Embed Size (px)
Citation preview

Piero Ruggenenti,1,2 Manuela Abbate,1 Barbara Ruggiero,1 Stefano Rota,2
Matias Trillini,1 Carolina Aparicio,1 Aneliya Parvanova,1 Ilian Petrov Iliev,1
Giovanna Pisanu,1 Annalisa Perna,1 Angela Russo,1 Olimpia Diadei,1
Davide Martinetti,1 Antonio Cannata,1 Fabiola Carrara,1 Silvia Ferrari,1
Nadia Stucchi,1 Giuseppe Remuzzi,1,2,3 and Luigi Fontana,4,5,6
on behalf of the C.RE.S.O. Study Group*
Renal and Systemic Effects of CalorieRestriction in Patients With Type 2Diabetes With Abdominal Obesity: ARandomized Controlled TrialDiabetes 2017;66:75–86 | DOI: 10.2337/db16-0607
In individuals with type 2 diabetes with abdominal obe-sity, hyperfiltration is a risk factor for accelerated glo-merular filtration rate (GFR) decline and nephropathy.In this academic, single-center, parallel-group, pros-pective, randomized, open-label, blinded end pointtrial, consenting patients with type 2 diabetes aged >18years, with waist circumference >94 (males) or >80 (fe-males) cm, serum creatinine <1.2 mg/dL, and normoal-buminuria were randomized (1:1) with permuted blocks to6 months of a 25% calorie restricted (CR) or standard diet(SD). Primary outcome was measured GFR (iohexol plasmaclearance). Analyses were by modified intention to treat. At6 months, GFR significantly decreased in 34 patients on CRand did not change appreciably in 36 on SD. Changes weresignificantly different between the groups. GFR and bodyweight reduction were correlated. GFR reduction waslarger in hyperfiltering (GFR >120 mL/min) than nonhy-perfiltering patients and was associated with BMI, waistcircumference, blood pressure, heart rate, HbA1c, bloodglucose, LDL-to-HDL cholesterol ratio, C-reactive protein,angiotensin II, and albuminuria reduction andwith increased glucose disposal rate (measured byhyperinsulinemic-euglycemic clamps). Protein and sodium
intake and concomitant treatments were similar betweenthe groups. CR was tolerated well. In patients with type2 diabetes with abdominal obesity, CR amelioratesglomerular hyperfiltration, insulin sensitivity, and othercardiovascular risk factors, effects that might translateinto long-term nephro- and cardioprotection.
Obesity, especially if centrally located (1), and diabetes (2)are both associated with renal dysfunction sustained byglomerular hyperfiltration (3,4), a risk factor for accelera-ted loss of renal function and onset and progression ofnephropathy (5). Thus, glomerular hyperfiltration mightbe one of the possible pathogenic links between obesityand chronic kidney disease (CKD) (6,7). Finding that bari-atric surgery ameliorates glomerular hyperfiltration asso-ciated with severe obesity (8) suggests that weight loss, inaddition to ameliorating a series of cardiovascular riskfactors, might also affect the onset and progression ofCKD (5,8). This invasive procedure is, however, necessar-ily restricted to a selected population at very high riskof obesity-related complications. Thus, calorie restriction
1IRCCS - Istituto di Ricerche Farmacologiche Mario Negri, Centro di RicercheCliniche per le Malattie Rare “Aldo e Cele Daccò,” Bergamo, Italy2Unit of Nephrology, Azienda Socio Sanitaria Territoriale Papa Giovanni XXIII,Bergamo, Italy3Department of Biomedical and Clinical Sciences, University of Milan, Milan, Italy4Department of Clinical and Experimental Sciences, Brescia University MedicalSchool, Brescia, Italy5Department of Medicine, Washington University in St. Louis, St. Louis, MO6CEINGE Biotecnologie Avanzate, Napoli, Italy
Corresponding author: Giuseppe Remuzzi, [email protected].
Received 11 May 2016 and accepted 24 August 2016.
Clinical trial reg. no. NCT01213212, clinicaltrials.gov.
This article contains Supplementary Data online at http://diabetes.diabetesjournals.org/lookup/suppl/doi:10.2337/db16-0607/-/DC1.
This article is featured in a podcast available at http://www.diabetesjournals.org/content/diabetes-core-update-podcasts.
P.R. and M.A. contributed equally to this research.
*A complete list of the of the C.RE.S.O. Study Group can be found in theSupplementary Data online.
© 2017 by the American Diabetes Association. Readers may use this article aslong as the work is properly cited, the use is educational and not for profit, and thework is not altered. More information is available at http://www.diabetesjournals.org/content/license.
See accompanying article, p. 14.
Diabetes Volume 66, January 2017 75
OBESITYSTUDIES

(CR) remains the principal method for inducing weight loss(9). However, no trial so far has formally tested the role ofCR and weight loss on glomerular filtration, in particular bydirectly measuring the glomerular filtration rate (GFR) insubjects with glomerular hyperfiltration and abdominalobesity (10).
Thus, we evaluated whether and to what extent mea-sured GFR (11) could be affected by CR in the context of acontrolled, randomized clinical trial “Caloric REstrictionin Subjects with abdominal Obesity and Type-2 diabetesat increased risk” (C.RE.S.O).
RESEARCH DESIGN AND METHODS
This academic, single-center, parallel-group, prospective,randomized, open-label, blinded end point (PROBE) trial wasconducted at the Clinical Research Center (CRC) for RareDiseases of the IRCCS - Istituto di Ricerche FarmacologicheMario Negri. Participants were identified among patientsreferred to the outpatient clinics of the CRC and thediabetology units of Bergamo, Treviglio-Caravaggio, Romanodi Lombardia, and Seriate Hospitals, all in Italy. Participantswere individuals with type 2 diabetes (American DiabetesAssociation criteria) aged .18 years old with abdominalobesity defined as waist circumference of .94 cm in menand .80 cm in women (12), serum creatinine ,1.2 mg/dL,and urinary albumin excretion (UAE) ,20 mg/min in over-night urine collections. They had a stable body weight andcalorie intake, and a stable diet with a standardized contentin micro- and macronutrients and salt, according to guide-lines (13), and no systematic changes in blood pressure (BP),glucose, and lipid-lowering medications during the previous6 months. We excluded patients with primary, immune-mediated, or ischemic kidney disease; urinary tract obstruc-tion or infection; concomitant therapy with renin-angiotensinsystem (RAS) inhibitors, steroids, or nonsteroidal anti-inflammatory agents; heart failure; uncontrolled diabetes;hypo- or hypernatremia from any cause; previous bariatricsurgery; depression; alcohol and drug abuse; pregnancy;ineffective contraception; perimenopausal age; cancer orchronic disease that might jeopardize study completion;primary endocrinological diseases; poor compliance; or wereunable to provide informed consent. The study conformedto the principles of the EU Clinical Trials Directive(2001/20/EC), Good Clinical Practice, and the Declarationof Helsinki. The ethics committee of the local health agencyin Bergamo, Italy, approved the study. All patients providedwritten informed consent. Data were recorded in dedicatedcase record forms and then entered into the database atthe CRC. The study was reported according to ConsolidatedStandards of Reporting Trials guidelines.
Baseline EvaluationsAbdominal circumference was measured at the end of anormal expiration at the level of the iliac crest. Body weightwas measured in duplicate in the morning after a 12-h fastwith the subject wearing a hospital gown and no shoes. TheBMI was calculated using the standard formula. Office BP
was measured with an oscillometric device (HEM-705CP;Omron, Tokyo, Japan) with the patient sitting after 15 minof rest. The average of three measurements, 2 minutesapart, was recorded. Blood for laboratory assessmentswas sampled the morning after overnight fasting. UAEwas measured in three consecutive overnight urine collec-tions, and the median was recorded.
