Embed Size (px)
Citation preview

Proteinuria as a surrogate Proteinuria as a surrogate outcome in CKDoutcome in CKD
UKPDSUKPDS
Rudy BilousRudy Bilous
Middlesbrough, UKMiddlesbrough, UK

UKPDS - DefinitionsUKPDS - Definitions
Microalbuminuria (MAU)Microalbuminuria (MAU) > 50 mg/L> 50 mg/L Clinical Proteinuria (CP)Clinical Proteinuria (CP) >300 mg/L>300 mg/L Spot urine sample annuallySpot urine sample annually Albumin concentration (ACR not reported)Albumin concentration (ACR not reported) Immunoturbidimetry 1988 (RIA previous)Immunoturbidimetry 1988 (RIA previous) Lower limit 2 mg/L Lower limit 2 mg/L CV 3.1 – 6.5% over range 4.4–136.7 mg/LCV 3.1 – 6.5% over range 4.4–136.7 mg/L

UKPDS - OutcomesUKPDS - Outcomes
Fatal / non fatal renal failure Fatal / non fatal renal failure (plasma creatinine > 250 (plasma creatinine > 250 M and/or RRT)M and/or RRT)
Aggregate microvascular (above +/or vitreous Aggregate microvascular (above +/or vitreous haemorrhage +/or photocoagulation.)haemorrhage +/or photocoagulation.)
Surrogate endpoints Surrogate endpoints (new MAU, CP, doubling plasma creatinine)(new MAU, CP, doubling plasma creatinine)
Latterly estimated creatinine clearance Latterly estimated creatinine clearance (eCrCl – CG formula) < 60 ml/min/1.73m(eCrCl – CG formula) < 60 ml/min/1.73m22
Reported per triennium, or B/L to year, or event Reported per triennium, or B/L to year, or event rate per number at a given time pointrate per number at a given time point

UKPDS OutcomesUKPDS Outcomes
No impact on primary renal outcomes of No impact on primary renal outcomes of either intensive glycaemic or tight blood either intensive glycaemic or tight blood pressure controlpressure control
Combined microvascular outcome heavily Combined microvascular outcome heavily weighted by photocoagulationweighted by photocoagulation

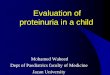
UKPDS Patient Randomisation for Glycaemic Control Study
Lancet 1998; 352 : 837-53

Glycaemic Control Trial 1Glycaemic Control Trial 1
ConventionalConventional
N = 1138N = 1138
IntensiveIntensive
N = 2729N = 2729
Baseline MAUBaseline MAU
UAC > 50mg/LUAC > 50mg/L
UncorrectedUncorrected
12.4 %12.4 %
(127)(127)
11.3 %11.3 %
(273)(273)
Baseline CPBaseline CP
UAC > 300mg/LUAC > 300mg/L
UncorrectedUncorrected
2.1 %2.1 %
(21)(21)
1.7 %1.7 %
(40)(40)

Glycaemic Control Trial 2Glycaemic Control Trial 2Conv’lConv’l IntensiveIntensive RRRR pp
HbA1c HbA1c Median Median 10y10y
7.9 %7.9 % 7.0 %7.0 % -- < 0.0001< 0.0001? t test? t test
Microvascular Microvascular endpointsendpoints
8.68.61000 pt yrs1000 pt yrs
11.411.41000 pt yrs1000 pt yrs
0.750.75(0.60-0.93)#(0.60-0.93)#
< 0.01< 0.01Log rankLog rank
MAU 9 y % MAU 9 y % ( number)( number)
25.4%25.4%(183/721)(183/721)
19.2%19.2%(338/1759)(338/1759)
0.760.76(0.62-0.91)*(0.62-0.91)*
< 0.001< 0.00122
CP 9 y %CP 9 y %(number)(number)
6.5%6.5%(47/721)(47/721)
4.4%4.4%(77/1759)(77/1759)
0.670.67(0.42-1.07)*(0.42-1.07)*
< 0.03< 0.0322
x2 PCr 0 -9y% x2 PCr 0 -9y% (number)(number)
1.76%1.76%(11/625)(11/625)
0.71%0.71%(11/1547)(11/1547)
0.400.40(0.14-1.20)*(0.14-1.20)*
< 0.03< 0.0322
(# 95 % CI ; * 99 % CI)x2PCr = doubling plasma creatinine

Copyright ©1998 BMJ Publishing Group Ltd. UK Prospective Diabetes Study Group, BMJ 1998;317:703-713
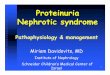
UKPDS Patient Randomisation to BP Study

Blood Pressure Trial 1Blood Pressure Trial 1
Less TightLess Tight
<180/105mmHg<180/105mmHg
N = 390N = 390
TightTight
<150/85 mmHg<150/85 mmHg
N = 758N = 758
Baseline MAUBaseline MAU
UAC > 50 mg/LUAC > 50 mg/L
CorrectedCorrected
16 %16 %
(53)(53)
18 %18 %
(114)(114)
Baseline CPBaseline CP
UAC >300 mg/LUAC >300 mg/L
CorrectedCorrected
4 %4 %
(13)(13)
3 %3 %
(18)(18)
UAC corrected to urine creatinine concentration of 8mM

