Embed Size (px)
Citation preview

Renin-Angiotensin System
• Aldosterone is produced in the adrenal cortex in response to low sodium levels
• Stimulates sodium reabsorption by distal convoluted tubules and collecting ducts
• When aldosterone is ↓ then less sodium is absorbed – the converse is true
• Aldosterone is a steroid that acts slowly to mediate changes in gene and protein expression – most
importantly, of Na/K-ATPase pumps and leak channels in the cortical collecting ducts.
• Also prevents loss of sodium via the same mechanism is salivary and sweat glands.
So what controls the release of aldosterone and therefore sodium absorption ?
Renin-Angiotensin System
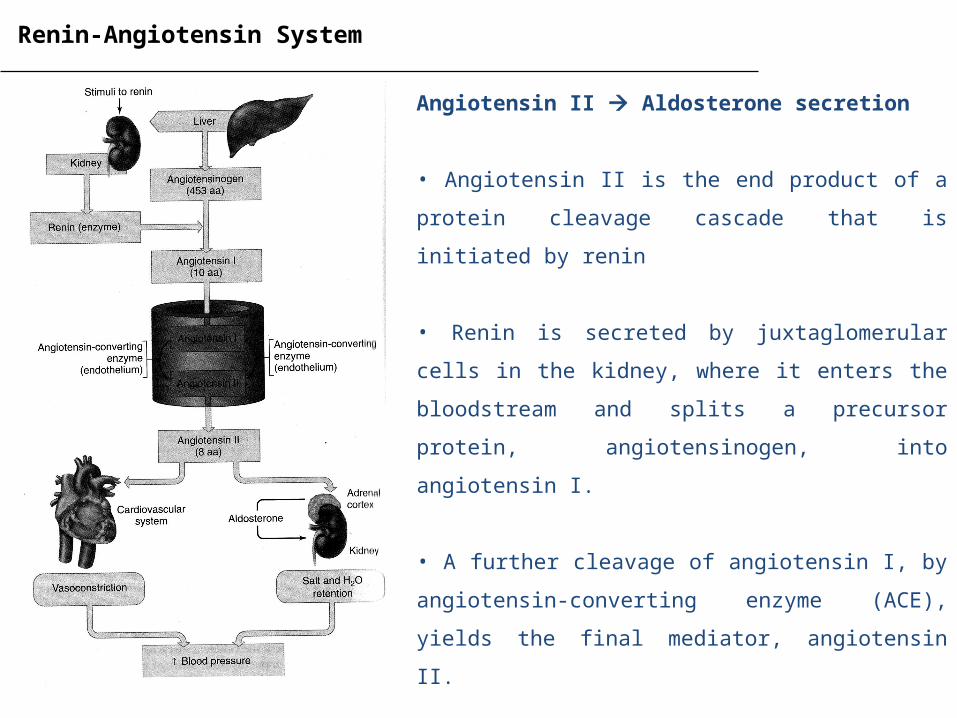
Angiotensin II Aldosterone secretion
• Angiotensin II is the end product of a protein cleavage
cascade that is initiated by renin
• Renin is secreted by juxtaglomerular cells in the kidney,
where it enters the bloodstream and splits a precursor
protein, angiotensinogen, into angiotensin I.
• A further cleavage of angiotensin I, by angiotensin-
converting enzyme (ACE), yields the final mediator,
angiotensin II.
