Embed Size (px)
Citation preview
Ramsey County
Comprehensive Family Assessment Guide For
Workers

1
Table of Contents
Background and Overview ....................................................................................................... 2
Evidence Based Practices ......................................................................................................... 2
Strength Focused Practice ....................................................................................................... 2
Stage One: Review Existing Information and the Transfer Meeting ....................................... 5
Stage Two: Engaging with the Family/Developing of a Comprehensive Family Functional Assessment ............................................................................................................................. 8
Stage Three: Development of Case Plan, Family Team Meetings and Intentional Visitation Practices ................................................................................................................................ 15
Stage Four Ongoing Assessment ............................................................................................ 23
Stage Five: Case Closure ....................................................................................................... 26
References ............................................................................................................................ 28
Documentation ..................................................................................................................... 29
Appendix ............................................................................................................................... 30
Active Listening ....................................................................................................................................................... 31
Stages of Change ..................................................................................................................................................... 31
Transfer Guide for Communications Between Intake and Ongoing ....................................................................... 33
Possible Questions To Engage Caregivers During the Functional Assessment Process .......................................... 34
Eco Mapping of Connections .................................................................................................................................. 44
2
Background and Overview
The Ramsey County Community Human Services Department is implementing a new model of Comprehensive Family Functional Assessment (CFA) for Child Protection Services. The University of Minnesota partnered with Ramsey County on the evaluation of this practice approach.
The intent of this new practice approach is to enhance caseworker’s skills in understanding the family functioning that contributes to children being unsafe or at risk and designing a case plan that has optimal chance at successfully changing behaviors.
This practice approach was developed based on the following foundations of quality practice:
• Engagement and relationship‐building • Involvement of families and youth in identifying their own needs and strengths • Cultural grounding • Family is a system • Identifying and including extended family and service providers • Individually tailored approach for families • All children are individualized • Empathy, authenticity, and transparency
Evidence Based Practices
This document articulates the need for child protection systems to adopt evidence based practices in its system reform and practice improvement efforts. Two specific evidence based practices are critical to the implementation of this practice approach.
Strength Focused Practice
Research from a variety of settings emphasize that families do better in changing behaviors that caused children to be unsafe and maintaining those changes when the efforts of the various people involved in their life are focused on building on the strengths and protective capacities that already exist within the family. Barry Duncan’s research emphasized that 55% of actual long term change stems from starting from the place where people already feel successful.1 This practice model builds on learning what families are already doing well in order to learn how to help them make changes in their day to day functioning.
1 Duncan, Barry. (1999). Heart and Soul of Change. APA Press.
3
Critical Thinking and Analysis
Critical thinking is the intellectually disciplined process of actively and skillfully conceptualizing, applying, analyzing, synthesizing, and/or evaluating information gather from, or generated by, observation, experience, reflection, reasoning, or communication, as a guide to belief and action.2 A well cultivated critical thinker:
• Raises vital questions and problems, formulating them clearly and precisely;
• Gathers and assesses relevant information, using abstract ideas to interpret it effectively, comes to well‐reasoned conclusions and solutions, testing them against relevant criteria and standards;
• Thinks open‐mindedly within alternative systems of thought, recognizing and assessing, as need be, their assumptions, implications, and practical consequences; and
• Communicates effectively with others in figuring out solutions to complex problems.
When a social worker implements an approach to critical thinking and analysis the research teaches us the following occurs:
• There is an increase accuracy of decisions
• They avoid cognitive biases
• They recognize errors and mistakes as learning opportunities
• They more accurately assess likelihood of attaining hoped‐for outcomes
• They make valuable contributions at case conferences
• The develop effective plans
• They respect and have empathy for others
• They continue to learn and enhance their skills
This Guide discusses a ten step process (divided into five stages) for this practice approach.
2 Michael Scriven & Richard Paul. (February 2005). National Council for Excellence in Critical Thinking Instructions.
4
Ten Steps of a Comprehensive Family Functional Assessment
Stage I: Transfer Communication and Information Review
1) Workers will review existing documentation and engage in a transfer communication with the intake worker.
Stage 2: Conducting a Comprehensive Family Functional Assessment
2) Following this review, workers will meet with the family and begin the engagement process that will ensure the family’s meaningful involvement throughout the case.
3) Workers will interview children, parents, and other relevant caregivers with special attention paid to the inclusion of fathers.
4) Workers will then meet with families and possibly staff from other relevant agencies to coordinate case planning and create a plan for future communication.
5) Specialized assessments (e.g. to address mental health concerns) will be carried out or appropriate referral made for assessment elsewhere.
Stage 3: Behaviorally Based Case Plan Development
6) Workers will use clinical judgment in consultation with supervisors and families to develop case plans including intentional visitation practices.
7) Workers will document all relevant case information in a timely manner.
Stage 4: Ongoing (Continuous Assessment)
8) Workers will conduct ongoing assessments of progress and needs.
9) Workers will exchange information with family members, service providers, and courts, updating service plans regularly.
Stage 5: Case Closure
10) Workers will reassess safety issues and child risks of the entire family prior to case closure.
5
Stage One: Review Existing Information and the Transfer Meeting
Overview The review of pertinent case documentation prior to meeting with the family is essential. It has several purposes:
• Ongoing workers will better understand client’s situation—and fully understand the threats of safety.
• Ongoing worker will understand if this family has been involved in the system previously which should heighten the seriousness of the potential for child maltreatment.
• Clients will not have to repeat information and will feel that what they have said previously has been heard and remembered
• More efficient use of time
• Informs worker that there are concrete needs that likely will need to be dealt with immediately
• Allows worker to prepare internally for the issues they will be confronting
The following documents should be reviewed prior to the Child Protection Worker making the initial contact:
Case With No Previous Child Protection Case Management
• The abuse and/or neglect report that necessitated the investigation
• The investigation summary including the specific safety threats identified and the safety plan that is in place to control or manage the safety threats
• Any collateral reports related to the investigation, i.e., police, medical, school reports
Case With Previous Child Protection Case Management
• Add to documents above: Intake reports, Intake summaries, closing summaries
• Review: o Safety threats identified in the past o Safety plan put in place and whether or not they were effective at controlling
or managing safety threats o What interventions and services were tried in the past and which were most
successful in changing behaviors that caused children to be unsafe

