted in a fl ood of applica-tions at two U.S. transplant centers.
It only takes potential donors a couple of minutes to confi dentially answer ques-tions about whether they have hyperten-sion, diabetes, frequent kidney stones or hepatitis, and whether they are current smokers or users of illicit drugs. The websites differentiate between abso-lute ineligibility—for example, having hepatitis C, HIV, or diabetes—and rela-tive ineligibility, such as being obese or currently smoking. Potential donors can then either proceed to a longer web-based health-status questionnaire or are brought to a webpage stating they are not currently suitable candidates.
The paperless format makes it easy to screen large numbers of people quickly and for people needing kidneys to alert friends and family by simply e-mailing the screening website’s URL.
Details of web-based donor screening programs at the University of California-San Francisco (UCSF) and Vanderbilt University in Nashville, Tenn., were presented at the American Society of Transplant Surgeons’ 2012 Annual State of the Art Winter Symposium.
“We’re having to redo some of our workflow because we’re getting so many potential donors—for example, one of the people on our transplant wait list has 19 potential donors,” said John Roberts, MD, Chief of Transplantation at UCSF. “It’s much more unlikely to get multiple potential donors stepping forward when the screening question-naire is on paper. That’s why we’re really excited about online screening.”
The Vanderbilt Kidney/Pancreas Transplant Program is having a simi-lar experience with their online kid-ney donor intake form, available at https://www.vanderbilthealth.com/transplant/30936.
“We are very excited about this new web-based tool and feel that it can be easily incorporated into many transplant programs,” noted Deonna Moore, MSN, a nurse practitioner for the Vanderbilt program who has been instrumental in the development and application of the web-based tool that has been in use since January 2011. In the past year, the tool has been used to screen more than 600 potential donors.
“The features of the web-based appli-cation increase the transplant center’s ability to attract donors and process them effi ciently, with the ultimate goal
being to potentially increase living kid-ney donation,” she said.
“One of the things I’ve been amazed about is the percentage of people who have Internet access and seem able to use it,” Dr. Roberts noted.
The UCSF website uses a BREEZE Transplant (MedSleuth, Inc., San Francisco; http:www.medsleuth.com/transplant/) platform. An analysis by Dr. Roberts’ team of 200 consecutive users of the website showed there was a 98% satisfaction rating and a 96% rating for ease of use. Moreover, since
the web-based approach was imple-mented there has been a 41% increase in rate of donor-questionnaire comple-tion and 50% increased productivity of the transplant nurse coordinators.
Another benefit is the immediate availability of donor information to clinicians compared with the previous several-week delay with paper-based screening.
Both the UCSF and Vanderbilt pro-grams have found that approximately 25% of people screened online are not suitable donors. ■
Donna Moore, MSN
Transplant-Related Urinary Complications DefinedBY ROSEMARY FREI, MScMIAMI BEACH, FLA.—A review of 635 kidney transplants performed at the University of Florida, Gainesville, has confi rmed that transplanted kidneys with more than one renal artery places recipients at increased risk for urinary complications.
The researchers found that renal-artery multiplicity in transplanted kidneys is associated with a statisti-cally signifi cant 2.5-fold higher risk of urinary complications compared with organs that have only one renal artery, according to a poster presentation at the American Society of Transplant Surgeons’ 2012 Annual State of the Art Winter Symposium.
Rupak Kulkarni, MD, and three other transplant surgeons analyzed the urinary complication outcomes of transplants performed between December 1, 2006 and December 31, 2010. All patients had at least six
months of follow-up data available.They evaluated 34 characteris-
tics of the donors and recipients. These included some parameters that have been evaluated in previous research–including donor and reci - pient age, donor and recipient race, and cold ischemia time of more than 24 hours. They also analyzed some that had not been previously exam-
ined, including whether the kidneys had been imported from outside of the local catchment area.
Urinary complications developed in 19 (4.6%) of the 635 transplants. These included 17 strictures (58.6%), seven leaks (24.1%), and fi ve (17.2%) stones or internal hematomas.
Univariate analysis revealed only two factors associated with a statistically
signifi cant increased risk of urinary complications: double-kidney trans-plantation, which was associated with a 2.72 times increased risk, and the presence of more than one renal artery, which was associated with a 2.48-fold increased risk. On multivariate analysis, however, only renal-artery multiplicity remained statistically signifi cant, with a 2.5-fold increased risk.
The researchers observed trends toward urinary complications with donor age of 60 years or older, re-trans-plants, and ligation of the lower pole artery, but these trends did not reach statistical signifi cance possibly because of the small sample size of subgroups with these complications.
“The results confi rm that our judg-ment regarding kidney choice—such as preservation of the inferior pole renal artery if previously transected—is resulting in excellent outcomes,” Dr. Kulkarni said. ■
John Roberts. MD
Post-Transplant Urinary Problems
Strictures were the most common urinary complication among 635 renal transplants studied at the University of Florida, Gainesville. Shown here are the proportions of each type of urinary complication.
Source: Kulkarni R, et al. Data presented at the American Society of Transplant Surgeons’ 2012 Annual State of the Art Winter Symposium.
