Embed Size (px)
Citation preview

Prosthetic Substitution of Thoracic Esophagusin Puppies: '
Use of Marlex Mesh with Collagen or Anterior Rectus Sheath
JULIUS LISTER, M.D., R. PETER ALTMAN,** M.D.,WV. ANTHONY ALLISON, M.D.
From the Department of Surgery, Tufts University School of Medicine, BostonFloating Hospital, and the Laboratories of Surgical Research, Harvard
Medical School, Peter Bent Brigham Hospital
THERE EAR several circumstances underwhich it is necessary to bridge a gap in theesophagus of the very young. In esophagealatresia without fistula the two blind endsof esophagus are ordinarily too far apart tobe sutured together directly. In instancesin which the esophageal ends must bebrought together under some degree oftension the chances of ultimate success ofthe operation are reduced to less thanoptimal. In order to lessen the tension atthe anastomosis, as much existing esopha-gus as possible must be preserved, and thenarrowed, dysplastic portion of the distalesophageal segment that forms the tracheo-esophageal fistula must be used to sutureto the dilated hypertrophic proximal pouch.This occasionally leads to malfunction fol-lowing an otherwise successful repair.18Such malfunction might be avoided if thedysplastic segment of esophagus could beresected and a more distal, more normal,level could be used for anastomosis.The purpose of this report is to describe
an experimental approach to the problemof bridging such esophageal gaps in the
* Submitted for publication November 16,1964.
** Postdoctoral Fellow, National Institute ofChild Health and Human Development.
Supported by USPHS Grant HD 00410 of theNational Institute of Child Health and HumanDevelopment.
812
young. Previous studies have usually beenundertaken with a view to re-establishmentof esophageal continuity in cases of re-sected carcinoma or stricture.'2 14, 23, 27Over the last 100 years a wide gamut ofmaterials has been used experimentally toreplace circumferential defects in this vitalorgan, both in the human and in animals.The earliest experimental attempts in-cluded the use of decalcified ivory tubesin 185428 and since that time variousmetals 6, 7, 8, 25 and plastics 1, 3, 4, 21, 24 as wellas pedicled and revascularized grafts oftissue have been utilized.9 15, 17 In most in-stances the results have been disappoint-ing."' 23 In the human studies the patientshave, by and large, been elderly and de-bilitated and have had metastatic disease.
Several animal studies have been re-ported with a somewhat greater degree ofsuccess. Neuhof and Ziegler 22 were ableto re-establish continuity of the cervicalesophagus in dogs, using rubber tubes. Es-tablishment of mediastinal adhesions in apreliminary stage was necessary to preventfatal mediastinitis. Boyd 5 reported substi-tutions of the thoracic esophagus in pigs,with several types of prosthesis. His bestresults were with a two-layer tube consist-ing of an inner Plexiglas lining and anouter coat of plastic foam. Lyons and hisgroup 20 replaced segments of the thoracicesophagus in dogs with various postheses,

Volume 162 PROSTHETIC SUBSTITUTION OF THORACIC ESOPHAGUS IN PUPPIESNumber 5
including steel coils, Silastic, Tygon andpolyethylene, with inconsistent results. Fry-fogle et al.10 also reported replacement ofsegments of the thoracic esophagus in dogsand used silicone rubber prostheses ofvarying rigidity. The studies reported haveused adult animals, and survival, ratherthan growth and development, has beenthe central thesis of the reports.
