Embed Size (px)
Citation preview

10/30/2019
1
RENAL PHARMACOLOGY
September 27, 2019
What the Urology Provider Should Know
LEARNING OBJECTIVE
• Review common urologic diagnosis that are at risk for renal disease.
• Review how we assess for renal disease and the methods and calculations available to determine or estimate GFR
• Review resources from National Kidney Foundation
• Review common pharmaceuticals prescribed by Urology that need to be adjusted in renal disease.
2
OVERVIEW: WHY DO WE DOSE DIFFERENTLY?
• In general patients with renal disease are more medically complex and fragile
• Goal of renal dosing is to achieve equivalent exposure of pharmaceuticals to patients and minimize toxicity without compromising efficacy.
• Renal disease alters the effects of many drugs• Can DECREASE effects of drug• More often – INCREASE the effects and potential for
toxicity
3
UROLOGY DIAGNOSIS WITH INCREASED RISK FOR RENAL DISEASE
• Neurogenic bladder/Spina Bifida• Posterior urethral valves/Lower urinary tract obstruction • Recurrent febrile UTI• High grade bilateral VUR• Solitary kidney• Recurrent kidney stones• Renal transplant
4

10/30/2019
2
ASSESSING FOR RENAL DISEASE
• Goal: Accurate, Safe, Simple and Cost-Effective Measurement.
5
• Not possible• Occurs in Millions of
glomeruli
Direct Measurement
• Estimates renal function• Record the clearance of a
marker/exogenous substance
Indirect Measurement
INDIRECT MEASUREMENT
• GFR describes the flow rate 0f filtered fluid through the kidney• Estimates the number of functioning nephrons. • The volume of plasma cleared from a specific substance per time is
expressed in ml/min• It is indexed for body surface area (BSA) and expressed in
ml/Min/1.73m2
• Many tools to measure estimated GFR (eGFR)
These estimates are used to diagnose renal disease and also to estimate renal drug
clearance. 6
CALCULATING GLOMERULAR FILTRATION RATE• Inulin
• Considered the Gold Standard for eGFR• Uncharged fructose polymer from the Jerusalem
artichoke• Rate inulin is cleared from blood plasma = GFR• Requires continuous IV infusion with blood and urine
sampling at specific time intervals.
PROBLEM: Invasive, cumbersome, smaller children require
catheterization for accurate timed urine collections.
7 Guido et al (2014)
OTHER WAYS TO CALCULATE EGFR
• Nuclear Medicine GFR Scans• Cr-EDTA• DTPA• I-iothalamate• Iohexol
• MRI - Urogram
PROBLEM: Invasive, costly, exposure to radiation – not always feasible
8Kim, Y., Ha, S., So, Y. et al. Eur Radiol (2014) 24: 413. https://doi.org/10.1007/s00330-013-3039-z

10/30/2019
3
IF ONLY THERE WAS ANOTHER WAY…
9
SERUM MARKERS FOR EGFR
Creatinine Cystatin C
10
CREATININE
• Most widely used endogenous marker of GFR
• Metabolic product of creatineand phosphocreatine found in muscle
• Some variation, but little from normal day to day
• Low cost to measure
11
CREATININE - LIMITATIONS
• Age Variation:• At birth serum creatinine
reflects maternal levels• Drops by 50% in 1st 7-10 days of
life• Continues to drop until 4-6
weeks of age
• GFR rises from 40 ml/min/1.73m2 at 1 week of life to adult levels at 2-3 years of age
12
https://www.nytimes.com/2018/04/11/magazine/black-mothers-babies-death-maternal-mortality.html

10/30/2019
4
CREATININE - LIMITATIONS
• Varies with muscle mass• Increase in muscle mass leads to
normal increase in creatinine• Creatinine can be misleading in
individuals with low muscle mass:
13
www.halloweencostomes.com
Spina Bifida
Neuromuscular Disease
Anorexia nervosa
Liver Cirrhosis
Non-ambulatory
CYSTATIN C• Small molecular weight protein• Produced at a constant rate in all nucleated cells. • Removed from the body by glomerular filtration
• The serum concentration of CysC is mainly determined by glomerular filtration = Good GFR marker
This is a better screening test for patients with low muscle mass/muscle
wasting
14
SMM1
CYSTATIN C - LIMITATIONS
• Cost – quoted 3 to 20 times more expensive than Creatinine.
• Evidence that Cystatin C is influenced by corticosteroid use (Bokenkamp et. Al, 1999)
15 16
Serum Creatinine & Cystatin C
eGFR& CrCl
IF
THEN
Usually…
But this is not the whole
picture

