Embed Size (px)
Citation preview

Delivering Public Service Reform in
Wigan
January 2016
Blank page

Contents Foreword Start Well Perfect Week (St. George’s Primary School) Children’s Innovation: Adolescent Mental Health Live Well Enhanced Alcohol Pathway Working Well Live Well Complex Dependency Team Co-ordinated Community Response to Domestic Abuse Community Risk Intervention Team (CRIT) Platt Bridge Place Based Integration
Age Well & Health and Social Care Integrated Neighbourhood Teams Integrated Health and Social Care: Locality Plan Hospital Discharge Enablers Workforce Reform: The Deal Spatial Planning


Foreword
This is the third Public Service Reform event in Wigan. Our first event brought partners together to discuss opportunities for public services in the borough to work differently together. Our second event focused on developing a shared understanding of some of the core characteristics of public service reform. This third event is intended to demonstrate some of the excellent work that has been tested and implemented in Wigan over the previous few years. The rationale for a fundamental reform of public services remains truer than ever in the light of rising demand, and reducing budgets. Securing a transformational reduction in demand, moving from reactive and high cost services to targeted and planned spend, reducing duplication, and delivering better outcomes, is at the heart of our PSR ambition. In this booklet are some examples of the work we have been doing. This is by no means a comprehensive list, but is here to demonstrate significant progress, and to exemplify some or all of the characteristics of PSR discussed at the last meeting.
Start Well o Perfect Week (St. George’s Primary School, Atherton) o Adolescent Mental Health Innovation Project
Live Well o Enhanced Alcohol Pathway o Working Well o Live Well Complex Dependency Team o Co-ordinated community response model to Domestic Abuse o Community Risk Intervention Team (CRIT) o Place Based Integrated Working (Platt Bridge)
Age Well, Integrated Health and Social Care o Integrated Neighbourhood Teams (INT’s) o Locality Plan o Hospital Discharge
Enablers o Workforce Reform: The Deal o Spatial Planning
In the workshops today we will hear directly from those involved in these and other projects. A key focal point is to discuss what needs to happen next to build on the good progress of partners in Wigan in the way public services work together, and also to consider what needs to happen to scale this work- to move from pilots and individual projects to the mainstreaming of reform. The strategic frameworks that guides our joint work in Wigan – for example the Locality Plan for health and care reform, the Council 5 year strategy ( Deal for the future), our borough wide mental health strategy, are all predicated in full or part on delivering the ambition of our PSR programme and supporting residents to be well, independent, and in control of their lives. Building on this great start is our priority and we hope that you enjoy the workshop. Will Blandamer Assistant Director, Reform and Partnerships, Wigan Council

START WELL

Perfect Week: St. George’s Primary School (Atherton)
Summary A ‘Perfect Week’ is a management tool that ‘suspends the rules’ for a short amount of time in a department or setting in order to trial new ways of working. Building on our experience of delivering a Perfect Week in a GP setting at Boston House Medical Centre we wanted to apply this learning to an Education setting for a week in May 2015. We know that that schools are one of the only agencies who see children and families on a daily basis and are well placed to facilitate an integrated approach that, in turn, could reduce duplicate and costly interventions and improve outcomes at the earliest stages. The activity that took place in Perfect Week was designed with partners, parents and the community.
What’s different?
Close partnership working within the school and with key agencies including Gateway, children’s social care, housing, leisure, CAMHS, police and fire and rescue.
Using intelligence together to target specific cohorts.
Reducing the number of times children, young people and their families have to tell their story by investing more time up front getting to the heart of the problem to get things right first time.
Making best use of community assets and investing in local community led solutions where it is safe to do so.
Access to evidenced interventions, with a focus on dealing with the ‘root cause’, building resilience and reducing demand.
A shared deal with the community that sets out commitments of public services and individuals, their families and communities.
Understanding whole system demand and service use so that we can respond appropriately in a joined up way.
Impact A significant amount of learning emerged from the Perfect Week and a comprehensive action plan has been developed to ensure this learning underpins the children’s transformation programme. Some of the key areas are:
Data and Intelligence: Schools hold a wealth of data and local knowledge and can play a key role in improving outcomes. This isn’t always possible as key information/ data held by services isn’t shared with schools.
Co-location of services: multi agency teams working on a locality footprint know the families and their needs.
Developing school capacity – schools can be empowered to deliver low level interventions such as early help and lower level CAMHS with the right training, information and advice.
Partnership working: professionals were able to get back to their core function – frontline. Wider services including housing, adult social care, Live Well, debt, Life Centres can play a key role in an integrated offer.
Family centred approach/ role of key worker – schools play an important role in an integrated model – they see children daily! Referral mechanisms, bureaucratic processes and hands offs can cause barriers and stop interventions from being timely.
The cost benefit analysis of the Perfect Week was profiled across a 5 year period and indicated a potential gross fiscal saving of £1,196,918 across public sector partners with a net fiscal saving of £995,465