In instances of esophageal atresia inwhich the gap between the discontinuousends of the esophagus mitigates against di-rect primary suture and in instances ofextensive stricture of the esophagus in chil-dren, the problem of bridging the esopha-geal defect is compounded by the necessi-ties of growth and development. Appropri-ate alimentation over a lifetime must beconsidered and one cannot be contentmerely with a passageway that permitsgustatory sensation for the limited dura-tion of an inevitably fatal malignant lesion.The initial size of the replaced esophagusmust be adequate, and it must be able topermit appropriate alimentation even as
the individual grows.It seemed important, therefore, to evalu-
ate prosthetic replacement in the animalwith a growth potential. On a theoreticalbasis, it was believed that an appropriateprosthetic tube needed to be semi-rigid inorder to prevent early leak at the proximalanastomosis, since there is no consistentintraluminal pressure in the esophagus tokeep a non-rigid prosthetic tube distended.One could anticipate that collapse of sucha tube would be obstructive and wouldcause proximal anastomotic leak. This theo-retical consideration seems to have beenborne out by previous studies.28
Other desirable characteristics of pros-thetic materials such as biologic inertnessand electrical neutrality have been thor-oughly covered in reviews of this field.16The alternatives of constructing the pros-
thetic tube of solid plastic sheet or ofwoven mesh were carefully considered.Potential contamination of the mediastinum
and pleural space through an open meshfavored the use of a tube with an im-permeable wall. On the other hand, if theprosthesis was to become incorporated intothe wall of the esophagus, a woven meshwould be necessary. Furthermore, the ideaof a woven mesh was more compatible withease of suturing to the esophageal wall.The work of Beall et al.2 and Harring-
ton et al.13 Nwrith the use of heavy Marlexmesh in circumferential replacement ofthe trachea, and the report of Sheena etal.26 in similar replacement of the cervicalesophagus in adult dogs, suggested thatthis material might be appropriate for thereplacement of segments of the thoracicesophagus in young animals.A series of experiments was undertaken
in which tubes of Marlex mesh were usedto substitute for excised segments of thethoracic esophagus in young puppies, andthe survivors of such substitution were ob-served for varying periods of time. Primaryattention was directed to the ability of theanimals to eat and gain weight, to evalua-tion of swallowing function by cine-esopha-grams and to gross and microscopic ex-
amination of the esophagus at varyingperiods following replacement.
Materials and Method
Marlex,* a linear polyethylene of highmolecular weight, extruded as a monofila-ment with a diameter of 0.67 mm. andwoven into a coarse, semi-rigid mesh, was
either heat-sealed or sewn into tubes meas-
uring 2 cm. in diameter and 5 cm. in length.Six- to 10-week-old puppies, weighing
between 7 and 12 pounds, were used as
experimental animals. Throughout most ofthis period mongrel pups were used. Thelast two animals operated upon were pure-
bred beagles. The puppies were procuredfrom various sources in the Boston area andwere in widely varying states of healthwhen they arrived in the laboratory. All
* Kindly provided by Dr. A. C. Beall, Jr.
813

LISTER, ALTMAN AND ALLISON Annals of SurgeryNovember 1965
)~
g
*= E Q
C,3
0
co ._,C
814

Volume 162 PROSTHETIC SUBSTITUTION OF THORACIC ESOPHAGUS IN PUPPIESNumber 5 815
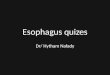
FIG. 2. (Left) Radiograph of a barium swallow 1 year after resection of a segment of thoracicesophagus and replacement with a prosthetic tube. There is dilatation of the esophagus proximal to thesite of substitution, which is represented by a very short narrowed segment. There is very little differ-ence in diameter between this segment and the distal esophagus. Cine studies showed prompt pas-sage of the dye across the narrowed area.
FIG. 3. (Right) Barium swallow x-ray 1 year after prosthetic substitution. The site of originalresection is marked only by irregularity of the esophageal wall.
animals were observed for several daysprior to operation, and if clearly diseasedwere not used. Complete courses of anti-sera against distemper and hepatitis viruseswere administered, and doses of toxoidwere given.
