Embed Size (px)
Citation preview

Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies
C. Michael Gibson, M.S., M.D.Professor of Medicine
Harvard Medical School
There WILL be off-label and/or investigational discussion in this presentation.

Conflict of Interest StatementPresent Research/Grant Funding
Angel Medical Corporation Bayer Corp.CSL BehringGoogleIkaria, Inc.Janssen PharmaceuticalsJohnson & Johnson Corporation Portola PharmaceuticalsStealth Peptides, Inc.St. Jude Medical
Consultant(all with moderate support)
Boston Clinical Research InstituteCardiovascular Research FoundationCSL BehringGilead Sciences, Inc.The Medicines CompanyNovo NordiskPfizerSt. Jude MedicalWeb MD
Consultant (with $0.00 monies received by Dr. Gibson)
Bayer CorporationJanssen PharmaceuticalsJohnson & Johnson CorporationOrtho McNeil
Spouse: Employee of Boston Clinical Research Institute, she has equity position
2
There WILL be off-label and/or investigational discussion in this presentation.

Learning Objectives
• Describe the results of the landmark trials in extended duration anticoagulation.
• Describe the design and rationale of the APEX trial.
• Describe the risks and benefits of betrixaban based on clinical research.
3
There WILL be off-label and/or investigational discussion in this presentation.

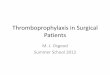
Previous Novel Oral Anticoagulant Trials of Extended Thromboprophylaxis in Acute Medically Ill Patients
5.7%
4.4%
Enoxaparin Rivaroxaban
3.1% 2.7%
Enoxaparin Apixaban
Inci
denc
e (%
) VTE
Even
ts
More M
ajor Bleeding
ADOPTEnoxaparin vs. Apixaban
MAGELLANEnoxaparin vs. Rivaroxaban
0.2% 0.5% 0.4%1.1%
p=0.44
p=0.04
p=0.02
p<0.001
ADOPT: Goldhaber SZ et al. N Engl J Med. 2011;365:2167-77MAGELLAN: Cohen AT et al. N Engl J Med. 2013;368:513-23
RRR=12.9%
RRR=22.8%
0
6
6
4
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this
presentation.

Betrixaban
• Oral factor Xa inhibitor• Renal clearance of administered dose (5%)• Renal clearance of absorbed dose (17%)• 1 day half-life (19-25 h)• Not a substrate for major CYP450 enzymes• Rapid onset Cmax achieved at 3-4 hours
• Safety and efficacy of 80 mg daily dose of Betrixaban previously described in approximately 1,200 patients in phase I and II studies
Connolly S et al. Eur Heart J 2013;34(20):1498-505Turpie A et al. Thromb Haemost 2009;101:68-76Cohen AT et al. Am Heart J 2014; 167:335-41
5
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

EvaluationExtended
Prophylaxis35 – 42 days
APEX Study DesignR
1:
1
Subj
ects
enr
olle
d(N
=7,5
13)
Enoxaparin40 mg Placebo
Betrixaban80 mg
Follow-up safety visit
30 Days After Visit 3
(+5 days)Betrixaban80 mg
Primary Efficacy Endpoint: Composite of asymptomatic proximal DVT (detected on ultrasound), symptomatic DVT (proximal or distal), non-fatal PE, and VTE-related death through Visit 3Primary Safety Endpoint: ISTH Major bleeding through 7 days after drug discontinuationNet Clinical Benefit: Composite of primary efficacy and primary safety endpoints
Dose adjustments in severe renal insufficiency (CrCl < 30 mL/min): Betrixaban 40 mg PO qd and Enoxaparin 20 mg SC qd
Standard Prophylaxis10 ± 4 days
Ultrasound & Visit 3
Day 35(+7 days)
Loading dose160 mg
6
Double blind, double dummy
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

Study Design: Key Inclusion Criteria
• Age/Risk Factors:− ≥ 75 yo OR− 60 - 74 yo with D-dimer ≥ 2x ULN OR− 40 - 59 yo with D-dimer ≥ 2x ULN and a history of either VTE, or
cancer*
• Anticipated to be severely immobilized for at least 24 hours after randomization with anticipated length of hospitalization ≥ 3 days
• Hospitalized for one of the following acute presentation:− Acute on chronic heart failure decompensation− Acute on chronic respiratory failure− Acute infection without septic shock− Acute rheumatic disorders− Acute ischemic stroke (w/ immobilization)
*Pre-amendment 3, other risk factors were allowed including: previous history of superficial VT, obesity, varicose veins of lower extremities, hormone therapy, thrombophilia, concomitant use of erythropoiesis stimulating agents
7
Gibson et. al. ISTH SSC 2016 – May 27, 2016
There WILL be off-label and/or investigational discussion in this presentation.