Adolescent Mental Health Innovation Project
Summary In Summer 2014, the Department for Education announced the creation of a £100m Innovation Programme with the aim to act as a catalyst for developing more effective ways of supporting vulnerable children. Local Authorities and / or organisations that work across social care, justice, health and education, were given the opportunity to apply for funding from the programme. Social Care and Adolescence Mental Health Project (Wigan Council and Wigan Borough Clinical Commissioning Group) were successful in securing almost £1m in funding to resolve the rapid escalation of complex mental health cases who become a Child Looked After.
What’s different?
Resolve local challenges in relation to young people presenting at A&E and subsequent admittance to paediatric and general medial assessment wards.
Builds an integrated assessment and care planning mechanism that can operate for Children’s Social Care and CAMHS Services.
Uses new conversation and an asset based approach with young people and their families to gain a better insight into how to resolve the problem.
Co-production; a series of workshops with staff and young people to ensure co-production was at the centre of service design.
Governance – established governance structures and mechanisms with partner agencies involving Children’s Social Care, Community CAMHS, WWL RAE and T4 CAMHs provision.
The YP reference group and peer support group will develop a campaign for young people ‘What is mental health.’ This will raise aware of mental health and provide key messages to appropriate support emotional health and well being.
A full cost benefit analysis is underway for the project and is demonstrating significant through the delivery of the service.
The team will have a role in developing building confidence and skills within both Children’s Social Care Services and 5BP Community CAMHs team. The team will also have a role within other residential provision and foster service.
Impact
An operational pathway is established that complements statutory functions with Children’s Social Care.
Recruitment of an integrated staff team from both NHS 5BP and Wigan Children’s Services. The team have been operational since September 2015.
A young person’s reference group has been established that will continuously shape service delivery. This group will develop a campaign for young people, “What is mental health” to raise awareness.
The service (SHARE) was expected to work with 20 young people as part of the bid however it is anticipated to work with 30 young people. It is currently working with 16 young people and is having real success
Since the implementation of the project a number of initial conclusions are starting to emerge: o Integrated service delivery provides staff with the confidence to take responsibility for the young
person rather that referring to another agency. o The model has empowered staff to find solutions that are not bound by thresholds and criteria o The cohort is complex and young people have had intermittent contact with CAMHs Services for a
significant period of time. o Parents and wider family often feel lost and unable to cope and manage the situation. o Support parents and family members to develop strategies to cope identify and respond
appropriately to risk

Live Well

Enhanced Alcohol Pathway
Summary Wigan borough has a higher than average rate in a number of alcohol indicators and feedback from GPs highlights the need of additional support around drugs and alcohol issues. In response to this additional investment has been provided through the Joint Commissioning Board to enhance the alcohol pathway. This has enabled an expansion of the primary care support, clinical interventions, Active Case Management (ACM) and the mutual aid element of the Wigan & Leigh Drug and Alcohol Recovery Partnership (Greater Manchester West NHS Trust and Addaction). Funding has also provided for additional nurse capacity and specialist nurse capacity regarding alcohol related liver disease within the Alcohol and Drugs Specialist Nurse Team at WWL NHS Trust.
What’s Different?
GPs are able to identify patients with a high risk of attending hospital in the next 12 months who have had previous alcohol specific admissions or outpatient appointments. GPs are also referring high risk patients with alcohol issues to INTs.
Wigan and Leigh Recovery Partnership are part of the Integrated Neighbourhood Team programme, with staff dedicated to each INT cluster and focused on the CCG risk stratification tool. This includes direct referrals from A&E / Wards at Royal Albert & Edward Infirmary.
The Wigan & Leigh Recovery Partnership deliver satellite clinics in three primary care locations across the Borough (in addition to Marsh Green). GPs from the surgeries can refer patients to the clinics where they are encouraged to engage with alcohol and drugs services, are triaged and are signposted / referred to appropriate intervention.
A series of Alcohol Guides has been produced and distributed to GPs across the Borough and to a range of other organisations. The Guides cover a general guide on alcohol (units and ways of cutting down) as well as a guide about The Wigan and Leigh Recovery Partnership (TRP) and how to access the Service.
The detection of an Alcohol Liver Disease pathway is being tested with referrals from A&E, alcohol and drug services and a limited number of GPs.
Staff, recovery champions and volunteers have been trained up in how to deliver Mutual Aid Partnership (MAP) techniques and strategies which can help provide new ways of coping with the effects of alcohol and drug misuse within the family.
Impact
The “expected” number of alcohol specific emergency admissions for 2014/15 was 1,099. The actual figure was 952. For quarter 4 of 2014/15 the expected number of emergency admissions was 275, the actual number being 209, a reduction of 66 admissions (a reduction of 24%) for the quarter.
The Treatment Outcomes Profile (TOPs) for clients at the start of and exit from treatment for Active Case Management clients between 1st January 2013 and 30th April 2015 (26 clients), the average units of alcohol consumed per day had reduced from on average 30 units per day at start of treatment to 12 units per day at treatment discharge.
The number of days alcohol had been consumed in the last 4 weeks had reduced from an average of alcohol consumed 25 days out of the last 28 days to 4 days out of the last 28 days.
Clients rating of their own psychological health increased from an average rating of 18 to 27. Clients rating of their own physical health increased from an average rating of 20 to 28. Quality of Life rating increased from an average of 18 to 28 for ACM clients.