Strictures
Leaks
Stones or internal hematomas
58.6% 24.1%
17.2%

28 Renal & Urology News MARCH 2012 www.renalandurologynews.com
CME FEATURE
BY WILLIAM F. FINN, MD
Gout, a chronic, progressive disease and the most prev-alent form of infl ammatory arthritis, causes signifi cant
morbidity and impaired quality of life.1,2 Because of its association with hyper-uricemia and crystallization of uric acid within joints, gout is considered a rheumatologic manifestation of renal disease.2,3 Hyperuricemia and gout are particularly common among those with chronic kidney disease (CKD), and per-sons with gout have a much higher inci-dence of CKD. While the prevalence of CKD in the US general population is approximately 13%,4 it approaches 40% among patients with gout.5
Etiology of gout onset
Chronic hyperuricemia is a prereq-uisite for the development of gout.1 Hyperuricemia can result from either overproduction or underexcretion of uric acid, or both, any of which may predispose the individual to gout.6 Overproduction of uric acid accounts for only 10% of gout cases. More com-monly, the causative factor is a decrease
in the kidney’s ability to secrete urate as a consequence of drugs or disease.
Both hyperuricemia (generally defi ned as a urate level >7.0 mg/dL in men and >6.0 mg/dL in women) and gout are signifi cant problems in recipients of renal and other solid organ transplants. The general incidence of hyperuricemia is between 2% and 18% with gout occur-ring in 0.1%-0.3%; in renal allograft recipients, hyperuricemia occurs in 19%-85% of patients, with the highest inci-dence in those treated with calcineurin inhibitors.7-9 Of these patients, between 3.5% and 28% are reported to have gout post-transplant.10,11 Patients without hyperuricemia prior to renal transplanta-tion appear to have the same incidence of gout as the general population.12 Based on Medicare claims data, new-onset gout may occur in as many as 13% of renal transplant recipients, with a cumulative incidence of 7.6% at 3 years post-trans-plant.13 Gout in renal recipients has been described as more aggressive than in the general population, with early onset, fast tophaceous progression, and involving unusual joints such as the hip, shoulder, and sacroiliac.14,15 Independent correla-tions with new-onset gout were found for use of cyclosporine compared with use of tacrolimus after discharge, male
Clinical Challenges and Renal Considerations in Managing GoutA case study examines the treatment of hyperuricemia and gout in a 57-year-old postmenopausal renal transplant recipient with intermittent gout attacks
William F. Finn, MD, is Professor of Medicine in the Division of
Nephrology and Hypertension at University of North Carolina
School of Medicine at Chapel Hill.
Release Date: March 2012Expiration Date: March 2013Estimated time to complete the educational activity: 1 hourThis activity is jointly sponsored by Medical Education Resources and Haymarket Medical Education and is supported by an educational grant from Savient Pharmaceuticals.STATEMENT OF NEED: Clinicians today face an increasing number of patients with gout. Nephrologists in particular must contend with complex cases in patients with varying degrees and stages of renal dysfunction in addition to other comorbidities and individual characteristics that affect treatment decisions and, ultimately, treatment success. As gout occurs in tandem with renal disorders, nephrologists must be able to appropriately identify and treat these patients.TARGET AUDIENCE: This activity has been designed to meet the educational needs of nephrologists and other clinicians involved in the treatment of patients with gout. EDUCATIONAL OBJECTIVES: After completing the activity, the participant should be better able to:
Describe how renal function affects the management of gout.• Evaluate current and emerging options for urate-lowering therapy with regard to their benefi ts • and limitations in patients with varying degrees of renal impairment.Discuss ways to motivate patient adherence to a long-term treatment plan the incorporates • lifestyle considerations and pharmacotherapy.
ACCREDITATION STATEMENT: This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Medical Education Resources (MER) and Haymarket Medical Education. MER is accredited by the ACCME to provide continuing medical education for physicians.CREDIT DESIGNATION: Medical Education Resources designates this enduring material for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.DISCLOSURE OF CONFLICTS OF INTEREST: Medical Education Resources ensures balance, independence, objectivity, and scientifi c rigor in all our educational programs. In accordance with this policy, MER identifi es confl icts of interest with its instructors, content managers, and other individuals who are in a position to control the content of an activity. Confl icts are resolved by MER to ensure all scientifi c research referred to, reported, or used in a CME activity conforms to the generally accepted standards of experimental design, data collection, and analysis. MER is committed to providing its learners with high-quality CME activities that promote improvements or quality in health care and not a commercial interest.
The faculty reported the following fi nancial relationships with commercial interests whose products or services may be mentioned in this CME activity:
Name of Faculty Reported Financial Relationship• William F. Finn, MD
• Anthony J. Bleyer, MD(Faculty Chair)
Consultant: Takeda Pharmaceuticals Speakers’ Bureau: Takeda Pharmaceuticals Consultant: Takeda Pharmaceuticals, Savient Pharmaceuticals
The content managers, Marjorie Hale, Jill Rovitzky Black, Susan Basilico, Jody A. Charnow, and Marina Galanakis of Haymarket Medical Education, and Victoria Smith, MD, of Medical Education Resources, have disclosed that they have no relevant fi nancial relationships or confl icts of interest.METHOD OF PARTICIPATION: There are no fees for participating in and receiving CME credit for this activity. During the period March 2012 through March 2013, participants must: 1) read the learning objectives and faculty disclosures, 2) study the educational activity, 3) complete the posttest and submit it online. Physicians may register at www.myCME.com/marchgout (March 2012), and 4) complete the evaluation form online.A statement of credit will be issued only upon receipt of a completed activity evaluation form and a completed post-test with a score of 70% or better.

