Embed Size (px)
Citation preview

Pulmonary Embolism and Infarction
Pulmonary Embolism
Falls under the spectrum of diagnosis called VTE
600,000 episodes occur yearly causing 200,000 deaths
Death is uncommon after proper dx and treatment is initiated
Majority of PE’s are from LE’s but only 30% have leg symptoms

Pathophysiology
Dislodged thrombi travel through Rt heart and lodge in pulmonary arterial circulation
Small emboli vs. large emboli

Risk Factors
Age (advanced) Cigarette smoking Extended travel history History of VTE** HTN HRT Immobilization** Recent joint
replacement
LE bone fx Malignancy** Obesity OCP’s Trauma Pregnancy Surgery w/in past 3
months** Stroke**

Risk Factors, cont.
Anticardiolipin syndrome Antithrombin III deficiency Factor V Leiden Lupus Anticoagulant Protein C or S deficiency Prothrombin G20210A mutation (Evaluation for above causes should be limited to pt’s with
recurrent or FHx of VTE)

Signs and Symptoms
Dyspnea (73%) Tachypnea (70%) Pleuritic Pain (66%) Rales (51%) Cough (37%) Tachycardia (30%) S4 (24%) Hemoptysis (13%)
Diagnosis
What do you order first?– CXR– EKG– ABG– Chem 7– CBC– Ddimer– Troponin– BNP
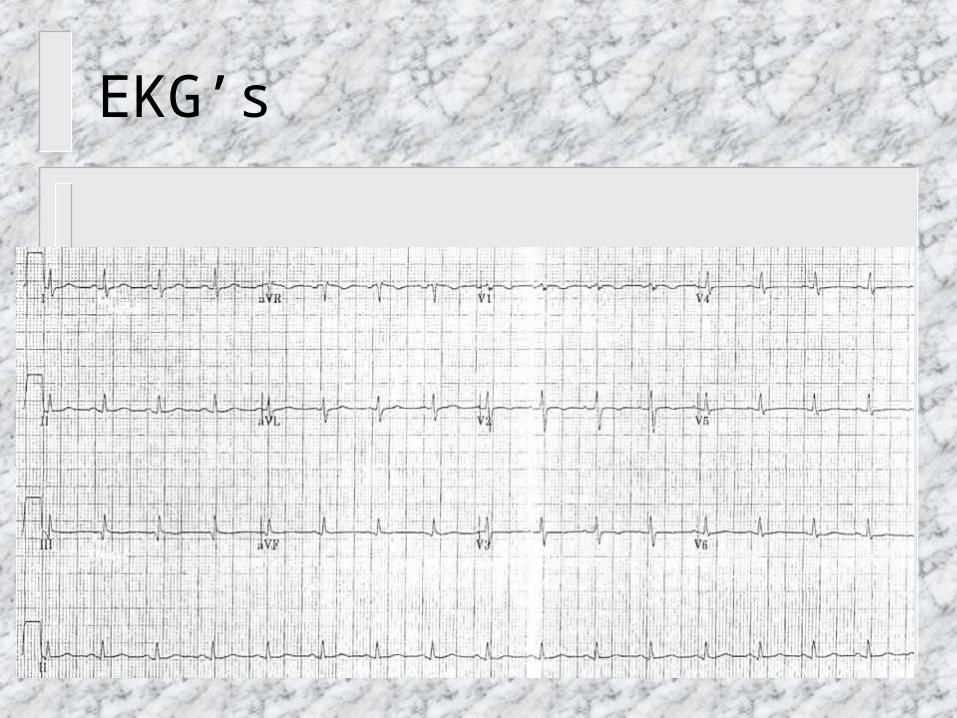
EKG’s
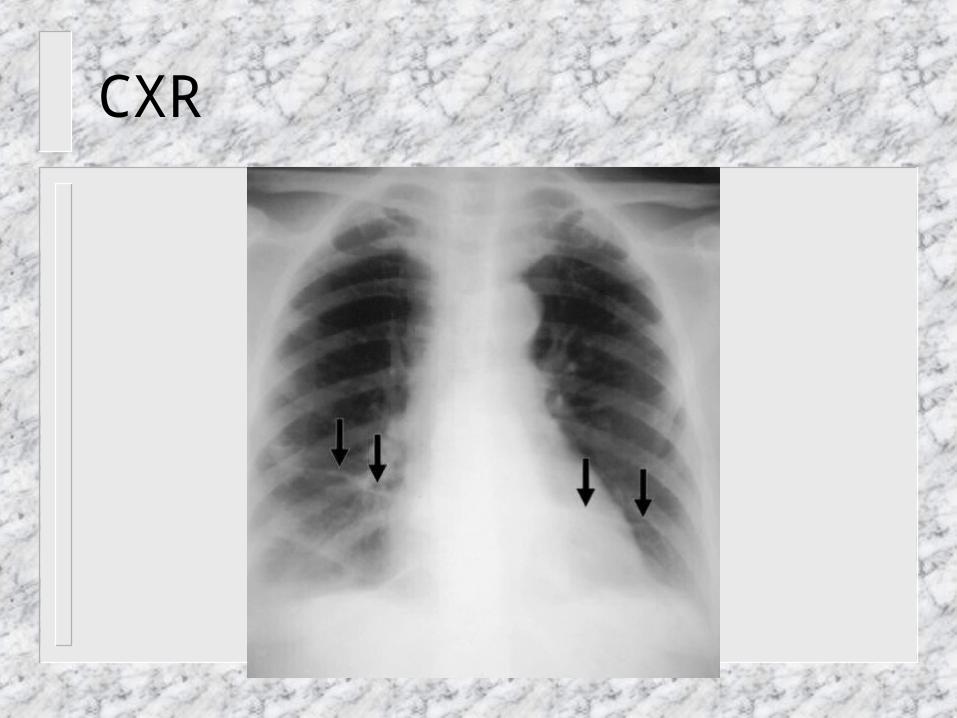
CXR

