Embed Size (px)
Citation preview

J AM COLL CARDIOL 731983:1:73- 81
Quantitative Contrast Angiography for Assessmentof Ventricular Performance in Heart Disease
HAROLD T . DODGE , MD, FACe, FLORENCE H . SHEEHAN. MD
Seattle , Was"ill~tol1
Contrast angiography provides much information aboutventricular and valvular size and function. This reviewdescribes the calculation of left ventricular chamber volume and wall thickness and the derivation of ejectionfraction, cardiac output, mass and wall tension and stress.In patients with valvular regurgitation, valve orifice areacan be calculated by using the angiographic output andregurgitant flow determined by comparing the angiographic output with the cardiac output measured usingFick or indicator-dilution techniques. By analyzing ventricular volume in conj unction with pressure, it is possible to assess pressure- volume work, compliance and
The deve lopment of improved X-ray technology , image intensifiers and filming techn iques over the past 30 years hasmade imag ing of the left ventricle by angiogra phic meth odsa valuable cl inical techn ique . Fro m images of the left ventricle. methods have been developed for determining dimensions . volume , stroke volume. wall thickness. mass andwall mot ion of the left ventricular chamber.
The first reports of measurements of left ventricular
chamber vo lumes in human bein gs using angiography weremade more than 25 years ago ( I ). These data were followedby studies in both experimental anima ls and human bein gsto develop and va lidate methods (2-5), establish norm alvalues for left ventricular volume (6 ,7) and dete rmine thechanges that occ ur in ventricular vo lumes with various typesof heart disease (as described in a previous review (8)). Thevarious methods for quantifying volume determinations havebeen ada pted to improve d high speed filming techn iquesusing cineangiography with differing projections (9- 12).
Met hods developed for determining left ventricular dimensions and mass (2,3,9- 11.13). when combined withcardiac cat heterization and measurement of left ventricular
From the Cardiovascular Research and Training Center. Universi ty ofWashington. Seatt le . Was hington . This study was supported in part byGrant HLl 9451-06 from the National Heart. Lung. and Blood lnstitute .Nationa l Institutes of Health . Bethesda . Maryland.
Address for reprints : Harold T . Dodge . MD. University of WashingtonRG-20. Seattle. Washington 98195.
I\;;1983 by the American College of Cardiology
contractility. Regional wall motion can be measured fromthe change in ventricular contour with time. When applied clinically, these methods and measurements havebeen used to determine the hemodyn amic characteristicsof the compensated and decompensated left ventricle invalvular and coronary heart disease. The informationderived from quantifying information in angiographicimages contributes to patient diagnosis, assessment ofprognosis and evaluation of therapy, and has added toour knowledge concerning the pathophysiology of heartdisease.
press ure. have made it possible to determ ine wa ll forces interms of tension and stress (14) and to estimate elastic properties of the ventricular myocardium in disease ( 15.16) .
This review will discuss the methods and the ir acc uracyfor determining left ventricular chamber dimensions. vo lume and mass from ventriculogra ms . The hemodynamiccharac ter istics of various heart diseases as determined byapplications of these techniques are described. With furth er
development of X-ray technology by such techniques asdigital subtraction angiograph y. improved imaging and further automation of various measure ments . quantitation ofinformatio n in cardiac image s will very likely have an increasi ngly impo rtant role in clinica l cardiology and card iovascu lar research.
Methods of Measurement
Ventric ular Volume
Problems. There are three majo r problem s when determining left ventricular chamber volumes from contras t ven triculograms: I ) image distortion from nonparallel X-raybeam s. from pincushion distortion in image intens ifier sys tem s and from cine project ion : 2) diffe ring left ve ntric ularimage project ions on the X-ray films resulting from the leftventric ular spatia l position and projections used for filming :and 3) selection of a suitable refe rence figure for volumecalcu lation from two project ions or a single projection (3\.
0735-10971831010073-09$03.00

74 ] AM COLL CAR oioi,J YX3: I :73-X 1
[)O[)(if\\J) SHEEll\~
Table 1. Normal Values for Left Ventricular Mass and Volumein Adults
curacy and reliability of volume measurement are also affected by interobserver and intraobserver variability in tracing the endocardial contour. Interobserver variability rangedfrom 6.6 to 20 ml for end-diastolic volume, from 5.9 to 10ml for end-systolic volume. and from 0.04 to 0.057c for theejection fraction (12.17.18). Intraobserver variability was3.3 ml in measuring end-diastolic volume. 3.2 ml for endsystolic volume, and O.02ek for ejection fraction (18). Thegreater variability between observers as opposed to withinobservers suggests that repeated studies on the same patientshould be analyzed by the same observer.
Stroke volume. The difference between the end-diastolic volume and the end-systolic volume provides a measure of left ventricular stroke volume. Several studies (4.19)
have shown that stroke volumes computed from the ventriculograms agree closely with stroke volumes computedby the independent Fick or indicator-dilution methods. Astudy (20) in which cardiac dimensions in human subjectswere monitored by measurements from epicardial radiopaque markers failed to demonstrate a systematic change indiastolic volume or stroke volume due to contrast mediumuntil at least the seventh beat after injection.
