Embed Size (px)
DESCRIPTION
Protocol Representation Model (PRM) in the Real World. Richard Young | Director, EMEA Monday, 17 th December, 2012. Per Patient Costs – USD ($). Pharmalot , reporting data from Cutting Edge Informatics, 26 Jul 2011. Challenges of Clinical Development. - PowerPoint PPT Presentation
Citation preview

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 1Optimizing Clinical Trials: Concept to Conclusion TM
Optimizing Clinical Trials:Concept to Conclusion™
Protocol Representation Model (PRM) in the Real World
Richard Young | Director, EMEAMonday, 17th December, 2012

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 2Optimizing Clinical Trials: Concept to Conclusion TM
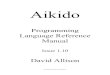
Per Patient Costs – USD ($)
Phase I Phase II Phase IIIa Phase IIIb Phase IV05,000
10,00015,00020,00025,00030,00035,00040,00045,00050,000
20082011
Pharmalot, reporting data from Cutting Edge Informatics, 26 Jul 2011

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 3Optimizing Clinical Trials: Concept to Conclusion TM 3© 2011 Medidata Solutions, Inc.
Challenges of Clinical DevelopmentIncreasingly
complex trials and trial design
Explosion of analytics and data related to trials
Increasing difficulty recruiting patients
Many processes continue to be siloed, manual or inefficient
Low visibility for performance management Growing importance of
emerging markets
High risks, delayed approvals, delayed
revenue
Struggle to adapt to emerging world of genomic-based drugs

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 4Optimizing Clinical Trials: Concept to Conclusion TM
From Data to IntelligenceConfidence in DECISION
Time / ResourceRAW Data
CLEAN Data
Standard Reports
Ad hoc Reports
What Happened ?
Why ?
What Will Happen ?
Best Outcome ?
EXPLORE
PREDICT
OPTIMISE
DATA INFORMATION KNOWLEDGE INTELLIGENCE

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 5Optimizing Clinical Trials: Concept to Conclusion TM 5© 2011 Medidata Solutions, Inc.
Protocol Representation Model• CDISC has a standard model for the protocol
• Protocol Representation Model (PRM)• The PRM was developed to
• Support the generation of a protocol document, • Support research study (clinical trial) registration and tracking, • Support regulatory needs, • Facilitate single-sourced, downstream electronic consumption
of the protocol content• In SIMPLE terms, PRM enables us to
• Define the core clinical components• Define the relationship between the components

