Embed Size (px)
Citation preview
Quiz 1
• 68 year old man presents with sudden
painless loss of vision right eye
• Whit next?
quiz 1 pic of the fundus
Quiz 2
• 78 year old woman presents with painful
inflamed right eye
• Whit next?
Pic of the affected eye
Quiz 3
• 28 year old man presents with acute onset
diplopia
• Whit next?
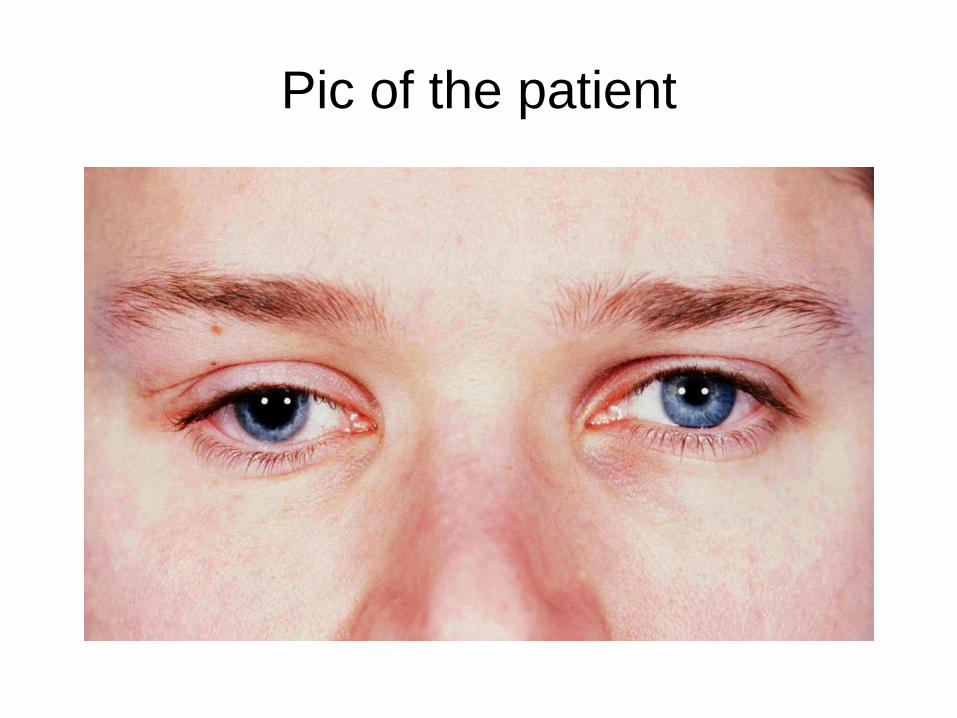
Pic of the patient
Quiz 4
• 78 year old woman presents with a watery
right eye
• Whit next?

Pic of the patient
Quiz 1 & algorithm
• 68 year old man presents with sudden
painless loss of vision right eye
• Whit next?
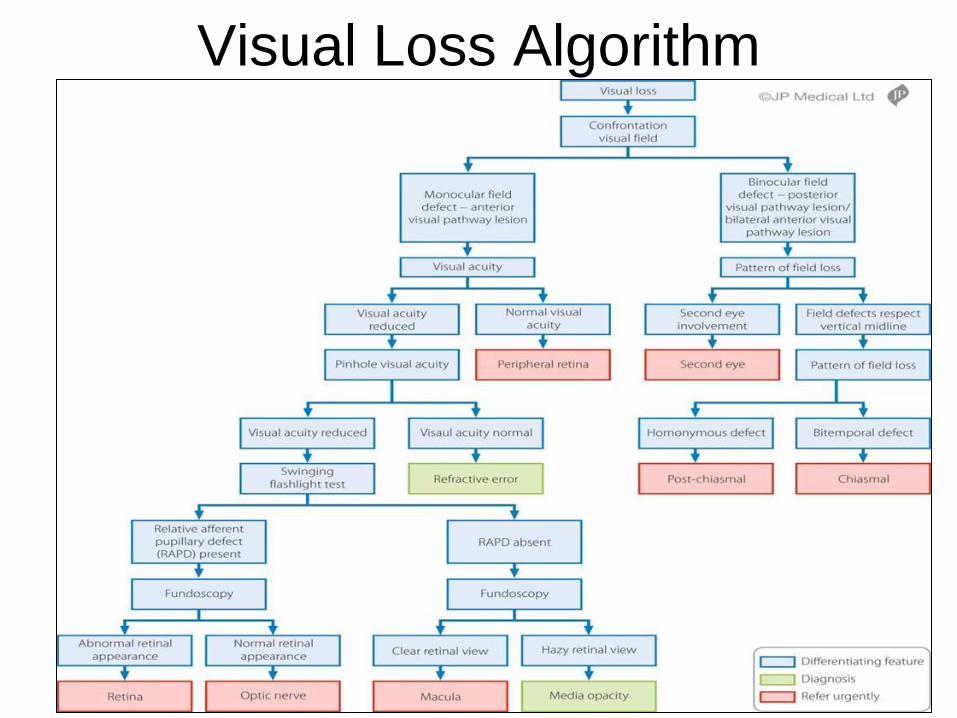
Visual Loss Algorithm
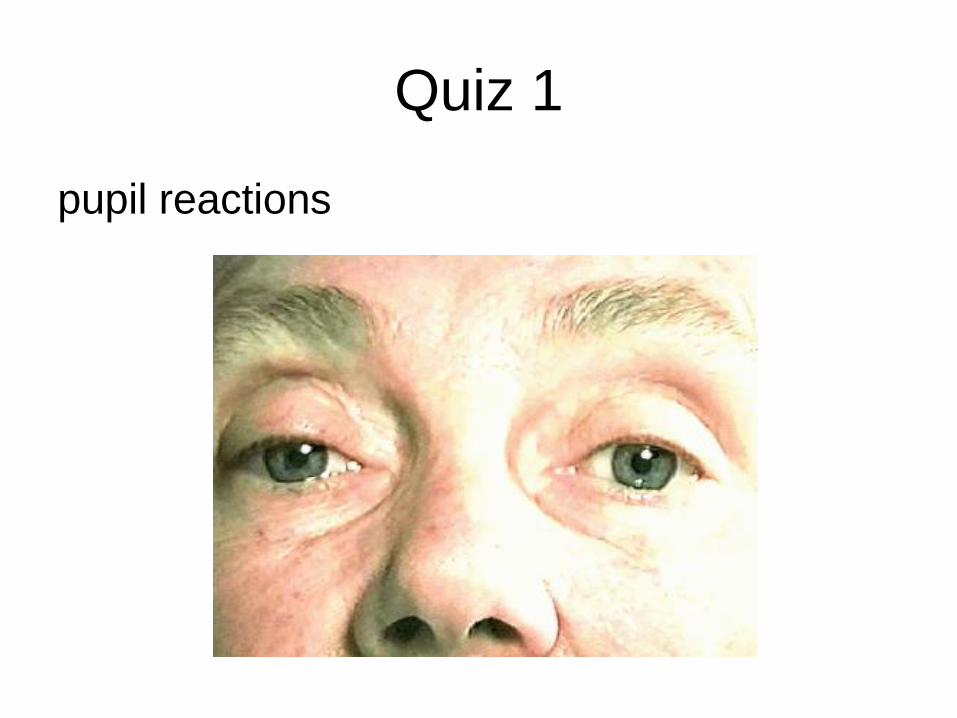
Quiz 1
pupil reactions
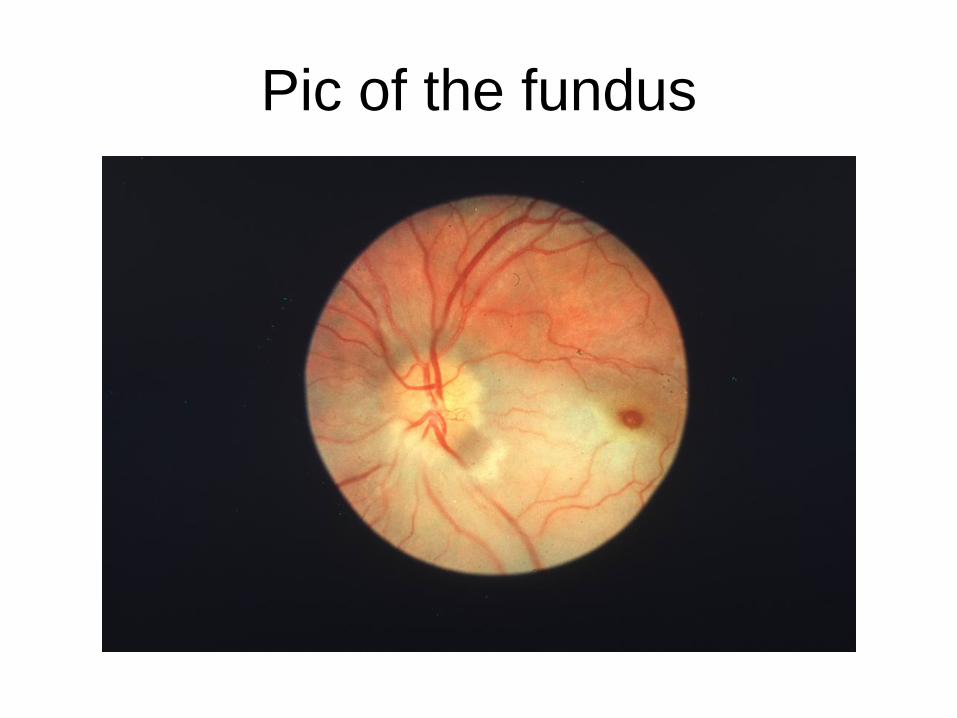
Pic of the fundus

Quiz 2 & algorithm
• 78 year old woman presents with painful
inflamed right eye
• Whit next?
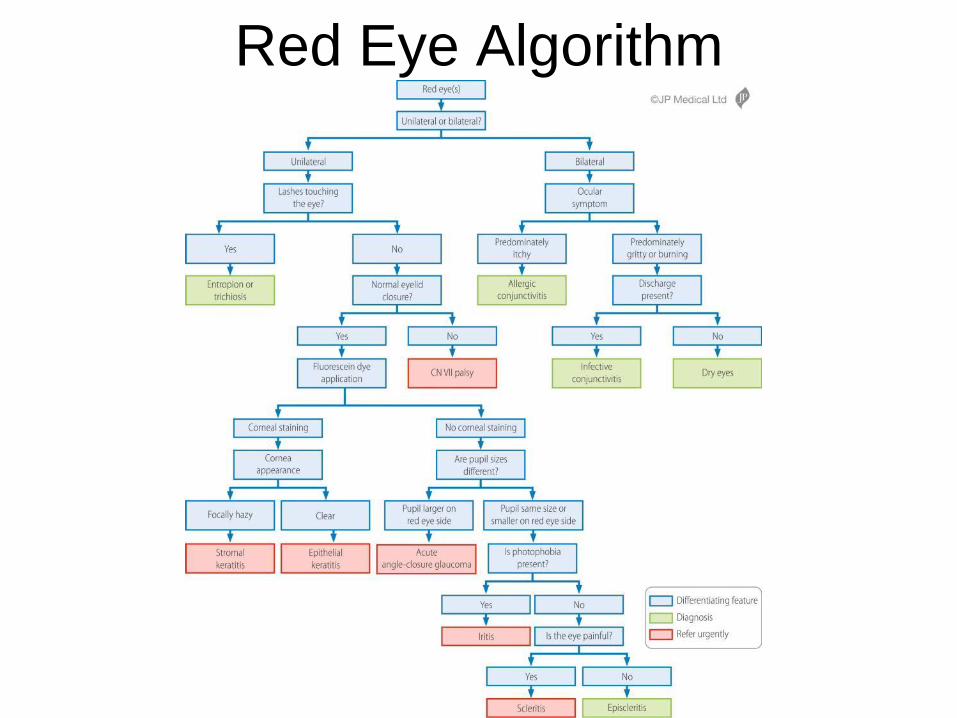
Red Eye Algorithm
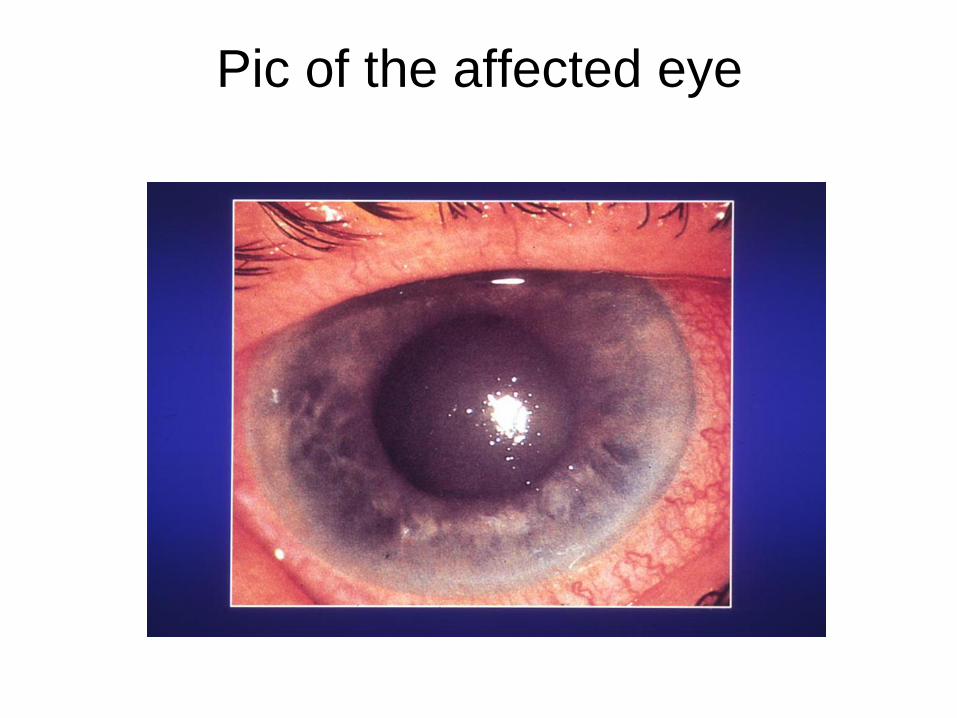
Pic of the affected eye
Quiz 3 & algorithm
• 28 year old man presents with acute onset
diplopia
• Whit next?