Normal values. Normal values for left ventricularchamber volume as determined by these methods have beenestablished (Table I). In the average adult. the normal enddiastolic volume ranges from 120 to 130 ml (6). The normalejection fraction or fraction of the end-diastolic volume thatis ejected is 0.67 ± 0.08 (mean ± standard deviation) (6).These values representing the normal adult are similar tothose found by other investigators (11.21). Normal valueshave also been determined for children and infants (7.22).
Values in ventricular dysfunction. In patients with depressed left ventricular myocardial function. the stroke volume is small relative to the end-diastolic volume. the leftventricle is usually dilated and the ejection fraction is reduced (23). An ejection fraction of less than 0.5 is usuallyconsidered abnormal. In patients with severe cardiomyopathy or myocardial damage from ischemic heart disease,the end-diastolic volume may be increased to 400 to 500ml and the ejection fraction depressed to less than 0.10.Even in the presence of compensated valvular heart disease.when there is ventricular dilation and hypertrophy in response to pressure and volume overloads. values for ejectionfraction are similar to those found in normal subjects (23).
Methods of measurement. In early studies to developand evaluate methods for computing left ventricular chamber volumes. the left ventricles of human hearts were distended with known volumes of barium sulfate paste andimaged with biplane orthogonal filming in differing projections (3). The projected dimensions and areas were determined from the images and corrected for X-ray distortion.and chamber volumes were calculated by several methodsand compared with the known volumes (3). These studiesdemonstrated that chamber volumes that were computedfrom the projected area of the left ventricular chamber andthe longest projected length (so-called area-length method)and by assuming an ellipsoid reference figure were closelycorrelated with known chamber volumes (r = 0.995) andhad a standard error of estimate of ± 8.2 cc.
With this method. volumes (V) were computed as
V = (7T/6)(L)(Da)(Db),
where L is the longest measured chamber length on eitherof the biplane films and Da and Db equal the transversediameters in the orthogonal projections computed from therespective projected chamber areas and lengths. Comparisons of known chamber volumes with computed volumesusing the calculated spatial length of the chamber and alsoby Simpson's rule were similar to those obtained by usingthe area-length method but required more complex calculations (3).
An analysis of biplane ventriculograms from subjectswith heart disease of various origins demonstrated that theminor diameters of the left ventricular chamber in the twoprojections were similar and that the direction of the longaxis of the left ventricle usually changed only a few degreesduring systole (9). Therefore. the projection of the long axisis thought to be relatively constant during systole and diastole. Furthermore. the maximal projected length of thechamber agreed closely with the calculated spatial length(midaortic valve to apex), and was usually represented inthe anteroposterior projection. It was then demonstrated thatchamber volumes could be calculated from ventriculogramstaken in the single anteroposterior projection (9).
Kennedy et al. (10) demonstrated that left ventricularchamber volumes computed from films taken in the singleright anterior oblique as well as the single anteroposteriorprojection could be closely correlated with volumes computed from biplane films. but with a systematic overestimation of volume. Because of the known systematic overestimation of volume obtained with all of these methods,the computed volumes in our laboratory are adjusted byregression equations that were determined in these earlierstudies (9.10). Both Wynne et al. (II) and Rogers et al.(12) demonstrated that similar equations can also be appliedto adjust volumes computed from biplane films taken inboth the right and left anterior oblique projections.
Interobserver and intraobserver variability. Ac-
End-diastolic volume
End-systolic volume
Ejection fraction
Mass
Wall thickness
70 ± 20 m l.nr'24 ± 10 m l/m"
0.67 ± 0.082.50 ± OAO g/kg10.9 ± 2.0 mm

QUANTITATIVE ANGIOGRAPHY AND HEART FUNCTION J AM COLL CARDIOL1983:1:73-81
75
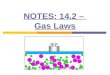
Figure 1. Left ventricular (LV) pressure, volume and cardiac output in apatient with severe mitral valve insufficiency. The effective stroke volume(SV) and flow were determined by the Fick method. Regurgitant (REGURG) volume = angiographic stroke volume minus effective strokevolume. Left ventricular minute output = angiographic stroke volumetimes heart rate; Regurgitant flow = regurgitant stroke volume times heartrate; A-V = arteriovenous; DIFF = difference; EDV = end-diastolicvolume; MIN = minute. (Reprinted. with permission. from Sodeman WAJr and Sodeman WA. Pathologic Physiology. Philadelphia: WB Saunders.1973:283.)
Left Ventricular Mass
In films having proper contrast, the thickness of the ventricular wall usually can be measured and used to estimatethe mass of the left ventricle (13). This method of measuringmass was validated by comparing calculated mass with leftventricular weight recorded at postmortem examination(25,26). Errors are found to arise when hypertrophy is eccentric or when pericardial thickening or fluid is present.