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 6Optimizing Clinical Trials: Concept to Conclusion TM 6© 2011 Medidata Solutions, Inc.
class P...
Product
+ typeCode: CD+ classCode: SET <CD>+ pre1938Indicator: BL+ expirationDate: TS::Material+ identi fi er: SET <II>+ name: SET<TN>+ description: ST+ formCode: CD+ statusCode: CD+ statusDateRange: IVL<T S>
Drug
+ lotNumberText: ST+ strength: RTO<PQ,PQ>+ activeIngredientInd icator: BL::Product+ typeCode: CD+ classCode: SET<CD>+ pre1938Indi cator: BL+ expirati onDate : TS::Material+ identi fier: SET<II>+ name: SET <T N>+ description: ST+ formCode: CD+ statusCode: CD+ statusDateRange: IVL<TS>
Device
+ reprocessedDeviceCode: CD+ avai lableForEvaluat ionIndicator: BL+ overTheCounterProductIndicator: BL+ si ng leUseDeviceIndi cator: BL+ deviceAge: PQ+ manufactureDate: TS::Product+ typeCode: CD+ classCode: SET <CD>+ pre1938Indicator: BL+ expirationDate : TS::Material+ identifier: SET<II>+ name: SET<TN>+ description: ST+ formCode: CD+ statusCode: CD+ statusDateRange: IVL<T S>
StudyAgent
+ leadAgentIndicator: BL+ comparatorIndi cator: BL+ statusCode: CD+ statusDateRange: IVL<TS>
TherapeuticAgent
+ identifier: II+ statusCode: CD+ statusDateRange: IVL<T S>
RegulatedProduct
+ approvalIdenti fier: SET<II>+ authori zationTypeCode: CD+ approvalStatusCode: CD+ expandedAccessStatusCode: CD
NonTherapeuticAgent
Biologic
+ lotNumberT ext: ST+ strength: RT O<PQ,PQ>::Product+ typeCode: CD+ classCode : SET <CD>+ pre1938Indicator: BL+ expirationDate: TS::Material+ identifier: SET<II>+ name: SET<TN>+ description: ST+ formCode: CD+ statusCode: CD+ statusDateRange: IVL<T S>
RegulatoryApplica tionSponsor
+ statusCode: CD+ statusDateRange: IVL<TS>
RegulatoryApplication
+ identifier: II+ typeCode: CD
RegulatoryAuthority
+ jurisdi ctionCode: CD+ statusCode: CD+ statusDateRange: IVL<TS>
Submission
+ typeCode: CD+ receiptDate: TS+ regulatoryAssessmentCode: CD+ assessmentDateRange: IVL<T S>
SubmissionUnit
+ typeCode: CD+ seri al NumberT ext: ST+ receiptDate: TS+ statusCode: CD+ statusDateRange: IVL<TS>
«StudyRel ationship»SubmissionUnitRelationship
Document
+ pub licTit le: ST+ offi cialTi tle: ST+ typeCode : CD+ pub licDescription: ST+ scientif icDescripti on: ST+ keywordCode: SET<CD>+ keywordText: SET<ST >+ text: ST+ revisionText: ST+ uni versal ResourceLocator: URL+ bibl iographicDesignat ion: ST+ languageCode: CD
StudyProtocol
+ acronym: ST+ phaseCode: CD+ diseaseCode: SET<CD>+ targetAnatomi cSiteCode: CD+ primaryPurposeCode: CD+ purposeStatement: ST+ designConfigurationCode: CD+ studySchematic: ED+ allocationCode: CD+ confi dential i tyCode: CD+ populationDescription: ST+ subjectT ypeCode: CD+ plannedStudySubjectExperience: ST+ acceptsHealthyVolunteersIndicator: BL+ targetAccrualNumberRange: IVL<INT>+ periodicT argetAccrualNumber: RT O<INT ,PQ>+ accrualReportingMethodCode: CD+ responsiblePartyCode: CD+/ multi InstitutionIndicator: BL+ participatingOrganizationTypeCode: CD+ participatingCountryCode: SET <CD>+ AECodingSystem: CD::Document+ publicTitl e: ST+ offici alTit le: ST+ typeCode: CD+ publicDescription: ST+ scientificDescription: ST+ keywordCode: SET<CD>+ keywordText: SET<ST>+ text: ST+ revisionText: ST+ universalResourceLocator: URL+ bibl iographicDesignation: ST+ languageCode: CD
«StudyRelationship»DocumentRelationship
OversightAuthority
Organization
+ identifier: SET<II>+ name: SET<ON>+ typeCode: CD+ description: ST+ postalAddress: AD+ tel ecomAddress: SET <T EL>+ statusCode: CD+ statusDateRange: IVL<T S>
OversightCommittee
+ typeCode: CD+ statusCode: CD+ statusDateRange: IVL<TS>
StudySite
+ identi fier: II+ leadOrganizat ionIndicator: BL+ reviewBoardApprovalNumberText: ST+ reviewBoardApprovalStatusCode: CD+ reviewBoardApprovalDate: TS+ targetAccrual Number: INT+ accrualStatusCode: CD+ accrualStatusDate: T S+ dateRange : IVL<TS>+ statusCode: CD+ statusDateRange: IVL<TS>
DocumentIdentification
+ identi fier: II+ primaryIndicator: BL+ typeCode: CD+ assi gnedDate: TS
«StudyRelationship»DocumentIdentificationRelationship
StudyOversightAuthority
Registry
+ name: ST+ acronym: ST
Activity
+ ident ifi er: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
Arm
+ name: ST+ typeCode: CD+ description: ST+ randomizationWeightText: ST
ExpandedAccessStudyProtocol