o Court history o Level of family’s cooperation
Transfer Meetings Between Intake and Ongoing Staff
See Transfer Guide in Appendix Talk with investigative worker and ask them to:
• Describe the specific safety threats identified in the safety assessment.
• Describe the behaviors or conditions of caregivers that contributed to the children being unsafe or at risk.
• Describe the safety plan that was put in place (in home or out of home). If the safety plan is an in‐home plan, define how the safety plan is controlling or managing the safety threats.
• Describe any safety threats to the worker that may exist.
Examples of family functioning that might contribute to child safety threats might include physical and mental health issues, developmental disabilities, domestic violence, and chemical dependency. The ongoing worker will be expected to compile additional information in these areas during the Comprehensive Family Functional Assessment.
BEST PRACTICE TIPS
• Ensure that you fully understand the safety threats that caused children to be unsafe…”substance abuse” is not a safety threat—how it gets acted out in parenting (or lack thereof) is the safety threat.
• Family’s history with CP—even if they were not “substantiated” what has been the family’s involvement in CP or other systems (such as Domestic Violence, etc.)
• Make sure you learn who else might have additional family information (i.e. community providers that have supported the family previously, kin who were identified but not contacted, etc.)
• Safety threats specific to each child –learn what these safety threats actually look like on a day to day basis.
6
During the review of the case documentation worker will identify any known aspects of family functioning that have contributed to child safety threats.
7
• Level of family engagement with the system and if they were deemed to be “resistant” what that looked like. Sometimes resistant is just another word for fear.
• Learn about the protective capacities of the family and how they are being used to keep children safe (specific to an in‐home safety plan).
• Learn about the natural supports (relatives and kin) as opposed to “artificial supports (community centers, agencies, etc.)
Stage Two: Engaging with the Family/Developing of a Comprehensive Family Functional Assessment
Overview
Talk with parents about strengths/protective factors, resources and needs and assess readiness to use help and make change (see “Stages of Change” in Appendix). The family should be encouraged to engage in self‐assessment about what they believe is happening and why they are now involved with the agency. Be aware and mindful of possible cultural factors. If appropriate, ask about cultural context of family issues. Workers may use the Signs of Safety (SOS) worksheet. Add to the SOS worksheet after meeting with children, review of records, discussion with providers, and extended support system.
In the first meeting with family the worker meets with family, builds rapport and engagement and demonstrates unconditional positive regard (be open and non‐judgmental). It is important to note that MN research on Alternative Response suggests that there is a direct correlation between family engagement and child safety.
Focus Areas in the Comprehensive Functional Assessment Process
Workers must always begin by explaining their role, their commitment to helping the family, their understanding of the safety threats and risks that were identified in the investigative process.
This is the opportunity for the worker to align themselves with the family in the process of working to change behaviors or conditions that caused children to be unsafe. Through a process over several meetings compile information about family functioning in the following key domain areas:
• Parenting/bonding/including history of how parents were cared for/parented • Living conditions/finances/housing food /basic needs and any immediate situatons
which may present as an emergency such as no utilities, unable to pay rent or mortgage.
• Kinship/neighbor care options– family connections–support system
• Caregivers mental health
8
A man should look for what is, and not for what he thinks should be.
Albert Einstein
• Domestic violence • Parents health
• Parent substance Use
For each child in the family:
• Child mental health/substance abuse
• Child health
• Child's developmental educational needs
See Possible Questions to Engage Caregivers in the Appendix
The focus of the Comprehensive Family Functional Assessment is to assess the underlying causal factors for behaviors and conditions affecting children such as family history, domestic
violence, substance abuse, mental health, chronic health problems, and poverty.
In a Comprehensive Family Functional Assessment, the family’s strengths and protective factors are also evaluated to identify resources that can support the family’s ability to meet its needs and better protect the children. The Comprehensive Family Functional Assessment incorporates information collected through the assessment of safety and integrates the information into a behaviorally focused individualized case plan.
Time perspective is needed in comprehensive family assessment—what led to the current problems as well as the likely impact of both the maltreatment and the response on the child and family.
A comprehensive assessment of family functioning completed early in the process of serving a family, increases the likelihood of that the services utilized will be targeted on addressing the issues that caused children to be unsafe.
9
The Comprehensive
Family Functional
Assessment seeks to
understand history and its
impact on future child
safety. It involves
recognizing patterns of
parental behavior over
time that have
contributed to children
b f
About Protective Capacities
Protective capacity is a CPS concept that has been around for a long time but just got this label within the past few years. Fundamentally, the concept is concerned with the question of whether a parent can and will protect his or her child. The concept of protective capacity is a powerful one for all of CPS – both safety intervention and remedial treatment. For this month, we’ll stay focused on the relevance to safety intervention. What is Protective Capacity? A protective capacity is a specific quality that can be observed and understood to be part of the way a parent thinks, feels and acts that makes him or her protective. Here’s a definition for caregiver protective capacities:
Personal and parenting behavioral, cognitive and emotional characteristics that specifically and directly can be associated with being protective of one’s young. These are unique strengths that contribute to being protective. Some might think of these characteristics as somewhere close to an instinct for protectiveness similar to a mother bear’s protective nature particularly with regard to priority and intensity. 3 Cognitive Protective Capacity
This refers to specific intellectual, knowledge, understanding and perceptions that contribute to protective vigilance. Here are some examples of cognitive characteristics:
• Accurate perception of a child
• Recognition of a child’s needs
• Understanding protective role
• Intellectually able
• Understands and recognizes threats
10
3 Action for Child Protection. 2003
This process of going from information to judgments is critical.
There is no ready “prescription” for
how these judgments are made; we must train staff to make
these essential judgments.
11
Emotional Protective Capacity This refers to specific feelings, attitudes and identification with the child and motivation that result in parenting and protective vigilance. Here are some examples of emotional characteristics:
• Emotional bond with the child
• Positive attachment with the child
• Love, sensitivity and empathy for the child
• Stability and emotional control
• Effectively meets own emotional needs
Behavioral Protective Capacity
This refers to specific action, activity and performance that is consistent with and results in parenting and protective vigilance. Here are some examples of behavioral characteristics:
• Physical capacity and energy
• Ability to set aside own needs
• Adaptive
• Assertive and responsive
• Takes action
• Impulse control
• History of being protective
BEST PRACTICE TIPS
Conducting an assessment is really an art form as much as it is a science. Assessment generates experience that as it unfolds either enhances or hinders the quality of the information provided by families as well as the success of the interventions.
The questions in the back of this document really provide an array of ways to engage the family in quality conversations that generate trust and real partnership. Most families are fearful of our involvement in their lives –and understandably so. Think of the power that we have in their eyes. We can choose to use that power for good or not. The better the assessment, the better our ability to make a real difference in family's lives.