In chronic heart disease ventricular hypertrophy occursin response to I) increased work from pressure and volumeoverload, and 2) chronic left ventricular dilation, even whenstroke work values are low. The type of hypertrophy differs
Volume Curves and Pressure-Volume Relations
Volume curve for the cardiac cycle. If ventricularchamber volume is calculated from each frame taken at rapidfilming rates such as 60 or 30 frames/s, volume measurements can be plotted with respect to time to construct avolume curve for the cardiac cycle. From analysis of theslopes of the ejection and filling values on these curves, therates of ventricular volume change during ejection and fillingcan be determined (27). The maximal rates of ejection andfilling are usually similar and typically in the range of 500mils. In patients with severe aortic or mitral valve insufficiency, peak values of over three times the normal are observed. Values for peak systolic volume change as low as200 mils are observed in patients with mitral and aorticstenosis and heart failure from severe myocardial disease.
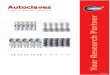
Pressure-volume curves. Construction of ventricularpressure-volume curves using the relation of chamber pressure and volume with respect to time provides informationconcerning the mechanical performance of the ventricle(Fig. 2) (4,5,8,15). The work performed in systole to eject
blood and the work performed in diastole to distend and fill
Tension and Stress
From knowledge of ventricular dimensions, wall thicknessand pressure, it is possible to estimate the forces within theventricular wall. Tension is the force that tends to pull apartthe edges of a slit in a thin-walled structure (for example.a balloon), expressed in terms of force per unit length ofslit by the Laplace equation. Stress is the wall force in athick-walled chamber, expressed in units of force per unitarea of the cut surface of a slit; it is equal to tension dividedby wall thickness. In an ellipsoid, tension (T I and T2) andstress (SI and S2) in the equatorial and meridional directions,respectively, are proportional to the principal radii of curvature (R 1 and R2) (14).
Initially. stress was calculated assuming a thin-walledmodel (J 4). Stress was also assumed to be constant fromthe endocardium to the epicardium. This model has providedinformation about the relation between stress and ventriculardilation and the effect of hypertrophy on stress (28-30).
More detailed thick-walled and finite element mathematicalmodels have also been developed (31 ).
with pressure and volume overload. With volume overload,ventricular mass increases proportionately to the increase involume with little increase in wall thickness, so that theend-diastolic volume to mass ratio is approximately 1.0.With pressure overload, there is little or no increase involume, but wall thickness and mass are increased and massto end-diastolic volume ratio exceeds 1.0 (27). The hypertrophy and increased wall thickness in compensated pressureand volume overload states are such that peak systolic wallstress values remain within the normal range (28).
258 .1
383 .1
115/15 .. III Hg0.67233 11I125.8 L/.. ln
23.3 L/atn
2.5 L/.ln
1.76 L/lllln/M 2
8.98 Vol
EFFECTIVESV::r::
EDV
LV PRESSUREEJECTION FRACTIONRECURC SVLV MIN OUTPUTRECURC FLOWEFFECTIVE FLOWCARDIAC INDEXA-V OXYGEN DIFF
Regurgitant Flow and Valve Areas
The demonstration that. in subjects without arrhythmias,shunts or valvular regurgitation, the angiographic strokevolume agrees closely with stroke volume determined byFick or indicator-dilution methods (4,19) has aided in thedevelopment of a method to quantify mitral or aortic valveregurgitant flow, or both (24). The regurgitant volume perstroke is calculated by subtracting the forward or effectivestroke volume determined by the Fick or indicator-dilutionmethods from the stroke volume measured by angiography(Fig. I). The accuracy of this method was confirmed bycomparing the valve orifice areas determined from the calculated regurgitant flow with orifice areas measured at surgery or postmortem examination (24).

76
200
180
::: 160I
~e 140
120
100
80
J AM Call CARDIOl1983;1:73-81
j'-
Ij
J
PRES SURE - mm KgliD
[ill SYSTOLIC WORK ' 129 Gm ·M
[@l WORK OF DISTENS ION ' 11 Gm ·M
EIl NEI WORK , 112 Gm·M
DODGE .\:\D SHETH\:\
Figure 2. Left.Ventricular pressure and volume curves plotted with respect to time afteronset of the QRS complex on the electrocardiogram. Right. Pressure-volume curveconstructed with positions marked to indicate: mitral valve closure (A). aortic valveopening (B) and closure (C). respectively.and mitral valve opening (D). There is noperiod of isovolumic contraction between Aand B owing to the mitral valve insufficiency.Values for work as calculated from the areasbeneath various portions of the curve are illustrated by the shaded areas. (Reprinted. withpermission. from Dodge HT. Baxley WA.Left ventricular volume and mass and theirsignificance in heart disease. Am J Cardiol1969:23:52X-37. )
the ventricle are determined from the area under the systolicand diastolic portions of the curve. respectively. The rateat which work is performed is ventricular power (27l.
Left ventricular work and peak ejection rates and powernormalized for end-diastolic volume have been used to assess myocardial performance (27). However. these valuesare difficult to determine and interpret. and at present seemto have no advantage over the simple measurement of ejection fraction.
Ventricular compliance can be assessed from the diastolicportion of the pressure-volume curve. Reduced compliancemay be caused by an increase in wall thickness or in musclestiffness. and results in elevation of end-diastolic pressure(16).
Contractility has been evaluated using the pressure-volume relations at end-systole to determine the slope. EES' ofthe line connecting end-systolic pressure and volume measurements recorded under different loading conditions. EES
is nearly independent of preload and afterload. In patients.the method requires repeated ventriculograms and there isdisagreement about the value of EES curves for comparingsubjects. because the pressure-volume curves of patientswith volume or pressure overload differ from those of normal patients regardless of contractile state (32).
