Embed Size (px)
Citation preview

ANTIPHOSPHOLIPID SYNDROME (D ERKAN, SECTION EDITOR)
Renal Involvement in Antiphospholipid Syndrome
Guillermo J. Pons-Estel & Ricard Cervera
# Springer Science+Business Media New York 2013
Abstract Renal involvement can be a serious problem forpatients with antiphospholipid syndrome (APS). However, thiscomplication has been poorly recognized and studied. It can bepresent in patients who have either primary or systemic lupuserythematosus-associated APS. Clinical and laboratory featuresof renal involvement in APS include hypertension, hematuria,acute renal failure, and progressive chronic renal insufficiencywith mild levels of proteinuria that can progress to nephrotic-range proteinuria. The main lesions are renal artery stenosis,venous renal thrombosis, and glomerular lesions (APS ne-phropathy) that may be acute (thrombotic microangiopathy)and/or chronic (arteriosclerosis, arterial fibrous intimal hyper-plasia, tubular thyroidization, arteriolar occlusions, and focalcortical atrophy). APS can also cause end-stage renal diseaseand allograft vascular thrombosis. This article reviews the rangeof renal abnormalities associated with APS, and their diagnosisand treatment options.
Keywords Antiphospholipid syndrome . Renalinvolvement . Nephropathy . Thrombotic microangiopathy .
Renal vein thrombosis . Renal artery thrombosis
Introduction
Antiphospholipid syndrome (APS) is a pro-thrombotic ac-quired autoimmune disease, characterized by vascular throm-bosis (arterial and/or venous) and pregnancy morbidity, andthe presence of antiphospholipid antibodies (aPL) [1•, 2].These antibodies are a heterogeneous family that reacts withserum phospholipid-binding plasma proteins (mainly β2
glycoprotein-I, prothrombin, protein C, protein S, annexin V,annexin II, and oxidized low-density lipoprotein), phospho-lipid–protein complexes, and anionic phospholipids [3, 4•, 5,6]. The aPL usually tested in routine laboratory practice arethe IgG and IgM anticardiolipina antibodies (aCL), detectedby use of enzyme-linked immunosorbent assay (ELISA), andthe lupus anticoagulant (LA), detected by use of clotting tests.The presence of IgG and IgM anti-β2 glycoprotein-I antibod-ies (aβ2GPI), also detected by use of ELISA, should also beassessed. A diagnosis of seronegative APS has been suggestedfor patients with clinical manifestations indicative of APS butwith persistently negative aCL, LA and aβ2GPI [7].
This pro-thrombotic syndrome can be primary or associat-ed with other conditions, particularly systemic lupus erythe-matosus (SLE), and may involve any organ and/or vessel.Renal involvement can be present in patients with eitherprimary or SLE-associated APS. Clinical and laboratory fea-tures of renal involvement in APS include hypertension, he-maturia, acute renal failure, and progressive chronic renalinsufficiency with mild levels of proteinuria that can progressto nephrotic-range proteinuria. The main lesions are renalartery stenosis, venous renal thrombosis, and glomerular le-sions (APS nephropathy) that may be acute (thrombotic mi-croangiopathy) and/or chronic (arteriosclerosis, arterial fi-brous intimal hyperplasia, tubular thyroidization, arteriolarocclusions and focal cortical atrophy) [8•]. APS can also causeend-stage renal disease (ESRD) and allograft vascular throm-bosis (Table 1) [9].
This article reviews the range of renal abnormalities asso-ciated with APS, and their diagnosis and treatment options.
