Embed Size (px)
Citation preview
Journal of Dental Sciences (2013) 8, 296e305
Available online at www.sciencedirect.com
journal homepage: www.e- jds.com
ORIGINAL ARTICLE
Push-out bond strength and SEM analysis oftwo self-adhesive resin cements: An in vitrostudy
Bogdan Baldea a, Gabriel Furtos b, Mark Antal c, Katalin Nagy d,Dragos Popescu e, Luminita Nica f*
aDepartment of Prosthodontics, Faculty of Dental Medicine, Victor Babes University of Medicine andPharmacy, 9 Revolutiei 1989 Avenue, 300070 Timisoara, Romania
bDepartment of Dental Materials, “Raluca Ripan” Institute of Research in Chemistry, 30 FantaneleStreet, 400294 Cluj-Napoca, Romania
cDepartment of Operative and Esthetic Dentistry, Faculty of Dentistry, University of Szeged, TiszaLajos Korut 64, H-6720 Szeged, Hungary
dDepartment of Oral Surgery, Faculty of Dentistry, University of Szeged, Dugonics ter 13, H-6720Szeged, Hungary
e Private Dental Clinic, 72 Martir Petru Domasneanu Street, 300351 Timisoara, RomaniafDepartment of Endodontics, Faculty of Dental Medicine, Victor Babes University of Medicine andPharmacy, 9 Revolutiei 1989 Avenue, 300070 Timisoara, Romania
Received 6 November 2012; Final revision received 28 December 2012Available online 21 May 2013
KEYWORDSfiber posts;push-out bondstrength;
root canal dentine;self-adhesive resincements
* Corresponding author. DepartmentRevolutiei 1989 Avenue, 300070 Timis
E-mail address: [email protected]
1991-7902/$36 Copyrightª 2013, Assochttp://dx.doi.org/10.1016/j.jds.2013.0
Abstract Purpose: The retentive strength of two self-adhesive resin cements used for thecementation of fiberposts into root canals filledwithmethacrylate-based sealer and corematerial(Resilon) was evaluated using the thin-slices push-out test on human molars.Materials and methods: RelyX Fiber Posts #3 (3M ESPE, Seefeld, Germany) were luted with RelyXU200 (3M ESPE) (n Z 10) and Maxcem Elite (Kerr Corporation, Orange, CA, USA) (n Z 10). Meanvalues of push-out bond strength for each group and root region (cervical, middle and apical) werecalculated. Datawere statistically analyzedwith one-way ANOVA and Tukey’s test (P< 0.05). Fail-ure modes were evaluated using optical microscopy and scanning electron micrography (SEM).Results: Without being statistically significant, the bond strength of RelyX was higher(8.23 � 4.46 MPa) when compared to that of Maxcem Elite (6.52 � 3.68 MPa).
of Endodontics, Faculty of Dental Medicine, Victor Babes University of Medicine and Pharmacy, 9oara, Romania.m (L. Nica).
iation for Dental Sciences of the Republic of China. Published by Elsevier Taiwan LLC. All rights reserved.1.007

Push-out bond strength of two resin cements 297
Conclusions: Significant differences (P < 0.05) were observed between the apical and cervicalregions. More frequent (>60%) adhesive failures at the resin cement-dentine interface wereobserved.Copyrightª 2013, Association for Dental Sciences of the Republic of China. Published by ElsevierTaiwan LLC. All rights reserved.
Introduction
Prefabricated composite resin fiber posts have been usedfor the restoration of endodontically treated teeth sincethe 1990s, when carbon fiber posts, with an elastic modulussimilar to dentine, were introduced.1 Adhesively lutedfiber-reinforced composite (FRC) posts were introduced in1997 and have increasingly been used since then for therestoration of endodontically treated teeth.2
The retention of fiber posts in root canals is dependentupon adhesion between the resin cement and thedentine, as well as on adhesion between the resin cementand the posts. However, the adhesion between the resincement and the dentine is considered to be the weakpoint in luting a fiber post.3 Although bonding betweenthe post and the root canal dentine plays a pivotal role inthe long-term success of a restoration, ensuring reliablebonding between the post and the composite core is alsonecessary. If the bonding of that interface is poor,de-bonding and/or fracture of the core and post canoccur.4 Successful bonding minimizes the wedging effectof the post within the root canal and requires less dentineremoval to accommodate a shorter and thinner post;in addition, it leads to lower susceptibility to toothfracture.1
Bonding to root canals might be difficult, because ofthe handling characteristics of the adhesive system, rootanatomy, tooth position, the presence of coronal residualtissue, the use of a light-curing technique, the experi-ence and skill of the operators, etc.5 Self-adhesive ce-ments were introduced in 2002 as a new subgroup of resincements.6 They were designed with the intent of inte-grating the favorable characteristics of different cementclasses into a single product.6 Their main advantage isthe simplicity of clinical use. These cements are ex-pected to offer properties analogous to those of resincements.
The aim of the present study was to evaluate thepush-out bond strength of two new self-adhesive resincements (SARCs) used for luting glass fiber posts intoendodontically treated root canals filled with methacry-late resin-based sealer (Epiphany SE, Pentron ClinicalTechnologies LLC) and core material (Resilon Epiphany,Pentron Clinical Technologies LLC). The failure modeswere examined by optical microscopy, and different in-terfaces of randomly selected samples were evaluatedwith scanning electron micrography (SEM) after the push-out test. The null hypotheses tested were as follows: (1)the type of resin cement does not affect bond strengthand (2) the region of the post/root canal does not influ-ence bond strength.
Materials and methods
Specimen preparation
Sample preparation and root canal fillingTwenty recently extracted, non-carious human maxillaryand mandibular molars, with one straight palatal or distalroot canal and fully developed apices, extracted for peri-odontal reasons, were selected for this study. All patientsprovided their informed consent. The study was approvedby the Commission on Bioethics of the Victor Babes Uni-versity of Medicine of Timisoara. After extraction, the teethwere cleaned of soft tissue and calculus and stored in 0.1%thymol solution steam at 9�C. Before use, teeth werewashed under running water for 24 hours, blot dried andstored in normal saline at 37�C and 95% humidity untiltesting.3
The crowns were sectioned 2 mm occlusally, above thecemento-enamel junction (CEJ), with a low-speed diamondsaw (IsoMet 1000, Buehler Ltd., Lake Bluff, IL, USA) withwater cooling (Fig. 1A), which exposed the pulp chamber. Thepulp chambers were opened completely, the dental pulp wasremoved and the root canal preparation was completed(Fig. 1B) with a size-40 master apical file, 10% taper, using acrown-down motion and nickel-titanium (NiTi) rotary GTinstruments (Dentsply Tulsa Dental, OK, USA). The toothsamples in which the size and shape of the root canal weredifferent from that of the post were excluded from thebeginning of the study and were not endodontically treated.All procedureswere performed using theOPMI Pico (Carl ZeissAG, Oberkochen, Germany) dental operating microscope.