Copyright ©1998 BMJ Publishing Group Ltd. UK Prospective Diabetes Study Group, BMJ 1998;317:703-713
Achieved Blood Pressure in UKPDS BP Study

Blood Pressure Trial 2Blood Pressure Trial 2Less TightLess Tight TightTight RRRR pp
Mean BP 6yMean BP 6y(estimated)(estimated)
156 / 85156 / 85mmHgmmHg
142 / 80142 / 80mmHgmmHg
-- < 0.0001< 0.0001? t test? t test
Microvascular Microvascular endpointsendpoints
19.219.21000 pt yrs1000 pt yrs
12.012.01000 pt yrs1000 pt yrs
0.630.63(0.44-0.89)#(0.44-0.89)#
< 0.01< 0.01? test? test
MAU 6 y % MAU 6 y % ( number)( number)
28.5%28.5%(78/274)(78/274)
20.3%20.3%(110/543)(110/543)
0.710.71(0.51-0.99)*(0.51-0.99)*
< 0.01< 0.01? ? testtest
CP 6 y %CP 6 y %(number)(number)
8.6%8.6%(24/274)(24/274)
5.3%5.3%(29/543)(29/543)
0.610.61(0.31-1.21)*(0.31-1.21)*
0.060.06? ? testtest
x2 PCr 9y %x2 PCr 9y % NSNS NSNS
(# 95 % CI ; * 99 % CI)

Copyright ©1998 BMJ Publishing Group Ltd. UK Prospective Diabetes Study Group, BMJ 1998;317:703-713
Surrogate outcomes in UKPDS BP Study

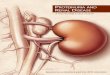
UKPDS Progression 1UKPDS Progression 1 5097 at baseline5097 at baseline 4727 (92.7%) 4727 (92.7%) No nephropathy No nephropathy 333 (6.5 %) 333 (6.5 %) MAU MAU (UAC > 50 mg/L)(UAC > 50 mg/L) 37 (0.7 %) 37 (0.7 %) CP CP (UAC > 300 mg/L)(UAC > 300 mg/L) At 10.4 yrs median follow up :At 10.4 yrs median follow up : 867867 MAUMAU 264264 CPCP 7171 Plasma Creatinine > 175Plasma Creatinine > 175MM 1414 Renal Replacement TherapyRenal Replacement Therapy 1717 Renal DeathsRenal Deaths

Progression rates for 5097 newly diagnosed Type 2 diabetic patients in UKPDS. Adler AI et al Kidney Int 2003 ; 63 : 225 - 32

UKPDS Progression 2UKPDS Progression 2
BaselineBaselineN = 5097N = 5097
5 yrs5 yrsN = 4791N = 4791
10 yrs10 yrsN = 2799N = 2799
15 yrs15 yrsN = 435N = 435
MAU or worseMAU or worse 7.3 %7.3 %(370)(370)
17.3 %17.3 %(830)(830)
24.9 %24.9 %(696)(696)
28.0 %28.0 %(122)(122)
CP or worseCP or worse 0.7 %0.7 %(37)(37)
3.1 %3.1 %(149)(149)
5.3 %5.3 %(148)(148)
7.1 %7.1 %(31)(31)
PCr > 175PCr > 175M M or RRTor RRT
00 0.4 %0.4 %(19)(19)
0.8 %0.8 %(22)(22)
2.3 %2.3 %(10)(10)

UKPDS Progression 3UKPDS Progression 3
Proportion alive Proportion alive at 10 yrsat 10 yrs
Years spent in Years spent in stage (IQR)stage (IQR)
No nephropathyNo nephropathy 87.1 %87.1 % 18.9 18.9
(7.8 – 37.8)(7.8 – 37.8)
MAUMAU 70.8 %70.8 % 10.9 10.9
(4.5 – 21.8)(4.5 – 21.8)
CPCP 65.1 %65.1 % 9.7 9.7
(4.0 – 19.4)(4.0 – 19.4)
PCr > 175PCr > 175M or M or RRTRRT
8.5 %8.5 % 2.5 2.5
(1.0 – 5.0)(1.0 – 5.0)

UKPDS Progression 4UKPDS Progression 4
38 % of 4031 developed MAU at 15 yrs38 % of 4031 developed MAU at 15 yrs 64 % had eCrCl > 60 ml/min/1.73m64 % had eCrCl > 60 ml/min/1.73m22
24 % had eCrCl < 60 ml/min/1.73m24 % had eCrCl < 60 ml/min/1.73m2 2 after MAUafter MAU 12 % had eCrCl < 60 ml/min/1.73m12 % had eCrCl < 60 ml/min/1.73m22 pre MAU pre MAU
29 % of 5032 developed reduced eCrCl 29 % of 5032 developed reduced eCrCl < 60 ml/min/1.73m < 60 ml/min/1.73m22 at 15 yrs at 15 yrs
51 % had UAC < 50 mg/L51 % had UAC < 50 mg/L 16 % had UAC > 50 mg/L after reduced eCrCl16 % had UAC > 50 mg/L after reduced eCrCl 33 % had UAC > 50 mg/L pre reduced eCrCl33 % had UAC > 50 mg/L pre reduced eCrCl
Thus MAU does not always precede declining Thus MAU does not always precede declining renal function renal function