GFR was measured by the plasma clearance of un-labeled iohexol (11) after a single, intravenous injectionof 5 mL iohexol solution (647 mg/mL Omnipaque 300;Nycomed Amersham Sorin, Milan, Italy). Participants witha GFR .120 mL/min (i.e., a GFR exceeding the upper limitof normal range for measured GFR) were defined as hyper-filtering, and those with a GFR #120 mL/min as nonhyper-filtering (5,14). The GFR was not normalized for the bodysurface area to avoid the confounding effect of changes inbody surface area associated with diet-induced changes inbody weight (15,16), and absolute GFR values were consid-ered for the analyses. On the following day, the total-bodyglucose disposal rate (GDR) was assessed with hyperinsulinemic-euglycemic clamp (17).
Randomization and MaskingParticipants were randomly assigned (1:1) to 25% CR orto continue on their already prescribed SD by a computer-generated list of random permuted blocks prepared by astatistician (Giovanni Antonio Giuliano) of the CRC, whowas not involved in the analyses. All data assessors weremasked to treatment allocation.
Intervention and Follow-upIntervention in the SD aimed to reinforce compliancewith the recommended diet. Patients in the CR arm wereprovided with personalized dietary guidelines to decreasetheir daily calorie intake by 25%. The nutrient compositionrecommended with both CR and SD interventions wasflexible to accommodate individual preferences but wasdesigned to provide 45–50% of energy from carbohydrates,30–35% from fat, and 15–20% from proteins, supply 100%of the daily recommended micronutrient intake, .20 g/dayof fiber, and ,300 mg/day of cholesterol. Patients wereencouraged to consume moderate and low glycemic indexand nutrient-dense foods (18). No particular lifestyle mod-ification was introduced. Dietary prescriptions were basedon energy intake at baseline, estimated by the subjects’ rest-ing metabolic rate (RMR) using the Mifflin predictive equa-tion (19), and results from the Physical Activity Recall (PAR)and Total Daily Energy Expenditure (TDEE) questionnaire(20). CR corresponded to a 25% calorie decrease from esti-mated total daily energy intake.
Patients allocated to the CR intervention were given aprescription of total calories to consume daily and dieta-ry plans based on exchange systems that deliver a fixedamount of calories per food portion. Weight loss goals wereset together with the patients, and to facilitate adherence,patient-dietitian contact (in person, by telephone, or e-mail)was provided throughout the study period once a weekduring the first 3 months and once every 2 to 3 weeks
76 Renal Effects of Calorie Restriction Diabetes Volume 66, January 2017

during the remaining 3 months. In case the patient-dietitiancontact did not prove enough for maintaining dietarycompliance, behavioral intervention strategies, such asstimulus control (avoiding triggers that prompt eating),social support (assistance from family members and friendsin modifying lifestyle behaviors), cognitive restructuring(thinking in a positive manner), problem-solving skills(systematic method of analyzing problems and identifyingpossible solutions), and relapse prevention (methods to helprecovery from episodes of overeating or weight regain),were provided.
Patients were instructed to keep daily records of theirweight and weekly fasting glucose measurements. One weekbefore each trimonthly follow-up visit, participants com-pleted a 7-day food diary using household measures.Diaries were analyzed by means of the dietary analysissoftware package MètaDieta, Version 1.0.2, 2009 (METEDAS.r.l., San Benedetto del Tronto, AP, Italy) and used to as-sess compliance in the allocated study group. The dietarysoftware uses official national food composition databasessuch as the INRAN (Istituto Nazionale di Ricerca per gliAlimenti) and the IEO (Istituto Europeo di Oncologia).
Clinical and laboratory parameters, including serum urealevels taken as an indirect marker of dietary protein intake,evaluated at baseline were reevaluated at 3 and 6 monthsafter randomization, with the exception of GFR and GDR,which were reevaluated at 6 months only (final visit). Ateach visit, adverse events were recorded, and physical andlaboratory parameters were assessed for safety.
MeasurementsBlood and urine samples were collected after subjects hadfasted overnight and were centrally analyzed at the CRCfor Rare Diseases. Routine laboratory parameters weremeasured by spectrophotometry (UniCel Synchron Clin-ical System DXC800; Beckman Coulter s.r.l., Milan, Italy).Glycated hemoglobin (HbA1c) values were expressed byusing mmol/mol units according to the International Fed-eration of Clinical Chemistry and Laboratory Medicine(IFCC) and were then converted to percentage valuesaccording to the National Glycohemoglobin Standardi-zation Program (NGSP) by using the online HbA1c converterat http://www.ngsp.org/convert1.asp.
Serum insulin and angiotensin II concentrations weremeasured by chemifluorescence (Access 2; Beckman Coulter,Inc.) and the enzyme immunoassay kit (Angiotensin IISPIE-IA; Bertin Pharma, Montigny le Bretonneux, France),respectively, and hs-CRP, apolipoprotein A, apolipoproteinB, and urinary albumin by rate nephelometry (Immage;Beckman Coulter, Inc.).
Statistical AnalysesThe primary end point was the change in GFR at the6-month follow-up versus baseline. Other outcomes includedchanges in GDR (coprimary outcome), BP, heart rate (HR),blood glucose, HbA1c, serum lipid, plasma renin activity,C-reactive protein (CRP), and safety variables, including vitalsigns, clinical laboratory tests, and adverse events.
Sample size was estimated for the main prespecifiedoutcome variable assuming a two-group t test (two-sided) ofthe difference between CR and SD. On the basis of GFRdata available at the database of the CRC at the time ofstudy planning, we assumed a baseline mean 6 SD GFR of111 6 19.0 mL/min. We predicted a 15% GFR reductionfrom 111 to 94.35 mL/min with CR and no change with SD.On the basis of these assumptions, a sample size of 29 evalu-able participants per group would give the trial 90% powerto detect as statistically significant (a = 0.05 two-tailed test)the expected difference in GFR change between the twotreatment groups. To account for a 20% dropout rate, weplanned to include 36 participants per group.
All statistical analyses were conducted by modifiedintention to treat, using SAS 9.1 and Stata 12 software.Changes in GFR and all other between-group effects wereassessed by ANCOVA, adjusted for baseline measures.Within-group comparisons were assessed by paired t tests,repeated-measures ANOVA, or the McNemar test. Corre-lations were tested with the Pearson r correlation coeffici-ent. Multiple regression models were used to investigatethe association between baseline independent covariatesand GFR changes. We considered age, sex, and those base-line covariates that, in simple regression models, were as-sociated with GFR change at an a = 0.10 level ofsignificance (two-tailed). In the case of correlated covari-ates, variable selection was guided by clinical criteria. Totest the relationships between changes in different con-sidered parameters and the concomitant 6-month changesin GFR, we first identified which one among the consideredanthropometric, clinical, and metabolic variables and se-rum lipids had a strongest correlation with the outcome.We then entered changes in these variables along withchanges in mean BP (taken as a surrogate of both systolicand diastolic BP) into a multivariable model consideringGFR changes at 6 months as the outcome variable. Dataare expressed as mean 6 SD, median (interquartile range),or number (%), unless otherwise specified. All P values weretwo-sided.
RESULTS
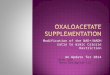
Of the 149 screened patients, 75 did not fulfill theselection criteria or declined to participate. From Septem-ber 2009 to May 2012, 36 of the 74 included patientswere randomized to CR and 38 to SD. Two participantswithdrew from the CR arm at treatment months 1 and5 because of noncompliance. One participant on the SDwas excluded at month 3 because of a protocol violation(initiation of RAS inhibition therapy during hospitaliza-tion because of atrial fibrillation), and another subjectwithdrew consent at month 3 for personal reasons. Thus,34 participants on CR and 36 on SD completed the studyand were available for final analyses (Fig. 1).