Irrigation was performed during instrumentation withsodium hypochlorite (NaOCl) 5.25%, which was deliveredthrough the master delivery tip (MDT) of the EndoVac sys-tem (Discus Dental, Culver City, CA, USA) until the end-odontic preparation was completed. The macrocannula ofthe EndoVac system was then used for a 30 second period ofirrigation with 5.25% NaOCl. The canal was then left full ofirrigant for 30 seconds. Three cycles of micro irrigationusing the microcannula placed at full working length fol-lowed. These involved the use, alternatively, of 5.25%NaOCl and 17% ethylenediaminetetraacetic acid (EDTA)solution.7 Finally, another cycle of micro irrigation usingEDTA as the final irrigant was performed, because the teethwere adhesively obturated using Resilon core material(Epihany, Pentron Clinical Technologies LLC) and EpiphanySE (Pentron Clinical Technologies LLC) as sealer. The canalswere then rinsed with distilled water and dried with paperpoints. Epiphany SE sealer (Pentron) was applied to the rootcanals using fine-medium paper points (Dentsply Maillefer,
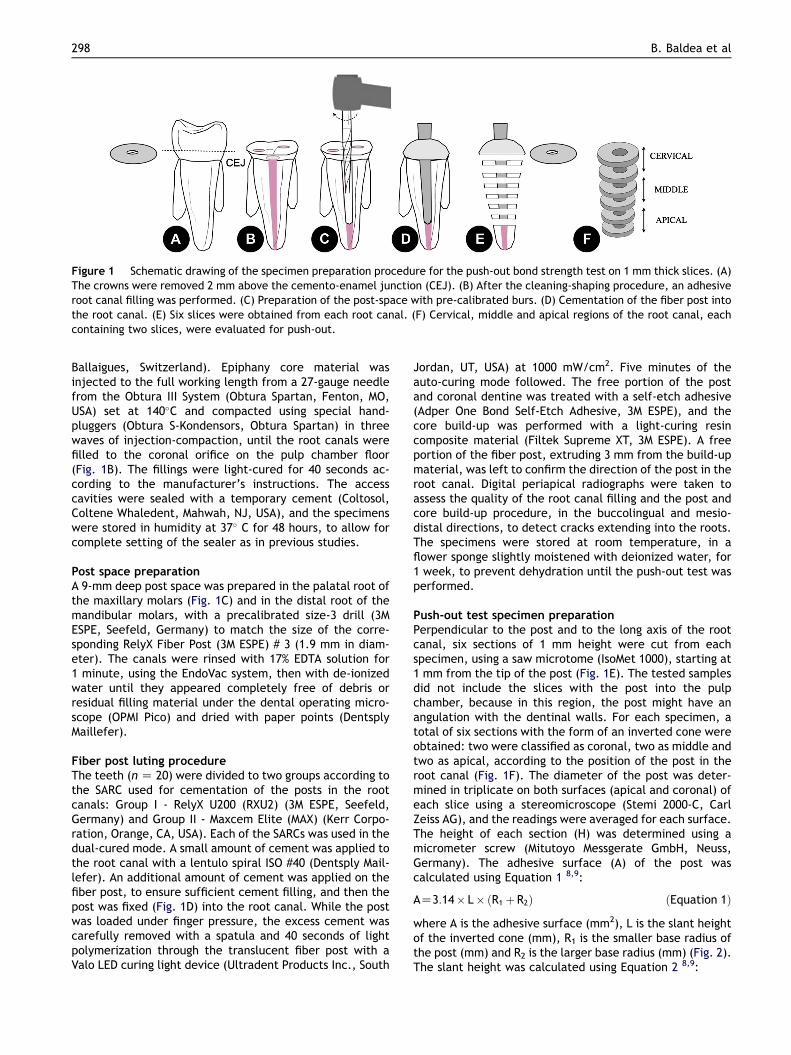
Figure 1 Schematic drawing of the specimen preparation procedure for the push-out bond strength test on 1 mm thick slices. (A)The crowns were removed 2 mm above the cemento-enamel junction (CEJ). (B) After the cleaning-shaping procedure, an adhesiveroot canal filling was performed. (C) Preparation of the post-space with pre-calibrated burs. (D) Cementation of the fiber post intothe root canal. (E) Six slices were obtained from each root canal. (F) Cervical, middle and apical regions of the root canal, eachcontaining two slices, were evaluated for push-out.
298 B. Baldea et al
Ballaigues, Switzerland). Epiphany core material wasinjected to the full working length from a 27-gauge needlefrom the Obtura III System (Obtura Spartan, Fenton, MO,USA) set at 140�C and compacted using special hand-pluggers (Obtura S-Kondensors, Obtura Spartan) in threewaves of injection-compaction, until the root canals werefilled to the coronal orifice on the pulp chamber floor(Fig. 1B). The fillings were light-cured for 40 seconds ac-cording to the manufacturer’s instructions. The accesscavities were sealed with a temporary cement (Coltosol,Coltene Whaledent, Mahwah, NJ, USA), and the specimenswere stored in humidity at 37� C for 48 hours, to allow forcomplete setting of the sealer as in previous studies.
Post space preparationA 9-mm deep post space was prepared in the palatal root ofthe maxillary molars (Fig. 1C) and in the distal root of themandibular molars, with a precalibrated size-3 drill (3MESPE, Seefeld, Germany) to match the size of the corre-sponding RelyX Fiber Post (3M ESPE) # 3 (1.9 mm in diam-eter). The canals were rinsed with 17% EDTA solution for1 minute, using the EndoVac system, then with de-ionizedwater until they appeared completely free of debris orresidual filling material under the dental operating micro-scope (OPMI Pico) and dried with paper points (DentsplyMaillefer).