Epidemiology
The true prevalence of renal involvement in APS is difficult toestablish because of its close correlation with SLE nephropa-thy. Retrospective series of patients with primary APS haveclaimed that renal involvement may fluctuate by approximate-ly 9–10 % [10, 11]. In the “Euro-phospholipid” project, itsprevalence among 1000 patients with APS was at baseline
This article is part of the Topical Collection on Antiphospholipid Syndrome
G. J. Pons-Estel :R. CerveraDepartment of Autoimmune Diseases, Hospital Clínic, Barcelona,Catalonia, Spain
G. J. Pons-Estel (*)Servei de Malalties Autoimmunes, Hospital Clínic, Villarroel 170,08036 Barcelona, Catalonia, Spaine-mail: [email protected]
Curr Rheumatol Rep (2014) 16:397DOI 10.1007/s11926-013-0397-0

approximately 3 % (glomerular thrombosis, 2 %; renal infarc-tions, 1 %; renal artery thrombosis, 0.5 %; renal vein throm-bosis, 0.2 %). However, this manifestation is clearlyunderestimated—either because renal biopsy is infrequentlyperformed on APS patients, who are frequently either underanticoagulation or thrombocytopenic, or because pathologistspay too little attention to APS nephropathy lesions in patientswith SLE nephritis [12]. This underestimation is confirmed byseveral cohort studies, in which APS nephropathy was specif-ically searched for, and in which its prevalence was in therange 10–40% [13–17]. Renal involvement has been reportedfor up to 71 % of patients with catastrophic APS [18].
Renal Manifestations Related to the APS
The presence of aPL has been associated with thrombosiswithin all the kidney vasculature (renal arteries,intraparenchymal arteries and arterioles, glomerular capil-laries and renal veins). Once developed, these lesions maylead to hypertension, acute renal failure, renal cortical necrosisthat can evolve to chronic renal failure, and ESRD. aPL mayalso be associated with thrombosis at the renal allograft intransplant patients.
Renal Artery Lesions
Renal artery involvement can be uni or bilateral, and usuallyconsists of occlusive lesions resulting from in-situ thrombosis,or of embolism from either a pre-existing upstream arteriallesion or a cardiac valve lesion. The most common clinicalmanifestation of renal artery thrombosis is the onset of severehypertension or the worsening of a previously-documentedsystemic hypertension, sometimes associated with pain in therenal area, hematuria, or renal failure [8•, 14, 19, 20]. Thislesion can also lead to renal infarction, ischemic acute renalfailure, and the slowly progressive ischemic chronic renal
insufficiency that is one of the main causes of renovascularhypertension.
The defining characteristic of artery involvement associat-ed with aPL is renal artery stenosis [21]. Sangle et al. [20]revealed the presence of renal artery stenosis by means ofmagnetic resonance renal angiography performed on 26 % of77 patients with aPL and uncontrolled hypertension. Stenoticlesions may be grouped into two different patterns with someunique features. The more frequent pattern is a noncriticalstenosis distal to the ostium of the renal artery, characterizedby smooth and well-delineated stenosis; the less commonpattern is a stenosis proximal to the ostium, occasionallyinvolving the aorta, which mimics atherosclerotic lesions[20–23]. It has been suggested that aPL have an importantfunction in accelerated atherosclerosis [24], and additionalobservations have suggested cross-reactivity between aPLand antibodies to oxidized LDL, HDL and Apo A-I, thusindicating a possible link between thrombotic and atheroscle-rotic complications [25, 26].
Imaging techniques, for example renal Doppler ultrasoundas a first-line procedure, followed if necessary by computedtomography, renal angiography, renal scintigraphy and gado-linium enhancement magnetic resonance angiography, shouldbe used for diagnosing and evaluating the extent of theselesions [27•].
Renal Vein Thrombosis
The association of aPL and renal vein thrombosis in patientswith SLE was first described by Asherson et al. [28].Thrombosis may occur in the main and/or minor renal veinsof patients with primary APS and patients with associatedSLE [29]. This manifestation has been especially associatedwith LA positivity, and is usually characterized by the pres-ence of nephrotic-range proteinuria. Consequently, if anypatient with persistently positive aPL suddenly developsheavy proteinuria, careful Doppler studies of the renal vascu-lature should be considered [30].
Intrarenal Vascular Lesions (APS nephropathy)
Presentation of APS nephropathy can vary widely, rangingfrom arterial hypertension in almost all patients to suddenacute renal failure requiring dialysis, or to mild and progres-sive chronic renal insufficiency with minimum levels of pro-teinuria that can progress to nephrotic range.
