Embed Size (px)
Citation preview
.) . . . . Rural Cross Roads . . . . .
1 Protecting Rural Communities From . @ 4
Terrorism: A Statewide, Community-based Model
A r t Clawson, MS, and Robert G Brooks, MD
ABSTRACT: Given the number of Americans who live in rural areas and the unique challenges they face in the provision of health care services, special attention to planning for and responding to terrorist acts is warranted. After September 11, 2001, Florida developed a statewide, community-based model that applies the public health principles of assessment, policy developmmf, and assur- ance. This model can serve as a possible framework for other states and communities.
There is perhaps no duty more fundamental to American government than the protection of the public’s health, safety, and welfare *
he tragic events of September 11, 2001, have captured the public’s attention and raised awareness of how critical it is for our nation, health care organizations, and public health agencies to be prepared and ready to respond
to terrorist acts Given the number of Americans (65 million) who live in rural locations, many of whom are in close proximity to potential military or economic terrorist targets, it is critical to consider the current status of preparedness in rural areas and to develop plans at the state and local level to ensure the readiness and response of the health systems in these areas The limited health infrastructure and fewer numbers of providers in rural communities make them more vulnerable and less able to respond Surveys of antiterrorist preparedness clearly reflect rural/urban differences, with at least two recent studies showing marked differences between rural and urban hospitals in their preparedness for terrorist acts 3,4 In a study from the northwest United States, for instance, Wetter and colleagues3 found that only 20% of all hospitals had a response plan for incidents involving biological or chemical weapons, with rural hospitals only one third as likely as urban sites to have such capacity A lack of available resources in rural areas could compromise rural readiness and the ability to respond to future events Additionally, a terrorist event in an urban area
T
might result in a mass exodus to a rural area, overwhelming the rural providers with fleeing sick and contaminated individuals The critical importance for effective emergency preparedness in rural areas led U S Health and Human Services Secretary Tommy Thomp- son to include the State Offices of Rural Health as essential partners in the development of state bioter- rorism plans Like many states, Florida is a target-rich environment for any type of terrorist attack or incident Florida has a large number of tourists (over 40 million annually), many seasonal residents, and a growing permanent population of over 16 million Florida is home to Disneyworld and other large theme attractions, collegiate and professional sports, several deepwater ports, large cities, and a handful of military installa- tions In this paper we present a statewide, community- based model developed in Florida since the events of 9- 11 that can serve as a possible framework for other states and communities
Emergenc y Response Structure Prior to September 11, 2001
Prior to September 11,2001, the Florida Department of Health (FDOH) and the Florida Department of Community Affairs’ Division of Emergency Manage- ment (FDEM) had in place a variety of systems and processes that supported traditional disaster prepared- ness and response in Florida’s 33 rural and 34 urban counties These systems had been sharpened and honed in the previous 10 years, beginning with the devastation in southem Florida caused by Humcane Andrew The FDEM is responsible for the coordination of emergency management and response across federal, state, and county agencies The FDEM also coordinates training, exercises, and response planning at the state and local levels to ensure that emergency responders in rural and urban counties are prepared when a disaster strikes The State Emergency Operations Center (EOC) in
For further information, contact: A r t Clawson, director of health affairs, Florida State University, College of Medicine, Tallahassee, FL 32306-4300; e-mail A r t ClawsonQmed fsu edu
winter 2003 Clawson and Brooks 7
Rural Cross Roads
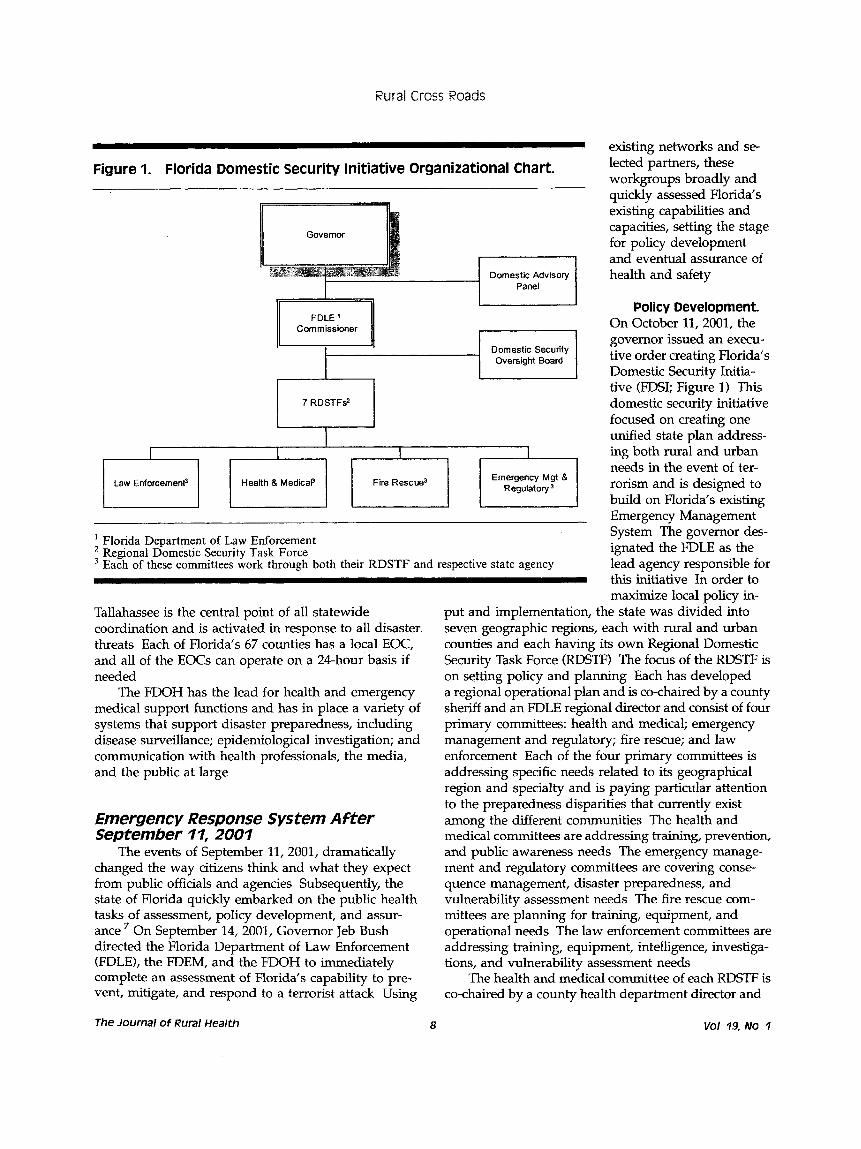
Law Enforcemenp Emergency M g t 8 Regulatory Health & MedicaP Fire Rescue3
' Florida Department of Law Enforcement Regional Domestic Security Task Force Each of these committees work through both their RDSTF and respective state agency