Fiber post luting procedureThe teeth (n Z 20) were divided to two groups according tothe SARC used for cementation of the posts in the rootcanals: Group I - RelyX U200 (RXU2) (3M ESPE, Seefeld,Germany) and Group II - Maxcem Elite (MAX) (Kerr Corpo-ration, Orange, CA, USA). Each of the SARCs was used in thedual-cured mode. A small amount of cement was applied tothe root canal with a lentulo spiral ISO #40 (Dentsply Mail-lefer). An additional amount of cement was applied on thefiber post, to ensure sufficient cement filling, and then thepost was fixed (Fig. 1D) into the root canal. While the postwas loaded under finger pressure, the excess cement wascarefully removed with a spatula and 40 seconds of lightpolymerization through the translucent fiber post with aValo LED curing light device (Ultradent Products Inc., South
Jordan, UT, USA) at 1000 mW/cm2. Five minutes of theauto-curing mode followed. The free portion of the postand coronal dentine was treated with a self-etch adhesive(Adper One Bond Self-Etch Adhesive, 3M ESPE), and thecore build-up was performed with a light-curing resincomposite material (Filtek Supreme XT, 3M ESPE). A freeportion of the fiber post, extruding 3 mm from the build-upmaterial, was left to confirm the direction of the post in theroot canal. Digital periapical radiographs were taken toassess the quality of the root canal filling and the post andcore build-up procedure, in the buccolingual and mesio-distal directions, to detect cracks extending into the roots.The specimens were stored at room temperature, in aflower sponge slightly moistened with deionized water, for1 week, to prevent dehydration until the push-out test wasperformed.
Push-out test specimen preparationPerpendicular to the post and to the long axis of the rootcanal, six sections of 1 mm height were cut from eachspecimen, using a saw microtome (IsoMet 1000), starting at1 mm from the tip of the post (Fig. 1E). The tested samplesdid not include the slices with the post into the pulpchamber, because in this region, the post might have anangulation with the dentinal walls. For each specimen, atotal of six sections with the form of an inverted cone wereobtained: two were classified as coronal, two as middle andtwo as apical, according to the position of the post in theroot canal (Fig. 1F). The diameter of the post was deter-mined in triplicate on both surfaces (apical and coronal) ofeach slice using a stereomicroscope (Stemi 2000-C, CarlZeiss AG), and the readings were averaged for each surface.The height of each section (H) was determined using amicrometer screw (Mitutoyo Messgerate GmbH, Neuss,Germany). The adhesive surface (A) of the post wascalculated using Equation 1 8,9:
AZ3:14� L� ðR1 þ R2Þ ðEquation 1Þwhere A is the adhesive surface (mm2), L is the slant heightof the inverted cone (mm), R1 is the smaller base radius ofthe post (mm) and R2 is the larger base radius (mm) (Fig. 2).The slant height was calculated using Equation 2 8,9:
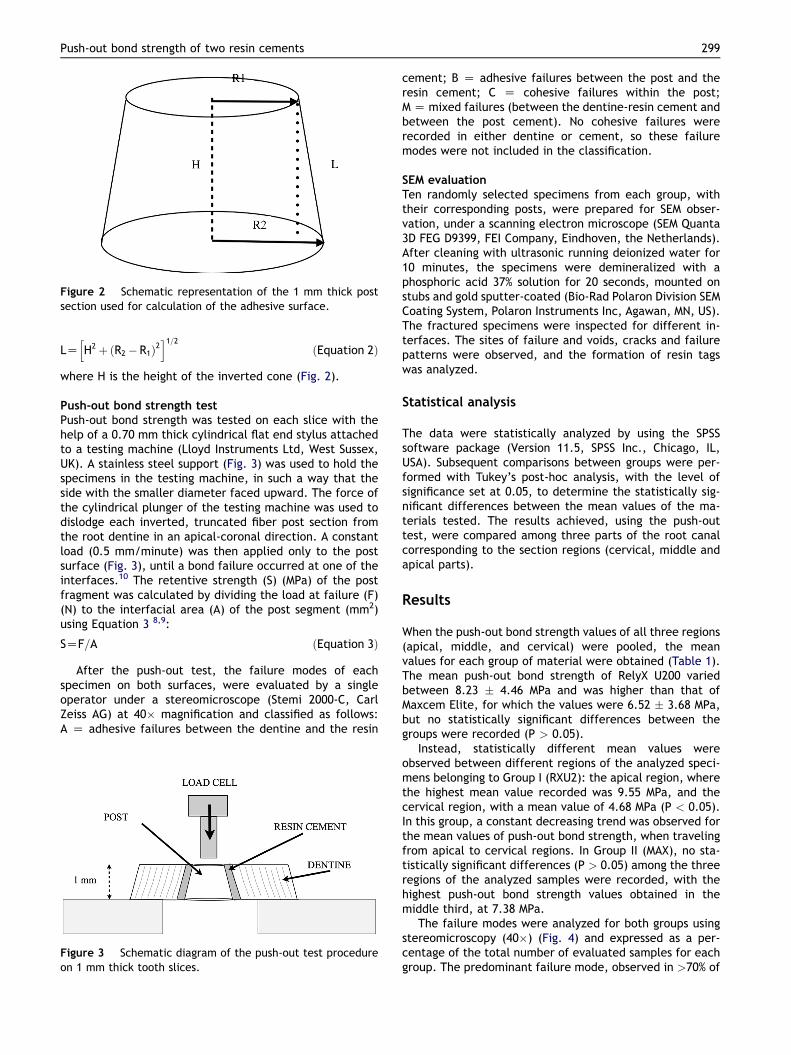
Figure 2 Schematic representation of the 1 mm thick postsection used for calculation of the adhesive surface.
Push-out bond strength of two resin cements 299
LZhH2 þ ðR2 � R1Þ2
i1=2ðEquation 2Þ
where H is the height of the inverted cone (Fig. 2).
Push-out bond strength testPush-out bond strength was tested on each slice with thehelp of a 0.70 mm thick cylindrical flat end stylus attachedto a testing machine (Lloyd Instruments Ltd, West Sussex,UK). A stainless steel support (Fig. 3) was used to hold thespecimens in the testing machine, in such a way that theside with the smaller diameter faced upward. The force ofthe cylindrical plunger of the testing machine was used todislodge each inverted, truncated fiber post section fromthe root dentine in an apical-coronal direction. A constantload (0.5 mm/minute) was then applied only to the postsurface (Fig. 3), until a bond failure occurred at one of theinterfaces.10 The retentive strength (S) (MPa) of the postfragment was calculated by dividing the load at failure (F)(N) to the interfacial area (A) of the post segment (mm2)using Equation 3 8,9:
SZF=A ðEquation 3Þ
After the push-out test, the failure modes of eachspecimen on both surfaces, were evaluated by a singleoperator under a stereomicroscope (Stemi 2000-C, CarlZeiss AG) at 40� magnification and classified as follows:A Z adhesive failures between the dentine and the resin
Figure 3 Schematic diagram of the push-out test procedureon 1 mm thick tooth slices.
cement; B Z adhesive failures between the post and theresin cement; C Z cohesive failures within the post;M Z mixed failures (between the dentine-resin cement andbetween the post cement). No cohesive failures wererecorded in either dentine or cement, so these failuremodes were not included in the classification.