One of the best-known andmost important renal features ofAPS nephropathy is thrombotic microangiopathy (TMA), anacute lesion that was reported to be present in up to 20 % ofpatients with primary APS who underwent renal biopsy [10].Histopathologically, TMA is characterized by the absence of
Table 1 Main renal lesions described in antiphospholipid syndrome
Renal artery stenosis
Renal vein thrombosis
Glomerular lesions (APS nephropathy)
Thrombotic microangiopathy
Arteriosclerosis
Arterial fibrous intimal hyperplasia
Tubular thyroidization
Arteriolar occlusions
Focal cortical atrophy
End-stage renal disease
Allograft vascular thrombosis
397, Page 2 of 7 Curr Rheumatol Rep (2014) 16:397

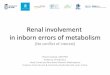
inflammatory cells and of vascular immune deposits, and bythe presence of fibrin thrombi in glomeruli and in the entireintrarenal vascular circulation (Fig. 1). Immunofluorescencestudies reveal that fibrin is the main constituent of thrombi inthe absence of immunoglobulins [31]. Although thrombi are acharacteristic feature of APS, they can also occur in manyother conditions caused by coagulation disturbances or endo-thelial cell injury, including thrombotic thrombocytopaenicpurpura, hemolytic uremic syndrome, scleroderma renal cri-sis, malignant hypertension, preeclampsia, cyclosporine tox-icity, chemotherapy and renal transplant rejection [13].
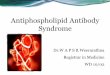
Among the chronic features of APS nephropathy, arterio-sclerosis is typically characterized by arterial fibrous intimalhyperplasia (FIH), an intimal thickening of the arteries andarterioles primarily caused by myofibroblastic cellular prolif-eration, with consequent lumen restriction and ischemia(Fig. 2). Focal cortical atrophy (FCA) involves the superficialcortex under the renal capsule, forming foci or triangles thathave sharp borders with the normal remainder of the cortex;this is accompanied by depression of the contour of the renalcapsule. In these atrophic areas all elements of the renalparenchyma are altered, in a pattern regarded as very typicalof APS nephropathy [32]. The glomeruli appear either smalland sclerotic, or large but virtually lacking the glomerularnetwork of capillaries. The tubules are atrophic and packedwith eosinophilic casts, resembling thyroid tissue (tubularthyroidization). The arterioles are occluded by fibrinmicrothrombi or, often, by fibrous tissue [8•].
Among the Hospital Clínic of Barcelona cohort of SLEpatients with APS nephropathy, TMAwas observed in 33.3 %of cases, whereas chronic lesions, specifically FIH and FCA,were observed in 44.4 % and 33.3 %, respectively. We ob-served a significant association between aPL and renal in-volvement. Patients with LA plus IgG aCL had an increasedprevalence of APS nephroapthy, suggesting that these aPLhave a direct effect on the development of renal involvement[17].
APS Nephropathy in Catastrophic APS
Renal involvement has been described as the most frequentclinical expression of catastrophic APS. When the initial 280patients from the “CAPS Registry” were evaluated, 71 % ofthem presented with renal involvement, usually resulting inrenal failure and laboratory evidence of glomerular damage(proteinuria, hematuria). When renal biopsy was performed,most cases had typical TMA. Immune-complex nephritis wasseldom observed, and renal infarctions were usually detectedduring investigation of patients presenting with abdominalpain [18]. In a study by Tektonidou et al. [33], including sixpatients with catastrophic APS on whom a kidney biopsy wasperformed, all subjects had acute and chronic renal vascularlesions compatible with diagnosis of APS nephropathy. Acuterenal lesions (TMA) were observed in all catastrophic-APSpatients. FIH and FCA were the most common chronic vas-cular lesions, occurring in four and three patients, respectively.When comparison was made with patients with non-catastrophic APS, the only difference between groups wasthe predominance of acute APS lesions in catastrophic APSpatients, a finding that was not surprising and was explainedby the acute nature of this syndrome.
