Embed Size (px)
Citation preview

BIONTM Neuromuscular Stimulation for Pressure Ulcer PreventionHilton Marc Kaplan & Anne-Caroline Dupont Salter
Alfred Mann Institute, University of Southern California
Pressure ulcers are a debilitating pathology resulting from pressure and shear in the soft tissues of immobilized patients129. Nomenclature varies widely (decubitus ulcers, pressure sores, bed sores, ischemic sores, etc.), and a multitude of therapies exist. The fact that so many therapies are available, is ironically testament to their own inadequacies.
Etiology
The pathogenesis of pressure ulcers (PUs) derives from a host of compounding etiological factors129:
Pressure over bony prominences is key. A reciprocal relationship between pressure intensity and pressure duration has been recognized since 1930. Just as high pressures over a short time may result in PUs, so can lower pressures over a longer time. Immobility that results in the inability to shift weight plays an important role because the tissues do not experience periodic relief from the pressures on them. Friction and shear are important factors too, because they can exacerbate the soft tissue damage. Tissue that is damaged, atrophied, scarred or infected demonstrates increased susceptibility to pressure. The elderly or immune compromised patient and the patient with wound healing or collagen-vascular diseases are at greater risk too. A lack of sensation, common in many poorly mobile individuals, aggravates the situation further, because the individual may forget to move even to the extent that he or she can. Insensate tissues also demonstrate compromised neurotrophic growth and repair mechanisms. Urinary and/or fecal incontinence may also be present in individuals whose immobility derives from the injury of the spinal cord or brain. The irritation can fuel maceration of the skin and contribute to further susceptibility to the effects of pressure. As blood vessels become occluded or narrowed the soft tissues which they supply necrose (break down and die)because they are starved of nutrients and oxygen, and because they accumulate toxic wastes and metabolites.
Costs – to the Patient and Society
Age- and pathology-matched patient trials have shown that hospital stays increase 3-5 fold in patients suffering from PUs, at significant hospital expense101. One of 3.6 immobile patients will develop PUs114. One group particularly prone to PUs is the spinal cord injured (SCI) patient group. Over 250,000 individuals have SCI in the US, and approximately 10,000 new injuries occur each year102. SCI most commonly results in paralysis, as well as repeated and serious associated complications such as PUs, incontinence, sexual dysfunction, etc. Healing and rehabilitation are also impacted by the psychological ramifications of depression, resentment, etc.103. The cost of treating PUs in the US has been estimated at over $ 55 Billion annually (based on an average increase in hospital stay of 21.6 days at $2,360 per day in almost 1.1 million patients per year101).

Staging of PUs
The National PU Advisory Panel Staging112 is a widely accepted method of staging PUs:
Stage I: Non-blanchable erythema of intact skin; the heralding lesion of skin ulceration.
Stage II: Partial thickness skin loss involving epidermis and/or dermis. The ulcer is superficial and presents clinically as an abrasion, blister or shallow crater.
Stage III: Full thickness skin loss involving damage or necrosis of subcutaneous tissue which may extend down to, but not through, underlying fascia. The ulcer presents clinically as a deep crater with or without undermining of adjacent tissue.
Stage IV: Full thickness skin loss with extensive destruction, tissue necrosis or damage to muscles, bone or supporting structures (e.g. tendon, joint, capsule, etc.).
Current Treatments
Current treatments usually involve months of care and hospitalization, including:
Tissue Load Reduction:
Specialized pressure support surfaces (air-fluidized, low-air-loss, alternating-air, static flotation [air or water], foam standard or Roho dry floatation mattress126), are used to reduce the continuous pressure on tissues.
Nursing Care and Allied Therapies:
Patients are supplied with nursing care and assistance for most of their activities of daily living. Typically, they must be turned or moved at least every 2 hours (which usually involves at least 2 staff members). Physiotherapists, occupational therapists, nutritionists, social workers and psychologists are all integral to successful treatment and rehabilitation as well.
More detailed guidelines on preventive care are given by the National PU Advisory Panel124, AMA and others132:
Skin Moisture Control:Careful management of skin moisture is essential to prevent maceration and minimize friction. Patients should be bathed only when needed for comfort or cleanliness; skin should be cleaned as soon as soiled with urine or stool; urine leaks must be assessed and treated; skin should be protected with cream or ointment; and absorbent pads and/or briefs with quick-drying surfaces should be used.
Prevention of Over-Drying of the Skin: Moisturizing the skin where needed.