SEM evaluationTen randomly selected specimens from each group, withtheir corresponding posts, were prepared for SEM obser-vation, under a scanning electron microscope (SEM Quanta3D FEG D9399, FEI Company, Eindhoven, the Netherlands).After cleaning with ultrasonic running deionized water for10 minutes, the specimens were demineralized with aphosphoric acid 37% solution for 20 seconds, mounted onstubs and gold sputter-coated (Bio-Rad Polaron Division SEMCoating System, Polaron Instruments Inc, Agawan, MN, US).The fractured specimens were inspected for different in-terfaces. The sites of failure and voids, cracks and failurepatterns were observed, and the formation of resin tagswas analyzed.
Statistical analysis
The data were statistically analyzed by using the SPSSsoftware package (Version 11.5, SPSS Inc., Chicago, IL,USA). Subsequent comparisons between groups were per-formed with Tukey’s post-hoc analysis, with the level ofsignificance set at 0.05, to determine the statistically sig-nificant differences between the mean values of the ma-terials tested. The results achieved, using the push-outtest, were compared among three parts of the root canalcorresponding to the section regions (cervical, middle andapical parts).
Results
When the push-out bond strength values of all three regions(apical, middle, and cervical) were pooled, the meanvalues for each group of material were obtained (Table 1).The mean push-out bond strength of RelyX U200 variedbetween 8.23 � 4.46 MPa and was higher than that ofMaxcem Elite, for which the values were 6.52 � 3.68 MPa,but no statistically significant differences between thegroups were recorded (P > 0.05).
Instead, statistically different mean values wereobserved between different regions of the analyzed speci-mens belonging to Group I (RXU2): the apical region, wherethe highest mean value recorded was 9.55 MPa, and thecervical region, with a mean value of 4.68 MPa (P < 0.05).In this group, a constant decreasing trend was observed forthe mean values of push-out bond strength, when travelingfrom apical to cervical regions. In Group II (MAX), no sta-tistically significant differences (P > 0.05) among the threeregions of the analyzed samples were recorded, with thehighest push-out bond strength values obtained in themiddle third, at 7.38 MPa.
The failure modes were analyzed for both groups usingstereomicroscopy (40�) (Fig. 4) and expressed as a per-centage of the total number of evaluated samples for eachgroup. The predominant failure mode, observed in >70% of
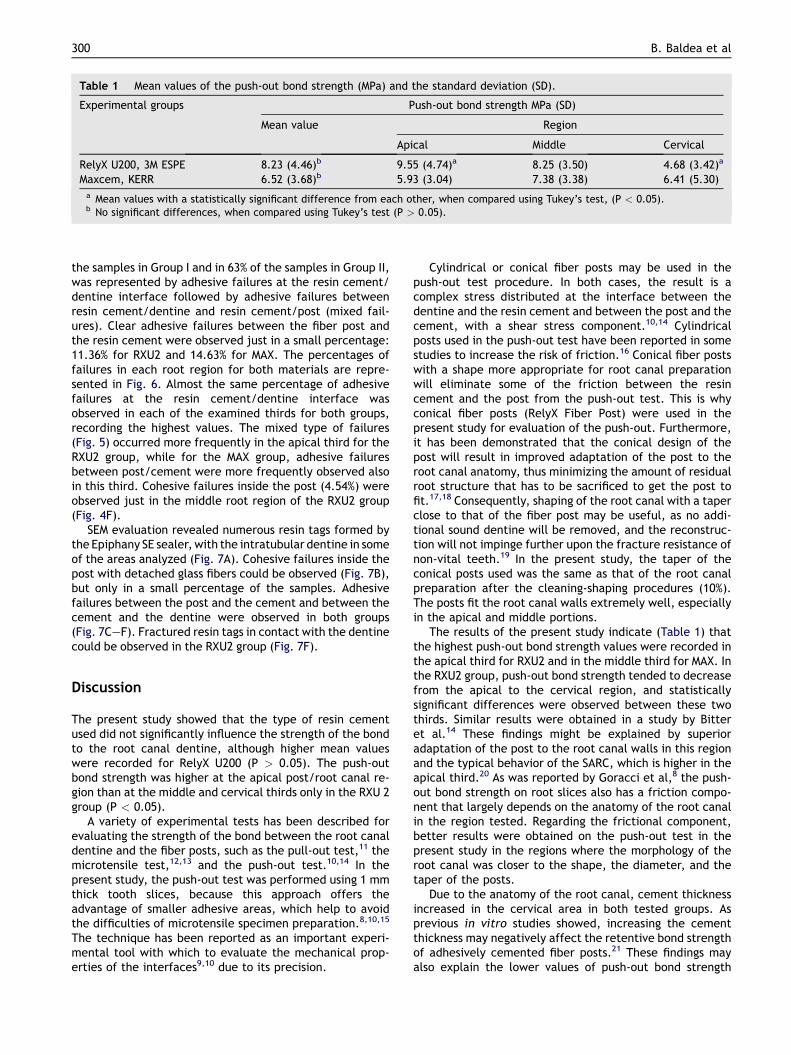
Table 1 Mean values of the push-out bond strength (MPa) and the standard deviation (SD).
Experimental groups Push-out bond strength MPa (SD)
Mean value Region
Apical Middle Cervical
RelyX U200, 3M ESPE 8.23 (4.46)b 9.55 (4.74)a 8.25 (3.50) 4.68 (3.42)a
Maxcem, KERR 6.52 (3.68)b 5.93 (3.04) 7.38 (3.38) 6.41 (5.30)a Mean values with a statistically significant difference from each other, when compared using Tukey’s test, (P < 0.05).b No significant differences, when compared using Tukey’s test (P > 0.05).
