-
Reliability of the Nyvad criteria forcaries assessment in
primary teeth
Mariana C. Sllos, Vera M. SovieroDepartment of Preventive and
CommunityDentistry, School of Dentistry, Universidade doEstado do
Rio de Janeiro, Rio de Janeiro,Brazil
One of the purposes of diagnosing dental caries is todetect and
classify the lesions, in order to select the mostappropriate
treatment for each tooth surface (1). Con-sidering the slower rate
of dental caries progression incontemporary populations, the
assessment of non-cavitated lesions is of great importance for
measuring theeectiveness of preventive approaches in
longitudinalstudies (26). If caries detection is restricted to
countingthe number of tooth surfaces with cavities, the earlystages
of the disease process are not considered. There-fore, caries
prevalence is underestimated and thebehaviour of individual caries
lesions cannot be moni-tored (7, 8). Many studies have conrmed that
highinterexaminer and intra-examiner agreement can beachieved even
when precavitated lesions are recorded(812), and since the 1950s,
the inclusion of non-cavitated lesions has been recommended
(1318).However, the World Health Organization decided not toinclude
enamel caries lesions in their caries index, mainlybecause the
diagnosis may not be reliable when thediagnostic threshold is set
at the non-cavitated level, justas it was considered that the
inclusion of enamel carieslesions would make a comparison of the
caries situationamongst countries worldwide more dicult
(19).Besides the inclusion of lesions at the non-cavitated
stage, the assessment of lesion activity is of majorimportance.
The decision on clinical treatment will varydepending on the
classication of the lesion as beingactive or inactive. Inactive or
arrested lesions may notneed any intervention, whereas active
lesions have to be
treated using non-operative procedures (such as oralhygiene
improvement and topical uorides) or operativetreatment (6, 7, 20).
The Nyvad caries diagnostic systemwas the rst classication system
to dene clear criteriafor the activity assessment of both
non-cavitated andcavitated lesions (8). Recently, an International
CariesDetection and Assessment System (ICDAS) has beensuggested
(4). This system is focused on the estimation oflesion depth and
does not include lesion activity in theirprimary caries codes. A
second score system to assessactivity has been suggested for use in
combination withthe primary ICDAS codes (21).Clinical studies have
shown that the Nyvad classi-
cation system has construct validity because activityassessment
reected the expected eects of uoridetoothpaste on caries lesions
(11, 22). Moreover, it hasalso been observed that caries activity
assessment haspredictive validity because active non-cavitated
lesionshave a signicantly greater risk of progressing to cavitythan
do inactive lesions (22). With the diagnosticthreshold set at
active vs. inactive lesions, the criteriahave also been shown to be
reliable, with kappa coe-cient values in permanent teeth ranging
between 0.68 and0.80 for intra-examiner agreement and between 0.74
and0.78 for interexaminer agreement (8). So far, the Nyvadcaries
classication system has been used successfully inclinical studies
(11, 2224), but more studies on its reli-ability in both permanent
and primary teeth are needed.The purpose of the present clinical
study was to assess
the interexaminer and intra-examiner reliability of the
Sellos MC, Soviero VM. Reliability of the Nyvad criteria for
caries assessment inprimary teeth.Eur J Oral Sci 2011; 119: 225231.
2011 Eur J Oral Sci
This study assessed the interexaminer and intra-examiner
reliability of the Nyvadcaries classication system in primary teeth
and calculated the mean examination time.The criteria were based on
visual and tactile examinations to dierentiate active andinactive
lesions at cavitated and non-cavitated levels. Eighty children (37
yr of age)were examined under standardized conditions by calibrated
examiners. At the toothsurface level, reliability was expressed as
percentage agreement and kappa coecient,using four diagnostic
thresholds: sound vs. diseased; sound or inactive lesion vs.
activelesion; intact surface vs. surface discontinuity; and sound
or non-cavitated lesion vs.cavitated lesion. Interexaminer and
intra-examiner kappa values were, respectively:0.82/0.86;
0.80/0.86; 0.90/0.94; and 0.95/0.98. At the individual level,
reliability ofestimates of the caries prevalence and of the decayed
or lled surface (dfs) counts wereassessed at three diagnostic
thresholds: sound vs. diseased; sound or inactive lesion vs.active
lesion; and sound or non-cavitated lesion vs. cavitated lesion. For
caries prev-alence, interexaminer and intra-examiner kappa values
were, respectively: 0.84/0.94;0.69/0.74; and 0.95/0.97. The mean
examination time was 226.5 s (SD = 128.5). Theuse of the Nyvad
caries diagnostic criteria in primary teeth showed reliable
results. Theexamination time was acceptable.