::StudyProtocol+ acronym: ST+ phaseCode: CD+ diseaseCode: SET<CD>+ targetAnatomi cSiteCode: CD+ primaryPurposeCode: CD+ purposeStatement: ST+ designConfigurationCode: CD+ studySchematic: ED+ al locationCode: CD+ confi dential ityCode: CD+ populationDescription: ST+ subjectT ypeCode: CD+ plannedStudySubjectExperience: ST+ acceptsHealthyVolunteersIndicator: BL+ targetAccrual NumberRange: IVL<INT>+ peri odicT argetAccrualNumber: RT O<INT,PQ>+ accrualReportingMethodCode: CD+ responsiblePartyCode: CD+/ mul ti Inst itutionIndicator: BL+ part icipatingOrganizationTypeCode: CD+ part icipatingCountryCode: SET <CD>+ AECodingSystem: CD::Document+ publicTitl e: ST+ offici alTit le: ST+ typeCode: CD+ publicDescription: ST+ scientificDescription: ST+ keywordCode: SET<CD>+ keywordT ext: SET <ST>+ text: ST+ revisionText: ST+ universalResourceLocator: URL+ bibl iographicDesignati on : ST+ languageCode: CD
InterventionalStudyProtocol
+ numberOfIntervent ionGroups: INT+ interventi onDescri pt ion: ST+ controlT ype: CD+ controlConcurrencyT ype: CD+ al locati onCode: CD+ bl indi ngSchemaCode: CD+ bl indedRoleCode: SET<CD>::StudyProtocol+ acronym: ST+ phaseCode: CD+ diseaseCode: SET<CD>+ targetAnatomicSiteCode: CD+ primaryPurposeCode: CD+ purposeStatement: ST+ designConfigurationCode: CD+ studySchematic: ED+ al locati onCode: CD+ confident ial ityCode: CD+ popul ationDescript ion: ST+ subjectT ypeCode: CD+ plannedStudySubj ectExperi ence: ST+ acceptsHeal thyVolunteersIndicator: BL+ targetAccrual NumberRange: IVL<INT>+ peri odicTargetAccrualNumber: RTO<INT,PQ>+ accrualReportingMethodCode: CD+ responsiblePartyCode: CD+/ mul tiInst itutionIndi cator: BL+ part icipat ingOrganizationT ypeCode: CD+ part icipat ingCountryCode: SET<CD>+ AECodingSystem: CD::Document+ publicTitle: ST+ officialT itle: ST+ typeCode: CD+ publicDescri pt ion: ST+ scient ificDescription: ST+ keywordCode: SET <CD>+ keywordT ext: SET <ST>+ text: ST+ revisionText: ST+ universalResourceLocator: URL+ bibl iographi cDesignati on: ST+ languageCode: CD
Material
+ identifier: SET<II>+ name: SET<TN>+ descripti on: ST+ formCode: CD+ statusCode: CD+ statusDateRange: IVL<T S>
Observ ationalStudyProtocol
+ samplingMethodCode: CD+ timePerspectiveCode: CD::StudyProtocol+ acronym: ST+ phaseCode: CD+ diseaseCode: SET<CD>+ targetAnatomicSiteCode: CD+ primaryPurposeCode: CD+ purposeStatement: ST+ designConfigurationCode: CD+ studySchematic: ED+ al locati onCode: CD+ confidential ityCode: CD+ populationDescri pt ion: ST+ subjectT ypeCode: CD+ plannedStudySubj ectExperi ence: ST+ acceptsHeal thyVolunteersIndicator: BL+ targetAccrual NumberRange: IVL<INT>+ peri odicTargetAccrualNumber: RTO<INT,PQ>+ accrualReportingMethodCode: CD+ responsiblePartyCode: CD+/ mul ti Inst itutionIndi cator: BL+ part icipatingOrganizationT ypeCode: CD+ part icipatingCountryCode: SET <CD>+ AECodingSystem: CD::Document+ publicTitle: ST+ officialT itle: ST+ typeCode: CD+ publicDescri ption: ST+ scientificDescription: ST+ keywordCode: SET <CD>+ keywordT ext: SET <ST>+ text: ST+ revisionText: ST+ universalResourceLocator: URL+ bibl iographi cDesignati on: ST+ languageCode: CD
OrganizationalContact
+ typeCode: SET<CD>+ pri maryIndicator: BL+ postalAddress: AD+ tel ecomAddress: SET <T EL>+ statusCode: CD+ statusDateRange: IVL<T S>
PerformedActiv ity
+ actualDateRange: IVL<TS>+ actualDuration: PQ+ effectiveDateRange: IVL<T S>+ effectiveDuration: PQ+ mi ssedInd icator: BL+ mi ssedReason: SET<SC>+ delayDuration: PQ::Activi ty+ identifier: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<T S>+ comment: ST
PerformedAdministrativeActiv ity
+ varianceReason: ST::PerformedActivity+ actualDateRange: IVL<TS>+ actualDuration: PQ+ effectiveDateRange: IVL<TS>+ effectiveDuration: PQ+ missedIndicator: BL+ missedReason: SET<SC>+ delayDuration: PQ::Activi ty+ identi fier: II+ nameCode: CD+ textDescri ption: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
Person
+ name: PN+ initi al s: ST+ postalAddress: AD+ telecomAddress: SET<TEL>+ educationLevelCode: CD+ academicDegree: SET <CD>+ ethnicGroupCode: SET<CD>+ raceCode: SET <CD>+ maritalStatusCode: CD+ primaryOccupationCode: CD+ occupationDateRange: IVL<TS>+ dea thIndicator: BL+ statusCode: CD+ statusDateRange: IVL<TS>::Biologi cEntity+ sexCode: CD+ birthOrder: INT+ birthCountryCode: CD+ birthDate: TS+ dea thDate: TS
BiologicEntity