• Angiotensin II is high during salt depletion and low when
salt intake is high, so it is the regulator of aldosterone
Renin-Angiotensin System
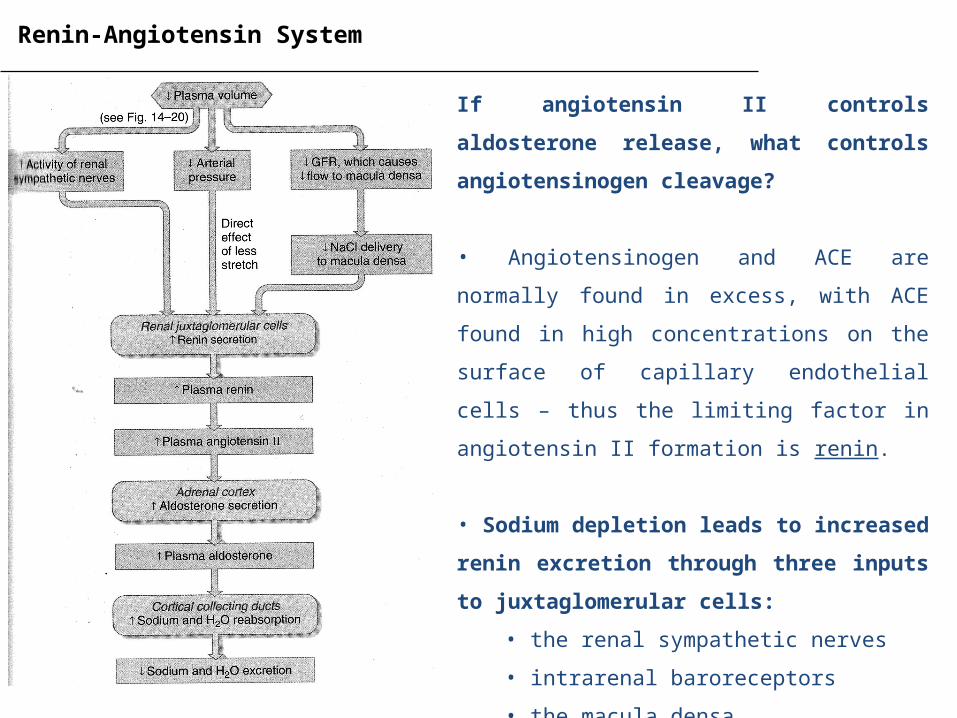
If angiotensin II controls aldosterone release, what
controls angiotensinogen cleavage?
• Angiotensinogen and ACE are normally found in
excess, with ACE found in high concentrations on the
surface of capillary endothelial cells – thus the limiting
factor in angiotensin II formation is renin.
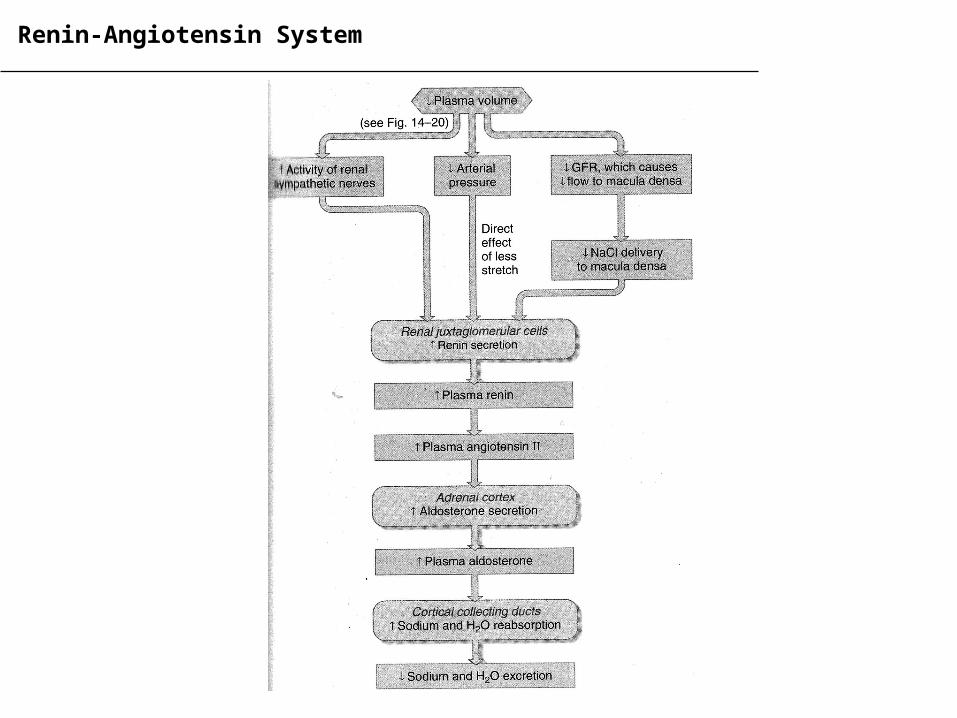
• Sodium depletion leads to increased renin excretion
through three inputs to juxtaglomerular cells:
• the renal sympathetic nerves
• intrarenal baroreceptors
• the macula densa
Renin-Angiotensin System
Renal sympathetic nerves:
• activated when low sodium leads to low plasma volume and therefore low blood pressure
• innervate the juxtaglomerular cells and stimulate renin secretion
Renin-Angiotensin System
Renal sympathetic nerves:
• activated when low sodium leads to low plasma volume and therefore low blood pressure
• innervate the juxtaglomerular cells and stimulate renin secretion
Intrarenal baroreceptors
• Juxtaglomerular cells, as a function of being found in the walls of the afferent arterioles, are
sensitive to changes in blood pressure within the kidneys
• Less stretching of the walls, due to a decrease in pressure, leads to an increase in renin
Renin-Angiotensin System
Renal sympathetic nerves:
• activated when low sodium leads to low plasma volume and therefore low blood pressure
• innervate the juxtaglomerular cells and stimulate renin secretion
Intrarenal baroreceptors
• Juxtaglomerular cells, as a function of being found in the walls of the afferent arterioles, are
sensitive to changes in blood pressure within the kidneys