Hypertension
Hypertension in association with livedo reticularis was one ofthe first manifestations associated with the presence of aPL, andwas described by Hughes in his original description of APS[34]. Nochy et al. [8•] reported that hypertension was present in93 % of 16 patients with APS renal involvement, and this wasone of the most important signs of underlying nephropathy.Thus, it is important to test for renal involvement in all patientswith hypertension andAPSwithout a clear underlying etiology;performance of glomerular filtration, renal ultrasound, nuclearFig. 1 TMA (arrow) in a renal glomerulus of a patient with primaryAPS
Fig. 2 FIH in a renal glomerulus of a patient with SLE and aPL withoutother manifestations of APS
Curr Rheumatol Rep (2014) 16:397 Page 3 of 7, 397

medicine technetium dimercaptosuccinic acid renal scans, andimaging of renal arteries and veins should be considered [35]. Ifrenal artery and/or vein thrombosis is diagnosed and treatedrapidly, these lesions respond well to anticoagulation with orwithout percutaneous balloon angioplasty, leading to recoveryof renal function and return to normal blood pressure [36, 37].
ESRD and Renal Transplantation
ESRD is a rare complication of primary APS. This was clearlyrevealed by Erkan et al. [38] in a prospective study of 39patients with primary APS who were followed over 10 years,during which time only one patient developed ESRD.
Several studies have revealed that patients with ESRD,from any cause, have a higher incidence of aPL positivitythan that found in the general population, although definitionsof positive aPL varied between the studies [9, 39–43].Additionally, one study byMatsuda et al. [44] found that theseaPL seemed to be mostly β2GPI-independent. In these stud-ies, the association of ESRD and aPL was irrespective of age,length of time on dialysis, sex, type of dialysis membrane,drug treatment, and chronic B and C hepatitis.
Possible causes of the presence of these antibodies includedialysis membranes [9], trauma to blood passing through thehemodialysis circuit [45], and induction by microbial agents[46] or their products, for example endotoxins present in thedialysate. Evidence suggests that aPL-positive patients under-going renal transplantation are at significantly increased riskof renal vascular thrombosis, graft failure, and systemicthrombosis. The presence of aPL seems to increase both theusual thrombotic risks associated with any major abdominalsurgery and the risk of renovascular thrombosis associatedwith renal transplant surgery. However, it is still uncertainwhether these antibodies are truly pathogenic in ESRD pa-tients or are just an epiphenomenon [47–52]. Recently, aprocedure for aPL-positive patients undergoing renal trans-plantation has been proposed by the Hospital for SpecialSurgery–Cornell in New York, revealing that perioperativeimmunosuppressives, given in addition to anticoagulation,can be beneficial for these patients irrespective ofhistocompatability profiles [53].
APS Nephropathy in SLE
As previously described, development of APS nephropathy inSLE may vary in frequency: from as low as 11.4 % in theHospital Clínic of Barcelona cohort of SLE patients [17], to39.5 % of SLE patients with aPL in the study by Tektonidouet al. [13]. Because of the retrospective design of all studies,and because the pathologists analyzed the biopsies specifical-ly to identify APS nephropathy lesions, the true prevalence of
APS nephropathy in SLE is not known for certain. Both acuteand chronic renal lesions, including fibrotic, proliferative andobstructive lesions caused by thrombotic changes, have beenfound in SLE patients in different cohorts [13–17].
In the Hospital Clínic of Barcelona cohort, we found thatpatients with LA plus IgG aCL had an increased prevalence ofAPS nephropathy, suggesting that these aPLmay have a directeffect on development of these lesions. When comparing SLEpatients with and without APS nephropathy, we found nodifference in the incidence of hypertension and nephroticsyndrome between groups. In contrast, serum creatinine levelswere significantly increased at the time of renal biopsy andtended to be higher at the end of follow-up for patients withAPS nephropathy. Despite this, no difference was observed inthe frequency of renal failure or of established renal damage atthe end of follow-up [17].
