Embed Size (px)
Citation preview
PULMONARY EMBOLISM/VTE CARE PROCESS MODELIMCP FALL CONFERENCE 2017
Scott Stevens, MD
Co-Director, Thrombosis Clinic & Thrombosis Research Group
Intermountain Medical CenterProfessor of Clinical Medicine
The University of Utah School of Medicine
• VTE is COMMON
Why a VTE Care Process Model?
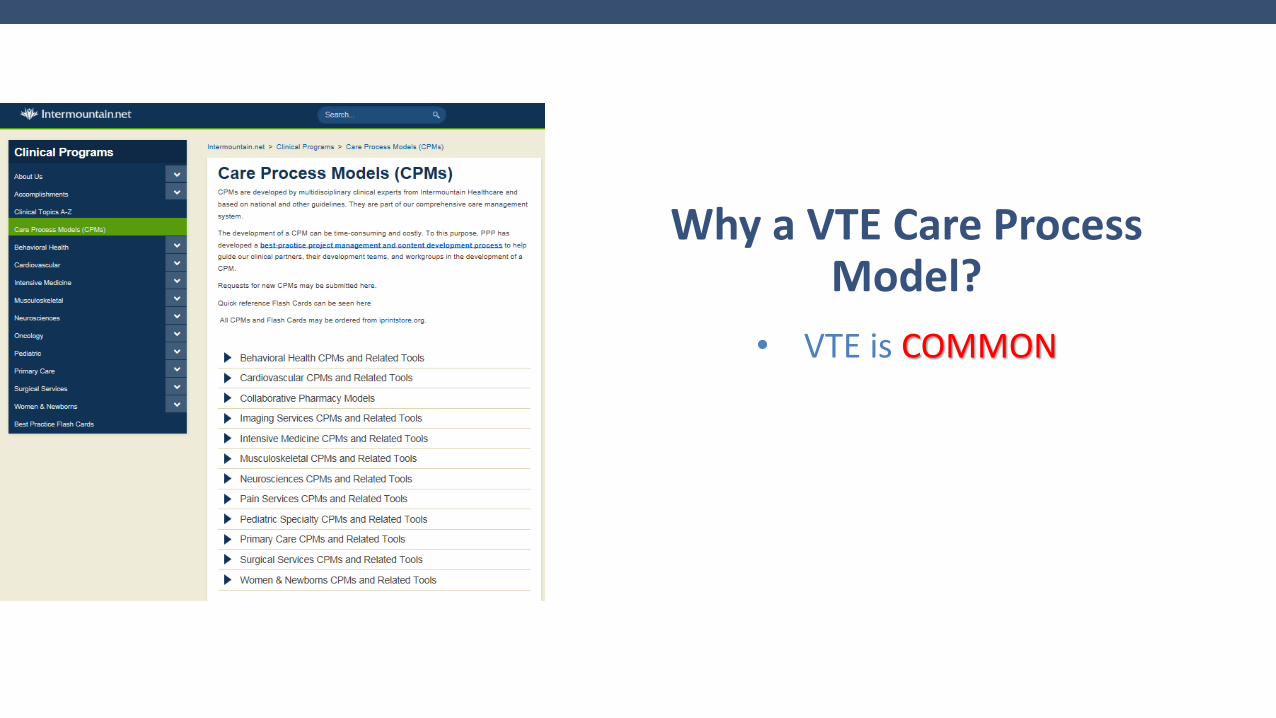
The Scope of the Problem
2006 2050
Fatal PE
N= 30,000
PE
N= 300,000
VTE
N= 950,000
Fatal PE
N= 60,000
PE
N= 600,000
VTE
N= 1,820,000
Arterioscler Thromb Vasc Biol. 2008 March ; 28(3): 370–372. Am J Hematol 2011;86:217-20
• VTE is CHALLENGING TO DIAGNOSE
Why a VTE Care Process Model?
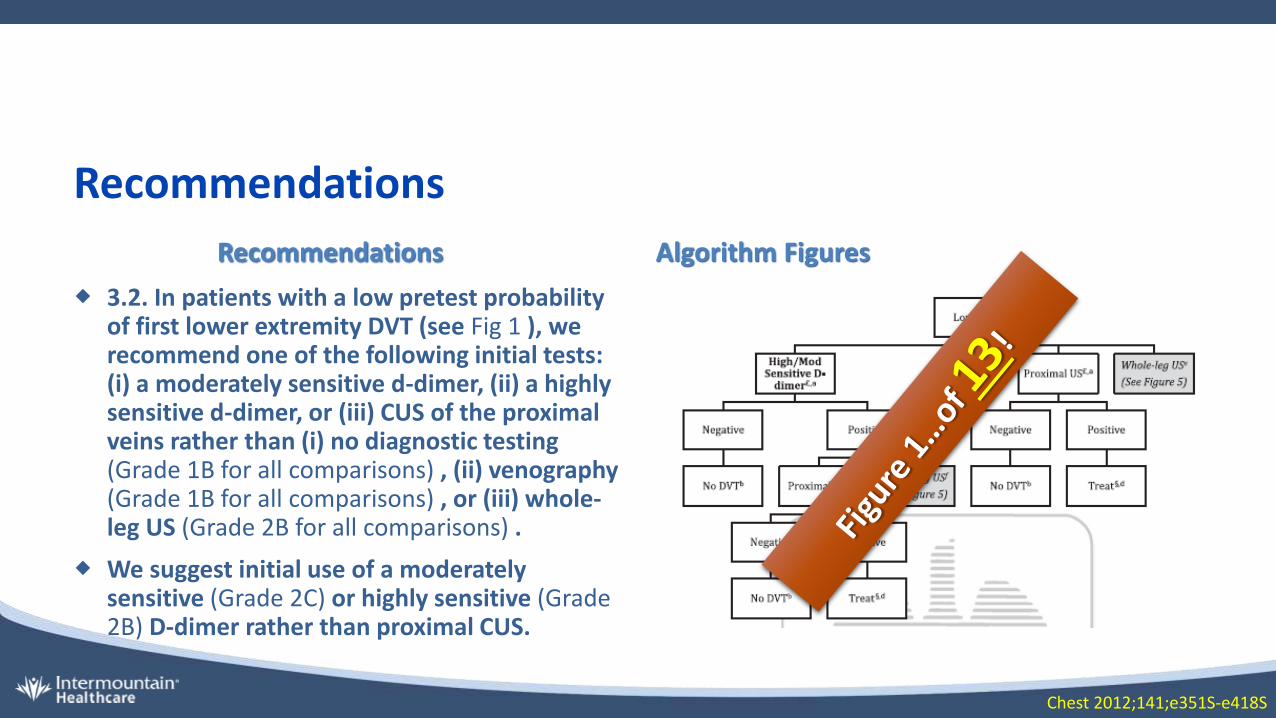
Recommendations
Recommendations Algorithm Figures
3.2. In patients with a low pretest probability of first lower extremity DVT (see Fig 1 ), we recommend one of the following initial tests: (i) a moderately sensitive d-dimer, (ii) a highly sensitive d-dimer, or (iii) CUS of the proximal veins rather than (i) no diagnostic testing (Grade 1B for all comparisons) , (ii) venography (Grade 1B for all comparisons) , or (iii) whole-leg US (Grade 2B for all comparisons) .
We suggest initial use of a moderately sensitive (Grade 2C) or highly sensitive (Grade 2B) D-dimer rather than proximal CUS.
Chest 2012;141;e351S-e418S
• IMAGING for VTE is OVERUTILIZED
Why a VTE Care Process Model?
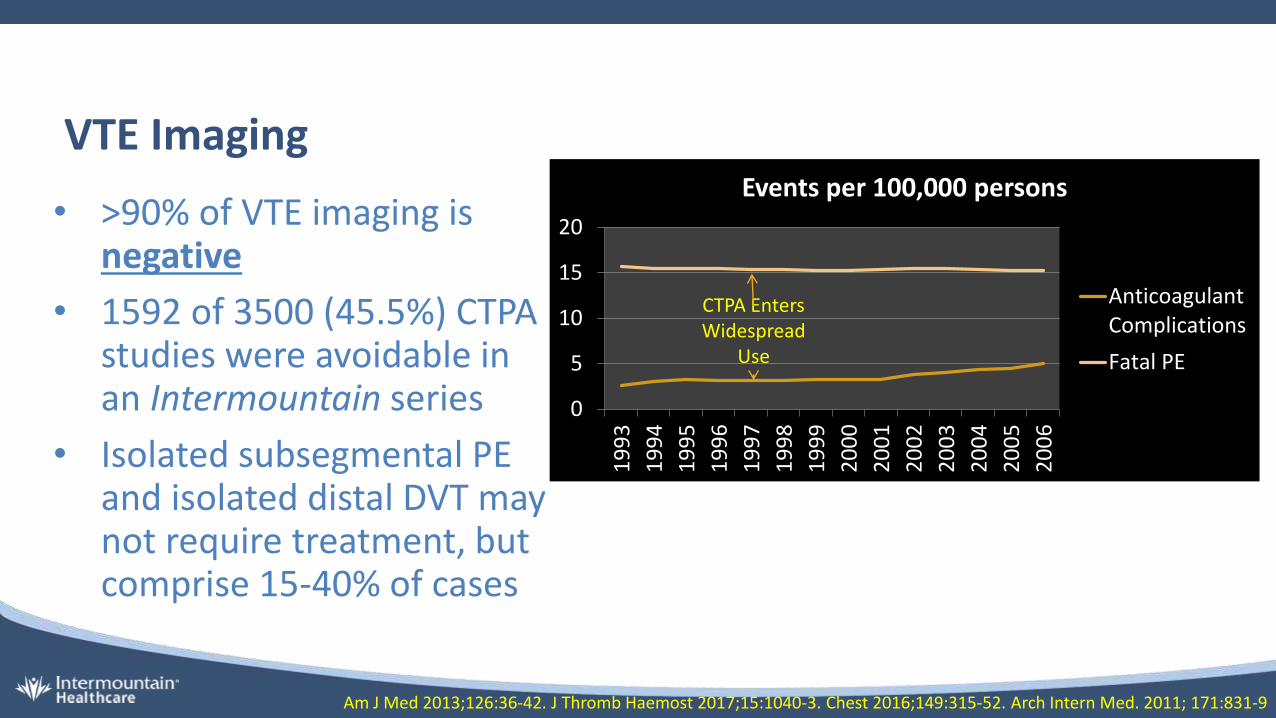
VTE Imaging
• >90% of VTE imaging is negative
• 1592 of 3500 (45.5%) CTPA studies were avoidable in an Intermountain series
• Isolated subsegmental PE and isolated distal DVT may not require treatment, but comprise 15-40% of cases
Am J Med 2013;126:36-42. J Thromb Haemost 2017;15:1040-3. Chest 2016;149:315-52. Arch Intern Med. 2011; 171:831-9
0
5
10
15
20
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
Events per 100,000 persons
AnticoagulantComplications
Fatal PE
CTPA Enters Widespread
Use
• VTE has MANY THERAPEUTIC CHOICES
Why a VTE Care Process Model?