300 B. Baldea et al
the samples in Group I and in 63% of the samples in Group II,was represented by adhesive failures at the resin cement/dentine interface followed by adhesive failures betweenresin cement/dentine and resin cement/post (mixed fail-ures). Clear adhesive failures between the fiber post andthe resin cement were observed just in a small percentage:11.36% for RXU2 and 14.63% for MAX. The percentages offailures in each root region for both materials are repre-sented in Fig. 6. Almost the same percentage of adhesivefailures at the resin cement/dentine interface wasobserved in each of the examined thirds for both groups,recording the highest values. The mixed type of failures(Fig. 5) occurred more frequently in the apical third for theRXU2 group, while for the MAX group, adhesive failuresbetween post/cement were more frequently observed alsoin this third. Cohesive failures inside the post (4.54%) wereobserved just in the middle root region of the RXU2 group(Fig. 4F).
SEM evaluation revealed numerous resin tags formed bythe Epiphany SE sealer, with the intratubular dentine in someof the areas analyzed (Fig. 7A). Cohesive failures inside thepost with detached glass fibers could be observed (Fig. 7B),but only in a small percentage of the samples. Adhesivefailures between the post and the cement and between thecement and the dentine were observed in both groups(Fig. 7CeF). Fractured resin tags in contact with the dentinecould be observed in the RXU2 group (Fig. 7F).
Discussion
The present study showed that the type of resin cementused did not significantly influence the strength of the bondto the root canal dentine, although higher mean valueswere recorded for RelyX U200 (P > 0.05). The push-outbond strength was higher at the apical post/root canal re-gion than at the middle and cervical thirds only in the RXU 2group (P < 0.05).
A variety of experimental tests has been described forevaluating the strength of the bond between the root canaldentine and the fiber posts, such as the pull-out test,11 themicrotensile test,12,13 and the push-out test.10,14 In thepresent study, the push-out test was performed using 1 mmthick tooth slices, because this approach offers theadvantage of smaller adhesive areas, which help to avoidthe difficulties of microtensile specimen preparation.8,10,15
The technique has been reported as an important experi-mental tool with which to evaluate the mechanical prop-erties of the interfaces9,10 due to its precision.
Cylindrical or conical fiber posts may be used in thepush-out test procedure. In both cases, the result is acomplex stress distributed at the interface between thedentine and the resin cement and between the post and thecement, with a shear stress component.10,14 Cylindricalposts used in the push-out test have been reported in somestudies to increase the risk of friction.16 Conical fiber postswith a shape more appropriate for root canal preparationwill eliminate some of the friction between the resincement and the post from the push-out test. This is whyconical fiber posts (RelyX Fiber Post) were used in thepresent study for evaluation of the push-out. Furthermore,it has been demonstrated that the conical design of thepost will result in improved adaptation of the post to theroot canal anatomy, thus minimizing the amount of residualroot structure that has to be sacrificed to get the post tofit.17,18 Consequently, shaping of the root canal with a taperclose to that of the fiber post may be useful, as no addi-tional sound dentine will be removed, and the reconstruc-tion will not impinge further upon the fracture resistance ofnon-vital teeth.19 In the present study, the taper of theconical posts used was the same as that of the root canalpreparation after the cleaning-shaping procedures (10%).The posts fit the root canal walls extremely well, especiallyin the apical and middle portions.
The results of the present study indicate (Table 1) thatthe highest push-out bond strength values were recorded inthe apical third for RXU2 and in the middle third for MAX. Inthe RXU2 group, push-out bond strength tended to decreasefrom the apical to the cervical region, and statisticallysignificant differences were observed between these twothirds. Similar results were obtained in a study by Bitteret al.14 These findings might be explained by superioradaptation of the post to the root canal walls in this regionand the typical behavior of the SARC, which is higher in theapical third.20 As was reported by Goracci et al,8 the push-out bond strength on root slices also has a friction compo-nent that largely depends on the anatomy of the root canalin the region tested. Regarding the frictional component,better results were obtained on the push-out test in thepresent study in the regions where the morphology of theroot canal was closer to the shape, the diameter, and thetaper of the posts.
Due to the anatomy of the root canal, cement thicknessincreased in the cervical area in both tested groups. Asprevious in vitro studies showed, increasing the cementthickness may negatively affect the retentive bond strengthof adhesively cemented fiber posts.21 These findings mayalso explain the lower values of push-out bond strength

Figure 4 Representative optical microscopy images (40�) of the failure types: (A) sample with RXU2 before testing (red arrowsdResilon filling material) and (B) adhesive failure on the dentine interface after testingdResilon remained on the cement surface(red arrows); (C) sample with MAX before testing and (D) mixed failure after testing (white arrowdadhesive failure betweencement and the post; red arrowdadhesive failure at the dentine interface); (E) sample with RXU2 before testing; and (F) cohesivefailure within the post after testing (red arrow). D Z dentine; P Z post.