Routine evaluation of aPL and renal biopsy for SLE patientswith laboratory features of renal involvement are importantmeasures to enable clinicians to distinguish between APSnephropathy and SLE nephropathy. This will help cliniciansselect the appropriate therapy; for patients with APS nephrop-athy, only antithrombotic agents should be chosen, whereascytotoxic agents are needed for patients with lupus nephritis.
Treatment and Follow up
General Recommendations
For all aPL-positive patients it is important to control riskfactors for thrombosis and atherosclerosis, including obesity,smoking, hypertension, diabetes, and hyperlipidemia. Theoral contraceptive pill and hormone replacement therapyshould be avoided, given their association with thromboem-bolic disease.
Renal Vein and/or Artery Thrombosis
After the initial heparin treatment, the current recommenda-tion for secondary thromboprophylaxis in APS patients is life-long warfarin, because of the risk of recurrent events.Regarding the intensity of anticoagulation, two randomizedcontrolled trials (RCT) have suggested that international nor-malized ratio (INR) levels of 2.0 to 3.0 may be sufficient forAPS patients suffering no complications. Although target INRlevels of 2.0 to 3.0 should be enough for APS patients withrenal vein thrombosis, for patients with arterial events theintensity of anticoagulation is controversial because only ap-proximately 25% of patients in RCT had arterial events. Thus,for patients with renal artery thrombosis or recurrent renalvein thrombosis, addition of antiplatelet agents to warfarin(target INR 2.0–3.0) [17, 27•] or adoption of higher INR targetranges of 3.0 to 4.0 may be required [51].
397, Page 4 of 7 Curr Rheumatol Rep (2014) 16:397

For patients with renal artery stenosis, thrombolysis or trans-luminal balloon angioplasty with or without stenting may beconsidered. For severe lesions not amenable to angioplasty andstenting, surgical intervention is suggested [24, 54].
APS Nephropathy
The optimum management of patients with only intrarenalvascular lesions (APS nephropathy), alone or in combinationwith SLE nephropathy, is unknown because no study hasspecifically addressed this problem. On the basis of our per-sonal experience, we recommend starting anticoagulationwith an INR target of 2.0–3.0 (as for any other patient withthrombotic APS), and adding antiplatelet agents or increasingtarget INR levels to 3.0–4.0 if no improvement is achieved.Alternatively, studies performed by Tsagalis et al. [52] andErkan et al. [55] recently reported stabilization of renal func-tion and proteinuria by use of rituximab. These studies pro-posed that rituximab might have a function in the treatment ofpersistently aPL-positive patients with non-criteria manifesta-tions of APS, by reducing the production of autoantibodies.
Catastrophic APS
When acute renal failure and severe thrombotic thrombocyto-penic purpura are present, catastrophic APS should besuspected. Treatment of this APS variant is based on the useof anticoagulants, glucocorticoids, and either plasma ex-change or intravenous immunoglobulins (IVIG). In the“CAPS Registry”, better recovery was achieved with thiscombination of therapy (69 % versus 54 %) [18].
Conclusions
During the last decade, clinicians, rheumatologists and ne-phrologists have increasingly recognized major kidney in-volvement in patients with APS, with specific clinical andhistological features that may lead to renal injury caused bythrombosis at any location within the renal vasculature. InAPS patients with such manifestations as systemic hyperten-sion, livedo reticularis , hematuria, proteinuria or renal insuf-ficiency without any other justifying etiology, prompt evalu-ation via renal biopsy should be performed. Special careshould be taken, however, for those patients receiving anti-platelet agents or anticoagulation, and the risk of hemorrhageshould be balanced against the potential benefits of a moreaccurate diagnosis. Testing for aPL must also be consideredfor patients with any of these manifestations [56••].
For patients with SLE and positive aPL, APS nephropathy,alone or associated with SLE nephritis, should be considered,to guide prompt therapeutic decisions that may help to preventthe development of renal failure.
Anticoagulation remains the default treatment for patientswith renal involvement caused by APS. Patients with cata-strophic features often also require glucocorticoids, plasmaexchange and/or IVIG therapy. Future studies may help toidentify better therapeutic targets.
Compliance with ethics guidelines
Conflict of interest Guillermo J. Pons-Estel and Ricard Cerveradeclare that they have no conflict of interest.