Friction Reduction:Lifting, rather than dragging, when repositioning; and using cornstarch on skin.
Changing of Position / Turning:At least every 2 hours if bed-ridden; at least every hour if confined to a chair; and every 15 minutes if able to shift own weight.
Optimization of Pressure Distribution:Keeping the patient as flat as possible if bed-ridden (raising the head of the bed as little and for as short a time as possible); using foam, gel, or air cushions to relieve pressure; and pillows or wedges to keep knees or ankles from touching each other.
Nutritional Support:Ensure adequate caloric intake of a balanced diet and food supplements as required.
Physiotherapy:Maintenance of range of motion so that a wider range of positions are possible.Prevention of systemic deconditioning (cardiopulmonary, cardiovascular, and musculoskeletal)
Social & Psychological resources (to encourage compliance with therapies):Social workers and vocational rehabilitation servicesPeer counseling and support groupsFormal psychotherapy &/or family therapy
Treatment of Complications and Supportive Treatment:
Where indicated:
Antibiotic cover (systemic and topical), swab cultures.Nutritional supplementation (enteral and parenteral).Blood transfusions, iron and folate supplementation.Pain management.Minimization of muscle spasticity (to optimize healing by secondary intention)125.
Wound Care and Surgical Interventions 127, 132 : Stage I:
Prevention of further skin damage.
Stage II:
Debridement (usually not necessary).Cleansing: isotonic saline; avoidance of high-pressure irrigation; manage hypergranulation tissue that may impede ulcer healing.Dressings: hydrocolloid wafers, semipermeable foam, or polyurethane film (occlusive / vacuum).
Stages III and IV:
Debridement: autolytic, mechanical (wet-to-dry dressing), enzymatic, or surgical.

Cleansing: isotonic saline, may use high-pressure irrigation; manage hypergranulation tissue that may impede ulcer healing.Dressings: if wound is shallow and clean – hydrocolloid wafers, semipermeable foam, or polyurethane film; if wound is deep and clean – fill dead space with wet gauze; If there is necrotic debris – wet-to-dry dressings; if there is excessive exudate – absorptive dressings.Surgical repair: once wounds are clean (< 100,000 organisms/cm2) and the patient is medically stable, a variety of reconstructive techniques may be utilized including: direct closure, skin grafts, skin flaps, musculocutaneous flaps, and free flaps.
The Gluteal Rotation Flap:
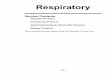
While a variety of musculocutaneous flaps are useful in treating PUs, the gluteal rotation flap is of particular relevance to this study. The gluteal rotation flap is an axial flap based on the inferior (and/or superior) gluteal artery, located between the greater trochanter and the ischial tuberosity125 (Fig.s 1 & 2). After excising the PU wound, the muscle flap is elevated, together with an overlying skin paddle which is supplied by musculocutaneous perforators. It may then be rotated superomedially to cover sacral PU wounds, or inferomedially to cover ischial PUs (Fig.s 3 & 4). In this way healthy muscle and skin are brought in to repair the deficient area, and provide healthy tissue over bony prominences, while scars are designed to lie away from these areas.

Fig.3: Rotation for Sacral PU Repair Fig.4: Rotation for Ischial PU Repair
Fig.1: Gluteus Maximus131
ischial tuberosity
hypogastric artery
superior gluteal artery
inferior gluteal artery& nerve
Fig.2: Neurovascular pedicles
greater trochanter

Postoperative care and Recurrence Rates:
Typically, at Rancho Los Amigos patients are nursed as inpatients for 8 weeks postoperatively. This involves 5 weeks of complete non-weightbearing, where the patient is nursed prone or on the unoperated side; 2 weeks of limited mobilization and 1 week of gradually increased sitting until ready for discharge. The cutaneous sutures are removed at the end of week 3. Throughout this process patients are educated on pressure management and skin inspection. This regimen is in keeping with the postoperative care guidelines as recommended by the AMA and others132.
Potential postoperative complications include132:Wound dehiscence / separationDelayed infection and abscessHematoma and seroma
Initial results with muscle flaps are generally good, although recurrence of PUs is common135,133,136. In the case of musculocutaneous flaps 33% recurred over 2-12 years (with cutaneous flaps recurrence rates were as high as 43%)136. As lack of sensation in the flap may contribute to this high recurrence rate, neurosensory musculocutaneous flaps have been advocated137,138. In the sensate patient gluteal rotation flaps offer this potential advantage.
In the face of ever-increasing limitations on health-resources, very high recurrence rates and advances being made in the wound healing realm (e.g. flotation-type beds, growth factors, etc.), Disa, Carlton & Goldberg133 attempted, in 1992, to define which patients might benefit most from surgery. This group reviewed data from 40 consecutive patients with 68 pressure sores operated on under a single surgeon between 1981 and 1989. Of 66 operations performed, 55 were musculo- or fasciocutaneous flaps, and 11 were cutaneous. Over a mean followup of 21 months (1-71) they recorded a 36% operative complication rate, and no mortalities. Despite an 80% healed rate at the time of discharge, 61% of PUs and 69% of patients had recurrent ulceration within a mean of 9.3 months (1-71 mo.s). The conclusion was that surgical reconstruction of PUs did not appear to be efficacious in young posttraumatic paraplegics or the cerebrally compromised elderly.
Adjuvant Therapies:
Adjuvant therapies include: electrical stimulation, hyperbaric oxygen, infrared or ultraviolet light, low-energy laser irradiation, ultrasound therapy, and topical applications of agents as varied as growth factors and maggot therapy.
For its wound-healing effects, only electrical stimulation of the skin has been recommended by the AHCPR (US Dept of Health and Human Services, Agency for Health Care Policy and Research) as an adjunct to conventional therapy for nonhealing ulcers128.