Study Design: Key Exclusion Criteria
• End stage renal disease with CrCl <15 mL/min, or requiring dialysis (first trial to enroll patients with CrCl <30 mL/min)
• Anticipated need for prolonged anticoagulation
• Current intake of dual antiplatelet therapy
• Anticipated major surgery
• History of clinically significant bleeding within 6 months prior to enrollment
• History of IC bleeding, head trauma, or known intracranial lesions
• History of significant GI, pulmonary or GU bleeding, ongoing chronic PUD or ongoing or acute gastritis within 2 years prior to enrollment
• Hgb < 10 g/dL (pre-amendment 3); Hgb < 9.5 g/dL or unstable/declining hemoglobin (possible active bleed) (post-amendment 3)
8
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

CONSORT Diagram
Randomized(n=7,513)
n=3,759
n=2,842
n=3,754
n=3,720
n=1,956
Enoxaparin Betrixaban
Did not receive any dose of study drug
n=34 n=38
n=2,893
n=1,914
n=3,721No ultrasound AND no symptomatic event
n=546 n=609
n=3,174 n=3,112
Cohort 1
Cohort 2
Cohort 1
Cohort 2
Cohort 3:Overall
efficacy population
Cohort 3:Overall efficacy population
mITTpopulation
mITTpopulation
9
Cohen et al. N Engl J Med. 2016; 375(6):534-44. There WILL be off-label and/or investigational discussion in this presentation.

0
2
4
6
8
10
Enoxaparin(N=2,313)
Betrixaban(N=2,314)
Enoxaparin(N=3,391)
Betrixaban(N=3,407)
Enoxaparin(N=3,720)
Betrixaban(3,721)
mITT Efficacy Analysis Including All Patients Who Received Study Drug Including Those
with Missing Ultrasound As Included in US FDA LabelEv
ent r
ate
(%)
Cohort 1D-dimer ≥ 2 x ULN
Cohort 2D-dimer ≥ 2 x ULN
or age ≥ 75 y
Cohort 3Overall efficacy
population
7.18%
5.70%6.02%
4.70%
5.99%
4.43%
P = 0.018RRR = 21.6%
P = 0.003RRR = 25.4%
P = 0.038RRR = 20.9%
n=166 n=132 n=204 n=160 n=223 n=165
P-values reported using the Mantel-Haenszel test stratified for dosing criteria in Cohort 1 and dosing and entry criteria in Cohort 2 and mITT. mITT defined as patients who received at least one dose of study drug. Symptomatic events from Day 1 till Day 42 or the date of Visit 3, if Visit 3 occurred before Day 42; Asymptomatic DVT between Day 32 and 47.
10
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

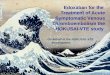
Subgroup Analysis: Primary EfficacyOverall Efficacy Population (Cohort 3)
Age ≥ 75 years Age < 75 years
≥ 2 VTE risk factors< 2 VTE risk factors
No dosing modificationP-gp inhibitorSevere renal insufficiency
MaleFemale
Acute decompensated HFAcute infection Acute respiratory failure Acute ischemic stroke Acute rheumatic disorders
Composite of Asymptomatic Proximal DVT, Symptomatic
Proximal or Distal DVT, Nonfatal PE, or VTE-related Death
Reason for Hospital Admission
Dosing Criteria
Additional VTE Risk Factors
Gender
Age
OverallRR (95% CI)
0.76 (0.63, 0.92)
0.75 (0.60, 0.95) 0.77 (0.54, 1.09)
0.82 (0.62, 1.09) 0.70 (0.54, 0.92)
0.68 (0.51, 0.89) 0.84 (0.64, 1.10)
1.06 (0.67, 1.70) 0.88 (0.40, 1.94)
0.70 (0.56, 0.87)
0.85 (0.62, 1.16) 0.72 (0.50, 1.02)0.89 (0.53, 1.49) 0.58 (0.34, 1.02) 0.63 (0.22, 1.78)
Event Rate(Enoxaparin)
Event Rate(Betrixaban)
223 / 3174 165 / 3112
152 / 2136 115 / 213871 / 1038 50 / 974
102 / 1447121 / 1727
81 / 140684 / 1706
114 / 1253109 / 1921
77 / 125288 / 1860
180 / 251133 / 553
120 / 242633 / 540
10 / 110 12 / 146
83 / 148169 / 854
69 / 142849 / 883
29 / 375 24 / 35333 / 363 18 / 3539 / 101 5 / 94
Favors EnoxaparinFavors Betrixaban10.80.60.40.20.1 2 3 4 65
P-value for interaction is non-significant for all analyses.All analysis were stratified for dosing and entry criteria.
11
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