Push-out bond strength of two resin cements 301
recorded in the cervical region for both groups. Otherstudies found that the cement thickness around the postdid not significantly affect the bond strength of fiber poststo root dentine.9,22
Self-adhesive resin cements are still relatively new, anddetailed information on their composition and adhesive
properties is scarce. The basic adhesion mechanism ap-pears to be based on the micromechanical retention andchemical interaction between the monomer acidic groupsand hydroxyapatite.6,23 Multifunctional monomers withphosphoric acid groups simultaneously demineralize andinfiltrate enamel and dentine.6,24
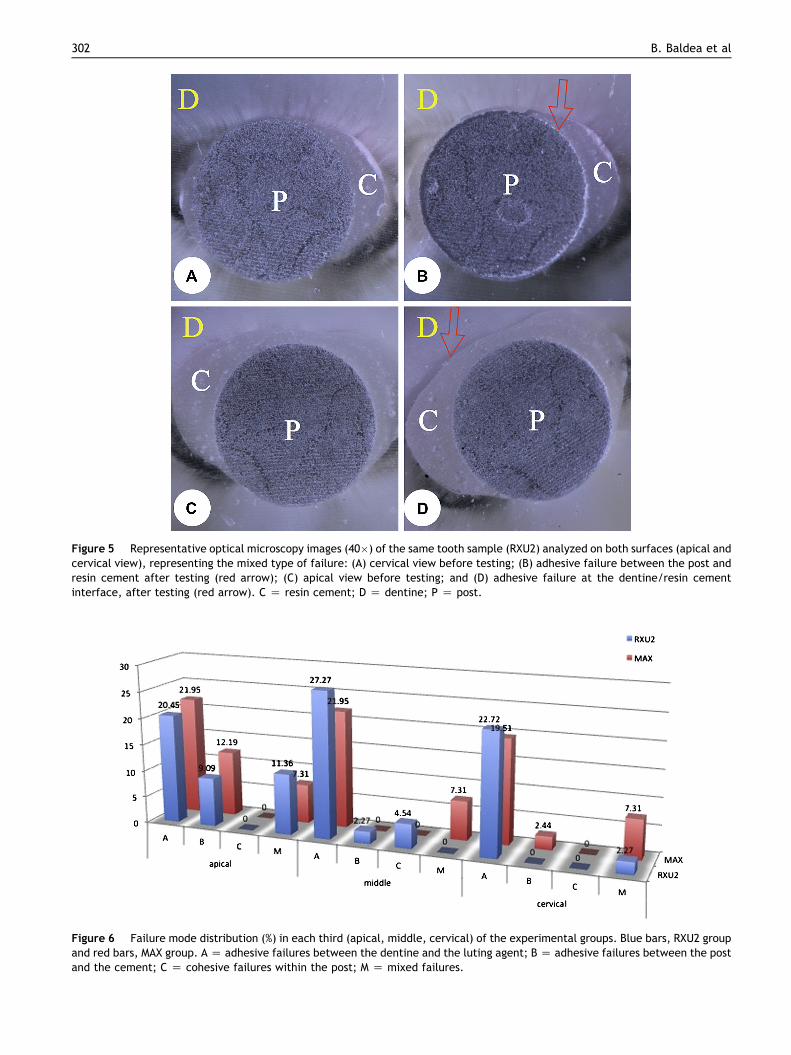
Figure 5 Representative optical microscopy images (40�) of the same tooth sample (RXU2) analyzed on both surfaces (apical andcervical view), representing the mixed type of failure: (A) cervical view before testing; (B) adhesive failure between the post andresin cement after testing (red arrow); (C) apical view before testing; and (D) adhesive failure at the dentine/resin cementinterface, after testing (red arrow). C Z resin cement; D Z dentine; P Z post.
Figure 6 Failure mode distribution (%) in each third (apical, middle, cervical) of the experimental groups. Blue bars, RXU2 groupand red bars, MAX group. A Z adhesive failures between the dentine and the luting agent; B Z adhesive failures between the postand the cement; C Z cohesive failures within the post; M Z mixed failures.
302 B. Baldea et al
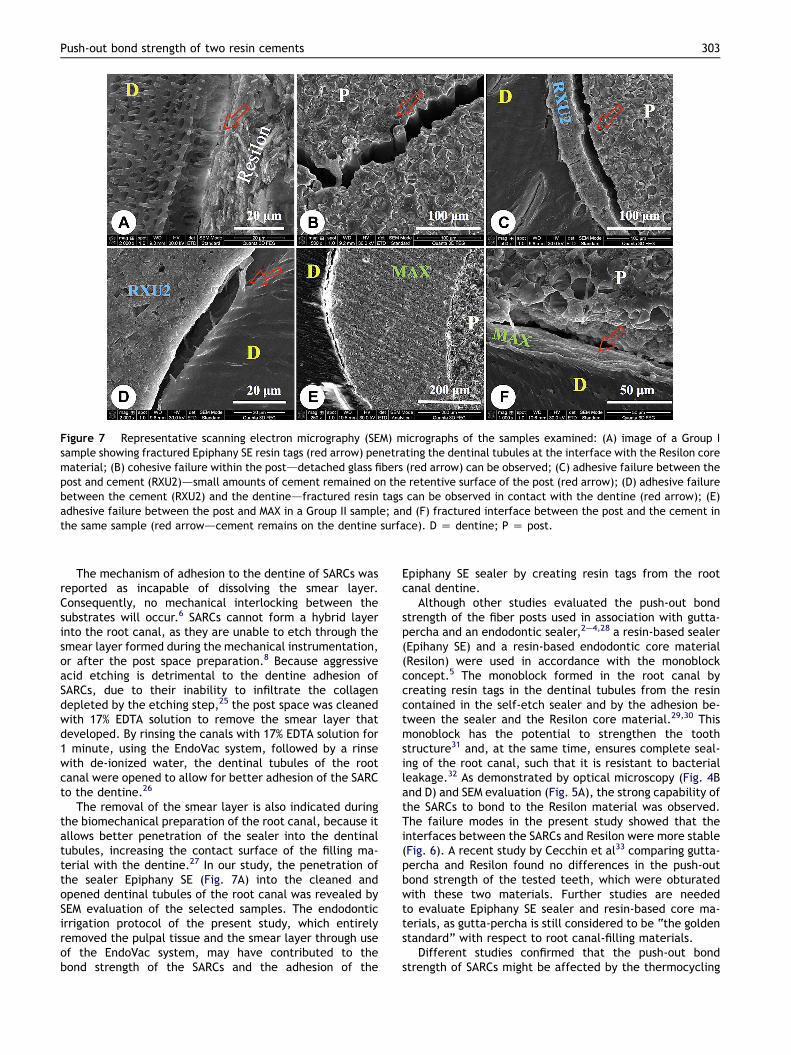
Figure 7 Representative scanning electron micrography (SEM) micrographs of the samples examined: (A) image of a Group Isample showing fractured Epiphany SE resin tags (red arrow) penetrating the dentinal tubules at the interface with the Resilon corematerial; (B) cohesive failure within the postddetached glass fibers (red arrow) can be observed; (C) adhesive failure between thepost and cement (RXU2)dsmall amounts of cement remained on the retentive surface of the post (red arrow); (D) adhesive failurebetween the cement (RXU2) and the dentinedfractured resin tags can be observed in contact with the dentine (red arrow); (E)adhesive failure between the post and MAX in a Group II sample; and (F) fractured interface between the post and the cement inthe same sample (red arrowdcement remains on the dentine surface). D Z dentine; P Z post.
Push-out bond strength of two resin cements 303
The mechanism of adhesion to the dentine of SARCs wasreported as incapable of dissolving the smear layer.Consequently, no mechanical interlocking between thesubstrates will occur.6 SARCs cannot form a hybrid layerinto the root canal, as they are unable to etch through thesmear layer formed during the mechanical instrumentation,or after the post space preparation.8 Because aggressiveacid etching is detrimental to the dentine adhesion ofSARCs, due to their inability to infiltrate the collagendepleted by the etching step,25 the post space was cleanedwith 17% EDTA solution to remove the smear layer thatdeveloped. By rinsing the canals with 17% EDTA solution for1 minute, using the EndoVac system, followed by a rinsewith de-ionized water, the dentinal tubules of the rootcanal were opened to allow for better adhesion of the SARCto the dentine.26
The removal of the smear layer is also indicated duringthe biomechanical preparation of the root canal, because itallows better penetration of the sealer into the dentinaltubules, increasing the contact surface of the filling ma-terial with the dentine.27 In our study, the penetration ofthe sealer Epiphany SE (Fig. 7A) into the cleaned andopened dentinal tubules of the root canal was revealed bySEM evaluation of the selected samples. The endodonticirrigation protocol of the present study, which entirelyremoved the pulpal tissue and the smear layer through useof the EndoVac system, may have contributed to thebond strength of the SARCs and the adhesion of the
Epiphany SE sealer by creating resin tags from the rootcanal dentine.