12
Also, when trying to make a distinction between a protective capacity and a strength, consider the characteristics of a protective capacity:
• A protective capacity is “Action Oriented”
• A protective capacity is something that the family can demonstrate has occurred in the past that has been effective in protecting children—not a promise of something to be done in the future.
• A protective capacity relies on a caregiver recognizing the need to protect.
During the assessment phase the worker will interview parents, children and key players –information will be enhanced over a series of interactions.
Get to know and build relationships with individual family members and “key players” keeping in mind the safety needs of the individual in regard to where and how the interviews will take place.
Ecomaps/genograms may be a helpful tool
See Ecomap To Maintain Connections tool in the Appendix
Meetings with children are opportunities to: o Gather information o Assess overall health, activity levels, development, communication skills, build
rapport o Ensure that children understand next steps and agency’s intent to help family o Explain court involvement, if pertinent, and what to expect in court hearings
Consult with relevant stakeholders involved with family
Talk with any relevant stakeholders. “Relevant” stakeholders include individuals involved in the child/family’s life who may provide additional insight/information about child/family functioning. They include family and kin, friends, neighbors, and providers. The purpose of these meetings is to gain a better understanding of the needs related to safety, permanency, and child well‐being; determine effective ways of engaging the family in changing behaviors; and identify what has been the impact of services provided. These conversations take place within a context of a shared understanding of the areas of common concern in working with families.
Talk with any providers active with the family to:
• Clarify the provider’s role
• Clarify what services are provided
• Clarify family’s needs
Consider whether specialized assessments are needed.
Remember that we must continue to learn each person’s “story” in order to best serve them.
When the worker’s observations indicate that there may be a need for specialized assessments (developmental, mental health, drugs, cognitive abilities of children or youth that may be affecting their education, specialized assessments related to handicapping conditions) the worker should:
• Consult with peers, supervisor and relevant stakeholders.
• Consider cultural appropriateness
• Focus the attention of the specialist on the specific areas of concern
• Have a sense of what effect the findings have on decision‐making in the case
• Incorporate the recommendations of the assessments into the service ‐plan These conversations are part of the process of engaging the family in participating in the services that promote the necessary changes. Particular attention should be paid to ongoing efforts to reach out to fathers who are not viewed as integral to the case by the mother. It would be helpful to include extended family members and people the parents/children view as supportive in this discussion.
Other agencies involved in serving the family, including tribal child welfare programs, also need to understand the comprehensive family functional assessment. Some of their interventions need to be coordinated with those of the child welfare agency to meet the needs of the family and to utilize existing protective factors to motivate family participation and effective use of service resources. In addition to the following Assessment of Child Functioning, per State of MN DHS requirements the worker will also:
13
• Offer developmental and mental health screening as needed

14
• Identify people who will be involved / resources (family, friends, providers, etc.) for case planning
• Get Release of Information when needed

