Embed Size (px)
Citation preview


Mohammad Mahdi Daei
Interventional Cardiologist
CAROTID ARTERY STENTING

MAGNITUDE OF THE PROBLEM
• 795,000 Americans annually suffer a STROKE
• 25% die
• #3 killer of Americans
• #1 cause of long term disability

THREE STROKE TYPES
IschemicStroke
Clot occludingartery85%
Intracerebral Hemorrhage
Bleedinginto brain
10%
Subarachnoid Hemorrhage
Bleeding around brain5%
WWW.ACPONLINE.ORG/ABOUT_ACP/CHAPTERS/OK/GORDON.PPT

MAJOR CATEGORIES OF ISCHEMIC STROKE
• Thrombosis
• Embolism
• Global-Ischemic or Hypotensive Stroke

THROMBOTIC STROKE
• Atherosclerosis: the commonest pathology of vascular obstruction leading to thrombosis
• Other pathological causes:• Fibro muscular dysplasia• Arteritis (Giant Cell & Takayasu)• Dissection of vessel wall • Hypercoaguability

EMBOLIC STROKE
• Two most common sources of emboli:• Left sided cardiac chambers• Artery to artery stroke: as in detachment of a
thrombus from ICA at the site of a plaque


STROKE
80 % of strokes : ischaemic in orgin 20 – 25 % of ischaemic stroke : carotid stenosis
Risk of stroke correlates with severity of carotid stenosis
Prevention

TREATMENT OPTIONS
Medical therapy
Carotid endarterectomy
Carotid artery stenting

CEA SUPERIOR TO MEDICAL THERAPY Asymptomatic carotid stenosis
Asymptomatic Carotid Surgery Trial (ACST) Carotid stenosis >60% : 5 yrs stroke rate reduced from 11.8% to 6.4%
10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1)
10 yrs stroke rate reduced from 17.9% to 13.4%
Asmptomatic Carotid Atherosclerosis Study (ACAS)
A. Halliday Lancet 2004
JAMA 1995
A. Halliday Lancet 2010

CAROTID ENDARTERECTOMY (CEA)

MATCHING PATIENT TO INTERVENTION Treatment decisions depends on patient-specific factors
1. Risk factors for CEA
2. Risk factors for CASMedical
Surgical / Anatomical

RISK FACTORS FOR CEA Medical risk factors
CHF and left ventricular dysfunction Unstable angina or recent MI (<30
days) Coronary artery disease (CAD) Open heart surgery needed within 6
weeks Severe pulmonary dysfunction

RISK FACTORS FOR CEA Surgical / Anatomical risk factors
Surgical Factors Restenosis after prior CEA Previous ablative neck surgery
(e.g. radical neck dissection, laryngectomy)
Previous neck irradiation Contralateral vocal cord
paralysis Tracheostomy
Local complications Infection Nerve injury Cervical haematoma Wound dehiscence

RISK FACTORS FOR CEA Surgical / Anatomical risk factors
Anatomical Factors High carotid bifurcation (above
C2) Extension of athersclerotic
lesion into intracranial ICA or proximal CCA below clavicle
Intraoperative or Peri-operative stroke

RISK FACTORS FOR CAS
Access
Arch
Target Vessel

MANAGEMENT ALGORITHM
HIGH risk for surgery
Favourable anatomy for
CAS
CAS
Unfavourable anatomy for
CAS
CEA
Symptomatic >= 50% CS
LOW risk for surgery
Asymptomatic >= 70% CS
BMT

CONCLUSIONS
• Carotid endarterectomy has been established as the gold standard for treatment of carotid artery stenosis• NASCET and ACAS trials
• Carotid stenting remains to be proven as a viable alternative to endarterectomy in all patients
• SAPPHIRE results suggest that CAS is at least equivalent to CEA in high risk patients
• ICSS results suggest that CAS may cause higher peri-operative morbidity in symptomatic patients
• CREST results suggest equivalency of CAS to CEA for all patients with carotid stenosis for composite endpoint of death / stroke/ MI• However, stroke is more common in CAS, and has a greater impact on quality of life, that MI


CAROTID WALLSTENT™ (BSCI)• S/E monorail closed cell• braided chromium cobalt• Diameter - 6, 8, 10 mm• Length - 30, 40, 50 mm• 5F - 6, 8 mm• 6F - 10 mm

FilterWire EZ™ (BSCI)
• One size fits 3.5 to 5.5mm vessel diameters
• 3.2F Profile
• 0.014’’ Monorail™ exchange system
• Preloaded wire
110 micron Polyurethane membrane
• Suspended Radiopaque Nitinol loop• Adapts to vessel sizes and diameter changes

GUIDANT ACCULINK/ACCUNETS/E OPEN CELL NITINOL WITH LONGITUDINAL LINKS

CAROTID STENT TECHNIQUE
• Angiography (pigtail, access catheter)
• Stiff hydrophilic guide wire (0.035”)
• Long interventional sheath or guide catheter
• Embolic protection device
• Appropriate size balloon catheter
• Self-expanding (FDA approved) carotid stent
• Closure device (optional)
Basic Equipment

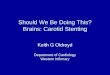
CAROTID STENT: TARGET LESION LOCATION
ICA alone: 3%
Bifurcation: 90%
CCA alone: 5%
Multiple: 2%

CAROTID STENT TECHNIQUE
• Femoral access • Arch angiography• Selective catheterization of target CCA • Wire placement in ECA • Sheath or GC placement in distal CCA • Placement of embolic protection device • Pre-dilation of lesion • Stent placement • Post-dilation of stent• Removal of EPD• Final angiography
Fundamental Steps

CAROTID STENTING NEED FOR COMPLETE INVENTORY
Diagnostic Catheters• Vitek• Simmons 1 and 2• Headhunter• Davis• Berenstein • HN2• Others
Guidewires• 0.035” exchange glidewire• 0.038” exchange glidewire• 0.035” Amplatz SS (1cm vs 4cm floppy)• Wholey exchange• 0.035” Rosen• 0.014 Spartacore• SV 14/5• 0.018” Roadrunner

Bovine Arch
Work-horse Guides

Simple Curved Catheters
IMAModified AR1 JR 4
‘Coronary catheters’
Consider using dedicated catheters!!!

Complex Curved Catheters
Simmons 1, 2, and 3 curves VTK


ANY QUESTIONS?