www.renalandurologynews.com MARCH 2012 Renal & Urology News 29
sex, age >34.3 years, higher body mass index (BMI) (>28.6 kg/m2), and more recent year of transplant (after 1996).13 Furthermore, new-onset gout was inde-pendently associated with decreased patient survival, with a 1-year mortality rate of 14.3%, as well as a 22% increased risk for graft loss.13 The improved quality of life gained through renal transplanta-tion may be offset by gout that becomes severe and debilitating.16
Pathogenesis of hyperuricemia
Uric acid is the end product of purine metabolism. The pKa of uric acid is approximately 5.3. At the physiologic pH of 7.4, the equilibrium between the undissociated acid and the salt form is signifi cantly shifted towards the salt form as monosodium urate. Because the amount of urate in the body is regu-lated by a balance between dietary purine intake, endogenous purine synthesis, and urate excretion (Figure 1), purine metabolism plays a signifi cant role in the pathogenesis of hyperuricemia leading to gout.2 Approximately 95% of uric acid produced by purine metabolism is freely fi ltered through the glomerulus.16 Urate is absorbed extensively in the proximal tubule via the organic anion transporter URAT1, then further reabsorbed by the kidney with sodium-dependent reabsorp-tion of anions, resulting in renal clear-ance of only 7% to 10% of the fi ltered load.2,16 Supersaturation of urate (which may occur at plasma levels >6.8 mg/dL) leads to the formation of monosodium urate crystals that may be deposited in joints and periarticular tissues, depending on the temperature, pH, and concen-trations of sodium and calcium within those structures.2,16
Urine pH may be as low as 4.4—a hydrogen gradient of 1000:1 compared to the 7.4 pH of plasma. At this pH, the equilibrium shifts from monosodium urate to uric acid. Uric acid nephro-lithiasis is principally due to a low uri-nary pH, leading to a predominance of uric acid in the urine, which is much less soluble than urate.
Case study: gout onset in a postmenopausal Tx patient
Mrs. G, a 57-year-old postmenopaus-al Caucasian woman, is 5’4” tall and weighs 138 lb, with a BMI of 23.7 kg/m2, and does not smoke or drink alcohol. She underwent renal transplantation
2 years ago for progressive kidney failure after an 11-year history of polycystic kidney disease. Her immu-nosuppressant regimen consists of tacrolimus 8 mg/day and azathioprine 100 mg/day. Mrs. G also takes a daily multivitamin and calcium and vitamin D supplements. She reports acute onset of redness, swelling, and pain in her right big toe that began 2 days ago. She has had similar epi-sodes intermittently over the past 3 months and is concerned that they may be becoming more frequent.
Discussion: risk factors in renal Tx patients
Mrs. G is representative of a renal trans-plant patient with gout. Transplant recipients and the general population share several risk factors for the devel-opment of hyperuricemia and gout, including increased BMI, hypertension, and insulin resistance or diabetes melli-tus, all clinical features of the metabolic syndrome.1,16 Treatment with loop or thiazide diuretics also increase the risk for hyperuricemia by inhibiting renal excretion of urate via the organic anion transporter OAT4.1,16 Renal impair-ment is associated with hyperurice-mia, particularly in postmenopausal women, and CKD is a signifi cant risk factor for gout.1,16 Interestingly, hyper-uricemia is common in patients with end-stage renal disease (ESRD), but gout is not.16
Calcineurin inhibitors: In trans-plant recipients, immunosuppressive therapy (particularly the calcineurin inhibitor [CNI] cyclosporine) is the most important risk factor for gout.6,16
Gout risk correlates with exposure to cyclosporine over time rather than the absolute dose or serum level. Due to its vasoactive properties and effect on interstitial structures, cyclosporine may decrease the renal clearance of urate by both reducing glomerular fi ltration rate (GFR) and impairing the handling of urate in the proximal tubules.6,16
Symptomatic hyperuricemia has been reported in 51% to 84% of patients treated with cyclosporine and 11% to 55% of those treated without a CNI. From 1.7% to 28% of those treated with cyclosporine developed gout com-pared with 0% to 23% of those not given a CNI.16
Medicare claims data indicated that the prevalence of new-onset gout
was signifi cantly lower in renal trans-plant patients treated with tacrolimus than those treated with cyclosporine (6.1% vs. 7.9%, P<0.05) within 3 years of transplantation.13 Some studies in small patient populations have reported a decrease in serum uric acid after switching from cyclosporine to tacrolimus16; others have found no advantage to tacrolimus over cyclosporine.17 In a 3-month trial, hyperuricemia occurred in 18.9% of patients treated with sirolimus (structurally similar to tacrolimus but with a different mechanism of action) and 54.1% of those treated with cyclosporine.16
Inhibitors of purine metabolism: Azathioprine is a prodrug, converted in the body to the active metabolites 6-mercaptopurine and 6-thioinosinic acid (Figure 2).16 Azathioprine inter-feres with nucleic acid metabolism although the exact mechanism of action is not known. Xanthine oxidase inhibi-tors potentiate azathioprine toxicity, so patients with gout must discontinue azathioprine before treatment with a xanthine oxidase inhibitor.