NeuroMuscular Electrical Stimulation for PU Prevention
Neuromuscular electrical stimulation (NMES) for pressure-relief has been researched for well over 2 decades now, with multiple papers indicating the positive benefits of this therapy 100,104,105. Current hypotheses of the mechanism that leads to prevention of pressure ulcers include weight shifting to relieve pressure and improve pressure distribution, increased muscle volume (more padding), and increased vascularity100,104,105.
A patent on using NMES for PU inhibition was filed with the USPTO in 1985, and issued in 1988. Assigned to The University of Michigan, it is based on transcutaneous NMES over potential PU sites and claims benefits from the resultant shifting of weight, muscle ‘blood pump’ effect, muscle hypertrophy (padding) and the ‘conditioning’ of atrophic muscles100.
In 2000 Bogie et al104 published an article in which the role of NMES in PU prevention was reviewed. They concluded that implantable NMES systems may have great potential for PU prevention, particularly for individuals who lack sensation or are physically unable to perform regular independent pressure relief.
Preliminary results of a more recent study by Bogie’s group105 were published in an abstract. They investigated the hypothesis that long-term use of NMES using an implanted stimulation system would produce a sustained improvement in tissue health, and may therefore provide an alternative technique for the prevention of pressure sores in veterans with spinal cord injury. Preliminary results show that interface pressures in the ischial region were significantly reduced (p<0.01). No details on stimulation parameters were offered.
Waiting for article / book (d.w. FJR pls Anne) to find out the particular paradigm used (what m.s were exercised, …) and what was measured (recurrence, …)?
It has been shown too that PU recurrence rates can be reduced from 20% to 6% using ES113.
Current Drawbacks
The limitations of current treatments are of great concern. Despite the wide variety of current preventive measures, PUs remain a significant pathology (as attested to by the high incidence of PUs (up to 38%150) and the extremely high recurrence rates even after flap surgery (61%133). ES – a therapy that has demonstrated significant potential benefits in the literature – remains unharnessed because of limitations imposed by the prerequisite “wiring” of patients.
BION Electrical Stimulation for Pelvic Pressure Ulcer Prevention
BIONs are injectable, wireless electrical stimulators that receive power and command signals by inductive coupling from an external transmission coil. One or more can be placed near or in various muscles and nerves and selectively activated with precise control of pulse current,

duration and timing. BIONs have been demonstrated to be safe and effective in chronic studies in animals and human subjects (). They are particularly suitable for use in the proposed clinical application because of their small size (2mm diameter x 16mm long), hermetic packaging, stable fixation in connective tissue, and virtually unlimited lifetime. The transmission coil to power and command the implants can be located in a cushion, seat or back of a wheel chair, avoiding any direct contact with or penetration of already fragile skin.
Two hypotheses guide this research: First we hypothesize that BION gluteal stimulation will reduce the incidence of PUs. Second, we hypothesize that the treatment will be accepted well by the subjects because it can be self-administered outside a clinic. Using BION microstimulators to electrically stimulate the gluteal muscles is a novel way to achieve the published benefits of ES, without the usual limitations as discussed above.
Fuhrer et al report that 65% of PUs are in the pelvic111.region. Gluteus maximus (gluteus) muscle stimulation will benefit both sacral and ischial lesions. These constitute 42-54% of all PUs according to four biennial national prevalence surveys108. Of these 30% are Stage III & IV111
(where surgery is the treatment of choice). We propose to achieve such gluteal stimulation with a single BION placed along the inferior gluteal neurovascular pedicle. Preliminary anatomic dissections and 3D CT reconstructions performed at the University of Southern California to map these pedicles indicate that the nerve trunk appears at a well-defined location as it exits from beneath the inferior edge of the piriformis muscle, before branching out under and into the substance of gluteus maximus109,110. Placement of a device at this site would facilitate full and reliable stimulation of gluteus.
Goal
The goal of this new treatment is two-fold:
1. to improve dynamic, short-term pressure distribution and increase dynamic, short-term blood perfusion to the area during stimulation.
2. to increase muscle mass, size and tone in that area so that there is a long-term decrease in peak pressure and density and a long-term increase in blood perfusion to the area in the periods between stimulation bouts (at rest).
Hypotheses
Primary hypotheses:We hypothesize that1. The subjects will be compliant and receive at least 80% of their prescribed BION
treatment.2. During stimulation, the BION will produce detectable contractions of the gluteus muscle.3. After 12 weeks of BION gluteal stimulation, localized pressure points when seated (at
rest, not stimulated) will be diffused (lower pressure density) (when compared with pre-treatment values) in the gluteal region that was stimulated.