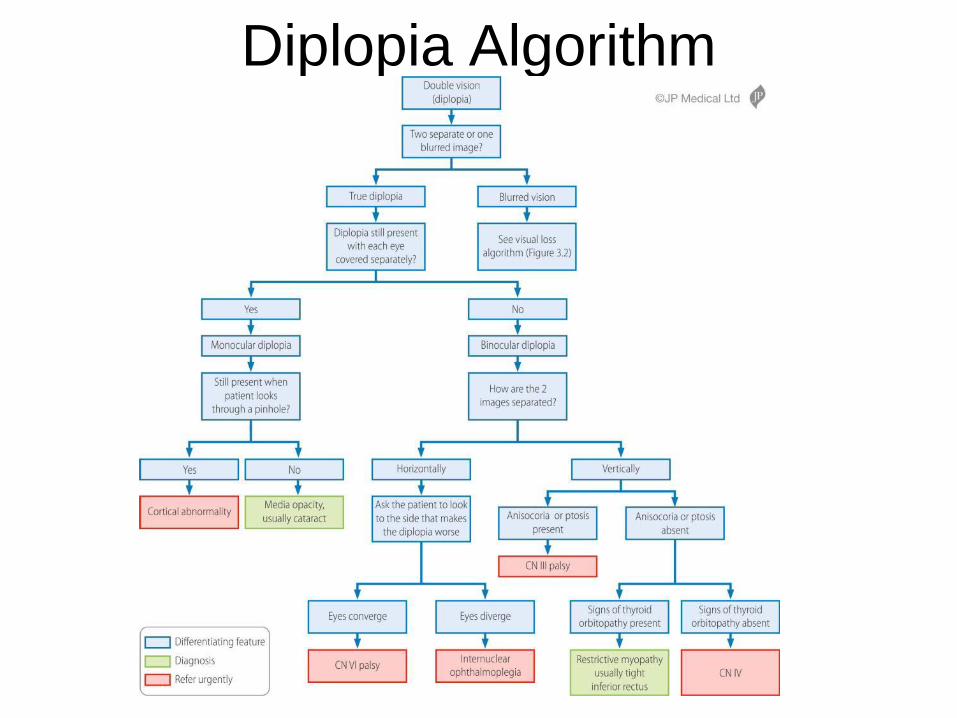
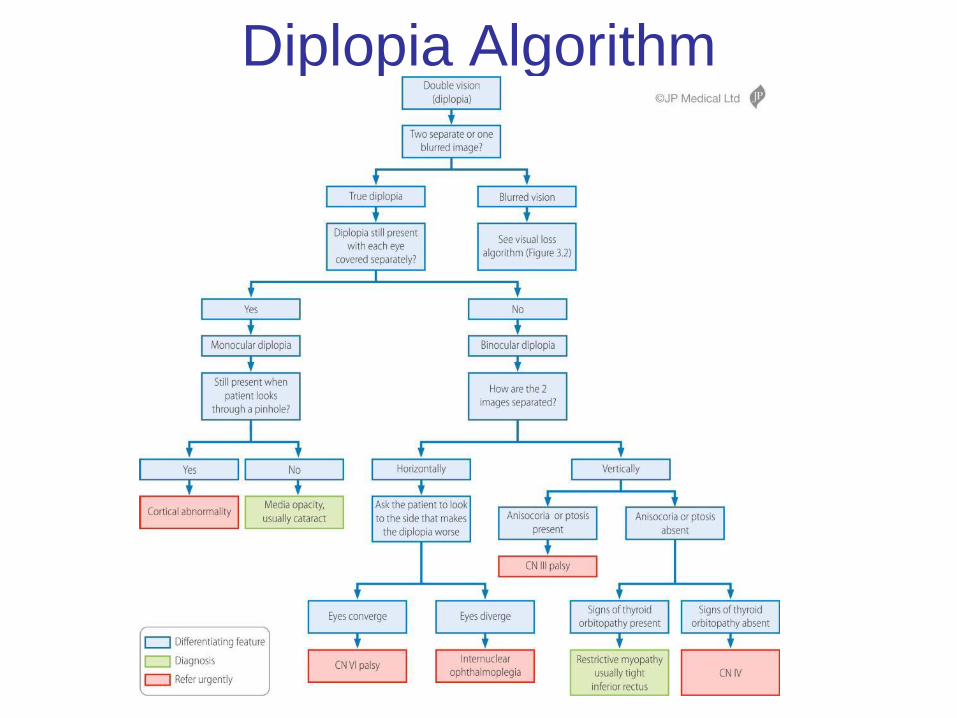
Diplopia Algorithm
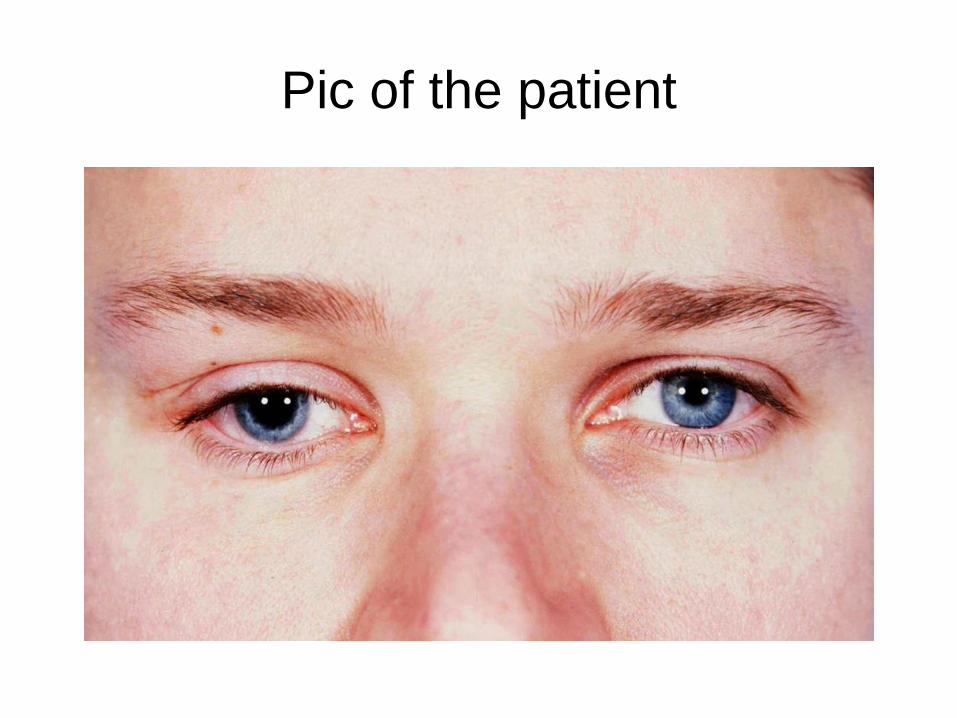
Pic of the patient
Quiz 4 & algorithm
• 78 year old woman presents with a watery
right eye
• Whit next?

Pic of the patient
Mark Wright Consultant
Ophthalmologist Lothian Health
and Edinburgh University
Algorithm based clinical teaching does it work?
elos/nes 2.2.16
Role & training of optometrists
• Optometrists are extending their role both diagnostically
and therapeutically & slowly taking over the role of GPs
in managing ‘primary care ophthalmology’
• Greater clinical expertise required by the 2006 GOS
contract however HES reluctant to devote time to
optometry/orthoptic teaching because of service
pressures
• Could algorithm based clinical teaching help?
Is there a place for diagnostic
algorithms in ophthalmology? • A partial solution to the ever increasing pressure on
hospital eye services (HES) is to improve the partnership between community optometrists and HES
• The following slides illustrate the results of three
prospective clinical trials which document the accuracy of the Edinburgh Eye Algorithms (5) when used by inexperienced clinicians in the three most commonly encountered clinical scenarios; red eye (s), visual loss and diplopia
• They highlight the existing diagnostic deficiencies within
our referral groups and demonstrate the significant improvement in these deficiencies when our simple diagnostic algorithms are applied to patients presenting with red eye (s), visual loss and diplopia
Edinburgh Red Eye Algorithm
• Baseline diagnostic accuracy for non ophthalmologists for patients presenting with AACG was 21% (GPs) – 64% (A&E)1 and for iritis (GPs) 44%2
• When equally inexperienced observers (GP 35%, A&E nurse practitioners 23%, opticians 18% etc) assessed patients presenting with red eye (s) using the Edinburgh Red Eye Diagnostic Algorithm the diagnostic accuracy for AACG rose to 100% (4/4 cases) and for iritis rose to 82% (9/11 cases)
• For all causes of red eye (s) the overall diagnostic accuracy was 72% (28/39)3
1 Siriwardena D, Arora AK, Fraser SG, McClelland HK, Claoue C. Misdiagnosis of acute angle closure glaucoma. Age Ageing. 1996;25(6):421-3.
2 Sheldrick JH, Vernon SA, Wilson A. Study of diagnostic accord between general practitioners and an ophthalmologist.
BMJ.1992; 304:1096-1098. 3 Accuracy of the Edinburgh Red Eye Algorithm. Eye 2015; 29: 619-624.
Edinburgh Visual Loss Diagnostic Algorithm
• The overall pre-algorithm diagnostic accuracy of referrers assessing patients presenting with visual loss was 51% (30/59). Individual accuracy was; optoms 67%, A&E doctors 33%, GPs 13%, other hospital specialties 0%
• The diagnostic accuracy improved to 84% (57/68) when inexperienced observers (4th year medical student 45% [31/68], junior ophthalmology trainee 37% opticians 18%) assessed the same cohort of patients using the Edinburgh Visual Loss Diagnostic Algorithm4
• The algorithm correctly diagnosed: retina in 71% of cases (5/7), macula in 86% (25/29), peripheral retina in 100% (2/2), optic nerve in 71% (5/7), media opacity in 89% (16/18), post chiasmal in 100% (4/4) and refractive error in 0% (0/1)
• Accuracy of diagnosis was similar for each algorithm user; medical student 81%, inexperienced ophthalmology trainee 84% and optometrist 92%.
4 The Accuracy of the Edinburgh Visual Loss Diagnostic Algorithm. Accepted for publication in Eye July 2015
Edinburgh Diplopia Diagnostic Algorithm
• The overall pre-algorithm diagnostic accuracy of referrers assessing patients presenting with diplopia was 24% (10/41). Individual accuracy was; A&E & other hospital doctors 20%, GPs 44%, optoms 36%. In 54% of the cases (22/41) the referrer did not make an attempt to diagnose the cause of the diplopia.
• The diagnostic accuracy improved to 82% (37/45) When
inexperienced observers (FY2 & 5th year medical student) assessed the same cohort of patients using the Edinburgh Diplopia Diagnostic Algorithm5
• The algorithm correctly diagnosed: CN III palsy in 6/6, CN IV palsy
in 7/8, cranial nerve (CN) VI palsy in 12/12, internuclear ophthalmoplegia in 2/2, restrictive myopathy in 4/4, media opacity in 1/1 and blurred vision in 3/3. The 7 incorrect diagnoses included; myasthenia gravis, Miller Fisher Syndrome,‘post head injury diplopia’ and two cases of dual CN (CN 111 & IV and 111 & VI) palsies.
• 5 The Accuracy of the Edinburgh Diplopia Diagnostic Algorithm; accepted eye January 2016
Edinburgh Eye Algorithms
• These are the first diagnostic eye algorithms to be subjected to scientific analysis and lead to significant improvements in the diagnostic accuracy of inexperienced clinicians in the three most commonly encountered ophthalmic scenarios
• We have offered these algorithms to all interested
parties; RCOph, College of Optometrists, RCEMedicine, RCGP etc. with an app under development
• A number of open access learning tools including
downloadable copies of the 5 diagnostic algorithms and narrated lectures accompanying the algorithms are available at https://www.eemec.med.ed.ac.uk/pages/resources/mw-ophthalmology-page
Approach to patients presenting
with red eye(s) • KEY POINTS IN THE OCULAR EXAMINATION AND
DECISION MAKING POINTS IN THE RED EYE ALGORITHM
• Unilateral vs bilateral redness
• Always look at the lids before the eye(s)!