Patient CharacteristicsAll 74 included patients were Caucasian, 56 (75.7%) weremale, and 11 (14.9%) were current smokers. Age averaged
diabetes.diabetesjournals.org Ruggenenti and Associates 77

59.8 6 7.1 years. At baseline, 34 participants (45.9%)were overweight (BMI 25–29.9 kg/m2) and 33 (44.6%)were obese (BMI $30 kg/m2), with a mean BMI of 29.8 63.8 kg/m2, and a waist circumference of 103.1 6 10.3 cm.The GFR averaged 107.9 6 20.0 mL/min, and 20 (27.0%)patients were hyperfiltering. BP, blood glucose, and serumlipids were relatively well controlled. Results for otherlaboratory parameters were unremarkable. Sociodemographic(Supplementary Table 1) and anthropometric, clinical, andlaboratory parameters (Table 1); calorie intake, energy con-sumption, and diet composition (Table 2); and distributionof concomitant medications (Table 3) at inclusion weresimilar between the groups, with the exception of someexcess of patients on statins in the SD group. Ten patientsper group were hyperfiltering (Table 1). Independently oftreatment allocation, the GFR at baseline correlated withbody weight, BMI, serum angiotensin II levels, the LDL-to-HDL ratio, and UAE (Supplementary Table 2).
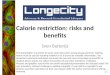
Treatment Effect on Kidney FunctionThe GFR significantly decreased by 7.6 6 11.7% (P =0.0006) with CR, whereas the 2.7 6 11.1% reduction ob-served with SD was not significant (P = 0.172). GFR changesversus baseline were significantly different between groups(P = 0.0472) (Table 1 and Fig. 2, top panel). Within thehyperfiltering group, the GFR significantly decreased by11.7 6 9.9% (P = 0.005) with CR, whereas the 5.3 69.0% reduction observed with SD failed to achieve sta-tistical significance (P = 0.095). In the nonhyperfilteringgroup, the GFR decreased by 3.8 6 8.1% (P = 0.032) withCR but did not change appreciably with SD (Table 1 andFig. 2, middle and bottom panel). GFR reduction tended tobe larger in patients with a BMI $30 kg/m2 than in those
with a smaller BMI. No significant change was observedwith SD in both BMI groups (Table 1).
UAE decreased significantly from 5.1 6 2.7 to 4.4 62.4 mg/min (P = 0.0248) in the CR group but did not changeappreciably in the SD group (Table 1 and SupplementaryFig. 1, bottom panel).
Treatment Effect on Other Considered Parameters
Anthropometric ParametersBody weight decreased by 4.7 6 5.5 kg (5.2 6 5.8%)in the CR group (P , 0.0001) and by only 0.6 6 1.6 kg(0.7 6 1.9%, P = 0.031) in the SD group (Table 1 andSupplementary Fig. 2, top panel). These changes weresignificantly different between groups (P = 0.0001). BMIconsistently decreased by 1.6 6 1.9 kg/m2 (5.2 6 5.8%,P , 0.0001) and waist circumference by 5.9 6 4.7 cm(5.8 6 4.5%, P , 0.0001) with CR and by only 0.2 60.6 kg/m2 (0.7 6 1.9%, P = 0.034) and 1.6 6 3.5 cm(1.5 6 3.4%, P = 0.009), respectively, with SD. Changeswere significantly different between groups (P , 0.0001 forboth parameters) (Table 1 and Supplementary Fig. 2, mid-dle and bottom panel).
Clinical and Laboratory ParametersSystolic (P = 0.0003), diastolic (P , 0.0001), and mean(P , 0.0001) BP consistently decreased with CR and onlymarginally decreased with SD. Interestingly, HR also de-creased significantly with CR (P = 0.0003) but did notchange appreciably with SD. Changes between groupswere significantly (P , 0.05) different for all consideredparameters (Table 1 and Supplementary Fig. 3).
Blood glucose (P = 0.0001) and HbA1c (P = 0.0001)levels both significantly decreased with CR, and on SD
Figure 1—Study flow chart. SAE, serious adverse event.
78 Renal Effects of Calorie Restriction Diabetes Volume 66, January 2017

the opposite trend was observed, which was signifi-cant for HbA1c (P = 0.039). Changes in both parameterswere significantly different (P = 0.0004 and P , 0.0001,respectively) between the groups (Table 1 and Fig. 3, topand middle panel). These changes were associated with asignificant increase in GDR with CR (P = 0.0007). GDRwas stable with SD, and GDR changes were significantlydifferent between the two treatment groups (P = 0.0075)(Table 1 and Fig. 3, bottom panel). In patients withoutlong-acting insulin therapy, insulin levels were similar
between treatment groups and did not change appreciablyduring the observation period.
Serum HDL levels increased (P = 0.043) and LDL levelsdecreased (P = 0.027) with CR. The opposite was observedin SD. Thus the LDL-to-HDL ratio significantly decreasedwith CR (P, 0.01) and tended to increase in SD. Changesin this parameter were significantly different between thegroups (P = 0.023) (Table 1). Other considered parametersdid not change appreciably within and between the groups(Table 1).
Table 1—Baseline and 6-month primary and secondary outcome measures in the two study groups
CR SD
Baseline 6 months Baseline 6 months P value†
Anthropometric variablesWaist circumference (cm) 104.1 (9.4) 98.2 (10.7)** 102.3 (10.2) 100.7 (9.9)* ,0.0001Weight (kg) 87.2 (13.7) 82.5 (13.2)** 83.4 (15.0) 82.8 (14.7)8 0.0001BMI (kg/m2) 30.0 (3.9) 28.4 (3.8)** 29.6 (3.8) 29.3 (3.7)8 ,0.0001BMI ,30 kg/m2 27.1 (1.7) 25.9 (1.9)88 27.0 (2.0) 26.8 (2.0) 0.0065BMI $30 kg/m2 33.7 (2.4) 31.6 (3.0)* 32.7 (2.9) 32.5 (2.7) 0.0064
Clinical parametersBP (mmHg)Systolic 127.8 (9.7) 121.1 (9.9)88 129.3 (9.1) 126.1 (8.6)8 0.0322Diastolic 80.5 (7.1) 75.3 (7.1)** 79.6 (7.3) 77.6 (7.3) 0.0349
MAP (mmHg) 96.3 (6.9) 90.6 (7.5)** 96.2 (7.3) 93.8 (7.1)8 0.0222HR (bpm) 68.2 (8.8) 63.7 (8.6)88 67.0 (8.7) 66.7 (7.8) 0.0094
Metabolic variablesGDR (mg/kg/min) 6.1 (2.3) 7.9 (3.1)88 6.4 (2.0) 6.6 (2.2) 0.0075Blood glucose (mg/dL) 138.9 (26.0) 120.8 (26.9)** 141.6 (25.6) 148.6 (41.5) 0.0004HbA1c (mmol/mol, IFCC)‡ 50.7 (11.1) 44.9 (7.6)** 48.4 (8.1) 51.3 (10.9)8 ,0.0001HbA1c (%, NGSP)‡ 6.8 (1.0) 6.3 (0.7)** 6.6 (0.7) 6.8 (1.0)8 ,0.0001Fasting insulin (mIU/L)^ 7.3 (3.4) 6.5 (5.4) 7.8 (4.6) 8.7 (4.6) 0.3738
LipidsCholesterolTotal (mg/dL) 171.2 (27.1) 167.3 (27.3) 171.4 (29.4) 172.8 (35.1) 0.3384HDL (mg/dL) 41.0 (11.3) 43.4 (10.8)8 41.8 (11.2) 41.0 (10.9) 0.0501LDL (mg/dL) 106.9 (26.1) 103.4 (27.8)8 105.8 (30.5) 106.8 (32.0) 0.3718LDL-to-HDL ratio 2.8 (0.97) 2.5 (0.91)* 2.6 (0.83) 2.7 (0.96) 0.0234