+ sexCode: CD+ birthOrder: INT+ birthCountryCode: CD+ birthDate: TS+ deathDate: T S
PlannedArm
+ targetAccrualNumber: INT::Arm+ name: ST+ typeCode: CD+ description: ST+ randomizationWeightT ext: ST
PlannedEligibilityCriterion
+ cri terionName: ST+ requiredResponse: ST+ value: ST+ cri terionCode: CD+ operator: ST+ displayOrder: INT::PlannedActivi ty+ name: SET <ST>+ actualIndicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPlannedActivi tyT ypeCode: CD+ additionalDurationDescripti on: ST+ plannedRangeOfRepetit ionsText: ST::Activi ty+ identi fier: II+ nameCode: CD+ textDescripti on : ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
PlannedObserv ation
::PlannedActivi ty+ name: SET<ST >+ actualIndicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPlannedActivityT ypeCode: CD+ additionalDurationDescription: ST+ plannedRangeOfRepeti tionsText: ST::Activi ty+ identi fi er: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET <CD>+ statusCode: CD+ statusDateRange: IVL<T S>+ comment: ST
PlannedActivity
+ name: SET<ST>+ actualIndicator: BL+ con tingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPlannedActivi tyTypeCode: CD+ additionalDurationDescription: ST+ plannedRangeOfRepetitionsT ext: ST::Activi ty+ identi fier: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
PlannedAdministrativeActiv ity
::PlannedAct ivi ty+ name: SET<ST >+ actualIndicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPlannedAct ivityT ypeCode: CD+ additionalDurationDescri ption: ST+ plannedRangeOfRepeti tionsText: ST::Activity+ identi fi er: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET <CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
StudyLegalSponsor
+ primaryIndicator: BL
LegalSponsor
StudyReference
+ medlineIdenti fierNumber: INT+ citationDescription: ST+ l inkPageDescript ion: ST+ universalResourceLocator: URL+ resultReferenceIndicator: BL
StudyResourcing
+ activeIndicator: BL+ inactiveComment: ST
StudySiteContact
+ roleCode: CD+ primaryIndicator: BL+ postal Address: AD+ telecomAddress: SET<TEL>+ statusCode: CD+ statusDateRange: IVL<TS>
StudySiteInvestigator
::StudySiteContact+ roleCode: CD+ primaryIndicator: BL+ postalAddress: AD+ telecomAddress: SET<TEL>+ statusCode: CD+ statusDateRange: IVL<TS>
StudyOutcomeMeasure
+ name: ST+ typeCode: SET <CD>+ primaryIndicator: BL+ timeFrameText: ST
StudyObjective
+ description: ST+ primaryIndicator: BL
StudyOverallStatus
+ statusCode: CD+ statusDate: TS+ anticipatedIndi cator: BL+ studyStoppedReasonCode: CD+ comment: ST
StudyRecruitmentStatus
+ statusCode: CD+ statusDate: TS
View Description:This View represents the core aspects of a protocol itself, the people, organizations and the roles they may play in the con text of a study.
HL7 RIM Entity
HL7 RIM Role
HL7 RIM Participati on
HL7 RIM Act
HL7 RIM ActRel ationship
Placeholder
Draft
Legend
IdentifiedBiologicEntity
+ identi fier: II+ typeCode: CD+ statusCode: CD+ statusDateRange: IVL<TS>
ClinicalResearchStaff
+ postal Address: AD+ telecomAddress: SET<TEL>+ statusCode: CD+ statusDateRange: IVL<TS>
HealthCareProvider
+ identi fi er: II+ certi ficateLi censeT ext: ST+ postal Address: AD+ telecomAddress: SET<TEL>+ statusCode: CD+ statusDateRange: IVL<TS>
HealthCareFacility
+ identi fier: II+ postalAddress: AD+ statusCode: CD+ statusDateRange: IVL<TS>
ResearchOrganization
+ typeCode: CD+ statusCode: CD+ statusDateRange: IVL<TS>
ResourceProv ider
+ identi fier: I I+ statusCode: CD+ statusDateRange: IVL<TS>
StudyResourceProv ider
+ primaryIndicator: BL
IdentifierAssigner
PlannedExclusionCriterion
::PlannedEligibi l ityCriterion+ cri terionName: ST+ requiredResponse: ST+ value: ST+ cri terionCode: CD+ operator: ST+ displayOrder: INT::PlannedActivi ty+ name: SET <ST>+ actualIndicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPlannedActivi tyTypeCode: CD+ additionalDurationDescription: ST+ plannedRangeOfRepeti ti onsText: ST::Activi ty+ identifier: II+ nameCode: CD+ textDescripti on : ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
PlannedInclusionCriterion
::PlannedEl igibili tyCriterion+ cri terionName: ST+ requiredResponse: ST+ value: ST+ cri terionCode: CD+ operator: ST+ displayOrder: INT::PlannedAct ivi ty+ name: SET<ST >+ actual Indicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPl annedAct ivi tyT ypeCode: CD+ additionalDurationDescription: ST+ plannedRangeOfRepetitionsText: ST::Activity+ identi fier: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<T S>+ comment: ST