Stage Three: Development of Case Plan, Family Team Meetings and Intentional Visitation Practices
The purpose of a comprehensive family functional assessment is to provide the information necessary to determine the functioning of the family and how it contributes to child safety, permanency and well being. Once the functioning of the family is understood, the family and the worker can partner to develop a case plan that has optimal chance at changing behaviors that caused children to be unsafe as well as contribute to the child’s overall well being.
The case plan should be completed only after analyzing all material the worker has collected with supervisory oversight and guidance and with the family’s involvement. The information gathered should be analyzed, and the results of the assessment should be linked to the development of the service plan. The case plan should reflect the “golden thread” that connects the planned services to the needs that have been identified.
When families have been active parts of an assessment process that identifies how the family functions that impacts child safety, family strengths and protective
capacities it is much easier to put that information to use in creating a service plan that really addresses what the family needs to safely care for their children. The least effective strategy in service planning is for the worker to develop a plan in the office and bring this plan to the families. This process communicates to the family that the worker “knows best” about what they need and minimizes the birth family’s control over their own destiny. It also negates the opportunity for the team members to actively participate in the planning. As in the process of assessment, service planning and service plan review are opportunities to build relationship and should not be short circuited.
Collecting and organizing comprehensive assessment information is not an end in itself; it must be used in focused ways in the service plan. The worker should ensure that the family members
15
Effective service planning that reduces safety threats and enhances child well being is a natural byproduct of a comprehensive assessment.
have an accurate understanding of why their situation was reported to child welfare and the specific behaviors or conditions have to change for their children to be safe.
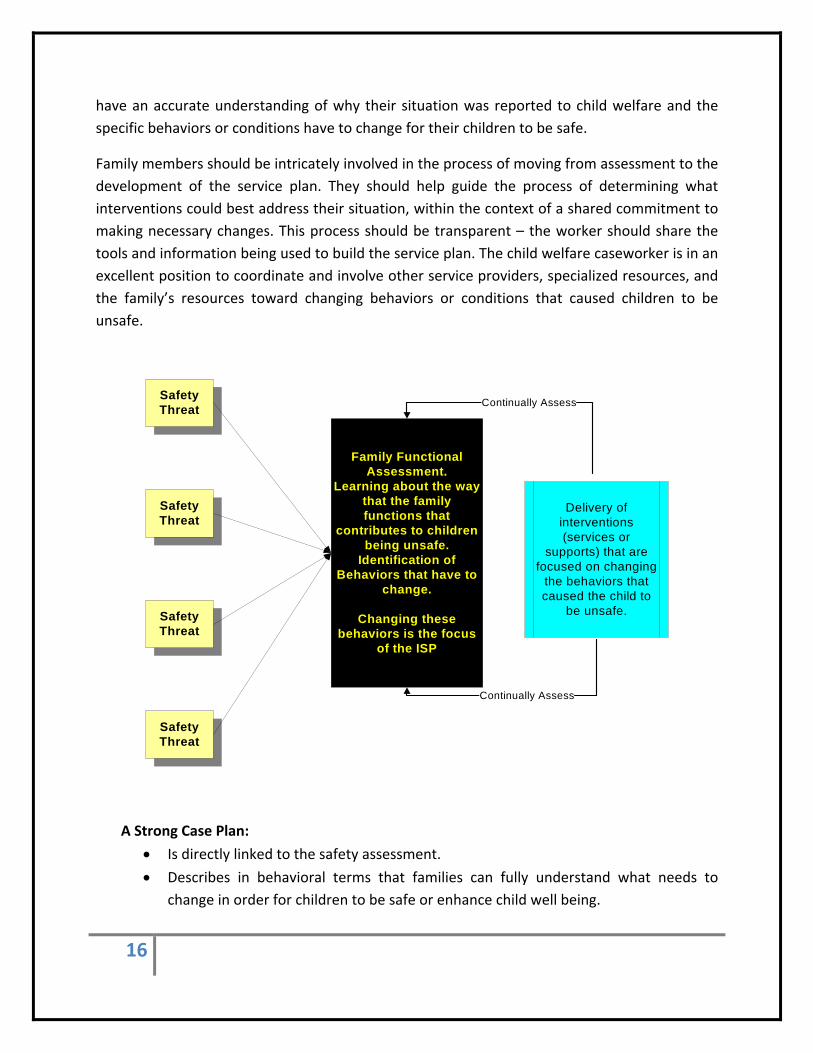
Family members should be intricately involved in the process of moving from assessment to the development of the service plan. They should help guide the process of determining what interventions could best address their situation, within the context of a shared commitment to making necessary changes. This process should be transparent – the worker should share the tools and information being used to build the service plan. The child welfare caseworker is in an excellent position to coordinate and involve other service providers, specialized resources, and the family’s resources toward changing behaviors or conditions that caused children to be unsafe.
Safety Threat
Safety Threat
Safety Threat
Safety Threat
Family Functional Assessment.
Learning about the way that the family functions that
contributes to children being unsafe.
Identification of Behaviors that have to
change.
Changing these behaviors is the focus
of the ISP
Delivery of interventions (services or
supports) that are focused on changing
the behaviors that caused the child to
be unsafe.
Continually Assess
Continually Assess
A Strong Case Plan:
• Is directly linked to the safety assessment.
16
• Describes in behavioral terms that families can fully understand what needs to change in order for children to be safe or enhance child well being.
• Identifies specific interventions and actions to address and facilitate the changes necessary for children to be safe
• Includes an ongoing assessment of how protective factors/capacities are supporting children in being safe.
• Includes family’s self‐identified strengths in the service planning process as a vehicle for motivate.
• Should be viewed by the family as achievable and realistic.
When Deciding What to Include in a Case Plan
There are times when we learn (either in the initial assessment of safety or in the assessment of family functioning) that the caregivers do not possess the capacities to safely care for their children. This may be due to the fact that the caregivers have significant cognitive limitations, mental illness that cannot be controlled through medication or therapy or physical disabilities that are impacting the day to day care of the child. When this is the case, our role moves from seeking to change behaviors that caused children to be unsafe and instead developing a “wrap” around the children to ensure their safety. This “wrap” may involve kin, community members, or an array of services. The chart on the following page provides a flow of the decision making process.
When developing a case plan with the family the worker must make judgments about:
• Based on their understanding of family functioning, determine if the behaviors or conditions that caused the children to be unsafe or at risk of future harm can actually change.
o If not, determine the most effective means to wrap supports around the children to ensure their safety as long as they are vulnerable.
o This requires an assessment of the protective capacity of those being asked to protect the children.
• How to prioritize services so that they address the areas of family functioning contributing to child safety issues.
• Which intervention will most effectively change the behaviors or conditions that caused children to be unsafe
• How to use family’s strengths as part of the planning process—motivating the family to change behaviors or conditions that caused children to be unsafe.
17
“People tend to support and be successful in directions that they themselves create.”