Mycophenolate mofetil is a prodrug converted to mycophenolic acid, a potent and reversible uncompetitive inhibitor of inosine monophosphate dehydrogenase. Unlike azathioprine, its metabolism is
Table 1. Considerations in Selecting Uric Acid-Lowering Therapy
Class and Agent Consideration
Drugs Used to Treat or Prevent Gout Flares
NSAIDs • Use with caution or may be contraindicated in patients with severe heart failure, ulcer disease, GI bleeding, aspirin- or NSAID-induced asthma, renal impairment
• May worsen renal function temporarily or permanently• Drug interaction with warfarin
Colchicine • Contraindicated in patients on dialysis• Dose adjustment needed for renal impairment• Can cause serious GI adverse effects• Drug interactions with cyclosporine, statins, macrolides
Corticosteroids • Use with caution in patients with diabetes or infection• Dose should be tapered to avoid rebound fl are
Drugs Used for Ongoing Management of Hyperuricemia
Xanthine oxidase inhibitors Allopurinol • Effective in patients who underexcrete or overproduce
uric acid• Dose adjustment needed for impaired renal function• Should not be used with azathioprine, 6-mercaptopurine • Target serum uric acid levels not achieved in some
patients without high doses• Rare but potentially fatal hypersensitivity syndrome
Febuxostat • Option for allopurinol hypersensitivity or intolerance• Effective in patients with or without renal insuffi ciency• Contraindicated for use with azathioprine,
6-mercaptopurine, and theophylline
Uricosuric Probenecid • Loses effectiveness as renal function declines
• May not be effective in patients treated with cyclosporine
• Risk for nephrolithiasis in patients with high uric acid production
• Adequate fl uid intake necessary• Twice-daily dosing required
Urate transporter Pegloticase • Administered by IV infusion every 2 weeks
• Relatively rapid dissolution of tophi• Infusion reactions and allergic reactions reported• Gout fl ares common in early months of treatment• May exacerbate CHF
NSAIDs = nonsteroidal anti-infl ammatory drugs; GI = gastrointestinal; IV = intravenous; CHF = congestive heart failureSources: Dubchak N, Flasca GF. 2010; Reindeers MK, Jansen TL. New advances in the treatment of gout: review of pegloticase. Ther Clin Risk Manag 2010;6:543-550.; Schumacher HR Jr, Chen LX. The practical management of gout. Cleve Clin J Med 2008;75 Suppl 5:S22-S25.; Terkeltaub R. 2009.

30 Renal & Urology News MARCH 2012 www.renalandurologynews.com
CME FEATURE
not affected by allopurinol, a signifi cant advantage in patients with gout.18
Among transplant recipients and the general population alike, gout is more common in men; in women, it occurs predominantly after menopause.16,19
Premenopausal gout is unusual. The fi rst metatarsophalangeal joint is most often involved, although wrists, knees, and elbows may be affected.6,16
Case: initial patient workup
Examination reveals erythema, swell-ing, warmth, and tenderness of the right first metatarsophalangeal joint with no evidence of tophi. Laboratory studies revealed a serum creatinine of 1.8 mg/dL, BUN of 25 mg/dL, albumin 4.0 g/dL, and an estimated GFR of 32 mL/min. The serum uric acid level of 7.2 mg/dL indicates hyperuricemia, and analysis of synovial fl uid aspiration con-fi rms the presence of monosodium urate crystals.6,19 The clinician explains that Mrs. G is experiencing acute symptoms of gout because the level of uric acid in her blood is elevated and crystals have formed in the joint, causing local dam-age leading to infl ammation, redness, and pain. The clinician recommends an increase in the prednisone dosage to help treat the acute fl are of gout. He gives Mrs. G information on uric acid-lowering drugs that they can discuss at her follow-up visit and recommends substituting mycophenolate mofetil for azathioprine.
They also review dietary changes that may limit the hyperuricemia.
Discussion: identifying urate levels
A serum uric acid level >6 mg/dL in both men and women favors crystalliza-tion of monosodium urate; the higher the urate level, the greater the risk of an acute attack. The presence of mono-sodium urate crystals in synovial fl uid is required for a defi nitive diagnosis of gout.6,16 Monosodium urate crystals damage bone and periarticular tissue through local mechanical pressure and acute or chronic infl ammation.6,16 Acute attacks of gout result from an infl am-matory response, in which monocytes and synoviocytes initially release proin-flammatory cytokines in response to the monosodium urate crystals.16,20 The subsequent accumulation of neutrophils within the synovial fl uid and membrane induces the release of several infl amma-tory mediators, of which interleukin-1β plays a central role.20 While acute attacks of gout may be self-limiting and respond rapidly to short-term anti-infl ammatory therapy, the chronic presence of monoso-dium urate crystals in joints can damage cartilage, bone, and soft tissues.16 Just as not all patients with hyperuricemia develop gout, not all patients with gout develop tophi.16
Patient education plays an impor-tant role in preventing the develop-ment of gout, particularly regarding
dietary precautions for renal transplant recipients.21 Increased serum uric acid levels are associated with red meat, fructose-sweetened beverages, and alcohol; dairy products, coffee, and vitamin C seem to decrease uric acid levels.22 Alcohol should be avoided or consumed only occasionally.16,21 (Go to www.renalandurologynews.com/gout1 for a more extensive list of dietary precautions.) Unfortunately, even if suc-cessful, dietary precautions may result in a decline in serum urate concentra-tions of only 1 mg/dL.
Case: pharmacotherapy regimen
Mrs. G expresses concern over her hyperuricemia persisting and triggering more attacks of gout, but she is reluctant to add another drug to her regimen. She asks if she can use pain medications as needed. The clinician and Mrs. G dis-cuss the benefi ts and risk of analgesics known to be effective for acute attacks of gout. The clinician emphasized that these agents do not treat the underlying chronic condition.
Discussion: managing infl ammation
The medical management of acute gout attacks in renal transplant recipients is similar to that for most patients, with anti-infl ammatory therapy initiated at the time of diagnosis (Table 1).6 Colchicine, a plant-derived product with a rapid onset
of action (usually within 48 hours), is effective in most patients.6,16,22 However, colchicine is associated with diarrhea, abdominal cramping, or nausea that may be related to its extensive enterohepatic recirculation.6,16 In some patients, the gastrointestinal (GI) symptoms precede pain relief.16 For the treatment of gout flares, the recommended doses have recently undergone revision (Table 1). Colchicine treatment in renal transplant patients is associated with myotoxicity, manifesting as weakness and reduced deep tendon refl exes, sometimes accom-panied by an elevated creatine kinase level; diagnosis is confi rmed by muscle biopsy.6,16 Although reversible, myotoxic-ity may be signifi cantly disabling.6 Patients receiving cyclosporine may be predis-posed to colchicine myotoxicity, and dose reduction is necessary in patients with advanced CKD.1
Nonsteroidal anti-infl ammatory drugs (NSAIDs) are an effective alternative to colchicine but can adversely affect renal hemodynamics, particularly in patients with diminished allograft function (Table 1).6,16 COX-2 inhibitors have not been well-studied in renal trans-plant patients and generally are thought to offer no advantage over traditional NSAIDs in terms of renal adverse effects. If used, renal function should be closely monitored and the agents discontinued with an increase in the serum creati-nine concentration.16,20 Furthermore, the association of COX-2 inhibitors with an
Figure 2. Metabolism of Azathioprine and Site of Action of the Xanthine Oxidase Inhibitor Allopurinol.