Regional Left Ventricular Wall Motion
Many laboratories have developed quantitative methods tomeasure the extent of wall motion (33-36). These methodsdiffer primarily in the motion vector assigned to the pointsor regions around the left ventricular contour (Fig. 3). Normal motion differs in different regions of the ventricle (34.36).To make comparisons. the motion of each region can beexpressed in units of standard deviations from the mean ofa normal reference group (34). Frame by frame analysis ofregional wall motion yields information on both the timingand the extent of motion in normal and diseased segmentsof the ventricle during systole and diastole (33.35).
Valvular Heart DiseaseThe application of quantitative angiographic measurementsis particularly helpful in evaluating patients with valvularheart disease.
Aortic Insufficiency
Ventricular volume and mass. In patients with aorticinsufficiency. the left ventricle dilates in response to thevolume overload. As in patients with mitral valve insuffi-

QUANTITATIVE ANGIOGRAPHY AND HEART FUNCTION J AM COLL CARDIOL1983;1:73-81
77
CHORD METHOD
RADIAL METHQD
AREA METHODFigure 3. Methods of measuring regional left ventricular wall motion.The chord and radial coordinate methods assume, respectively, that motionproceeds toward a long axis or central point. The area method measureschange in area of the regions of the ventricle.
ciency, this volume overload may be very large, with strokevolumes approaching (but rarely exceeding) 300 ml andoutputs of 25 to 30 liters/min. Left ventricular stroke workmay be elevated to three or four times the normal amount.The increase in end-diastolic volume is proportional to thevolume of regurgitant flow. The end-systolic volume is alsoincreased so that in compensated aortic insufficiency theejection fraction remains relatively normal (8,23,27,37-40).
An increase in muscle mass, or hypertrophy, accompanies the ventricular dilation (29,30,38).of the hypertrophy, peak systolic wall stress usually remainsnormal, although the left ventricular chamber is dilated andthe ventricle becomes more spherical. This distributes stressmore evenly than is the case in normally eccentric heartswhere stress is much greater in the equatorial than in themeridional direction (29).
As seen in pressure-volume curves (Fig. 4), isovolumicrelaxation and isovolumic contraction are shortened or eliminated (5,23.40). Diastolic pressure is often normal, evenin patients with considerable ventricular enlargement. Thisindicates that the elastic properties of the ventricle are alteredin chronic disease, resulting in increased compliance (38.40).
Effect of heart rate. Heart rate influences the hemodynamics of aortic insufficiency. Judge et al. (41) showedthat increasing the heart rate, particularly when there isbradycardia, causes a reduced regurgitant flow per strokeand reduced end-diastolic volume and pressure, althoughregurgitant flow per minute is essentially unchanged. Thishemodynamic effect of heart rate may account for the observation that some patients with aortic insufficiency mayexperience dyspnea and angina at rest, but tolerate exercisewell.
Ejection fraction. A reduced ejection fraction in patients with chronic aortic insufficiency indicates decreasedmyocardial performance rather than inadequate hypertrophyfor the work overload, as is evidenced by normal or depressed peak systolic stress values (42). With a decrease in
1= mitral stenosis2 = mitral regurgitation3 = aortic stenosis4= aortic regurgitation5 = aortic stenosis 8< regurgitation
GOO500400
.""·--_a_\ .-._._._......\ ''''',4\ ." '\. ,
\ .". -,'. .~
I ' , ..-._._;_._._._._;-i
300Volume (rnt )
I i
100 200o
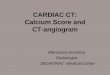
Figure 4. Pressure-volume curves from patients with different types of heart disease. The curve from the patientwith mitral stenosis (1) shows well defined isovolumiccontraction and relaxation periods. a normal stroke volumeand relatively normal stroke work. The other patients havelarger stroke work values as estimated by the areas underthe systolic limbs of the curves. The patients with aortic(4) or mitral (2) regurgitation and aortic stenosis and regurgitation (5) have elevated stroke work values with largestroke volumes. as is shown by the excursion of the curvesalong the horizontal or volume axis. Patients with valvularinsufficiency have a shortening or absence of isovolumiccontraction and relaxation periods. Patients with aorticvalve stenosis (3) have elevated systolic pressures. Patients with large stroke volumes have elevated end-diastolic volumes. (Reprinted, with permission, from Sodeman WA Jr and Sodeman WA. Pathologic Physiology.Philadelphia: WB Saunders, 1973:286.)

78 J AM COLL CARDIOL1983:1:73-81
DODGE A'JD SHEEH.\N
ejection fraction. there is an increase in end-diastolic pressure and a further increase of end-diastolic volume and mass.Indeed, the largest end-diastolic volumes are observed inpatients with aortic insufficiency. and may reach 700 to 800011 (27). This marked chamber dilation is associated withmassive ventricular hypertrophy. with left ventricular massvalues occasionally in excess of 700 g. particularly whensome associated aortic valve stenosis exists (29).