Prof. Vera Mendes Soviero, Faculdade deOdontologia, Clnica de
Odontopediatria,Universidade do Estado do Rio de Janeiro UERJ, Av.
28 de Setembro, 157 (2/ andar), VilaIsabel, 20511-030 Rio de
Janeiro RJ, Brazil
Telefax: +552128686372E-mail: [email protected]
Key words: dental caries; diagnosis; primaryteeth;
reliability
Accepted for publication March 2011
Eur J Oral Sci 2011; 119: 225231DOI:
10.1111/j.1600-0722.2011.00827.xPrinted in Singapore. All rights
reserved
2011 Eur J Oral Sci
European Journal ofOral Sciences
-
Nyvad caries classication system for caries assessmentand
classication in primary teeth and to calculate themean examination
time.
Material and methodsThe study sample consisted of 80 children
[45 boys and 35girls; 37 yr of age (mean age 5.1 yr)], with a high
cariesexperience, from a government school in Rio de
Janeiro,Brazil. Children had to have at least four primary
incisorsremaining to be included in the study. All children in
thestudy sample were born and raised in an urban area thathad a
uoridated water supply (0.41.5 mg l)1 of uoride).Informed consent
was obtained from parents, and the studywas approved by the
Committee for Ethics in Research atthe Rio de Janeiro State
University.Dental examinations were carried out in a dental
chair
under standardized conditions (compressed air for 35 s,articial
light, cotton rolls, a dental mirror, and a sharpprobe) by two
calibrated examiners (V.S. and M.S.), inde-pendently. Children had
their teeth brushed by the rstexaminer before the examination.
Then, they werepositioned in the dental chair and, if necessary,
additional
biolm was removed during the examination using aprobe. Only
primary teeth were recorded at the tooth sur-face level.The Nyvad
criteria are based on visual and tactile
diagnoses to assess caries lesion activity at three
progressionstages: the non-cavitated stage; the enamel
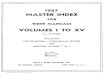
discontinuitystage; and the cavitated stage (8, 25). The codes used
toclassify the criteria in primary teeth are shown in Fig. 1. Inthe
event of doubt, examiners were instructed to choose thecode
representing the less severe status. However, in thepresence of two
or more caries lesions on the same toothsurface, themost severe
caries lesion was registered accordingto the following severity
scale: active lesion>inactive lesion,and cavitated
lesion>surface discontinuity>non-cavitatedlesion. Each child
was examined on two dierent days. Theexaminer M.S. performed the
rst examination, and theexamination time was measured using a
digital chronometer,which was started as soon as the dental mirror
was placed inthe childs mouth. Immediately following the rst
examina-tion, V.S. carried out the second examination.Oneweek
later,M.S. repeated the examination.The examiners were trained for
2 wk by two of the
authors of the criteria (Drs B. Nyvad and V.Machiulskiene),with
the training being based on clinical examinations and
A-a
B-a
C-a
A-b
B-b F-a F-b
G
I
H
J
C-b
A-c E-a E-b E-c
D-a D-b D-c
Fig. 1. Clinical aspects of the Nyvad caries diagnostic codes in
primary teeth. A-a, A-b, and A-c: code 0, sound surfaces; B-a and
B-b:code 1, active non-cavitated lesions; C-a and C-b: code 2,
active enamel discontinuity; D-a, D-b, and D-c: code 3, active
cavitatedlesions; E-a, E-b, and E-c: code 4, inactive non-cavitated
lesions; F-a and F-b: code 5, inactive enamel discontinuity; G:
code 6, inactivecavitated lesion; H: code 7, lling; I: code 8,
lling associated with an active lesion; J: code 9, lling associated
with an inactive lesion.
226 Sellos & Soviero
-
discussions. Calibration was performed in a pilot studyinvolving
30 children, which was carried out under the sameconditions as the
present study.