Source: Adapted from Stamp L, et al 2005.
Mercaptopurine
Allopurinol
Azathioprine
6-Thiouric acid(inactive metabolite)
Xanthineoxidase
Figure 1. Overview of the Pathogenesis of Gout
Source: Adapted from Choi HK, et al. 2005
Urate level
Urate supersaturation
and crystallization
Gout
Dietary purine load
Endogenous purine synthesis
Renal excretion
Gut

www.renalandurologynews.com MARCH 2012 Renal & Urology News 31
DISCLAIMER: The content and views presented in this educational activity are those of the authors and do not necessarily refl ect those of Savient Pharmaceuticals, Medical Education Resources, or Haymarket Medical Education. The authors have disclosed if there is any discussion of published and/or investigational uses of agents that are not indicated by the FDA in their presentations. The opinions expressed in this educational activity are those of the faculty and do not neces-sarily represent the views of Savient Pharmaceuticals, Medical Education Resources, or Haymarket Medical Education. Before prescribing any medicine, primary references and full prescribing information should be consulted. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications on dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities. The information presented in this activity is not meant to serve as a guideline for patient management.
increased risk for adverse cardiovascular events signals judicious use in patients with existing risk.16
Corticosteroids are another anti-infl ammatory treatment option for acute gout attacks (Table 1).16,21 Many renal transplant recipients are on maintenance doses of corticosteroids. An increased dose may be effective for acute gout symptoms, but must be tapered after symptom resolution to avoid rebound attacks.16,21 Oral corticosteroids should be limited to short courses for acute episodes, and intra-articular formula-tions are useful when joint involvement is limited and they are accessible.16
Case: monitoring drug protocols
The clinician understands Mrs. G’s desire to limit her medications. He indicates that there is a high likelihood that gout will recur, and he asks her to call if she develops symptoms again. He provides her with extra glucocorticoid tablets to take if she has a recurrence, reiterating that she should call.
Discussion: more treatment options
Gout is the only chronic form of arthritis that can be cured.16 When serum uric acid levels are reduced over the long term, monosodium urate crystals in joints, soft tissue, and tophi dissolve, and acute attacks of gout subside.16 Uric acid-lowering therapy may be considered after the fi rst acute gout attack, since attacks will recur in most organ trans-plant recipients.16 Serum uric acid levels should be maintained below 6 mg/dL by reducing uric acid formation with the xanthine oxidase inhibitors allopurinol and febuxostat or increasing urate excre-tion with the uricosuric agent probenecid (Table 1).16,22
Xanthine Oxidase Inhibitors: Allopurinol is a purine analog that reduces uric acid production by inhib-iting xanthine oxidase and is considered fi rst-line therapy for most gout patients.20 Serum uric acid decreases markedly with-in the fi rst 24 hours after administration and a peak effect occurs at 2 weeks.19 In controlled clinical trials, allopurinol 300 mg/day lowered serum uric acid by about 33% in a population in which 25% to 30% had detectable tophi.20
Allopurinol is metabolized in the liver to its active agent, oxypurinol, which is excreted predominantly by the kidney. Because serum oxypurinol levels vary inversely with renal function, dose adjust-ments of allopurinol are recommended for patients with CKD. GI disturbance and rash are common adverse effects.22 Allopurinol hypersensitivity syndrome, although rare, has been associated with higher doses, diuretic use, renal insuf-fi ciency, and higher concentrations of oxypurinol.22 Because studies identifying this relationship may have been fl awed, it remains uncertain whether higher doses are a risk factor for this syndrome.