Regional performance. More recent studies (43) havedemonstrated a selective depression of regional performanceinvolving the anterior wall or apex in patients with aorticor mitral valve insufficiency and no coronary artery disease.This suggests that studies of regional contraction may provide earlier evidence of a failing myocardium than do studiesof the overall ejection fraction. The basis for regional performance abnormalities is not clear at this time.
Chronic versus acute aortic regurgitation. The net result of chronic aortic valve regurgitation is ventricular dilation to accommodate the volume overload and sustainforward output. Hypertrophy occurs in response to the increased work and chamber dilation to maintain normal peaksystolic wall stress. As a result of the hypertrophy, total leftventricular oxygen consumption and coronary blood floware increased (23,42,44).
In contrast, acute aortic regurgitation produces a volumeload for which the heart cannot immediately compensate.The result is an increase in diastolic pressure and the development of congestive heart failure with little ventriculardilation and no hypertrophy (45).
Mitral Insufficiency
Chronic mitral insufficiency. In this condition. as inchronic aortic insufficiency. the left ventricle is dilated inproportion to the regurgitant flow and stroke volume. However. left ventricular hypertrophy is less severe for comparable regurgitant volumes. probably because much of theregurgitation flows into a low pressure left atrium in earlysystole during what is normally isovolumic systole (37).Isovolumic contraction is shortened or eliminated (Fig. 4)(15,23). The left atrium is also dilated with increased compliance to accept the volume of regurgitant flow. Becauseof the dilation and increased compliance in the left atriumand ventricle. patients with chronic mitral valve insufficiency may have normal left ventricular diastolic pressure.left atrial pressure and pulmonary vascular pressure despitelarge volumes of regurgitant flow. Thus. patients are oftenable to tolerate considerable volumes of mitral regurgitationfor extended periods without having symptoms (46).
The ejection fraction is usually normal in primary mitralvalve insufficiency. but is reduced when the insufficiencyis secondary to ischemic heart disease or cardiomyopathy.As in patients with aortic regurgitation. dilation is accompanied by decreased eccentricity as the ventricle assumes amore spherical shape (29,47).
Acute mitral insufficiency. The development of compensatory left ventricular and left atrial dilation and of increased compliance are functions of chronicity of the disease(45). In patients with acute mitral valve insufficiency. asoccurs in patients with ruptured chordae tendineae, there islittle ventricular dilation and hypertrophy and the compliance of the left ventricle. left atrium and pulmonary venoussystem is low. Accordingly. there may be significant increases in left ventricular end-diastolic pressure. left atrialpressure and pulmonary vascular pressure. even with onlymoderate volumes of mitral regurgitant flow (48).
Aortic Stenosis
In response to chronic pressure overload in patients withaortic valve stenosis, the left ventricle is hypertrophied withan increased wall thickness but with little or no increasedvolume (39). Despite ventricular systolic hypertension. peaksystolic wall stress is normal in patients with compensatedaortic stenosis because the wall forces are distributed overa greater cross-sectional area (8.14.39). However. the increased wall thickness may result in a stiff diastolic ventriclewith reduced compliance and an elevated diastolic pressure.which does not necessarily indicate failure (38-40).
Symptoms and signs of decompensation may occur because of the severity of the stenosis or because of depressedmyocardial performance. The degree of stenosis becomescritical and limits cardiac output when the orifice area isless than 1.0 crrr'. Depressed myocardial performance isindicated by a reduced ejection fraction and increased diastolic volume (28,40). The increased afterload may causea greater depression of the ejection fraction than is observedin other types of heart disease having depressed myocardialperformance.
Mitra/ Stenosis
In patients with mitral stenosis. stroke volume and cardiacoutput are reduced because of obstruction of the mitral valve.Although the left ventricular ejection fraction is reduced toless than 0.40 in approximately one-third of patients withmitral stenosis. the left ventricle is usually not dilated (49).The mechanism for the reduced ejection fraction is unknown. but it may be a result of previous rheumatic carditis.
Evaluation of Valve Surgery
Aortic regurgitation. Quantitative angiography has beenuseful for evaluating the functional response to surgery invalvular heart disease. Valve replacement for aortic regurgitation results in reductions of end-diastolic and end-systolic volumes. mass. wall stress and stroke work to normalor near normal levels. The end-diastolic pressure. aorticpressure. eccentricity and cardiac output also return towardnormal (50.51). The ejection fraction changes little if it wasnormal preoperatively: it may improve from a depressed

QUANTITATIVE ANGIOGRAPHY AND HEART FUNCTION J AM cou, CARDIOL1983:1:73- 81
79
13 14 15 16 17 18 19 2:Q8 , 1. 11 12
\ I- -- - - - - .=-
V
I
123.56 7
v ........ l.--l--'~- ...... ,/ ...t....: ....... <,-- ,-- - - -. -'r - - /'- ,>-
I'-.. ~
I I I
. 75
. 25
.se
1 2 3 .. 5 6 7 8 I) 18 11 12 13 1 4 IS 16 17 18 19 2G
CHOHD 'U'''.R
,.,,;
C . TI ME TO MINIMUM
e
B. FRACTIONAL SHORTENI C~ .....
i~;:
~
A. RAO PROJECTIOpreoperative level , but this is not always the case (50, 5 l ).Studies have shown that depressed preoperative ventricularfunction. as indicated by the ejection fraction. is associatedwith a poorer prognosis and recovery of function after surgery . Accordingly, it has been recommended (52) that patients undergo aortic valve replacement before depre ssedmyocardial performance develops.