• Less stretching of the walls, due to a decrease in pressure, leads to an increase in renin
Macula densa
• Located near the loops of Henle – senses sodium conc. in tubular fluid that passes through
• Additionally, decreased sodium decreased GFR decreased tubular flow
• Both of these inputs result in the further secretion of renin
System has multiple redundancies to prevent further loss of sodium and decreasing blood pressure
Renin-Angiotensin System
Diabetic Kidney Disease (DKD)
Diabetic Kidney Disease (DKD)
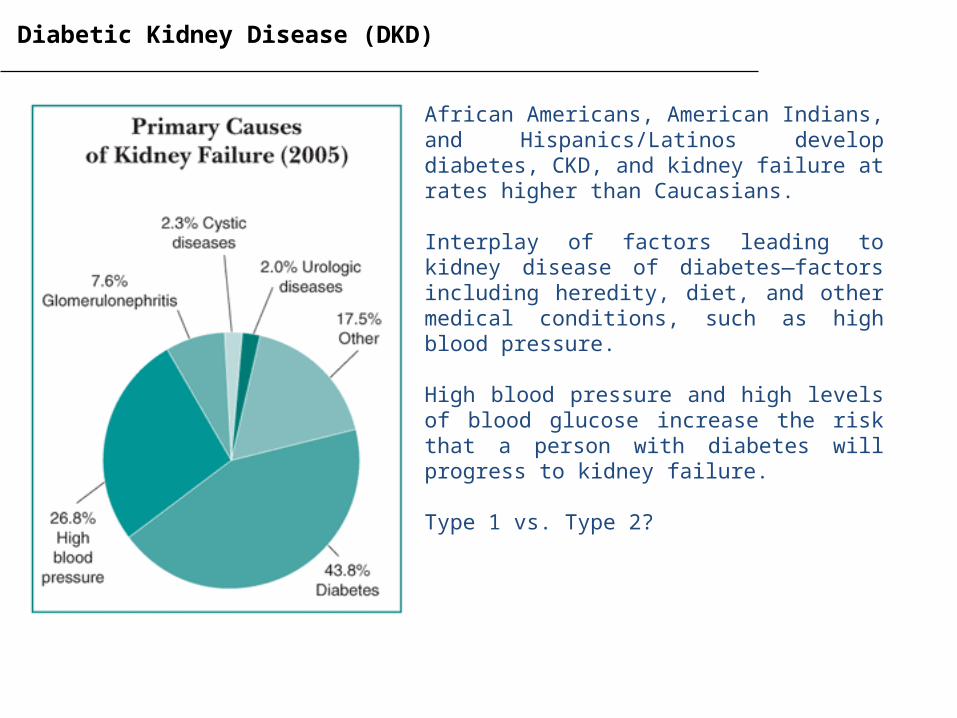
African Americans, American Indians, and Hispanics/Latinos develop diabetes, CKD, and kidney failure at rates higher than Caucasians.
Interplay of factors leading to kidney disease of diabetes—factors including heredity, diet, and other medical conditions, such as high blood pressure.
High blood pressure and high levels of blood glucose increase the risk that a person with diabetes will progress to kidney failure.
Type 1 vs. Type 2?
Diabetic Kidney Disease (DKD)
• Diabetes mellitus (DM) now accounts for more cases of end-stage renal disease (ESRD) than any
other cause of chronic kidney disease (CKD).
• In the USA, four out of every 10 new cases of ESRD arise due to diabetic kidney disease (DKD)
• Roughly 30% of individuals with type 1 and 10% of those with type 2 diabetes will develop DKD
• Glycemic control along with currently available pharmacotherapies slow, but do not stop, the
progression of DKD towards ESRD - for these patients, the only available solution is renal replacement
therapy (i.e., transplantation or dialysis).
• Given the epidemic levels of obesity and type 2 DM in the populations of many Western nations, a
comprehensive understanding of the etiology of DKD is urgently needed so that novel therapies can be
developed.