Conduct CFA identifying how the family functions that contribute to the child being unsafe or at risk
of harm
No
Yes
Is it likely that This area of functioning
will lead to harm of a child in the foreseeable
future? (RISK)
No Yes
Do Not Include In Case Plan
Identified Behaviors are Include in Case
Plan along with services to support behavior changes
Can This Functioning of the Family Be
Changed?
What are the behaviors And ways that the family
functions that need to change
NO
Identified supplemental
Services or supports included in Case
Plan
What are the family circumstances that
need to be supplemented
Has the functioning of the parents in this arealed to maltreatment in the
past? Review Safety Assessment
18
19
When Making Referrals to Community Providers The Worker Must:
Share safety threats or risks that exist. Share the specific behaviors or conditions that have to change to remove safety threats and reduce risks.
Be specific about the kinds of information to be included in the reports
BEST PRACTICE TIPS
Workers need to make detailed referrals to community partners that focus their efforts. As challenging as this may be, in the absence of this kind of specific direction we may not get the support that we need from providers to change the behaviors of caregivers that caused children to be unsafe or at risk.
This requires enhanced focus and clarity in the referral process.
Family Team Meetings as Part of the Case Planning Process
Conducting a family meeting with the parents, children, and identified providers, family and friends can assist the worker and family in designing a case plan that has optimal change of success and is supported by individuals who care about the child and their family.
Honoring Culture, Race and Ethnicity
One of the benefits of Family Meetings is the ability they provide to learn about the cultural, racial and ethnic background of the family and how their background impacts parenting decisions.
Culture includes race, religion, ethnicity, family values, lifestyle, family composition, customs, values and beliefs. The family itself is the most important source of information about its unique characteristics, historical roots, and cultural values.4 Culturally competent workers can
4 Berg, I.K. & Kelly, S. (2000). Building Solutions in Child Protective Services. New York: Norton.
help families to have a positive experience in planning and participating in parenting and other family access time by:
Respecting the client’s perspective.
Listening well enough to learn about people who are different from themselves.
Avoiding judgment from bias, stereotypes, or cultural myths.
Asking the family to explain the significance culture has for them, especially regarding family traditions, child rearing and discipline practices, spiritual beliefs and traditions.
In order to best serve families of diverse backgrounds we believe one needs to possess “cultural humility”. Cultural humility “involves the curiosity and motivation to understand the web of meaning in which children and families live, and the reflective capacity to examine our own cultural values and assumptions. It requires a commitment to appreciating the similarities and differences between one’s own culturally shaped goals and priorities and those of the children and families. It requires as well an obligation to ‘rein in’ our power and authority, so that the voices of children and family members can be fully valued and heard.” These meetings help provide a fuller picture of the family situation and networks, and they help clarify who can be involved in the change process as the worker develops the case plan. Exploring the family’s broader connections to faith communities, tribal or cultural bonds, and neighbors helps families focus on the resources that not only define them but could also help address their current needs.
In preparation for a team meeting the worker should:
• With parents identify key people
• Obtain parental consent to contact all key people and invite them to the meetings
• Prepare each invitee by explaining how family meetings work and the issues that will be discussed
20
Conduct a Family Team Meeting to engage kin in the case planning and to ensure that everyone understands their role.
• Clarify what the participants have contributed in terms of assisting with identified needs and the parents’ views about this
• Support family meeting participants in planning how each might help the family
• Identify and review what the participants have committed to do
• Consider whether there are any people who should not be present due to safety issues
Further refine the case plan using the information gathered at the 30 day meeting. This may or may not be the case.
Worker should consult with their supervisor regarding the content of the case plan—ensuring that it is specifically linked to identified safety threats.
Intentional Visitation Practices as part of the Case Planning Process
Historically conducting visitation may have been viewed as one thing among many things that workers have to do, (something to be checked off) RATHER than visits being intentionally planned and focused on building protective capacities and changing behaviors that caused children to be unsafe or at risk of future
harm.
In this model of practice the visitation activities are explicitly linked to helping parents change the behaviors that caused children to be unsafe or at risk of future harm. This means that the visitation activities need to be carefully planned and everyone involved in the visitation process must be aware of the focus of the visit activities. (This includes visitation center staff, case aides, kin or others involved in supporting the visitation efforts.
The visitation plan serves as an agreement between the agency serving the child in placement and the child’s family. It clarifies the structure of visiting, logistics, necessary tasks that are linked to learning new parenting skills—changing parenting behaviors that caused children to be unsafe or at risk of future harm, and the roles and responsibilities of placement caregivers, family members, and agency staff. A written plan reassures children and their families that the agency is invested in protecting family relationships. Research on parental visiting of children in
21
The cornerstones to an effective team meeting include:
• Everyone desires respect
• Everyone needs to be heard
• Everyone has strengths
• Judgments can wait
• Partners share power
22
foster care indicates a strong relationship between the development of a visiting plan and actual visitation by parents. Child welfare worker attitudes and behaviors that express encouragement for visiting also have a positive influence on parent visitation.5
Following each visit the worker or the person supporting the worker in the visitation asks the birth parents the following question:
• Did the visit activities help them to develop the behaviors so that they can more safely care for their children?
• What else do they think that they could do or what else other skills to they need to develop to safely parent their children
Best Practice Tips
It is nearly impossible to actually facilitate effective intentional visitation practices without the support of a team of individuals. This is why we placed the Family Team Meeting section PRIOR to the Intentional Visitation Practices section of this document. Engaging families in the process of supporting visitation will reduce the workload pressures on the worker and will expand the resources available to support visitation.
5 Center for Advanced Studies on Child Welfare. ( 1997).

Stage Four Ongoing Assessment
Workers must develop a Mindset of “Continuous or Ongoing Assessment”
Assessing the progress of families in changing behaviors that caused children to be unsafe is the foundation of the ongoing assessment of process. The purpose of ongoing assessment is not to evaluate the compliance of the family but to evaluate the efficacy of the interventions in changing behaviors or conditions that caused children to be unsafe.
This also helps you identify when you should move initiate Concurrent Planning activities.
There should be a complete periodic reassessment of the change in behaviors or conditions that caused children to be unsafe or at risk of future harm based on new events or information. Use a variety of formal and informal situations to reassess progress as all contacts are opportunities to gather information.
23
Strategies that can facilitate discussion about progress include using scaling questions, timelines, “temperature gauge” charts (measuring progress toward changing behaviors that
24
caused children to be unsafe or at risk of future harm), and other behaviorally oriented graphics.
For periodic reassessment of progress to occur, it is important that service providers provide timely, specific reports on progress that address changes in behaviors or conditions that caused children to be unsafe.
Case Plan review should occur whenever:
• Families make progress in changing behaviors or conditions that caused children to be unsafe
• When families face setbacks
• Parent’s stage of readiness to change evolves or deteriorates
• New information is received (e.g., parent reveals history of abuse)
• Family circumstances change (e.g., parent moves in or out of household)
• Any time any member of the team requests it.
BEST PRACTICE TIP
Anytime you meet with a family, you are evaluating the success of the family in making changes that caused the children to be unsafe. In a sense this means that you are always reviewing the case plan and always trying to find out of the services and interventions are the BEST to effect change. Remember the definition of insanity is doing the same thing over and over and expecting different results. If the services are not working—consider changing them!
Share Information with Family and Other Providers Throughout the Life of the Case
Workers will exchange information with the family, extended family members, service providers, and court regularly. As information on circumstances and needs is gathered from different sources, the caseworker should meet with the family to help them understand the following:
• The specific safety threats that were identified in the safety assessment
• The behaviors or conditions that need to change to address the identified safety threats
25
• How the specific services and visitation activities are focused on helping to support the change in behaviors required for children to be safe.
Timetable for Ongoing Assessments:
Quarterly o SDM (risk reassessment, reunification) o Court reviews o Case plan – reviewed every 3 months, updated every 6.
Ongoing – done all the time o Wellbeing o Safety o Monthly face to face with each child involved in case plan
Stage Five: Case Closure
Case closure is a significant decision that should reflect the removal of the threats to child safety and the building of a support system for the family that can assist in addressing any ongoing risks that may exist.
Permanency usually initiates a period of transition for the child and family. Post‐permanency services are typically required to support families and children as they work to achieve a new equilibrium.
Once post‐permanency services are provided, case closure becomes a possibility, and the child and family’s situation are re‐assessed in the new context. Questions similar to those raised in the beginning phase of the case are explored and answered prior to making the final determination to close the case:
Assess these issues:
Have any of the safety threats that were identified been brought under control?
How do the child and the parents view their situation and the possibility of case closure?
If the child has been reunified with his or her parents, do the parents continue to demonstrate the changes in behaviors (enhanced protective capacities)?
What kinship resources continue to be available, including resources of the tribe or clan to which the family belongs?
What specific community services are needed and utilized by the child or youth and the parents to support their current level of functioning and prevent reoccurrence of those problems that required service.
Workers will reassess whether or not the behaviors that caused the children to be unsafe at case closure and will consult with the supervisor.
26
Achieving permanence for a child family reunification, adoption, or another permanency plan does not immediately result in case closure.