Aortic stenosis. In patients with aortic stenos is or combined aortic stenos is and regurgitation. valve replacementresult s in reductions in left ventricular mass , end-diastolicand peak systolic pressures. stress and stroke work. andincreases in aortic systolic and diastoli c pressure (50). Ejection fraction improves in most cases . even if it was lowpreoperatively (50).
Mitral regurgitation. In patients with mitral regurgitation. the ejection fraction does not increase after surgeryand may even decrease (53). Although there are reductionsin end-diastolic volume. end-diastolic pressure and strokevolume , hypertrophy does not regre ss and stroke work decreases only slightly (53). Nevertheless. long-term survivalin patients with mitral regurgitation is significantly impro vedby surgery (54). Patients with a severely abnormal left ventricle. with a greatly reduced ejection fraction and markeddilati on . have a poorer long-term prognosis even with surgery than do patients with mitral insufficiency and morenormal vent ricular performance (53.54).
Coronary Artery DiseaseRegional wall motion abnormalities. Coronary artery
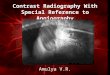
disease causes regional wall motion abnormalities. whichin early studies (55) were found in the distribution of stenosed or occluded arteries. More recent studies (56) usingtechniques for quantifying the extent of coronary artery stenosi s and for more' accurately determining the extent andtiming of regional wall motion abnormalities have demonstrated a significantly increased frequency of regional hypokinesia and delayed regional contraction or relaxation. orboth , when stenoses in the major coronary arterie s cau semore than 60 to 70% reduction of diameter or a minimalluminal area of less titan 1.0 mrrr' . Thi s occurs in patient swithout a histo ry of myocardial infarction (34.35,57), Whenmore than 20 to 30% of the endocardial contour becomesakinet ic , end-diastolic volume is increased and ejection fraction reduced (58). However, the extent of regional hypokinesia or akinesia may not be reflected by the global ejection fraction becau se of compensatory hyperkinesia ofuninvolved regions of the myocard ium (Fig . 5) (35).
Delayed regional wall contract ion or relaxation (Fig. 5)is common and contributes to the decreased systolic functionand increased diastolic stiffness of the left ventricle in patient s with coronary heart disease 03 .35.57) . The mechanisms for the regional asyn chrony are not completelyunder stood.
Figure 5. Rcgional wall motion calculated by the chord methud <.351ina patient with isolated stenosisof thc right coronary artery. A, End-diastolicand end-systolic endocardial contours. B. Fractional shortening at eachchord in the patient (solid line) is compared with th~ normal mcan ± I or2 standard deviations (dashed lines). There is inferior hypokinesia andcompensatory anterior hyperkinesia. resulting in normal ejection fractionof 67'7('. C, Time to minimal distance from the endocardial contour to thelong axis. This patient had hypokinesia without prolongation of contractiontime.
Yentricular dilation in patients with coronary heart disease. as in patients with other forms of heart disease. isassoci ated with hypertrophy. but to a lesser extent than isseen in those patients having other types of heart disease.Ventricular aneurysms may cause substantial increa ses inventricular dimensions and volume, resulting in increasedwall stress. The volume of the aneurysm usually chan geslittle during systole: therefore systolic expansion doe s notcontribute significantly to the mechanical defect.
Ejection fraction and revascularization surgery.Ventricular performance as expressed by the global ejectionfract ion has been shown to be an important predictor ofsurvival in patients with coronary heart disease (59 ). Indeed ,it is a more important pred icto r than is the number of stenosed coronary arteries. Studi es to date (59) have indicatedthat survival is improved after coronary revascularizationsurgery. particularly in patients with two or three vessel

80 J AM COLL CARDIOL1983:1:73-81
DODGE AND SHEEHAN
disease and moderate depression (0.30 to 0.50) of ejectionfraction.
Although survival improves after surgery, global left ventricular function as measured by the ejection fraction doesnot improve as a result of surgery in the majority of patients(60). However, some studies (61) have demonstrated lessening of regional hypokinesia after successful revascularization surgery. These results indicate that regional wall motion analysis is more sensitive than the global ejection fractionnot only for detecting ventricular dysfunction but also forevaluating therapy.
References1. Dodge HT, Tannenbaum HL. Left ventricular volume in normal man
and alterations with disease (abstr). Circulation 1956;14:927.
2. Chapman CB. Baker 0, Reynolds J, Bonte FJ. Use of biplane cinefluorography for measurement of ventricular volume. Circulation1958;18:1105-17.
3. Dodge HT, Sandler H, Ballew DW, Lord 10 Jr. The use of biplaneangiocardiography for the measurement of left ventricular volume inman. Am Heart J 1960;60:762-76.
4. Gribbe P. Comparison of angiocardiographic and direct Fick methodsin determining cardiac output. Cardiology 1960:36:20-9.
5. Arvidsson H. Angiocardiographic determination of left ventricularvolume. Acta Radiol [Diagn] (Stockh) 1961;56:321-39.
6. Kennedy JW, Baxley WA. Figley MM. Dodge HT, Blackmon JR.Quantitative angiography. I. The normal left ventricle in man. Circulation 1966;34:272-8.