Secondary hypotheses: We hypothesize that:
1. During stimulation, peak pressure will be decreased significantly on the contralateral side of the contraction.
2. After 12 weeks of BION gluteal stimulation, muscle size (both cross-sectional area and volume) will be increased (when compared with pre-treatment values) on the side of stimulation.
3. Gluteal muscle perfusion will be increased during stimulation, when compared with value at rest.
4. After 12 weeks of BION gluteal stimulation, perfusion of the gluteal maximus muscle (at rest and during stimulation) will be increased when compared with pre-treatment values.
Overview
Optimal placement of a BION for gluteal stimulation is near the gluteal pedicle. Unfortunately, external landmarks for the pedicle are not reliable, especially in individuals who have atrophied gluteus muscles. During gluteal flap surgery to repair pressure ulcers in the buttock area, the gluteal pedicle is exposed, giving the surgeon the opportunity to implant a BION with full view of the area. We propose to implant a BION near the gluteal pedicle during gluteal flap surgery and subsequently stimulate the gluteus muscle daily in order to provide short and long-term pressure relief and reduction of pressure ulcer reoccurrence. The BION treatment schedule will be incorporated into the healing/treatment schedule of the flap surgery and in-patient time at Rancho. Moreover, all subjects will receive normal nursing pressure care in parallel to the BION therapy (including relief of pressure with cushion, etc).

Treatment schedule
The BION treatment schedule will have to incorporate the healing/treatment schedule of the flap surgery and in-patient time at Rancho.
Insert Study Plan Excel Sheet here
Week no. 1 2 3 4 5 6 7 8 9 – 12 13 – 20
Surgical MilestonesFlap surgery events
Flap
surg
ery
Stitc
hes r
emov
ed
Dis
char
ge
12-w
k fo
llow
-up
20-w
k fo
llow
-up
MobilityPosition for healing Lying Lying with
movement
Some SittingStart to
sit
Wheelchair
Location Rancho HomeFollow up x x x x xBION Training x x x x x x x BION Therapy treatment x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x x
For three weeks after the surgery, the patient recovering from gluteal rotation flap surgery is in a prone position at Rancho. At the fourth week, the stitches are removed and the patient is allowed to perform movements but is still kept in a prone position. BION muscle strengthening (“BION Training”) would start as movement is allowed (in the 4th week). The patient starts sitting briefly during the 7th week and starting in the 9th week, the patient can sit in his wheelchair. During the 9th week, BION stimulation would start being used for pressure relief (“BION Therapy”). Can you start treatment while the patient is lying down to increase muscle strength and tone? May need a different coil…The patient self-administers treatment by pressing one of three start buttons on a control box that can be programmed by the clinician with up to three different stimulation programs. The control box (called a Personal Trainer) records the pattern and duration of usage; this information is automatically uploaded into each patient’s personal database in the clinician’s personal computer whenever the patient returns for a follow-up visit.
BION Training:
Starting with 1 hour per day (broken down in 15 min sessions) and increasing to 5 hours per day (with sessions a maximum of 2 hours in length, sessions to be separated by at least 30 minutes of rest), 10 sec ON, 5 sec OFF at 5 Hz. The low frequency is chosen because it produces unfused contractions that are not very forceful in nature and therefore will not produce much movement of the buttock and leg area, but should facilitate circulation by their pumping action. Previous studies in rats with a model of disuse atrophy have shown that such low frequency stimulation is effective in preventing atrophy (), possibly because it activates the calcium kinase pathway

responsible for maintenance and development of muscle mass. Previous clinical studies of BIONs to prevent shoulder subluxation following stroke and to strengthen quadriceps in patients with osteoarthritis have used 2-5pps stimulation with success ().
BION Therapy:
Starting when the patient starts sitting in his wheelchair, BION stimulation will be applied whenever the patient is in his wheelchair, for a minimum of 5 hours, with a cyclic paradigm : 3 sec ON, 7 sec OFF (at 20-33 Hz for a tetanic contraction). If the patient cannot sit (with stimulation) for at least 5 hours per day, the missed time will be made up with muscle strengthening time in order to maintain strength.
STIMULATION PROTOCOLS
STIMULATION PARAMETER MUSCLE TRAINING MUSCLE TREATMENT
AMPLITUDE (mA) 1-8 (5) 1-8 (2)intense pulse to recruit all fibres lower pulse ... as much as is needed
FREQUENCY (Hz) 1-2 20-33low f : initiates minimal movement high f : to achieve tetanic contractions
DUTY CYCLE (s) 3 on, 3 off 2 on, 4 off
lower force contractions ... can use more of duty cycle without risking fatigue or compromising blood supply
as needed to shift weight, without becoming annoying; adequate rest to avoid fatigue or compromising blood supply
Testing:
Testing will be scheduled for before stimulation starts, at discharge from Rancho, and during follow-up visits at Rancho, for up to a total of 5 evaluation sessions. Testing includes MIR measurements of muscle cross-sectional areas and volume, Thalium scan, and pressure mapping Testing is in greater details in the Outcome Measure section.
Inclusion / Exclusion criteria
Inclusion:
Subject has had a spinal cord injury and has bilateral lower limb paralysis Subject cannot contract voluntarily his gluteus muscle