Slide 14
SMM1 3-4 times more expensive to check Cystatin C at outside labSilich, Meghan M, 6/7/2019

10/30/2019
5
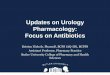
17 National Kidney Foundation
1.2 1.2 1.2
98ml/min/1.73m2 66ml/min/1.73m2 46ml/min/1.73m2
Normal or CKD1(if damage present)
Stage 2 CKD(if damage present)
Stage 3 CKD
18
https://www.kidney.org/atoz/content/gfr
GFR <30 start
discussions regarding
dialysis and renal
transplant
>/= 90
89 to 60
59-45
44-30
29-15
< 15
HOW TO CALCULATE ESTIMATED GFR
• National Kidney Foundation Website (Pediatric and Adult)
• https://www.kidney.org/professionals/KDOQI/gfr_calculatorPed
• Cell Phone App: eGFR calculator by National Kidney Foundation
(Adult, not all Pediatric)
19
GFR CALCULATOR APP
• CKD-EPI Creatinine Equation
• MDRD Study Equation
• CKD-EPI Cystatin and Creatinine 2012 Equation
• Cockcroft-Gault Formula
• Revised Bedside Schwartz Formula
20

10/30/2019
6
COCKCROFT-GAULT FORMULA
21
• Created in 1973. Only looked at 249 men and is not adjusted for BSA
• Serum creatinine• Weight• Age• Gender
A great start, but not always
accurate
MDRD STUDY EQUATION
22
• Created in 1999 & estimates for BSA• More robust study group (1628
patients with CKD)
• Serum Creatinine• Age• Gender • Race
More accurate than 24–hour
urine or CG Higher Average Muscle mass for male gender
and Black Race
CKD-EPI CREATININE
23
• Developed 2009.
• Equally accurate in <60 eGFR from MDRD and more accurate in subgroup eGFR>60 then MDRD
• Serum Creatinine
• Accounts for age, gender, and race
More accurate if eGFR >60
CKD-EPI CYSTATIN AND CREATININE EQUATION
24
• The newest Adult based equation – Created in 2012
• Combines measurements of Serum Creatinine & Cystatin C
• Accounts for age, gender and race
More data= more accurate
eGFR

10/30/2019
7
PEDIATRICS -- REVISED BEDSIDE SCHWARTZ FORMULA
• This is the Most common calculation in Pediatrics
• Accounts for serum Creatinine and Height.
• Can use “arm span” for children as a estimate of height if unable to obtain height standing
25
PEDIATRICS• Creatinine-based “Bedside Schwartz”
equation (2009) • Just creatinine. Most commonly used.
• Cystatin C-based equation (2012) • Just Cystatin C
• Creatinine-Cystatin C-based CKiDequation (2012)
• Both Cr and CysC
26
https://www.kidney.org/professionals/KDOQI/gfr_calculatorPed
These can easily be obtained via National Kidney Foundation website
Bing search
27
Link to National Kidney Foundation Pediatric GFR
NKF: Calculates the Bedside Schwartz, Cystatin C, and the CKiD equation for eGFR
PROBLEM WITH EGFR/CREATININE CLEARANCE
• Estimates of GFR for renal function are a useful guide, but not precise
• More important to be precise as the renal dysfunction worsens or when accurate values are needed (transplant, narrow therapeutic index, dosage adjustments)
• Use multiple eGFR calculations • Consider a 24 hour urine collection
for CrCl• Lean on recommendations of
Nephrology & Pharmacology colleagues
28
Art versus Science