Triglycerides (mg/dL) 99.0 (35.7) 85.4 (34.3)8 117.8 (70.0) 132.1 (126.3) 0.1182Apolipoprotein A (mg/dL) 136.2 (19.6) 135.0 (15.9) 136.9 (16.8) 132.2 (21.8) 0.2030Apolipoprotein B (mg/dL) 84.3 (17.6) 79.9 (18.6) 86.4 (19.2) 86.4 (20.9) 0.1278
Other markershs-CRP (mg/dL) 0.32 (0.28) 0.20 (0.20)* 0.25 (0.33) 0.27 (0.34) 0.0164AST (IU/L) 22.6 (4.1) 20.2 (3.5)** 22.7 (5.4) 25.7 (17.7) 0.0067ALT (IU/L) 26.0 (7.8) 21.9 (6.4)** 26.2 (10.3) 34.2 (47.2) 0.0089CPK (IU/L) 149.0 (141.4) 123.0 (67.9) 132.1 (89.5) 113.5 (73.2)8 0.798Angiotensin II (pg/mL) 4.6 (3.5) 3.5 (2.9) 4.0 (2.7) 5.0 (4.2) 0.0421Urea (mg/dL) 37.6 (8.3) 39.5 (8.7) 38.8 (9.4) 39.0 (7.7) 0.3930
Kidney functionGFR (mL/min)Overall 107.8 (21) 100.2 (16.5)88 109.2 (19) 106.5 (20.2) 0.0472Hyperfiltering 134.4 (8.7) 118.1 (8.5)* 130.9 (8.8) 123.8 (13.2) 0.245Nonhyperfiltering 96.7 (12.9) 92.7 (12.9)8 99.4 (13.2) 98.6 (17.9) 0.237BMI ,30 kg/m2 99.5 (18.6) 95.2 (15.7)8 104.1 (17.3) 104.4 (18.4) 0.079BMI $30 kg/m2 118.2 (19.6) 106.4 (15.8)* 115.1 (19.7) 108.9 (22.6) 0.279
UAE (mg/min)# 5.1 (2.7) 4.4 (2.4)8 4.5 (2.7) 4.3 (2.3) 0.268
Data are mean (SD). ALT, alanine aminotransferase; AST, aspartate transaminase; CPK, creatine phosphokinase; MAP, mean arterialpressure. ‡Normal range: 25.0–28.9 mmol/mol or 4.4–5.7%; †Changes in the CR compared with the SD group at 6 months afteradjustment for baseline values by ANCOVA; ^Analysis excluded patients receiving long-acting insulin therapy; °P , 0.05; *P # 0.01;°°P # 0.001; **P # 0.0001 vs. baseline within the same treatment group; #Log-transformed.
diabetes.diabetesjournals.org Ruggenenti and Associates 79

Changes in BP, metabolic control, and serum lipidswere not explained by changes in concomitant treatmentbecause the distribution of different BP and lipid-loweringmedications in the two groups did not change appreciablyduring the study and because the proportion of patients onoral hypoglycemic agents similarly increased in both groups(Table 3).
Other Laboratory ParametersAspartate transaminase (P = 0.0001) and alanine amino-transferase (P = 0.0001) levels decreased with CR andtended to increase with SD. Changes between the groupswere significantly different (P = 0.0067 and P = 0.0089,respectively (Table 1). Creatine phosphokinase did not
change appreciably within and between the groups. hs-CRPlevels significantly decreased (P = 0.0075) on CR and didnot change appreciably with SD, whereas serum angioten-sin II levels tended to decrease with CR and to increase withSD. Changes in both variables were significantly differentbetween groups (P = 0.0164 and P = 0.0421, respectively)(Table 1 and Supplementary Fig. 1, top and middle panel).
Calorie Intake, Energy Consumption, and DietCompositionAccording to the 7-day food diaries, mean energy intakedecreased by 14.95 6 17.8% (P, 0.0001) with CR and by5.35 6 15.7% (P = 0.049) with SD. These changes weresignificantly different between the groups (P = 0.0061),
Table 2—Baseline and 6-month metabolic parameters and daily diet macro- and micronutrients in the two study groups
CR SD
Baseline 6 months Baseline 6 months P value†
Metabolic parametersRMR (kcal) 1,614.3 (236.8) 1,558.7 (233.6)** 1,544.0 (255.7) 1,536.1 (250.7)8 0.0001MET (h/day) 34.5 (3.7) 34.8 (4.2) 34.6 (3.1) 35.0 (4.9) 0.9293TDEE (kcal) 2,327.4 (459.2) 2,254.3 (405.9)8 2,230.8 (430.0) 2,245.0 (523.1) 0.1630Calorie intake (kcal) 1,899.5 (496.5) 1,570.9 (384.6)** 1,896.5 (524.1) 1,760.5 (423.8)8 0.0061
MacronutrientsProtein (%) 17.7 (2.2) 20.1 (2.6)88 18.5 (2.5) 18.3 (2.6) 0.0006Total lipid (%) 34.5 (5.7) 35.7 (4.8) 34.4 (5.1) 34.4 (6.0) 0.2719Carbohydrate (%) 48.0 (6.9) 44.4 (5.3)* 47.2 (6.4) 47.5 (7.8) 0.0132Protein (g) 81.0 (19.6) 74.6 (18.3)8 82.4 (20.6) 75.8 (20.0)* 0.9686Total lipid (g) 70.9 (22.3) 59.8 (12.1)88 68.9 (21.2) 63.2 (16.1)8 0.1134Carbohydrate (g) 234.4 (69.1) 183.9 (61.2)** 230.2 (76.5) 211.8 (60.3)8 0.0074Total dietary fiber (g) 23.6 (8.7) 23.9 (6.5) 20.1 (6.9) 18.7 (6.0) 0.0053Alcohol (g) 8.3 (10.9) 5.9 (7.4) 12.2 (13.4) 13.8 (13.0) 0.0047MUFA (g) 30.5 (9.7) 24.8 (5.2)** 28.8 (9.4) 26.9 (8.2) 0.0488PUFA (g) 9.3 (3.8) 9.7 (3.1) 8.6 (3.8) 8.2 (2.8) 0.0534Saturated fats (g) 22.8 (7.9) 16.4 (4.4)** 23.0 (7.4) 20.7 (6.3)8 0.0001Animal protein (g) 52.5 (15.1) 46.7 (11.1)8 56.1 (15.0) 50.4 (15.0)* 0.0337Vegetable protein (g) 27.3 (10.5) 27.9 (10.5) 25.1 (8.9) 24.3 (8.8) 0.2098
MicronutrientsCalcium (mg) 857.7 (341.8) 849.4 (250.1) 824.8 (226.6) 775.8 (347.0) 0.3771Iron (mg) 12.6 (4.3) 14.2 (4.5)8 11.7 (4.0) 11.3 (3.6) 0.0042Magnesium (mg) 225.75 (89.9) 230.25 (63.8) 252.5 (68.1) 232.7 (68.1) 0.0335Phosphorus (mg) 1,287.9 (387.7) 1,280.55 (280.1) 1,251.0 (331.0) 1,174.2 (359.4) 0.0099Potassium (mg) 3,111.3 (912.4) 3,241.0 (610.35) 2,911.4 (728.9) 2,815.1 (689.5) 0.0109Sodium (mg) 2,024.1 (874.3) 1,821.1 (854.3) 2,026.8 (699.2) 1,906.7 (800.9) 0.6323Zinc (mg) 11.5 (3.3) 11.25 (2.5) 11.1 (2.8) 10.4 (3.0)8 0.2234Copper (mg) 1.0 (0.47) 0.94 (0.29) 0.95 (0.37) 0.94 (0.32) 0.8506Selenium (mg) 36.9 (14.1) 38.2 (15.6) 38.8 (15.4) 38.0 (16.5) 0.7106Vitamin A (mg) 1,137.4 (648.3) 1,311.1 (823.9) 1,208.7 (643.0) 1,245.8 (677.1) 0.5430Vitamin D (mg) 3.0 (2.4) 3.0 (1.9) 2.5 (1.5) 2.5 (1.7) 0.3194Vitamin E (mg) 10.0 (3.4) 10.7 (2.4) 8.7 (2.7) 9.2 (3.2) 0.1025Vitamin C (mg) 137.0 (70.4) 170.8 (77.5) 106.8 (49.3) 101.5 (48.7) 0.0002Thiamin (mg) 1.2 (0.34) 1.1 (0.33) 1.1 (0.34) 1.0 (0.29) 0.1313Riboflavin (mg) 1.6 (0.52) 1.7 (0.41) 1.6 (0.45) 1.5 (0.44) 0.0232Niacin (mg) 20.4 (6.9) 19.8 (5.8) 21.3 (6.4) 18.8 (4.5)* 0.1798Pantothenic acid (mg) 2.1 (0.79) 2.3 (0.66) 2.4 (0.71) 2.3 (0.79) 0.3889Vitamin B6 (mg) 1.8 (0.47) 1.9 (0.44) 1.7 (0.43) 1.6 (0.40) 0.0587Folate (mg) 295.7 (112.5) 337.6 (106.3) 261.1 (105.6) 265.4 (89.5) 0.0066b-Carotene (mg) 3,754.9 (3,187.05) 4,545.2 (2,018.3) 3,320.9 (2,279.7) 3,572.6 (2,150.1) 0.0332
Data are mean (SD). MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acids. †Changes in the CR group compared withthe SD group at 6 months after adjustment for baseline values by ANCOVA; °P , 0.05; *P # 0.01; °°P # 0.001; **P # 0.0001 vsbaseline within the same treatment group.