Evaluation
The agreement was rst analyzed at the tooth surface
level.Interexaminer and intra-examiner reliability of the
cariesdiagnostic codes (09) was assessed. Then, the codes
weredichotomized at four category thresholds: (i) sound (code 0)vs.
diseased (codes 19); (ii) sound or inactive lesion (codes0, 4, 5,
6, 7, and 9) vs. active lesion (codes 1, 2, 3, and 8); (iii)intact
surface (codes 0, 1, 4, 7, and 9) vs. surface disconti-nuity (codes
2, 3, 5, 6, and 8); and (iv) sound or non-cavitated lesion (codes
0, 1, 2, 4, 5, 7, and 9) vs. cavitatedlesion (codes 3, 6, and 8).
The results were expressed aspercentage agreement and Cohens kappa
coecient foreach diagnostic threshold.At the individual level, the
caries prevalence (the per-
centage of children with caries) and the extent [the decayedor
lled surface (dfs) count for each child] was estimatedconsidering:
(i) all caries lesions (codes 19); (ii) active carieslesions (codes
1, 2, 3, and 8); and (iii) cavitated caries lesions(codes 3, 6, and
8). For the dfs, interexaminer andintra-examiner agreement was
assessed using the methoddescribed by Bland & Altman (26). In
this analysis, thedierence between the dfs counts obtained in the
rst andsecond examination is plotted against the mean count ofboth
examinations. Based on the SD of the dierences,upper and lower
limits of agreement are calculated, whichresults in an interval
where 95% of the dierences betweenthe examinations are found. For
caries prevalence, agree-ment was assessed by percentage agreement
and Cohenskappa coecient for each diagnostic threshold.
The MannWhitney U-test was used to verify the inu-ence of the
childrens age and caries experience on the meanexamination time.
The signicance level for all of theanalyses was set at 5% (a =
0.05).
Results
A total of 6,400 tooth surfaces from 80 children weresuitable
for the study. Table 1 presents the intra-examiner and
interexaminer percentage agreement andkappa values at the
tooth-surface level. In general, kappavalues were 0.80 or higher in
all analyses, with theexception of a kappa value of 0.76 when
considering allcodes from 0 to 9. The percentage agreement varied
from0.96 to 0.99. The highest kappa values (0.95 and 0.98)were
observed when a positive diagnosis was based onthe presence of
cavitation. Lower kappa values (0.80 and0.86) were observed when a
positive diagnosis was basedon the presence of an active lesion. In
all the analyses theintra-examiner agreement had slightly higher
values thanthe interexaminer agreement.Among the 6,400 tooth
surfaces examined, disagree-
ments between examiners were observed in 242 (3.8%)cases. Most
of these disagreements (65.3%; 158/242)concerned the dierentiation
between sound surfaces andnon-cavitated lesions, representing 2.5%
(158/6,400) ofall tooth surfaces. From the total number of
disagree-ments, 33.5% (81/242) were related to the
dierentiationbetween sound surfaces and inactive
non-cavitatedlesions, representing 1.3% (81/6,400) of all tooth
sur-faces; 26.0% (63/242) concerned disagreement between
Table 1
Percentage agreement, kappa coecient values, and respective 95%
CIs for interexaminer (V.S. M.S. 1st) and intra-examiner(M.S. 1st
M.S. 2nd) examinations considering all codes and four diagnostic
thresholds (n = 6,400 tooth surfaces)
Interexaminer(V.S. M.S. 1st)
Intra-examiner(M.S. 1st M.S. 2nd)
Nyvad criteria Percentage agreement = 96 Percentage agreement =
97(codes 09) j = 0.76 j = 0.83Diagnostic thresholds ) + ) +1. Sound
vs. diseased (n) ) 5794 91 5813 58
+ 77 438 74 455Percentage agreement (95% CI) 97 (9798) 98
(9798)Kappa (CI) 0.82 (0.800.85) 0.86 (0.840.86)
2. Sound or inactive lesions vs. active lesions (n) ) 6020 76
6031 35+ 46 258 53 281
Percentage agreement (95% CI) 98 (9798) 99 (9899)Kappa (95% CI)
0.80 (0.760.83) 0.86 (0.830.89)
3. Intact surface vs. surface discontinuity (n) ) 6090 35 6096
12+ 18 257 21 271
Percentage agreement (95% CI) 99 (9899) 99 (9999)Kappa (95% CI)
0.90 (0.880.93) 0.94 (0.920.96)
4. Sound or non-cavitated lesion vs. cavitated lesion (n) ) 6192
9 6198 5+ 11 188 3 194
Percentage agreement (95% CI) 99 (9999) 99 (9999)Kappa (95% CI)
0.95 (0.920.97) 0.98 (0.960.99)
Code 0, sound surfaces; code 1, active non-cavitated lesions;
code 2, active enamel discontinuity; code 3, active cavitated
lesions; code4, inactive non-cavitated lesions; code 5, inactive
enamel discontinuity; code 6, inactive cavitated lesion; code 7,
lling; code 8, llingassociated with an active lesion; code 9, lling
associated with an inactive lesion; +, positive diagnoses; ),
negative diagnoses.