Tallahassee is the central point of all statewide coordination and is activated in response to all disaster threats Each of Florida's 67 counties has a local EOC, and all of the EOCs can operate on a 24-hour basis if needed
The FDOH has the lead for health and emergency medical support functions and has in place a variety of systems that support disaster preparedness, including disease surveillance; epidemiological investigation; and communication with health professionals, the media, and the public at large
Emergency Response System After September 11, 2001
The events of September 11,2001, dramatically changed the way citizens think and what they expect from public officials and agencies Subsequently, the state of Florida quickly embarked on the public health tasks of assessment, policy development, and assur- ance On September 14,2001, Governor Jeb Bush directed the Florida Department of Law Enforcement (FDLE), the FDEM, and the FDOH to immediately complete an assessment of Florida's capability to pre- vent, mitigate, and respond to a terrorist attack Using
The Journal of Rural Health 8
existing networks and se- lected partners, these workgroups broadly and quickly assessed Florida's existing capabilities and capacities, setting the stage for policy development and eventual assurance of health and safety
Policy Development On October 11,2001, the governor issued an execu- tive order creating Florida's Domestic Security Initia- tive (FDSI; Figure l) Thys domestic security initiative focused on creating one unified state plan address- ing both rural and urban needs in the event of ter- rorism and is designed to build on Florida's existing Emergency Management System The governor des- ignated the FDLE as the lead agency responsible for this initiative In order to maximize local policy in-
put and implementation, the state was divided h to seven geographic regions, each with rural and urban counties and each having its own Regional Domestic Security Task Force (RDSTF) The focus of the RDSn is on setting policy and planning Each has developed a regional operational plan and is co-chaired by a county sheriff and an FDLE regional director and consist of faur primary committees: health and medical; emergency management and regulatory; fire rescue; and law enforcement Each of the four primary committees is addressing specific needs related to its geographical region and specialty and is paying particular attention to the preparedness disparities that currently exist among the different communities The health and medical committees are addressing training, prevention, and public awareness needs The emergency manage- ment and regulatory committees are covering come- quence management, disaster preparedness, and vulnerability assessment needs The fire rescue com- mittees are planning for training, equipment, and operational needs The law enforcement committees are addressing training, equipment, intelligence, inves tiga- tions, and vulnerability assessment needs
The health and medical committee of each RDSTF is co-chaired by a county health department director and

Rural Cross Roads
a hospital chief executive officer (CEO) and includes representation from rural healthcare facilities and or- ganizations within each of the regions These groups meet monthly and make recommendations to the newly created Office of Public Health Preparedness (OPHP) in the FDOH These seven RDSTFs work closely with local agencies and organizations to address their domestic security needs and initiatives to ensure a coordinated statewide approach The FDOH is committed to making certain that hospitals, first responders, and health professionals in all 67 counties reach certain core levels of capability, regardless of their population size At the center of this commitment is the idea that no region gets left behind For example, all caches of personal protection equipment allocated for hospitals will be distributed proportionately to each region based on the number of hospitals within each region, regardless of size
Assessment. Much of the assessment of readiness capabihties has come from the regional health and medical committees Their assessment included a com- prehensive survey of the health care industry in their respective regions and identified and prioritized a range of preparedness issues to be addressed The survey included demographic data by county, key impacts within each region, and a regional budget to address each area of concern The information gathered was reported by each county in each region The pre- paredness needs of each region were reported in the following categories: regional preparedness (general requirements); hospital/ physician preparedness needs; laboratory preparedness needs; pharmaceutical pre- paredness needs; health department preparedness needs; and EMS preparedness needs These recommen- dations focused on the training, equipment, supplies, personnel, and facilities needs within each region’s rural and urban areas For example, Florida’s health and emergency management organizations are trained for mass-casualty events related to hurricanes and fires Traditional disaster training needs to be expanded to include bioterrorist agents and epidemic and contagious disease precautions/protocols, from identification to treatment The audience for training ranges from specific health professionals to the general public