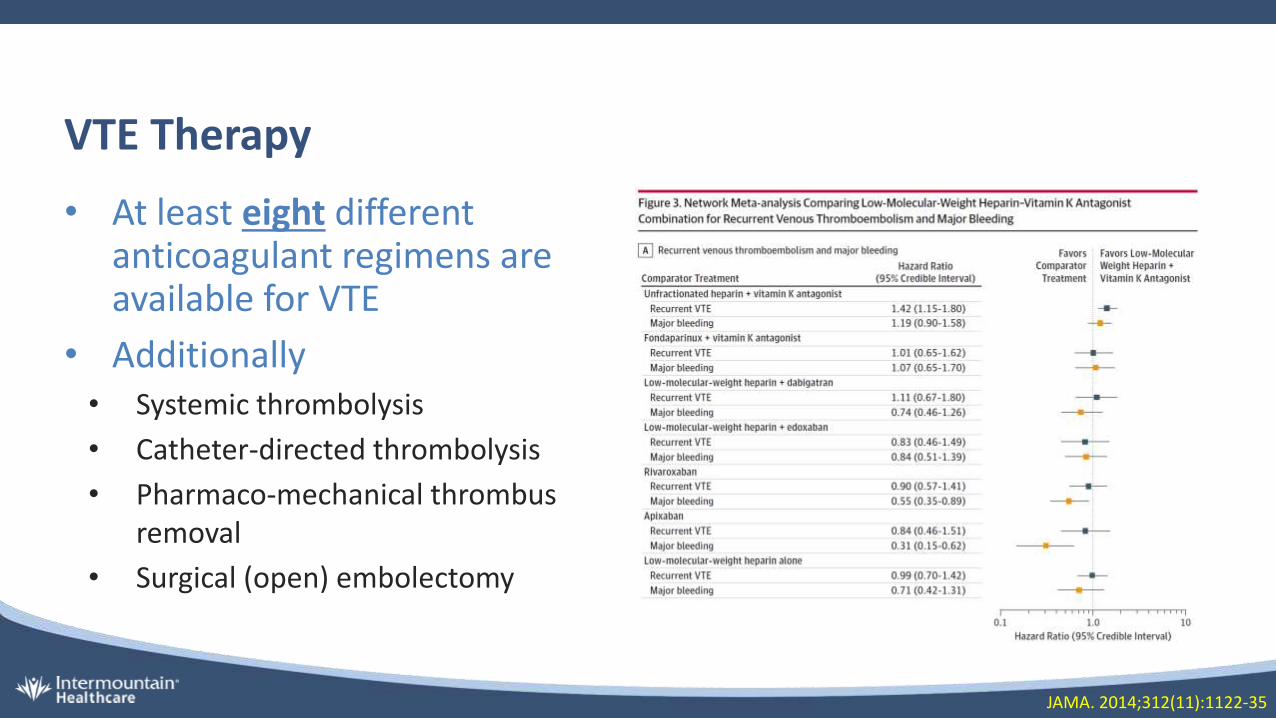
VTE Therapy
• At least eight different anticoagulant regimens are available for VTE
• Additionally• Systemic thrombolysis
• Catheter-directed thrombolysis
• Pharmaco-mechanical thrombus removal
• Surgical (open) embolectomy
JAMA. 2014;312(11):1122-35
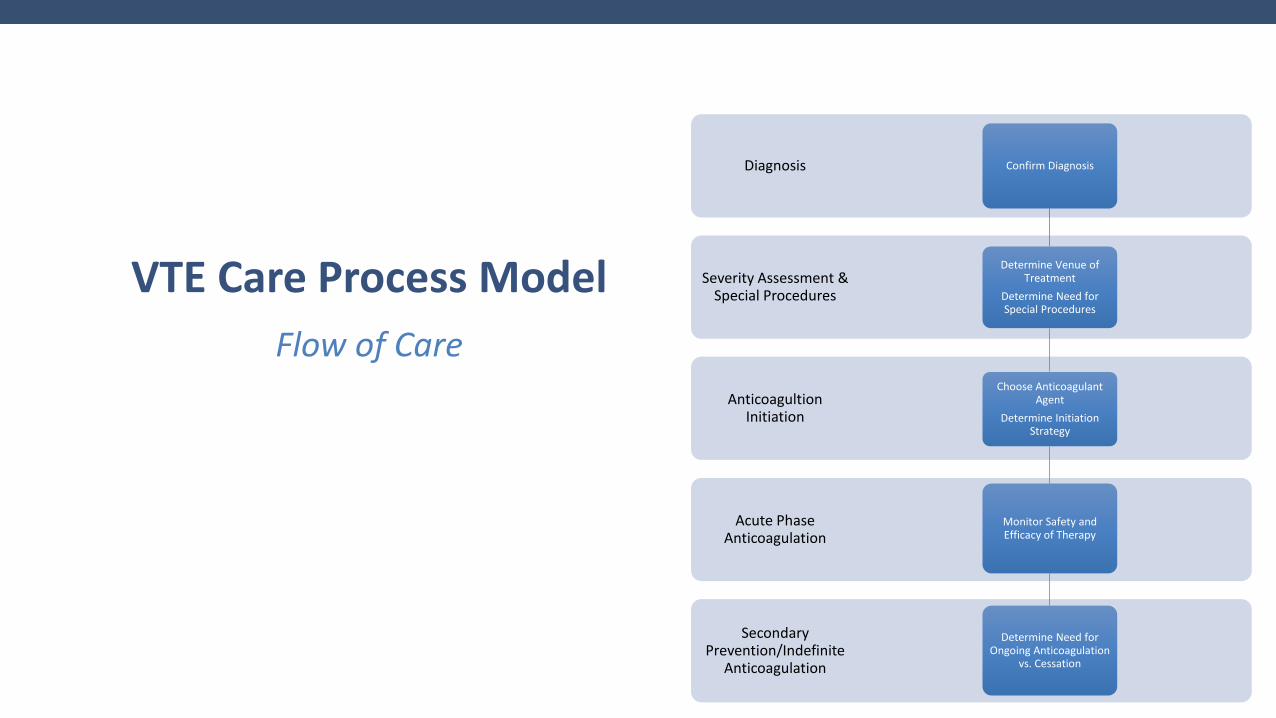
VTE Care Process Model
Flow of Care
Secondary Prevention/Indefinite
Anticoagulation
Acute Phase Anticoagulation
Anticoagultion Initiation
Severity Assessment & Special Procedures
Diagnosis Confirm Diagnosis
Determine Venue of Treatment
Determine Need for Special Procedures
Choose Anticoagulant Agent
Determine Initiation Strategy
Monitor Safety and Efficacy of Therapy
Determine Need for Ongoing Anticoagulation
vs. Cessation
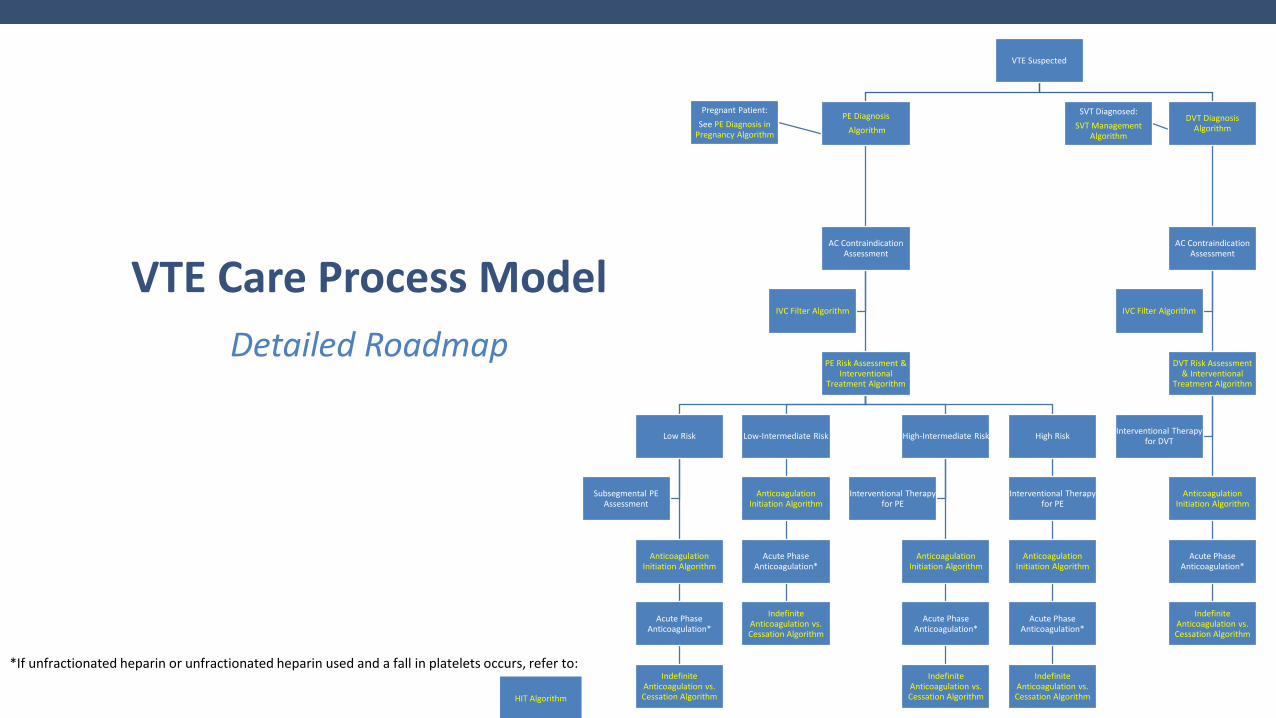
VTE Care Process Model
Detailed Roadmap
VTE Suspected
PE Diagnosis
Algorithm
AC ContraindicationAssessment
PE Risk Assessment & Interventional
Treatment Algorithm
Low Risk
Anticoagulation Initiation Algorithm
Acute Phase Anticoagulation*
Indefinite Anticoagulation vs. Cessation Algorithm
Subsegmental PE Assessment
Low-Intermediate Risk
Anticoagulation Initiation Algorithm
Acute Phase Anticoagulation*
Indefinite Anticoagulation vs. Cessation Algorithm
High-Intermediate Risk
Anticoagulation Initiation Algorithm
Acute Phase Anticoagulation*
Indefinite Anticoagulation vs. Cessation Algorithm
Interventional Therapy for PE
High Risk
Interventional Therapy for PE
Anticoagulation Initiation Algorithm
Acute Phase Anticoagulation*
Indefinite Anticoagulation vs. Cessation Algorithm
IVC Filter Algorithm
Pregnant Patient:
See PE Diagnosis in Pregnancy Algorithm
DVT Diagnosis Algorithm
AC Contraindication Assessment
DVT Risk Assessment & Interventional
Treatment Algorithm
Anticoagulation Initiation Algorithm
Acute Phase Anticoagulation*
Indefinite Anticoagulation vs. Cessation Algorithm
Interventional Therapy for DVT
IVC Filter Algorithm
SVT Diagnosed:
SVT Management Algorithm
*If unfractionated heparin or unfractionated heparin used and a fall in platelets occurs, refer to:
HIT Algorithm
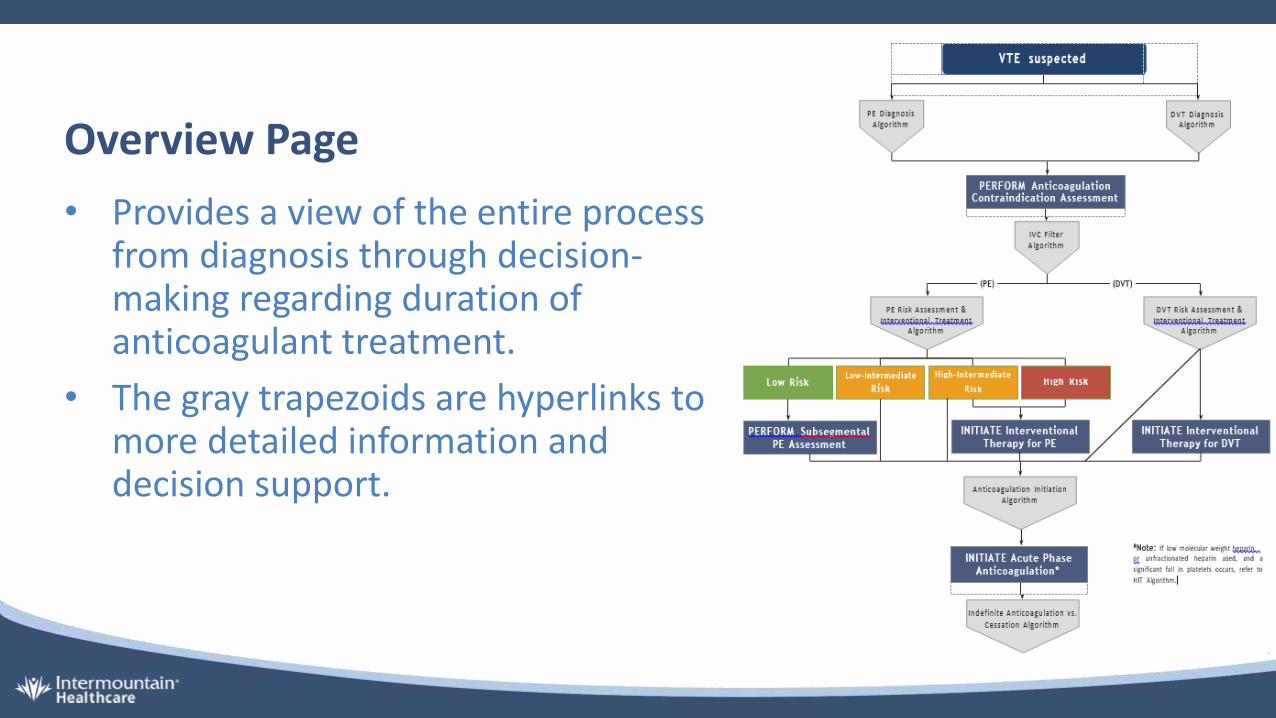
Overview Page
• Provides a view of the entire process from diagnosis through decision-making regarding duration of anticoagulant treatment.