10/30/2019
8
29
Samantha is a 13 year old female with a history of sacral agenesis with resultant neurogenic bladder and recurrent UTI. S/p APV creation and bilateral ureteral reimplants. She is on a CIC regimen of every 3-4 hours
via APV and overnight drainage. She is on Ditropan TID. Most recent labs 7/2019 showed Creatinine 0.65, CysC 1.0 and BUN 14. Her height
at this visit was 148cm.
BRAIN BREAK
30
Photo cred:
Thomas Kolon
GENERAL RENAL DOSING INFO
• If there is an adjustment it is listed in the formulary as “renal dosing”
• The dosing will often tell you at which Creatinine Clearance (CrCl) an adjustment is needed.
• Estimated GFR = good estimate of CrCl
• Dosing will either extend the time interval between doses (ex: Q8 goes to Q12) or it will decrease the actual dosage (ex: 100mg to 75mg)
Goal – Patient receive the safe, therapeutic dose without causing toxicity
31
THERAPEUTIC INDEX• Safe window that shows the ratio
between where the drug is toxic and effective.
• Narrow – Small change in drug concentration can cause toxicity or loss of efficacy
• Renally cleared: Aminoglycosides (Amikacin, Gentamicin), Vancomycin, Digoxin, Lithium.
• Check drug levels for therapeutic monitoring (these can take days to come back)
• Wide – Even large changes in drug concentration may only cause a modest impact or response.
32

10/30/2019
9
MEDICATIONS TO BE COVERED
• Urinary Incontinence – Anticholinergics, B3 Agonists, Serotonin Norepinephrine Reuptake Inhibitors
• Alpha 1 Antagonists• Testosterone • Antibiotics• Probiotics & Supplements• Pain Management – NSAIDS, Narcotics
33
ANTICHOLINERGICS
• Dosage Adjustments:• Tolterodine (Detrol): • Fesoterodine (Toviaz): All Begin at CrCl 30• Solifenacin (Vesicare):
• No Dosage Adjustments:• Oxybutynin (Ditropan)• Trospium (Sanctura)• Darifenacin (Enablex)
34
SMM1
B3 AGONIST
• Mirabegron (Myrbetriq): • CrCl 15-30 ml/min- Max 25 mg daily• CrCl <15ml/min- Not recommended
35
• Duloxetine (Cymbalta): • CrCl <30ml/min: not recommended
• Venlafaxine (Effexor): • CrCl <70: reduce dose
SEROTONIN NOREPINEPHRINE REUPTAKE INHIBITORS (DULOXETINE, VENLAFAXINE)
ALPHA 1 ANTAGONISTS
• Dosage Adjustments: Siladosin (Rapaflo):
Begin at CrCl 50Alfuzosin (Uroxatral):
Begin at CrCl <30Tamsulosin (Flomax):
Begin at CrCl <10
• No Dosage Adjustments:• Doxazosin (Cardura)• Terazosin (Hytrin)
36

Slide 34
SMM1 Silich, Meghan M, 9/12/2019

10/30/2019
10
TESTOSTERONE
• Testosterone cypionate:Contraindicated in serious renal impairment. Talk to a pediatric pharmacologist/nephrologist if considering
37
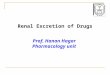
70
60
50
30
20
0 20 40 60 80
CEFAZOLIN, IMIPENEM …
CEFIXIME, CEFEPIME, …
CEFTAZIDIME, …
CEFDINIR, UNASYN, …
CEFOTAXIME
Antibiotics – When Dose Adjustment Begin
ClCr/eGFR
38
PROBIOTICS AND SUPPLEMENTS• Concern for use in immunosuppressed,
renal transplant & chronically ill patients. • Widespread use of antibiotics (prophylactic and
therapeutic dosing) affects the patient microbiota.• Introducing a new bacteria can cause rapid and
unsuspected growth
• Organ Transplant- Probiotics create a risk of translocation of bacteria (bacteria can transverse gut and invade lymph, liver, spleen, kidney, blood stream).
• Not well regulated/controlled. • If using consider USP/Gold Label certifications
39
PAIN MANAGEMENT: NSAIDS• NSAID use can compromise existing renal
function• If patient already has impaired renal function
they are at greater risk of renal toxicity.
• Reduces renal blood flow and can cause renal decompensation (usually reversible).
• Long-term NSAID use may result in renal papillary necrosis and other renal injury.
• If CrCl is <30ml/minute avoid use entirely
40

