Embed Size (px)
Citation preview

Br HeartrJ 1993;70:489-496
BRITISH CARDIAC SOCIETY
Radiation hazards to the cardiologist
A report of a subcommittee of the British Cardiac Society
In 1988 a Working Party of the CardiologyCommittee of the Royal College of Physiciansand the Royal College of Radiologists issueda short report Radiation Protection as Appliedto Cardiology. This report stressed the impor-tance of adequate training in radiation pro-tection and appropriate working practice. Inthe report the introduction of interventionalprocedures was identified as a cause of someconcern. Interventional techniques such asangioplasty, balloon dilatation of valves, andcatheter ablation are now commonly used.Recent reports of the exposure of cardiolo-gists/radiologists to high levels of radiationduring some of these procedures haveprompted the British Cardiac Society to com-mission the present report.The present report refers to the operator as
"the cardiologist" but we recognise that radi-ologists too perform coronary angiography,cardiac catheterisation, coronary angioplasty,and other interventional procedures.Radiologists, unlike cardiologists, are fre-quently involved in x ray based proceduresother than those involving the heart and soare probably more aware of the cumulativeoccupational radiation exposure. Some stud-ies have shown that interventional cardiolo-gists may be receiving a higher dosage thantheir radiological counterparts, which sug-gests that there may be room for improve-ment in the radiation hygiene of cardiologists.
CommitteemembershipA J Camm (chairman),J Reid (Royal College ofRadiologists),M Raphael (BritishCardiac Society),P Wilde (Royal Collegeof Radiologists),R Boyle (British CardiacSociety),M Clarke (British Pacing& ElectrophysiologyGroup),S Qureshi (BritishPaediatric CardiacAssociation),M Rothmnan (BritishCardiovascularInterventional Society),A Shaw (Institute ofPhysical Sciences inMedicine)Correspondence to:Professor A. John Camm,Department of CardiologicalSciences, Medical School,St. George's Hospital,Cranmer Terrace, London,SW17 ORE
Exposure to radiationEvery x ray exposure has two components:the main or primary beam and the scatteredradiation, known simply as scatter. The mainbeam carries the diagnostic information and,being of high intensity, constitutes the chiefradiation hazard to the patient. Scatter con-
sists of radiation of lower energy deviated inall directions, including backwards, from themain beam. Scattered radiation is the chiefradiation hazard to the staff of catheterisationlaboratories. It also degrades the quality ofthe diagnostic information obtained. Thequality and quantity of scatter depend not
only on the patient but also on variousaspects of the primary beam.
For this reason control of the primarybeam is one of the two major ways of reduc-
ing irradiation of staff and patients and of
improving image quality. The type of scatter
produced depends on the energy of the pri-
mary beam. Low energy (low kVp) beamsproduce low energy scatter that tends to beabsorbed within the patient and not to escapeto irradiate the staff or to degrade the image.Thus oblique (thick) projections through thepatient, which drive up the kVp, increasepatient and staff dose and reduce picturequality. Projections where the x ray tube(under couch) is on the same side as theoperator result in exposures that are 10 timeshigher than when the image intensifier is onthe same side as the operator.A serious side effect of increasing the kVp
is that the iodine absorption of x rays declinesand hence the quality of visualisation by thecontrast agent deteriorates. All cardiologistssee this in their daily practice, where the radi-ographic quality of LAO cranial and RAOcaudal views is much lower than PA or RAOprojections in the same patient. Often, how-ever, the choice of projection is not open tous because the requirement to remove overlapand foreshortening are of fundamental impor-tance and may demand a thick projection.
DOSE QUANTITIESThe absorbed dose is a measure of the amountof energy imparted per unit mass by ionisingradiation to a tissue or organ. The specialunit for absorbed dose is the gray (Gy). Onegray is equivalent to one joule per kilogram.
Different types of radiation cause variousbiological effects. The equivalent dose weightsthe absorbed dose for the harmfulness of eachradiation type. For x rays, the radiationweighting factor is unity so that the equiva-lent dose, measured in sieverts (Sv), equalsthe absorbed dose in grays.The equivalent dose received by different
tissues (or organs) is frequently non-uniform,particularly in diagnostic radiology, while thesusceptibility to harm from a given radiationdose is also tissue dependent. The concept ofeffective dose is introduced so that risks associ-ated with irradiation of various tissues can beadded to determine the risk to the body as awhole. This is the most useful quantity forassessing and comparing overall risk. Theeffective dose is defined as the sum of theequivalent doses to all tissues, each weightedwith the relative risk (mainly of cancer pro-duction) for the specific tissue. The tissueweighting factors, which have recently beenrevised (ICRP 1991), add up to unity so thatthe sum of risks to individual tissues receiving
489
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Camm, Reid, Raphael, Wilde, Boyle, Clarke, Qureshi, Rothman, Shaw
a given dose is the same as the risk from uni-form whole body irradiation at that doselevel. The effective dose is also measured insieverts.