Working Well
Summary Working Well is a GM programme that began operating across the region in March 2014 to support Employment and Support Allowance (ESA) claimants who have completed the Work Programme without finding employment. Phase one of the programme in Wigan has been delivered by Ingeus with the objective of building an offer of intensive and integrated support, helping individuals tackle the specific barriers to work. The expansion of Working Well is a central pillar of the GM devolution agreement with plans for an expanded programme to support 50,000 people across the region to progress towards employment. The agreement also makes provision for a GM joint commission, with the DWP, on Work Programme provision that draws on and complements Working Well expansion, a reformed post 19 skills landscape and broader employment and skills reform and a reshaped FE post 19 skills system
What’s different?
GM provision delivering locally as part of a wider integrated partnership with multi-agency case conferencing used to identify progression and lead partners.
Local employment support delivered locally as part of an integrated network with focus on the right service for the right individual at the right time.
A mental health pathway has been established to provide holistic support with IAPT provision where appropriate for the borough. Working Well provision will sit as part of this.
Supported Employment delivering Supported Traineeships and Internships.
Business Engagement Officers are making links between local businesses and employment support.
Partnership agreements developed with new employers entering the borough to provide local employment opportunities.
The GM eco system has been planned with partners to deliver a fully co-ordinated employment journey for individuals.
Impact
30 people have secured employment via Working Well
24 individuals with disabilities into work via Supported Employment. Since November 2014 Wigan’s unemployment figures have significantly improved:
o All Age claimant counts reduce by 29.81%
o All Age 6 month plus claimant counts reduce by 25%
o Youth claimant counts reduce by 51.35% and Youth 6 month plus claimant counts reduce by 43.75%
All Age Unemployment
November 2014
October 2015
November 2015
% Monthly Change
% Annual Change
Bolton 4,380 2,985 2,895 -3.02% -33.90%
Bury 2,105 1,600 1,675 4.69% -20.43%
Manchester 10,450 6,660 6,565 -1.43% -37.18%
Oldham 2,620 2,225 2,200 -1.12% -16.03%
Rochdale 2,775 2,035 2,020 -0.74% -27.21%
Salford 3,790 2,655 2,615 -1.51% -31.00%
Stockport 3,545 2,125 2,035 -4.24% -42.60%
Tameside 2,605 1,860 1,880 1.08% -27.83%
Trafford 1,935 1,315 1,325 0.76% -31.52%
Wigan 3,925 2,820 2,755 -2.30% -29.81%
Greater Manchester 38,125 26,275 25,970 -1.16% -31.88%

Live Well Complex Dependency Team
Summary In 2014, Wigan identified a significant challenge with complex and chaotic individuals known to be placing a high demand and high cost on public services. Characteristically, cases had been referred across the system on the basis of specific issues (housing, anti-social behaviour, mental health and drug and alcohol abuse). Insights from the Council’s ‘Creative Council’ work, alongside wider insights from behavioural economics, ethnography, innovation and co-production work pointed to the need for new conversations with service users and residents and a step back from the deficit based, managerial approaches. Wigan Council funded a pilot project to test the hypothesis that an early intervention team, working to the above principles, would be able to reduce demand from these complex individuals that were bouncing round public sector systems being constantly assessed but not receiving an intervention. The Live Well Team consists of nine individuals drawn from a wide variety of existing services, adopting a multi agency approach and sharing specialist expertise within its own ranks
What’s different?
The Live Well approach offers new thinking, new insights and new solutions to what might be described as “wicked issues” that often require a better understanding of the complex factors at play.
The team is comprised of staff from a number of different agencies and background, working in a place based approach and engaging adults of working age with a complex dependency on public services, including health and care services.
Up to 40% of the risk stratification of non-elective admissions are adults of working age and there is a demonstrable overlap with the live well cohort, to progress with this cohort the team is regularly working with and in integrated neighbourhood teams (INT’s)
The team has adopted an innovative approach to capturing key information to inform a robust evaluation and cost benefit analysis, including a chaos indicator and information about trigger points and predictors in order to influence mainstream services.
In the field the team has sought to collect information around as many of their cases as proved viable in the following areas and this included relationships to services in areas of mental health, ASB, drugs and alcohol abuse, life dynamics (chaos, health, money, work, social attitudes), predictors and trigger points and resilience.
Impact
The work of the team is substantially informing the further development of the risk stratification tool.
Improved mental and physical health due to reduction in alcohol and substance misuse.
More sustainable tenancies due to improved management of finance
Reduction in debt.
A significant reduction in police call outs for the top ten address for GMP leading to increased capacity for the force.
15 individuals have found employment – leading to a reduction in benefit payments and an increase in productivity for the Borough.
Evidence of reduction in GP and A&E attendance.
A robust cost benefit analysis for the team has identified that for every £1 spent, Live Well generates a Financial Return on Investment of £2.65 with a one year pay back period.
£2.6M
Benefits Delivered – over 5 years