• The gray trapezoids are hyperlinks to more detailed information and decision support.

Highlights
Diagnosis
VTE: The Early Diagnostic Toolkit
Pre 1960’s
1980’s
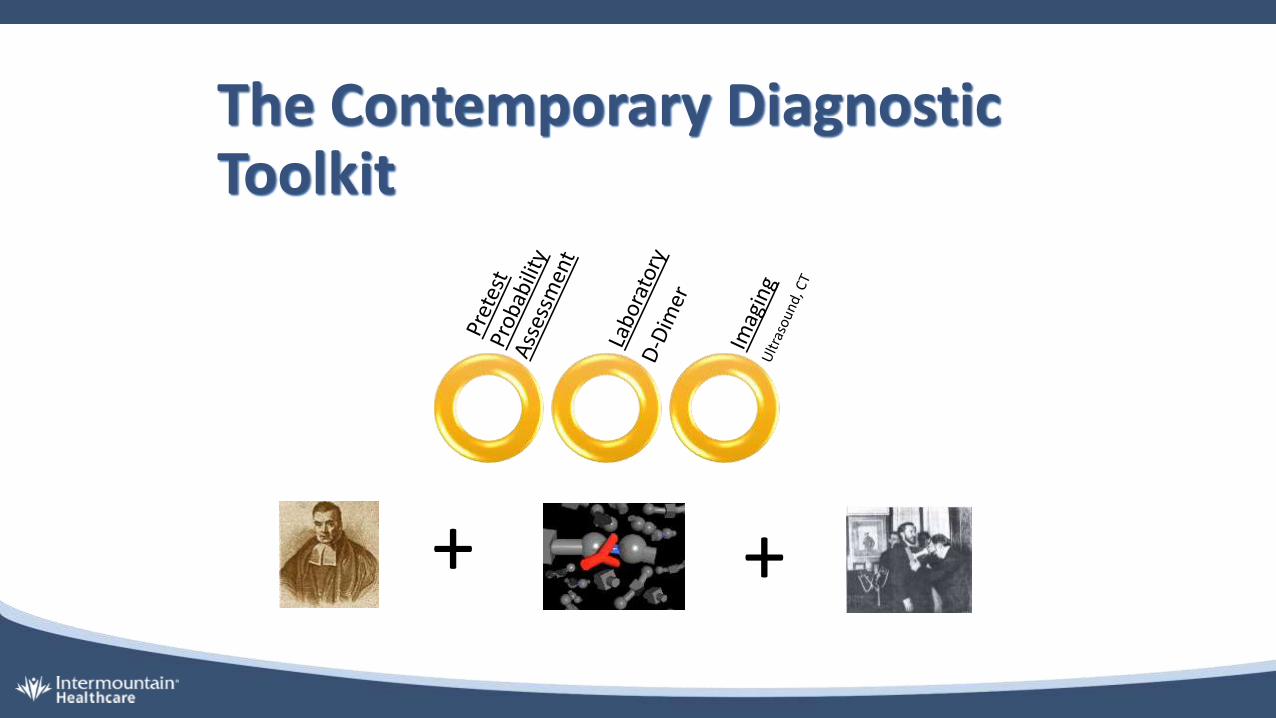
+ +
The Contemporary Diagnostic Toolkit
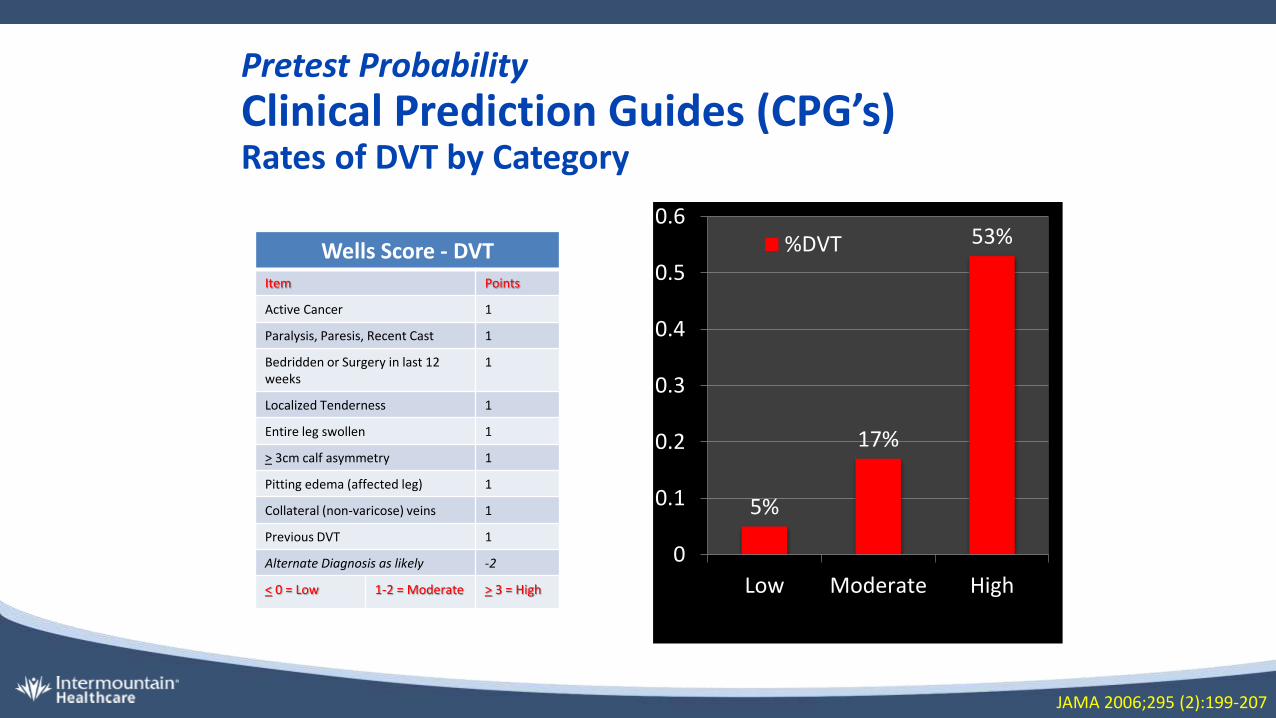
Pretest Probability
Clinical Prediction Guides (CPG’s)Rates of DVT by Category
5%
17%
53%
0
0.1
0.2
0.3
0.4
0.5
0.6
Low Moderate High
%DVT
JAMA 2006;295 (2):199-207
Wells Score - DVTItem Points
Active Cancer 1
Paralysis, Paresis, Recent Cast 1
Bedridden or Surgery in last 12 weeks
1
Localized Tenderness 1
Entire leg swollen 1
> 3cm calf asymmetry 1
Pitting edema (affected leg) 1
Collateral (non-varicose) veins 1
Previous DVT 1
Alternate Diagnosis as likely -2
< 0 = Low 1-2 = Moderate > 3 = High
Thromb Haemost 2000; 83: 416–20. Ann Intern Med 2006; 349: 144-165
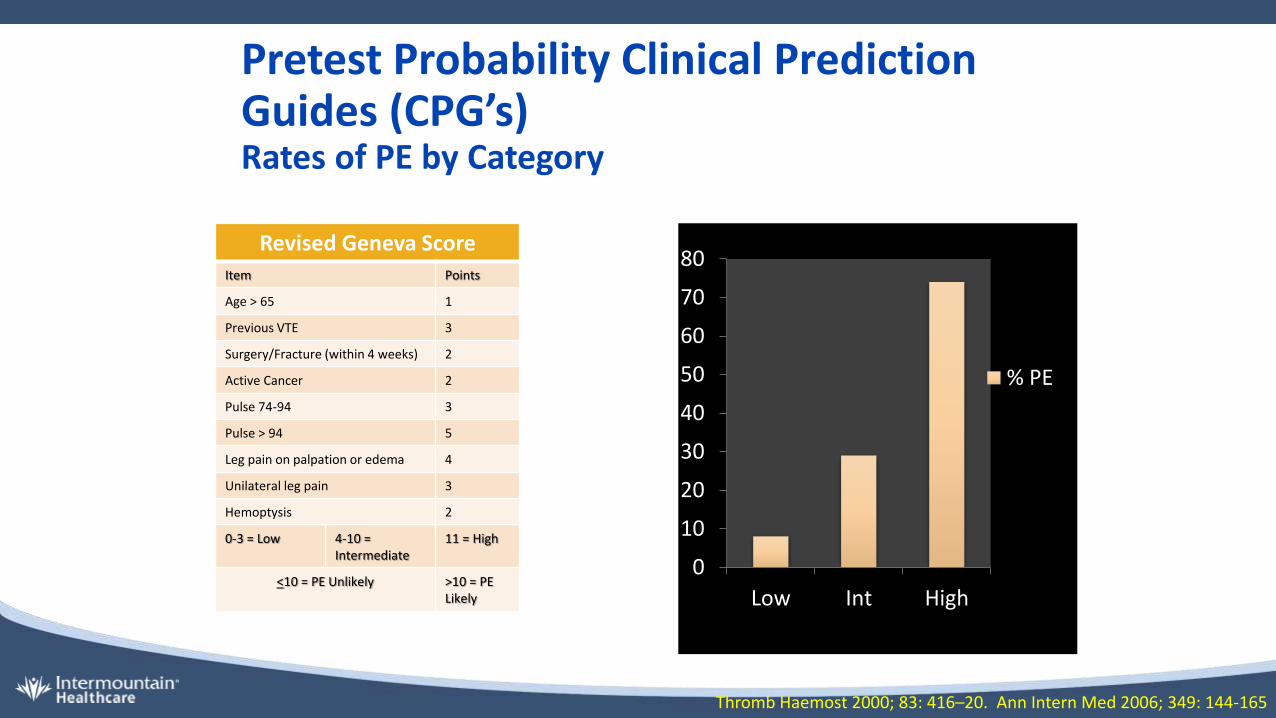
Revised Geneva ScoreItem Points
Age > 65 1
Previous VTE 3
Surgery/Fracture (within 4 weeks) 2
Active Cancer 2
Pulse 74-94 3
Pulse > 94 5
Leg pain on palpation or edema 4
Unilateral leg pain 3
Hemoptysis 2
0-3 = Low 4-10 = Intermediate
11 = High
<10 = PE Unlikely >10 = PE Likely
0
10
20
30
40
50
60
70
80
Low Int High
% PE
Pretest Probability Clinical Prediction Guides (CPG’s)Rates of PE by Category
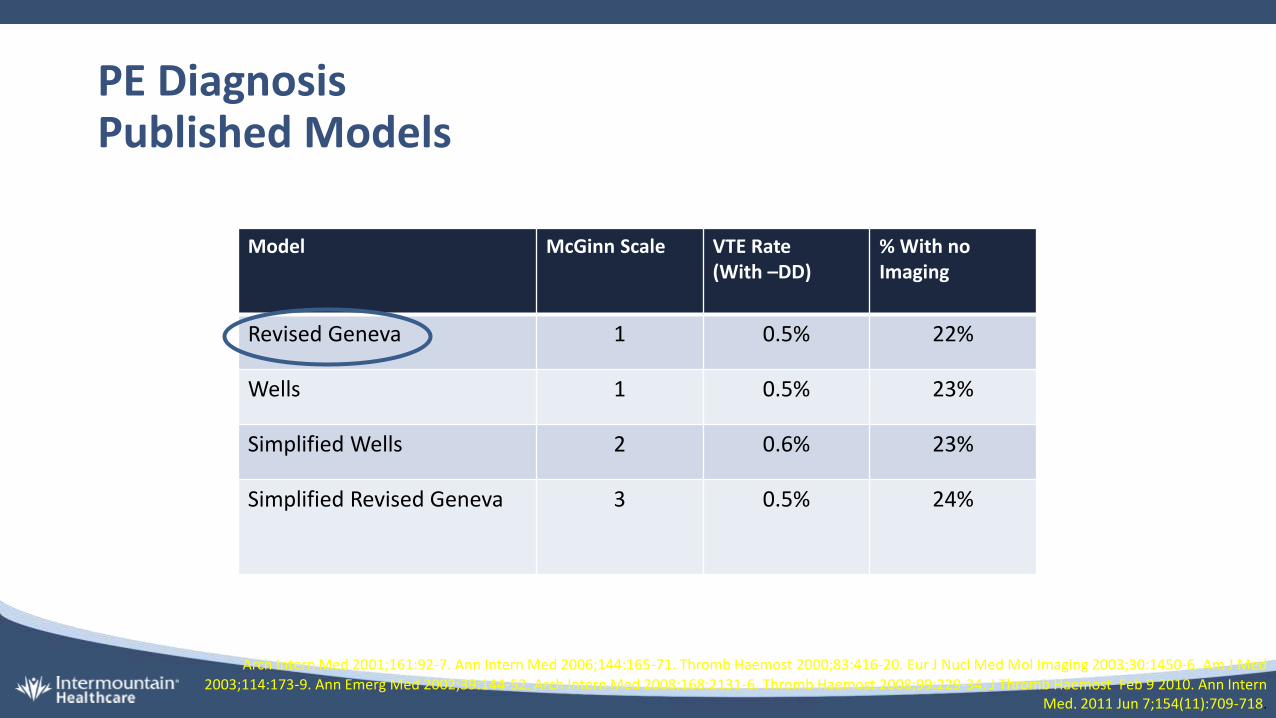
PE DiagnosisPublished Models
Model McGinn Scale VTE Rate(With –DD)
% With no Imaging
Revised Geneva 1 0.5% 22%
Wells 1 0.5% 23%
Simplified Wells 2 0.6% 23%
Simplified Revised Geneva 3 0.5% 24%
Arch Intern Med 2001;161:92-7. Ann Intern Med 2006;144:165-71. Thromb Haemost 2000;83:416-20. Eur J Nucl Med Mol Imaging 2003;30:1450-6. Am J Med 2003;114:173-9. Ann Emerg Med 2002;39:144-52. Arch Intern Med 2008;168:2131-6. Thromb Haemost 2008;99:229-34. J Thromb Haemost Feb 9 2010. Ann Intern
Med. 2011 Jun 7;154(11):709-718.