80 Renal Effects of Calorie Restriction Diabetes Volume 66, January 2017

whereas RMR, MET, and TDEE did not change appreciablywithin and between the groups (Table 2). The reduction incalorie intake achieved in the CR, compared with the SDgroup, was largely explained by a reduced intake of carbo-hydrates and alcohol, whereas the total intake of proteinswas similar between the groups as documented by dataobtained by dietary diaries evaluation, including data onphosphate intake (Table 2), and by serum urea values thatwere very similar between the treatment groups and didnot change appreciably throughout the entire study period(Table 1). The dietary intake of monounsaturated fattyacids, saturated fats, animal proteins, and fat decreased,whereas the intake of total fiber, polyunsaturated fattyacids, and vegetable fat increased with CR compared withSD (Table 2). Subjects in the CR group introduced signifi-cantly more iron, magnesium, phosphorus, potassium, vita-min C, riboflavin, folate, and b-carotene than those in the SDgroup, whereas the intake of other dietary micronutrientswas similar between the groups. In particular, sodium intakewas very much the same at inclusion and decreased similarlyin the two groups during the study (Table 2).
Correlation Analyses and Predictors of GFR ReductionGFR reduction significantly correlated with body weight(P = 0.048), BMI (P = 0.017), and the GFR (P = 0.008) at
inclusion. At multiple regression analyses, consideringthe variables listed in Table 1, which at simple regressionanalyses were associated with the outcome at a signifi-cance level of P , 0.10, GFR reduction was predicted byCR (P = 0.045) and baseline GFR (P = 0.004).
GFR reduction also significantly correlated with areduction in daily calorie intake, body weight, BMI, waistcircumference, systolic, diastolic, and mean BP, bloodglucose, serum triglyceride levels, and an increase in GDR(Table 4). The correlation between changes in GFR andbody weight was significant in the study group as a whole(r = 0.409, P = 0.0007) and in patients with CR (r = 0.438,P = 0.0095) considered separately but not in those withSD (r = 0.271, P = 0.133). Multivariable regression
Table 3—Patients with concomitant medications at baselineand at the 6-month follow-up in the two treatment groups
Concomitantmedications
CR (n = 34) SD (n = 36)
Baseline 6 months Baseline 6 months
Hypoglycemicagents
Any 19 29 18 29Oral hypoglycemic
agents alone 17 26 15 26Insulin and oral
hypoglycemicagents 2 3 3 3
Antihypertensiveagents
Any 12 12 11 13Diuretic 5 7 0 3b-Blocker 2 3 6 6Calcium-channel
blockers 4 6 3 3Sympatholytic
agents 1 1 0 1ACE inhibitors,
angiotensinblockers 0 0 0 2
Lipid-loweringagents
Any 10 10 21 19Statin alone 9 9 21 18Fibrate alone 1 1 0 oStatin and fibrate 0 0 0 1Antiplatelet agent 2 2 8 7
Data are absolute number. No significant difference was ob-served between the two groups at baseline and at 5 months orbetween changes at 6 months vs. baseline in the two groups.
Figure 2—GFR at baseline and at the 6-month follow-up accordingto randomization to CR or SD in the entire study group (top panel)and in the two subgroups with (middle panel) or without (bottompanel) hyperfiltration at inclusion.
diabetes.diabetesjournals.org Ruggenenti and Associates 81

analyses showed the reduction in mean BP was the stron-gest predictor of GFR reduction. The association of weightreduction with GFR reduction was borderline significant,whereas changes in blood glucose and serum triglycerideshad no predictive value (similar findings were observedwhen diastolic BP was entered into the model instead ofmean BP) (Table 4). Independently of treatment alloca-tion, 1 mmHg of mean BP reduction and 1 kg of weightloss were associated with a mean GFR reduction of 0.45and 0.60 mL/min, respectively.
SafetyOnly two serious adverse events occurred, both in the SDgroup. Overall, nonserious adverse events were generallymild and transient in nature and were similarly distrib-uted between the groups. Viral and respiratory tractinfections were slightly more frequently reported in theSD group, whereas musculoskeletal events tended to bemore frequent with CR (Table 5). No event, however, wasconsidered to be treatment related by the investigators.
DISCUSSION
In this PROBE clinical trial in patients with type 2 diabe-tes and abdominal obesity, the 6-month CR significantlydecreased GFR compared with SD, an effect that waslargely driven by GFR reduction in patients with a higherGFR to start with and which was associated with areduction in waist circumference, body weight, BMI,
Figure 3—Blood glucose (top panel), HbA1c (middle panel), and theGDR (bottom panel) are shown at baseline and at the 6-monthfollow-up according to randomization to CR or SD.
Table 4—Correlation and multivariable analyses of therelationships between GFR changes (mL/min) at 6 monthscompared with baseline and concomitant changes in otherconsidered covariates
Correlationanalyses
Multivariableanalyses
r P value SbC P value
Anthropometric parametersWeight 0.41 0.0007 0.2379 0.0613BMI 0.39 0.011Waist circumference 0.32 0.0095
Clinical parametersSystolic BP 0.27 0.030Diastolic BP 0.41 0.0006MAP 0.39 0.0012 0.2484 0.0384HR 0.041 0.746
Metabolic parametersGDR 20.25 0.048Blood glucose 0.30 0.016 0.0764 0.5511HbA1c 20.02 0.87Fasting insulin 0.23 0.068
Serum lipidsCholesterol
Total 0.14 0.270HDL 20.01 0.935LDL 0.02 0.815LDL-to-HDL ratio 0.07 0.604
Triglycerides 0.35 0.0043 0.2031 0.1022Apolipoprotein A 0.10 0.429Apolipoprotein B 0.10 0.436
Other markershs-CRP 0.01 0.968AST 20.13 0.284ALT 20.11 0.363CPK 20.05 0.688Angiotensin II 0.20 0.108UAE 0.21 0.97
ALT, alanine aminotransferase; AST, aspartate transaminase;CPK, creatine phosphokinase; MAP, mean arterial pressure;SbC, standardized b-coefficient.