Co-ordinated Community Response Model to Domestic Abuse
Summary Domestic Violence and Abuse remains a key issue within the Wigan Borough. Over 50% of our Troubled Families have one or more incident of domestic abuse, 81% Youth Offending Team clients have significant domestics abuse in their background and 41% of all violent crime is domestic abuse related. The Co-ordinated Community Response Model aims to take a holistic approach to support victims and perpetrators, brining agencies together to work in an integrated and co-ordinated way in or der to affect behaviour change. The new model addresses risk and need at all levels. The Integrated Safeguarding and Public Protection team is a co-located multi agency team that addresses medium and high risk cases through daily planning meetings. The Refuge and the Community Outreach services were re-commissioned and extensive training has been provided for front line staff. Finally, Operation Strive, funding through the Office of the Police Crime Commissioner, aims to provide a more robust approach to incidents that are categorised as standard risk.
What’s different?
The Integrated Safeguarding and Public Protection (ISAPP) team deliver a more timely and robust response to incidents of domestic violence and abuse. Victims and Perpetrators are offered support within 48/72 hours of any incident. Previously this would have been up to 4 weeks as a plan would not have been made until the next MARAC (Multi Agency Risk Assessment Conference) meeting was held.
A holistic approach is taken which aims to address the root case of the issue through a multi-agency team of professionals who can support on key areas such as housing, home safety, drugs and alcohol, and parenting .
Agencies work in partnership rather than in silos and this is more efficient with joint visits being made across agencies.
Timely and appropriate interventions are available for the cohort.
Refuge is now seen as a place of transition and every effort is made to move families into more sustainable tenancies.
A new outreach service is offering a range of appointment led and drop in support across the borough rather than in fixed venues.
Operation Strive is offering repeat visits to standard risk incidents ensuring that appropriate follow up and offers of support are made and any further issues are identified and addressed.
A Young Person’s Domestic Violence Advocate has been appointed and as well as carrying a case load, they spend time in schools training on healthy relationships.
Impact
Cost benefit analysis has shown a 20% reduction in re-victimisation for those clients that have plans through the ISAPP approach.
There has been a significant increase in successful prosecutions – we have gone from one of the worst performing courts to one of the top five performing courts in the country. This is as a result of increased evidence collection and willingness to give evidence from victims as a result of improved engagement.
Fiscal savings to the wider system of £585,000 per anum.
Average length of stay at the Refuge has gone from over six months to less than 7 weeks, increasing capacity and ensuring that the disruption to families is kept to a minimum.