Laboratory
Highly Sensitive• Sensitivity 93-95%
• ELISAs, quantitative latex or immunoturbidimetric
Moderately Sensitive• Sensitivity 85%
• Whole blood assay
Di Nisio et al. J Thromb Haemost 2007;5 (2):296-304
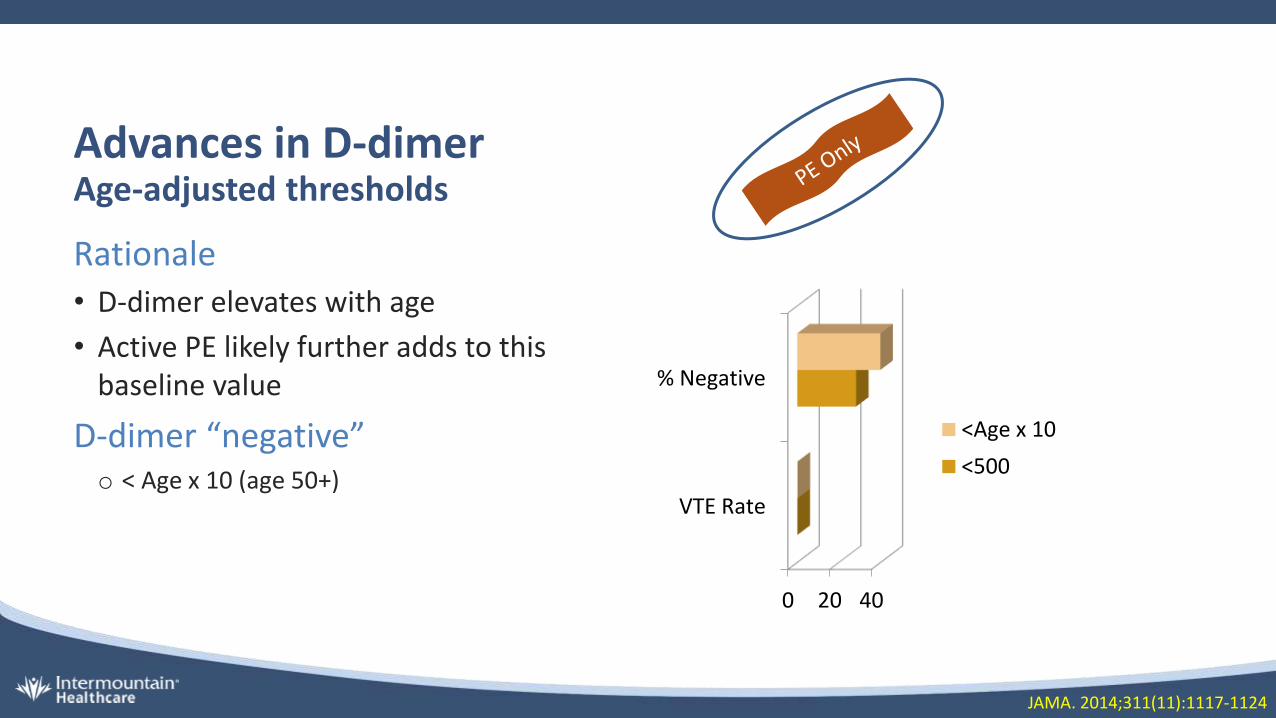
Advances in D-dimerAge-adjusted thresholds
Rationale• D-dimer elevates with age
• Active PE likely further adds to this baseline value
D-dimer “negative”o < Age x 10 (age 50+)
0 20 40
VTE Rate
% Negative
<Age x 10
<500
JAMA. 2014;311(11):1117-1124
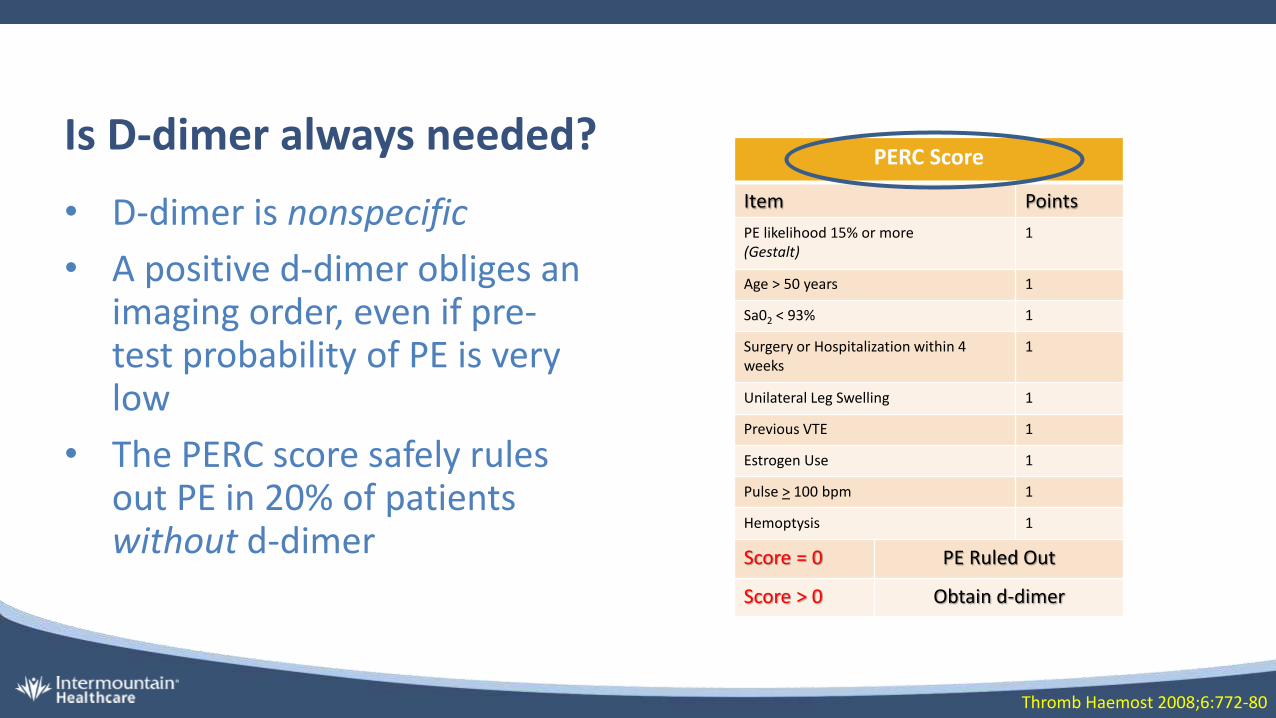
Is D-dimer always needed?