Caries assessment in primary teeth 227
-
sound surfaces and active non-cavitated lesions, repre-senting
0.9% (63/6,400) of all tooth surfaces; and 5.8%(14/242) concerned
disagreement between active non-cavitated lesions and inactive
non-cavitated lesions,representing 0.2% (14/6,400) of all tooth
surfaces. Theremaining disagreements (34.7%; 84/242) were related
toother combinations. The cross-tabulation showing theinterexaminer
agreement is available as supportinginformation (Table
S1).Disagreements in intra-examiner examinations were
observed in 171 (2.7%) of the 6,400 tooth surfaces andthe
majority (70.7%; 121/171) were again related to thedierentiation
between sound surfaces and non-cavitatedlesions. The
cross-tabulation showing the intra-examineragreement is available
as supporting information(Table S2).Comparison between examinations
was also made
based on caries prevalence (Table 2) and dfs count(Table 3),
which are variables at the individual level.Considering the
presence of at least one surface withcaries (codes 19) or with
cavitated lesions (scores 3, 6, or8), the percentage agreement on
caries prevalence washigh, ranging from 93.8% to 98.7% with
correspondingkappa values ranging from 0.84 to 0.97. The
lowestagreement was observed when caries diagnosis at theindividual
level was based on the presence of at least onesurface with an
active lesion (codes 1, 2, 3, or 8). In thiscase, the interexaminer
percentage agreement was 85%(j = 0.69) and the intra-examiner
percentage agreementwas 87.5% (j = 0.74).Table 3 shows the mean dfs
(i.e. the number of tooth
surfaces aected by caries per subject) for both examin-
ers according to three diagnostic thresholds. In no situ-ation
was the mean dfs statistically signicantly dierentamong
examinations. Table 4 shows the data related tothe analysis of the
interexaminer and intra-examineragreement on dfs counts. The mean
dfs dierencebetween examinations was below 1 in all
situations,indicating a high level of agreement for the three
diag-nostic thresholds. The limits of agreement denote theinterval
which holds 95% of the dierence: the smallerthe range between the
limits, the higher the agreement.The narrowest interval was
observed when the diagnosticthreshold was set at the cavity level
(from )0.72 to 0.67surfaces for intra-examiner analysis, and from
)1.40 to1.60 surfaces for interexaminer analysis), indicating
veryhigh agreement. The wider interval (from )4.90 to 4.60surfaces)
was seen for interexaminer agreement when alltypes of lesions were
included in the dfs counts. Whenonly active caries lesions were
included in the dfs counts,the limits of agreement ranged from
)3.90 to 3.20surfaces for interexaminer analysis and from )3.20
to3.60 surfaces for intra-examiner analysis.The mean examination
time was 226.5 s (SD =
128.5 s) and was not inuenced by the childrens age,whereas it
was inuenced by their caries experience(Table 5).
Discussion
This study assessed the interexaminer and
intra-examineragreement on caries diagnosis in primary teeth using
theNyvad classication system. Usually, agreement in caries
Table 2
Interexaminer (V.S. M.S. 1st) and intra-examiner (M.S. 1st M.S.