Community Risk Intervention Team (CRIT)
Summary GMFRS has been working closely with North West Ambulance Service (NWAS) and Greater Manchester Police (GMP) for some time to improve quality of life outcomes for people in a way that also reduces impact on blue light services, benefits the National Health Service and Public Health provision, and realises financial benefits for all partners. This resulted in the introduction of Community Risk Intervention teams (CRIT) with teams funded by Greater Manchester Fire and Rescue Authority (GMFRA) being introduced in Wigan, Salford and Manchester boroughs. Thirty team members were recruited to facilitate delivery in all three boroughs from January 2015. The pilot was used to prove the concept prior to the arrival of £3.73m of Fire Transformation Funding (FTF) to enable the expansion of CRIT across Greater Manchester.
What’s different?
CRIT delivers a holistic prevention service in the homes of those identified as most at risk by the partners in the project, fitting a wide range of risk reduction equipment to mitigate risk and referring onto specialist services where appropriate.
The team have responded to calls to cardiac arrests and 27 other categories of life threatening calls alongside NWAS, falls in the home (where no injuries were apparent) on behalf of NWAS and ‘concerns for welfare’ on behalf of GMP.
On 1st March 2016, GMFRS will begin piloting a new front line delivery role across prevention and protection.
Improved information sharing between all partners and improved referral pathways between all organisations involved.
Teams are made up of responders trained in similar ways to GMFRS’ Community Safety Advisors, NWAS’ Community First Responders, GMP officers trained in mental health response and Local Authority officers trained in mental health awareness.
A holistic approach to home safety – giving risk reduction advice regarding fire, falls, crime and general detrition in health.
Installation of assistive technology and equipment at the point of service to reduce the risk of fire, falls and carbon monoxide poisoning and burglary.
Impact
Response to cardiac has been scaled up and absorbed as business as usual within a fire fighter delivery model in September 2015.
Benefits extend beyond fiscal and social value as the scale of delivery by GMFRs will improve the quality of life of recipients of our service whilst partners should see a reduction in demand for their services over a period of time.
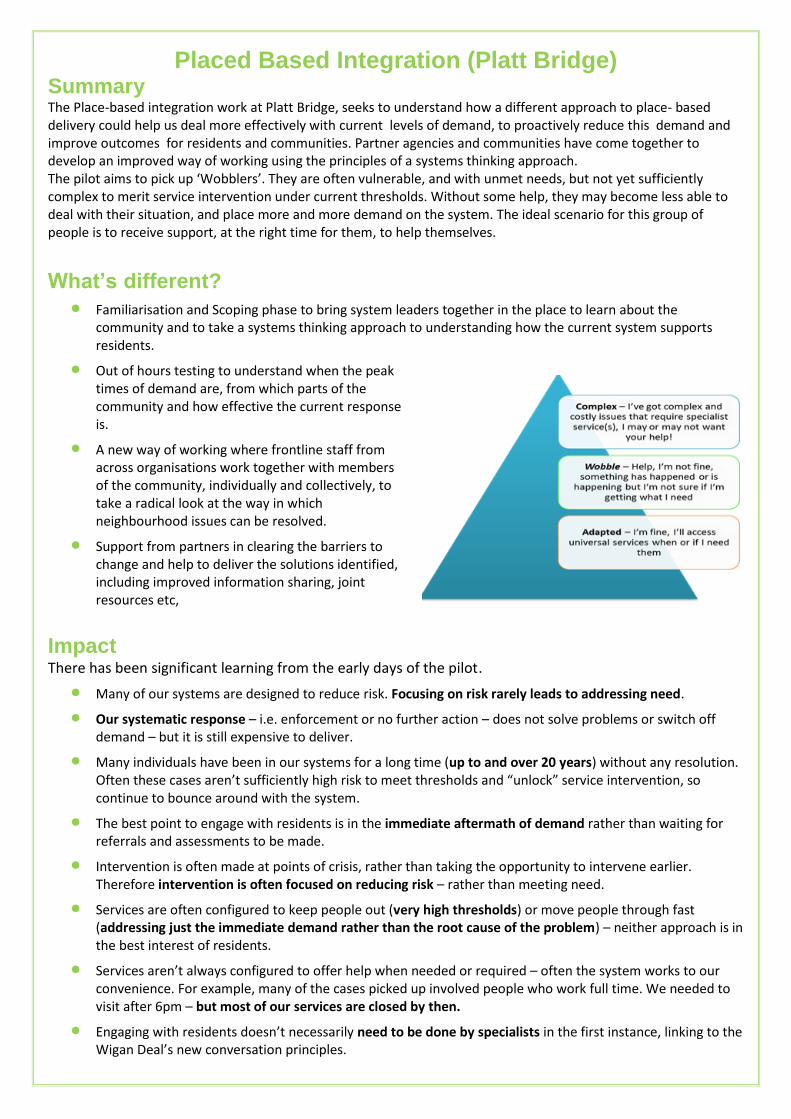
Placed Based Integration (Platt Bridge) Summary The Place-based integration work at Platt Bridge, seeks to understand how a different approach to place- based delivery could help us deal more effectively with current levels of demand, to proactively reduce this demand and improve outcomes for residents and communities. Partner agencies and communities have come together to develop an improved way of working using the principles of a systems thinking approach. The pilot aims to pick up ‘Wobblers’. They are often vulnerable, and with unmet needs, but not yet sufficiently complex to merit service intervention under current thresholds. Without some help, they may become less able to deal with their situation, and place more and more demand on the system. The ideal scenario for this group of people is to receive support, at the right time for them, to help themselves.
What’s different?
Familiarisation and Scoping phase to bring system leaders together in the place to learn about the community and to take a systems thinking approach to understanding how the current system supports residents.
Out of hours testing to understand when the peak times of demand are, from which parts of the community and how effective the current response is.
A new way of working where frontline staff from across organisations work together with members of the community, individually and collectively, to take a radical look at the way in which neighbourhood issues can be resolved.
Support from partners in clearing the barriers to change and help to deliver the solutions identified, including improved information sharing, joint resources etc,
Impact There has been significant learning from the early days of the pilot.
Many of our systems are designed to reduce risk. Focusing on risk rarely leads to addressing need.
Our systematic response – i.e. enforcement or no further action – does not solve problems or switch off demand – but it is still expensive to deliver.
Many individuals have been in our systems for a long time (up to and over 20 years) without any resolution. Often these cases aren’t sufficiently high risk to meet thresholds and “unlock” service intervention, so continue to bounce around with the system.
The best point to engage with residents is in the immediate aftermath of demand rather than waiting for referrals and assessments to be made.
Intervention is often made at points of crisis, rather than taking the opportunity to intervene earlier. Therefore intervention is often focused on reducing risk – rather than meeting need.
Services are often configured to keep people out (very high thresholds) or move people through fast (addressing just the immediate demand rather than the root cause of the problem) – neither approach is in the best interest of residents.
Services aren’t always configured to offer help when needed or required – often the system works to our convenience. For example, many of the cases picked up involved people who work full time. We needed to visit after 6pm – but most of our services are closed by then.
Engaging with residents doesn’t necessarily need to be done by specialists in the first instance, linking to the Wigan Deal’s new conversation principles.