• D-dimer is nonspecific
• A positive d-dimer obliges an imaging order, even if pre-test probability of PE is very low
• The PERC score safely rules out PE in 20% of patients without d-dimer
Thromb Haemost 2008;6:772-80
PERC Score
Item Points
PE likelihood 15% or more(Gestalt)
1
Age > 50 years 1
Sa02 < 93% 1
Surgery or Hospitalization within 4 weeks
1
Unilateral Leg Swelling 1
Previous VTE 1
Estrogen Use 1
Pulse > 100 bpm 1
Hemoptysis 1
Score = 0 PE Ruled Out
Score > 0 Obtain d-dimer
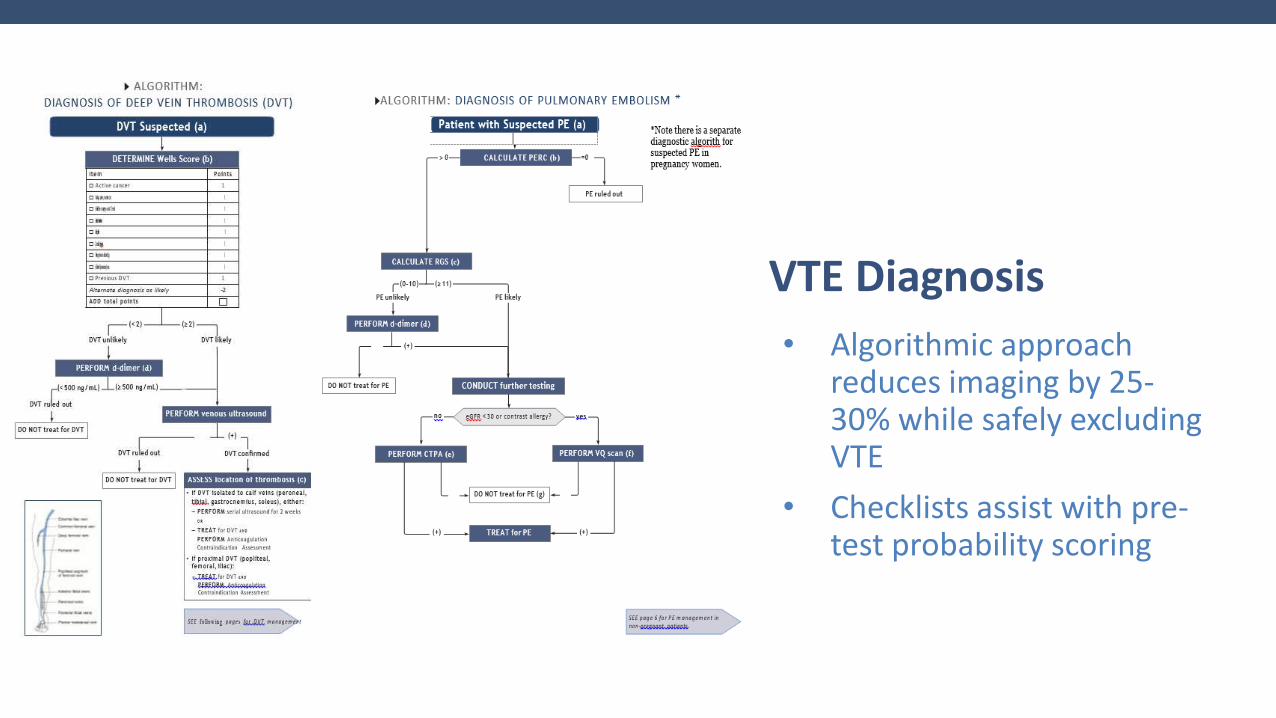
• Algorithmic approach reduces imaging by 25-30% while safely excluding VTE
• Checklists assist with pre-test probability scoring
VTE Diagnosis

Highlights
Selection of Anticoagulant
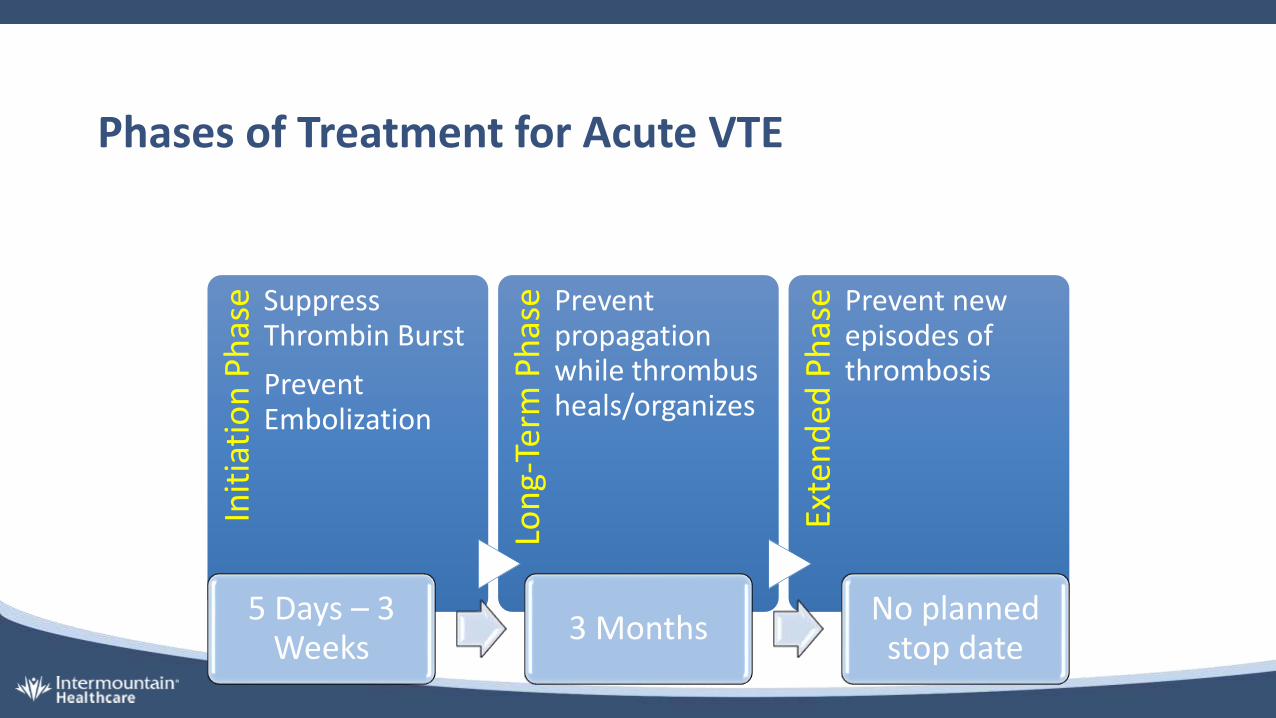
Phases of Treatment for Acute VTE
Init
iati
on
Ph
ase Suppress
Thrombin Burst
Prevent Embolization
Lon
g-Te
rm P
has
e Prevent propagation while thrombus heals/organizes
Exte
nd
ed P
has
e Prevent new episodes of thrombosis
5 Days – 3 Weeks
3 MonthsNo planned
stop date

Treatment OptionsInitiation Long Term Extended
UFH/LMWH + Warfarin(5+ Days)
Warfarin @ INR 2-3 Warfarin @ INR 2-3
Enoxaparin 1mg/kg BID (5-10 days)
Dabigatran 150 BID Dabigatran 150 BID
Enoxaparin 1mg/kg BID(7 days)
Edoxaban 60mg Daily Edoxaban 60mg Daily
Apixaban 10mg BID(7 days)
Apixaban 5mg BID(6 months)
Apixaban 2.5mg BID
Rivaroxaban 15mg BID(21 days)
Rivaroxaban 20mg Daily Rivaroxaban 20mg Daily
Dalteparin 200 IU/Kg Daily(1 month)
Dalteparin 150 IU/Kg Daily Dalteparin 150 IU/Kg Daily(? Reduce dose)
Enoxaparin 1mg/kg BID Enoxaparin 1mg/kg BID Enoxaparin 1mg/kg BID (?Reduce Dose)
Swit
cher
sLo
ader
sC
ance
r
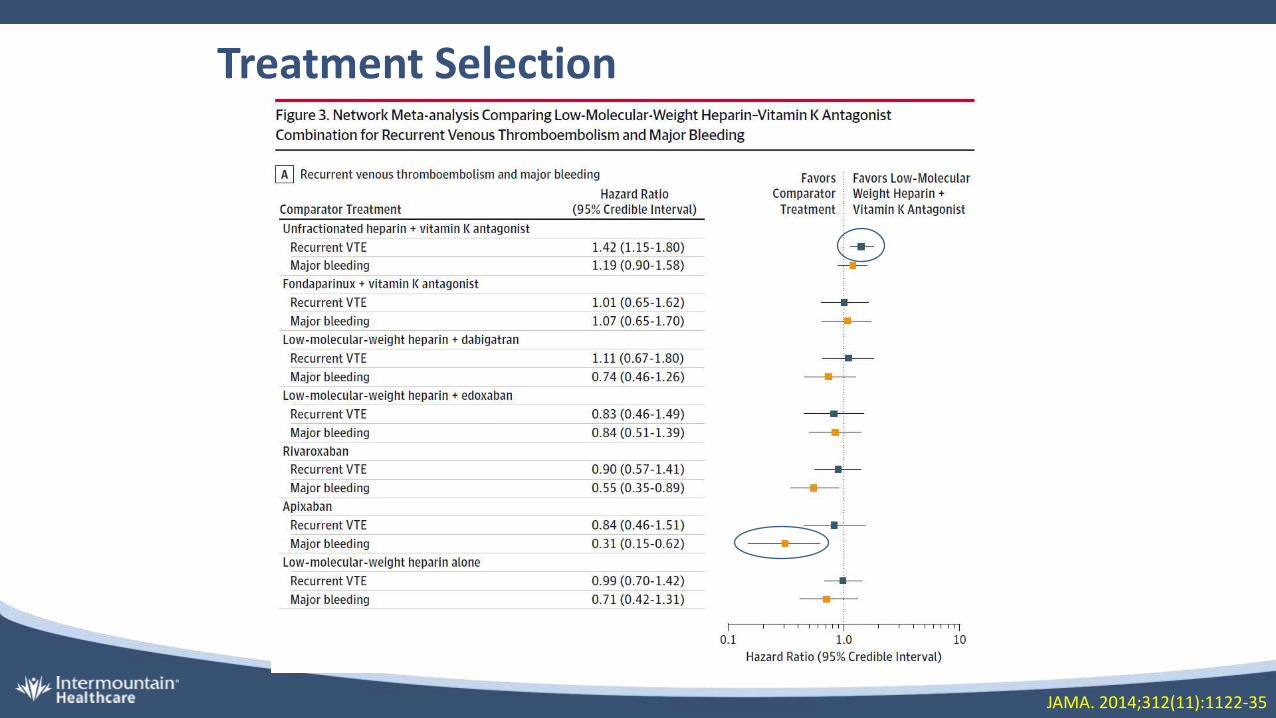
Treatment Selection
JAMA. 2014;312(11):1122-35
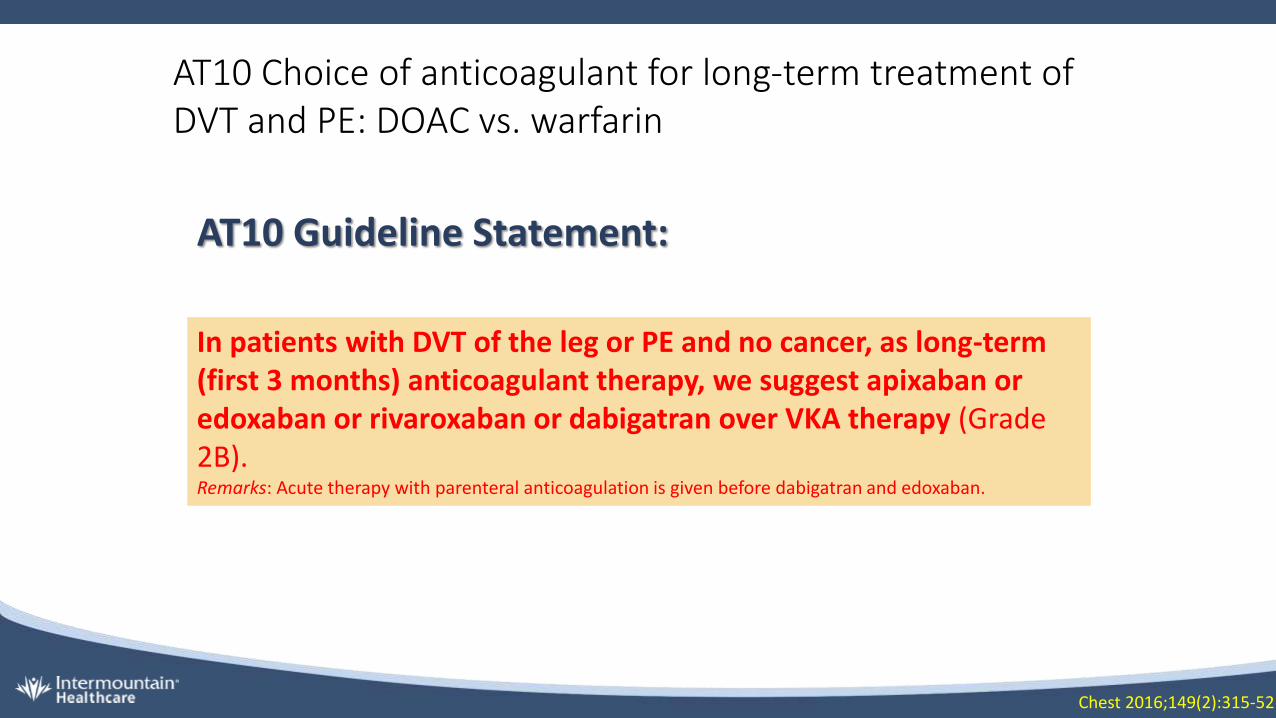
AT10 Guideline Statement:
AT10 Choice of anticoagulant for long-term treatment of DVT and PE: DOAC vs. warfarin
In patients with DVT of the leg or PE and no cancer, as long-term (first 3 months) anticoagulant therapy, we suggest apixaban or edoxaban or rivaroxaban or dabigatran over VKA therapy (Grade 2B).Remarks: Acute therapy with parenteral anticoagulation is given before dabigatran and edoxaban.