Diabetic Kidney Disease (DKD)
• Many efforts are being aimed at identifying the earliest signs of DKD so that treatments can be
instituted before irreversible renal injury occurs.
• It is now widely recognized that proteinuria, specifically microalbuminuria, is one of the earliest
clinically identifiable markers of diabetes-induced renal damage.
• The appearance of protein in the urine (predominantly the 67-kDa albumin) indicates a compromised
glomerular filtration barrier.
• A strong correlation has been identified between the likelihood of progression to ESRD and the level
of albuminuria - now considered a continuous variable in that even quantities of albumin that are in
the upper end of what is considered the “normal” range (<30 mg/day) are associated with an increased
risk for the development of later-stage chronic kidney disease.
• Individuals with DKD presenting with a high urinary protein excretion rate advance more quickly to
ESRD than do those with low proteinuria
Diabetic Kidney Disease (DKD) - Podocytopathies
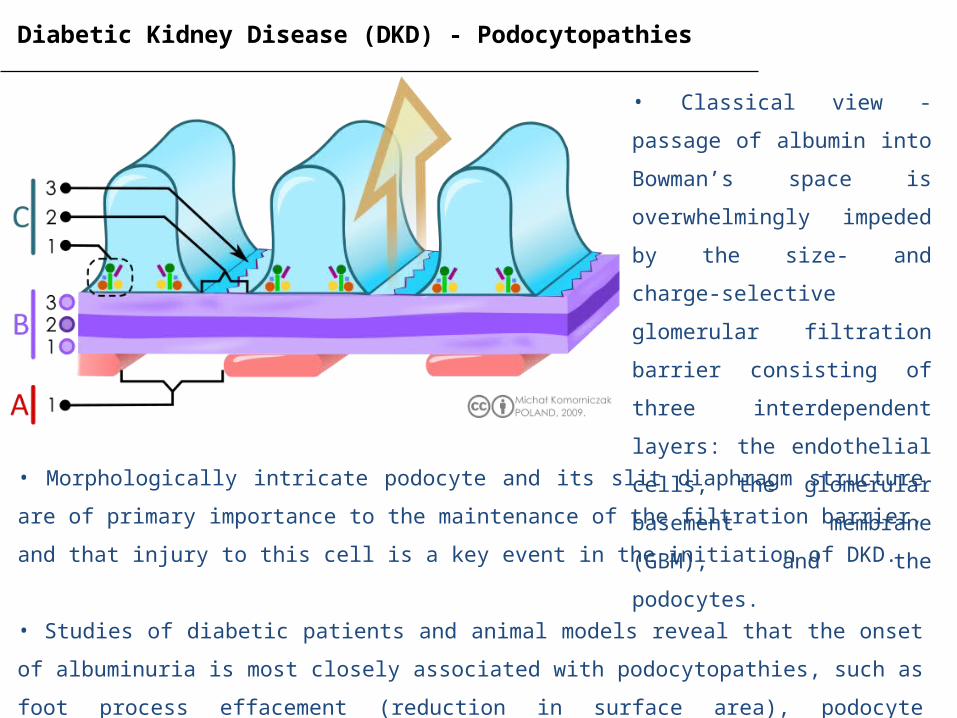
• Classical view - passage of
albumin into Bowman’s space is
overwhelmingly impeded by the
size- and charge-selective
glomerular filtration barrier
consisting of three
interdependent layers: the
endothelial cells, the glomerular
basement membrane (GBM), and
the podocytes. • Morphologically intricate podocyte and its slit diaphragm structure are of primary importance to the
maintenance of the filtration barrier, and that injury to this cell is a key event in the initiation of DKD.