Subject is between 18 and 70 years old Subject sits in a wheelchair for at least 5 hours per day Attending physician considers the subject in general good health (other than SCI and
pressure ulcer wound) Subject is having gluteal rotation flap surgery for pressure ulcer treatment in which the
inferior gluteal pedicle will be exposed but not damaged or sacrificed in any way (for any pressure ulcer wound).
subject is mentally capable of understanding the goals and the application of therapy subject is able to apply the therapy (with or without help) once discharged from Rancho subject is willing and capable of giving informed consent subject is willing and capable of traveling to testing center at the schedule described
above
Exclusion:
subject is pregnant, nursing, or planning on becoming pregnant in the next 12 months
subject has an electronic implant (ex: heart pacemaker, etc) subject has large metallic implant (e.g.: plates, hip joints) in the buttock/pelvic area
(small metal implants, such as bone screws and metal sutures are acceptable). subject has any condition associated with wound healing abnormality (e.g.:
connective tissue disorder, immune disorder, diabetes, clinical obesity) subject is malnourished the attending physician has concerns about the healing of this subject (e.g.: heavy
smoking, excessive and poorly-managed incontinence) subject has concurrent concomitant condition affecting the buttock/pelvic area,
including other pressure wound not corrected by the flap surgery. Claustrophobia or fear of having an MRI scan done. subject has damage to the inferior or superior gluteal neurovascular pedicles.
Justification for inclusion and exclusion criteria:
Inclusion:
Spinal cord injury and paralysis of the lower limbs: This study is specifically designed for wheelchair-bound patients with SCI because this population is at high risk of developing pressure ulcers, partially because of the difficulty of relieving pressure on the buttocks when seated.
No voluntary contractions of the gluteus muscle: this therapy will stimulate the gluteus muscle to contract. If it can contract voluntarily, BIONs are unlikely to be necessary.
Age: subjects above the age of 70 are considered elderly and that population has been shown to be more prone to pressure ulcers because of two risk factors: compromised nutrition and reduced skin elasticity. Subjects under the age of 18 rarely show pressure ulcers and are often not responsible for their entire care.

Sits in wheelchair for a minimum 5 hours/day: the therapy and equipment are designed to be used in a wheelchair because that is when the person is at most risk of developing pressure sores.
Good health: other important generalized health problems may be confounding variables in this study as they could affect skin health as well.
Gluteal flap surgery: to reduce the number of surgical procedures and take advantage of the opportunity to see the nerve pedicle, the BION will be implanted during a gluteal flap surgery that is already necessary for the subject.
Mentally competent: the subject has to be able to give informed consent and has to be able to understand the why and the how to apply the therapy.
Able to apply the therapy (or have it applied): because this is a self-applied treatment, the subject has to be able to set up and apply the therapy on his/her own or to have a caregiver who can do it at the prescribed schedule in order to achieve compliance.
Informed consent: because this is a research project with an investigational device, the subject has to be willing and able to give informed consent.
Able to travel to Rancho at prescribed schedule: In order for this study to have valid data, we need to ensure that the subject is capable and willing to visit the center at the prescribed schedule for testing and treatment.
Exclusion:
Pregnancy and nursing: The effects of BION™ treatments in pregnant or nursing women have not yet been investigated fully. In addition, the uncommon occurrence of strokes in this vulnerable population may render the risk of including them greater than the potential benefit.
Electronic Implant: Patients with electronic implants will not be accepted into the trial because the electromagnetic field produced by the external coil might potentially interfere with a pacemaker or other electronic implants. The effects of electromagnetic fields on electronic implants such as pacemakers have yet to be characterized.
Metallic Implant: Patients with large metallic implants will not be accepted into the trial because these metallic implants might potentially interfere with the electromagnetic field produced by the external magnetic coil.
Healing condition: other health problems that may affect the healing capability of the skin are confounding variables.
Malnourishment: patients who are malnourished are at more risk for healing problems and recurrence of pressure sores because healing requires calories and protein and because