Chest 2016;149(2):315-52
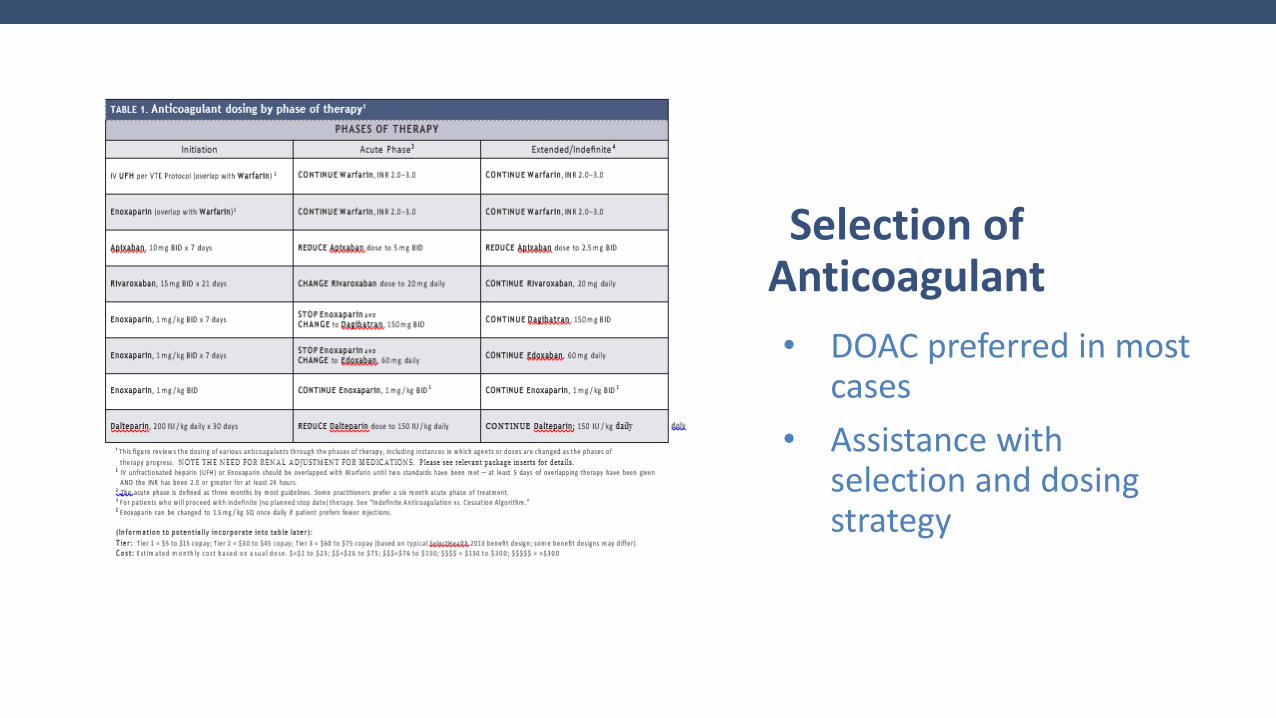
• DOAC preferred in most cases
• Assistance with selection and dosing strategy
Selection of Anticoagulant
Highlights
Treatment Venue

PE Risk Stratification
ESC System
Acu
te P
E
Low Risk
Low-Intermediate Risk
High-Intermediate Risk
High-Risk
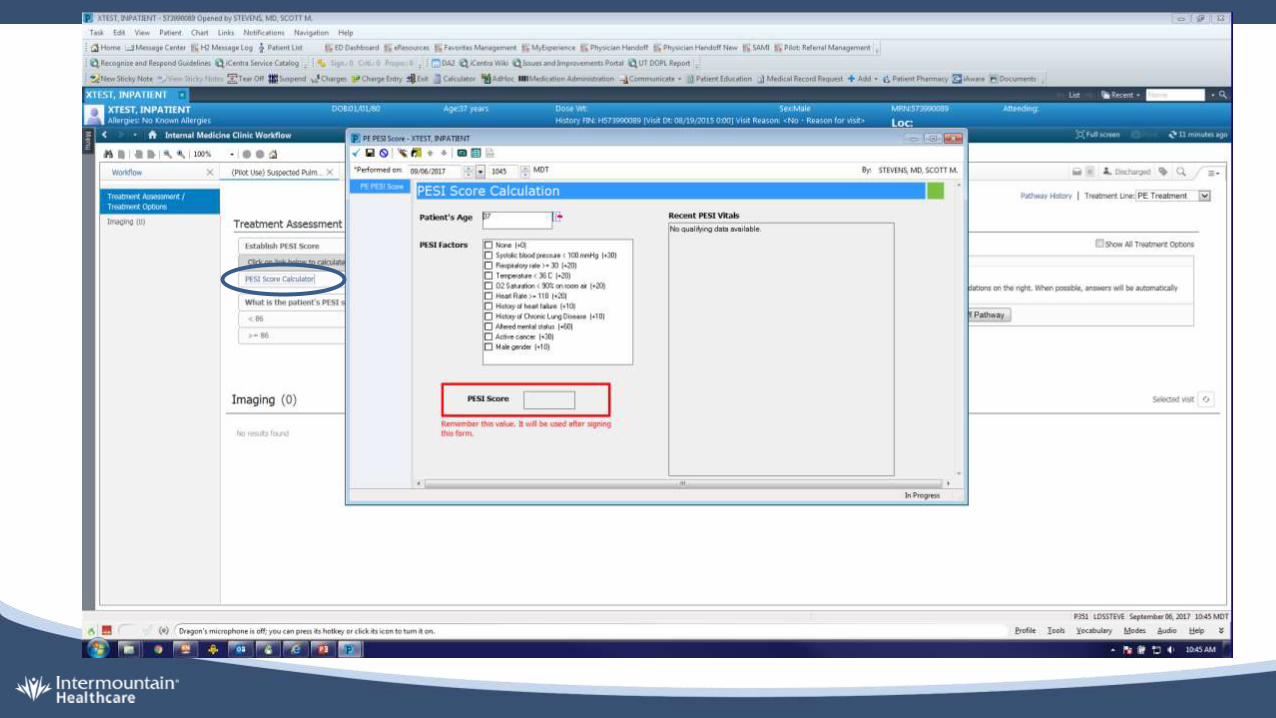
PESI Score
Item Points
Age Age x 1
Male 10
History of Cancer 30
History of Heart Failure 10
History of Chronic Lung Disease 10
Pule > 110 bpm 20
SBP < 100 mmHg 30
Respirations > 30/min 20
Temperature < 36 20
Altered Mental Status 60
Sa02 < 90% 20
Class I < 65
Class II 66 - 85
Eur Heart J 2008;29:2276-315. Lancet 2011;378:41-8
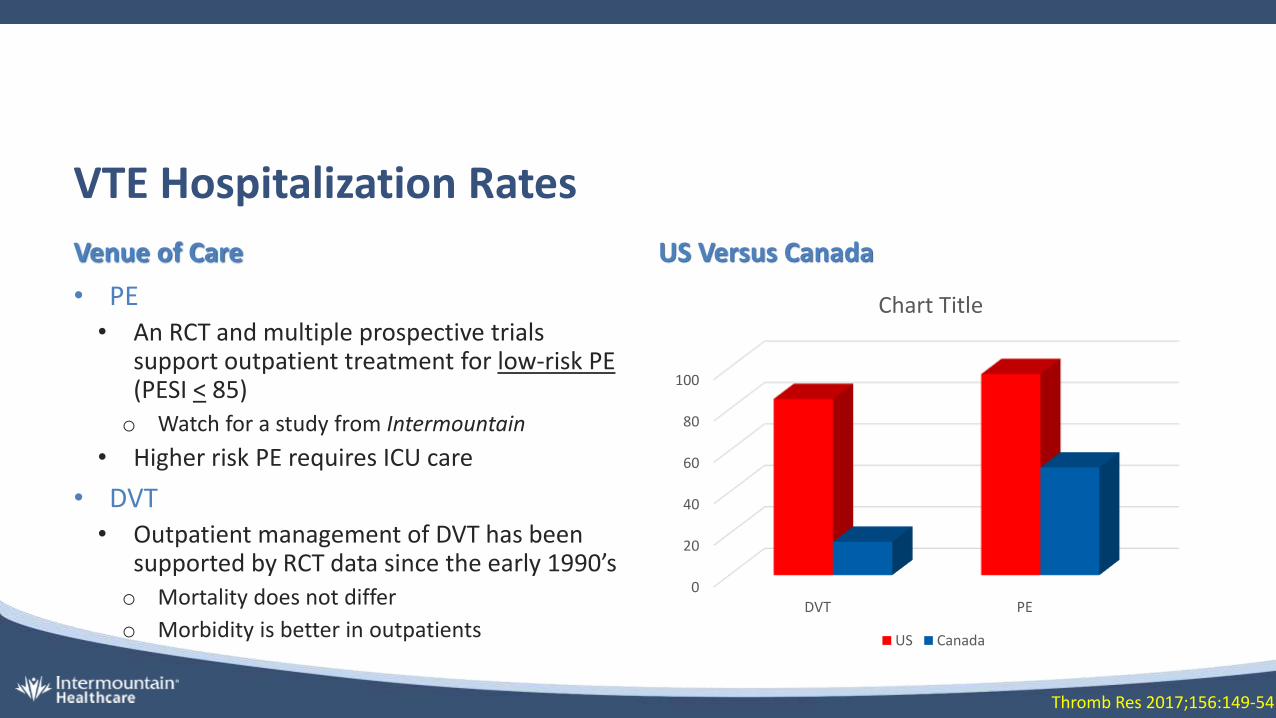
VTE Hospitalization Rates
Venue of Care US Versus Canada
• PE• An RCT and multiple prospective trials
support outpatient treatment for low-risk PE(PESI < 85)o Watch for a study from Intermountain
• Higher risk PE requires ICU care
• DVT• Outpatient management of DVT has been
supported by RCT data since the early 1990’so Mortality does not differ
o Morbidity is better in outpatients
0
20
40
60
80
100
DVT PE
Chart Title
US Canada
Thromb Res 2017;156:149-54
AT10 Guideline Statement:
AT10 Treatment of Acute PE Out of the Hospital
In patients with low-risk PE and whose home circumstances are adequate, we suggest treatment at home or early discharge over standard discharge (eg, after first 5 days of treatment)(Grade 2B).