DOSE LIMITSThe system of protection recommended bythe International Commission on Radio-logical Protection (ICRP) for all practicesthat involve radiation exposure to people isbased on the principles that the practice mustbe justified, that all exposures should be aslow as reasonably achievable (ALARA princi-ple), and that individual exposures are subjectto dose limits (table 1).
United Kingdom legislation laid out in theIonising Radiations Regulations (1985),based on earlier ICRP recommendations(ICRP 1977) has similar equivalent dose lim-its for specific organs but stipulates highereffective dose limits for occupationallyexposed individuals (table 2).
In view of the increased risk estimates inthe more recent ICRP recommendations(ICRP 1991) additional guidance has beenpublished, as an adjunct to the 1985 regula-tions (Health and Safety Commission 1991).This aims to restrict a worker's exposure toless than three tenths of 15 mSv per year,averaged over any five consecutive years anddetails a course of action if this constraint isexceeded. The National RadiologicalProtection Board (NRPB) commenting onthe ICRP recommendations also concludesthat "once pregnancy is declared, the expo-sure of the pregnant woman should be furtherrestricted so as to limit the effective dose atthe fetus to 1 mSv" (NRPB 1991).Dose limits are set at a level above which
risk is considered unacceptable. The latestrisk estimate for a fatal cancer averaged for apopulation of working age is 4% per sievert(ICRP 1991), so that an annual effective doseof 15 mSv would represent a cancer risk of 1in 1667 per year. The dose limits for the lensof the eye and the skin are set to preventdeterministic radiation effects that occurabove a threshold dose level.
Dose monitoringThe Ionising Radiations Regulations (IRR)1985 require that any employee likely toexceed three tenths of any relevant dose limitmust be designated as classified. Classifiedworkers are subject to individual dose assess-ment and medical surveillance. Personal doseassessment of non-classified workers may becarried out to demonstrate that doses arerestricted to below the classification level.
Table 1 ICRP radiation dose limits for occupationally exposed individuals
Dose quantity Annual dose limit
Effective dose 20 mSv (averaged over any five year period,with no more than 50 mSv in a single year)
Effective dose for a pregnant woman 2 mSv (to the surface of the abdomen duringthe declared tern of the pregnancy)
Equivalent dose to the lens of the eye 150 mSvEquivalent dose to slin, hands, and feet 500 mSv
Table 2 UK effective dose limitsDose quantity Annual dose limit
Effective dose 50 mSvEffective dose for pregnant 10 mSv (during the declaredwomen term of the pregnancy)
Cardiologists and other staff involved withcatheterisations and interventional radiologytherefore need to be monitored and may needto be designated as classified according to theIRR Guidance Notes (National RadiologicalProtection Board 1988) and IRR ApprovedCode of Practice (Health and SafetyCommission 1985). It is likely that most car-diologists will not enter the classified catego-ry. This, however, can only be decided uponby regular dose monitoring.
Dose assessment requires continuous indi-vidual whole body monitoring, normally witha film or thermoluminescent dosemeter(TLD) badge worn on the trunk under theprotective lead apron. There is evidence thatmonitoring under the apron gives a betterestimate of effective dose than dosemetersworn outside the apron for the most likelycombinations of scattered x ray energies andlead apron thickness (Faulkner and Harrison1988). It has been suggested that effectivedose can be estimated from a single dose-meter worn outside an apron (ICRP 1982,Jones 1986) but this may overestimate theeffective dose by a factor of 5-20. Furtherevidence is emerging that the revised ICRPtissue weighting factors, which give moreweight to body organs that are protected,improved the agreement between the wholebody dose estimated by monitoring beneathan apron and the effective dose.
In addition, routine or at least periodicmonitoring is also required for unprotectedorgans, which may include eyes, hands, thy-roid, or even lower legs, if their exposure islikely to contribute more than one tenth ofthe effective dose. This is possible if theseorgans receive more than one tenth of theirdose limit, which is often the case in cardiolo-gy. If unprotected organs in the head areexposed to more than one tenth of their doselimit, the estimate of effective dose can berefined by calculating a weighted combina-tion of head and body dosemeter readings(Gill et al 1980). Again film or TLD badgesor TLD extremity dosemeters can be used formonitoring. When eye doses are monitoredthe dosemeter should be worn on the fore-head or attached to the inside of normal orprotected glasses. Dosemeters worn on theshoulder may overestimate eye doses (Jeans etal 1985) and are therefore not recommended.Doses to the unprotected thyroid can bemonitored with an appropriate dosemeterworn over the thyroid or on the collar, whileextremity doses can be measured with a TLDattached to the hand or fingertip or with afilm badge worn on the wrist.
Alternatively, the dose to unprotected partsof the body can be indicated by a suitably
490
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Radiation hazards to the cardiologist
calibrated electronic direct-reading, integrat-ing dosemeter. This may be particularly use-ful for making initial dose assessments and todetermine which body sites may require fur-ther monitoring. Audible alarm dosemeters,particularly worn outside the apron on thehead or neck, may be particularly valuable fortrainees and, intermittently, for more experi-enced operators. It is remarkable how quicklythis sharpens radiation hygiene.The duration of monitoring periods will
depend on dosemeter type. For routine moni-toring each film or TLD badge will normallybe worn for one month but monitoring withTLD extremity dosemeters may require sev-eral days or weeks, whereas instant readoutdosemeters may be used to monitor doses forindividual examinations. For short monitor-ing periods it is important that any extrapola-tions to longer durations use realisticworkloads.