Forty-one puppies were operated upon(Fig. 1). The first group of 24 animalswere anesthetized with ether deliveredthrough a copper kettle via an endotrachealtube. Intubation was accomplished afterintravenous administration of 3 to 5 ml. ofsodium pentothal. A Harvard respiratorwas used and was adjusted to provide ade-quate ventilation of the lungs after thechest was opened. All animals were sub-jected to right lateral thoracotomy andtranspleural approach to the esophagus.The azygos vein was divided, a longitudinalincision was made in the parietal pleuraand an 8 to 10-cm. segment of the thoracicesophagus was removed. Marlex mesh
tubes, 5 cm. in length and 2 cm. in diameter,were sutured in continuity with the cutends of the esophagus. Each anastomosiswas accomplished with a single layer ofinterrupted sutures of 5-0 arterial silk. Thetubes were sutured into place within thelumen with an overlap at each end of ap-proximately 2 mm. The parietal pleura wasthen approximated with several sutures of5-0 silk and the chest was closed in layerswithout an intercostal tube in most in-stances. In several cases because of oozingof blood a No. 14 French catheter wasplaced through a separate stab wound andwas connected to underwater seal untilthe puppies had completely reacted, afterwhich the tubes were removed.Animals were kept without food or drink
for the first 5 postoperative days and weregiven 400,000 units of crystalline penicillinand 0.50 Gm. of streptomycin daily for 5days. During this period fluids were ad-

LISTER, ALTMAN AND ALLISON Annals of SurgeryNovember 1965
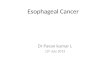
F1G. 4. (Top) Low-power photomicrograph of a section across the area of esophageal substitution1 year postoperatively. Normal esophageal layers are separated by a 2-mm. length in which theepithelium is thinner than normal. The underlying fibrosis contains disorderly bundles of skeletal musclefibers.
FIG. 5. (Bottom) Low-power photomicrograph showing hypertrophy of the muscularis proximal tothe substituted site. The stenotic segment is very short and the epithelium is intact (the apparentdiscontinuity is artifactual).
ministered subcutaneously. On the sixthday small amounts of water were offeredby mouth, and if tolerated, larger feedingsof milk were given. On the seventh daystrained meats were begun, and the quan-
tity was gradually increased until thepuppy was offered all the meat that he
would take.The 17 animals comprising the second
phase of the experiment were anesthetizedwith fluothane delivered through a copperkettle or Fluotec, by a technic describedelsewhere.19 No barbiturates were used.The exposure of the esophagus and the in-sertion of the Marlex tubes were similar to
those in the first group. In the first sevenanimals a sheet of compressed collagenwas sutured into place around the Marlextube. A single row of interrupted 5-0 silksutures was used to fix the collagen to themuscularis on the esophageal side of eachanastomosis, and a row of sutures joinedthe collagen to itself in a longitudinal seam.
In the remaining ten puppies a rectangu-lar piece of anterior rectus sheath was re-
moved through a paramedian abdominalskin incision and was sutured around theMarlex tube in similar fashion to the col-
' Kindly provided by Ethicon, Inc.
816

Volume 162 PROSTHETIC SUBSTITUTION OF THORACIC ESOPHAGUS IN PUPPIESNumber 5
lagen. The immediate postoperative treat-ment of these animals was identical to thatemployed in the first group.
The surviving animals of the first groupwere observed in the laboratory until 6weeks postoperatively when they were
transferred to an animal farm. They were
kept there until 1 year after the initial op-
eration when they were brought back tothe laboratory for further study. The sur-
vivors of the remaining group were ob-served within the animal laboratory untilthey died or were sacrificed. Animals were
classified as survivors if they lived beyondthe 30th day after esophageal substitution.
Results
Group I: Marlex Mesh Alone
In the first group of 24 animals, six(25%o) survived the first month and all ofthese went on to survive for 1 year, afterwhich they were subjected to reoperation.Those that failed to survive died within thefirst 48 hours after operation in all but one
instance. Three animals had cardiac arrestsduring operation and could not be resusci-tated. The remaining 15 were all foundto have extensive empyema, fibrinous ad-hesions and atelectasis bilaterally (moremarked on the right side) at postmortemexamination. One of these was doing wellclinically and had begun to receive strainedmeat by mouth when he died suddenly 7days after operation. At postmortem ex-
amination most of the administered foodwas found in his right pleural space. Ex-amination of the esophagus revealed a con-
siderable walling off of the Marlex tube,with incorporation of two thirds of the cir-cumference of the tube and its entirelength by fibrosis. On the right lateral as-
pect, however, there was no fibrosis, andthis apparently was the site of contamina-tion of the pleural space.