• Presence of fluorescein staining esp. if the cornea is clear
• Corneal appearance; clear or hazy; focally or diffusely hazy
• Difference in the pupil size (anisocoria)
• Presence of photophobia
• (Pattern of redness; diffuse or sectorial)
• Direct ophthalmoscope gives an illuminated magnified view
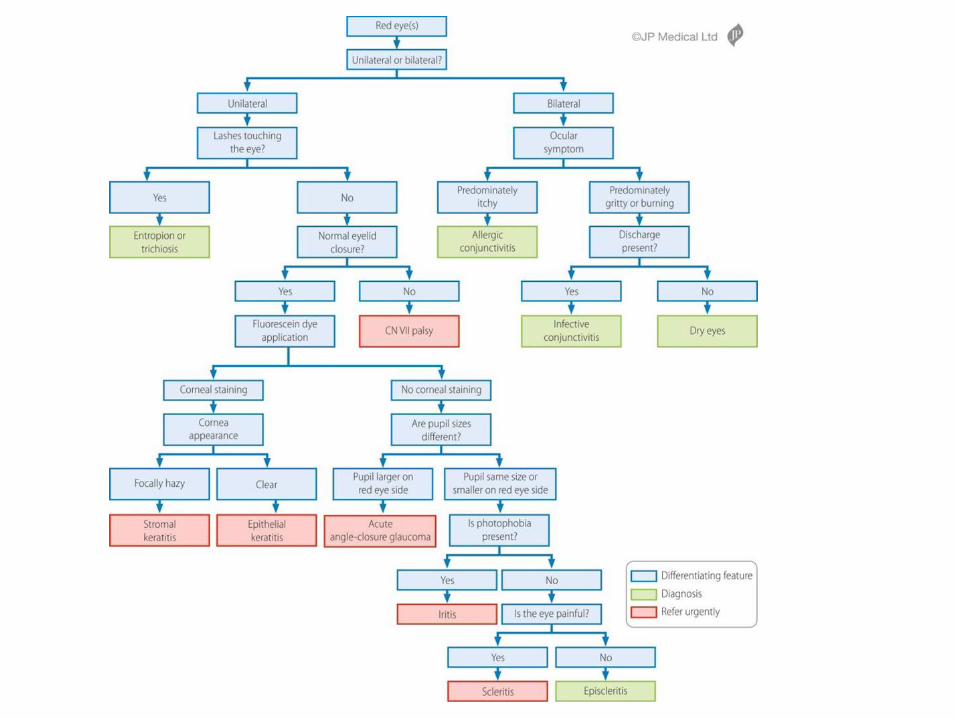
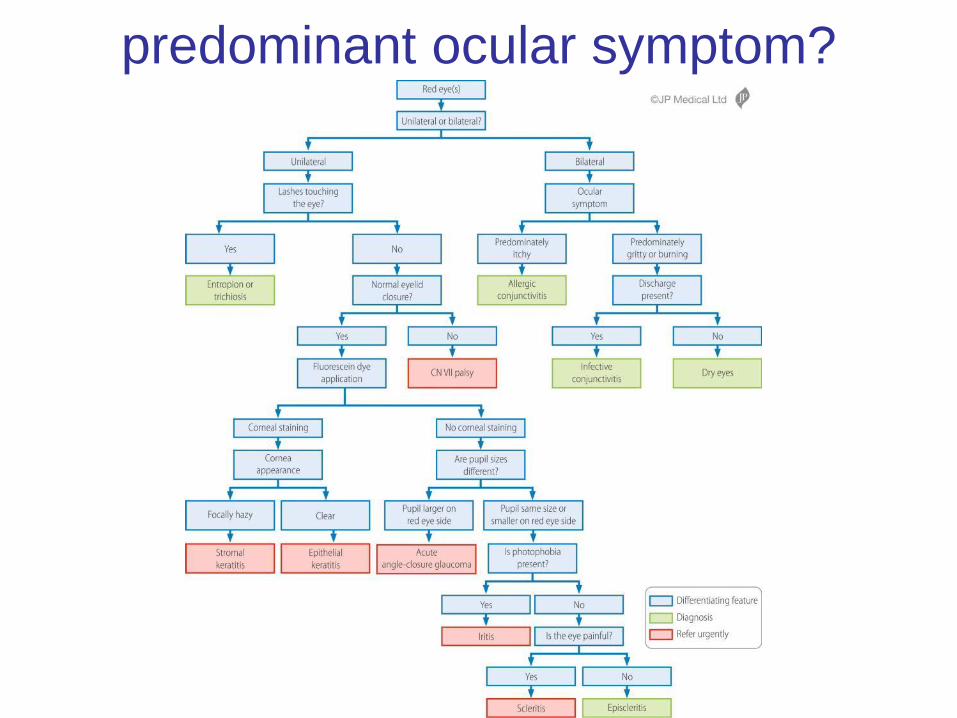
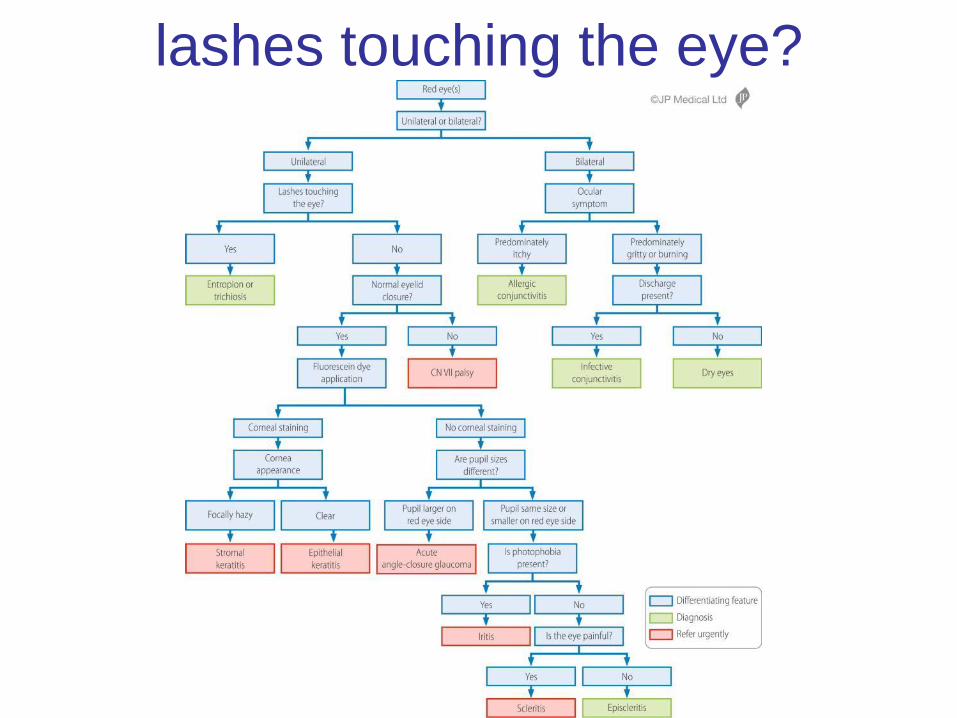
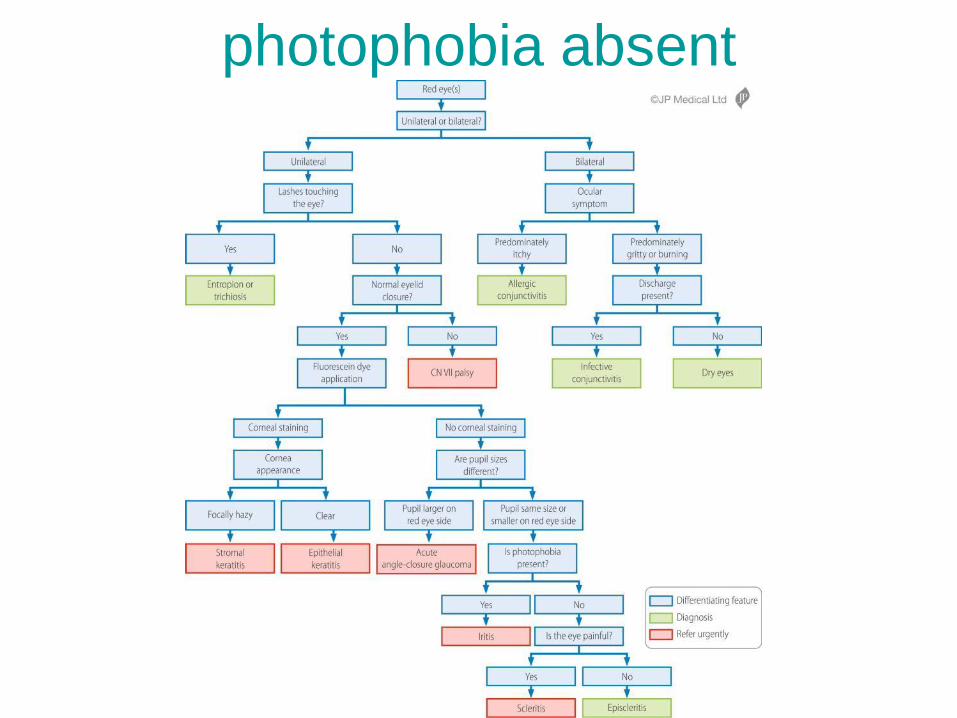
Red Eye Algorithm
2 practical skills
• Careful observation!
• Use of fluorescein dye
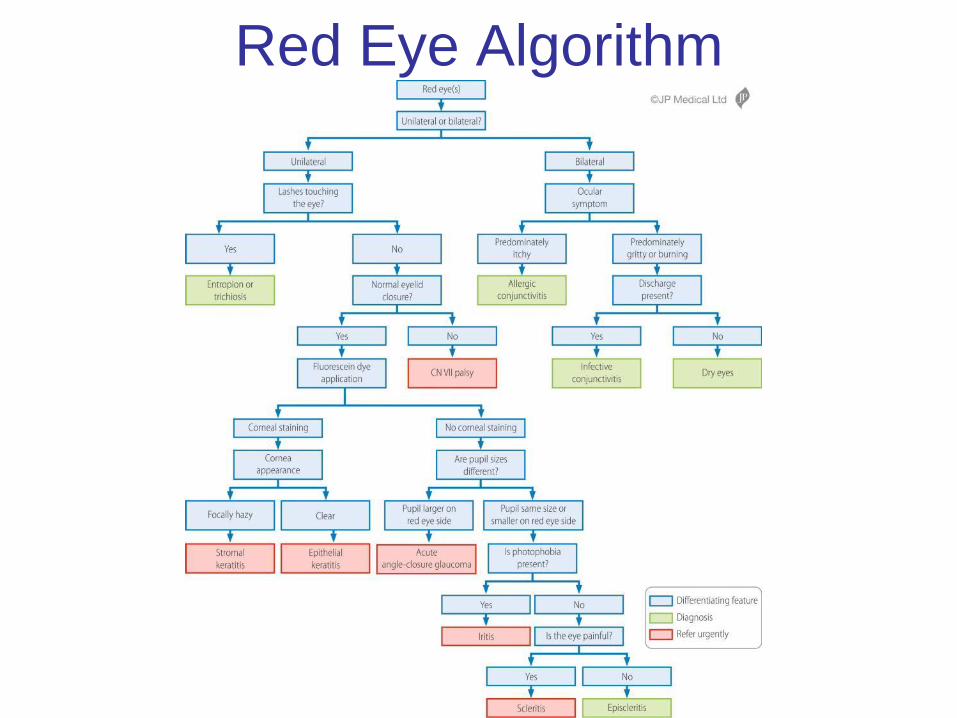
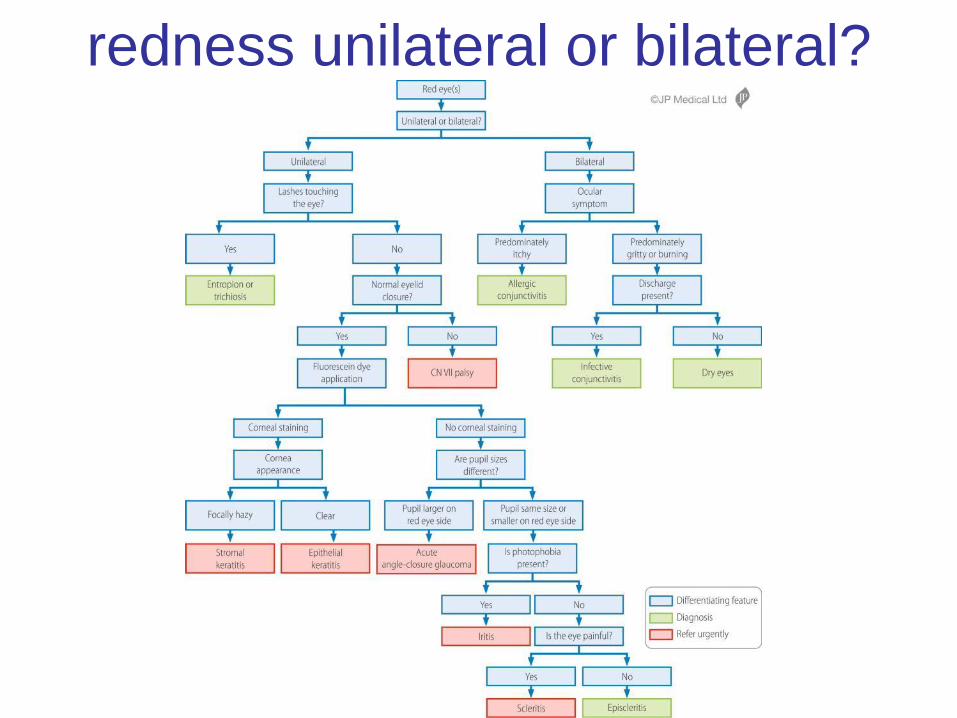
Red Eye Algorithm
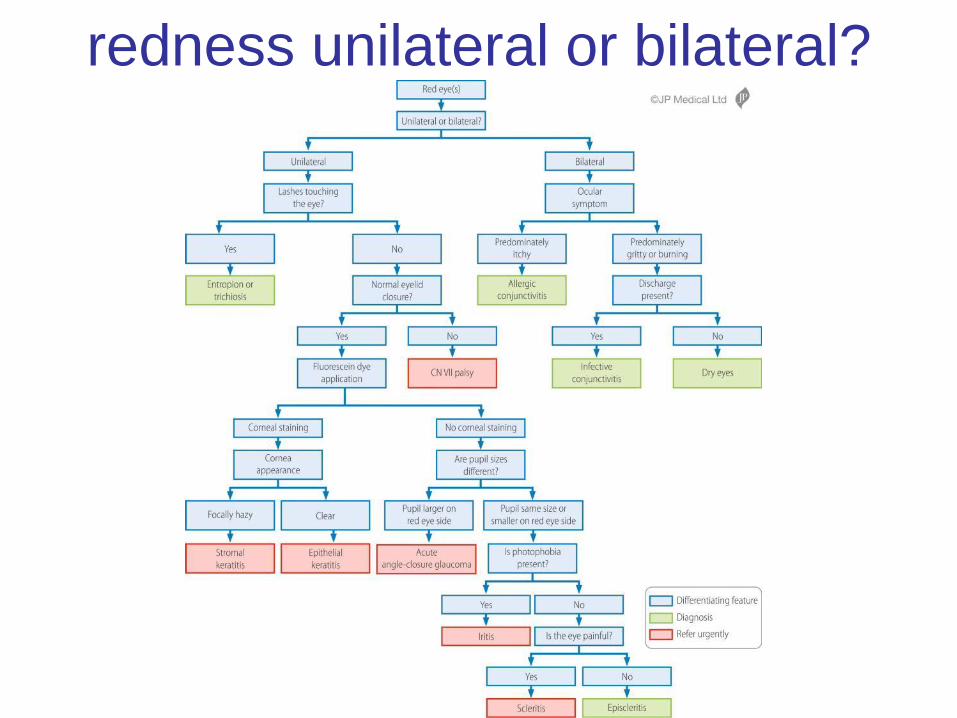
redness unilateral or bilateral?