Reduction ofradiation exposureThe simplest and most effective ways toreduce irradiation of patients and staff are toemploy the ALARA principle and the inversesquare law. However, much can be achievedby modifying or upgrading existing equip-ment and paying attention to radiation shield-ing. In all hospitals there are radiologists whoprovide a body of experience that may be ofvalue to cardiologists. Full cooperationbetween cardiologists and radiologists willhelp to reduce the exposure to radiation.
PHYSICAL BARRIERSThe patient's thorax becomes a powerfulsource of scattered x rays. The scattered radi-ation is particularly intense at table height onthe tube side of the table and in certain pro-jections (LAO craniocaudal and lateral). Thisscatter can be interrupted by physical barrierscommonly made from lead-impregnated rub-ber or leaded glass. A simple, ceiling mount-ed, cantilever-suspended, leaded glass screen,which incorporates a leaded skirt, can reducesecondary scatter to the torso and head of theoperator by up to a factor of 10. Such screensare readily available from all major manufac-turers of cineangiographic equipment. It isalso possible to mount leaded rubber skirtson the table side or in the form of a saddleacross the patient's thighs. These will giveadditional substantial reductions in scatteredradiation to the operator. They can usually beconstructed in-house from old lead aprons.
PERSONAL PROTECTIONMany makes and types of lead apron areavailable. These come in various lead equiva-lent thickness from 0-25 mm to 0-5 mm. It isadvisable to wear the heaviest apron that canbe used with comfort. Many of the newmakes of apron give much better thyroid andlateral thoracic protection (especially impor-tant to female staff) than the obsolete BritishStandard BS3793 aprons. The older type ofapron can be upgraded by Velcro belts to
keep the side apertures closed and separate
thyroid collars can be added. This latter pre-caution is frequently overlooked and it isimportant because the thyroid is very radio-sensitive. So too is the lens of the eye. Leadedglass prescription spectacles are available butthey are heavy and can become uncomfort-able during a long intervention. If a leadedglass cantilever screen is available and proper-ly used, leaded spectacles are not necessary.
FLUOROSCOPYFluoroscopy was originally used mainly forbeam positioning of the cine run. However,with the advent of interventional proceduressuch as angioplasty, ductus and septal defectclosures, and, in particular, radiofrequencyablation of accessory atrioventricular path-ways, fluoroscopy times can be exceptionallylong. It is therefore vital to use low dose ratefluoroscopy. A modern sensitive image inten-sifier must be used and two variations onstandard continuous fluoroscopy are avail-able-pulsed fluoroscopy and digital noiseintegration
Pulsed fluoroscopy can reduce radiationexposures by up to 30% and its short x raypulses prevent motion blurring of fast movingdetails. It is therefore useful when very accu-rate positioning of balloons, guidewires, orinterventional devices is required. It has thedisadvantage that if the pulse rate is too low a"Charlie Chaplin" or "slide show" effect isobtained. Because there is a trade off betweendose rate and the number of pulsed fluoro-scopic frames per second most centres stilluse standard continuous fluoroscopy.
Digital noise integration with a real timemotion detector in the digital processor andthe addition of real time edge enhancement, canhalve the fluoroscopic dose in digital systems.
CINEANGIOGRAPHYOf all radiodiagnostic procedures, cinean-giography delivers one of the highest radia-tion dosages to patients, and consequently tostaff. This is because high resolution imagesat high frame rates in multiple projections areneeded. The sensitivity of image intensifiershas been greatly improved but it may also bedesirable to reduce the frame rate and thedosage per frame.
Frame rate reductionThe human eye registers flicker at frame ratesof less than 20 frames per second (fps). Mostconventional cineangiographic systems run at25 or 30 fps, but some older laboratories stilloperate at 50 fps. Each laboratory should usethe lowest acceptable frame rate.
Dose reduction perframeBecause of the physical principles involved inproducing x ray images there is a compromisebetween decreasing the dose and increasingthe amount of "noise". There is therefore a
level below which quantum mottle degradesimages to unacceptable levels.
DIGITAL CARDIAC ANGIOGRAPHYThe physical constraints of conventional
491
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Camm, Reid, Raphael, Wilde, Boyk, Clarke, Qureshi, Rothman, Shaw
cineangiography leave little room for develop-ment. However, digital imaging technologycan be used in cardiac angiography. Likecineagiography, reducing the dose increasesthe quantum mottle. But digital contrastenhancement can produce images of satisfac-tory contrast and resolution with up to 30%less radiation per frame than cineangiogra-phy. With a technique known as "infilling"frame rates as low as 12-5 fps can be runwithout appreciable flicker thus reducing to aquarter the dose to patient and staff at 50 fps.