The clinical course of the surviving ani-mals in this group varied in the first sev-
eral postoperative days. Some puppies were
active and appeared well from. the earlypost-anesthetic hours. Others were febrileand lethargic for the first 24 hours butgradually recuperated. The feeding pat-tern in this group was similar to that ob-served by Neuhof.22 From the second tothe fourth or fifth weeks most meals were
followed by regurgitation and then re-
feeding. All animals began to gain weightin the second week, and by the sixth weeklittle or no regurgitation was noted. Canneddog meat was begun in the fifth or sixthweek in all instances. At first this wasgiven as a thick gruel by mixing with milkin a blender, but a transition was gradu-ally made to standard dog meat, afterwhich the animals were moved to the ani-mal farm.During the ensuing 10 or 11 months the
animals gained weight steadily and grewinto normal-appearing adult dogs. By theend of a year the weights varied from 28to 38 pounds and represented an averagethree-fold increase from the time of thefirst operation. One of the three femalescame into heat at 10 months of age.Cine-esophagrams at the end of a year
revealed relative narrowing, varying fromminimal to moderate, at the site of replace-ment (Fig. 2, 3). In each instance thenarrowed segment was short in length.Varying degrees of dilatation of the esopha-
gus proximal to the area were seen, butpassage of the barium across the site ofprosthetic replacement was always prompt.
After 1 year, re-exploration was carriedout through a right thoracotomy. In eachinstance there were extensive adhesions be-tween the pleural layers. The esophaguswas dissected free and a long segment was
removed for gross and microscopic exami-nation.
In no instance was the Marlex tubefound within the gastrointestinal tract. Thearea of prosthetic replacement was markedby a short segment of narrowing of theesophageal wall, varying in length fromto 3 mm. There was minimal to marked
817

LISTER, ALTMAN AND ALLISON Annals of SurgeryNovember 1965
FIG. 6. Higher-power photomicrograph of the section shown in Fig. 7 at the junction of the proximalesophageal segment and the anastomotic site.
dilatation of the esophagus proximal to thenarrowed segment, and the distal esophagusappeared normal. The lumen at the nar-rowed site varied in diameter from 2 to 3cm. In all specimens the mucosa wasgrossly intact.
Microscopic examination (Fig. 4-6) ofthe esophageal wall revealed a continuouslining of stratified squamous epithelium,thinned at the site of narrowing. There wasa varying degree of muscular hypertrophyproximal to the narrowed segment, and thenarrowed segment itself was representedby submucosal overgrowth of fibrous con-nective tissue in which scattered and dis-organized bundles of skeletal muscle tis-sue were seen. No distinct muscular layerbridged the short anastomotic segments.
The microscopic appearance of the distalesophagus was normal.
Group II: Marlex Surrounded by Col-lagen or Anterior Rectus Sheath
Of the seven animals in which the Marlexprosthesis was surrounded with sheets ofcompressed collagen, five died within 48hours of empyema. At the time of post-mortem examination the collagen wasfound to be in varying states of dissolution,with gross leaking through the intersticesof the underlying tube. Two puppies inthis group survived for 12 and 14 days,respectively. The clinical course of deathin both was that of advancing neurologicsigns, and a diagnosis of distemper was
818

Volume 162 PROSTHETIC SUBSTITUTION OF THORACIC ESOPHAGUS IN PUPPIESNumber 5
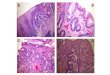
FIG. 7. Photograph ofa sagittal section throughthe thoracic esophagusexcised 3 weeks afterprosthetic substitution.The inner aspect of theMarlex tube can be seenand is incorporated byfibrous connective tissue.The outer aspect hasbeen sharply dissectedfrom the mediastinumand the esophagus hasbegun to grow over theends of the prosthesis.
made by our consultant veterinariaipostmortem examination there was n(
dence of empyema or pleural adheThe Marlex tubes were surrounded ar
corporated by ingrowing fibrosis, an(
esophagi had to be sharply dissectedthe surrounding structures of the metinum.