82 Renal Effects of Calorie Restriction Diabetes Volume 66, January 2017

systolic and diastolic BP, blood glucose, serum LDL-to-HDL cholesterol levels, and amelioration of insulinsensitivity, as assessed by hyperinsulinemic-euglycemicclamps in all patients. Of interest, every 1 kg of weightloss was associated with ;0.6 mL/min GFR reduction. CRand SD were both tolerated well, and no adverse effectspossibly related to inadequate or unbalanced nutrientsupply were observed throughout the study. Treatmenteffect was unlikely explained by changes in factors inde-pendent of CR that can affect glomerular hemodynamics,such as protein and sodium intake, which was very similarbetween the treatment groups. Moreover, baseline patientcharacteristics and distribution of concomitant medica-tions at inclusion and during the study were also similarbetween groups. Thus, study results appear to reflect agenuine effect of CR on glomerular filtration.
These findings could have clinical implications, becausepersistent hyperfiltration predicts a faster GFR declineand an excess risk of progression to micro- or macro-albuminuria in patients with type 1 (2) or type 2 diabetes(5,21), whereas amelioration of hyperfiltration is associ-ated with a slower GFR decline in the long-term andnephroprotection (5). We previously found that in a largecohort of patients quite similar to the C.RE.S.O. cohort, alarger GFR reduction at 6 months strongly and indepen-dently predicted a slower GFR decline in the long-term (5). Inparticular, a 7.6% short-term GFR reduction similar to thatachieved by CR predicted a mean long-term GFR decline of0.08 (SEM 013) mL/min/1.73m2 per month, whereas a 2.7%reduction similar to that observed in patients on SD predicteda long-term decline of 0.36 (SEM 0.07) mL/min/1.73m2 per
month. If the above findings are generalized to our C.RE.S.O.cohort, we can speculate that CR might reduce the rate oflong-term GFR decline by approximately four- to fivefoldcompared with SD. This renoprotective effect might translateinto a rate of renal function loss similar to that observed inhealthy adults with aging (22). Interestingly, the benefit of CRon glomerular dysfunction was more consistent and clinicallyrelevant in those patients with the highest GFR at baseline.Thus, the renoprotective effect of CR is expected to be largerright in those patients who, because of hyperfiltration, are atincreased risk of accelerated renal function loss (5).
Finding that a large part of the effect of CR on kidneyfunction appeared to be explained by the reduction in BPand, to a lesser extent, by weight reduction is consistentwith the hypothesis that an early rise in GFR in obesity islargely mediated by sodium retention (23). Increased re-nal sodium reabsorption, which appears to be mediatedby activation of the renin-angiotensin-aldosterone system(RAAS) and sympathetic system and by altered intrarenalphysical forces, may eventually result in volume expansionand increased BP (24). Moreover, increased proximal tubularreabsorption may reduce sodium chloride delivery to themacula densa and cause, via deactivation of tubuloglomeru-lar feedback, reductions in afferent arteriolar resistance andincreases in glomerular perfusion and filtration (8,23,25).Thus, we speculate that CR might reduce the GFR by re-ducing the sodium pool and therefore reducing BP and kid-ney perfusion. This effect could be mediated by decreasedRAAS and sympathetic activity, as suggested by the reduc-tion in angiotensin II levels and heart rate we observed withCR compared with SD. Enhanced responsiveness to natri-uretic peptides, which may even precede CR-induced weightloss, might also play a role (26). Moreover, by reducingtubular sodium reabsorption, CR might enhance sodiumchloride delivery to the macula densa, restore preglomerularresistances, and therefore, limit glomerular hyperperfusionand consequent hyperfiltration. These findings, however,must be interpreted with caution because of the post hocand observational nature of the analyses and becausemechanisms mediating the effects of CR on kidney func-tion should be investigated in prospective pathophysiologystudies.
CR was also associated with other clinically relevantfunctional and metabolic effects:
1. Amelioration of metabolic, BP, and lipid control: Thesechanges were associated with a significant increase inGDR with CR compared with SD, an effect that indi-cated amelioration of insulin sensitivity. This func-tional effect most likely explained blood glucose andHbA1c reduction in the active treatment arm andprobably could have at least partly contributed to BPreduction and amelioration of dyslipidemia in this sub-group. However, this effect could not be explained bychanges in energy consumption and concomitant med-ications, which were similar between the groups. Inde-pendent of involved mechanisms, amelioration of the
Table 5—Serious and nonserious adverse in the twotreatment groups
CR SD
Serious adverse eventsAtrial fibrillation 0 1Prostatic intraepithelial neoplasia 0 1Total 0 2
Nonserious adverse eventsFlu-like symptoms, cough, bronchitis, sinusitis 2 9Stranguria, cystitis 4 2Cervical, shoulder, knee pain 4 1Muscular strain/pain 4 1Tooth extraction/ache, gingivitis 3 3Traumatic back, ankle, wrist pain 3 1Headache/migraine 0 2Transient lymphocytopenia/eosinophilia 2 0Basal cell carcinoma right zygomas 0 1Prostatic hypertrophy 1 0Nephrolithiasis 0 1Right finger Dupuytren’s fibromatosis 0 1Vagal reaction 1 0Epigastralgia 0 1Cervical hernia 0 1Labyrinthitis 1 0Transient liver transaminases increase 0 1Transient CRP increase 0 1Total 25 26
diabetes.diabetesjournals.org Ruggenenti and Associates 83

functional and metabolic parameters mentioned abovecan be seen in the context of an overall amelioration ofmetabolic syndrome and are expected to translate intoa clinically relevant reduction in long-term cardiovascu-lar risk. Interestingly, the increase in GDR was alsoindependently associated with GFR reduction, a findingthat is consistent with the hypothesis that insulin re-sistance may also have a role in the pathogenesis ofglomerular hyperfiltration (27).
2. Reduction in sympathetic tone and RAAS activity: Thesignificant decrease in HR and serum angiotensin IIlevels observed with CR compared with SD mighthave clinical relevance. Indeed, a high resting HR haslong been independently associated with an increasedrisk of all-cause mortality and cardiovascular complica-tions in type 2 diabetes (28), as well as in the generalpopulation (29), and more recently, with new onset andworsening of retinopathy and nephropathy (30), find-ings that are most likely explained by the increase in BPand sympathetic activity associated with overweightand obesity (31). Consistently, long-term CR reducedthe HR and improved its variability in overweight butotherwise healthy adults, an effect associated with re-duced sympathetic activity and a concomitant in-crease in parasympathetic nervous system tone (32).RAAS activation is another cardiovascular risk factorthat has also been involved in the pathogenesis of glo-merular hyperfiltration and progression of renal dis-ease in experimental and human diabetes (33,34).Actually, the initial state of hyperfiltration associatedwith excessive adiposity, especially if centrally located,is largely sustained by raised systemic and renal pro-duction of angiotensin II (35), which may promotesystemic and local chronic inflammation, reactive ox-ygen species formation, lipogenesis, and hyperten-sion (35,36), with progressive renal dysfunction andstructural damage (37). We consistently found that6 months of CR significantly reduced CRP, a systemicmarker of inflammation and an independent cardio-vascular risk factor (38). The small reduction in albumin-uria we observed with CR might also have clinicalrelevance because albuminuria has been identified asan independent and continuous risk factor for renaland cardiovascular disease, even in the normal albu-minuric range (39).