Human and animal rights and informed consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. •Hughes GR. Thrombosis, abortion, cerebral disease, and the lupusanticoagulant. Br Med J (Clin Res Ed). 1983;287:1088–9.Originaldescription of antiphospholipid syndrome .
2. Espinosa G, Cervera R. Antiphospholipid syndrome. Arthritis ResTher. 2008;10:230.
3. Alessandri C, Conti F, Pendolino M, et al. New autoantigens in theantiphospholipid syndrome. Autoimmun Rev. 2011;10:609–16.
4. •Miyakis S, LockshinMD, Atsumi T, et al. International consensusstatement on an update of the classification criteria for definiteantiphospholipid syndrome (APS). J Thromb Haemost. 2006;4:295–306. Classification criteria of antiphospholipid syndrome .
5. Favaloro EJ, Silvestrini R. Assessing the usefulness ofanticardiolipin antibody assays: a cautious approach is suggestedby high variation and limited consensus in multilaboratory testing.Am J Clin Pathol. 2002;118:548–57.
6. Reber G, Schousboe I, Tincani A, et al. Inter-laboratory variabilityof anti-beta2- glycoprotein I measurement. A collaborative study inthe frame of the European Forum on Antiphospholipid AntibodiesStandardization Group. Thromb Haemost. 2002;88:66–73.
7. Hughes GR, Khamashta MA. Seronegative antiphospholipid syn-drome. Ann Rheum Dis. 2003;62:1127.
8. •Nochy D, Daugas E, Droz D, et al. The intrarenal vascular lesionsassociated with primary antiphospholipid syndrome. J Am SocNephrol. 1999;10:507–18. Relevant description of intrarenal APSlesions .
9. Garcia-Martin F, De Arriba G, Carrascosa T, et al. Anticardiolipinantibodies and lupus anticoagulant in end-stage renal disease.Nephrol Dial Transplant. 1991;6:543–7.
10. Sinico RA, Cavazzana I, Nuzzo M, et al. Renal involvement inprimary antiphospholipid syndrome: retrospective analysis of 160patients. Clin J Am Soc Nephrol. 2010;5:1211–7.
11. Vlachoyiannopoulos PG, Kanellopoulos P, Tektonidou M,Moutsopoulos HM. Renal involvement in antiphospholipid syn-drome. Nephrol Dial Transplant. 2001;16 Suppl 6:60–2.
12. Cervera R, Piette JC, Font J, et al. Antiphospholipid syndrome:clinical and immunologic manifestations and patterns of diseaseexpression in a cohort of 1,000 patients. Arthritis Rheum. 2002;46:1019–27.
Curr Rheumatol Rep (2014) 16:397 Page 5 of 7, 397

13. Tektonidou MG, Sotsiou F, Nakopoulou L, et al. Antiphospholipidsyndrome nephropathy in patients with systemic lupus erythema-tosus and antiphospholipid antibodies: prevalence, clinical associa-tions, and long-term outcome. Arthritis Rheum. 2004;50:2569–79.
14. Daugas E, Nochy D, Huong DL, et al. Antiphospholipid syndromenephropathy in systemic lupus erythematosus. J Am Soc Nephrol.2002;13:42–52.
15. Cheunsuchon B, Rungkaew P, Chawanasuntorapoj R, et al.Prevalence and clinicopathologic findings of antiphospholipid syn-drome nephropathy in Thai systemic lupus erythematosus patientswho underwent renal biopsies. Nephrology (Carlton). 2007;12:474–80.
16. Miranda JM, Jara LJ, Calleja C, et al. Clinical significance ofantiphospholipid syndrome nephropathy (APSN) in patients withsystemic lupus erythematosus (SLE). Reumatol Clin. 2009;5:209–13.
17. Silvariño R, Sant F, Espinosa G, et al. Nephropathy associated withantiphospholipid antibodies in patients with systemic lupus erythe-matosus. Lupus. 2011;20:721–9.