2nd) reliability in the assessment of caries prevalence(percentage
of children with caries) according to three diagnostic thresholds
(n = 80 subjects)
Diagnostic thresholds
Interexaminer estimate Intra-examiner estimate
V.S.M.S.1st Agreement j
M.S.1st
M.S.2nd Agreement j
At least one surface aected by caries (codes 19) 72.5 73.8 93.8
0.84 73.8 73.8 97.5 0.94At least one surface with active caries
lesions (codes 1, 2, 3, or 8) 58.8 61.3 85.0 0.69 61.3 61.3 87.5
0.74At least one surface with cavitated caries lesions (codes 3, 6,
or 8) 40.0 37.5 97.5 0.95 37.5 38.8 98.7 0.97
Code 0, sound surfaces; code 1, active non-cavitated lesions;
code 2, active enamel discontinuity; code 3, active cavitated
lesions; code4, inactive non-cavitated lesions; code 5, inactive
enamel discontinuity; code 6, inactive cavitated lesion; code 7,
lling; code 8, llingassociated with an active lesion; code 9, lling
associated with an inactive lesion.
Table 3
Mean decayed or lled surface (dfs) and SD for examiners V.S. and
M.S (1st and 2nd examinations) according to three
diagnosticthresholds (n = 80 children)
Diagnostic thresholds
Mean dfs (SD)
V.S. M.S. 1st M.S. 2nd
Tooth surfaces aected by caries (codes 19) 6.59 (8.57) 6.71
(8.44) 6.53 (8.33)Tooth surfaces with active lesions (codes 1, 2,
3, or 8) 3.80 (5.85) 4.18 (5.99) 3.95 (5.86)Tooth surfaces with
cavitated lesions (codes 3, 6, or 8) 2.55 (4.63) 2.46 (5.53) 2.49
(4.53)
Code 0, sound surfaces; code 1, active non-cavitated lesions;
code 2, active enamel discontinuity; code 3, active cavitated
lesions; code4, inactive non-cavitated lesions; code 5, inactive
enamel discontinuity; code 6, inactive cavitated lesion; code 7,
lling; code 8, llingassociated with an active lesion; code 9, lling
associated with an inactive lesion.
228 Sellos & Soviero
-
diagnosis is analyzed at the tooth surface level whencodes are
assigned to each surface. Although this type ofanalysis is
important to identify how reproducible themethod is, it does not
show the impact of agreement levelon epidemiological data.No two
examiners, and not even the same examiner,
are expected to agree completely or give identical resultsin
repeated examinations. However, it is most importantto know whether
this disagreement could cause problemsin clinical practice (i.e.
cause the clinician to choose aninappropriate treatment, or bring
about a misleadingconclusion to a clinical study) (26).The high
reproducibility of the Nyvad caries classi-
cation system in the present study was in accordancewith results
from studies carried out on permanent teethin young individuals (8,
24). As also observed in previousstudies (8), disagreements were
concentrated on thedierentiation between sound surfaces (code 0)
andnon-cavitated lesions (codes 1 and 4). Therefore,non-cavitated
stages still represent the major problem inclinical
diagnosis.Despite its common usage, the Cohen kappa coe-
cient is not always the most suitable indicator forassessing
agreement. It was originally proposed to mea-sure agreement between
two examiners when subjects areclassied into two nominal
categories. The extension ofits application to multicategory data
may result in mis-
leading interpretations. When kappa is used for multi-category
data, the categories should be grouped tobecome dichotomies. Even
so, kappa values can behighly inuenced by the way in which
multicategoryclassications are grouped. (27)A more comprehensive
analysis should also focus on
the disagreements and their possible impact on the -nal
outcomes. Thereby, it would provide a betterunderstanding of the
diculties related to each level ofdiagnosis and allow for a more
profound comparisonbetween studies. A detailed analysis of
disagreementsmay identify some of their eects on clinical
researchand practice. In the present study, most of the
dis-agreements were between sound surfaces (code 0)
andnon-cavitated lesions (codes 1 and 4). In the case ofinactive
lesions, this would not result in any over-treatment in a clinical
situation, because neither soundsurfaces nor inactive lesions
require any intervention.This disagreement has often been related
to stainedssures on occlusal surfaces. In the case of active
le-sions, it could be a relevant disagreement in terms ofthe
clinical practice as it could change the treatmentdecision.