StudyRelationship
+ typeCode: CD+ inversionIndicator: BL+ contextControlCode: CD+ contextConductionIndicator: BL+ sequenceNumber: INT+ priori tyNumber: INT+ pauseQuanti ty: PQ+ checkpointCode: CD+ spli tCode: CD+ joinCode: CD+ negationIndicator: BL+ conjunctionCode: CD+ separableIndicator: BL+ subsetCode: CS+ uncertaintyCode: CD+ description: ST+ probabil i ty: REAL+ evaluableExpressionCode: CD+ comment: ST
PlannedProcedure
+ methodCode: CD+ approachSiteCode: CD+ targetSiteCode: CD+ targetSiteCondit ionCode: CD::PlannedAct ivi ty+ name: SET<ST >+ actual Indicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPl annedAct ivi tyT ypeCode: CD+ additionalDurationDescription: ST+ plannedRangeOfRepeti tionsText: ST::Activity+ identi fi er: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<T S>+ comment: ST
PlannedSubstanceAdministration
+ dose: PQ+ doseDescription: ST+ doseFrequencyCode: CD+ doseRegimen: ST+ doseFormCode: CD+ doseTotal: PQ+ routeOfAdministrat ionCode: CD+ locationOfDoseAdmi nistra tionCode: CD+ treatmentVehicleCode: CD+ treatmentVehicleAmount: PQ::PlannedActivi ty+ name: SET<ST>+ actualIndicator: BL+ contingentIndicator: BL+ studyFocusIndicator: BL+ inStudySegmentPlannedActivi tyTypeCode: CD+ additi onalDurationDescrip tion: ST+ plannedRangeOfRepetit ionsT ext: ST::Activi ty+ identi fier: II+ nameCode: CD+ textDescription: ST+ categoryCode: CD+ subcategoryCode: CD+ reasonCode: SET<CD>+ statusCode: CD+ statusDateRange: IVL<TS>+ comment: ST
StudyContact
+ roleCode: SET<CD>+ primaryIndicator: BL+ postalAddress: AD+ telecomAddress: SET <T EL>+ statusCode: CD+ statusDateRange: IVL<T S>
StudyInvestigator
+ identi fier: II+ signatureText: ST+ dateRange : IVL<TS>::StudyContact+ roleCode: SET<CD>+ primaryIndicator: BL+ postalAddress: AD+ telecomAddress: SET<TEL>+ statusCode: CD+ statusDateRange : IVL<TS>
0..*
functions as / is represented by
0..1
1
identi fies / associates to
1
0..*
oversees / isoverseen by
1
0..1
is issued by / i ssues
0..*
1..*
groups / is groupedby1
1..*
is a di vision of /is di vided into
1
0..*
performs / is performed at
0..1
1
plays / is played by
0..*
1
plays / is played by
0..1
1plays / is played by
0..*
0..1
plays / is playedby
0..1
0..1
plays / is played by
0..*
1
functions as / is represented by
0..*
1
submits / is submitted by
1
1..*
1
1
associates asubmission uni tto / isassociated to asubmission uni tvia
1..*
0..*
is includedin / includes
1..*
1..*is associated to a submi ssion via /associ ates a submissi on to 1
1..*
groups / is groupedby
0..1
1
associates to / maybe the target for0..*
1
associates from / is i denti fied by
0..*
0..*executes/ is executed at
1
0..*
associates from / may bethe source for
1
0..*
oversees / is overseen by
0..*
1
is played by / plays
0..1
0..1
plays/ is played by
0..1
1plays / is played by0..1
1
is played by / plays
0..1
1
is scoped by / scopes0..*
0..1
funct ions as / i s represented by
0..*
0..1
plays / is played by
0..1
1
plays / is played by
0..*
0..1
has component /used as component0..*
1
operates as /represen ted by
0..*
1
provides / isprovided by 1
0..1
is issued by / issues
0..*
0..1
plays / is played by
1
1
plays / is played by
0..1
0..1
plays/ is played by
0..*
1
is played by / plays
0..*
0..*
is evaluating / is a research topi c in
11
is used as / is fulfi lled by
0..*
1
scopes / is scoped by
1..*
1
plays / is played by
0..1
1..*
is measured by / measures
1..*
0..1
is operational i zedby/ is descri bed by
0..*
0..1
is responsible for /is theresponsibi lity of 1
1
operates as / represented by
0..*
1
plays / is played by
0..*
0..*
describes / i s described by
1..*
0..*
is the resource for / is resourced by
0..*
1
is scoped by / scopes0..*
1scopes/ is scoped by
0..*
1..*
contains / iscontained in
1
1..*
describes / has
1
0..*
describes / may have
1
0..*
plays / is played by
1
0..*
scoped by / scopes
1
0..*
is scoped by / scopes
1
0..1
plays / is played by
0..1
0..*
controls / is control led by1
0..*
is scoped by / scopes
1
0..1 plays / is played by
0..*
1..*
participates in / i sconducted by
1
0..1
functions as / is represented by
0..*
0..1
functions as/ is represented by
0..*