18. Cervera R, Bucciarelli S, Plasin MA, et al. Catastrophicantiphospholipid syndrome (CAPS): descriptive analysis of a seriesof 280 patients from the “CAPS Registry”. J Autoimmun. 2009;32:240–5.
19. Asherson RA, Noble GE, Hughes GR. Hypertension, renal arterystenosis and the “primary” antiphospholipid syndrome. JRheumatol. 1991;18:1413–5.
20. Sangle SR, D’Cruz DP, Jan W, et al. Renal artery stenosis in theantiphospholipid (Hughes) syndrome and hypertension. AnnRheum Dis. 2003;62:999–1002.
21. Sangle SR, D’Cruz DP. Renal artery stenosis: a new facet of theantiphospholipid (Hughes) syndrome. Lupus. 2003;12:803–4.
22. George J, Shoenfeld Y. The anti-phospholipid (Hughes) syndrome:a crossroads of autoimmunity and atherosclerosis. Lupus. 1997;6:559–60.
23. Harats D, George J, Levy Y, et al. Atheroma: links withantiphospholipid antibodies, Hughes syndrome and lupus. QJM.1999;92:57–9.
24. Rysava R, Zabka J, Peregrin JH, et al. Acute renal failure due tobilateral renal artery thrombosis associated with primaryantiphospholipid syndrome. Nephrol Dial Transplant. 1998;13:2645–7.
25. Delgado Alves J, Kumar S, Isenberg DA. Cross-reactivity betweenanticardiolipin, anti-high-density lipoprotein and anti-apolipoproteinA-I IgG antibodies in patients with systemic lupus erythematosus andprimary antiphospholipid syndrome. Rheumatology (Oxford).2003;42:893–9.
26. Vaarala O, Alfthan G, Jauhiainen M, et al. Crossreaction betweenantibodies to oxidised low-density lipoprotein and to cardiolipin insystemic lupus erythematosus. Lancet. 1993;341:923–5.
27. • Tektonidou MG. Renal involvement in the antiphospholipid syn-drome (APS)-APS nephropathy. Clin Rev Allergy Immunol.2009;36:131–40. Comprehensive description of APS nephropathy.
28. Asherson RA, Khamashta MA, Hughes GR. Hypertension and theantiphospholipid antibodies. Clin Exp Rheumatol. 1993;11:465–7.
29. Lai NS, Lan JL. Renal vein thrombosis in Chinese patients withsystemic lupus erythematosus. Ann Rheum Dis. 1997;56:562–4.
30. D’Cruz DP. Renal manifestations of the antiphospholipid syn-drome. Lupus. 2005;14:45–8.
31. Gigante A, Gasperini ML, Cianci R, et al. Antiphospholipid anti-bodies and renal involvement. Am J Nephrol. 2009;30:405–12.
32. Alchi B, Griffiths M, Jayne D. What nephrologists need to knowabout antiphospholipid syndrome. Nephrol Dial Transplant.2010;25:3147–54.
33. Tektonidou MG, Sotsiou F, Moutsopoulos HM. Antiphospholipidsyndrome (APS) nephropathy in catastrophic, primary, and systemiclupus erythematosus-related APS. J Rheumatol. 2008;35:1983–8.
34. Hughes GR. The Prosser-White oration 1983. Connective tissuedisease and the skin. Clin Exp Dermatol. 1984;9:535–44.
35. D’Cruz D. Renal manifestations of the antiphospholipid syndrome.Curr Rheumatol Rep. 2009;11:52–60.
36. Godfrey T, Khamashta MA, Hughes GR. Antiphospholipid syn-drome and renal artery stenosis. QJM. 2000;93:127–9.
37. Rossi E, Sani C, Zini M, et al. Anticardiolipin antibodies andrenovascular hypertension. Ann Rheum Dis. 1992;51:1180–1.
38. Erkan D, Yazici Y, Sobel R, LockshinMD. Primary antiphospholipidsyndrome: functional outcome after 10 years. J Rheumatol. 2000;27:2817–21.
39. Dayal NA, Isenberg DA. Endstage renal failure in primaryantiphospholipid syndrome—case report and review of literature.Rheumatology (Oxford). 2003;42:1128–9.