Digital review facilityIn long or complicated interventional proce-dures the operator may need to see a repeatedimage to check the position of a catheter orguidewire. Digital equipment has a continu-ous replay mode, which allows the operatorto reflect on the progress of the case, ratherthan giving multiple repeat bursts of fluo-roscopy. This may seem to be only a subjec-tive advantage but in practice it is a real one.A similar advantage is given by a "digital roadmapping" facility.
Operator riskThe hands and eyes are at particular risk ofsignificant radiation exposure even when anoperator follows the correct guidelines forradiation protection. The doses incurred bythe eyes and hands during the various proce-dures performed in the catheterisation labora-tory depend on the apparatus, the nature ofthe procedures performed, and the skill of theoperators. Most references to physiciandosage incurred during cardiac catheterisa-tion are unhelpful because they date back tothe period when intensifiers were inefficient,apparatus was of the fixed tube variety, andcatheterisation skills were poorly developed.Current practice uses sensitive image ampli-fiers, compound angulated x ray sets, andmuch shorter examination times because ofthe greater skills of the operators.
Begg et al (1975) using the PhilipsCardiodiagnost and Sones technique requireda mean fluoroscopy time of 8-4 minutes withan average cine recording time at 30 fps of 54seconds. The index finger dose was 0-28 mSvand the lens dose was 0009 mSv per proce-dure with the lead curtain in position anddoses were 10 to 20 times higher if the leadcurtain was not in position. Begg et al com-mented that the dose delivered by cine radi-ography was almost 10 times greater thanthat needed for fluoroscopy and that use ofthe lead overleaf curtain reduced radiation byfactors as great as 18:1. They also comment-ed that the radiation dose to the angiographerwas 5-10 times greater in intensity in theLAO projection than in the RAO projection.
Baiter et al (1978) compared the Sonestechnique of coronary angiography with andwithout the protective lead curtain at theCleveland clinic with measurements at StJoseph's Hospital with the lead curtain. Thelead curtain reduced dose to the eye from.0-06 mSv per procedure to 0 019 mSv per
procedure, and with shorter fluoroscopy andcine times at St Joseph's Hospital the eyedose was only 0 004 mSv per procedure.Similarly, the hand dose was reduced from0-08 mSv per procedure without the lead cur-tain to 0 021 mSv per procedure with thelead curtain. It was 0 003 mSv per procedureat St Joseph's Hospital.
Finci et al (1987) compared the radiationexposure to the operator from straightforwardcoronary angiography with that from singleand double vessel coronary angioplasty. Theirpaper does not make it clear whether theirapparatus was of the most modem varietybecause they obtained longitudinal tilt byrotating the table, rather than by rotating thetube. They also used biplane ventriculogra-phy. For angiography the fluoroscopy timewas 223 seconds, for single vessel angioplastyit was 1023 seconds, and for double vesselangioplasty it was 1186 seconds. For angio-graphy the cine time was 49 seconds, forsingle vessel angioplasty it was 32 seconds,and for double vessel angioplasty it was 49seconds. Finci et al calculated that for angio-graphy the dose to the operator was 0-06 mSvfor the eyes and 0 3 mSv for the left hand.For single vessel angioplasty the dose to theeyes was 0-04 mSv and to the left hand it was0.3 mSv, and for double vessel angioplastythe eye dose was 0 03 mSv and the dose tothe left hand was 0 47 mSv. Although theirfluoroscopy times for angiography were quiteshort the eye dose is significantly higher thanthat obtained by the previous workers. Thismay reflect the use of biplane filming and rel-atively unsophisticated apparatus.
Calkins et al (1991) measured the radiationdosages incurred by the operator duringintracardiac catheter ablation procedures.Even with protective lead glass in positionthey found the dose to the left hand was 1mSv per procedure and the dose to the leftmaxilla, the equivalent of the eye dose, was0-28 mSv per procedure.From these figures (table 3) it is possible to
estimate the number of cases of each proce-dure that the trained operator can perform inthe course of a year and still remain withinthree tenths of the relevant dose limit (45mSv per year for the eyes and 150 mSv peryear for the hands) (table 4). In table 4 it isassumed that each operator performs onlyone type of procedure.
Because most cardiologists undertake vari-ous procedures the factors in table 5 must beused to calculate the approximate totals for amix of procedures. The total number of casesallowable in a year for any individual operatoris also heavily influenced by that individual'sradiation hygiene and by the equipment thatis used. On current best estimates, with mod-em apparatus, the eye dose incurred duringcoronary angiography from the arm rangesfrom about 0 004 mSv to 0-02 mSv when aprotective lead curtain but not a lead glasseye shield is used. The worst case wouldallow an operator to perform over 2000 coro-nary angiograms without eye irradiation lead-ing to their becoming a classified operator.