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 7Optimizing Clinical Trials: Concept to Conclusion TM 7© 2011 Medidata Solutions, Inc.
• Summary of Study Design (EXAMPLE)• This is a prospective, randomized, double-blind, double-dummy, placebo
controlled, forced-titration, multicenter, parallel group trial. Stage I or II hypertensive patients, age 18 years of age or older, who meet all other inclusion and exclusion criteria and successfully complete the placebo run-in period will be randomized at the site level.
Protocol Representation Model

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 8Optimizing Clinical Trials: Concept to Conclusion TM 8© 2011 Medidata Solutions, Inc.
• Summary of Study Design (EXAMPLE)• This is a prospective, randomized, double-blind, double-dummy, placebo
controlled, forced-titration, multicenter, parallel group trial. Stage I or II hypertensive patients, age 18 years of age or older, who meet all other inclusion and exclusion criteria and successfully complete the placebo run-in period will be randomized at the site level.
Protocol Representation Model
Subject age description
ConfigurationDegree of blindPopulation
disease description

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 10Optimizing Clinical Trials: Concept to Conclusion TM 10© 2011 Medidata Solutions, Inc.
Protocol Representation Model

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 11Optimizing Clinical Trials: Concept to Conclusion TM 11© 2011 Medidata Solutions, Inc.
Objective #1
Endpoint #1
Procedure #1
Variable #1
Variable #2
Procedure #2
Variable #3
Variable #4
Objective #2
Endpoint #2
Procedure #3
Variable #5
Variable #6
Protocol Representation Model