Chest 2016;149(2):315-52
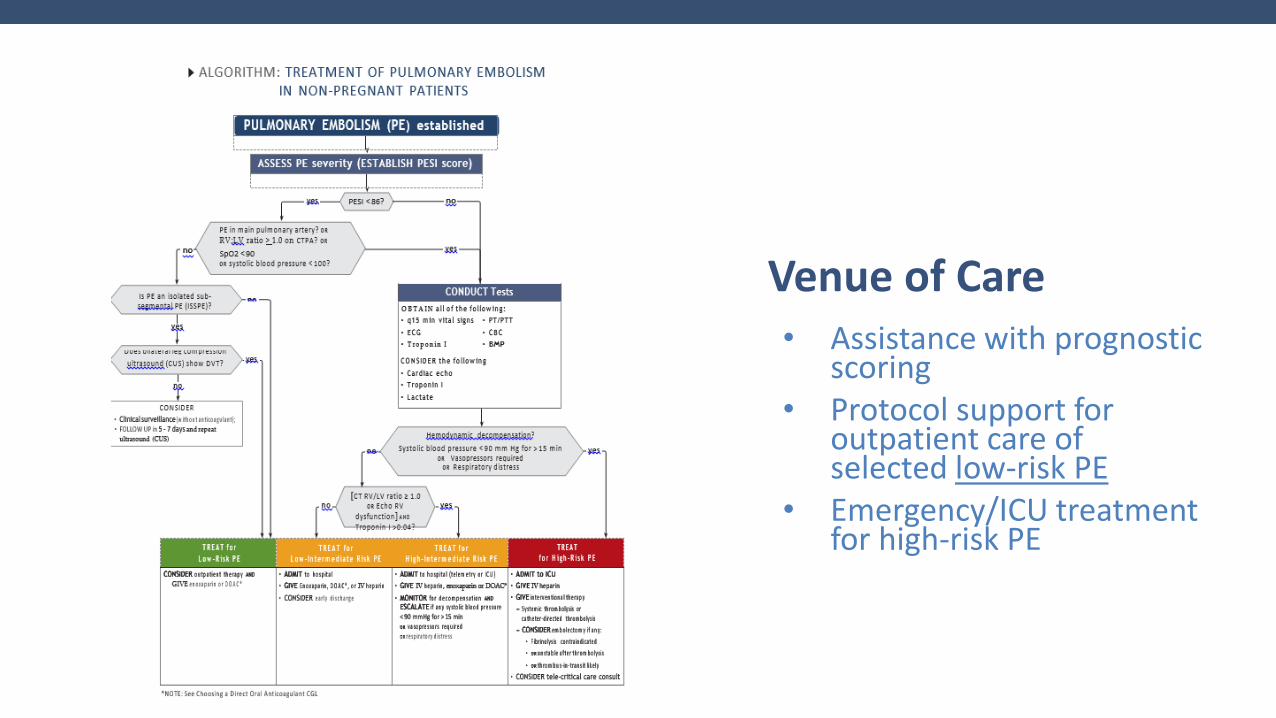
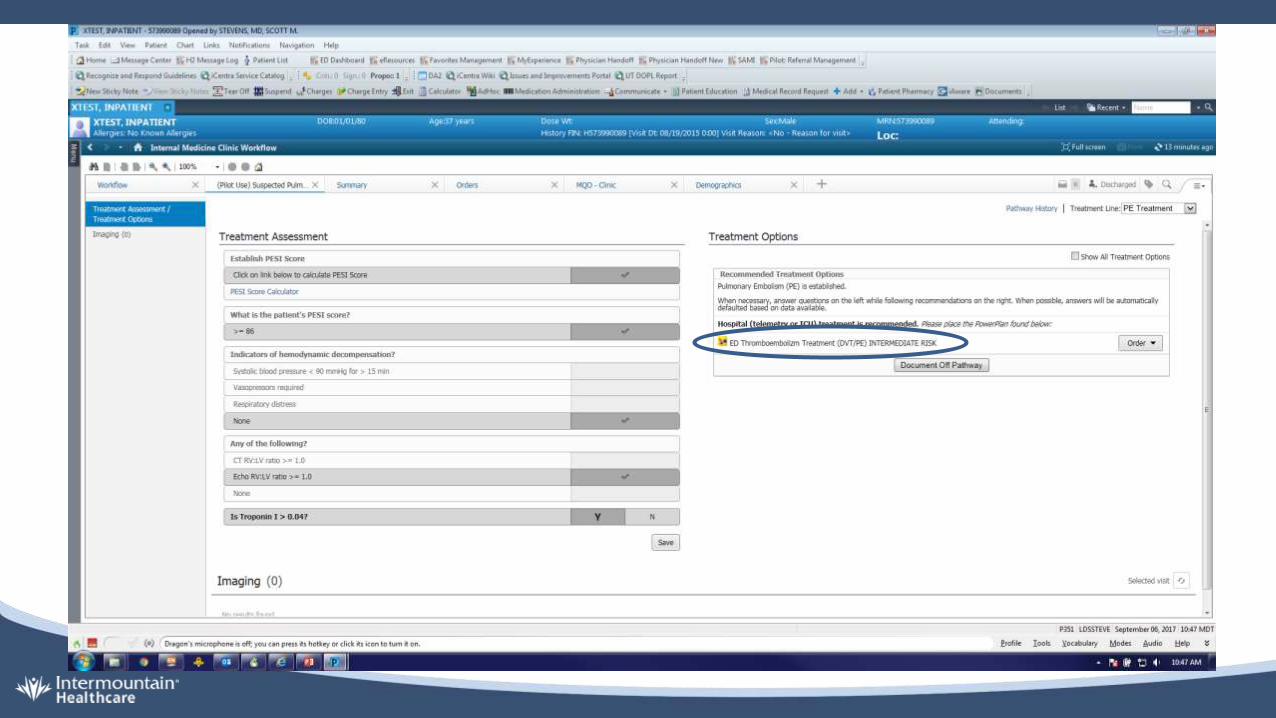
• Assistance with prognostic scoring
• Protocol support for outpatient care of selected low-risk PE
• Emergency/ICU treatment for high-risk PE
Venue of Care
Highlights
Avoiding Overtreatment
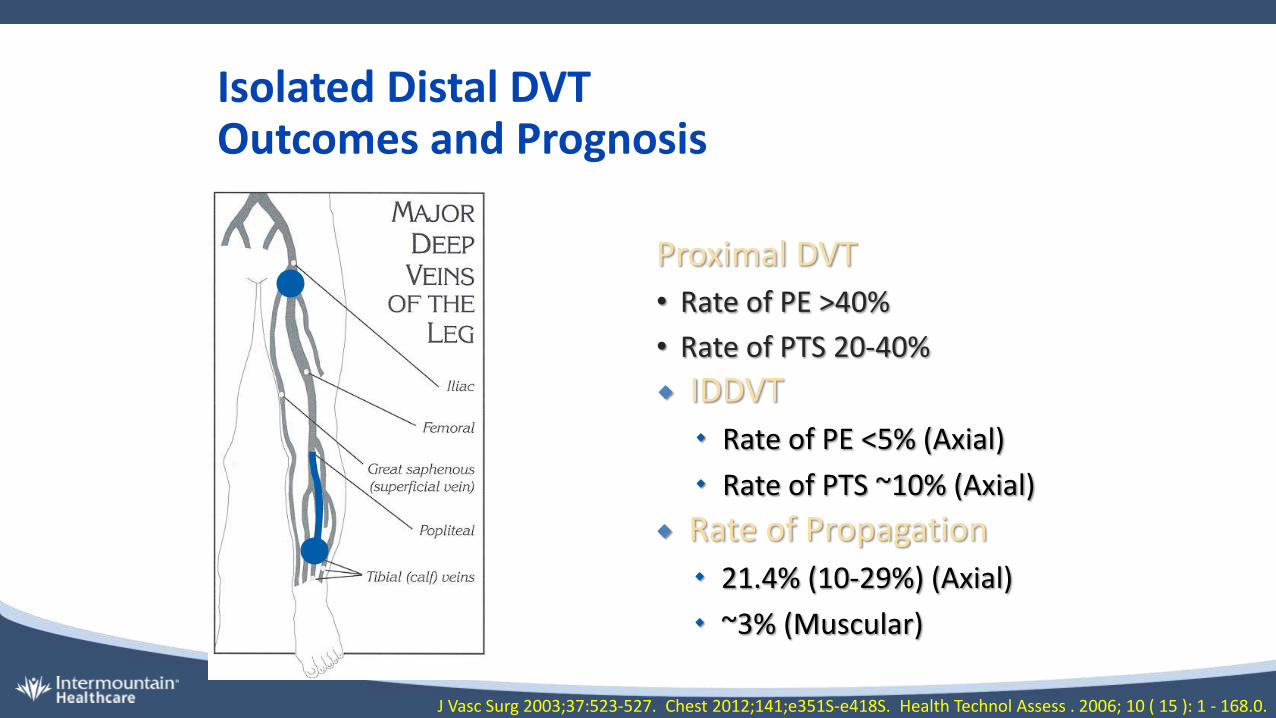
Isolated Distal DVT Outcomes and Prognosis
Proximal DVT• Rate of PE >40%
• Rate of PTS 20-40%
IDDVT
Rate of PE <5% (Axial)
Rate of PTS ~10% (Axial)
Rate of Propagation
21.4% (10-29%) (Axial)
~3% (Muscular)
J Vasc Surg 2003;37:523-527. Chest 2012;141;e351S-e418S. Health Technol Assess . 2006; 10 ( 15 ): 1 - 168.0.
AT10: Whether to Anticoagulate Isolated Distal Deep Vein Thrombosis
Extension Risk Factors
• Positive D –dimer
• Extensive or close to the proximal veins
• No reversible provocation
• Cancer
• Prior DVT
• Inpatient
13. In patients with acute isolated distal DVT of the leg and (i) without severe symptoms or risk factors forextension (see text), we suggest serial imaging of the deep veins for 2 weeks over anticoagulation (Grade 2C).
Chest 2016;149(2):315-52
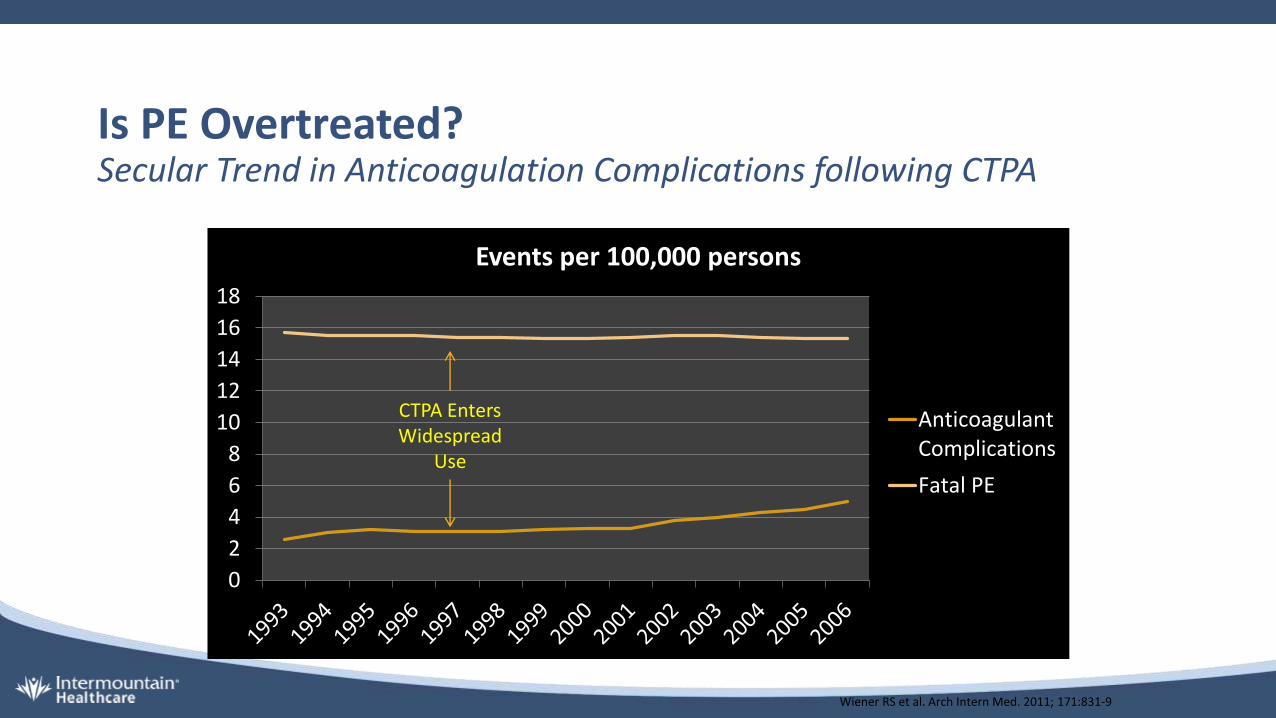
Wiener RS et al. Arch Intern Med. 2011; 171:831-9
Is PE Overtreated?Secular Trend in Anticoagulation Complications following CTPA
0
2
4
6
8
10
12
14
16
18
Events per 100,000 persons
AnticoagulantComplications
Fatal PE
CTPA Enters Widespread
Use
Evaluation of Individuals with Pulmonary Nodules: General Approach
42. In patients with subsegmental PE (no involvement of more proximal pulmonary arteries), no proximal DVT in the legs, and a low risk for recurrent VTE (see text), we suggest clinical surveillance over anticoagulation(Grade 2C).
AT10: Whether to Anticoagulate SubsegmentalPulmonary Embolism
43. In patients with subsegmental PE (no involvement of more proximal pulmonary arteries), no proximal DVT in the legs, and a high risk for recurrent VTE (see text), we suggest anticoagulation over clinical surveillance (Grade 2C).