Although other studies evaluated the push-out bondstrength of the fiber posts used in association with gutta-percha and an endodontic sealer,2e4,28 a resin-based sealer(Epihany SE) and a resin-based endodontic core material(Resilon) were used in accordance with the monoblockconcept.5 The monoblock formed in the root canal bycreating resin tags in the dentinal tubules from the resincontained in the self-etch sealer and by the adhesion be-tween the sealer and the Resilon core material.29,30 Thismonoblock has the potential to strengthen the toothstructure31 and, at the same time, ensures complete seal-ing of the root canal, such that it is resistant to bacterialleakage.32 As demonstrated by optical microscopy (Fig. 4Band D) and SEM evaluation (Fig. 5A), the strong capability ofthe SARCs to bond to the Resilon material was observed.The failure modes in the present study showed that theinterfaces between the SARCs and Resilon were more stable(Fig. 6). A recent study by Cecchin et al33 comparing gutta-percha and Resilon found no differences in the push-outbond strength of the tested teeth, which were obturatedwith these two materials. Further studies are neededto evaluate Epiphany SE sealer and resin-based core ma-terials, as gutta-percha is still considered to be “the goldenstandard” with respect to root canal-filling materials.
Different studies confirmed that the push-out bondstrength of SARCs might be affected by the thermocycling

304 B. Baldea et al
of the samples before testing,14,34,35 or by the time forwhich the samples were stored between luting of the fiberposts into the root canal and the mechanical testing.12 Inthe present study, all samples were tested for push-outbond strength 7 days after curing, similarly to previousstudies.12,28 In the studies mentioned, the bond strengthvalues noted after 7 days of storage were higher than after24 or 48 hours. An explanation of these higher values,recorded at 7 days, may be related to a higher degree ofmonomer to polymer conversion, which increases the de-gree of conversion.36
According to the manufacturer’s instructions (3M ESPE),the procedure used for post luting requires no pretreatmentbecause the machine-shaped outer surface of the post willprovide a sufficient retentive surface for the resin cement,despite its inert chemical behavior.37 Analysis of thecohesive failures within the post (Fig. 4F) revealed that thefracture lines might propagate throughout the resin matrixof the post (Fig. 7B), and this could be influenced by a non-uniform distribution of the glass-fibers inside the post, bythe highly adhesive properties of the luting cement or bythe high frictional effect with the dentinal walls. Also,other studies regarding the bond strength of SARCs reportedcohesive failures inside the post,38,39 but they did notexplain them. The push out bond strength test has animportant frictional component between the post and thedentine.8 As the cohesive failures inside the post wereobserved in the present study only in the RXU group (Fig. 6),it can also be supposed that in these samples the frictionalcomponent was higher, enhanced by the good retentivestrength between the post and the cement (Figs. 4F and7B).
Regarding their clinical characteristics, both cementsproved to be easy to use, making the technique more pre-dictable compared to the use of other types of luting ce-ments. RXU2 had a better flow capability, and fewer voidswere observed in this group when compared to MAX. Goodadhesion between the RelyX Fiber Posts and SARCs, RXU2,and MAX, was observed. Instead, adhesive failures betweenthe dentine and the resin cement were commonlyobserved, which may be attributed to stress under clinicalconditions.14,40 These findings are in agreement with pre-vious studies,3,8,20,39 which showed that most of the fail-ures occurred at the cement-dentine interface.
Within the limitations of this in vitro study, the followingconclusions may be drawn:
1. The mean push-out bond strength of teeth samplescontaining RelyX U200 was higher than that observedfor Maxcem Elite.
2. The most fragile region appeared to be the adhesiveinterface between the SARC and the dentine. There-fore, it can be presumed that the interface betweenthe SARC and fiber post was more stable in this study.
Acknowledgments
This study received financial support from project POSDRU/88/1.5/S/63117, co-financed by the European Social Fund,Sectorial Operational Programme for Human ResourcesDevelopment 2007e2013. The authors also thank the
project COST Action TD0906 “Biological Adhesives fromBiology to Biomimetics” for meeting support.
References
1. Sidoli GE, King PA, Setchell DJ. In vitro evaluation of a carbonfiber-based post and core system. J Prosthet Dent 1997;78:5e9.
2. Bitter K, Kielbassa AM. Post-endodontic restorations withadhesively luted fiber-reinforced composite post system: areview. American J Dent 2007;20:350e60.
3. Manicardi CA, Versiani MA, Saquy PC, Pecora JD, de Sousa-Neto MD. Influence of filling materials on the bonding interfaceof thin-walled roots reinforced with resin and quartz fiberposts. J Endod 2011;37:531e7.
4. Perdigao J, Gomes G, Augusto V. The effect of dowel space onthe bond strengths of fiber posts. J Prosthodont 2007;16:154e64.
5. Tay FR, Pashley DH. Monoblocks in root canals: a hypotheticalor a tangible goal. J Endod 2007;33:391e8.
6. Radovic I, Monticelli F, Goracci C, Vulicevic ZR, Ferrari M. Self-adhesive resin cements: a literature review. J Adhes Dent2008;10:251e8.
7. Nielsen BA, Craig Baumgartner J. Comparison of the EndoVacsystem to needle irrigation of root canals. J Endod 2007;33:611e5.
8. Goracci C, Sadek FT, Fabianelli A, Tay FR, Ferrari M. Evaluationof the adhesion of fiber posts to intraradicular dentin. OperDent 2005;30:627e35.
9. Coniglio I, Magni E, Cantoro A, Goracci C, Ferrari M. Push-outbond strength of circular and oval-shaped fiber posts. Clin OralInvestig 2011;15:667e72.
10. Goracci C, Tavares AU, Fabianelli A, et al. The adhesion be-tween fiber posts and root canal walls: comparison betweenmicrotensile and push-out bond strength measurements. Eur JOral Sci 2004;112:353e61.