• Studies of diabetic patients and animal models reveal that the onset of albuminuria is most closely
associated with podocytopathies, such as foot process effacement (reduction in surface area), podocyte
hypertrophy, detachment, apoptosis, and epithelial-to-mesenchymal transition
Diabetic Kidney Disease (DKD)
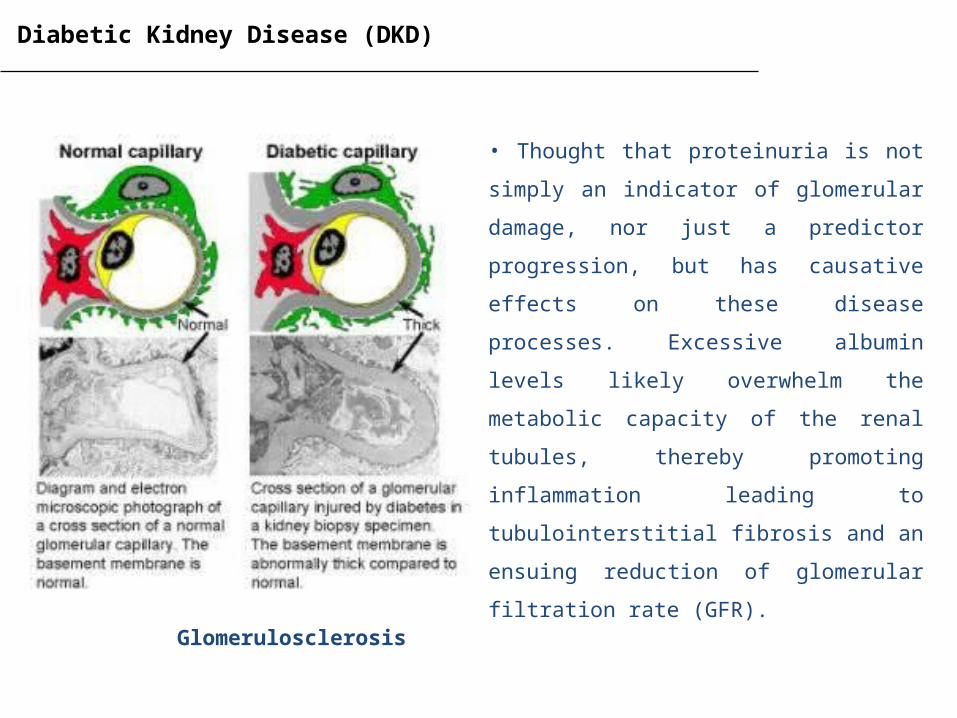
• Thought that proteinuria is not simply an
indicator of glomerular damage, nor just a
predictor progression, but has causative effects on
these disease processes. Excessive albumin levels
likely overwhelm the metabolic capacity of the
renal tubules, thereby promoting inflammation
leading to tubulointerstitial fibrosis and an
ensuing reduction of glomerular filtration rate
(GFR).
Glomerulosclerosis
Mediators of Podocytopathies in DKD
The Renin-Angiotensin System (RAS)
• RAS has been implicated in the progression of DKD - angiotensin-converting enzyme inhibitors (ACEi)
and angiotensin II receptor blockers (ARBs) slow disease progression
• ACEi and ARBs were thought to improve the clinical outcome in diabetic patients via their blood
pressure–lowering effects, acting, in part, to mitigate hyperfiltration-enhanced glomerular capillary
pressure (Pgc) - the podocyte is susceptible to the mechanical forces brought about by elevated Pgc.
• However, under conditions that reproduce a diabetic milieu (e.g., high glucose, mechanical stretch),
podocytes are driven to express several RAS components, including angiotensinogen, with angiotensin
I and II levels appeared to be enhanced by high glucose.
• Locally acting RAS that appears to induce apoptosis and TGF-β (important for fibrosis)
Mediators of Podocytopathies in DKD
Reactive Oxygen Species (ROS)
• Within the kidney, as in other organs and tissues (i.e., vasculature), hyperglycemia and RAS activation
promote oxidative stress, defined as damage to macromolecules caused by ROS (i.e., O2–, H2O2, NO,
and ONOO–)
• Studies have shown that exposure of cultured mouse podocytes to high glucose promoted ROS
generation and possible downregulation of other mediators – eNOS-deficient db/db mice display
severe glomerular lesions and albuminuria
• ROS generation in the podocyte may have other deleterious roles in addition to its proapoptotic
actions. ROS could induce actin filament polymerization, leading to cytoskeletal dysfunction and
resulting in structural changes to foot processes and slit diaphragms.
Treatment for DKD ?
C-Peptide
• Produced as a result of cleavage of pro-insulin into function insulin
• Is not just a by-product – is capable of binding to cellular receptors and altering gene expression
Bardoxolone methyl
• Antioxidant inflammation modulator
• In 21-day phase 1 trial in 60 oncology patients showed a favorable response in 49 patients (82%).
Serum creatinine levels decreased a mean of 19.3%, and estimated glomerular filtration rate (eGFR)
increased a mean of 20.9%. The effect appeared to be greater in patients with established chronic
kidney disease (CKD; 13 of 60 patients); in these patients, eGFR increased a mean of 27.6%.
Olmesartan medoxomil – angiotensin II receptor blocker