Chest 2016;149(2):315-52
Progression Risk Factors
• Hospitalized or immobile patient
• Active cancer
• No reversible risk factors
• D-dimer elevated (marked, unexplained)
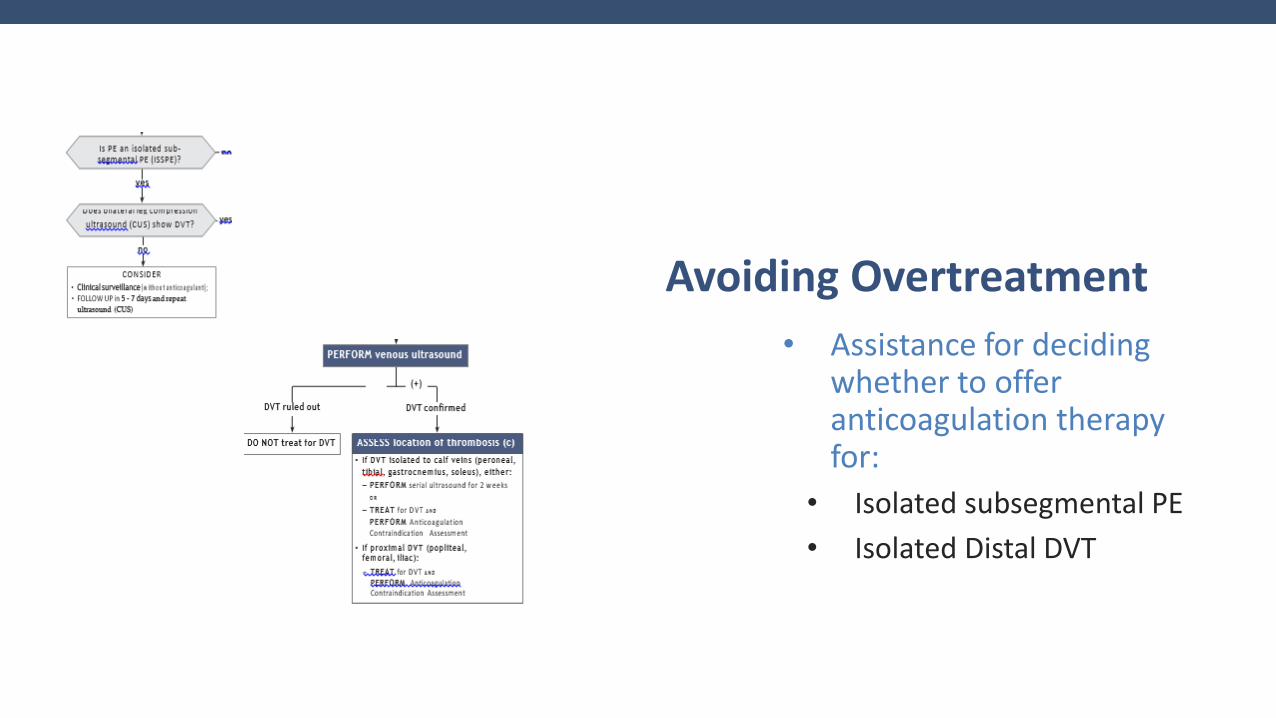
• Assistance for deciding whether to offer anticoagulation therapy for:
• Isolated subsegmental PE
• Isolated Distal DVT
Avoiding Overtreatment
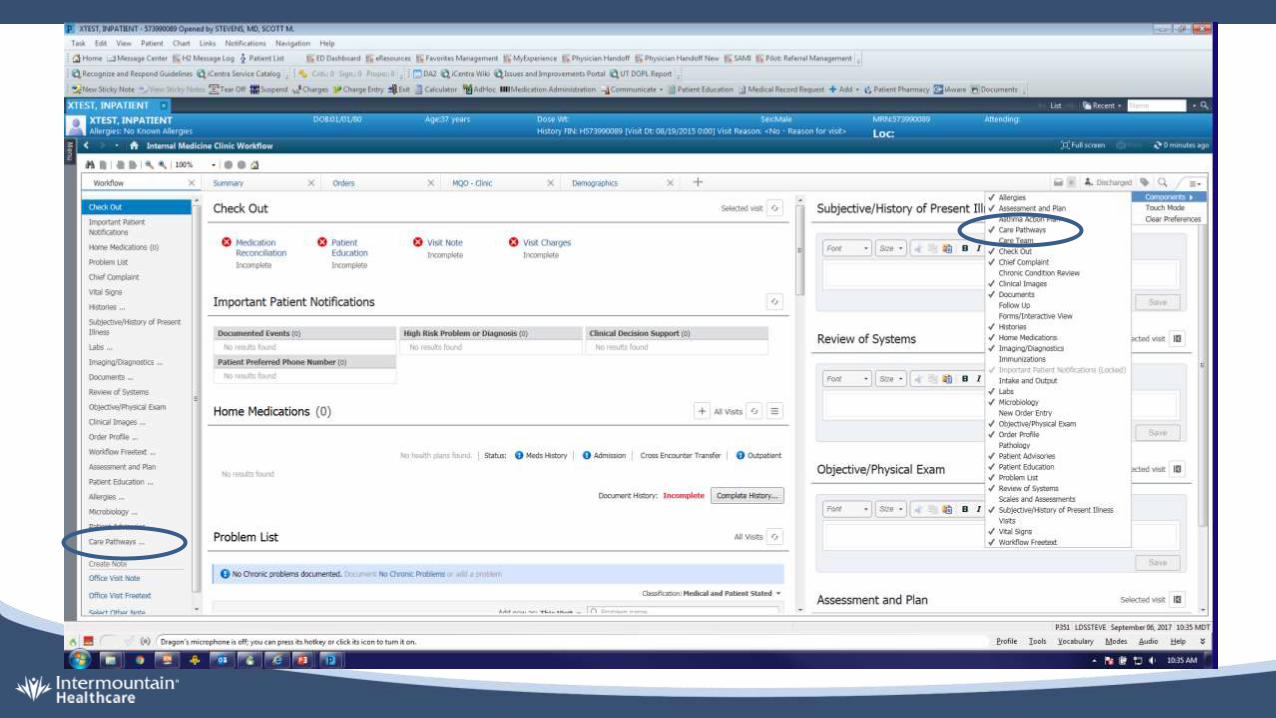
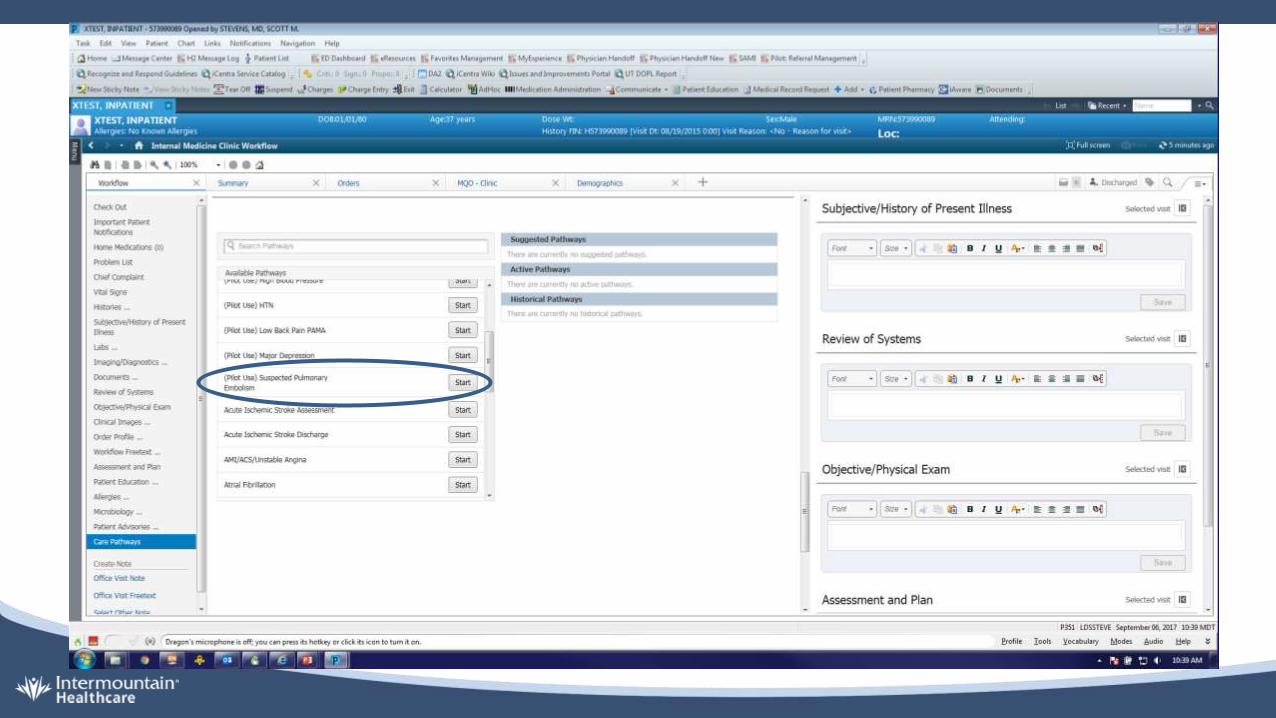
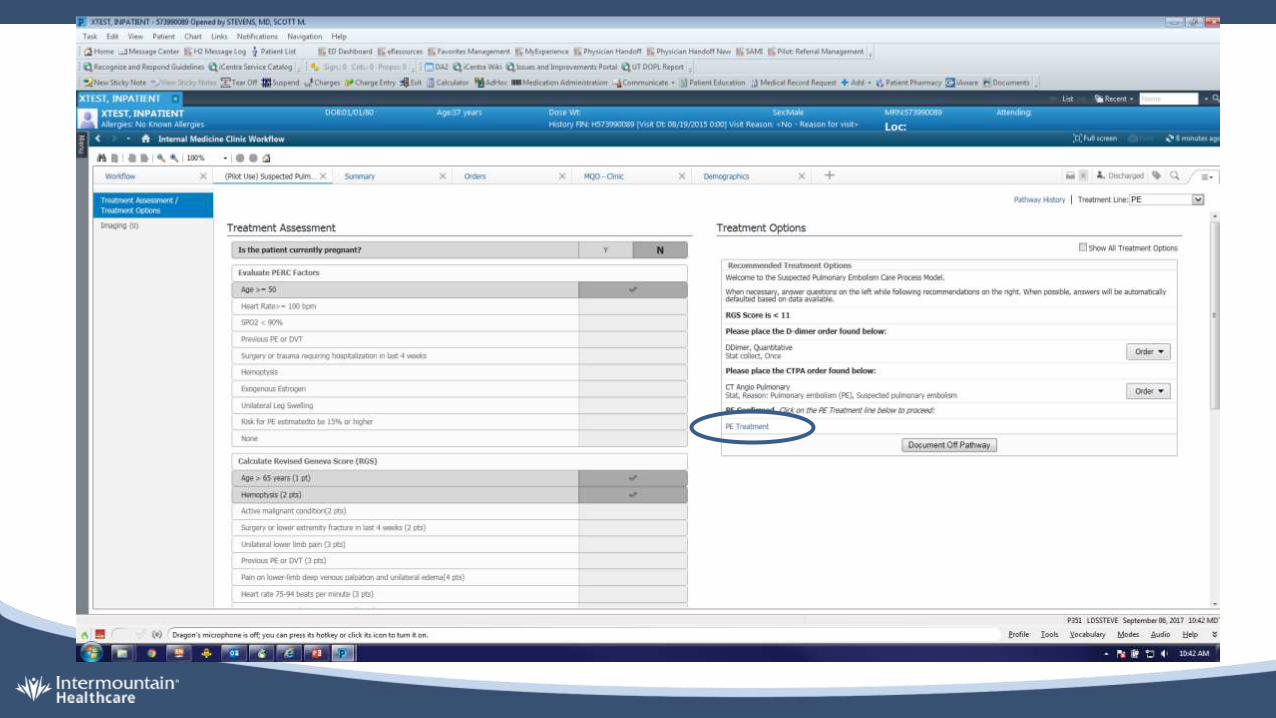
This is Intermountain, right?
Where are my eProtocols?
The VTE Care Pathway in iCentra
The VTE CPM Team
Stacy HillingCarl BlackColleen RobertsDavid JacksonDon LappeC. Gregory ElliottJames HellewellJoseph BledsoeKaren ConnerKathryn KutlerMark KringlenMark MankivskyNancy NelsonPeter HaugRich PattenScott StevensScott WollerSteven HessTerry Clemmer
Thank you!
Please help us improve the [email protected]
Type “ClinicalProcess” into your browser
https://m.intermountain.net/clinical/pages/all-care-process-models-(cpms).aspx