7. Graham TP Jr. Jarmakani JM, Canent RV Jr, Morrow MN. Left heartvolume estimations in infancy and childhood: reevaluation of methodology and normal values. Circulation 1971;43:895-904.
8. Dodge HT, Sandler H, Baxley WA, Hawley RR. Usefulness andlimitations of radiographic methods for determining left ventricularvolume. Am J Cardiol 1966:18:10-24.
9. Sandler H, Dodge HT. The use of single plane angiocardiograms forthe calculation of left ventricular volume in man. Am Heart J1968;75:327-34.
10. Kennedy JW, Trenholme SE, Kasser IS. Left ventricular volume andmass from single-plane cineangiocardiogram. A comparison of anteroposterior and right anterior oblique methods. Am Heart J1970;80:343-52.
II. Wynne J, Greene LH, Mann T, Levin D, Grossman W. Estimationof left ventricular volumes in man from biplane cineangiograms filmedin oblique projections. Am J Cardiol 1978;41:726-32.
12. Rogers WJ, Smith LR, Hood WP Jr, Mantle JA, Rackley CE, RussellRO Jr. Effect of filming projection and interobserver variability onangiographic biplane left ventricular volume determination. Circulation 1979:59:96-104.
13. Rackley CE, Dodge HT, Cobe YD Jr, Hay RE. A method for determining left ventricular mass in man. Circulation 1964;29:666-71.
14. Sandler H. Dodge HT. Left ventricular tension and stress in man. CircRes 1963;13:91-104.
15. Bunnell IL, Grant C, Greene DG. Left ventricular function derivedfrom the pressure-volume diagram. Am J Med 1965:39:881-94.
16. Grossman W. Barry WHo Diastolic pressure-volume relations in thediseased heart. Fed Proc 1980:39:148-55.
17. Cohn PF, Levine JA, Bergeron GA, Gorlin R. Reproducibility of theangiographic left ventricular ejection fraction in patients with coronaryartery disease. Am Heart J 1974:88:713-20.
18. Dodge HT. Sheehan FH, Stewart OK. Estimation of ventricular vol-
ume, fractional ejected volumes. stroke volume and quantitarion ofregurgitant flow. Ill: Proceedings of the International Symposium onAngiocardiography. Titisee, West Germany. February 1982. Stuttgart.West Germany: Georg Thieme Verlag (in press).
19. Dodge HT. Ray RE, Sandler H. An angiocardiographic method fordetermining left ventricular stroke volume in man. Circ Res 1962:11:73945.
20. Vine DL. Hegg TD, Dodge HT. Stewart DK, Frimer M. Immediateeffect of contrast medium injection on left ventriclar volumes andejection fraction: a study using metallic epicardial markers. Circulation1977;56:379-84.
21. Sanmarco ME, Bartle SH. Left ventricular volume determinations:comparison of angiographic and thermal washout techniques (abstr).Circulation 1964:30(suppl IiJl:III-151-2.
22. Miller GAH. Swan HJe. Effect of chronic pressure and volume overload on left heart volumes in subjects with congenital heart disease.Circulation 1964;30:205-16.
23. Dodge HT, Baxley WA. Hemodynamic aspects of heart failure. AmJ Cardiol 1968;22:24-34.
24. Sandler H, Dodge HT, Hay RE. Rackley CEo Quantitation of valvularinsufficiency in man by angiocardiography. Am Heart J 1963;65:50113.
25. Hugenholtz PG, Kaplan E, Hull E. Determination of left ventricularwall thickness by angiocardiography. Am Heart J 1969:78:513-22.
26. Kennedy JW, Reichenbach DD. Baxley WA. Dodge HT. Left ventricular mass: a comparison of angiocardiographic measurements withautopsy weight. Am J Cardiol 1967;19:221-3.
27. Dodge HT, Kennedy JW, Petersen JL. Quantitative angiocardiographic methods in the evaluation of valvular heart disease. FrogCardiovasc Dis 1973;16:1-23.
28. Hood WP, Rackley CE, Rolett EL. Wall stress in the normal andhypertrophied human left ventricle. Am J Cardiol 1968:22:550-8.
29. Dodge HT, Frimer M, Stewart DK. Functional evaluation of the hypertrophied heart in man. Circ Res 1974:34.35(suppl Il):II-122-7.
30. Gould KL. Lipscomb K, Hamilton GW. Kennedy JW. Relation ofleft ventricular shape, function and wall stress in man. Am J Cardiol1974:34:627-34.
31. Yin FCP. Ventricular wall stress. Circ Res 1981;49:829-42.
32. Sagawa K. Editorial: the end-systolic pressure-volume relationshipof the ventricle: definition, inodifications and clinical use. Circulation1981:63:1223-7.
33. Clayton PD. Bulawa WF. Klausner Se. Urie PM, Marshall HW,Warner HR. The characteristic sequence for the onset of contractionin the normal human left ventricle. Circulation 1979;59:671-9.
34. Dodge nt. Sheehan FH, Kliman SH, et al. Quantitative relationshipof coronary stenosis and ventricular hypokinesia. IEEE Comput Cardiol 198L377-80.