extremely thin patients experience more pressure in areas of bony protuberances than people with more adipose tissue.
Concerns about healing: If the attending physician has concerns about healing that have not been mentioned here, he/she should be able to exclude the subject (e.g.: heavy smoker; badly managed incontinence).
Concomitant condition of the buttock/pelvic area, including other pressure wounds: any condition that may affect the healing rate and add a confounding variable to the study needs to be excluded; another pressure wound not treated by the flap surgery will require care and possibly prevent the subject to sit in his/her wheelchair, preventing BION treatment to be applied.
Claustrophobia: one of the primary outcome measures for this study is muscle volume, for which MRI scans will be required. A subject suffering from claustrophobia will not be able to have the MRI done.
Outcome measures
Primary Outcome Measures:
Compliance (diary and personal trainer) peak pressure distribution (with pressure interface system):
peak pressure (absolute value) average of 4 top peak pressure values
high pressure distribution – weighted average, showing where 50% of the pressure is applied (in the smallest region possible)
muscle cross-sectional and volume of gluteus (by MRI) muscle perfusion (Tl-scint & DTI possibility – to rediscuss with Pat Colletti) before and
after exercise, and before and after treatment subject satisfaction questionnaire
Secondary Outcome Measures:
skin color and quality (by visual examination)(PU scale: probably Braden / Norton … still to finalize)
reperfusion time (by pressure and visual examination) recurrence of wounds (by visual examination, photography and history) BMI side-symmetry of pressure (distribution of pressure between the two sides)
Data Analysis

Need to have actual outcome measures finalized to determine n, then d.w. FJR re: stats)
Data analysis: How can you compare before/after if the patients have just had surgery on the affected structures?Ask Frances for help in coming up with a statistical power test to justify patient numbers.
3.6.1. Sample Size Considerations
This study has a repeated measures structure in which subjects serve as their own controls. Repeated measures will be made prior to implant to confirm that the condition under study is stable or worsening on conventional treatment. Outcome measures obtained at various points during treatment are compared with previous values to determine changes and trends attributable to the treatment or withdrawal of the treatment. A within-arm design will be used to compare prestimulation versus poststimulation changes using paired t-tests or Wilcoxon statistical methods (Table 2 below). For evaluations conducted over the longer term, trends will be studied with conventional regression methods and, where appropriate, by ANOVA according to recommendations of the Statistical Consultation and Research Center, Los Angeles, California.
We have used two outcome measures to perform a power analysis. In each case, the change in the outcome variable due to treatment has been estimated from values in the literature and our own experiences to date with study subjects who are being treated for acute shoulder subluxation. A detailed rationale for the selection of values follows, and the Table below summarizes our predictions quantitatively.
Table 2: Summary of Statistical PlanTrial Analytic method Primary Site Outcome measure Effect Size SD Source N calc.
N+extraChronic stroke, shoulder subluxationWe are not using US paired t or Wilcoxon, 1-arm, repeated measures USC Humeral displacement 7mm 7 Faghri, 1994 8 15
USC
The size of each study has been determined using statistical power calculations based upon means and standard deviations of key outcome measures that have been published in previous studies of similar clinical problems and therapies. In these estimations, we assumed that the number of subjects in each arm would be equal and used t-tests to compare continuous variables according to the relationship:
where N = total number of subjects required
Za = the standard normal deviate for a (Za = 1.96 if a = 0.05 and two-tailed and Za = 1.645 if a = 0.05 and one-tailed)
Zb = the standard normal deviate for b (Zb = 0.84 when b = 0.20)
S = standard deviation of the outcome variable, chosen to be conservatively large if more than one value was found in the literature