10/30/2019
11
PAIN MANAGEMENT: NARCOTICS
• Use with caution in patients with renal impairment; oxycodone clearance may decrease. Half life of narcotics in increased in the presence of renal dysfunction.
• Morphine, Codeine - Avoid in renal failure/dialysis
• Tramadol, Hydromorphone, Oxycodone –use with caution/close monitoring.
41
IN SUMMARY
• Drug doses should usually be reduced in proportion to the estimated reduction in clearance of the active drug moiety.
• Patient factors to consider in adjusting drug doses include the degree of renal impairment and patient size.
• Do the best you can with estimating GFR. When in doubt obtain updated Creatinine and Cystatin C or consider dosing with a medication that does not have renal side effects, or narrow therapeutic index if possible.
• Stop and think before prescribing anything (even OTC) and check formulary recommendations for specific renal adjustments and check with nephrology and pharmacology.
42
REFERENCES• Bokenkamp, Domanetzki, Zinck, Schumann, Byrd, Brodehl. Cystatin C serum concentrations
underestimate glomerular filtrationrate in renal transplant patients. Clinical Chemistry, 1999; 45:1866-1868.
• Doogue, M. P., & Polasek, T. M. (2011). Drug dosing in renal disease. The Clinical biochemist. Reviews, 32(2), 69–73.
• Fox JA, Dudley AG, Bates C, Cannon GM Jr. Cystatin C as a marker of early renal insufficiency in children with congenital neuropathic bladder. J Urol. 2014 May;191(5 Suppl):1602-7. doi: 10.1016/j.juro.2013.09.093. Epub 2014 Mar 26. PubMed PMID: 24679869.
• Novak TE, Mathews R, Martz K, Neu A. Progression of chronic kidney disease in children with vesicoureteral reflux: the North American Pediatric Renal Trials Collaborative Studies Database. J Urol. 2009 Oct;182(4 Suppl):1678-81. doi: 10.1016/j.juro.2009.02.085. Epub 2009 Aug 18. PubMed PMID: 19692051.
• Odeh R, Noone D, Bowlin PR, Braga LH, Lorenzo AJ. Predicting Risk of Chronic Kidney Disease in Infants and Young Children at Diagnosis of Posterior Urethral Valves: Initial Ultrasound Kidney Characteristics and Validation of Parenchymal Area as Forecasters of Renal Reserve. J Urol. 2016 Sep;196(3):862-8. doi: 10.1016/j.juro.2016.03.137. Epub 2016 Mar 25. PubMed PMID: 27017936.
• Routh JC, Cheng EY, Austin JC, Baum MA, Gargollo PC, Grady RW, Herron AR, Kim SS, King SJ, Koh CJ, Paramsothy P, Raman L, Schechter MS, Smith KA, Tanaka ST, Thibadeau JK, Walker WO, Wallis MC, Wiener JS, Joseph DB. Design and Methodological Considerations of the Centers for Disease Control and Prevention Urologic and Renal Protocol for the Newborn and Young Child with Spina Bifida. J Urol. 2016 Dec;196(6):1728-1734. doi: 10.1016/j.juro.2016.07.081. Epub 2016 Jul 27. PubMed PMID: 27475969; PubMed Central PMCID: PMC5201100.
43
REFERENCES
• Crass, R., Rodvold, K., Mueller, B., & Pai, M. (n.d.). Renal Dosing of Antibiotics: Are We Jumping the Gun? Clinical Infectious Diseases. https://doi.org/10.1093/cid/ciy790
• Greene, TomAU, Levey, Andrew S.TI - Assessing Kidney Function — Measured and Estimated Glomerular Filtration RatePT - Journal ArticleDP - 2006TA - New England Journal of MedicinePG - 2473-2483VI - 354IP - 23AID - 10.1056/NEJMra054415 [doi]PMID -167604474100 - https://www.nejm.org/doi/full/10.1056/NEJMra054415SO - New England Journal of Medicine June 8, 2006 354(23):2473
• Filler, Guido, et al. "Methods of assessing renal function." Pediatric Nephrology, vol. 29, no. 2, 2014, p. 183+. Academic OneFile, http://link.galegroup.com.proxy.library.upenn.edu/apps/doc/A357966847/AONE?u=upenn_main&sid=AONE&xid=f447620a. Accessed 18 June 2019.
• Khanal, A., Peterson, G., Jose, M., & Castelino, R. (2017). Comparison of equations for dosing of medications in renal impairment. Nephrology, 22(6), 470–477. https://doi.org/10.1111/nep.12834
• Kim, Y., Ha, S., So, Y. et al. Eur Radiol (2014) 24: 413. https://doi.org/10.1007/s00330-013-3039-z
44

10/30/2019
12
45