3. Decrease in liver aminotransferase levels: This effectwas most likely explained not only by reduced alcoholintake but also by weight loss and improved insulinresistance achieved by CR. Elevated liver enzymesare a risk of progressive nonvirus-related nonalcoholicfatty liver disease in type 2 diabetes and associatestrongly with increased HbA1c, insulin resistance, andobesity. Reduced liver aminotransferase levels through CRcould preserve liver function and reduce steatohepatitisbecause primary prevention requires weight loss, im-proved glucose control, and metabolic syndrome ame-lioration (40).
Strengths and LimitationsThe number of participants was estimated a priori on thebasis of the expected treatment effect, which made itpossible to adequately power analyses despite the rela-tively small sample size. Moreover this was a pilot, ex-ploratory, and technically challenging study, and renalfunction, insulin sensitivity, and albuminuria were mea-sured by gold standard techniques, which, by reducing therisk of random data fluctuations, increased the statisti-cal power of the study analyses. Protein intake was notmonitored by measuring urinary urea excretion because24-h urine collections were not available. However,finding that serum urea levels were stable over time andcomparable between treatment groups at all visits, alongwith data from dietary diaries evaluation, confirmed thatprotein intake was comparable between the groups andstable over time, and reasonably, could not explain theGFR changes observed with calorie restriction. Thisconclusion is corroborated by finding that a reduction indietary proteins of at least 50–60% is needed to obtain anappreciable change in GFR and that protein intake in bothC.RE.S.O. groups was more than double that reportedin previous studies of patients with diabetes with low-protein diets (41,42).
Despite the highly labor-intensive design, the studyhad a high retention rate of enrolled participants andgood adherence to the study interventions, as shown bythe successful weight and waist circumference reductionachieved by CR. These findings confirm that complianceto dietary recommendations is an achievable goal, pro-vided that dietitians and doctors are strongly motivatedand are devoted enough to also transmit their motiva-tions to more disinclined patients. A “trial effect” mostlikely explained why some weight loss was also observedin controls on the SD during the treatment period, aneffect that most likely diminished between-group differ-ences in at least some of the considered outcome vari-ables. Finding that the treatment effect was captureddespite this limiting factor provided additional evidenceof the robustness of the results. However, whether theseresults can also be generalized to obese patients withoutdiabetes must be investigated.
One major strength was the PROBE design, whichallowed blinded analyses of outcome variables despite theopen design, and at the same time, minimized costs andclosely reflected standard clinical practice, which shouldmake the results more easily applicable in routine medicalcare (43). Changes in considered variables over thefollow-up period were consistent and uniformly con-firmed the potential beneficial effect of CR on a seriesof renal and cardiovascular risk factors. However, whetherthis short-term effect will/can translate into long-term nephro- and cardioprotection in this clinical contextneeds to be addressed in longer and appropriately pow-ered trials.
84 Renal Effects of Calorie Restriction Diabetes Volume 66, January 2017

ConclusionsThe CR-induced negative energy balance results in sub-stantial improvements of several major risk factors for theinitiation and progression of CKD in patients with diabeteswith abdominal obesity and no evidence of renal involvement.In particular, CR and weight loss, along with amelioration ofinsulin resistance and other functional and metabolic abnor-malities, achieved a significant short-term reduction in the GFRthat conceivably reflected amelioration of glomerular hyper-filtration and that resembled the reduction observed after aninvasive procedure such as bariatric surgery (8). Long-termrandomized clinical trials are needed to assess whether CRmay achieve clinically relevant protection against progressiverenal function loss and development of nephropathy in thelong-term as well as reduce overall patient cardiovascular risk.
Acknowledgments. The authors are indebted to Flavio Gaspari, whosupervised the laboratory analyses; Jorge Arturo Reyes Loaeza, Claudia PatriciaFerrer Siles, Karen Courville, Patricia Espindola, Silvia Prandini, Veruscka Lecchi,and Svitlana Yakymchuk, who took care of the study participants; GiovanniAntonio Giuliano, who generated the list of random permuted blocks; Nadia Rubisand Giulia Gherardi, who, respectively, supervised the monitoring of the studyand the activities of the day hospital of the CRC; Paola Boccardo, who took careof the ethical and regulatory aspects of the trial; Norberto Perico and the staff ofthe CRC, who contributed to the conduction of the study (all from IRCCS - Istitutodi Ricerche Farmacologiche Mario Negri, Centro di Ricerche Cliniche per leMalattie Rare “Aldo e Cele Daccò”, Bergamo, Italy); and Antonio Bossi (AziendaSocio Sanitaria Territoriale [ASST] Ospedali di Treviglio-Caravaggio and Romanodi Lombardia), Ruggero Mangili (ASST Ospedale Bolognini di Seriate), RobertoTrevisan (ASST Ospedale Papa Giovanni XXIII of Bergamo), and the staff of theiroutpatient clinics for their major contribution to patient screening and selection.Funding. This research was supported by grants from the Istituto Superiore diSanita/National Institutes of Health Collaborative Projects of the Italian Ministryof Health, the Bakewell Foundation, and the Longer Life Foundation (an RGA/Washington University Partnership).
The sponsors had no role in conducting study and reporting the results.Duality of Interest. No potential conflicts of interest relevant to this articlewere reported.Author Contributions. P.R. wrote the final version of the manuscript.P.R., M.A., S.R., G.R., and L.F. wrote the study protocol. P.R., M.A., G.R., and L.F.contributed to data analyses and interpretation. P.R., G.R., and L.F. had theoriginal idea. M.A., B.R., S.R., M.T., C.A., A.Pa., and I.P.I. identified, treated,and monitored study participants and contributed to data recording. M.A. andG.P. prescribed CR or SD and monitored compliance to the recommended diets.M.A. and L.F. wrote the first draft. A.Pe. and A.R. performed the statisticalanalyses. O.D. monitored the study. D.M. prepared the database and helped indata handling. A.C., F.C., S.F., and N.S. performed the GFR measurements andlaboratory tests. All of the authors had direct access to original data, criticallyrevised the draft, and approved the final manuscript. G.R. is the guarantor of thiswork and, as such, had full access to all the data in the study and takesresponsibility for the integrity of the data and the accuracy of the data analysis.