27
The following should be completed at the point of closing the case:
• SDM risk reassessment
• RCW 1478 case closing form
• MN Safety Assessment
• Case closing interview
• Satisfaction survey regarding services provided (separate from worker performance.) [To be developed]
28
References
Children’s Bureau. (2009). Schene, Pat. Comprehensive Family Assessment Guidelines for Child Welfare. [Electronic Version] from http://www.acf.hhs.gov/programs/cb/pubs/family_assessment/index.htm.
Contra Costa County Children and Family Services. (2008). Comprehensive Assessments for Positive Family Outcomes (CAPFO) Demonstration Project. Launch Version Starship CAPFA Operator’s Manual.
Minnesota Department of Human Services. (2006). Family Centered Practice Guide: Engaging Assessing, and Building Strengths with Families.
NRCFCPP &NRCFCP. (2002). Lutz, Lorrie L. Family centered Assessment Guidebook: The Art of Assessment [Electronic Version] from http://www/hunter.cuny.edu/sicwirj/nrcfcpp/downloads/tools/family_centered _assessment_guidebook.pdf.
Prochaska, J.M. & Prochaska, J.O. (2002). In Children’s Bureau (2009) Comprehensive Family Assessment Guidelines for Child Welfare. [Electronic Version] from http://www.acf.hhs.gov/programs/cb/pubs/family_assessment/index.htm.
Ramsey County Community Human Services Department. Short Form: Family Centered Assessment Tool.
University of Maryland School of Social Work Center for Families. (2004). Grandparent Family Connections Intervention Manual.
.

29
Documentation
At the completion of the initial process of family assessment and when the information is updated, clear and full documentation should be included in the case file. Documentation incorporates what is known from the assessment of safety concerns, risks, strengths, protective factors, and needs; and it is framed in a way that suggests what expectations, services and interventions would help meet the family’s needs. Each child should be mentioned individually in documentation. Although the family’s signature is needed on the service plan, the signature alone is not sufficient documentation of the family’s involvement in the process. [ICWA requirements]
“Timely” documentation Relevant info: Done within 48 hours o Any information tied to case plan goal o Any information identified with MA billing o Any information critical to the immediate / emergency decision making in a case related to
the improvement or decrease in safety, wellbeing, or stability.
Daily info: done within week (5 days)
o Court conversations o Phone calls o Meetings o Review reports o Client visits
30
Appendix

31
Active Listening
Using Active Listening Skills to Develop the Helping Relationship 6– Active listening combines talking and listening skills. This skill allows clients to feel understood. In addition, it provides a means through which clients are encouraged to express themselves. In listening to clients’ messages, social work interns’ responses should mirror information provided by clients. If feelings are communicated, the active listening response should convey feelings, and should be of equivalent intensity (Cournoyer, 2005).
The skill of active listening is used when social work interns closely observe clients and carefully listen to what is said. After listening, the practitioner reflects to the clients what is observed, avoiding common pitfalls such as responding in a manner that mimics what has been said; interpreting of clients’ comments or behaviors; or focusing only on a part of a communication rather than attending to what the message as a whole is conveying. (Cournoyer, 2005).
Active listening represents a clear demonstration that interns and other practitioners have understood what clients have expressed. This understanding of what clients are saying facilitates the development of positive regard for the working relationship between clients and the program. If workers do not listen actively, they are likely to Miss Key parts of clients’ messages and thereby misunderstand, distort or misrepresent what clients are trying to convey. This also destroys the positive regard that has been built between clients and the practitioner.
Stages of Change
The quality of family involvement is related to their “stage of change”— their readiness for accepting the reality of their situation and their willingness to change. Family involvement is therefore dynamic, evolving as their readiness and capacity to change evolve. Understanding stages of change helps caseworkers make important decisions; for example, there are service plan implications if a parent refuses to or is unable to recognize problems in his or her parenting. Moreover, assessing stages of change helps caseworkers in engaging the parent to move forward in specific ways in the change process. The bottom line, however, remains the importance of family engagement no matter what the stage of change.
6 Grandparent Family Connections Intervention Manual. ( pp. 70)
32
Stages of Change*
• Pre-contemplation: Initial resistance to change. For example, “I have done nothing wrong and resent CPS' involvement.”
• Contemplation: A family member becomes aware of the problem but has not yet made an effort to change. For example, "I know I should clean up this messy house and handle the kids better."
• Preparation: A family member is intending to take some action to change. For example, “Where can I get information on substance abuse treatment?” It is important to distinguish intention from actually taking action.
• Action: A family member changes his or her behavior and/or environment. For example, “I've started to work real hard to change,” with specific examples of actions taken.
• Maintenance: Family members work to prevent relapse and maintain the gains they have made during the change process. For example, “I have not had a drink in the past six months.”
*Prochasca & Prochasca, 2002
33
Transfer Guide for Communications Between Intake and Ongoing
Initial Transfer Meeting:
1. Concise description of the reason(s) the family came to the attention of the system.
2. Results of the safety and risk assessment—“The child was found to be unsafe due to the presence of the following safety threats….”
3. Description of the safety plan that was put in place and how it is managing or controlling the identified safety threats.
4. Description of the behaviors or conditions of the caregiver’s that have to change in order for the child to be safe or to minimize child risk.
Add this to court presentation or case staffings:
5. Describe the interventions that were put in place to change the behaviors or conditions that caused the children to be unsafe or at risk.
6. Success of the interventions in changing the behaviors or conditions that caused the children to be unsafe.
34
Possible Questions To Engage Caregivers During the Functional Assessment Process
(These questions have been compiled by the following contributors, Lorrie L. Lutz President of L3 P Associates, LLC; Grandparent Family Connections Intervention Manual and University of Maryland Social Work Center for Families).
NOTE: We would never ask all of these questions but a select few based on the family’s dynamics.
A. Family Telling Their Story
• What are your perceptions why the system is involved in your life —or why your child has been removed from your care?
• Do you believe that any of our safety and risk concerns are valid? • What has your life been like in the past year? Have there been any big events or changes? How are you and your child dealing with these changes?
• Describe your childhood – what was it like growing up in your family?
B. Day To Day Parenting
General Approach to Parenting
• Do you feel that your children are on a par with other kids their age? (Listen to their description of the problem. Talk to referral source. Observe interactions in interview.)
• What’s a typical day like for you and your children? (Be sure to ask each person interviewed.)
• How do you get your children to listen to you? (Observe: Does caregiver overreact or under‐react to child behaviors. Does child show evidence of fear of caregiver?)
• What’s it like for you to parent the children? Is it what you expected?
• Parenting is not something that you wake up and know how to do…it is just hard for all of us. Do you ever get lost as a parent?
• (Observe appropriateness of authority role as evidenced by interactions.)
• Do you and your children have the opportunity to eat meals together?
• Scaling question—On a scale of 1‐10, where are you at in comparison with where would you like to be as a parent?
• Could you describe each of your children?
• Could you describe a great memory you have of your family.
• When is a time when your child was very successful—what part did you play in that success?
• What is one special way that you show love to your children?