492
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Radiation hazards to the cardiologist
Table 3 Average radiation doses Upper limit ofdoselprocedure (mSv)
Procedure Eye Hand
Simple angiography 0-02 0-02Angioplasty 0-03 0-3Pacemakers 0-05 0-15Catheter ablations 0-3 1-03/10 Dose limit 45 150
Table 4 Approximate annual number of individualprocedures to achieve three tenths of dose limits (if no otherprocedures are undertaken
Procedure Eye Hand
Angiography 2250 7500Angioplasty 1500 500Pacemaker 900 1000Catheter ablations 150 150
Hand doses range from 0-02 mSv down to0 003 mSv per case, allowing an individual tostudy more than 7000 cases a year beforeclassification on the basis of hand irradiation.
For angioplasty the figures are somewhatinconsistent but they suggest that while theeye doses are little different from those ofsimple coronary angiography the hand dosesare about ten to one hundred times higher. Ifthe figures of Finci et al (1987) are correctoperators would be limited by hand doses to500 procedures per year. For catheter abla-tions the information seems well based. Theeye dose, even with a protective lead glass, isaround 0-3 mSv, giving a limit of 150 cases ayear. The hand dose is virtually 1 mSv percase, giving a similar limit of about 150 casesa year. Clearly the operator dose in catheterablations may easily lead to classification. Nodirect measurements are available for opera-tor dose during pacemaker insertions butJeans et al (1985) estimated an eye dose of005 mGy and a hand dose of 0-15 mGy perprocedure, figures that are difficult to recon-cile with those given for angiography.
Such calculations clearly do not apply totrainees (Renaud 1992), who take significant-ly longer than their senior colleagues andincur a higher radiation dose. The radiationburden of trainees should be very closelysupervised and remain within the limits.Trainees should do fewer procedures untilthey gain sufficient expertise.
Investigational and interventionalproceduresPAEDIATRIC INTERVENTIONPaediatric cardiological facilities are availableat 17 centres in the United Kingdom. There
Table 5 Maximum workload based on exposure to radiation (factor x number ofProcedures)
TotalSimple Catheter permitted
Exposure Angiogram Angioplasty Pacemaker ablation score
Eye 0-02 +0 03 +0-05 +0-3 <45Hand 0-02 +0 3 +0-15 + 1-0 <150Eye and Hand 0-02 +0 09 + 0-05 +0-3 <45
are between two and six consultant paediatriccardiologists. Thus about 55 consultants and20 junior staff in the United Kingdom areinvolved in the catheter laboratory work.
Each year about 4000 paediatric cardiaccatheterisation procedures are performed inthese centres. Most are diagpostic proceduresbut about 33% are interventional (from 10%to 60% for different centres). There has beenan annual increase in the number of inter-ventions since 1982: before that date allprocedures were diagnostic. Diagnosticcatheterisation lasts from 30 minutes to twohours whereas interventional procedures takefrom two to four hours. The types of inter-ventions have also changed over the last 10years. Initially only balloon dilatation of thepulmonary valve was accepted as an alterna-tive to surgery, but nowadays many othercongenital cardiac lesions are also amenableto non-surgical treatment. These includeballoon dilatation in aortic stenosis, coarcta-tion, and re-coarctation; in branch-pulmonaryartery stenosis; in tetralogy of Fallot, and instenosed venous channels. Coil embolisationfor arteriovenous fistulas, umbrella occlusionof arterial ducts and laser valvotomy for con-genitally atretic valves are becoming accept-able and recognised treatments. More andmore stents are being implanted and non-surgical closure of atrial and some ventricularseptal defects may become routine in the nexttwo years.
In the early part of the experience of everypaediatric cardiologist interventional proce-dures take a long time to complete andinvolve long fluoroscopy times. With experi-ence these times become shorter. Some of thetreatments are for congenital lesions withhigh risks from surgery and so the risks ofradiation have to be balanced against the risksof the lesion and its alternative treatments.However, every attempt is made to ensurethat the patient receives the lowest dose pos-sible.
ADULT CORONARY INTERVENTIONSCoronary angiographyThe definition of the coronary anatomy byinvasive techniques forms the larger part ofthe workload of any catheter laboratory. In1990 a total of 58 197 coronary angiographicprocedures were undertaken in the UnitedKingdom by 46 of the 51 cardiac units withcoronary angiography facilities. Each unitperformed between 274 and 3300 proce-dures. Approximately 25% of these patientswent on to coronary artery bypass grafting(CABG) and another 14.5% had percuta-neous transluminal coronary angioplasty(PTCA).