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 12Optimizing Clinical Trials: Concept to Conclusion TM
A New World..........
Results:
• Simplify protocols• Reduce number of procedures and cost per patient• Reduce effort setting up downstream systems• Eliminate effort associated with cleaning and analyzing
’excess’ data
• Avoid amendments/rework• Reduce cycle time (creation and review of clincial
deliverables)• Reduce duplicate data entry, reformatting and rewriting of
information
People/Behaviours: Process: Technology:
• More disciplined approach• Willingness to seek peer feedback• Business acumen - ability to
assess trade-offs bertween time cost value & risk
• Focus on outcomes & audience (start with the end in mind, consider consumers)
• Shift from study level to project level planning
• Plan -> Design -> Document• Leverage project level information• Apply study specific information• Generate clinical deliverables• Streamline review & approval
• Electronic study design tool (inc. content management capabilities and publishing templates)
• Integration with • upstream planning and study
registration solutions• downstream data collection
solutions• benchmarking data and
clinical standards
• Shift from clinical document management to information management
• Increase the quality and consistency of clinical information• Align objectives, endpoints and procedures
Strategy/Goal:
• Demonstrate traceability from strategy to plan to study design
• Support parallel development of Protocol, RAP, eCRF and CSR • Leverage industry benchmarks
Modular Authoring
Tem
plat
es
and
Reu
seF
easi
bilit
y A
sses
smen
tR
evie
w/ A
ppro
val/
Dis
trib
utio
nA
utho
ring
Pla
nnin
g &
stu
dy d
esig
n
CIL
Medidata Designer
Enter study id
1
Trigger: CIL ‘wants to’
1
Study Information Skeleton Created
Automatic
Medidata Designer2, 3
Grow study information in Design environment
8Medidata Designer
CIL / EST2,3,4,5,6,7
Medidata Designer
Select delivery template(s)
9CIL / EST
9
8,9 10Automatic
Medidata Designer
Populate study information from Design env
Medidata Designer
CIL / EST11
Develop WORD content within Design env
9
Templates include:- CSP- Protocol- RAP- eT&E- CSR focus document / shel l- Disclosure summary (tbd)
12CIL / EST
12
Upload deliverables to eDX for review
eDX
eDX
Approval of deliverables
Governance
eDX
13
15
12
Review of deliverables
Internal / External
14
17
IMMS
CIL / EST
PIER
16CIL / EST
Upload approved deliverables to PIER
16
15
Upload approved deliverables to IMMS
Conduct Protocol Specific Feasibility
??
Regional Medical Director
Or does this input to WORD content?
Do we need Inc /Exc flow into eDX in order to perform
feasibility analysis (ref SB)? Or is this just manual
reference?
Draft
Final
Internal functionality not mapped: review, report, ppt
Internal references utilised in growing the information but not mapped :
- Reference content- Standard procedures
- Indicative costs
What is captured here?- new content or
- content that cannot go into design environment
IR interface for tables/listing & graphs – where?
Would details for adaptive trials have to be added here?
Trigger:1, Want wider input2, Develop WORD
content
Trigger??
Comments / Edits
Comments / Edits
‘Approved’ / FPAData Input and Output
1.Study id’s 2. Medium term study design (OneCDP)3. Study Master Data (MDM)4. Library of approved standard content (eProtocol) {All studies, Asset , study level}5. Legacy information (IMMS )6. Standard procedures (within system from MDR ?)7. Indicative costs (eProtocol)8. Study information 9. Document Template Library10. Study information from design envi ronment in template11. Addi tional information captured in WORD in design envi ronment12. Draft deliverable13. Review deliverable14. Final ‘Approvable’ Del iverable15. Approved Deliverable16. Publ ished Deliverable17 Archived Deliverable18. eDocument Metadata
2
15,16Technical Authoring Team
Store & Manage Deliverable Metadata
Medidata Designer9
Technical Authoring Team
6
??
eProtocol , IMMS
Technical Authoring Team
Metadata Search of Ref Content for Reuse
9
eProtocol
18
2
Define Deliverables Templates
Technical Authoring Team
Copy Existing Deliverables Content: ??
??
??
Scope:Start = medium term study design onwardsEnd = approval , publishing & archiving of all study deliverables; del iverable metadata to facili tate re-use
eSignature or workflow transfer
to IMMS

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 13Optimizing Clinical Trials: Concept to Conclusion TM
A New World Realised
PRM

The Typical Protocol in 2012
• Average of 13 endpoints – 1 primary and 5 ‘key’ secondary
• Median of 170 total procedures• 85 procedures support primary and key secondary
endpoints
• Median 50 inclusion and exclusion criteria and 180+ case report form pages
• Requires study volunteers to make 11 visits over an average of 175 days
14Source: Tufts CSDD, 2012

Mean Number of Data Points Collected per Study
Phase I Phase II Phase III Pase IV
110,833
378,446
929,203
675,652
15Source: Medidata Solutions Worldwide, 2012

Rising Protocol Complexity and Burden (All TAs, All Phases)
00 – 03 04-07 08-11Unique procedures per protocol (median) 20.5 28.2 30.4
Total procedures per protocol (median) 105.9 158.1 166.6
Total investigative site work burden (median units)
28.9 44.6 47.5
Total eligibility criteria 31 49 N/A
Median study duration in days 140 154 175
Median number of CRF pages per protocol 55 180 N/A
16
Getz, Campo, Kaitin. Variability in Protocol Design Complexity by Phase and Therapeutic Area. DIJ 2011 45(4); 413-420.
Source: Tufts CSDD

• Ongoing shift from acute to chronic diseases
• Pipeline composition shift from traditional NCEs to biologics
• Focus on doing more in earlier development phases
• Phase IV becoming more robust and sophisticated
• Growing requirements from purchasers and payers
• Habit and legacy protocol templates and authoring practices
• Risk mitigation/risk avoidance
Primary Drivers of Protocol Complexity