Proportion of patients reaching a renal event in UKPDS. 4032 with no albuminuria, 5032 with normal plasma creatinine at baseline. Microalbuminuria >50mg/L, macroalbuminuria > 300 mg/L, reduced CrCl < 60 ml/min. Retnakaran et al Diabetes 2006 ; 55 : 1832 - 9

UKPDS Progression 5UKPDS Progression 5MAUMAU
756 events756 events
CPCP219 events219 events
CrClCrCl584 events584 events
Age atAge atPer 5 yPer 5 y
__ __ 2.152.15(1.98-2.31)(1.98-2.31)
Male sexMale sex 1.181.18(1.01-1.39)(1.01-1.39)
1.471.47(1.06-2.02)(1.06-2.02)
0.550.55(0.42-0.75)(0.42-0.75)
Indo AsianIndo Asian 2.022.02(1.59-2.60)(1.59-2.60)
2.072.07(1.36-3.15)(1.36-3.15)
1.931.93(1.38-2.72)(1.38-2.72)
WaistWaistcmcm
1.011.01(1.004-1.016)(1.004-1.016)
1.0161.016(1.006-1.026)(1.006-1.026)
0.950.95(0.94-0.96)(0.94-0.96)
SmokingSmoking 1.201.20(1.01-1.42)(1.01-1.42)
__ 1.251.25(1.03-1.52)(1.03-1.52)
Stepwise proportional hazards regression model . HR with 95 % CI

UKPDS Progression 6UKPDS Progression 6MAUMAU
756 events756 events
CPCP219 events219 events
CrClCrCl584 events584 events
UACUACPer 20 mg/LPer 20 mg/L
1.0041.004(1.002-1.007)(1.002-1.007)
1.0091.009(1.005-1.012)(1.005-1.012)
1.0091.009(1.002-1.015)(1.002-1.015)
Plasma CrPlasma CrPer 10 Per 10 MM
__ 1.0871.087(1.005-1.175)(1.005-1.175)
1.341.34(1.28-1.40)(1.28-1.40)
Systolic BPSystolic BPPer 10 mmHgPer 10 mmHg
1.151.15(1.11-1.20)(1.11-1.20)
1.151.15(1.07-1.24)(1.07-1.24)
1.1071.107(1.06-1.16)(1.06-1.16)
LDLCLDLCmMmM
__ 1.171.17(1.02-1.18)(1.02-1.18)
__
TriglycerideTriglyceridemMmM
1.091.09(1.04-1.14)(1.04-1.14)
1.151.15(1.09-1.21)(1.09-1.21)
__
Stepwise proportional hazards regression model . HR with 95 % CI

UKPDS CaveatsUKPDS Caveats
Primary renal outcomes too infrequentPrimary renal outcomes too infrequent Mix of therapeutic and pathological Mix of therapeutic and pathological
microvascular outcomesmicrovascular outcomes Surrogate renal outcome used urinary Surrogate renal outcome used urinary
albumin concentration with high cut offalbumin concentration with high cut off No allowance of impact of antihypertensive No allowance of impact of antihypertensive
therapies on UACtherapies on UAC

UKPDS ConclusionsUKPDS Conclusions
Strong evidence of effectiveness of Strong evidence of effectiveness of glycaemic and BP control in prevention of glycaemic and BP control in prevention of increases in albuminuriaincreases in albuminuria
Significant reduction in those doubling Significant reduction in those doubling plasma creatinine (albeit small numbers)plasma creatinine (albeit small numbers)
Demonstration of poor prognosis for those Demonstration of poor prognosis for those with worsening renal functionwith worsening renal function
Relatively slow progression of albuminuria Relatively slow progression of albuminuria toward renal impairment in T2DMtoward renal impairment in T2DM
Discordance between eCrCl and UAC Discordance between eCrCl and UAC

BibliographyBibliography Intensive blood-glucose control with SUs or Intensive blood-glucose control with SUs or
insulin …. UKPDS 33. insulin …. UKPDS 33. Lancet 1998 : 352 : 837-53Lancet 1998 : 352 : 837-53
Tight blood pressure control….UKPDS 38 Tight blood pressure control….UKPDS 38 BMJ 1998: 317 : 703 – 13BMJ 1998: 317 : 703 – 13
Development and progression of Development and progression of nephropathy… UKPDS 64. Adler AI et al nephropathy… UKPDS 64. Adler AI et al KI 2003 : 63 : 225-32KI 2003 : 63 : 225-32
Risk Factors for renal dysfunction …. Risk Factors for renal dysfunction …. UKPDS 74. Retnakaran R et al UKPDS 74. Retnakaran R et al Diabetes 2006 : 55 : 1832 - 9Diabetes 2006 : 55 : 1832 - 9