Coronary angioplastyThe past 12 years have seen the emergence ofPTCA for the treatment of some forms ofcoronary narrowing. Each cardiologist hashad to perform many more procedures, witha concomitant increase in the risk of radiationexposure. More recently the scope for inter-vention has increased. As the experience of
493
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Camm, Reid, Raphael, Wilde, Boyle, Clarke, Qureshi, Rothman, Shaw
operators has grown, along with enhance-ments in technology, so has the ability to treatmore complex coronary disease.A survey in 1990 by the British
Cardiovascular Intervention Society (BCIS)showed that the number of angioplasties inthe United Kingdom was 7445 performed at51 centres, with individual centres doingbetween 10 and 428 procedures. Data on
PTCA were received from another five cen-tres for which information about cardiaccatheterisations was not available. The totalnumber of PTCAs performed in the UnitedKingdom in 1990 was 8459.The exposure to radiation is related to the
experience of the operator, the complexity ofthe procedure, the nature of any additionalintervention carried out, and factors relatedto equipment and procedure. In the UnitedKingdom the experience of coronary angio-plasty is small with over 50% of centres (27)performing fewer than 150 procedures perannum. Sixteen centres do fewer than 100procedures and five do fewer than 50, where-as in the United States more than 66% ofprocedures are carried out by 30% of thecatheter laboratories. Worldwide figures indi-cate that the coronary angioplasty procedurerate will grow at about 12% per annum andthis level of growth has been seen in previousyears in the United Kingdom.
Additional interventional procedures are
now being seen in the United Kingdom andvarious drills, slicing devices, lasers, andstents are being used in a few cases. In 1990,135 such procedures were undertaken.These are usually longer, more complex pro-cedures with increased radiation exposuretime.
Currently, 180 cardiologists perform coro-
nary angioplasty procedures. BCIS has indi-cated that about 400 PTCAs per million are
required. The present workload is about 170per million. Each operator performs justunder 50 procedures per annum. To reachthe BCIS target each operator will have tomore than double his or her workload.
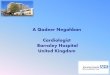
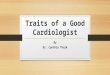
Recent trends in thereduction ofprocedure andscreening times (inminutes) forradiofrequency ablation inthe United Kingdom. Datakindly provided by DavidCunningham on behalfofthe British Pacing andElectrophysiology Group.
500
450
400
350
300
250
200
150
100
50
0
RADIOFREQUENCY ABLATIONFew centres within the United Kingdom offerradiofrequency ablation. At these centres one
or two consultants perform the proceduresand this is likely to remain the pattern forsome time. As well as the operator up to twonurses, two technicians, and two radiogra-phers will be exposed to radiation during theprocedures. Nursing and radiography staff areroutinely monitored and in most studiesreceive substantially less radiation than theprimary operator.A radiofrequency database has been set up
by the British Pacing and ElectrophysiologyGroup (BPEG). Currently from 50 to 110ablations per year are performed by radio-ablation at the six main centres.The clinical indications for radiofrequency
ablation include "atrioventricular nodal"pathways, accessory pathways, and ectopicarrhythmogenic sites within the atrium andventricle. Because of the variety of conditionstreated the time taken per case ranges fromone to six hours with screening times ofbetween 12 minutes and 85 minutes. A totalof 480 cases were identified from the six cen-
tres and the average x ray screening time was62 minutes (figure).The individual operator will therefore be
exposed to between 2100 and 4600 minutesper year of extra radiation. We expect that thenumber of cases will double within the nexttwo years. This increase could double indi-vidual radiation exposure unless more spe-cialists are trained in this technique.Though there is a learning curve radiation
exposure times for radiofrequency ablationare unlikely to become appreciably shorterbecause the figures quoted above are similarto those of large centres in the United Statesand Europe.
PACEMAKERSEach year in the United Kingdom about13 000 pacemakers are implanted by at least200 cardiologists in more than 125 pace-maker centres. The implantation rate is less
0 2 4 6 8 10 12 14 16 18 20 22
Time from first RF procedure (mnth)
rProcedure time i Screening time
3 -\ ~~~~--g - - - - - - - - - - - ------------- - - - - - - --...... --.-.
0 LaD'QEb % 0 a.0I I~~~~~~~,1 I Ir
494
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Radiation hazards to the cardiologist
than in most other European and NorthAmerican countries. The workload per centreranges from 25 to 700 pacemakers per yearand individual cardiologists may implant upto 200 pacemakers each year. About 80% ofall implants are single chamber pacemakers.Pacemaker implantation takes 2-10 minutesof fluoroscopy time with an experienced oper-ator. However, much of the pacemakerimplantation workload is undertaken byjunior staff who may take much longer.
In recent years there has been an appropri-ate trend towards the implantation of moredual chamber units but an inappropriatetrend towards the implantation of pacemakersby less experienced operators at district gen-eral hospitals. These factors have generallyresulted in a greater total radiation exposurebut because more cardiologists are nowimplanting pacemakers the effect on theexposure of individuals to radiation is moredifficult to ascertain. Cardiologists nowimplant endocardial defibrillators. This pro-cedure probably involves a substantially high-er radiation burden than does dual chamberpacing and although the total number ofimplantations in the United Kingdom is lowthe workload is presently concentrated in afew centres.
OTHER ADULT CARDIAC INTERVENTIONSSome forms of stenosed heart valves can betreated by balloon dilatation and some chan-nels can be closed by deployable balloons orbaffles (for example, the patient ductus arte-riosis occluder). Techniques are being devel-oped and the number of procedures, theindications, and long-term results are unclear.Development will continue and allowancemust be made for this when the potentialradiation exposure of the cardiologist isassessed. Balloon dilatation of valves probablyinvolves a similar radiation burden as angio-plasty.
