Embed Size (px)
Citation preview

Quality management and clinical audits in nuclear medicineResults form IAEA projects
Maurizio Dondi, MDNMDI/IAEAVienna, IMIC 2016

Quality Management program?
• A QMS is a means by which nuclear medicine facilities can show their:– Level of patient care they provide – Customer orientation by following a process of self‐and external evaluation (audits)
– Adherence to national and/or international standards– Commitment to quality of care

Why embarking in a QM program?
• In many countries a requirement bylaw for accreditation with health care providers– In EU:
• Directive 96/29/Euratom ‐ laying down basic safety standards for the protection of the health of workers and the general public against the dangers arising from ionizing radiation.
• COUNCIL DIRECTIVE 2013/59/EURATOM of 5 December 2013
http://eur‐lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2014:013:0001:0073:EN:PDF

The international setting: LMIC • Very diversified levels of implementation• Possible lack of financial and/or human resources; • Limited training; lack of educational opportunities; limited professional network
• Overall need to raise the standards of practice and improve performance due to competition from other modalities

QUANUM project:QUality Management Audits in NUclear Medicine
• A project started in 2006 to identify a tool to help NM practitioners to:
• self‐assess their practices; • receive an external team of auditors supported by IAEA• Receive recommendations• and implement remedial actions
• The output is a program on quality management implementation: (QUANUM)

Comprehensive audit


Outputs from Excel tool

QUANUM auditing missions

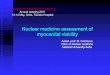
Results: average of Conformances/Category
Average: 73.9±8.3% (mean±1SD), ranging between 56.6% and 87.9%

Results: average of Non Conformances/Category

Prioritization of Non Conformances

Results: itemization and translation of NCs into priorities
ITEM
Nr. of Critical and
Major priorities
%
1 Managerial; Organization and Documentation 229 26.02%
2 Education and training 42 4.77%
3 Patient radiation protection and safety 78 8.86%
4 Staff radiation protection and safety 152 17.27%
5 QA/QC and management of equipment and SW 100 11.36%
6 Lack of human resources 32 3.64%
7 Radiopharmaceutical preparation, dispensing and handling 139 15.80%
8 Clinical quality of diagnostic and therapeutic procedures 35 3.98%
9 Facility design 73 8.30%
Total 880
Nr of audits reviewed 38
Average nr. of critical and major priorities notified ~23

Results: translation of NCs into Critical and Major priorities

Why embarking into an external audit?
Negative perception:
• Costs (staff time):– Review of internal processes– Creation of SOPs
• Lack of funds to address possible critical issues
• Potential threat to activities
Positive side:
• Different perspective on daily routines (peer review)
• Assess compliance of any level of NM centre to international standards
• Alignment of working practices to international standards
• Accountability

Clinical audit on Myocardial Perfusion Imaging:
Assessing outcome of training in nuclear cardiology

Training in NC (last 10 years)• Through Regional Training Courses• Usually 20+ participants are involved
• Different levels of complexity
Region # of training courses # of participants
Africa 8 155
Asia 10 208
Middle East 3 55
Eastern Europe 13 285
Latin America and Caribbean 7 193
Total 41 896

Trends of NC practice in low‐middle income countries
Region Institutions
CV Procedures
Average/center/year
2010
CV Procedures
Average/center/year
2015
Percentage
Change
Africa 16 469 695 +48,2%
Asia 29 897 833 ‐7,3%
Eastern Europe 35 561 567 +1%‐
Latin America
Caribbean33 990 1051 +6,1%
Western Europe 8 1245 1680 +34,9%
Source: IAEA NUMDAB

Rationale & objectives of the project
• Assessing the outcome of IAEA activities in NC
• Re‐shape those activities if needed
• Introduction of the concept of TQM– Help NC labs to validate their performance and quality of work– Improve when necessary

Participating centres are enrolled

Reporting form

Initial results (6 cases; 9 participants; 5 experts)
K‐value Interpretation
<0.00 Poor agreement
0.01‐0.20 Slight agreement
0.21‐0.40 Fair agreement
0.41‐0.60 Moderate agreement
0.61‐0.80 Substantial agreement
0.81‐1.00 Almost Perfect agreement

Almost perfect
Strong
Moderate
Weak
Minimal
None
Agreement level

Differences betweenthe groups are not statistically significant
Groups

Need of Standardization: recognize artifacts!•Mechanical & electronical
–Energy window–Detector center‐of‐rotation and alignment –Flood field non‐uniformity •Biological
–Myocardial hypertrophy –Left bundle branch block –Cardiac position with thorax•Patient‐related artifacts
–Soft‐tissue attenuation •breast lateral chest‐wall fat diaphragm
–Superimposed abdominal visceral activity–Motion artifacts
Processing artifacts– Selection of cardiac axes – Selection of apex and base for polar map

Conclusions
• QUANUM audits– Program easy to apply to all levels of NM
practices– Introduces the concept of internal (self)
auditing– Clinical services rendered with good standards – Radiation protection and radiopharmacy issues
to be closely scrutinized
• MPI clinical audit– Technically difficult to run (raw data transfer)– High variability of results– Need to strengthen the basics