11. De Santis R, Prisco D, Apicella A, Ambrosio L, Rengo S,Nicolais L. Carbon fiber post adhesion to resin luting cement inthe restoration of endodontically treated teeth. J Mater SciMater Med 2000;1:201e6.
12. Vano M, Cury AH, Goracci C, et al. Retention of fiber postscemented at different time intervals in canals obturated usingan epoxy resin sealer. J Dent 2008;36:801e7.
13. Magni E, Mazzitelli C, Papacchini F, et al. Adhesion betweenfiber posts and resin luting agents: a microtensile bondstrength test and an SEM investigation following differenttreatments of the post surface. J Adhes Dent 2007;9:195e202.
14. Bitter K, Meyer-Lueckel H, Priehn K, Kanjuparambil JP,Neumann K, Kielbassa AM. Effects of luting agent and ther-mocycling on bond strengths to root canal dentine. Int Endod J2006;39:809e18.
15. Bouillaguet S, Scutt A, Alander P, et al. Hypothermal and me-chanical stresses degrade fiber-matrix interfacial bondstrengthin dental fiber-reinforced composites. J Biomed Mater Res BAppl Biomater 2006;76:98e105.
16. Toman M, Toksavul S, Sarıkanat M, Firidino�glu K, Akin A. Theevaluation of displacement resistance of glass FRC posts toroot dentine using a thin slice push-out test. Int Endod J 2009;42:802e10.
17. Grandini S, Goracci C, Tay FR, Grandini R, Ferrari M. Clinicalevaluation of the use of fiber posts and direct resin restorationsfor endodontically treated teeth. Int J Prosthodont 2005;18:399e404.
18. Schwartz RS, Robbins JW. Post placement and restoration ofendodontically treated teeth: a literature review. J Endod2004;30:289e301.

Push-out bond strength of two resin cements 305
19. Cheung W. A review of the management of endodonticallytreated teeth: post, core and the final restoration. J Am DentAssoc 2005;136:611e9.
20. Zicari F, Couthino E, De Munck J, et al. Bonding effectivenessand sealing ability of fiber-post bonding. Dent Mater 2008;24:967e77.
21. D’Arcangelo C, Cinelli M, De Angelis F, D’Amario M. The effectof resin cement film thickness on the pullout strength of afiber-reinforced post system. J Prosthet Dent 2007;98:193e8.
22. Perez BE, Barbosa SH, Melo RM, et al. Does the thickness of theresin cement affect the bond strength of a fiber post to theroot dentin? Int J Prosthodont 2006;19:606e9.
23. Van Landuyt KL, Yoshida Y, Hirata I, et al. Influence of thechemical structure of functional monomers on their adhesiveperformance. J Dent Res 2008;87:757e61.
24. Ferracane JL, Stansbury JW, Burke JT. Self-adhesive resin ce-ments e chemistry, properties and clinical considerations. JOral Rehabil 2011;38:295e314.
25. De Munck J, Vargas M, Van Landuyt K, Hikita K, Lambrechts P,Van Meerbeek B. Bonding of an auto-adhesive luting materialto enamel and dentin. Dent Mater 2004;20:963e71.
26. Barbosa De Souza F, Sincler Delfino C, Lacalle Turbino M,Braz R. Deproteinized dentin: a favorable substrate to self-bonding resin cements? J Biomed Mater Res B Appl Biomater2011;98:387e94.
27. Nunes VH, Silva RG, Alfredo E, Sousa-Neto MD, Silva-Sousa YT.Adhesion of Epiphany and AH Plus Sealers to human root dentintreated with different solutions. Braz Dent J 2008;19:46e50.
28. Bandeca MC, Kassem AS, El-Mowafy O, et al. Influence ofstorage times on bond strength of resin cements to root canal.Mater Res 2010;13:25e8.
29. Resende LM,Rached-Junior FJ, VersianiMA, et al. A comparativestudy of physicochemical properties of AH Plus, Epiphany, andEpiphany SE root canal sealers. Int Endod J 2009;42:785e93.
30. Costa JA, Rached-Junior FA, Souza-Gabriel AE, Silva-Souza YT, Souza-Neto MD. Push-out strength of methacrylate
resin-based sealers to root canal walls. Int Endod J 2010;43:698e706.
31. Teixeira FB, Teixeira EC, Thompson JY, Trope M. Fractureresistance of roots endodontically treated with a new resinfilling material. J Am Dent Assoc 2004;135:646e52.
32. Shipper G, Ørstavik D, Teixeira FB, Trope M. An evaluation ofmicrobial leakage in roots filled with a thermoplastic syntheticpolymer-based root canal filling material (Resilon). J Endod2004;30:342e7.
33. Cecchin D, Farina AP, Souza MA, Carlini-Junior B, Ferraz CC.Effect of root canal sealers on bond strength of fibreglass postscemented with self-adhesive resin cements. Int Endod J 2011;44:314e20.
34. Sadek FT, Goracci C, Monticelli F, et al. Immediate and 24-hourevaluation of the interfacial strengths of fiber posts. J Endod2006;32:1174e7.
35. Mazzoni A, Marchesi G, Cadenaro M, et al. Push-out stress forfibre posts luted using different adhesive strategies. Eur J OralSci 2009;117:447e53.
36. Bandeca MC, El-Mowafy O, Saade EG, Rastelli ANS, Bagnato VS,Porto-Neto ST. Changes on degree of conversion of dual-cureluting light-cured with blue LED. Laser Physics 2009;19:1050e5.
37. Zhang L, Wang Y, Radovic I, Chieffi N, Chen J, Ferrari M.Adhesion of two dual-cure core resins to silica fiber poststreated with different bonding agents. Int Dent SA Australas Ed2006;5:70e80.
38. Dimitrouli M, Gunay H, Geurtsen W, Luhrs A-K. Push-outstrength of fiber posts depending on the type of root canalfilling and resin cement. Clin Oral Invest 2010;15:273e81.
39. Dimitrouli M, Geurtsen W, Luhrs A-K. Comparison of thepush-out strength of two fiber post systems dependent ondifferent types of resin cements. Clin Oral Invest 2011;16:899e908.
40. Van Meerbeek B, De Munck J, Yoshida Y, et al. Buonocorememorial lecture. Adhesion to enamel and dentin: currentstatus and future challenges. Oper Dent 2003;28:215e35.





