Prob
abilit
y of
Sym
ptom
atic
Eve
nt (%
)
Time (Days)
Enoxaparin
Betrixaban
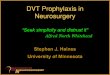
1.44%
0.93%
Through Visit 3HR = 0.65 (0.42, 0.99)ARR = 0.51%NNT = 196
p=0.043
Through End of Trial*HR = 0.56 (0.38, 0.84)ARR = 0.80%NNT = 125
p=0.004
1.84%
1.04%
Parenteral Therapy
Visi
t 3
Symptomatic VTEAll Patients Randomized
Composite of Symptomatic Proximal or Distal DVT, Non-Fatal PE, or VTE-related Death
*End of Trial defined as final follow-up visit (30 + 5 days after Visit 3)
12
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

13
Stroke Type Enoxaparin(N=3716)
Betrixaban(N=3716)
Relative Risk (95% CI) p-value
All-cause stroke 0.97% (36) 0.54% (20) 0.56 (0.32, 0.96) 0.032
Ischemic 0.91% (34) 0.48% (18) 0.53 (0.30, 0.94) 0.026
Hemorrhagic 0.03% (1) 0.03% (1) 1.00 (0.06, 15.98) 1.00
Uncertain type 0.03% (1) 0.03% (1) 1.00 (0.06, 15.98) 1.00
TIA 0.13% (5) 0.11% (4) 0.80 (0.22, 2.98) 0.74
All-cause stroke or TIA 1.10% (41) 0.65% (24) 0.59 (0.35, 0.97) 0.034
Stroke or TIAModified Intent-to-Treat Population
Gibson et al. Circulation. 2017;135(7):648-55There WILL be off-label and/or investigational discussion in this presentation.

14Stroke or TIAModified Intent-to-Treat Population – Received 80 mg
Gibson et al. Circulation. 2017;135(7):648-55
Stroke Type Enoxaparin(N=2991)
Betrixaban(N=2986)
Relative Risk(95% CI) p-value
All-cause stroke 30 (1.00%) 14 (0.47%) 0.47 (0.25, 0.88) 0.016
Ischemic 28 (0.94%) 13 (0.44%) 0.47 (0.24, 0.90) 0.019
Hemorrhagic 1 (0.03%) 0 (0.00%) – 0.32
Uncertain type 1 (0.03%) 1 (0.03%) 1.00 (0.06, 16.01) 1.00
TIA 5 (0.17%) 3 (0.10%) 0.60 (0.14, 2.51) 0.48
All-cause stroke or TIA 35 (1.17%) 17 (0.57%) 0.49 (0.27, 0.87) 0.012
There WILL be off-label and/or investigational discussion in this presentation.

15Time to Ischemic Stroke Among Subjects with CHF or Ischemic Stroke at Entry
Modified Intent-to-Treat Population
Gibson et al. Circulation. 2017;135(7):648-55There WILL be off-label and/or investigational discussion in this presentation.

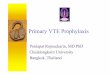
Primary Safety Endpoint: ISTH Major BleedingSafety Population
Major bleeding events (ISTH) through 7 days after drug discontinuation
0.0
0.2
0.4
0.6
0.8
1.0
Enoxaparin (N=3,716) Betrixaban (N=3,716)
Even
t rat
e (%
)
n=21
0.57%0.67%
p = 0.55
n=25
Safety population defined as patients who received at least one dose of active study drug. Analysis by actual treatment. NNH not reported given p=NS.
16
Cohen et al. N Engl J Med. 2016; 375(6):534-44. There WILL be off-label and/or investigational discussion in this presentation.

Secondary Safety EndpointSafety Population
Major or clinically relevant non-major bleeding events (ISTH) through 7 days after drug discontinuation
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Enoxaparin (N=3,716) Betrixaban (N=3,716)
Even
t rat
e (%
)
n=59
1.59%
3.12%
p < 0.001
n=116
Safety population defined as patients who received at least one dose of active study drug. Analysis by actual treatment.
17
Cohen et al. N Engl J Med. 2016; 375(6):534-44. There WILL be off-label and/or investigational discussion in this presentation.