Although total agreement is not expected,disagreements must be
avoided as much as possible. Itis important to reinforce that
improvement in agree-ment is highly related to the quality of
training andexperience of the examiners (8, 10, 22, 23).
Table 5
Mean examination time in seconds (s) according to age and number
of aected tooth surfaces
n Mean time (s) SD Min. Max.
Age*3650 months 24 203.29a 136.17 47 6015170 months 29 224.17b
134.75 54 586Older than 71 months 27 249.74c 114.78 66 525
Number of aected tooth surfaces**0 22 106.64a 45.57 47 22616 29
191.72b 58.38 74 313 7 29 352.31c 112.74 178 601
Max., longest examination time; Min., shortest examination
time.*MannWhitney U-test (a b; a c; b c: P > 0.05).**MannWhitney
U-test (a b; a c: P < 0.01); (b c: P = 0.01).
Table 4
Interexaminer (V.S. M.S. 1st) and intra-examiner (M.S. 1st M.S.
2nd) agreement in the assessment of number of tooth surfacesaected
by caries per subject [decayed or lled surface (dfs)] according to
three dierent thresholds (n = 80 subjects)
Diagnostic thresholds Examiners
Mean dfsdierenceper subject
Limits ofagreement
Range of the dfsdierences betweenthe two examinations
Surfaces aected by caries (codes 19) V.S. M.S. 1st )0.13 [)4.90;
4.60] [)6; 14]M.S. 1st M.S. 2nd 0.20 [)3.50; 3.90] [)9; 6]
Surfaces with active lesions (codes 1, 2, 3, or 8) V.S. M.S. 1st
)0.40 [)3.90; 3.20] [)8; 6]M.S. 1st M.S. 2nd 0.22 [)3.20; 3.60]
[)10; 6]
Surfaces with cavitated lesions (codes 3, 6, or 8) V.S. M.S. 1st
0.03 [)1.01; 1.06] [)2; 5]M.S. 1st M.S. 2nd )0.03 [)0.72; 0.67]
[)2; 1]
Code 0, sound surfaces; code 1, active non-cavitated lesions;
code 2, active enamel discontinuity; code 3, active cavitated
lesions; code4, inactive non-cavitated lesions; code 5, inactive
enamel discontinuity; code 6, inactive cavitated lesion; code 7,
lling; code 8, llingassociated with an active lesion; code 9, lling
associated with an inactive lesion.
Caries assessment in primary teeth 229
-
For numerical variables, such as dfs counts, the Bland&
Altman method (26) is considered an appropriatemethod with which to
assess agreement between repeatedmeasurements: the narrower the
interval, the higher theagreement between measurements. As
expected, thenarrowest interval of agreement was found to be
whenthe cut-o point was set at cavitated lesions. However,for the
other two cut-o points, considering all codes oronly active
lesions, the limits of agreements were notexcessively wide and the
nal mean dfs count did notdier signicantly between examiners or
within anexaminer (Tables 4 and 5). These results encourage theuse
of more comprehensive assessment of carious lesionsin clinical
studies.In our opinion, the main advantage of the Nyvad caries
classication system is the ability to assess the
progressionstage and activity of the lesions simultaneously, using
avery straightforward code system. In addition, thedierentiation
between enamel discontinuity and a dentincavity provides important
information for monitoringcaries progression. The theoretical
underpinning of theNyvad caries classication system is to provide a
dis-cernible link between the diagnosis and the best
treatmentoption.Although dental biolm has to be removed from
the
tooth surfaces to allow proper visualization of earlycarious
lesions, professional cleaning of the teeth is notrecommended
before examination using the Nyvad sys-tem. Most of the biolm is
usually removed duringtoothbrushing, and only those surfaces where
the patientdoes not usually clean eectively will remain covered
bybiolm. In the present study, children were assisted bythe
examiner during toothbrushing because they werevery young.When
visual examination combining surface features
(opacity, roughness, colour, and location of the lesion) isnot
enough to classify activity, tactile examination usinga probe is
recommended (8). For a proper understandingof the surface texture,
the probe must be sharp.However, the intention is not to test
whether the probecatches irregularities on the enamel, but rather
to feelthe texture or the consistency of the lesion. For
enamellesions, the tip of the probe must be placed at an angle
ofabout 30 to the tooth surface and be moved gentlyacross the
lesion, so that the dierence between thesmooth texture of a sound
surface or inactive lesion andthe rough texture of an active lesion
can be felt. Fordentin lesions, tactile examination, using slight
pressure,dierentiates hard tissue from soft tissue or a
leatheryconsistency. In fact, surface texture has been consideredas
a better indicator of activity than colour (7, 20). Thatis why
activity assessment may not be based only on thecolour of the
lesion, especially for dentin lesions. Manydark-brown dentin
lesions have a leathery consistency,indicating that they are still
active. As the transitionbetween active and inactive stages does
not occurinstantaneously, mixed lesions must be considered
asactive. We believe that all these considerations onactivity
assessment were of great importance for the highlevels of agreement
achieved on activity assessment in thepresent study. Disagreement
on the dierentiation
between active and inactive lesions was very
infrequent,indicating a good reproducibility of activity
assessmentwhen a consensus on the presence of the lesion
wasreached.For proper detection of non-cavitated lesions, tooth
surfaces must be dried and visualized under goodillumination.