IMPACT: Amendment Prevalence19
Note: All values are means *Analysis excludes protocols without any amendments
Protocol Phase
Number ofAmendments*
Number of Changes
per Amendment
Phase I 2.0 5.6
Phase II 2.6 6.8
Phase III 3.6 8.5
Phase IIIb/IV 2.3 8.3ALL
PROTOCOLS 2.4 6.9
• 46% of all amendments occur BEFORE first patient first dose• 37% of all amendments are considered ‘avoidable’
Source: Tufts CSDD, 2012

IMPACT: Extraneous Protocol Data
• Two primary areas of ‘protocol waste’ – (1) Essential procedures performed excessively (2) Extraneous and unused procedures
• New 2012 Tufts CSDD study among 15 participating pharmaceutical and biotechnology companies to assess cost of ‘non-core’ procedures– Study sponsored by Medidata Solutions
• N = 117 PII/III protocols; N= 22,143 procedures analyzed; cost data N=16,607 procedures
• Global, multiple therapeutic areas, No pediatric, devices, orphan diseases and No extensions
20

Procedure Classifications
Core• Procedures supporting primary and/or
secondary objectives• Procedures supporting primary, *key*
secondary and safety endpoints
Non-Core• Procedures supporting tertiary and exploratory
objectives and endpoints• Procedures supporting *supportive* secondary and
exploratory endpoints• Safety and efficacy procedures that are not included
as an endpoint or objective• Procedures not tied to an endpoint or objective
Required - GCP Compliance• Screening requirements• Informed Consent• Drug dispensing (compliance)
Standard Procedures • Performed in all trials: concommitant
medications, demographics, adverse event assessment etc...

One-out-of-Four Phase II/III Protocol Procedures are ‘Non-Core’
22
57.8%24.1%
8.8%
9.4%
Core NonCore Required Standard Procedures
Source: Tufts CSDD, 2012

$1 Million in Direct Procedure Costs per Protocol is Paying for Non-Core Activity
Overall$000
Phase II$000
Phase III$000
All $6,001 $2,068 $9,174
Core $3,133 (52%) $1,316 (64%) $4,599 (50%)Non-Core $1,051 (18%) $262 (13%) $1,688 (18%)Required $1,372 (23%) $329 (16%) $2,214 (24%)Standard $474 (7%) $161 (8%) $673 (7%)
23
* All values are means; Aggregate of costs for all patients receiving the procedures scheduled per visit per protocol
Source: Tufts CSDD, 2012

Conservative Impact of Extraneous Protocol Data Costs• The total direct cost to industry to perform ‘Non-Core procedures is an
estimated $3.7 billion annually – Only counts an investigational drug in clinical development once although it may
be in active clinical trials for multiple indications. – Counts only one clinical trial per active compound per phase when multiple trials
are likely conducted simultaneously.
• This study only examined direct procedure cost and does not include the indirect cost of personnel time to capture, monitor, clean, analyze, manage and store tertiary and exploratory procedure data.
• The ethical cost of exposing study volunteers to the risk of performing less essential, and unnecessary, procedures has also not been considered in this analysis.
24

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 25Optimizing Clinical Trials: Concept to Conclusion TM

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 26Optimizing Clinical Trials: Concept to Conclusion TM
Potential Financial ImpactMeasured over implementation stage
Eliminate costs
Reduce effort
Improve Quality and Consistency
Focus on Study Design
30-50% efficiency gain in protocol development process (authoring and review cycles)Sponsor experience and Medidata best practice
$150k/late phase study decrease in study costs through linking exerciseSponsor experience
$453k/per controllable amendment reductionKen Getz, Tufts Center for Study of Drug Development study results on costMedidata best practice
30-50% EDC study start-up time and effort reductionMedidata best practice
50% time saving exporting to ClinicalTrial.govSponsor and Medidata expected results
Decrease costs of collecting/storing/validating/managing unnecessary patient data$3,354/per day for 100% SDV per PICAS
Integration

© 2011 Medidata Solutions, Inc. – Proprietary and Confidential© 2012 Medidata Solutions, Inc. – Proprietary and Confidential 29Optimizing Clinical Trials: Concept to Conclusion TM
Conclusions• Adopting PRM, ENABLES
• Significant process change involved in adoption• Real business value can be demonstrated• Opportunity to
• Influence trial cost and complexity• Drive reuse and efficiency• Interface with other standards
• Application of standards will enable organizations to build BI and analytic capability never possible before
• Adopting PRM, WILL• Drive significant operational, clinical, ethical and technical savings/benefits



















![PRM PPT[1]](https://img.pdfslide.us/doc/110x75/577d23931a28ab4e1e9a2ea5/prm-ppt1.jpg)