E = expected effect size
Estimates based on predicate studies, often with different designs and patient profiles, must be interpreted with caution. An increase of sample size by approximately 50% (N+extra) compensates for attrition of subjects, which is common in populations of elderly, sick or community-living individuals. Where no standard deviation of effect size was reported, but standard deviations for stimulated and control subjects were described we have adopted a conservatively large value for standard deviation because we anticipate that chronic subjects may respond more variably to treatment.
The two measures considered to reflect efficacy of treatment best are the amount of joint subluxation before and after treatment Data from Faghri et al. (1994), in a study with a similar design but using surface stimulation in acute patients, suggest a mean improvement in humeral-head displacement of approximately 7mm. After the 6 week treatment period, mean V value of the control group was 9.8 mm ± 6.8 mm whereas the experimental group mean was 2.5 mm ± 3.6 mm. With these values, at least 8 subjects in each group are needed to achieve statistical significance.
We could not find data on muscle atrophy and subsequent remediation by electrical stimulation in stroke survivors. The numbers in table 3 are extrapolated from the results of electrical stimulation of rat muscles using similar parameters. From our preliminary studies in acute stroke survivors, we have found that muscle thickness shows more modest changes than we obtained in rats. There are several reasons why we cannot anticipate the degree of change accurately prior to conducting the experiment. We do not know if the BIONs will recruit all of the muscle or if all study participants will tolerate stimulation that recruits most of the muscle. Our preliminary results in human subjects already suggest that 5% may be too generous an expectation for improvement; some subjects showed this degree of improvement but others showed little change in muscle thickness. Thus, it is likely that more subjects would be required to identify an improvement in shoulder subluxation. We have estimated that at least 15 study participants should be recruited for each of the 2 study groups.
Most of the data analysis will be a comparison between before and after treatment values. Therefore, student t-tests are adequate.
Risks & Benefits
PROCEDURE / Damage to the inferior or superior gluteal neurovascular pedicles
As these patients are already undergoing gluteal rotation flap surgery, both the superior and inferior gluteal neurovascular pedicles will be exposed and easily in reach130. Possible further risks can occur at 2 stages during the procedure:1. Once the inferior gluteal pedicle is palpated (the pulsatile artery can be felt easily), the
BION will be laid alongside this pedicle under vision, and so some limited elevation of the flap will be required to visualize this (with possibly an additional light source (e.g. a

headlight). At no time will the pedicle be opened or further dissected out, other than with the usual normal blunt dissection approach. The BION will be placed with its Tantalum electrode (anode) closest to the inferior gluteal pedicle, and the Iridium electrode can lie either proximally alongside the pedicle or away from the pedicle. Its final position will be tested intra-operatively using an external coil placed outside of a sterile polyurethane drape (so as not to compromise the sterile field at any time), and operated by an assistant.
2. To prevent the BION from moving in the early post-operative period until the tissues stick back down and the spaces developed close up, it will be affixed via a single 5/0 Vicryl suture around the Tantalum stem at either end of the implant. It will secure the BION to adjacent connective tissue or gluteus maximus fascia, and must be placed so as not to injure the pedicle.
We anticipate that both of these 2 stages together will require minimal increased duration (an increased surgical time of 5-10 minutes at most, in a 1-2 hour procedure); or risk (for patients who are undergoing this surgery already, by a skilled and highly dexterous surgeon, having a wealth of experience with all surgical aspects of this procedure and the relevant anatomy).
Risks
The risks during the implantation of the BIONs are the same as for the flap surgery; however, because these patients are already undergoing gluteal rotation flap surgery, the only concern here is the ADDED risk of having the BION implanted during the surgery.
During the gluteal rotation flap surgery, both the superior and inferior gluteal neurovascular pedicles will be exposed and easily in reach130. Possible further risks can occur at 2 stages during the procedure:Once the inferior gluteal pedicle is palpated (the pulsatile artery can be felt easily), the BION will be laid alongside this pedicle under vision, and so some limited elevation of the flap will be required to visualize this (with possibly an additional light source (e.g. a headlight). At no time will the pedicle be opened or further dissected out, other than with the usual normal blunt dissection approach. It is unlikely, but possible, that the artery and or nerve will be mistakenly cut or damaged. To prevent the BION from moving in the early post-operative period until the tissues stick back down and the spaces developed close up, it will be affixed via a single 5/0 Vicryl suture around the tantalum stem at either end of the implant. It will secure the BION to adjacent connective tissue or gluteus maximus fascia, and must be placed so as not to injure the pedicle. It is unlikely, but possible, that tissue will be damaged during the suturing. We anticipate that both of these 2 stages together will require minimal increased duration (an increased surgical time of 5-10 minutes at most, in a 1-2 hour procedure); or risk (for patients who are undergoing this surgery already).
There is a small possibility that a foreign body reaction to the device may occur; in this case, the device could be removed in a short procedure.

Benefits
A possible benefit for subjects in this study is the possible decrease in pressure wound recurrence, as well as better gluteal muscle health (including increased muscle size and increased blood perfusion) on the stimulated side.
A possible benefit for society is a better understanding of stimulation parameters for this particular application, as well a better understanding of wound healing in general.
Budget
Insert Budget Excel Sheet here