The requirement of compressed air andarticial light is therefore a
prerequisite for the Nyvadcaries classication system, as well as
for other cariesclassication systems that aim to detect initial
cariouslesions; otherwise, non-cavitated lesions are
underesti-mated.The mean examination time is not frequently
men-
tioned in reliability studies in the literature. In thepresent
study, the mean time needed for the examina-tion was less than
expected. The average examinationtime for each child was 3 min and
46 s. In a previousstudy, with older children and adolescents, the
exami-nation time was estimated to be between 5 and 8 min(8). This
dierence was probably because more toothsurfaces are present in
mixed or permanent dentitionscompared with the primary dentition.
We expected thatyounger children would need more time for
examina-tion because it is often more dicult to control
theirbehaviour in the dental chair. However, age did notinuence
examination time. Probably, behaviour con-trol was not a problem in
the present study becauseboth examiners were specialized in
paediatric dentistry.On the other hand, the more the tooth surfaces
wereaected by caries the longer the examination took be-cause, if a
tooth surface was not sound, examinersneeded additional time to
reect and assign a code tothat surface.This present study concludes
that the Nyvad caries
classication system showed a high level of agreementand suitable
examination time, and may be consideredreliable for dental caries
clinical studies in primary teeth.More studies on the reliability
of the system should beperformed with larger samples and in
populations withdierent rates of caries prevalence to conrm
thesendings.
Acknowledgements We gratefully acknowledge Professors BenteNyvad
(Denmark) and Vita Machiulskiene (Lithuania) for their
generous introduction to the clinical use of the criteria, Prof.
Vibeke
Baelum (Denmark) for her relevant suggestions on statistical
analysis and Soraya Leal (Brazil) for her contribution to the
nal
version of this manuscript.
References1. Baelum V, Heidmann J, Nyvad B. Dental caries
paradigms in
diagnosis and diagnostic research. Eur J Oral Sci 2006;
114:263277.
2. Ismail AI. Clinical diagnosis of precavitated carious
lesions.Community Dent Oral Epidemiol 1997; 25: 1323.
3. Nyvad B. Diagnosis versus detection of caries. Caries Res
2004;38: 192198.
4. Pitts NB. ICDAS an international system for cariesdetection
and assessment being developed to facilitate cariesepidemiology,
research and appropriate clinical management.Community Dent Health
2004; 21: 193198.
230 Sellos & Soviero
-
5. Ismail AI. Visual and visuo-tactile detection of dental
caries.J Dent Res 2004; 83: C56C66.
6. Thylstrup A, Bruun C, Holmen L. In vivo caries models
mechanisms for caries initiation and arrestment. Adv Dent Res1994;
8: 144157.
7. Nyvad B, Fejerskov O. Assessing the stage of caries
lesionactivity on the basis of clinical and microbiological
examina-tion. Community Dent Oral Epidemiol 1997; 25: 6975.
8. Nyvad B, Machiulskine V, Baelum V. Reliability of a newcaries
diagnostic system differentiating between active andinactive caries
lesions. Caries Res 1999; 33: 252260.
9. Machiulskine V, Nyvad B, Baelum V. A comparison ofclinical
and radiographic caries diagnoses in posterior teeth of12yearold
Lithuanian children. Caries Res 1999; 33: 340348.
10. Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H,Pitts
NB. The International Caries Detection and AssessmentSystem
(ICDAS): an integrated system for measuring dentalcaries. Community
Dent Oral Epidemiol 2007; 35: 170178.
11. Lima TJ, Ribeiro CC, Tenuta LM, Cury JA.
Low-fluoridedentifrice and caries lesion control in children with
differentcaries experience: a randomized clinical trial. Caries Res
2008;42: 4650.
12. Assaf AV, Meneghim MC, Zanin L, Mialhe FL, PereiraAC,
Ambrosano GMB. Assessment of different methods fordiagnosing dental
caries in epidemiological surveys. CommunityDent Oral Epidemiol
2004; 32: 418425.
13. Parfitt GJ. A standard clinical examination of the teeth.Br
Dent J 1954; 96: 296300.
14. Backer-Dirks O. Longitudinal dental caries study in
children915 years of age. Arch Oral Biol 1961; 6: 94108.
15. Pitts NB, Fyffe HE. The effect of varying diagnostic
thresh-olds upon clinical caries data for a low prevalence group. J
DentRes 1988; 67: 592596.
16. Neilson A, Pitts NB. The clinical behaviour of free
smoothsurface carious lesions monitored over 2 years in a group
ofScottish children. Br Dent J 1991; 171: 313318.
17. Pitts NB. Diagnostic tools and measurements impact
onappropriate care. Community Dent Oral Epidemiol 1997; 25:
2435.
18. EkstrandKR, Ricketts DNJ, Kidd EAM, Qvist V, Schou
S.Detection, diagnosing, monitoring and logical treatment
ofocclusal caries in relation to lesion activity and severity: an
invivo examination with histological validation. Caries Res
1998;32: 247254.
19. WHO. Oral Health Surveys: basic methods, 4 edn. Geneva:WHO,
1997.
20. Holmen L, Thylstrup A, Artun J. Clinical and
histologicalfeatures observed during arrestment of active enamel
cariouslesions in vivo. Caries Res 1987; 21: 546554.
21. Ekstrand KR, Martignon S, Ricketts DJN, Qvist V.Detection
and activity assessment of primary coronal carieslesions: a
methodologic study. Oper Dent 2007; 32: 225235.
22. Nyvad B, Machiulskine V, Baelum V. Construct and pre-dictive
validity of clinical caries diagnostic criteria assessinglesion
activity. J Dent Res 2003; 82: 117122.
23. Gonzalez MC, Ruz JA, Fajardo MC, Gomez AD, MorenoCS, Ochoa
MJ, Rojas LM. Comparison of the def index withNyvads caries
diagnostic criteria in 3-and 4-year-old Colom-bian children.
Pediatr Dent 2003; 25: 132136.
24. Machiulskine V, Baelum V, Fejerskov O, Nyvad B. Preva-lence
and extent of dental caries, dental fluorosis, and devel-opmental
enamel defects in Lithuanian teenage populationswith different
fluoride exposures. Eur J Oral Sci 2009; 117: 154160.
25. Machiulskine V, Nyvad B, Baelum V. Prevalence andseverity of
dental caries in 12-year-old children in Kaunas,Lithuania 1995.
Caries Res 1998; 32: 175180.
26. Bland JM, Altman DG. Statistical methods for
assessingagreement between two methods of clinical
measurement.Lancet 1986; 327: 307310.
27. Maclure M, Willett WC. Misinterpretation and misuse ofthe
kappa statistic. Am J Epidemiol 1987; 126: 161169.
Supporting informationAdditional Supporting Information may be
found in the onlineversion of this article:
Table S1. Distribution of diagnoses at the inter-examiner
examin-ations based on Nyvad criteria.
Table S2. Distribution of diagnoses at the intra-examiner
examin-ations based on Nyvad criteria.
Please note: Wiley-Blackwell is not responsible for the content
orfunctionality of any supporting materials supplied by the
authors.Any queries (other than missing material) should be
directed to thecorresponding author for the article.
Caries assessment in primary teeth 231
-
This document is a scanned copy of a printed document. No
warranty is given about the accuracy of the copy.Users should refer
to the original published version of the material.