In the remaining ten puppies the Mprosthesis was encircled by a rectanganterior rectus sheath. Seven of thesemals (70%) survived 30 or more pc
erative days. One of the early deathcurred on the seventh postoperativeand postmortem examination revealedpyema and atelectasis. One of the su
fixing the rectus fascia to the esopEacross the proximal anastomosis had brand the graft was exposed. Another ardied on the second postoperative dayalso was found to have empyema andfect in the rectus fascia at the sitetear inadvertently made when the r
sheath was taken from the abdominalThe third death was in the fourthoperative week and was due to distenAt postmortem examination there wa
evidence that empyema had occurredpleural adhesions were minimal. Thethesis was completely infiltrated with fsis and there was fixation by fibrou,corporation of the prosthesis to therounding mediastinal structures. The r
sheath could not be delineated as a discretestructure (Fig. 7). The ingrowing eso-phageal wall overlapped each end of theprosthesis by about 1 cm., leaving a 21/2-cm. length of fibrosis between the advanc-ing mucosal edges.The seven survivors did well in the early
postoperative period. They were all begunon oral feedings on the sixth day. In twoanimals there was mild regurgitation offeedings in the third and fourth postopera-tive weeks, respectively. One animal con-tinued to vomit (Puppy 26) and died ofinanition 2 months postoperatively. An-other (Puppy 30) did not vomit until 21'2months after operation, at which time herequired re-exploration.
Survivors. Puppies were observed fordifferent intervals up to 5 months in orderto study the progress of the grafted esopha-gus. Since their courses varied, they willbe described individually.
Puppy 21 bad a completely benign postopera-tive course. Serial eine-esophagrams showed goodswallowing function. He was re-explored 3 monthspostoperatively-the graft was still in place, thetwo encroaching ends of esophagus were sepa-rated by approximately 3 mm. of fibrosis and overthis fibrotic area the waist of the graft was stillfixed. A biopsy was taken. The esophageal defectthus created was sutured together with inter-rupted sutures of 5-0 silk and the chest was
closed. There were no adhesions between thepleural surfaces except at the site of previous
819
--A Is,
.0..oOK
..
1."INEW-.+. %. .,Awla,-10 -.1-1Q.
.. -%,.;; lw -.,:. 4 ...Oqp
,!, ."O. :i VW`.a-,:; % bk

820 LISTER, ALTMAN AND ALLISON
FIG. 8. (Top) Radiograph of a barium swallowmade 3 weeks after esophageal prosthetic substitu-tion. Barium passes through and around the tubeand there is walling off of the operated site.
FIG. 9. (Bottom) Barium swallow x-ray madenearly 3 months after esophageal substitution,showing marked stenosis. The prosthetic tube isno longer present. At re-exploration there wassufficient esophageal length to permit resection ofthe stenotic segment and end-to-end anastomosis.
Annals of SurgeryNovember 1965
pleural closure. After the second operation thepuppy continued to do well, and feeding wasstarted again 5 days postoperatively. Postoperativecine-esophagrams continued to show good swallow-ing function. The subsequent benign course wasinterrupted by an infection with distemper thatoccurred 5 months after the initial prosthetic sub-stitution and eventuated in the death of the ani-mal. At postmortem examination there were stillvery few pleural adhesions and these were con-fined to areas of pleural suture. There was noevidence of the prosthetic tube and the esophaguswas healed. There was very minimal narrowingover a 2-mm. segment and very little dilatation ofthe proximal esophagus. This puppy weighed 6pounds at the time of initial operation. His weightwas 22 pounds just prior to the onset of his finalillness. Weight gain was progressive throughoutthe period of observation except immediately afterthe second operation.