Mercaptopurine is the active metab-olite of the immunosuppressant azathioprine (Figure 2). Xanthine oxidase inactivates the conversion of mercaptopurine to inactive 6-thiopurine. Inhibiting xanthine oxidase increases cir-culating levels of mercaptopurine that can induce myelosuppression and other toxic effects relatively quickly.11,21 The avail-ability of mycophenolate mofetil obvi-ates the need to reduce the starting dose of allopurinol.16,21
Febuxostat, a non-purine selective xan-thine oxidase inhibitor, is an appropriate option for patients with allopurinol inef-fectiveness, hypersensitivity, or intoler-ance.20,22 Clinical trials have demonstrated improved efficacy of febuxostat over allopurinol to meet target serum uric acid concentrations in many patients, including those with CKD, and with-out an increased incidence of hyper-sensitivity reactions.20,22 Febuxostat 40 or 80 mg/day produced similar uric acid-lowering effects in patients with and without renal insufficiency.22 In
addition, chronic febuxostat therapy may result in dissolution of tophi and has a favorable impact on quality-of-life parameters with prolonged (5 years) treat-ment.20,22 Unlike allopurinol, febuxostat is metabolized primarily in the liver with little renal elimination, so there is no need for dose adjustment in patients with CKD.20 Possible side effects include elevations in hepatic enzymes and GI disturbances.22 Febuxostat may have a lower propensity for drug toxicity than allopurinol because it neither directly regulates pyrimidine metabolism nor is incorporated into nucleotides.20 However, febuxostat is contraindicated for use with azathioprine and 6-mercaptopurine because it prolongs the half-life of these purine analogs.22
Uricosuric Agents: Rather than decreas-ing uric acid formation, uricosuric agents increase uric acid excretion. Probenecid, most commonly used, interferes with renal uric acid or anion exchange to block reabsorption of uric acid in the proxi-mal tubules.22 Uricosuric agents are not advised in patients who are overproducers of uric acid and whose urinary uric acid levels are already high (ie, >800 mg/day) because of the risk of nephrolithiasis. This risk can be reduced through adequate hydration, alkalinization of the urine, and renal sonograms at regular inter-vals.6,22 Uric acid excretion should be monitored periodically in probenecid users; high fl uid intake is advised for patients with 24-hour uric acid excre-tion >750 mg.6 Probenecid becomes progressively less effective with declin-ing GFR, and it may be ineffective in patients taking cyclosporine.6, 20 There are a number of potential drug interactions with probenecid. Clinicians prescribing probenecid should make sure that patients alert them of medication changes made by other clinicians. These issues, coupled with the availability of allopurinol and febuxostat, have limited the use of this agent.22 Probenecid requires more than once-daily dosing; treatment is initiated at low doses and titrated upward gradually, with maintenance doses ranging from 500 mg/day to 3 g/day.22
Conclusions
Hyperuricemia and gout are common among renal transplant recipients and
present challenges to the manage-ment of both immunosuppression and hyperuricemia. The relatively high prevalences of hyperuricemia and gout in this patient population are attribut-able to abnormal renal urate transport mechanisms due to the use of CNIs and/or intrinsic renal tubular defects. The risks and benefits of pharmaco-logic agents used to treat acute attacks of gout and chronic hyperuricemia must be evaluated carefully for their effects on serum uric acid levels and drug-drug interactions. ■
REFERENCES
1. Roddy E, Doherty M. Epidemiology of gout. Arth Res Ther 2010;12:223.
2. Choi HK, Mount DB, Reginato AM. Pathogenesis of gout. Ann Intern Med 2005;143:499-516.
3. Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia in the US general population. Arthritis Rheum 2011;63:3136-3141.
4. Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA 2007;298:2038-2047.
5. Fuldeore MJ, Riedel AA, Zarotsky V, et al. Chronic kidney disease in gout in a managed care setting. BMC Nephrol 2011;12:36.
6. Clive DM. Renal transplant-associated hyperuricemia and gout. J Am Soc Nephrol 2000;11:974-979.
7. Bieber J, Terkeltaub R. Gout: on the brink of novel therapeutic options for an ancient disease. Arthritis Rheum 2004;50:2400-2414.
8. Delaney V, Sumrani N, Daskalakis P, et al. Hyper-uricemia and gout in renal allograft recipients. Transplant Proc 1992;24:1773-1774.
9. Lin H, Rocher L, McQuillan M, et al. Cyclosporine induced hyperuricemia and gout. N Engl J Med 1989;321:287-292.
10. Ben Hmida B, Hachicha J, Bahloul Z, et al. Cyclosporine-induced hyperuricemia and gout in renal transplants. Transplant Proc 1995;27:2722-2724.
11. Stamp L, Ha L, Searle M, et al. Gout in renal transplant recipients. Nephrology 2006;11:367-371.
12. Hernandez-Molina G, Cachafeiro-Vilar A, Villa A, et al. Gout in renal allograft recipients according to the pretransplant hyperuricemic status. Transplantation 2008;86:1543-1547.
13. Abbott KC, Kimmel PL, Dharnidharka V, et al. New-onset gout after kidney transplantation: incidence, risk factors and implications. Transplantation 2005;80:1383-1391.
14. Baethge BA, Work J, Landreneau MD, McDonald JC. Tophaceous gout in patients with renal trans-plants treated with cyclosporine A. J Rheumatol 1993;20:718-720.
15. Pascual E. Gout update: from lab to the clinic and back. Curr Opin Rheumatol 2000;12:213-218.
16. Stamp L, Searle M, O’Donnell J, Chapman P. Gout in solid organ transplantation: a challenging clinical problem. Drugs 2005;65:2593-2611.
17. Kanbay M, Akcay A, Huddam B, et al. Infl uence of cyclosporine and tacrolimus on serum uric acid levels in stable kidney transplant recipients. Transplant Proceed 2005;37:3119-3120.
18. Jacobs F, Mamzer-Bruneel MF, Skhiri H, et al. Safety of the mycophenolate mofetil-allopurinol combination in kidney transplant recipients with gout. Transplantation 1997;64:1087-1088.
19. Harris MD, Liegel LB, Alloway JA. Gout and hyperuri-cemia. Am Fam Physician 1999;59:925-934.
20. Terkeltaub R. Novel therapies for treatment of gout and hyperuricemia. Arthritis Res Ther 2009;11:236.
21. Baroletti S, Bencivenga GA, Gabardi S. Treating gout in kidney transplant recipients. Prog Transplant 2004;14:143-147.
22. Dubchak N, Flasca GF. New and improved strategies for the treatment of gout. Int J Nephrol Renovasc Dis 2010;3:145-166.
The formation of uric acid crystals (shown above) in the synovial fl uid.
© S
COTT
CAM
AZIN
E /
PHO
TO R
ESEA
RCHE
RS, I
NC.

32 Renal & Urology News MARCH 2012 www.renalandurologynews.com
CME FEATURE
CME Post-testExpiration Date: March 2013Medical Education Resources designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Participants should claim only the credit commensurate with the extent of their participation in the activity. Physician post-tests must be completed and submitted online. Physicians may register at no charge at www.myCME.com/marchgout. You must receive a score of 70% or better to receive credit.