In 1990 dilatation of the mitral valve wasthe most common valve procedure in adultsin the United Kingdom with 20 centres per-forming 213 procedures. The total number ofall types of valve dilatations was 309.
Voluntary registration schemeAt present it seems likely that, with the possi-ble exception of cardiologists undertakingcatheter ablation procedures, the averagepotential exposure to radiation is not exces-sive. However, workloads, work practices,and equipment standards vary considerably.Furthermore, in most areas the number ofinvestigations and interventional procedureswhich involve exposure to radiation are set toincrease. There are no plans to increase com-mensurately the number of cardiologistsand/or radiologists who undertake these pro-cedures. Thus the exposure of cardiologists toradiation should be monitored more carefullyin the future than in the past. Some form ofprospective audit should be carried out:
(a) The most strict form of audit is com-pulsory registration of operators. This would
be difficult to enforce and would be counter-productive because it would alienate manyoperators.
(b) At present a basic level of radiationmonitoring for all staff is achieved withdosemeter badges. This aims to satisfy legisla-tive requirements but is inadequate for a doseaudit because the workload (number and typeof procedures) and doses to unprotectedorgans or extremities may not be recorded.Standard dosimetry should be instituted.Two badges should be worn-one under thelead apron on the hip nearest the x ray tubeand the other at the neck level on the thyroidcollar on the outside of the apron.
(c) A voluntary registration scheme isattractive because a body of reasonablydetailed information could be obtained fromat least a proportion of operators andbecause, as interest and awareness in thissubject grows, the number of people partici-pating in the scheme will increase. A volun-tary system has the benefit that thoseparticipating in it would be sufficiently inter-ested to complete some form of annualreturn.A voluntary registration scheme with data
returned annually is the most useful form ofaudit for assessment of the exposure of cardi-ologists to radiation. All interventional cardi-ologists and others frequently exposed toradiation should be encouraged to register.
INFORMATION REQUIREDIt is considered that registration of individu-als, rather than of catheterisation laboratoriesis appropriate, because each cardiologist maywork in an individual way and in more thanone laboratory and the dose to an individualis of most concern. There is no reason whyseveral or all individuals from one centreshould not be registered.The annual return from each individual
should contain the following information:* Name and institutions where the proce-
dures were carried out.* The number of each type of diagnostic and
interventional procedures carried out bythat individual during the year. All forms ofprocedure that require ionising radiationshould be logged, including diagnostic car-diac angiography, coronary angioplasty,valve dilatation and other interventionaltechniques, paediatric cardiac catheterisa-tion, electrophysiology, pacemaker implan-tation, and ablation procedures. The logshould include the length of screeningtime, the equipment used and whether theindividual was first or second operator.
* Results of the monitoring proceduresundertaken by the registrant as a conse-quence of participating in this scheme.
ORGANISATION OF REGISTRATION SCHEMEIt is clear that this scheme will require a data-base to be maintained with facilities for mailout and some facilities for analysis. The twomost suitable organisations that might runthe database are the British Cardiac Societyand the Cardiac Radiology Group of the
495
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from

Camm, Reid, Raphael, Wilde, Boyle, Clarke, Qureshi, Rothman, Shaw
Royal College of Radiologists. It is appropri-ate for the British Cardiac Society to run thedatabase in conjunction with the radiologistsin order to maintain proper input and interestfrom both groups.The database should be open to participa-
tion by all those involved in invasive tech-niques whether junior medical staff orconsultant and whether radiologist or cardiol-ogist.The database should be endorsed by the
British Cardiac Society and its affiliatedgroups such as BPEG, BPCS and BCIS.Their members should be expected to jointhis scheme. Cardiologists in training shouldlog radiation exposure in their training manu-als and submit annual reports to the database.
Summary and recommendationsThe development of interventional tech-niques that require substantial fluoroscopyand cinangiography times has increased theexposure to radiation of interventional cardi-ologists. At the same time the maximum per-mitted exposure to radiation has beensignificantly reduced. It is therefore appropri-ate to alert all cardiologists using ionisingradiation to the need for radiation hygiene.The recommendations set out below are de-signed to promote this heightened awareness.1 Cardiologist exposure to radiation shouldbe monitored with two dosemeter badges,one placed beneath the lead apron and oneoutside the apron.2 The radiation dose reports should bereturned to the cardiologist and to thecatheter laboratory(ies). The informationshould be charted in the area of the catheterlaboratory(ies).3 The British Cardiac Society and/or itsaffiliated groups should be responsible fororganising specific cardiology radiationcourses.4 Cardiologists should be encouraged tojoin a voluntary register to log their exposureto radiation. The register should be set upand maintained by the British CardiacSociety.5 Recording of exposure to radiation shouldbe part of the training log of cardiologists intraining.6 The workload of cardiologists should beset at a level less than would be likely toexceed three tenths of all relevant dose limitsof radiation exposure.7 Where necessary staffing levels should beincreased or practice patterns reviewed inorder to prevent excessive radiation doses tocardiologists.8 When a cardiac catheterisation laboratoryis replaced or upgraded careful consideration
should be given to radiation protection of staffand the use of low dose equipment.