35
Discipline
• Do your children know pretty much what to expect in terms of how they’ll be punished?
• How were you disciplined as a child?
• What is a day in your life as a parent like?
• What is one creative way that you have dealt with your child’s frustrating behavior?
Developmental Stimulation
• Is this (the room you’re in) where your kids spend most of their time playing? (Observe various toys, books, games. Too much? Too little? Age appropriateness? Determine what the children like to play.)
• What sorts of activities do you and your children do together in your free time? What’s your experience been like with your children’s schools? Have you been able to meet your children’s teachers? Do you like school? How are you doing in school?
• How do the children get along with each other? Do you have to get involved if they fight or do they work it out amongst themselves?
C. Living Conditions/Finances
• How long have you lived here? Are you satisfied with your housing? Your neighborhood? (Pay attention to safety concerns. Observe the conditions of the household. If possible take the opportunity to view multiple rooms.) If something needed to be repaired, how would it get fixed? Is your landlord responsive to your requests?
• Do you want to stay here? Are you able to afford the rent or mortgage? Is there anything that will get in the way of your staying in the home?
• What is your primary source of income? I know it’s a struggle but if no emergencies arise are you able to pay your monthly expenses with what you receive? If you receive TCA have you been told you need a job to continue to get benefits? Are you able to take care of your family’s needs?
• Do you find that you frequently run out of food stamps or money before your next check comes?
• How do you get to appointments and other places? (Assess level of difficulty)
• Where is the best place you ever lived? Why did you like it?
• What would make where you live today more like your best place?
• Have you ever applied for public assistance (TANF, food stamps, day care subsidy, or utility assistance)?
36
D. Family Connections and Supports
• When you need help with something are there family members or friends you turn to? What about your neighbors?
• How supportive is your family? Can you rely on them?
• Is finding adequate child care a major concern for you?
• Do you feel comfortable with your child’s babysitter or do you wish you could find someone else?
• (Look on intake for children’s health care provider) Where do your children go for health care? Where do you go? How satisfied are you with the care you receive? What about dental care?
• Can you tell me a little about the 3 most important relationships in your life right now?
• Do you currently have any physical condition that makes it hard to care for the home, yourself, the children? In the past, have you had difficulty caring for the home, yourself, or the children? How about emotional stresses that may have made it difficult to care for yourself, the home, or the children?
• How does your family have fun? What activities do you and your child like to do outside of the home?
• Who do you trust?
• Are you involved with any church or community group?
• Sometimes when you don’t know how you are going to feed your children, it is hard to focus on anything else‐‐‐do you ever struggle like this? Who helps you during these times?
E. Caregiver History
You have told me a lot about you and your family, including your needs. It would help if I knew more about you. I’d like to ask you some questions about things that may be difficult to talk about. Your answers will help me to understand you and your family better, but please let me know if there’s anything you don’t feel comfortable discussing.
• What was your childhood like? Who’d you live with? When you look back do you feel positive about your childhood?
• Have you or anyone else in your family been a victim of sexual abuse? What about domestic violence? (If yes, find out if they received counseling.)
• Do you use alcohol or any other substance? (If yes) How much? How often? Have you in the past?
• What do you do when you get really ticked off at another adult? (If response indicates use of physical violence, ask) Have you ever been arrested for assault?
• Has anyone ever assaulted you, either verbally or physically?