40. Prieto LN, Suki WN. Frequent hemodialysis graft thrombosis:association with antiphospholipid antibodies. Am J Kidney Dis.1994;23:587–90.
41. Brunet P, Aillaud MF, San Marco M, et al. Antiphospholipids inhemodiálisis patients: relationship between lupus anticoagulant andthrombosis. Kidney Int. 1995;48:794–800.
42. Gronhagen-Riska C, Teppo AM, Helantera A, et al. Raised con-centrations of antibodies to cardiolipin in patients receiving dialysis.BMJ. 1990;300:1696–7.
43. Sitter T, Spannagl M, Schiffl H. Anticardiolipin antibodies andlupus anticoagulant in patients treated with different methods ofrenal replacement therapy in comparison to patients with systemiclupus erythematosus. Ann Hematol. 1992;65:79–82.
44. Matsuda J, Saitoh N, Gohchi K, et al. beta 2-Glycoprotein I-dependent andindependent anticardiolipin antibody in patients withend-stage renal disease. Thromb Res. 1993;72:109–17.
45. Fastenau DR, Wagenknecht DR, McIntyre JA. Increased incidenceof antiphospholipid antibodies in left ventricular assist systemrecipients. Ann Thorac Surg. 1999;68:137–42.
46. Gharavi AE, Pierangeli SS. Origin of antiphospholipid anti-bodies: induction of aPL by viral peptides. Lupus. 1998;7 Suppl 2:S52–4.
47. Ozmen S, Danis R, Akin D, Batun S. Anticardiolipin antibodies inhemodyalisis patients with hepatitis C and their role in fistulafailure. Clin Nephrol. 2009;72:193–8.
48. Roozbeh J, Serati AR, Malekhoseini SA. Arteriovenous fistulathrombosis in patients on regular hemodialysis: a report of 171patients. Arch Iran Med. 2006;9:26–32.
49. Stone JH, Amend WJ, Criswell LA. Antiphospholipid antibodysyndrome in renal transplantation: occurrence of clinical events in96 consecutive patients with systemic lupus erythematosus. Am JKidney Dis. 1999;34:1040–7.
50. Vaidya S, Wang CC, Gugliuzza C, Fish JC. Relative risk of post-transplant renal thrombosis in patients with antiphospholipid anti-bodies. Clin Transplant. 1998;12:439–44.
51. Lim W, Crowther MA, Eikelboom JW. Management ofantiphospholipid antibody syndrome: a systematic review.JAMA. 2006;295:1050–7.
52. Tsagalis G, Psimenou E, Nakopoulou L, Laggouranis A. Effectivetreatment of antiphospholipid syndrome with plasmapheresis andrituximab. Hippokratia. 2010;14:215–6.
53. Domingues V, Dadhania D, Hartona C, Pastore R, Erkan D. Hospitalfor Special Surgery—Cornell protocol for antiphospholipid antibodypositive patients undergoing renal transplantation. 14th InternationalCongress on Antiphospholipid Antibodies. Rio de Janeiro,2013.
397, Page 6 of 7 Curr Rheumatol Rep (2014) 16:397

54. Aizawa K, Nakamura T, Sumino H, et al. Renovascular hyperten-sion observed in a patient with antiphospholipid–antibody syn-drome. Jpn Circ J. 2000;64:541–3.
55. Erkan D, Vega J, Ramon G, et al. A pilot open-label phase II trial ofrituximab for non-criteria manifestations of antiphospholipid syn-drome. Arthritis Rheum. 2013;65:464–71.
56. •• Cervera R, Tektonidou MG, Espinosa G, et al. Task force onCatastrophic Antiphospholipid Syndrome (APS) and non-criteriaAPS Manifestations (I): catastrophic APS, APS nephropathy andheart valve lesions. Lupus. 2011;20:165–73. Recommendations forthe diagnosis and management of APS nephropathy from a taskforce of APS experts .
Curr Rheumatol Rep (2014) 16:397 Page 7 of 7, 397