Definitive Imaging Studies
Pulmonary Angiography– Requires right heart catheterization and 4
injections of iodinated contrast– Associated with 5% morbidity and 0.5%
mortality rate– Reserved when other tests are all inconclusive


Figure 1.Massive pulmonary thromboembolism, seen at pulmonary angiography
in a patient with recent resection of colonic cancer, undergoing chemotherapy,
who had suddenly collapsed in the ward.
V/Q scans
97% specific when “high probability” 95% predictive value when high clinical
probability 14% false positive rate Normal perfusion scan excludes PE Intermediate requires further work-up

Normal perfusion images
Normal ventilation on the left with abnormal perfusion scan on the right

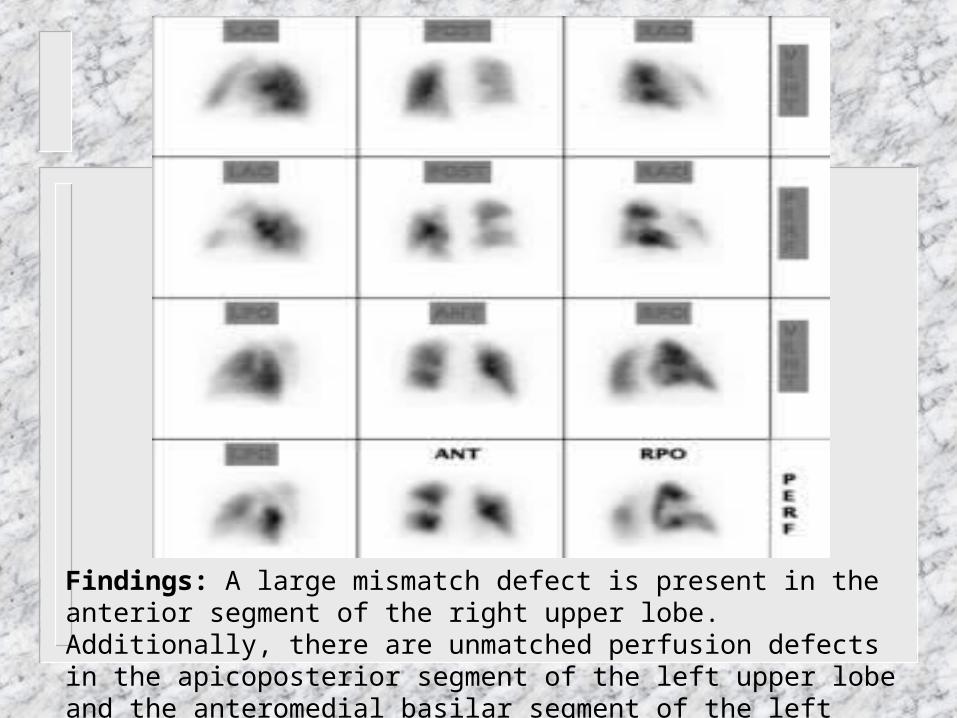
Findings: A large mismatch defect is present in the anterior segment of the right upper lobe. Additionally, there are unmatched perfusion defects in the apicoposterior segment of the left upper lobe and the anteromedial basilar segment of the left lower lobe.