Age Well,
Integrated Health and Social Care

Integrated Neighbourhood Teams
Summary Integrated Neighbourhood Teams (INT) review and case manage suitable individuals that have a greater than 30% on the risk score, these multidiscipline teams decide on a course of action for each individual. This targeted approach will help the individual to manage their conditions and avert the need to access acute services in the future. This approach is supported by the avoiding unplanned admissions service across primary care.
What’s different?
Risk Stratification is being used to help to identify those at increasing risk of rehospitalisation within the next 12 months (Risk Score >30%).
Multidisciplinary teams from multiple organisations sit across three localities (Ashton, Leigh & Wigan), these meet on a monthly basis to discuss patients that have been referred in to INT and devise suitable course of action tailored to that individual.
Holistic packages of care which gives the individual to have a single contact rather than multiple. Drug and Alcohol partnership are now part of the INT’s with staff dedicated to each INT cluster these
individuals was previously being referred back to the GP. Integrated way of working has improved the patient journey helping to drive up the quality of care they
receive. GP practices are reviewing within primary care over 2% of the highest risk patients and providing additional
practice based care where appropriate Primary care link workers are working with patient requiring lower levels of support and case management.
Impact
1.4% of the population has been identified as eligible for active case management (risk score >=30%)
Since April 2103 there have been 7,833 case management plans put into place that are still active, of which 1,230 fall within the INT (the others fall under GPs and End of Life).
There have been significant reductions in secondary care activity for those receiving active case management (those identified >=30% RS). Between 2012/13 and 2014/15 there was reductions in A&E admissions (-52%), Inpatient NEL admissions (-63%), Inpatient admissions (-21%) and Outpatient admissions (-17%).
Active case management is contributing to reducing costly unscheduled admission in Wigan. The Borough of Wigan has a reducing trend of accident and emergency attendances and resultant hospital
admissions. The only borough in Greater Manchester to show a reduction for 2 years.
Locality Plan
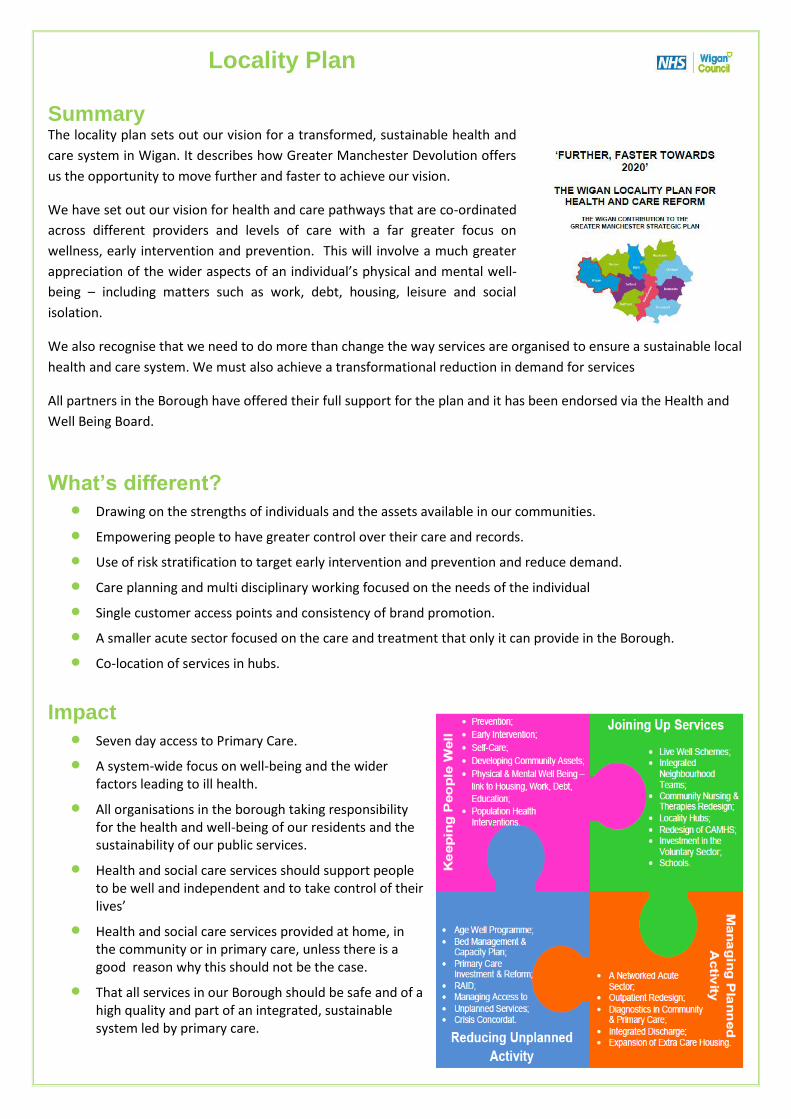
Summary The locality plan sets out our vision for a transformed, sustainable health and
care system in Wigan. It describes how Greater Manchester Devolution offers
us the opportunity to move further and faster to achieve our vision.
We have set out our vision for health and care pathways that are co-ordinated
across different providers and levels of care with a far greater focus on
wellness, early intervention and prevention. This will involve a much greater
appreciation of the wider aspects of an individual’s physical and mental well-
being – including matters such as work, debt, housing, leisure and social
isolation.
We also recognise that we need to do more than change the way services are organised to ensure a sustainable local
health and care system. We must also achieve a transformational reduction in demand for services
All partners in the Borough have offered their full support for the plan and it has been endorsed via the Health and
Well Being Board.
What’s different?
Drawing on the strengths of individuals and the assets available in our communities.
Empowering people to have greater control over their care and records.
Use of risk stratification to target early intervention and prevention and reduce demand.
Care planning and multi disciplinary working focused on the needs of the individual
Single customer access points and consistency of brand promotion.
A smaller acute sector focused on the care and treatment that only it can provide in the Borough.
Co-location of services in hubs.
Impact
Seven day access to Primary Care.
A system-wide focus on well-being and the wider factors leading to ill health.
All organisations in the borough taking responsibility for the health and well-being of our residents and the sustainability of our public services.
Health and social care services should support people to be well and independent and to take control of their lives’
Health and social care services provided at home, in the community or in primary care, unless there is a good reason why this should not be the case.
That all services in our Borough should be safe and of a high quality and part of an integrated, sustainable system led by primary care.