Puppy 22 also had a completely benign post-operative course. A cine-esophagram was made 3weeks following esophageal substitution and re-vealed the tube to be in place and functioningwell (Fig. 8). The repeat cine-esophagram at 6weeks showed very little change. At 3 monthsanother cine-esophagram was made and againshowed the graft in place. Swallowing functionwas satisfactory. Three and one half months fol-lowing substitution this puppy was again operatedupon. A minimal amount of pleural adhesionswere encountered and the lung appeared normal.The esophagus was healed over the prosthetictube which remained at its original site. On re-moval of the thoracic esophagus and opening ofthe organ, the prosthetic tube was found lyingfree within the lumen. The mesh was completelyinfiltrated by fibrosis but the tube was patent andits lumen was not encroached upon. There wasminimal ulceration of the mucosa where it cameinto contact with the midportion of the prosthetictube, and this appeared to be the remnant of in-complete epithelization. This puppy weighed 10pounds at the time of initial operation and weighed24 pounds immediately prior to the exploratoryoperation.
Puppy 23 did well following esophageal re-placement and was able to tolerate feedings un-eventfully. A cine-esophagram made 6 weeks post-operatively revealed the prosthetic tube to be inplace within the esophagus and to be functioningnormally. At about 8 weeks he began to have anasal discharge and neurologic signs suggested adiagnosis of distemper. He died 2 days later andat postmortem examination the esophagus wasfound to be healed, with the mucosa intact, andthe prosthetic tube was found in the lumen of the

Volume 162 PROSTHETIC SUBSTITUTION OF THORACIC ESOPHAGUS IN PUPPIESNumber 5
stomach. There was minimal narrowing over a2-mm. segment representing the site of prostheticreplacement and no evidence of proximal dilata-tion.
Puppy 24 did well and was able to be ad-vanced in diet according to schedule. He had noregurgitation. Cine-esophagrams at 6 weeks and9 weeks revealed the graft to be in place and tobe functioning adequately. Three weeks later hedeveloped evidence of distemper and died within2 days. At postmortem examination the esophaguswas well healed, the prosthesis was still in placein the esophagus and was only loosely fixed at itswaist.
Puppy 27 was able to tolerate solid feedingsby the sixth postoperative day and a cine-esopha-gram at 3 weeks showed good function across theprosthetic tube. She regurgitated feedings duringthe third postoperative week and demonstrated a
fairly typical pattern of refeeding the regurgitatedmeal and then retaining it. This regurgitation never
quite subsided and gradually became more severe.
When another cine-esophagram was made 6weeks after the esophageal substitution, the pros-
thetic tube was no longer in place within theesophagus and there was an area of marked nar-
rowing over a moderately long segment (Fig. 9).This caused delayed passage of dye, though some
of the dye did pass beyond the stenotic segment.Vomiting was persistent and when the animal was
re-explored on the 45th postoperative day, theimpression of marked narrowing of the esophaguswas confirmed. The proximal esophagus was
dilated and the stenotic area was 2 cm. in length.The lumen was narrowed to a diameter of 1 cm.
and the mucosal surface was intact. The prosthetictube was found within the stomach. This puppy
weighed 6 pounds at the time of initial operationand 10 pounds by the twelfth postoperative day;her weight remained stable for the ensuing 4weeks, dropping finally to 8 pounds at the timeof re-exploration.
Puppies 29 and 30 are, as of this writing,alive 3 months after esophageal substitution.Puppy 29 has never vomited and progressivelyhas gained weight from 12 pounds at the time ofoperation to 23 pounds. Cine-esophagram at 3months showed good function with the graft stillin place.