Redness unilateral or bilateral?
bilateral red eyes
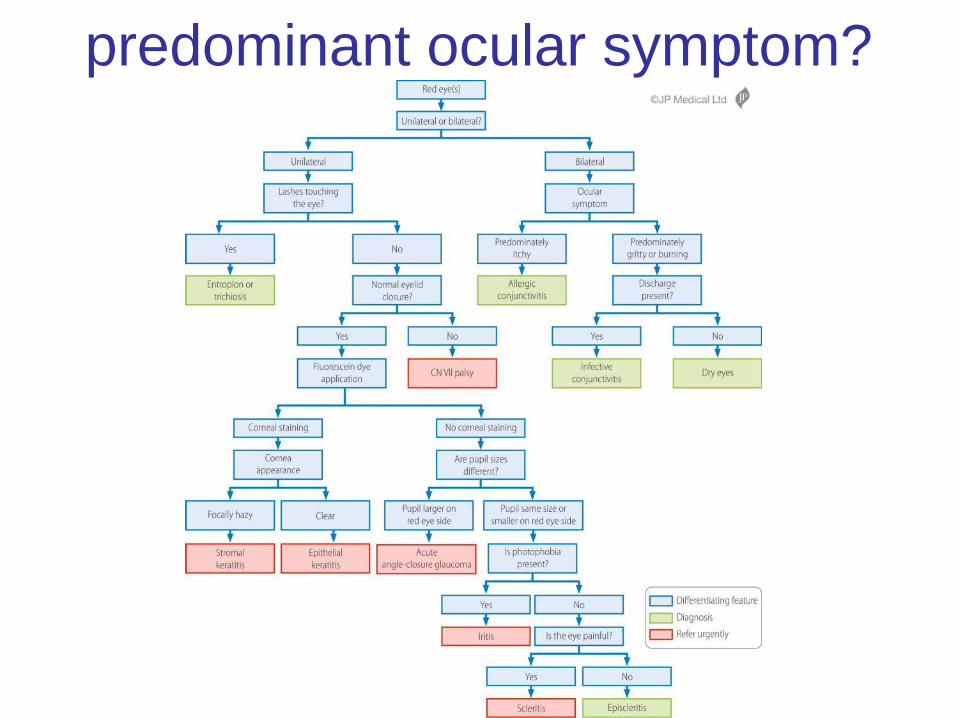
predominant ocular symptom?
predominant symptom itch
• allergic conjunctivitis which is;
• often associated with atopy; asthma, eczema and hay fever
• can be associated with a stringy more than a purulent discharge
• treatment is allergen avoidance if possible and optanolol drops if not
predominant ocular symptom?
predominant symptom gritty
and burning with discharge
present
• infectious conjunctivitis
• the discharge is usually purulent
• very difficult to distinguish bacterial from viral on clinical grounds
• Most will settle with no treatment, if it fails to improve topical chloromycetin drops during the day and ointment at night
• Swab for chlamydia if symptoms persist
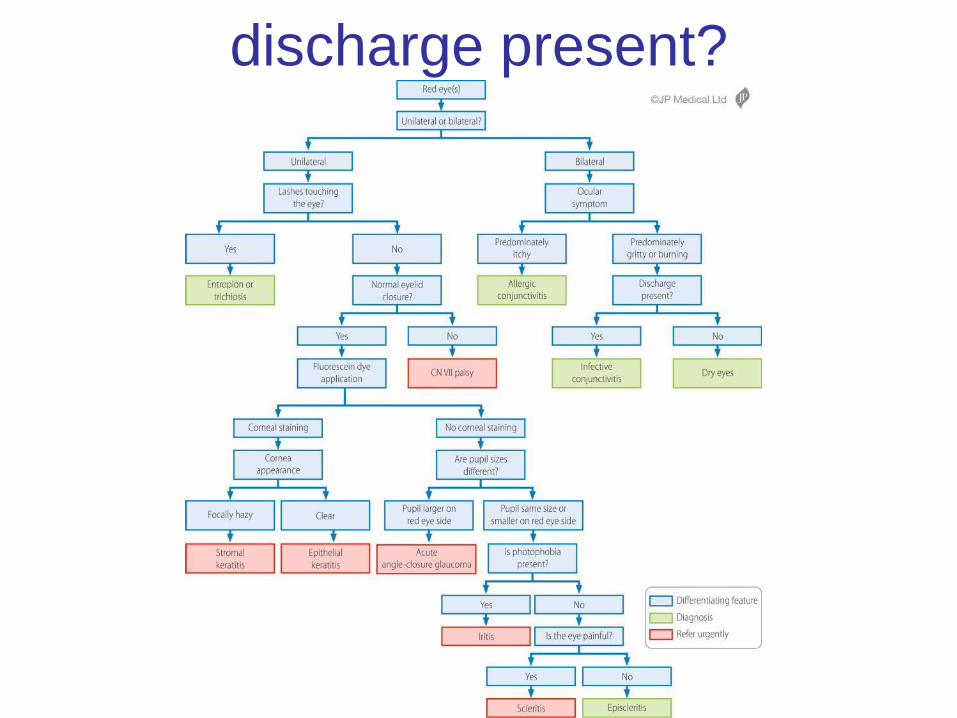
discharge present?
predominant ocular symptom
gritty and burning with no discharge
• dry eyes
• eyes are minimally red
• almost always in older patients
• Unilateral only in the presence of incomplete
closure i.e. facial nerve palsy
• Treatment is long term ocular lubricants;
viscotears during the day and lacrilube at night
redness unilateral or bilateral?
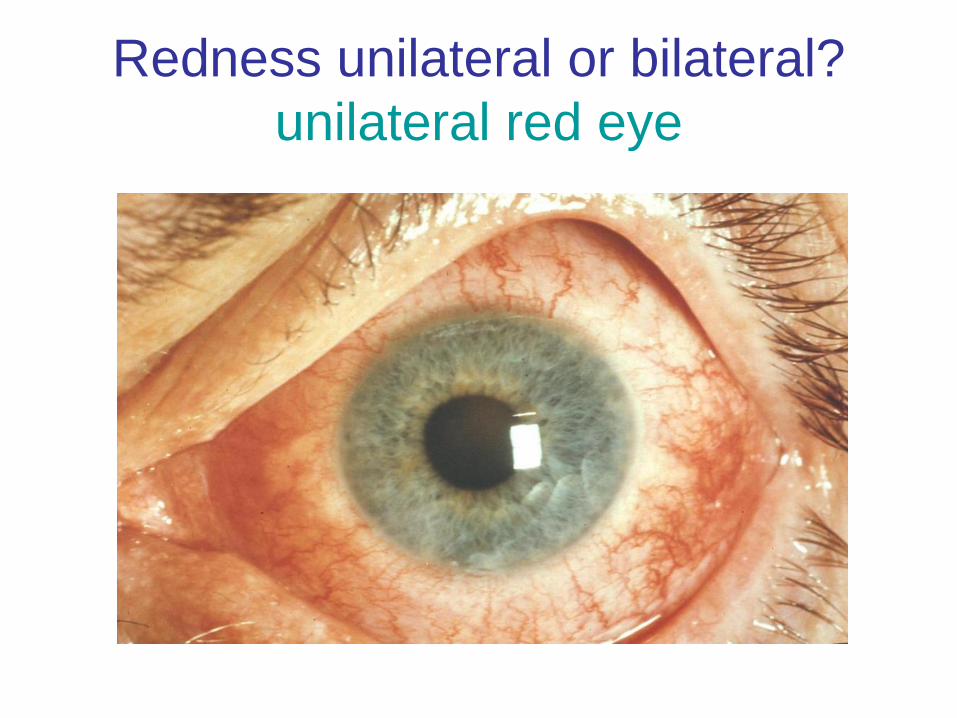
Redness unilateral or bilateral?
unilateral red eye
Red eye; signs
• The second thing to
check in a patient with
a red eye(s) is……….

Red eye; signs-look at the
lids! • Lid margin lesions
• Entropion/trichiasis
• Lagophthalmos
lashes touching the eye?
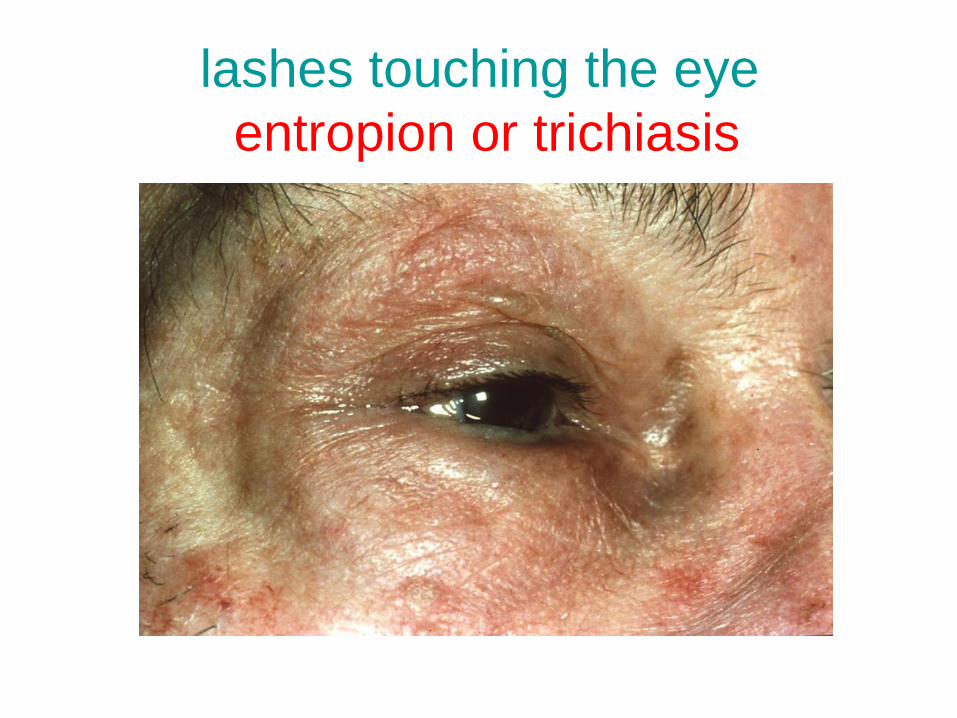
lashes touching the eye
entropion or trichiasis
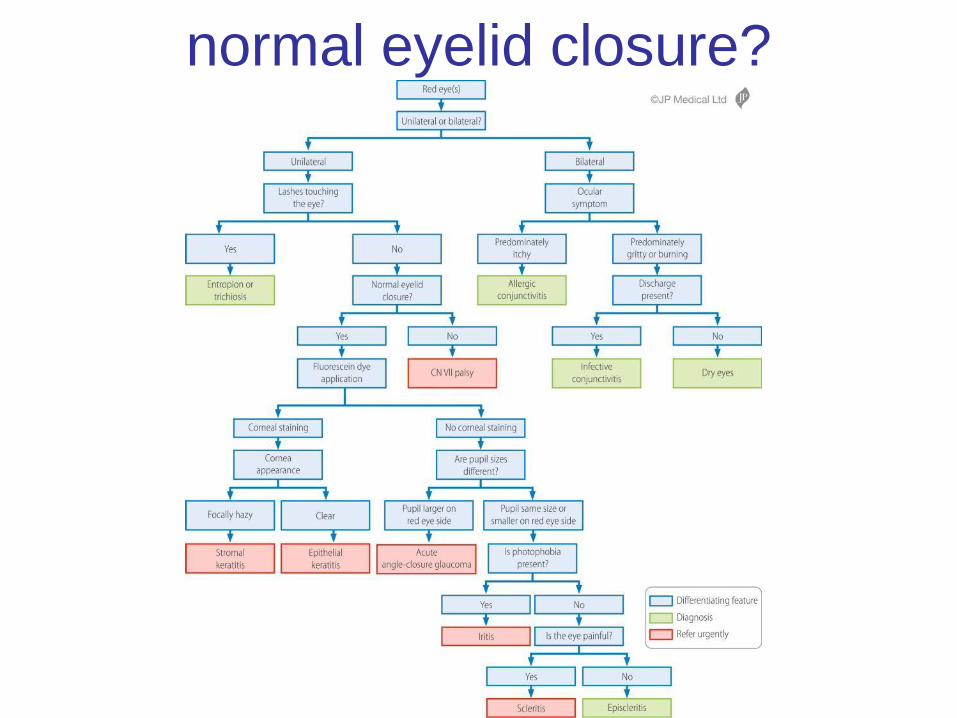
normal eyelid closure?