References
100. Levine SP, “Functional Electrical Stimulation for Pressure Sore Inhibition”, USPTO Patent 4,727,878, 1988 March 1 (filed 1985 Sept 26; Assignee: The University of Michigan, Ann Arbor, Mich.).
101. National Decubitus Foundation, “Cost Savings Through Bedsore Avoidance”, National Decubitus Foundation, 4255 S. Buckley Rd., Suite 228, Aurora, CO 80013 (www.decubitus.org/cost/cost.html).
102. Wells C & Hooker S, “The Spinal Injured Athlete”, Adapted Physical Activity Quarterly, 7:265-285, 1990.103. Rimmer J, “Fitness and Rehabilitation Programs for Special Populations”, p.238, Brown and Benchmark,
Madison, WI, 1994.104. Bogie KM et al, “Electrical Stimulation for Pressure Sore Prevention and Wound Healing”, Asst Technol
12:50-66, 2000.105. Bogie KM et al, “Improving the Health of Paralyzed Tissue using Electrical Stimulation”, U.S. Department of
Veterans Affairs, Rehabilitation Research & Development Service, 3rd National Rehabilitation R&D Meeting, www.vard.org/va/02/htm/rrds_feb_2002_confbogie1.htm, Feb 2002.
107. HK DCES IEEE Paper.108. Fourth National PU Prevalence Survey.109. Grays.110. HK dissection.111. Fuhrer, Garber et al '93.112. National Pressure Ulcer Advisory Panel, “Pressure Ulcers: Incidence, economics, Risk Assessment”,
Consensus Development Conference Statement, West Dundee, Illinois, S-N Publications Inc., 1989.113. Stacy RW, "Health & Economic Benefits of FES Induced Active Physical Therapy", 1986.114. 1 in every 3.6 immobile person develop pressure ulcers (Nick).124 National Pressure Ulcer Advisory Panel, “Clinical Practice Guideline on Pressure Ulcers in Adults: Prediction
and Prevention”, www.npuap.org.125. Wilhelmi BJ & Neumeister M, "Pressure Ulcers, Surgical Treatment and Principles", eMedicine,
www.emedicine.com/plastic/topic462.htm, Feb 14 2002.126. U.S. Department of Health and Human Services, "PU Treatment - Quick Reference Guide for Clinicians",
AHCPR Publication No. 95-0653, Rockville, MD, Dec 1994.127. Dharmarajan TS & Ahmed S, “The Growing Problem of Pressure Ulcers – Evaluation & Management for an
Aging Population”, Postgraduate Medicine, Vol. 113,5, May 2003.128. Bergstrom N et al, "Treatment of Pressure Ulcers. Clinical Practice Guideline No. 15", US Dept of Health and
Human Services, Agency for Health Care Policy and Research, Rockville, MD, AHCPR Publication 95-0652, www1.neweb.ne.jp/wb/decubitus/Clinical_Practice_Guideline.htm, 1994.
129. Yarkony GM, “Pressure Ulcers: A Review”, Arch Phys Med Rehabil, 75:908-917, Aug 1994.130. McGraw JB & Arnold PG, “McGraw & Arnold’s Atlas of Muscle and Musculocutaneous Flaps”, Hampton
Press Publishing Company, Inc., Norfolk, VA, 1986.131. Mathes SJ & Nahai F, “Clinical Atlas of Muscle and Musculocutaneous Flaps”, CV Mosby Company, St
Louis, MO, 1979.132. NGC Guideline, "Pressure Ulcer Prevention and Treatment Following Spinal Cord Injury", National Guideline
Clearinghouse (evidence-based clinical practice guidelines), Agency for Healthcare Research & Quality, U.S. Department of Health & Human Services, American Medical Association, American Association of Health Plans, www.guideline.gov/summary/summary.aspx?doc_id=2589&nbr=1815, Dec 2003.
133. Disa JJ, Carlton JM, Goldberg NH, “Efficacy of Operative Cure in Pressure Sore Patients”, Plastic & Reconstructive Surgery, 89(2):272-8, Feb 1992; Comment in: Plast Reconstr Surg. 1992 Nov;90(5):930.
134. Olshansky K, “Essay on Knowledge, Caring, & Psychological Factors in Prevention & Treatment of Pressure Ulcers”, adapted from Panel Discussion at 2nd Annual Wound Healing Symposium, Medical College of Virginia, Richmond, VA, www.woundheal.com/pubs/bedsorePub01.htm, May 1993.
135. Vohra RK & McCollum CN, “Fortnightly Review: Pressure Sores”, British Medical Journal, 309:853-857, http://bmj.bmjjournals.com/cgi/content/full/309/6958/853#R64, Oct 1994.
136. Relander M, Palmer B. Recurrence of surgically treated pressure sores. Scand J Plast Reconstr Surg 1988;22:89-92.
137. Luscher NJ, de Roche R, Krupp S, Kuhn W, Zach GA. The sensory tensor fasciae latae flap: a 9-year follow-up. Ann Plast Surg 1991;26: 306-11.

138. Leasavoy MA, Dubrow TJ, Korn HN, Cedars MG, Castro DJ. "Sensible" flap coverage of pressure sores in patients with meningomyelocele. Plast Reconstr Surg 1990;85:390-4.
150. National Pressure Ulcer Advisory Panel, "Pressure Ulcers in America: Prevalence, Incidence and Implications for the Future", Cuddigan, J., Ayello, E.A., & Sussman, C. (Eds.), Reston VA: NPUAP, 2001.