Fatal Bleeding and ICHSafety Population
n=9
Even
t rat
e (%
)
0
0.05
0.1
0.15
0.2
0.25
Enoxaparin(N=3,716)
0.03% 0.03%
0.19%
0.05%
n=7 n=2
p = 0.18
n=1 n=1Betrixaban(N=3,716)
Enoxaparin(N=3,716)
Betrixaban(N=3,716)
Fatal Bleeding ICHSafety population defined as patients who received at least one dose of active study drug. Analysis by actual treatment.
18
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

Unger et al of FDA suggests that net clinical outcome analyses include events that are clinically meaningful and are of similar clinical significance such as fatal or irreversible events.
Benefit = Non-hemorrhage CV death + Non-fatal PE + MI + ischemic stroke
Harm = Fatal Bleeding + ICH
19
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

Fatal or Irreversible OutcomesAll Patients Randomized
Non-hemorrhage cardiopulmonary death + Non-fatal PE + MI + ischemic stroke + Fatal bleeding + ICH
20
*End of Trial defined as final follow-up visit (30 + 5 days after Visit 3) Gibson et al. J Am Heart Assoc. 2017;6(7)
Through Visit 3HR = 0.71 (95% CI: 0.55-0.90)ARR = 1.18%NNT = 85
Through End of Trial*HR = 0.70 (95% CI: 0.57-0.88)ARR = 1.53%NNT = 65
There WILL be off-label and/or investigational discussion in this presentation.

Fatal or Irreversible OutcomesAll Patients Randomized – Received 80 mg
Non-hemorrhage cardiopulmonary death + Non-fatal PE + MI + ischemic stroke + Fatal bleeding + ICH
21
*End of Trial defined as final follow-up visit (30 + 5 days after Visit 3) Gibson et al. J Am Heart Assoc. 2017;6(7)
Through Visit 3HR = 0.62 (95% CI: 0.47-0.83)ARR = 1.47%NNT = 68
Through End of Trial*HR = 0.64 (95% CI: 0.50-0.83)ARR = 1.77%NNT = 56
There WILL be off-label and/or investigational discussion in this presentation.

RRR = 29.0% (8.0, 46.0)p<0.001
9.30%
6.50% p=
HR = (95% CI)
n= n=
%
%
0%
2%
4%
6%
8%
10%
Enoxaparin(n=1,822)
Betrixaban(n=1,838)
9.0%
6.4%
MAGELLAN
Primary Efficacy Endpoint Central D-dimer ≥ 2 x ULN: MAGELLAN vs. APEX
APEXRRR = 29.5% (11.6, 43.9)
p=0.002
MAGELLAN and APEX analyses through 35 days Cohen A et al. J Throm Haemost. 2014;12:479-87
0%
2%
4%
6%
8%
10%
Enoxaparin(n=1,348)
Rivaroxaban(n=1,285)
9.3%
6.5%
n=125 n=84 n=165 n=118
22
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

Comparison to Previous Novel Oral Anticoagulant Trials of Extended Thromboprophylaxis in Acute Medically Ill Patients
p<0.001
3.1%2.7%
5.7%
4.4%
7.03%
5.3%
0.2% 0.5% 0.4%1.1%
0.57% 0.67%
Inci
denc
e (%
)
VTE
Even
ts
Major Bleeding
ADOPTApixaban
MAGELLANRivaroxaban
APEXBetrixaban
Enoxaparin Apixaban Enoxaparin Rivaroxaban Enoxaparin Betrixaban
p=0.04 p<0.001 p=0.55
p = 0.44
p = 0.02
p* = 0.006
* Overall efficacy population analysis used for comparison purposes
RRR = 12.9%
RRR = 22.8%
RRR* = 24.0%
0
8
2
4
23
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.

Summary
• In an mITT analysis that includes all patients treated with study drug performed by the FDA in the label and pre-specified in the protocol, Betrixaban reduced the composite endpoint of symptomatic and asymptomatic events as well as symptomatic events
• Betrixaban was not associated with a significant increase in major, ICH, or fatal bleeding but was associated with more CRNM bleeding
• Betrixaban reduced stroke
• Betrixaban reduced fatal or irreversible events
24
Gibson et. al. ISTH SSC 2016 – May 27, 2016There WILL be off-label and/or investigational discussion in this presentation.