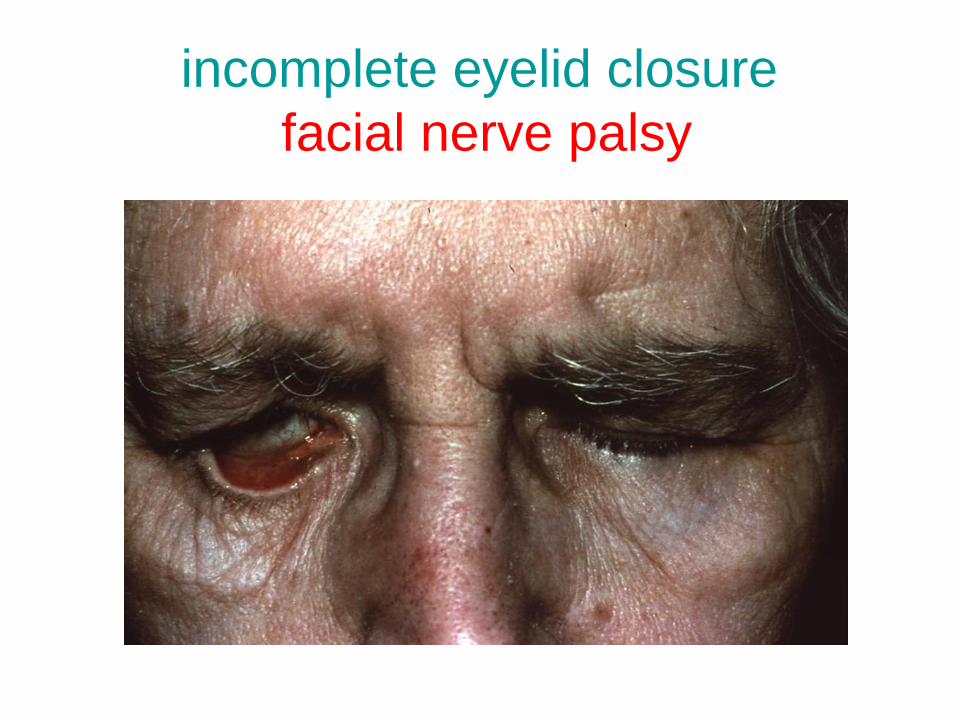
incomplete eyelid closure
facial nerve palsy
Red eye(s); the most important
single thing to do to a red eye(s)
is…………
1. Check the vision
2. Digitally estimate the intraocular
pressure
3. Instil fluorescein dye
4. Evert the lid looking for a sub tarsal F.B.
5. Check the pupil reactions
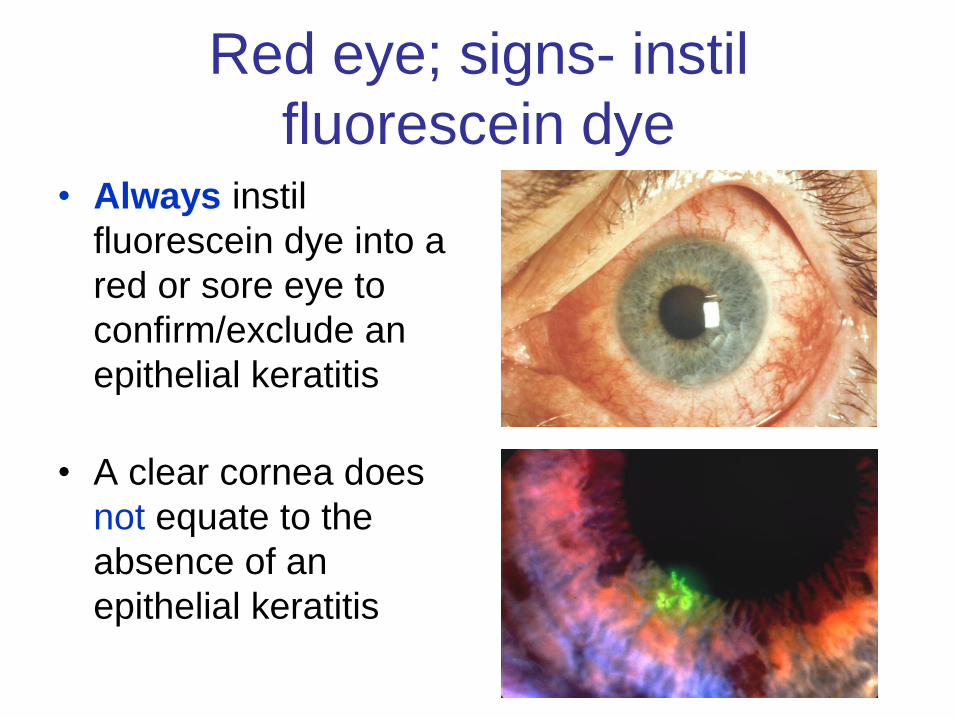
Red eye; signs- instil
fluorescein dye • Always instil
fluorescein dye into a
red or sore eye to
confirm/exclude an
epithelial keratitis
• A clear cornea does
not equate to the
absence of an
epithelial keratitis
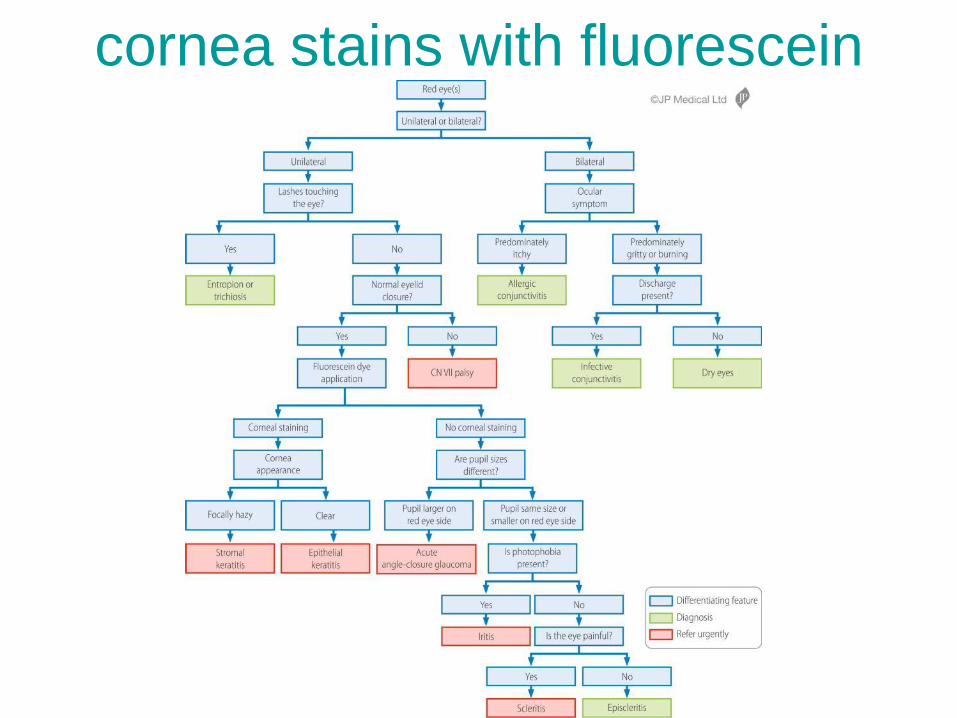
cornea stains with fluorescein
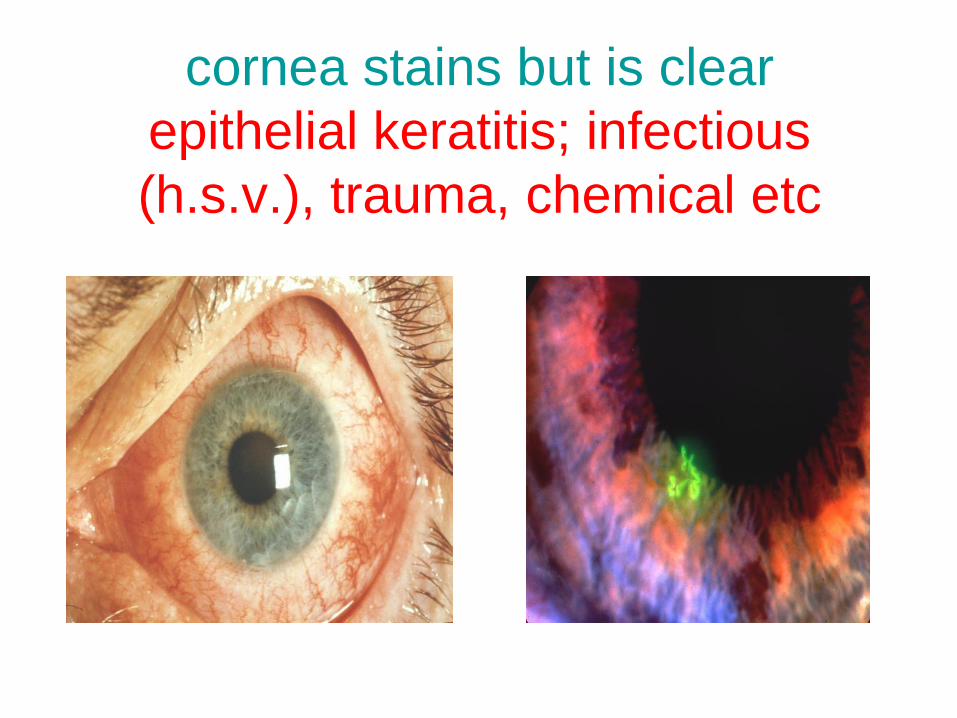
cornea stains but is clear
epithelial keratitis; infectious
(h.s.v.), trauma, chemical etc

cornea stains and is hazy
stromal keratitis; abscess
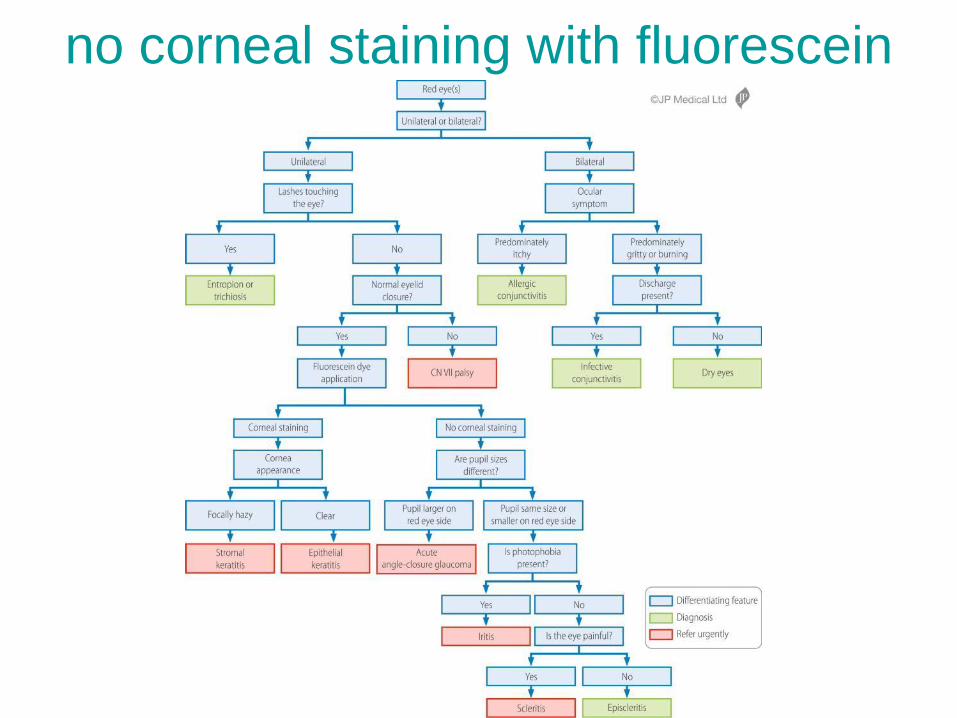
no corneal staining with fluorescein
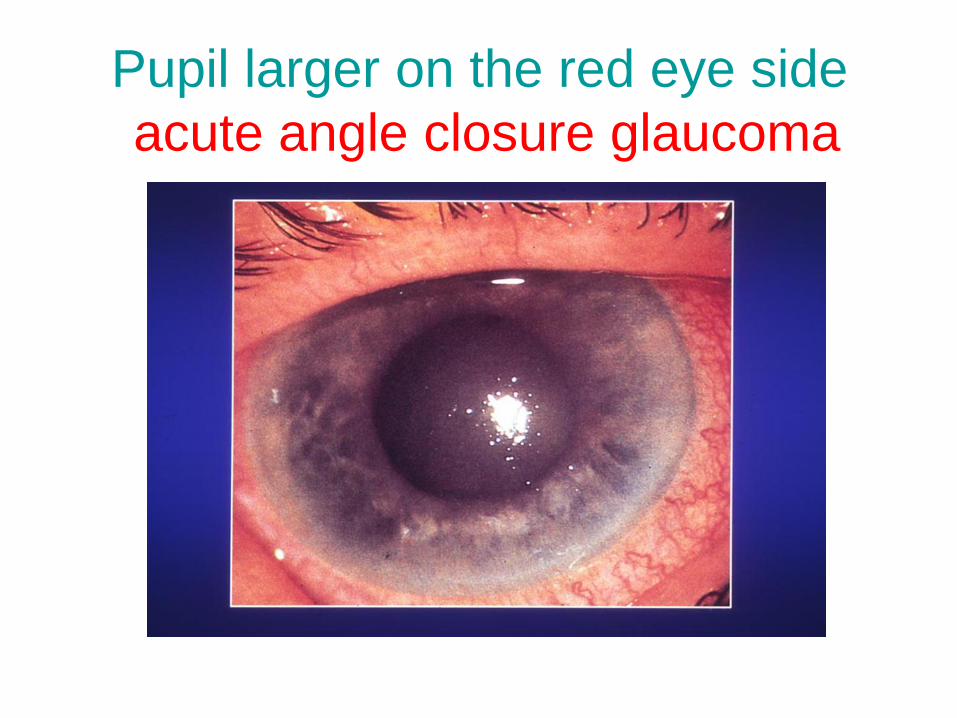
Pupil larger on the red eye side
acute angle closure glaucoma
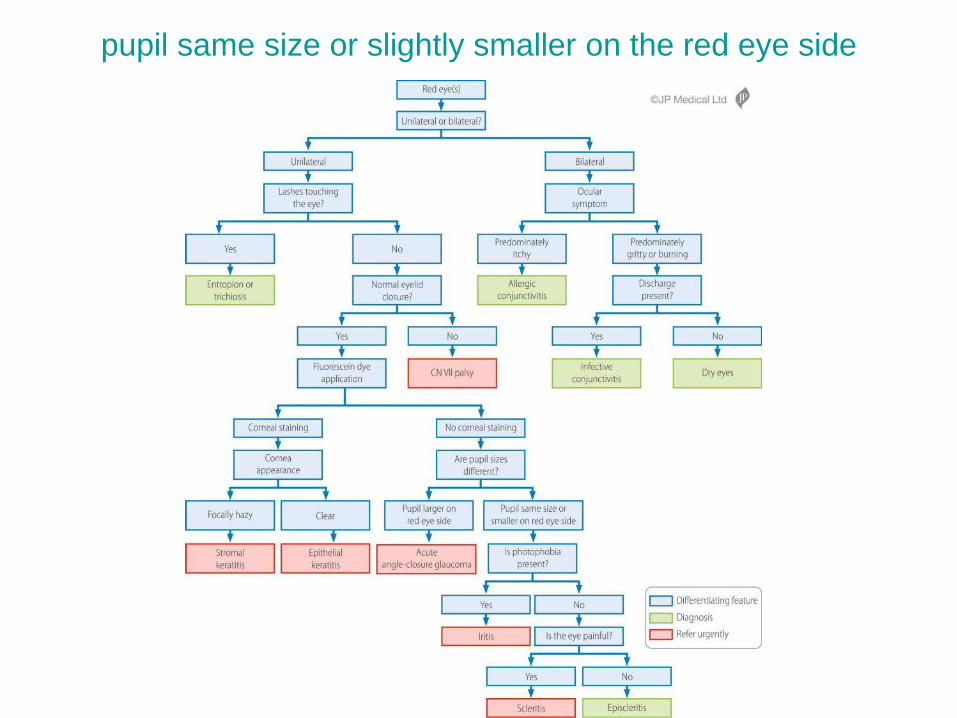
pupil same size or slightly smaller on the red eye side
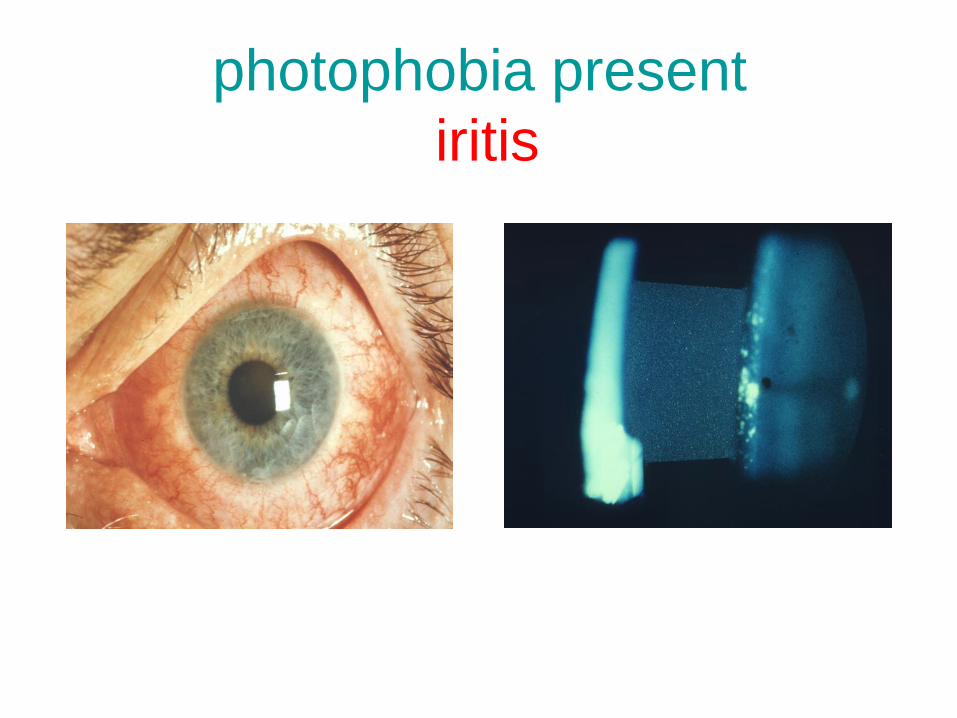