Despite the presence of standards through the FDOH and FDLE, the assessment data indicated wide variations in the availability, type, specification, and standards in several key areas of preparedness The state EMS system, for instance, would be challenged to manage an extremely large number of people requiring decontam- ination from chemical exposure Since EMS providers in rural communities often perform decontamination, a greater concern may be those victims (up to 80%) who reach the hospital without accessing the EMS system
In a report published prior to last year‘s terrorist events, the American Hospital Association concluded that mass casualties would generally overwhelm the capacity of hospitals and the health care system in our country Florida‘s survey also showed a significant variation in the capacity and capability of hospitals to effectively provide quarantine, isolation, and decon- tamination services Many of the facilities surveyed indicated that a major obstacle to providing these services is lack of funding to make the capital improve- ments necessary to keep the facilities and equipment current This is particularly true for the rural facilities that have historically been underfunded In addition, tourism peaks and rapid urban population growth have created overcrowding, diversion, and continuing capac- ity constraints that will require alternate site plans for response to a mass-casualty event The RDSTFs have identified a primary hospital and secondary hospitals for each region The integrated approach to the development and implementation of regional hospital plans for mass- casualty events includes hospital bed capacity, isolation and quarantine, overcrowding and diversion, equipment management, special needs patients, essential goods and services, security, and medical waste The flexibility for expanding bed capacity includes the use of available civilian, VA, and military hospital capacity; quick conversions of alternative sites; set-up of alternative sites in underserved rural areas; and the integration of support services from other disaster management agencies Florida’s survey has shown that undercapital- ized rural and small hospitals have the greatest needs Both of the committees advising the OPHP have recommended that allocation of funds received for hospitals be distributed based on number of hospitals in each region, regardless of their size, rather than a population-based formula
Florida, like other states, is experiencing staffing shortages among essential care providers The number of health professionals in the state’s rural areas is limited and the possibility of their exposure to a biological agent prior to its identification is high This exposure could incapacitate them, leaving rural communities without immediate health care treatment and urban communities without alternative backup support Plans are being developed to capitalize on retired/volunteer healthcare professionals by identifying, training, and preparing them for rapid deployment
Finally, the level of supplies, drugs, and emergency procedures varies widely across the state and facilities Through the RDSTFs, current programs are developing an integrated approach to site-specific, local, regional, state, and federal stockpiles for responders and victims
Winter 2003 Cla wSOn and Brooks 9

Rural Cross Roads
Assurance. The Executive Order of October 2001 also spelled out the duties and composition of a Do- mestic Security Oversight Board and a Domestic Secu- rity Advisory Panel (Figure 1) The Oversight Board is responsible for the policies of the seven RDSTFs This statewide board ensures consistency, communication, and accountability; sets benchmarks and monitors progress; identifies common protocols and needs; and ensures that all levels of government (federal, state, and local) work in concert The Domestic Security Advisory Panel is charged with providing advisory assistance to the governor, the legislature, and the chief of domestic security; providing and evaluating recommendations to combat terrorism in Florida; and serving as a liaison between the governor, the legislature, and the chief of domestic security