Puppy 30 began to vomit 21, months followingesophageal substitution. Vomiting since that timehas been progressive and the animal's weight hasdropped from 21 pounds at 10 weeks to 15 poundsat the end of the third postoperative month.Cine-esophagram 1 week after the onset of vomit-ing showed no evidence of the prosthetic tube.There was a tight stenosis at the site of the
esophageal substitution. This puppy was re-ex-plored 3 months after the initial operation. Ad-hesions were minimal. There was tight stenosisover a 2-mm. length of esophagus, with milddilatation proximal to the stenosis. The esophageallength was such as to permit resection of 3 cm. ofesophageal wall proximal and 2 cm. distal to thenarrowed area, and to allow easy direct anasto-mosis of the remaining esophagus. The openedspecimen showed a very tight but short stenoticsegment with an intact mucosal lining.Comment. In most animals there was
radiographic evidence that the prosthetictubes remained in place through the first 3postoperative months. As long as the tuberemained there was no narrowing of thelumen and the bolus of barium appeared topass through and around the tube withminimal delay proximal to the prosthesis.After the prosthesis became dislodged,some luminal narrowing occurred. The de-gree and extent of this narrowing dependedon the length of time during which theprosthesis remained in situ. In Puppy 27the 6-week cine-esophagram indicated thatthe graft was no longer in place and therewas fairly marked narrowing over what ap-peared to be a several-centimeter segment.This animal went on to die 1 week later.In Puppy 30 the prosthesis was no longerpresent at 21/2 months. Stenosis developed,but over a shorter segment. The puppiesthat still had the tube in place at 3 monthsdeveloped little stenosis and little or nofunctional impairment.
Microscopic examination of the resectedspecimens at various intervals after sub-stitution confirmed the serial progression ofevents that were suggested by the grossfindings. In the earliest specimens therewas fibrous incorporation of the Marlexwith fixation to the mediastinum. As thetwo cut ends of esophagus approachedeach other epithelization was complete,and the substituted segment, now muchshorter than the original esophageal defect,was marked by a thin lining of stratifiedsquamous epithelium with underlying fi-brosis. Scattered bundles of skeletal muscle
821

822 LISTER, ALTMAN
fibers were present in the scarred area inall puppies but the one with severe ste-nosis. The esophageal wall proximal anddistal to the substituted site consisted ofnormal-appearing epithelium and muscu-
laris.Discussion
As previously stated, the purpose of thisstudy was to evaluate growth and develop-ment in experimental animals followingprosthetic esophageal substitution in theyoung. The primary concern was not withrate of survival but with observation ofthose animals that did survive. We were
naturally interested in producing as many
survivors as possible so that as a by-productof the study we examined the surgical tech-nics and their effect on survival statistics.
Survival. It appeared that when sur-
vival beyond the immediate postoperativeperiod occurred, a progressive series ofevents within the esophagus could be pre-
dicted. Incorporation of the Marlex meshby fibrosis appeared to occur early and was
complete whenever early leakage throughthe mesh could be prevented, or if the re-
sistance of the animal was such as to per-
mit survival despite empyema. Thus inGroup I no covering was used to surroundthe Marlex tube. Those animals that sur-
vived showed evidence, at re-exploration,of extensive pleural adhesions, which sug-gested that an early empyema had oc-
curred. One fourth of the animals in GroupI survived, and their survival no doubt was
a consequence of host resistance. When a
barrier to leakage was established by en-
circling the tube with an impermeablelayer and when this barrier remained in-tact for the early postoperative period, a
higher percentage of animals could be pre-dicted to survive. Further, in these GroupII animals late examination of the pleuralspaces did not reveal the same evidence ofhealed empyema that was present in GroupI. Anterior rectus sheath provided an ef-fective barrier. Attempts to use compressed
AND) ALLIS;ON Annals of SurgeryNovember 1965
collagen sheets as a temporary impermeablelayer failed in most instances. Most of thecollagen used was untanned. There wasevidence that tanned collagen may providean effective barrier against leaking and per-mit survival. The number of observationswith this material were small and its useis being further investigated. The advantageof a synthetic material is obvious. Theprocurement of fascia is tedious and prob-ably not feasible in the newborn infant.
Establishment of Esophageal Continu-ity. As the Marlex tube became incor-porated into the surrounding mediastinalstructures by fibrosis the ends of the esoph-agus appeared to grow toward each otheron the outer aspect of the implanted tube.The tube was always invaginated into thelumen and this probably accounted for thefact that the esophageal wall grew on theoutside of the tube. Esophageal growthincluded both the mucosal and muscularlayers, and as the advancing edge of epi-thelium passed over the underlying fibrousMarlex tube, the latter peeled away fromthe mucosal surface. When the ingrowingends of esophagus met each other they ap-peared to undergo an auto-anastomosis, atwhich time separation of the tube becamecomplete. The tube then passed downwardinto the stomach. When the animals wereobserved for a long enough period of timethe absence of the tube at postmortem ex-amination suggested that it had beenpassed on out through the lower gastro-intestinal tract.