photophobia present
iritis
photophobia absent
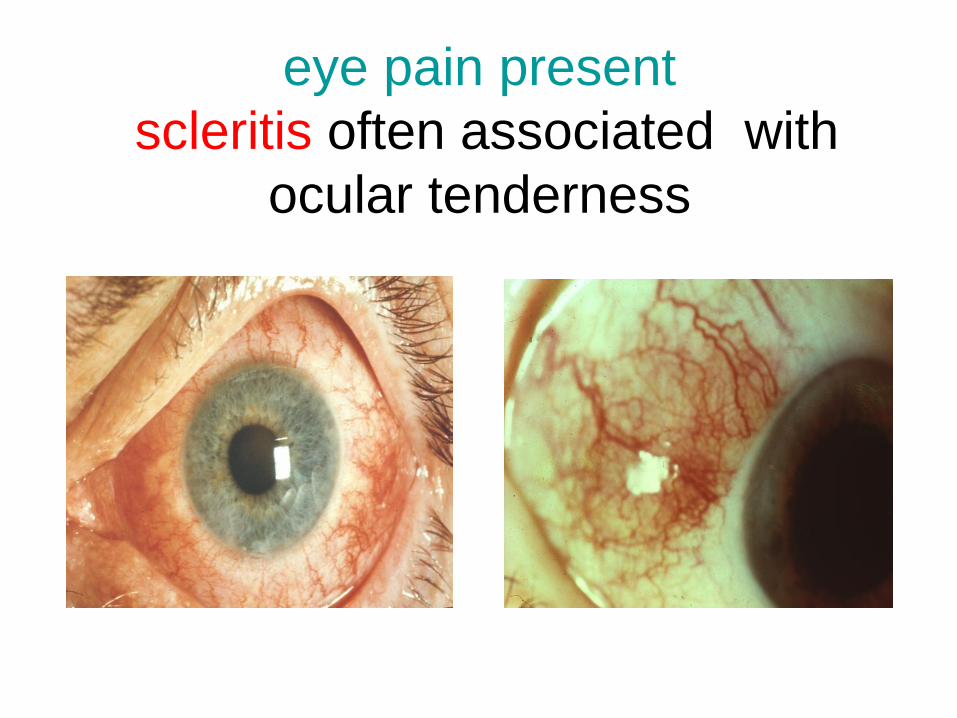
eye pain present
scleritis often associated with
ocular tenderness
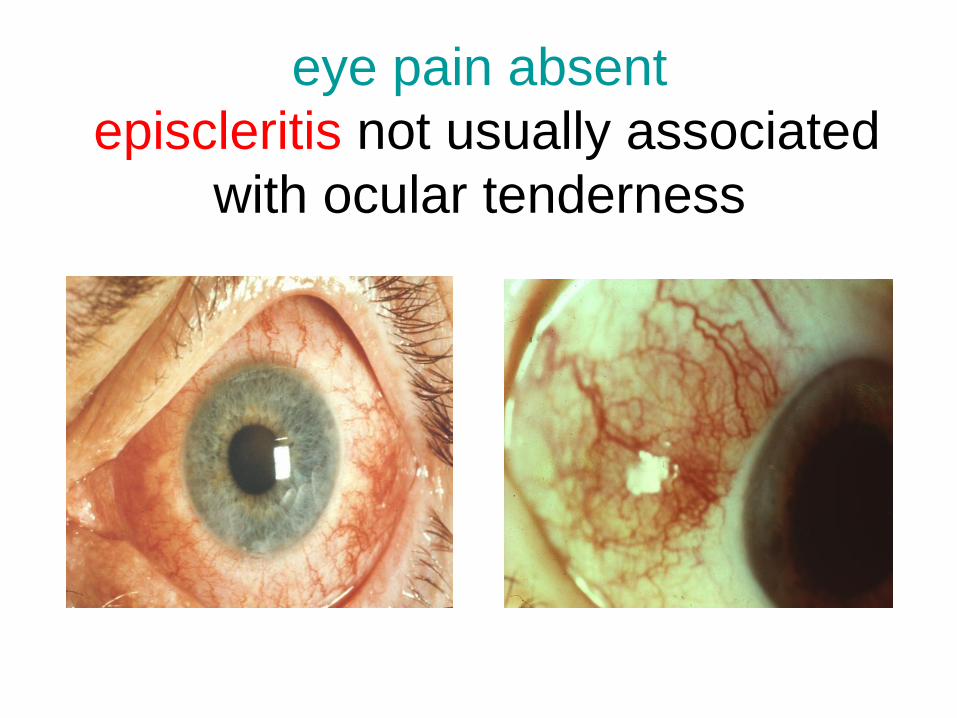
eye pain absent
episcleritis not usually associated
with ocular tenderness
Approach to patients
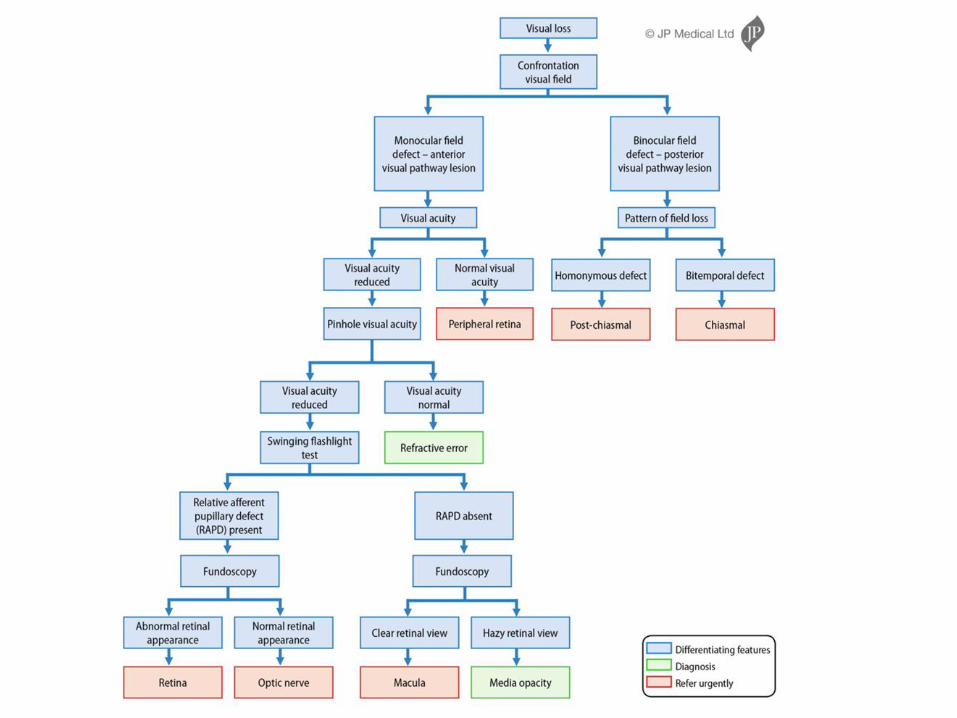
presenting with visual loss
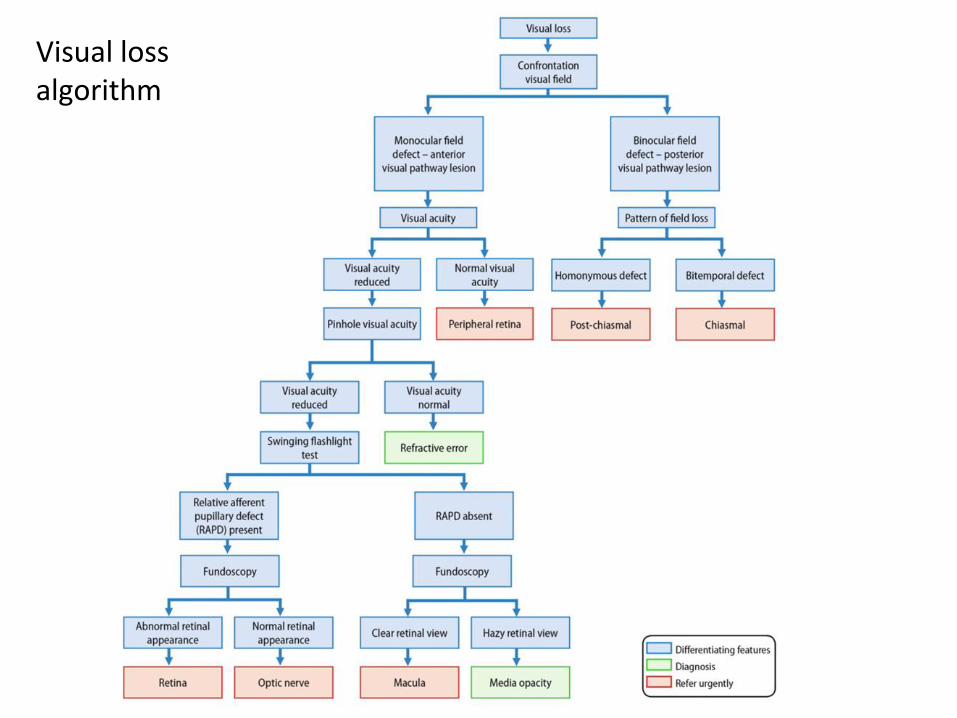
• Key step is to map out the patient’s visual field defect using confrontational visual fields which will allow you to locate which part of the visual pathways are affected
• Measure the visual acuity and if reduced again with the pinhole
• The only specialised test required is the swinging flashlight test to determine whether an RAPD is present
• Lastly, use the history and PMH/age etc to best guess the likely cause and then confirm using the ophthalmoscope
Visual Loss Algorithm
4 practical skills
• Confrontational visual field
• Visual acuity
• Pupil reactions (rapd)
• Fundoscopy
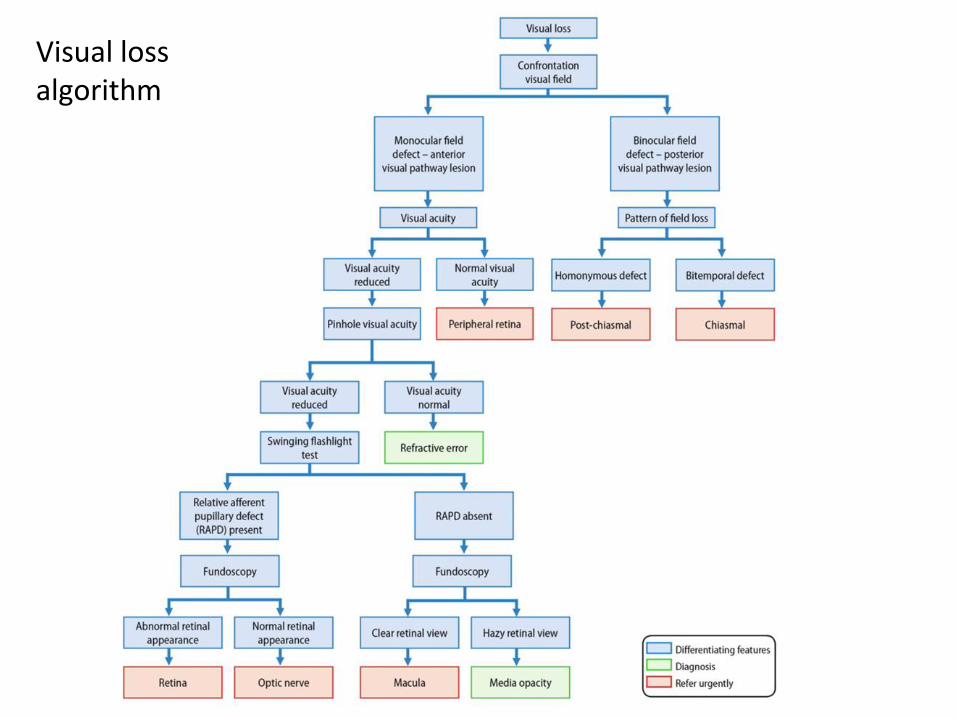
Visual loss algorithm
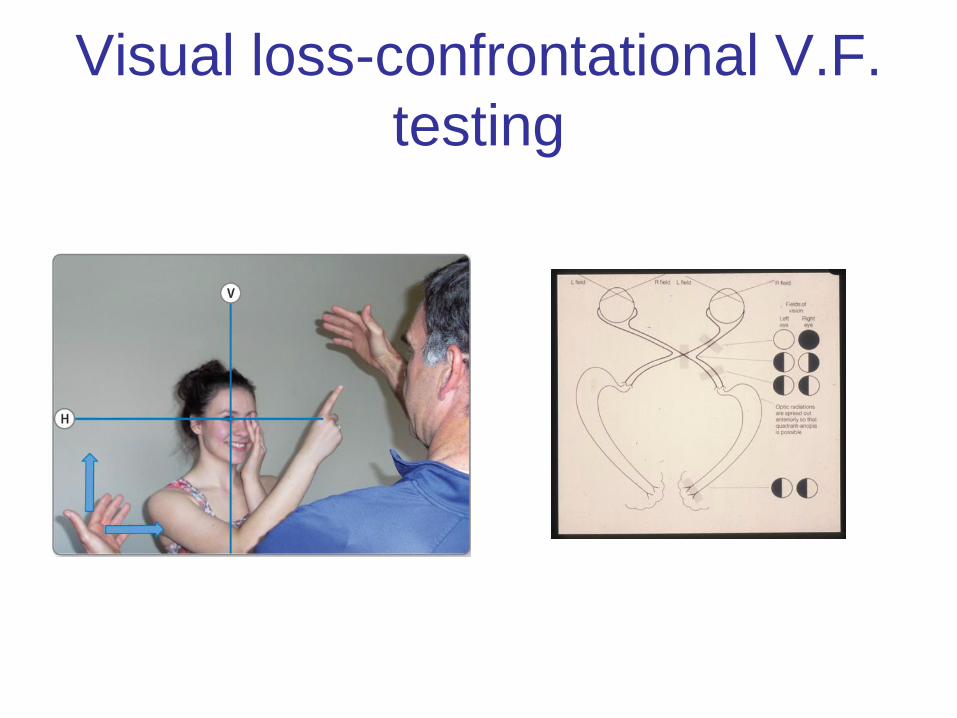
Visual loss-confrontational V.F.