1. Among renal transplant recipients:The progression and clinical fea-a. tures of gout are comparable to those in the general population.Tophaceous progression gener-b. ally occurs at the same rate as in the general population, but manifests in unusual joints, such as the shoulder.Gout has been observed to c. be more aggressive than in the general population.Tophi formation tends to be d. markedly slower, although acute attacks of gout recur more frequently than in the general population.
2 The most important risk factor for gout among renal transplant recipients is:
Extended duration of pre-a. transplant kidney diseaseHypertension, elevated body b. mass index, and other compo-nents of the metabolic syndromeTreatment with loop or thiazide c. diureticsUse of immunosuppressive d. agents, especially cyclosporine
3. Dietary regimens used to manage gout:
Restrict consumption of alcoholic a. beverages and foods high in vitamins A and C Require the elimination of red b. meat, alcoholic beverages, dairy products, and caffeineOffer effi cacy comparable to c. medication useMay result in only limited reduc-d. tions in serum urate concentra-tion, even if successfully followed
4. Maintenance doses of corticoster-oids used by some renal transplant recipients:
Are usually suffi cient to manage a. acute symptomsCan be increased to treat acute b. gout symptoms, and then
maintained at the higher dose to reduce risk of recurrence Can be increased to treat acute c. gout symptoms, but must be tapered thereafter to minimize risk of rebound attacks Must be tapered in response d. to acute gout attacks, with therapy resuming after symptom resolution
5. You are asked to see a kidney transplant patient with recurrent gout. His immunosuppressive regimen includes tacrolimus, azathio-prine, and prednisone. Which of the following is true?
Switching from tacrolimus to a. cyclosporine is likely to decrease gout attacks.Adding allopurinol and continuing b. present immunosuppressants is a good option to prevent future gout attacks.Adding febuxostat and continuing c. current immunosuppressants is a good option to prevent future gout attacks.Changing azathioprine to myco-d. phenolate and adding allopurinol is a good option to prevent future gout attacks.
6. When starting therapy with a xan-thine oxidase inhibitor (allopurinol or febuxostat), which of the following is NOT true?
The goal is to reduce uric acid a. levels below 6.0 mg/dL.Combined therapy with an anti-b. infl ammatory agent (colchicine, NSAID, prednisone) is necessary to reduce the likelihood of induc-ing an acute gout fl are.If an acute gout fl are occurs, the c. xanthine oxidase inhibitor should be held until the fl are is over.Over time, infl ammatory d. changes may resolve, tophaceous deposits may regress, and anti-infl ammatory agents may be stopped.
BY NAYANAH SIVALONDON—Low-risk non-muscle invasive bladder cancer (NMIBC) could be safely managed by periods of active surveillance rather than aggres-sive resection surgery and frequent cystoscopic follow up, Jeremy Crew, MD, a consultant urologist surgeon at Oxford University Hospital, experi-enced in the technique, told attendees at the Renal and Bladder Cancer 3rd
National Conference. Guidelines from the European
Association of Urology state that low-risk NMIBC should be managed by fre-quent cystoscopy, at three months and (if negative) subsequent cystoscopies at nine months and yearly for a minimum of fi ve years. When a recurrent tumor is detected, a resection under general anesthetic is indicated, allowing for his-topathologic examination and grading of the tumor.
Active surveillance is not a new con-cept, Dr. Crew said. “Urologists have been ahead of the game on this, with low-risk prostate cancers and for small renal masses.” He proposes that the strategy could be an option for patients with low-risk NMIBC.
Avoiding unnecessary surgery might be benefi cial to the patient particularly if the tumor is low risk. “There is a sug-gestion that by not resecting the tumor you are not going to disseminate blad-
der cancer cells throughout the bladder, which can then implant in the raw area that was just resected. So perhaps by applying a more conservative approach you may actually reduce the rate at which the tumor recurs.”
Cost, in terms of managing the patient and the surgeon’s time, is another advantage for active surveil-lance, Dr. Crew said.
Typically, patients with signifi cant comorbidities, where general anesthet-ic and resection could be a risk, may be managed using more conservative options, such as active surveillance, but Dr. Crew thinks this option could be extended to patients with low-risk NMIBC tumors who are otherwise fi t and healthy.
There are, however, disadvantages, Dr. Crew said, such as lack of histologic data. Without such data, it cannot be ascertained whether a tumor seen through a cystoscope is a low-grade cancer, and this can cause patient anxiety. “Some patients are not cut out for active surveil-lance and they may be anxious about leaving the cancer untreated,” he said.
By looking at the evidence base, Dr. Crew said that progression rate and growth rate of tumors under 5 mm in diameter was zero or minimal within a one-year surveil-lance period. “I think low-risk NMIBC can be safely managed by periods of active surveillance,” he said. ■
LIVING KIDNEY donors are at no higher risk for requiring acute dialy-sis than non-donors, according to a recent study.
Investigators led by Amit X. Garg, MD, of the University of Western Ontario in London, compared 2,027 living kidney donors with 20,270 matched non-donors. After a median follow-up period of 6.6 years, only one donor received acute dialysis, which translated into 6.5 events per 100,000 person-years, according to an online report in Nephrology Dialysis Transplantation. This rate was no dif-ferent statistically from the non-donor group, in which 14 subjects required acute dialysis, for a rate of 9.4 events per 100,000 person-years.
“The overall incidence of acute dialy-sis is very small and will not occur in over 99.99% of donors in the decade following donation,” the investigators wrote. “During this time, living kidney donors are unlikely to suffer from the inciting events that may pre-dispose to acute kidney injury.”