BibliographyAgarwal SK, riesen EJ, Huddleston AL, Rao RP. The effec-
tiveness of glass lenses in reducing exposure to the eyes.Radiology 1978;129:810-1 1.
Balter S, Sones FM Jr, Brancato R. Radiation exposure to theoperator performing cardiac angiography with U-arm sys-tems. Circulation 1978;58:925-65.
Begg FR, Hans LR. Radiation exposure to angiographer dur-ing coronary arteriography using the U arm image amplifi-er. Cath Cardiovasc Diag 1975;1:261-5.
Cagnon CH, Benedict SH, Mankovich NJ, Bushberg JT,Seibert JA, Whiting JS. Exposure rates in high-level-controlfluoroscopy for image enhancement. Radiology 1991;178:643-6.
Caltins H, Niklason L, Sousa J, El-Atassi R, Langberg J,Morady F. Radiation exposure during radiofrequencycatheter ablation of accessory atrioventricular connections.Circulation 1991;84:2376-82.
Cousin AJ, Lawdahl RB, Chakraborty DP, Koehler RE. Thecase for radioprotective eyewear/facewear. Practical implica-tions and suggestions. Invest Radiol 1987;22:688-92.
Dash H, Leaman DM, Operator radiation exposure duringpercutaneous transluminal coronary angioplasty. JfAm CollCardiol 1984;4:725-8.
Faulkner K, Harrison RM. Estimation of effective dose equiv-alent to staff in diagnostic radiology. Phys Med Biol 1988;33:83-91.
Finci L, Meier B, Steffenino G, Roy P, Rutishauser W.Radiation exposure during diagnostic catheterisation andsingle and double vessel percutaneous transluminal coro-nary angioplasty. Am J Cardiol 1987;60:1401-3.
Gertz EW, Wisnesli JA, Gould RG, Akin JR. Improved radia-tion protection for physicians performing cardiac catheteri-sation. Am Jf Cardiol 1982;50:1283-6.
Gill JR, Beaver PF, Dennis JA. The practical implications ofICRP recommendations regarding dose equivalent limitsfor workers to staff in diagnostic x-ray departments.Proceedings of fifth international Congress of the IRPA.Jerusalem: IRPA, 1980:15-18.
Grant SCD, Bennet DH, Mather JM. Reduction of radiationexposure to the cardiologist during coronary angiographyby the use of a remotely controlled mechanical pump forinjection of contrast medium. Cath Cardiovasc Diag 1992;25:107-9.
Health and Safety Commission. The protection of personsagainst ionising radiations arising from any work activity.Approved Code of Practice. London: HMSO 1985.
Health and Safety Commission. Dose limitation-restrictionof exposure. Approved Code of Practice, Part 4. London:HMSO, 1991.
Holmes DR Jr, Wondrow MA, Gray JE, Vetter RJ, FellowsJL, Julsrud PR. Effect of pulsed progressive fluoroscopy onreduction of radiation dose in the cardiac catheterisationlaboratory. JAm Coil Cardiol 1990;15:159-62.
ICRP. Recommendations of the International Commission onRadiological Protection. Ann ICRP 1977:publication 26.
ICRP. General principles of monitoring for radiation protec-tion of workers. Ann ICRP 1982.publication 35.
ICRP. 1990 Recommendations of the InternationalCommission on Radiological Protection. Ann ICRP 1990:publication 60.
The ionising radiations regulations 1985. StatutoryInstrument No 1333. London: HMSO, 1985.
Jeans SP, Faulkner K, Love HG, Bardsley RA. An investiga-tion of the radiation dose to staff during cardiac radiologicalstudies. BrJ Radiol 1985;58:419-28.
Jeans SP, Faulkner K, Love HG, Bardsley RA. Routine moni-toring of eye dose (reply). BrJRadiol 1985;58:1227-8.
Kosnik LT. Personnel exposure in the cardiac catheterisationlaboratory. Health Phys 1986;50: 144-7.
Klein LS. Radiofrequency catheter ablation. Safety and prac-ticality. Circulation 1991;84:2594-7.
McParland BJ, Nosil J, Burry B. A survey of the radiationexposures received by the staff at two cardiac catheterisa-tion laboratories. BrJ Radiol 1990;63:885-8.
National Radiological Protection Board. Guidance notes forthe protection of persons against ionising radiations arisingfrom medical and dental use. London: HMSO, 1988.
National Radiological Protection Board. Board advice follow-ing publication of the 1990 recommendations of the ICRP.NRPB-M321. Chilton: NRPB, 1991.
Renaud L. A 5 year follow up of the radiation exposure to in-room personnel during cardiac catheterisation laboratory.JAm Coll Cardiol 1990;15:159-62.
Russel JGB. The radiogenic hazards of working in a radiologydepartment. Clin Radiol 1991;44:145-6.
496
on July 5, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.5.489 on 1 N
ovember 1993. D
ownloaded from