testing
Visual loss-swinging flashlight
test (RAPD)
• Run the video clip of the RAPD
Visual loss algorithm
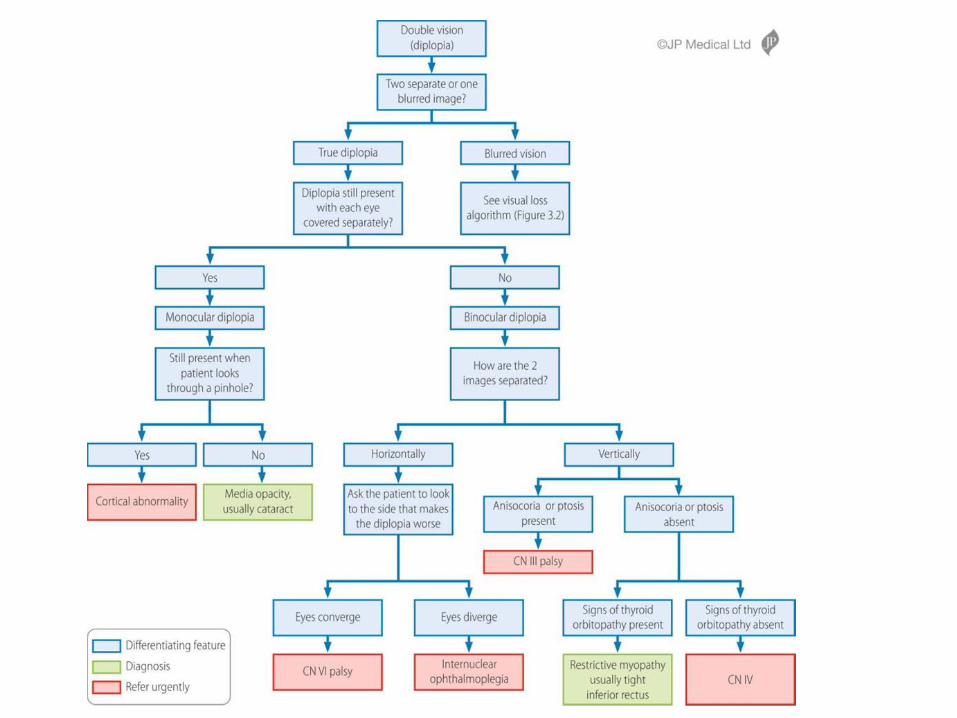
Approach to patients presenting with
diplopia; clarify the history
• Clarify the patient means they see two separate
images i.e. true diplopia and not one blurred image
• Secondly ask if when the patient covers each eye
separately the double image goes i.e is the diplopia
monocular or truly binocular
Diplopia Algorithm
1 practical skill
• Careful observation
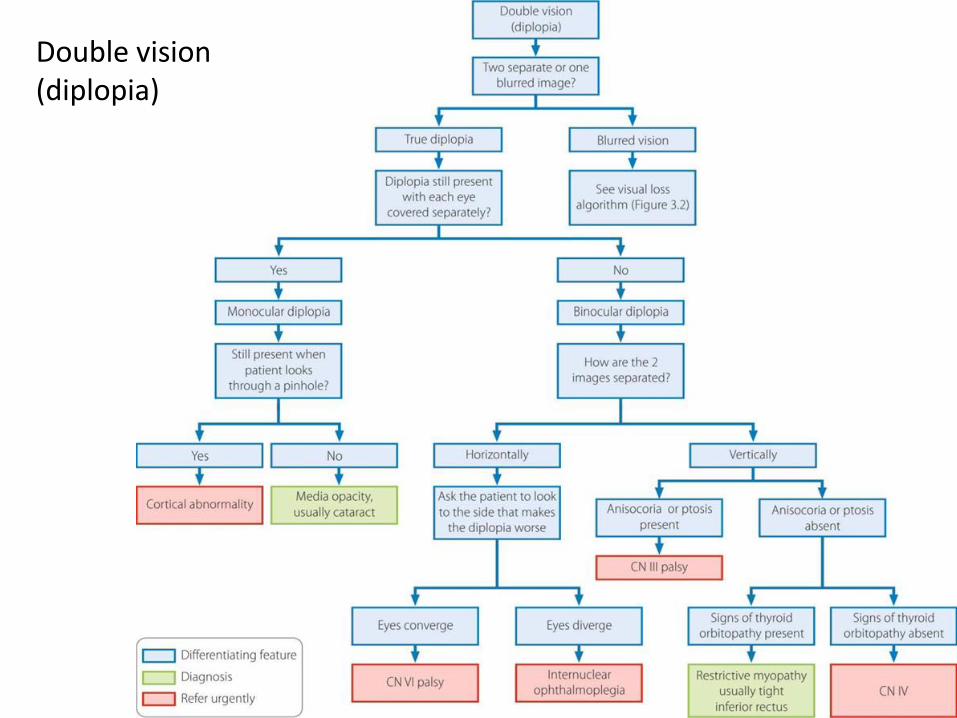
Double vision (diplopia)
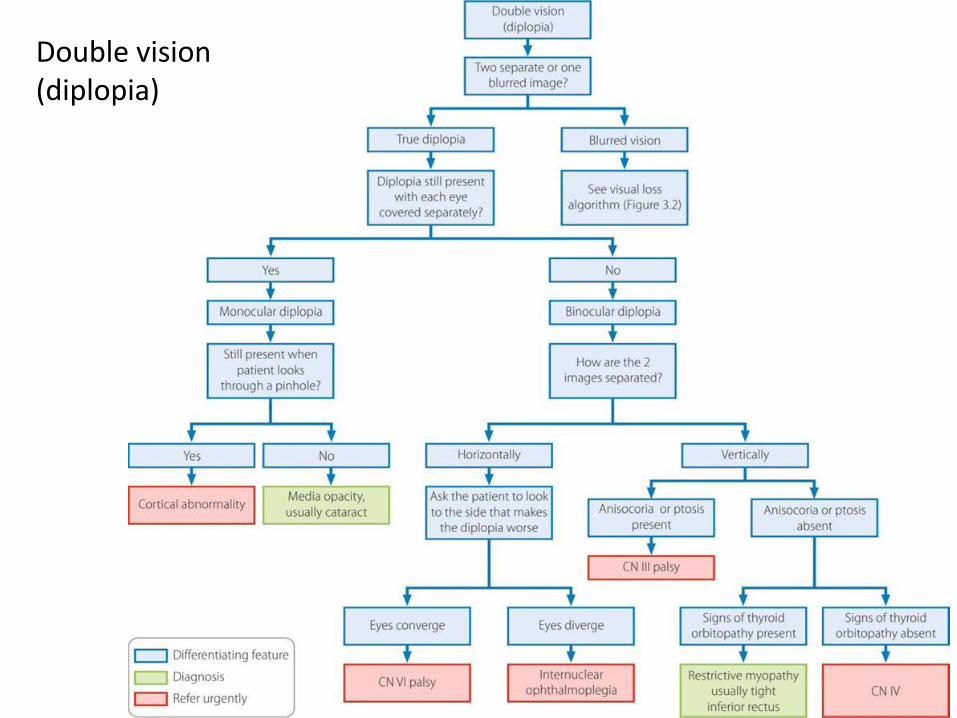
Double vision (diplopia)
Any Questions?
If time, quiz time!
MW is your patient!
• A number of open access learning tools
including downloadable copies of the 5
diagnostic algorithms and narrated lectures
accompanying the algorithms are available
at
https://www.eemec.med.ed.ac.uk/pages/re
sources/mw-ophthalmology-page
Quiz 1
• 28 year old man presents with acute onset
diplopia
• What next?
Diplopia Algorithm
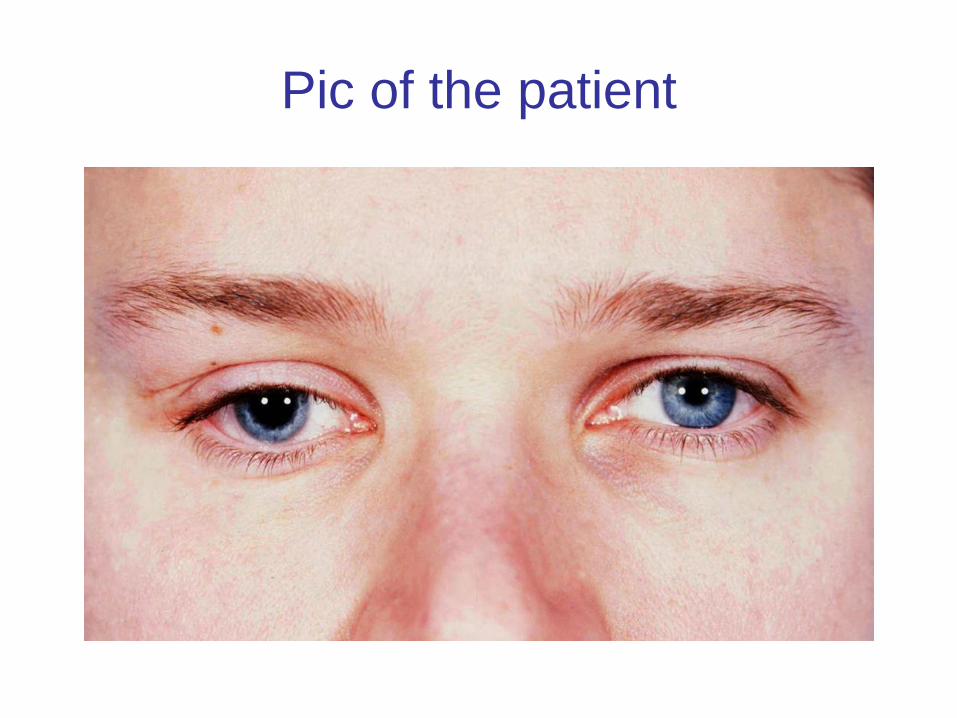
Pic of the patient
Quiz 2
• 68 year old man presents with sudden
painless loss of vision right eye
• What next?