Helical CT scan
CTPA (CT pulmonary angiography) is considered first line modality by some clinicians
Specificity (87-97%) Sensitivity (53-60%) Added benefit of suggesting alternative dx Neg result is insufficient to exclude PE in
mod to high risk patients (need to perform NIV of LE’s)


CT Pulmonary Angiography. Arrow points to thrombus in right upper lobe pulmonary artery.
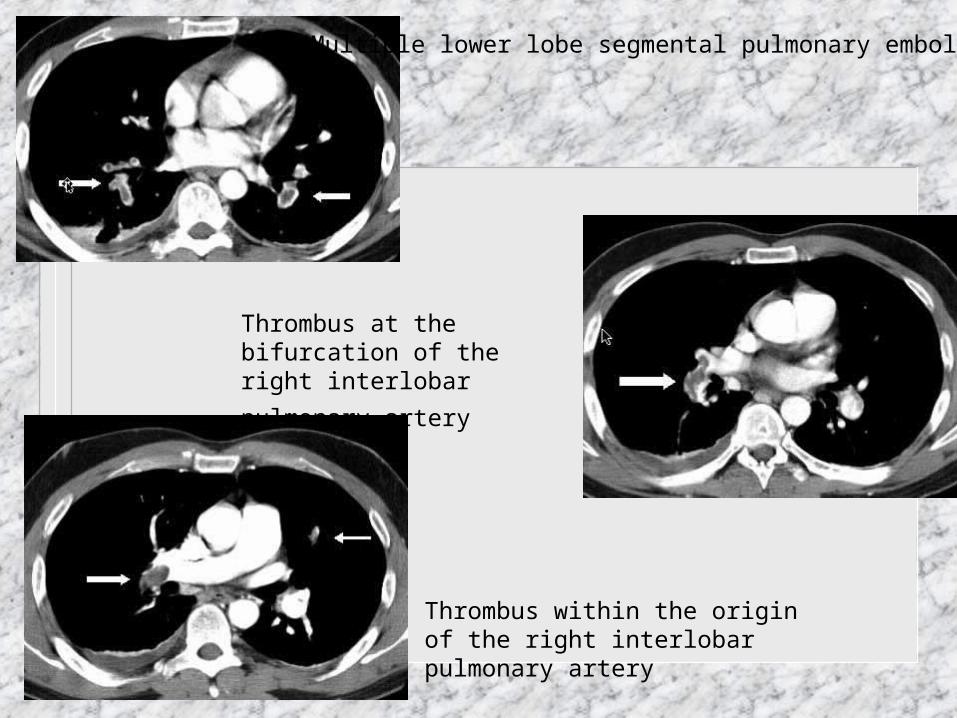
Thrombus within the origin of the right interlobar pulmonary artery
Multiple lower lobe segmental pulmonary emboli
Thrombus at the bifurcation of the
right interlobar pulmonary artery

Other Studies
Magnetic Resonance pulm angiography– minimal value in dx
LE evaluation– useful when clinical suspicion is high and V/Q
scan is unequivocal– ultrasound is 90% sensitive for DVT

Other Studies, cont.
Echocardiogram– used for risk stratification when pts are
hemodynamically unstable– Common findings include RV dysfunction, RV
dilation, and patent foramen ovale– McConnell Sign:
normal contraction of RV apex despite moderate to severe RV free wall hypokinesis
94% specific for PE

Treatment
Heparin Coumadin LMWH IVC filters

IVC or Greenfield filters
Heparin vs. LMWH
LMWH– developed in the 90’s– 1-2x daily, SQ– no monitoring needed– provides immediate anticoagulation– can be used in outpatients– 2004 American College of Chest Physicians:
LMWH has therapeutic equivalence to unfractionated heparin in proximal DVT’s and VTE

Coumadin
INR goal of 2-3 Duration is
controversial 2004 ACCP consensus
statement provides the guidelines for long-term treatment
ACCP guidelines
1. Pts with first epidode caused by reversible risk factor should have 3 months of warfarin treatment.
2. Pts with first episode of idiopathic PE should have 6-12 months of warfarin and be considered for indefinite therapy.
3. PE and cancer should have LMWH for 3-6 months and then warfarin indefinitely.
ACCP guidelines, cont.
4. Pts with first PE with antiphospholipid Ab’s or 2+ thrombophilic conditions should be treated for 12 months or indefinitely.
5. Two or more episodes of PE should be considered for indefinite treatment.
See www.chestjournal.org for full consensus guidelines.

Treatment, cont.
Thrombotic therapy– reserved for hemodynamically unstable patients– many contraindications
Pulmonary Embolectomy– unstable pts with contraindications to
thrombolysis– severe RV dysfunction– catheter based procedure