The secretary of the FDOH also created the OPHP, which is responsible for the statewide coordination of the planning done by the seven health and medical committees of the RDSTF and for the distribution of all federal and state funds related to their recommenda- tions The OPHD is supported by the Advisory Committee for Public Health Preparedness and Re- sponse on Biotemorism (CPHPR) and the Hospital Bioterrorism Preparedness Planning Committee (HBPPC) The membership of these committees is as diverse as the health care industry in Florida, repre- senting both rural and urban providers and communi- ties The CPHPR assists the OPHP in identifymg, assessing, and prioritizing resources needed to respond as detailed in the Centers for Disease Control (CDC) Cooperative Agreement The HBPPC provides direction to the OPHP for the ongoing program and meets regularly to review and assess program initiatives and make funding recommendations
Adequate funding is critical to any assurance effort. Florida is eligible to receive $47 1 million from the federal government through CDC and HRSA grants to address bioterrorism The Department of Justice (DOJ) is providing approximately $9 million of additional funding with about $1 7 million to help equip hospitals in seven regions, the state laboratories, and a number of EMS services Additionally, the FDOH has a long-established EMS grants program with at least 10% of the annual funding specifically reserved for rural communities Key health partners involved in the process to idenbfy priority areas for funding include the RDSTF health and medical committees, the CPHPR and HBPPC advisory com- mittees , all 67 County Health Department directors (33 of the 67 CHD directors are in designated rural counties), the FDOH-appropriate rural staff, hospitals, and health organizations
Conclusion Florida has made sigruficant progress toward ad-
dressing domestic security issues by fully utilizing the defined core functions (assessment, policy development, and assurance) of public health agencies and continuing to involve essential groups in reviewing and making policy recommendations But there are still some poten- tial barriers that will need to be addressed The national public health infrastructure, which frequently has been a low priority for funding and has been steadily declining for years, has become a high priority and is being bet&r funded, but there is a real concern regarding how long this momentum will last if the prevention of terrorist activity loses the public’s interest and support The m a 1 health infrastructure, already strained through years of underfunding and demands placed on it, requires ongoing, dedicated funding if there is to be a rural safety net With the needs in all communities surpassing the current funds available, there is concern that the rural communities will continue to be overshadowed by the nonrural communities
FDSI, a statewide community-based model, offm other states a possible integrated framework to address both rural and urban concerns As our nation addresses for the first time terrorist acts on our home soil, we have a unique opportunity to not only advocate for long- needed rural public health resources,1o but to improwe dialogue and collaboration among the states to devdop the most comprehensive system of care our country has ever known
References 1
2
3
4
5
6
7
8
9
10
Hodge JG Jr Bioterrorism law and policy: critical choices in putblic health J Law Med Ethics 200230254-261 OLeary DS JCAHOs president testifies at Congressional bia- terrorism hearings Joint Comm Perspect 2001;21(12) Wetter DC, Daniel1 WE, Treser CD Hospital preparedness for victims of chemical or biological terrorism A m J Public Health
Treat KN, Williams JM, Furbee PM, Manley WG, Russell FK, Stamper CD Jr Hospital preparedness for weapons of mass destruction incidents: an initial assessment Ann Emerg Med
Office of Rural Health Policy Rural Communities and Emergency Preparedness Rockville, Md: Health Resources and Services Administration, US Dept of Health and Human Services; 2 W Florida Department of Health Domestic Security in Florida May 2002 Institute of Medicine committee for the Study of the Future of Public Health The Future of Public Health Washington, DC: National Academy Press; 1988 Bentley JD Hospital preparedness for bioterrorism Public Hmkh
Florida Hospital Association FZoridaS Domestic Security Initintiws March 2002 Snider LB, Bellamy GR Unique advocacy opportunities for m a 1 preparedness public health agencies J Rural Health 2002;18:
2001;91:710-716
2001;38:562-565
Rep 2001;116(~~~~1):36-39
388-390
The JOUrrIal of Rural Health 10 VOl 19, NO 1





