37
F. Caregiver Personal Characteristics
• Impulse control – refer back to “What do you do when you get really ticked off at another adult?” and observe interactions with family members. Do you see yourself as a “laid‐back” person or do you tend to “go off” when you get mad? Do you ever get into trouble because of your reactions?
• Cooperation – Observe response to interviewer and openness to agency involvement.) You may have worked with other programs in the past. How were they helpful? How were they not helpful?
• Emotional stability – Observe congruence between affect and content. Observe range of emotional responses. Do you see yourself as a moody person or are you mostly pretty much the same? Which feeling – happy, sad, angry, or scared – describes how you feel most of the time?
G. Medical Needs Of Caregivers
• Do you have a doctor (medical provider)? Dentist? When was the last time that you saw the doctor/dentist?
• Do you have any health conditions that impact your ability to care for your children?
• Has your health ever held you back from getting a job or taking care of your children?
• Are there any medications that you are taking?
H. Parent’s Mental Health
• Do you ever feel like you just can’t take it anymore?
• Do you ever have a hard time just getting going in the morning? When you cannot “get going” who takes care of your child?
• Do you have a mental health diagnosis? If so, are you on any medications? Do you take them regularly?
I. Parent Substance Use
• How do you get through a bad day?
• Has your drinking or drug use caused job, school, family, or legal problems?
• Do you ever use prescription drugs in ways other than prescribed?
• Do others in the home abuse alcohol or other drugs?
J. Family Violence
• On a scale of 1‐10 where would you rate your relationship with your partner/spouse/significant other? What would bring you closer to a 10?
38
• All couples argue, how do you resolve conflict in your family? Have the police ever been called to your home? Have you ever been concerned about the safety of your children when you argue with your partner?
• Has your child ever scared you or threatened to physically harm you?
• Questions to ask the child:
• What happens when there is an argument?
• Have you ever seen or heard someone in your family hurt another family member?
• Are you ever afraid something is going to happen to you or to your parents?
• Do you have a pet—if so have you ever been worried about the safety of your pet?
• Has any of your siblings scared you or threatened to physically harm you or any member of the household?
K. Child Well Being Child Substance Use
• Are you concerned about your child’s use of substances (legal or illegal) or alcohol?
• Have you (the child) ever felt like you should cut back on your drinking or drug use—or felt bad or guilty about it?
• Has your drinking or drug use caused school, family, or legal problems?
• Have you ever felt annoyed by criticism of your drinking or drug use?
• Do you ever think about drinking or using drugs when you are in school?
• Do your peers ever pressure you to drink or use drugs? What do you say?
• Do others in the home use alcohol or other drugs?
Child/Youth Mental Health
• Does your child have any behavioral problems that worry you? If so, please describe your child’s behaviors.
• Has your child ever been evaluated for mental health issues by anyone? If so, what was the outcome? What were you told to do to help your child?
• Have you had to miss work or school because of your child’s problems?
• Is your child on any medication for emotional or behavioral issues? Do you give your child this medication regularly?
• Questions to Ask the Child/youth
• On a scale of 1‐10 how would you describe how happy you are? Scared you are? Confident you are?
• How do you handle stress in your life?
• Do you ever feel so down that you think about “ending it all”?
39
Child/Youth Educational Issues
• What about your child/youth’s school performance makes you proud? • What is your child’s best subject? Where does your child struggle in school?
Questions to ask the child/youth
• Do you ever have problems understanding what your teacher is saying? Do you have any trouble reading the board?
• What is the hardest part of school for you?
• Do you ever skip school? Where do you go when you skip school?
Medical Needs of Child
• Does your child have a doctor (medical provider)? Dentist? When was the last time that your child went to the doctor/dentist?
• Does your child have any health conditions that cause you concern?
• Have any of your children’s health issues ever kept you from going to work?
• Are there any medications that your child is taking?
• Do you know if your child is sexually active?
40
Additional Guidelines for Interviewing Children
Philosophy: This best practice guideline for interviewing children was developed in accordance with Contra Costa County, Children and Family Services’ mission statement; to keep children safe, promote permanency, and to conform with current statute.
Setting the Interview
(In general, interviews can be more effective in the context of an activity)
1. Introduce self and role:
I’m a social worker; do you know what a social worker is? Even if they say yes, explain. Do you have any more questions before we start?
As a social worker, there are some things I can and cannot keep confidential… Give examples (i.e. I won’t tell your friends/teachers/etc).
Do you know why I came to see you today or why you came to see me? Explain.
2. Building Rapport/Assessing Development:
Hold are you, school, teacher, pets, and reflective questions (give up detail about self: pet, sports, video games, activities).
How are you feeling? If they don’t say “nervous” or something, say, “I talk to lots of kids and some kids feel excited, nervous, etc…How are you feeling? What are you missing in school right now?
DON’T ASK: “Do you know the difference between a truth and a lie? PLAY A GAME: For example, “What color is this pen?” “Red”. If someone said it was black, would that be the truth or a lie? “If I say this is a chair, what would you say?”
Gathering Information
1. Open‐ended Questions/How to elicit more:
• Tell me more about that • Tell me about a time when… • What happened then? • Did anything else happen? • Was anyone else around? • Do you remember when, what were you doing?
41
• Has it happened since? • How did you feel when…..? • I wasn’t there so…. • Even if you think I know, tell me anyway. • Even if you think it doesn’t matter… • You told ____________ something happened….. • What happens to someone when they get in trouble?
2. Home Life:
• We are going to talk about your day from the time you wake up to the time you go to sleep.
• Where do you sleep? Who puts you to bed? Who sleeps in the room and where? • Who wakes you up in the morning? • What do you have for breakfast? What is your favorite food? • What happens at dinnertime? • Do you have chores? What happens if you don’t do your chores? • Who stays home with you if you are sick? • Clothes – Who buys them for you? What was the last time you received something
new? What is your favorite outfit? Where do you keep your clothes? • How do you like living here? • What do you like best/least about living here? • What do you do for fun? • Who is your favorite person in the family? Why? • Who would you go to if you needed help if someone harmed you or threatened you?
Has anyone ever done that? • Has anyone ever told you not to tell this SW something because you might get removed
or hurt? • Looks like you have a bruise on your knee. How did that happen? • What happens when someone is really liked by the caretaker? • What happens when the foster parent/caretaker has to be somewhere without you?
Who watches you? • How do you feel about that? • Is there anyone you don’t like to stay with? Why? • What happens when the foster parent/caretaker gets mad? • If you could change something here, what would it be?
3. Education
• Do you go to school? How do you get to school?

42
• What’s your teacher’s name? Do you like your teacher? • What’s the easiest thing about school? What’s the toughest? • What happens after school? How do you get home? Do you have to do homework? • Who helps you? • Have you missed any school? • Tell me about your school. What grade? Friends at school? What don’t you like about
school? What do you do at recess? Recent grades?
4. Medical/Dental/Therapy
• Are you going to counseling? How do you like it? What do you do? Do you think it’s helpful?
• Have you been sick recently? Who is your doctor? • When was the last time you saw a dentist? Who is your dentist?
5. Family/Visits
• Do you have contact with your Mother? Father? Sibs? Others? When was the last time you saw any of them?
• Talked to them on the phone? Do you have phone numbers? Do you want contact? Do you want to write to your family? Do you have private/confidential time with family? (if appropriate)
6. Court
• The next court hearing is…. • Do you wish to attend (current statute requires for any child aged 10 and over)? • If appropriate, share purpose of the hearing and possible outcomes • Is there anything you would like me to tell the Judge? • You have an attorney and someone from his or her office may be visiting you.
7. Safety
• If something happens to you or someone else scares you, hurts you or makes you sad, who would you tell?
• (Brainstorm who they could tell). • Is there anything that you don’t want to tell me or are afraid to tell me? • Have you told someone else? Who? • Does anyone else know about it? Who?

43
Closure
• Do you have any questions? Anything else you want to talk about? • Discuss what information will be shared with caregiver. Is there anything you would like
me to talk about with your foster parents/caregiver? • Provide business card (if age appropriate) with emergency number listed letting the
child know that they have the right to call you anytime. • Thank child for participation (not for giving information).

Eco Mapping of Connections
44