Wigan and Leigh Homes - Hospital Discharge Role
Summary Through joint working between the NHS Clinical Commissioning Group and Wigan Council a need was identified to establish an Integrated Hospital Discharge Team was needed to improve discharge arrangements from hospital. It has been identified that high costs to the public purse were incurred by individuals admitted to hospital being unable to return home either because their accommodation is unsuitable due to health or disability issues or because they have no permanent accommodation. To alleviate some of this pressure a Specialist Housing Advisor role was established, based within the hospital discharge team, with the main objective of developing a referral pathway between ward staff and Wigan Leigh Homes. The focus of the role is on early intervention at the point of admission instead of discharge and consequently to reduce the number of delayed discharges and the associated costs to the public purse. Due to its success a second role has been established to focus on individuals with complex multiple needs that frequently use hospital services inappropriately.
What’s different?
Improved information sharing with health service staff.
Advising customers on their housing rights and responsibilities.
Providing housing training for colleagues from other agencies.
Ability to access temporary accommodation in crisis.
Play a major part in the safeguarding of vulnerable adults.
Provide rapid responses to situations.
Access support for those individuals who may inappropriately use hospital services.
Identify housing solutions that meet patients’ needs.
Ensure the best use is made of the housing stock.
Impact
Due to the success of the original post agreement was given in September 2015 to fund an additional post until October 2015. Funding is now in place for both posts until April 2016.
Significant savings to public services across several performance measures including the cost of a bed within Wigan infirmary, cost of step-down bed (outside of Wigan Infirmary), bed days saved and the average number of bed days saved agreed at 5 days per case.
Since April 2015 until November 2015 a total saving of £136,750 has been made against two of the performance measures above; number of bed days saved (Infirmary) and number of step-down beds saved.
Officers have assisted a further 133 customers who required advice and assistance regarding their housing situation but which was not preventing their discharge from hospital.
Of the 133 cases, 58% were given advice and assistance, 11% were signposted to other services for additional support for long term sustainability, 11% were housed to alternative accommodation, 17% resulted in no further action and 3% of cases are on-going.