References1. Chagnac A, Weinstein T, Korzets A, Ramadan E, Hirsch J, Gafter U. Glo-merular hemodynamics in severe obesity. Am J Physiol Renal Physiol 2000;278:F817–F8222. Yip JW, Jones SL, Wiseman MJ, Hill C, Viberti G. Glomerular hyperfiltrationin the prediction of nephropathy in IDDM: a 10-year follow-up study. Diabetes1996;45:1729–1733
3. Sasson AN, Cherney DZ. Renal hyperfiltration related to diabetes mellitusand obesity in human disease. World J Diabetes 2012;3:1–64. Wuerzner G, Pruijm M, Maillard M, et al. Marked association betweenobesity and glomerular hyperfiltration: a cross-sectional study in an Africanpopulation. Am J Kidney Dis 2010;56:303–3125. Ruggenenti P, Porrini EL, Gaspari F, et al.; GFR Study Investigators. Glo-merular hyperfiltration and renal disease progression in type 2 diabetes. DiabetesCare 2012;35:2061–20686. Foster MC, Hwang SJ, Larson MG, et al. Overweight, obesity, and thedevelopment of stage 3 CKD: the Framingham Heart Study. Am J Kidney Dis2008;52:39–487. Chang Y, Ryu S, Choi Y, et al. Metabolically healthy obesity and developmentof chronic kidney disease: a cohort study. Ann Intern Med 2016;164:305–3128. Chagnac A, Weinstein T, Herman M, Hirsh J, Gafter U, Ori Y. The effects ofweight loss on renal function in patients with severe obesity. J Am Soc Nephrol2003;14:1480–14869. Tsai AG, Wadden TA. In the clinic: obesity. Ann Intern Med 2013;159:ITC3-1–ITC3-15; quiz ITC13–1610. Bolignano D, Zoccali C. Effects of weight loss on renal function in obeseCKD patients: a systematic review. Nephrol Dial Transplant 2013;28(Suppl. 4):iv82–iv9811. Gaspari F, Perico N, Ruggenenti P, et al. Plasma clearance of nonradioactiveiohexol as a measure of glomerular filtration rate. J Am Soc Nephrol 1995;6:257–26312. International Federation of Diabetes. The IDF Consensus Worldwide Defi-nition of the Metabolic Syndrome [Internet], 2006. Available from https://www.idf.org/webdata/docs/IDF_Meta_def_final.pdf. Accessed 7 July 201613. Associazione Medici Diabetologia - Società Italiana di Diabetologia. StandardItaliani per la Cura del Diabete Mellito 2009-2010 [Internet], 2010. Available fromhttp://www.aemmedi.it/files/Linee-guida_Raccomandazioni/2010/2010-2010_linee_guida.pdf. Accessed 7 July 201614. Jerums G, Premaratne E, Panagiotopoulos S, MacIsaac RJ. The clinicalsignificance of hyperfiltration in diabetes. Diabetologia 2010;53:2093–210415. Nelson RG, Bennett PH, Beck GJ, et al.; Diabetic Renal Disease StudyGroup. Development and progression of renal disease in Pima Indians withnon-insulin-dependent diabetes mellitus. N Engl J Med 1996;335:1636–164216. Fufaa GD, Weil EJ, Lemley KV, et al. Structural predictors of loss of renalfunction in American Indians with type 2 diabetes. Clin J Am Soc Nephrol 2016;11:254–26117. Parvanova AI, Trevisan R, Iliev IP, et al. Insulin resistance and micro-albuminuria: a cross-sectional, case-control study of 158 patients with type 2diabetes and different degrees of urinary albumin excretion. Diabetes 2006;55:1456–146218. Holloszy JO, Fontana L. Caloric restriction in humans. Exp Gerontol 2007;42:709–71219. Frankenfield DC, Rowe WA, Smith JS, Cooney RN. Validation of severalestablished equations for resting metabolic rate in obese and nonobese people.J Am Diet Assoc 2003;103:1152–115920. Blair SN, Haskell WL, Ho P, et al. Assessment of habitual physical activity bya seven-day recall in a community survey and controlled experiments. Am JEpidemiol 1985;122:794–80421. Silveiro SP, Friedman R, de Azevedo MJ, Canani LH, Gross JL. Five-yearprospective study of glomerular filtration rate and albumin excretion rate innormofiltering and hyperfiltering normoalbuminuric NIDDM patients. DiabetesCare 1996;19:171–17422. Lindeman RD, Tobin J, Shock NW. Longitudinal studies on the rate ofdecline in renal function with age. J Am Geriatr Soc 1985;33:278–28523. D’Agati VD, Chagnac A, de Vries AP, et al. Obesity-related glomerulopathy:clinical and pathologic characteristics and pathogenesis. Nat Rev Nephrol 2016;12:453–47124. Naumnik B, Myśliwiec M. Renal consequences of obesity. Med Sci Monit2010;16:RA163–RA170
diabetes.diabetesjournals.org Ruggenenti and Associates 85

25. Chagnac A, Herman M, Zingerman B, et al. Obesity-induced glomeru-lar hyperfiltration: its involvement in the pathogenesis of tubular sodium re-absorption. Nephrol Dial Transplant 2008;23:3946–395226. Dessì-Fulgheri P, Sarzani R, Serenelli M, et al. Low calorie diet enhancesrenal, hemodynamic, and humoral effects of exogenous atrial natriuretic peptidein obese hypertensives. Hypertension 1999;33:658–66227. De Cosmo S, Menzaghi C, Prudente S, Trischitta V. Role of insulin resistancein kidney dysfunction: insights into the mechanism and epidemiological evidence.Nephrol Dial Transplant 2013;28:29–3628. Hillis GS, Woodward M, Rodgers A, et al. Resting heart rate and the risk ofdeath and cardiovascular complications in patients with type 2 diabetes mellitus.Diabetologia 2012;55:1283–129029. Caetano J, Delgado Alves J. Heart rate and cardiovascular protection. Eur JIntern Med 2015;26:217–22230. Hillis GS, Hata J, Woodward M, et al. Resting heart rate and the risk ofmicrovascular complications in patients with type 2 diabetes mellitus. J Am HeartAssoc 2012;1:e00283231. Rossi RC, Vanderlei LC, Gonçalves AC, et al. Impact of obesity on autonomicmodulation, heart rate and blood pressure in obese young people. Auton Neurosci2015;193:138–14132. de Jonge L, Moreira EA, Martin CK, Ravussin E; Pennington CALERIE Team.Impact of 6-month caloric restriction on autonomic nervous system activity inhealthy, overweight, individuals. Obesity (Silver Spring) 2010;18:414–41633. Zatz R, Dunn BR, Meyer TW, Anderson S, Rennke HG, Brenner BM. Pre-vention of diabetic glomerulopathy by pharmacological amelioration of glomerularcapillary hypertension. J Clin Invest 1986;77:1925–193034. Steckelings UM, Rompe F, Kaschina E, Unger T. The evolving story of theRAAS in hypertension, diabetes and CV disease: moving from macrovascular tomicrovascular targets. Fundam Clin Pharmacol 2009;23:693–703
35. Kim S, Soltani-Bejnood M, Quignard-Boulange A, et al. The adipose renin-angiotensin system modulates systemic markers of insulin sensitivity and acti-vates the intrarenal renin-angiotensin system. J Biomed Biotechnol 2006;2006:2701236. Ruiz-Ortega M, Ruperez M, Lorenzo O, et al. Angiotensin II regulates thesynthesis of proinflammatory cytokines and chemokines in the kidney. Kidney IntSuppl 2002: S12–S2237. Henegar JR, Bigler SA, Henegar LK, Tyagi SC, Hall JE. Functional andstructural changes in the kidney in the early stages of obesity. J Am Soc Nephrol2001;12:1211–121738. Salazar J, Martínez MS, Chávez M, et al. C-reactive protein: clinical andepidemiological perspectives. Cardiol Res Pract 2014;2014:60581039. Ruggenenti P, Porrini E, Motterlini N, et al.; BENEDICT Study Investi-gators. Measurable urinary albumin predicts cardiovascular risk amongnormoalbuminuric patients with type 2 diabetes. J Am Soc Nephrol 2012;23:1717–172440. Ahmed A, Wong RJ, Harrison SA. Nonalcoholic Fatty Liver Disease Review:Diagnosis, Treatment, and Outcomes. Clin Gastroenterol Hepatol 2015;13:2062–207041. Rudberg S, Dahlquist G, Aperia A, Persson B. Reduction of protein intakedecreases glomerular filtration rate in young type 1 (insulin-dependent) di-abetic patients mainly in hyperfiltering patients. Diabetologia 1988;31:878–88342. Jones SL, Kontessis P, Wiseman M, et al. Protein intake and blood glucoseas modulators of GFR in hyperfiltering diabetic patients. Kidney Int 1992;41:1620–162843. Hansson L, Hedner T, Dahlöf B. Prospective randomized open blinded end-point (PROBE) study. A novel design for intervention trials. Prospective Ran-domized Open Blinded End-Point. Blood Press 1992;1:113–119
86 Renal Effects of Calorie Restriction Diabetes Volume 66, January 2017