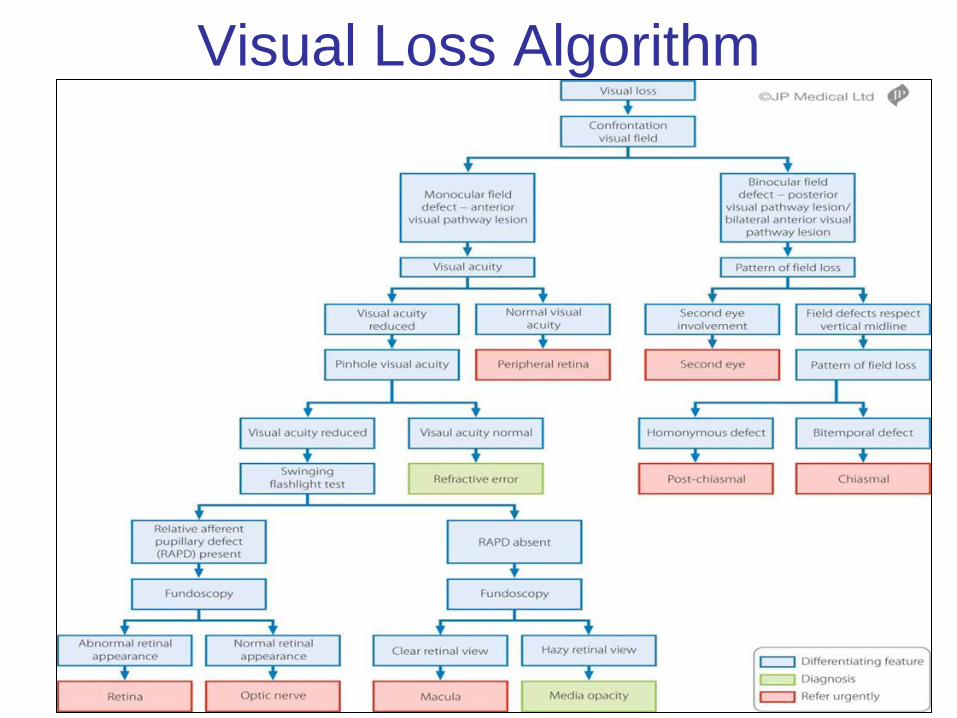
Visual Loss Algorithm
Quiz 2
• Show pupil reactions (RAPD video)
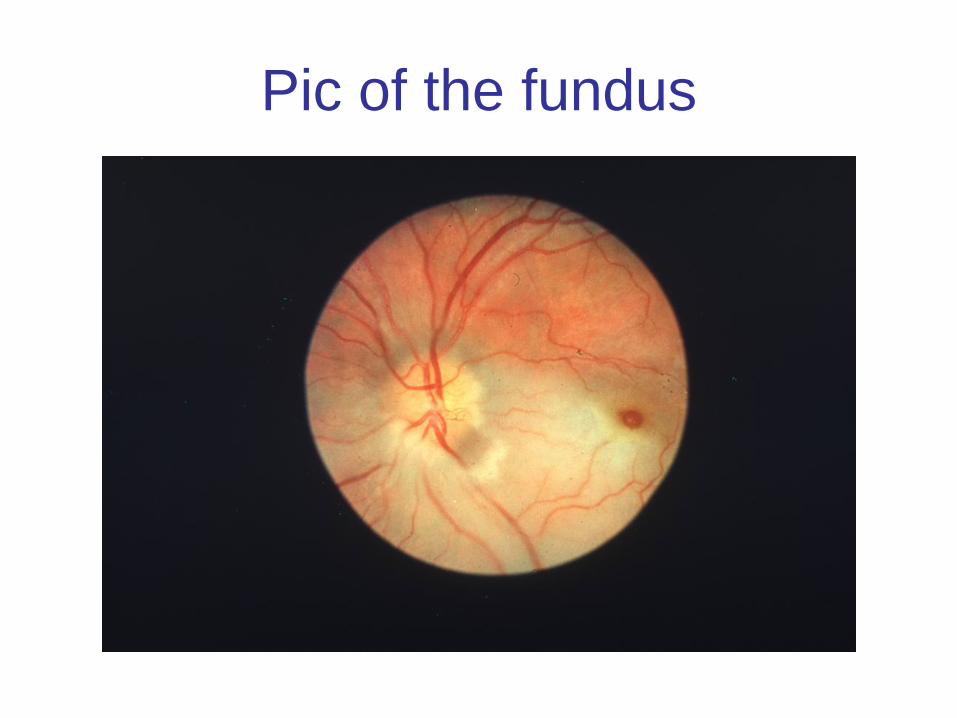
Pic of the fundus
Quiz 3
• 78 year old woman presents with painful
inflamed right eye
• What next?
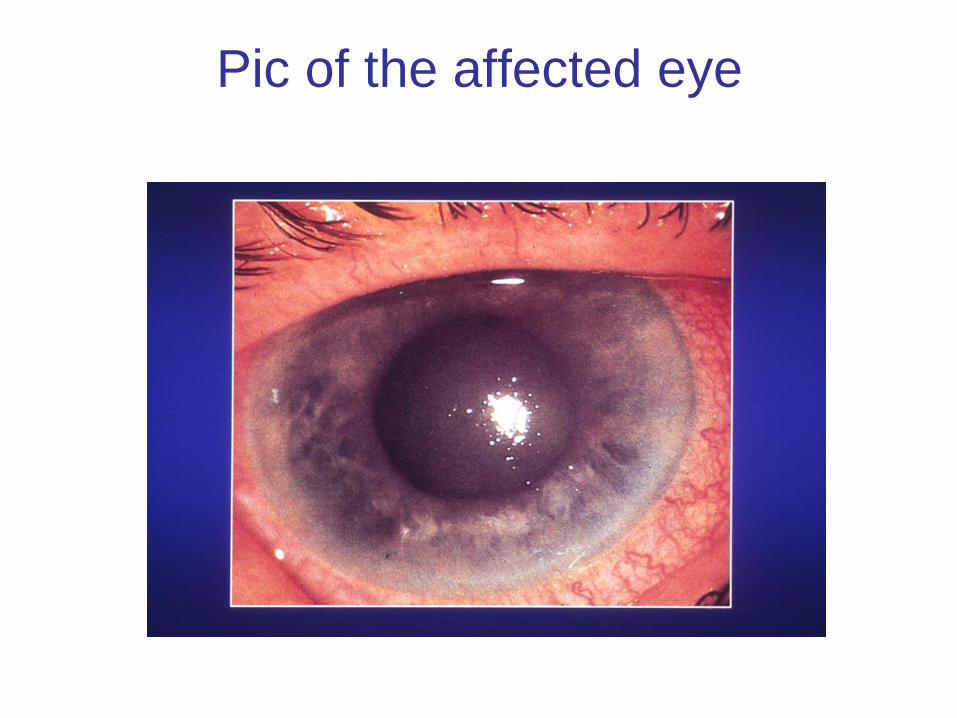
Pic of the affected eye
Quiz 4
• 8 year old boy presents with a difference
noted in his pupil sizes
• What next?
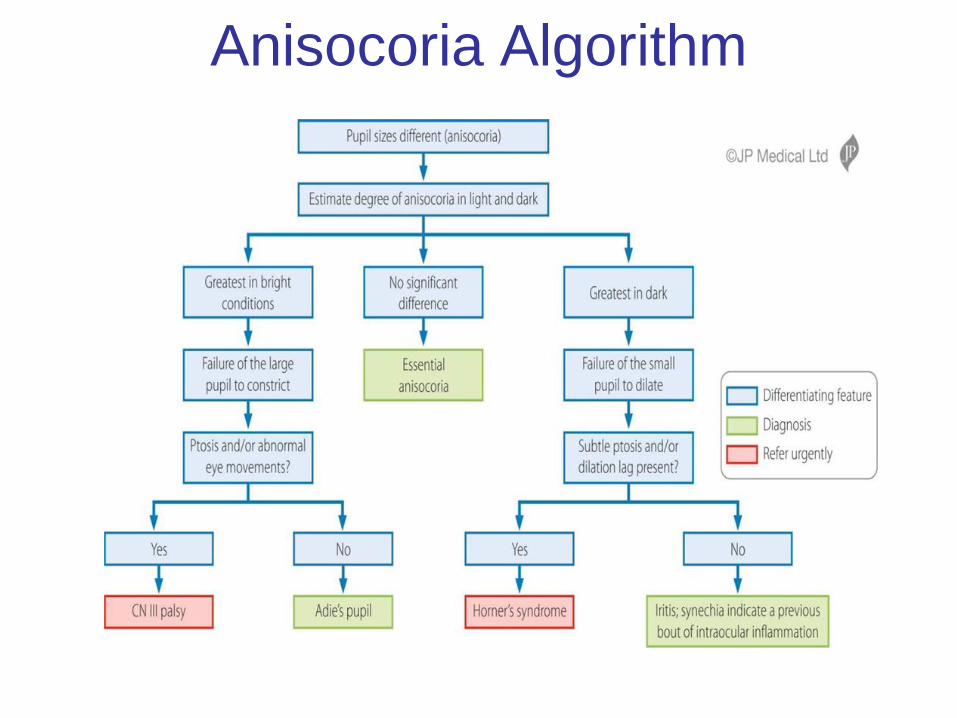
Anisocoria Algorithm
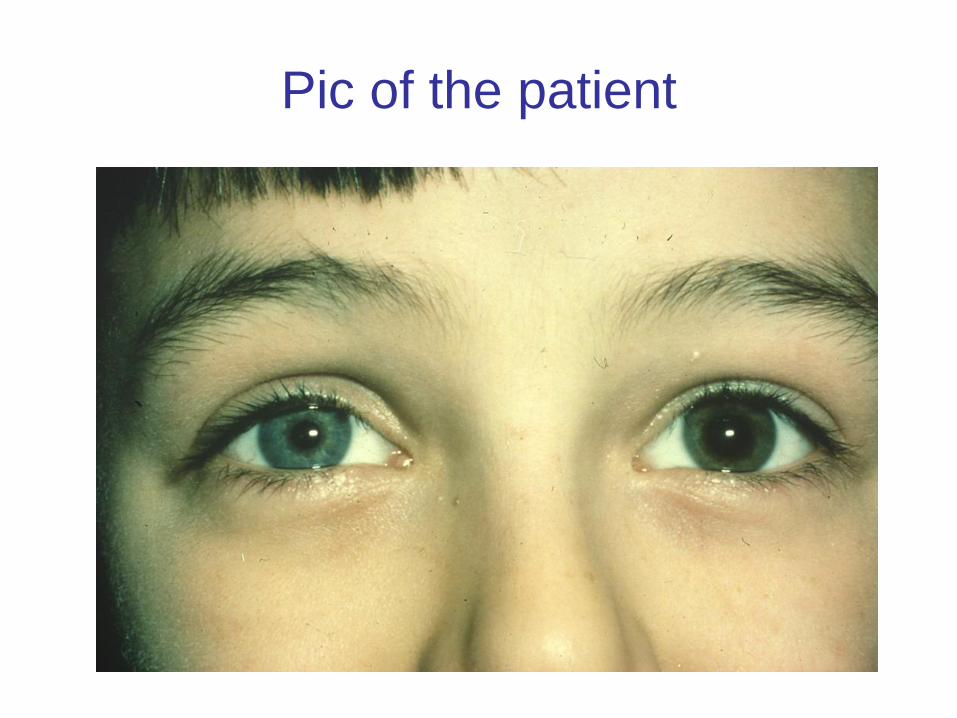
Pic of the patient
Quiz 5
• 78 year old woman presents with a watery
right eye
• What next?
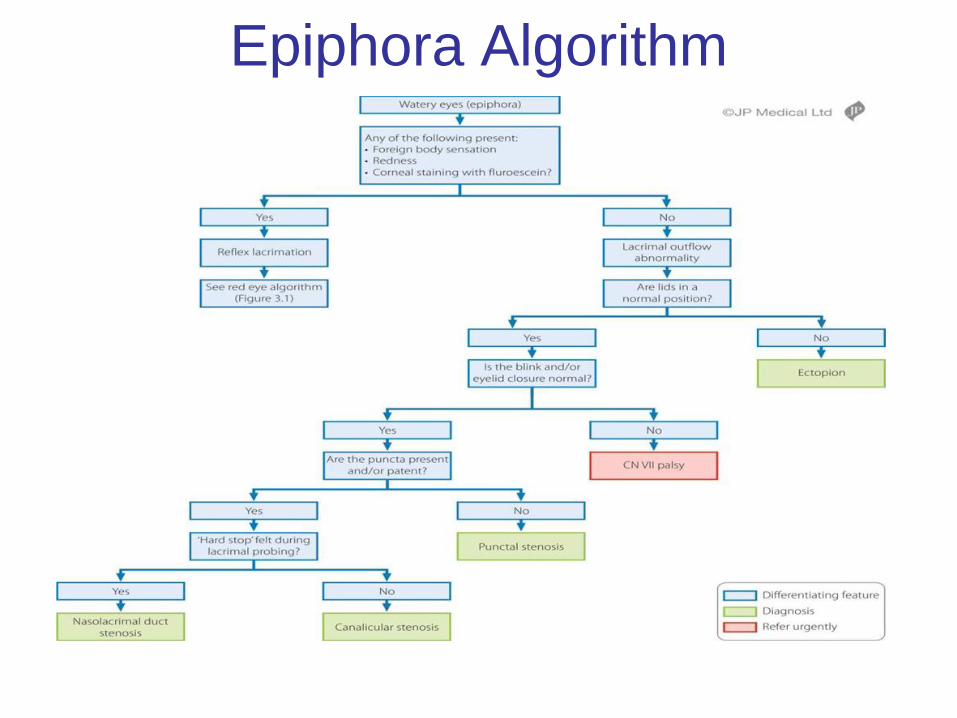
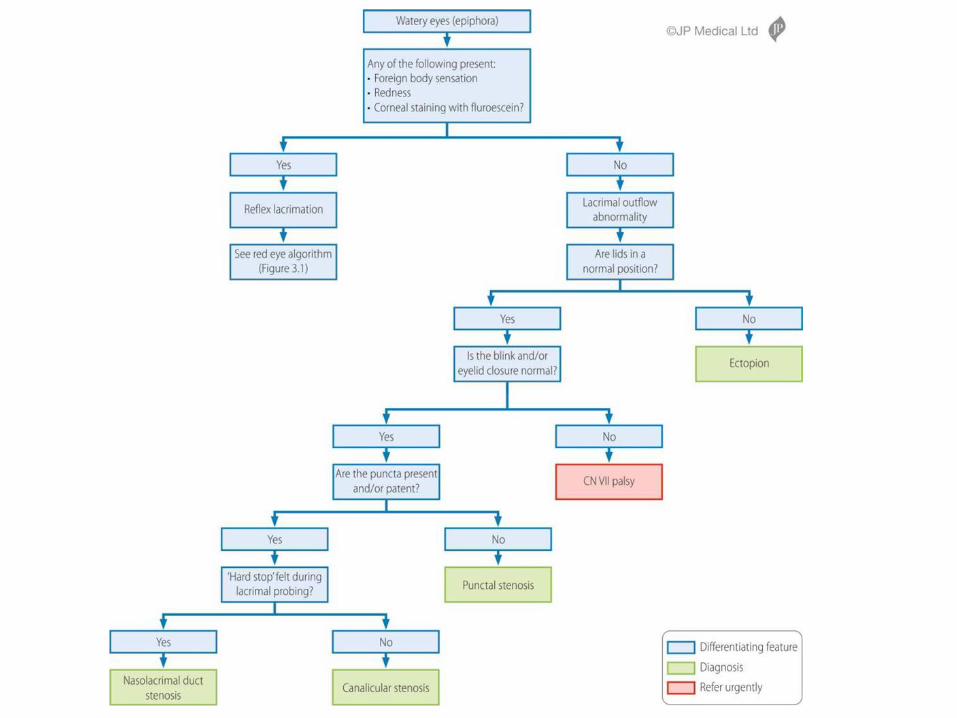
Epiphora Algorithm

Pic of the patient