Enablers

Workforce Reform: The Deal Summary As an overarching approach to our transformation work, The Deal for Adult Social Care and Health has introduced new ways of working. Customers and citizens are viewed as unique individuals with assets, gifts and talents, rather than a collection of needs and deficits to be assessed. We support people to live the best life they can connecting to the capacity in their local communities, rather than fitting them into a prescriptive range of traditional and often more expensive services. The key pillars of the Deal are simple
“Different conversations” with residents to better understand individual assets, recognising strengths, gifts and talents.
“Know your community” to respond to needs.
What’s different?
Connecting people with community solutions for example a local community hub, social group or buddy Developing community capacity through co production, different relationships and asset transfer.
Staff are provided with the time and skills required to explore issues and gain a greater insight into what would make a difference to service user’s lives.
The approach has enhanced the awareness from staff of what is available within the community to support the move away from traditional support services and aids more effective early intervention.
By enabling a greater focus holistically on the individual has provided greater opportunity to support both the service user and their carer.
Set piece training is a key component of the approach to ensure that all staff receive consistent information and understand the core principles, and acts as a ‘rite of passage’. A further version of the training, tailored to the frontline provider workforce is currently being rolled out.
Impact
Over 800 staff trained in the new approach, including staff from key partners such as Bridgewater and WWL as well as neighbouring authorities.
The training has been very positively received and has gained significant interest across a wide range of local and GM public service partner organisations, and has also attracted national interest as a contemporary way of working relevant to public service reform.
The approach is being used to fundamentally refocus the way services are commissioned. A Deal for providers has been developed that is a partnership with ethical and high quality providers together with robust quality assurance based on customer experience.
Over 100 referrals being received through the Community Knowledge Inbox per month. Successful Community Link Worker Trial resulting in funding being obtained from to further trial the
approach with primary care. Adult Social Care and Health as the largest single budget area has absorbed a large share of the Council’s
saving requirements with over £25m successfully reduced from the budget since 2011/12. A fundamental review of day services resulting in closing 10 tired and costly day centres and moving to
provision that meets the needs of those service users with complex needs whilst helping to develop a market that encourages independence and greater choice and control by the individual.
Spatial Planning
Summary Partners in Wigan have been working hard together to redesign public services so that we can reduce (or re-profile) increasing levels of demand on local public services, meet our significant budget reduction requirements and improve the offer and outcomes for local people from our services. The need to have a common vocabulary and shared understanding across partners in local public services of the different levels of spatial planning across the borough is becoming more acute as we progress on our journey of reform.
What’s different?
A move away from building based services to a flexible delivery in the community.
Providing integrated services wrapped around individuals and families, the days
Providing integrated services wrapped around individuals and families, the days of different public services offering elements of support for elements of residents’ lives from different buildings are over.
A new deliver model with partners and communities, with an asset based approach at the heart.
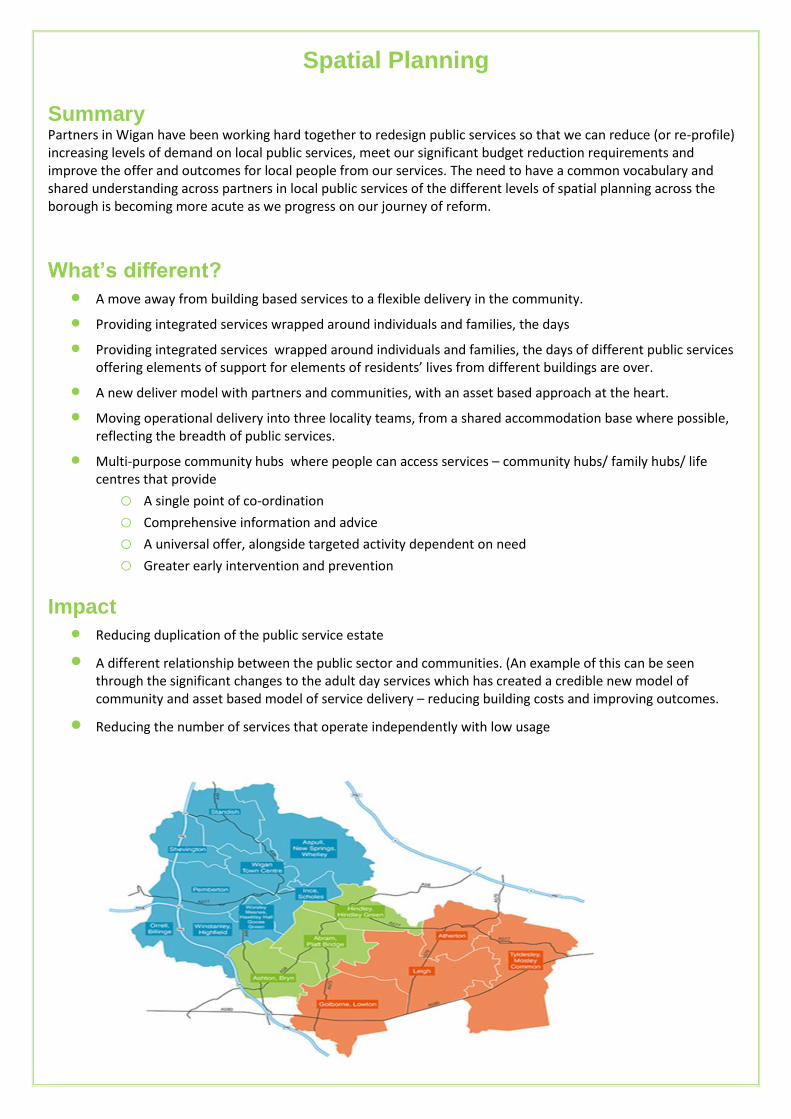
Moving operational delivery into three locality teams, from a shared accommodation base where possible, reflecting the breadth of public services.
Multi-purpose community hubs where people can access services – community hubs/ family hubs/ life centres that provide o A single point of co-ordination o Comprehensive information and advice o A universal offer, alongside targeted activity dependent on need o Greater early intervention and prevention
Impact
Reducing duplication of the public service estate
A different relationship between the public sector and communities. (An example of this can be seen through the significant changes to the adult day services which has created a credible new model of community and asset based model of service delivery – reducing building costs and improving outcomes.
Reducing the number of services that operate independently with low usage