Dr. Garg and his colleagues added that when such events occur, “it is possible that the remaining kidney adequately compensates to prevent acute kidney injury.”
The researchers said they focused on severe acute kidney injury treated with acute dialysis “as this outcome is well ascertained in our data sources and is the most worrisome event.” ■
Living Kidney Donors Not at Higher Acute Dialysis Risk
Active Surveillance for Bladder Cancer

34 Renal & Urology News MARCH 2012 www.renalandurologynews.com
P icking the right investments for your retirement savings is no easy task. There are more than
10,000 mutual funds and countless stocks and bonds on the market. But to simplify your search, consider a target-date fund. These mutual funds are designed to serve people who will retire in a particular year such as 2020 or 2040. Holding broad collections of stocks and bonds, the funds offer one-stop shopping. By buying a single fund, you can own a diverse portfolio that should deliver competitive results and avoid the worst losses in downturns.
Because the funds are convenient solutions, they have become favor-ite investments for 401(k) and other retirement plans. Many employers have selected target funds as default options. Unless employees opt for other choices, plan contributions are automatically invested in target funds. Even during the financial crisis, investors contin-ued pouring into the funds. Now the target funds rank as one of the fastest-growing fund categories, with $345 bil-lion in assets.
A typical target fund achieves diver-sifi cation by investing in a collection of other funds. T. Rowe Price Retirement 2040 invests in a group of 18 funds. Holdings include T. Rowe Price Growth Stock Fund, T. Rowe Price Interna-tional Stock Fund, and T. Rowe Price New Income Fund, a bond portfolio. About 40 companies offer target funds. Top choices include Invesco Balanced-Risk 2020, Fidelity Freedom 2020, and T. Rowe Price Retirement 2020.
Shifting from stocks to bondsFunds that are designed for people who will retire in 2040 or 2050 start with big allocations to stocks. As the retirement date approaches, the port-folios gradually sell stocks and shift to bonds. Fidelity Freedom 2050 starts with 90% of assets in stocks. By the time the saver retires 40 years later, the fund will only have 49% in stocks. The
shift is made automatically according to a predetermined plan. Savers need not make any decisions.
The funds aim to become more con-servative as the saver ages. While stocks tend to deliver bigger returns over the long term, they are riskier than bonds. The target funds seek to focus on bonds during the stage when aging retirees will need reliable income and can’t afford to suffer big losses.
Aggressive fundsThough all the funds become more conservative over time, they follow dif-ferent strategies. Some funds are aggres-sive and hold relatively large stock positions, while other funds are more cautious and have large bond stakes. At the aggressive end of the spectrum is Goldman Sachs 2040, which has 85% of assets in stocks. A more cautious choice is Fidelity Freedom 2040, which has 71% of assets in stocks.
Which fund should you take? That depends on your tolerance for volatility. Either aggressive or cautious funds can work. But before you buy any fund, make sure you pick one that suits your temperament.
In bull markets, the aggressive funds should record the best gains. In the dif-fi cult markets of recent years, the tamer choices have done the best. The impact
of the divergent approaches became clear during the third quarter of 2011. In a peri-od when most stocks dropped sharply, the aggressive Goldman Sachs fund lost 17.7%, while the cautious Fidelity fund only dropped 13.1%. During the past three years, the cautious Fidelity Freedom fund has returned 11.2% annually, while the Goldman Sachs choice lagged with a return of 9.4%.
When you shop for a fund, pay partic-ular attention to the portfolio allocation after the retirement date. Some funds
reach their fi nal allocation on the retire-ment date. After that the allocation stays fi xed—no matter how many years an investor holds the account. Other funds continue lowering their stock allocations after the retirement date.
Among funds that are aggressive after the retirement date is American Century LIVESTRONG 2050. The fund starts with 85% of assets in stocks and gradu-ally lowers the figure to 45% on the retirement date. After that the allocation
stays put. Wells Fargo Advantage DJ Target 2050 takes a different approach. The fund starts with 85% of assets in stocks. By the retirement date, there are only 23% of assets in stocks. Then the allocation keeps shifting, so that fi ve years after retirement only 15% of assets are in stocks. For wary investors who worry about losing their nest eggs after retire-ment, a cautious choice like the Wells Fargo fund may be a sensible solution.
Conservative approachesFaced with volatile markets, some funds have been tinkering with their allocations, shifting to more conservative approaches. But T. Rowe Price has not changed its allocation during the rough times. The company’s 2055 fund has about 90% of assets in stocks. At retirement, the allocation reaches 55%. Then the fi gure keeps falling, reaching 40% 10 years after retirement. T. Rowe Price argues that clients should prepare for retirements that can last 30 years. Retirees should own stocks that can deliver long-term capital gains.
While all the target funds own stocks and bonds, some portfolios hold espe-cially broad mixes that include special-
ized assets. Goldman Sachs 2020 holds emerging market bonds. Those yield more than U.S. securities and can help to diversify portfolios. The managers of Fidelity Freedom 2020 argue that retirees should prepare for infl ation, which can erode the purchasing power of people living on fi xed income. For protection the Fidelity fund owns com-modities. Those can rise along with infl ation. Fidelity also holds infl ation-protected bonds. ■
Your MoneyTarget-date funds offer one-stop shopping for investment vehicles and enable investors to own a diverse portfolio BY STAN LUXENBERG
Some funds are aggressive and hold relatively large stock positions, while other funds are more cautious and have large bond stakes.
Many employers have selected target funds as default options.
© IS
TOCK
PHO
TO.C
OM
/ T
RAVE
LLIN
GLI
GHT