35. Stewart OK, Dodge HT, Frimer M. Quantitative analysis of regionalmyocardial performance in coronary artery disease. Cardiovasc Imag1m Process 1975;72:217-24.
36. Gelberg HJ. Brundage BH, Glantz S, Parmley WW. Quantitative leftventricular wall motion analysis: a comparison of area, chord andradial methods. Circulation 1979;59:991-1000.
37. Miller GAH, Kirklin JW, Swan HJe. Myocardial function and leftventricular volumes in acquired valvular insufficiency. Circulation1965;31:374-84.
38. Grant C, Greene DG, Bunnell IL. Left ventricular enlargement andhypertrophy: a clinical and angiocardiographic study. Am j Med1965;39:895-904.
39. Kennedy JW, Twiss RD, Blackmon JR, Dodge HT. Quantitativeangiocardiography. III. Relationships of left ventricular pressure, volume, and mass in aortic valve disease. Circulation 1968;38:838-45.
40. Dodge HT, Hay RE, Sandler H. Pressure-volume characteristics ofthe diastolic left ventricle of man with heart disease. Am Heart J1962;64:503-11.

QUANTITATIVE ANGIOGRAPHY ANDHEARTFUNCTION J AM COLLCARDIOL1983;1:73-81
81
41. Judge TP, Kennedy JW, Bennet LJ, et al. Quantitative hemodynamiceffects of heart rate in aortic regurgitation. Circulation 1971;44:35567.
42. Osbakken M, Bove AA, Spann JF. Left ventricular function in chronicaortic regurgitation with reference to end-systolic pressure, volumeand stress relations. Am J Cardiol 1981;47:193-205.
43. Osbakken MD, Bove AA, Spann JF. Left ventricular regional wallmotion and velocity of shortening in chronic mitral and aortic regurgitation. Am J Cardiol 1981:47:1005-9.
44. Baxley WA, Dodge HT, Rackley CE, Sandler H. Pugh D. Left ventricular mechanical efficiency in man with heart disease. Circulation1977;55:564-8.
45. Wigle D. Labrosse CJ. Sudden, severe aortic insufficiency. Circulation1965;32:708-20.
46. Braunwald E. Mitral regurgitation: physiologic, clinical and surgicalconsiderations. N Engl J Med 1969;281:425-33.
47. Vokonas PS, Gorlin R, Cohn PF, Herman MV, Sonnenblick EH.Dynamic geometry of the left ventricle in mitral regurgitation. Circulation 1973;48:786-96.
48. Baxley WA, Kennedy JW. Feild B. Dodge HT. Hemodynamics inruptured chordae tendineae and chronic rheumatic mitral regurgitation.Circulation 1973;48:1288-94.
49. Kennedy JW, Yarnall SR, Murray JA, Figley MM. Quantitative angiocardiography. IV. Relationships of left atrial and ventricular pressure and volume in mitral valve disease. Circulation 1970;41:817-24.
50. Kennedy JW, Doces 1. Stewart DK. Left ventricular function beforeand following aortic valve replacement. Circulation 1977;56:944-50.
51. Carroll JD, Gaasch WHo Left ventricular volume. mass, and functionfollowing surgical correction of chronic aortic regurgitation. Herz1981;6:131-7.
52. Hirshfeld JW Jr, Epstein SE. Roberts AJ, Glancy DL, Morrow AG.Indices predicting long-term survival after valve replacement in patients with aortic regurgitation and patients with aortic stenosis. Circulation 1974;50:1190-9.
53. Kennedy JW. Doces JD. Stewart DK. Left ventricularfunction beforeand following surgical treatment of mitral valve disease. Am Heart J1979;97:592-8.
54. Hammermeister KE. The effect of surgical therapy on covariate-survival relationships in patients with mitral valve disease. Herz 1981;6:22636.
55. Herman MV, Heinle RA, Klein MD, Gorlin R. Localized disordersin myocardial contraction: asynergy and its role in congestive heartfailure. N Engl J Med 1967;277:222-32.
56. Brown BG, Bolson EL, Dodge HT. Arteriographic assessment ofcoronary atherosclerosis: review of current methods. their limitations,and clinical applications. Arteriosclerosis 1982;2:2-15.
57. Gibson DG. Prewitt TA, Brown OJ. Analysis of left ventricular wallmovement during isovolumic relaxation and its relation to coronaryartery disease. Br Heart J 1976:38:1010-9.
58. Klein MD, Herman MV. Gorlin R. A hemodynamic study of leftventricular aneurysm. Circulation 1967;35:614-30.
59. DeRouen TA, Hammermeister KE, Dodge HT. Comparisons of theeffects on survival of coronary artery surgery in subgroups of patientsfrom Seattle Heart Watch. Circulation 1981;63:537-45.
60. Hammermeister KE, Kennedy JW, Hamilton GW, et al. Aortocoronary saphenous-vein bypass: failure of successful grafting to improveresting left ventricular function in chronic angina. N Engl J Med1974;290:186-92.
61. Wolf NM. Kreulen TH, Bove AA, et al. Left ventricular functionfollowing coronary bypass surgery. Circulation 1978;58:63-70.