It appeared to take 3 months for theesophageal auto-anastomosis to be com-plete and for the tube to become dislodged.In two of the instances in which the tubeseparated away prematurely there wasrnarked stenosis and vomiting. The tubecan be thought of as serving as a stent overwhich the cut ends of the esophagus grewtoward each other in an effort to re-estab-lish esophageal continuity.The end result was a single anastomotic

Volume 162 PROSTHETIC SUBSTITUTION OF THORACIC ESOPHAGUS IN PUPPIESNumber S
line. The appearance of the auto-anasto-mosis was similar-on radiographic, grossand microscopic examination-to that of a
direct-suture anastomosis. The gap whichhad been bridged by the Marlex tube was
replaced by a scarred segment, adequate inmost instances to permit sufficient alimenta-tion for growth and development. Whenthe tube became displaced in less than 3months, stenosis was severe. In one case
the displacement occurred very early andthe stenotic segment was relatively long. Inthe other instance, the tube separated awaybetween the sixth and tenth weeks. Thestenotic segment was short and the lengthof the esophagus was adequate to permitdirect anastomosis after resection of thestenosis.The animals in this experiment were ob-
tained through various sources in the Bos-ton area and in general were not availableas litters, so that comparison to nonoperatedlitter mates was not possible. The last twoanimals operated upon were part of a
litter which is under our observation andthis represents the beginning of a series ofsuch controlled studies.
Prosthetic Material. Some commentsconcerning the nature of the prosthetic tubeare in order. As pointed out above, thesemi-rigidity of the tube appeared to beimportant. Preliminary experiments in thislaboratory involved the use of tubes ofcommercially available Marlex mesh andknit. These tubes were collapsible andtheir use always resulted in leakage at the
proximal anastomosis. Tubes of solid plas-tic materials do not permit fibrous incor-poration and must rely on sutures to holdthem in place. The incorporation of a meshby fibrosis aids importantly in the functionof the prosthetic tube as a long-term stent.Sutures become broken and dislocated andthe 3-month period during which the stentmust remain in place would appear tomake even the most nonabsorbable suturesunreliable in this regard.
Summary and ConclusionsForty-one 6- to 10-week-old puppies were
subjected to replacement of 10-cm. defectsin the thoracic esophagus with tubes ofheavy Marlex mesh, 5 cm. in length and2 cm. in diameter. Thirteen of the animals(327%) survived beyond the first 30 post-operative days and were studied for vary-ing periods up to 1 year.
The prostheses at first became incor-porated by fibrosis. The cut ends of esopha-gus grew toward each other on the outeraspect of the prosthetic tubes and eventu-ally met to form auto-anastomoses. Thefibrosed prostheses served as stents whileesophageal ingrowth was occurring, gradu-ally peeling away from the advancingepithelization. When separation was com-
plete, the prosthetic tubes passed throughthe gastrointestinal tract. The end resultwas usually a single anastomotic line, simi-lar in radiographic, gross and microscopicappearance to that of an ordinary anasto-mosis created by direct suture.
Stenosis occurred in those instances inwhich the prosthetic stent became dis-placed prior to 3 months after esophagealsubstitution. The extent and severity ofstenosis increased as the period duringwhich the stent was in situ became shorter.
In 11 of the 13 survivors, weight gainwas progressive and development proceedednormally. Of the six animals studied for1 year following substitution there was an
average weight gain of 20 pounds, repre-
senting a three-fold increase.When tubes of heavy Marlex mesh were
used as single layered prostheses, 25 per
cent of the animals survived. Those thatdied succumbed to empyema caused byleakage through the interstices of the tube.When sheets of compressed collagen
were used as outer layers to prevent leak-age, none of the animals survived. In fiveinstances the collagen was untanned andthere was early disintegration of the col-lagen with development of empyema anddeath within 48 hours. In two instances
823

LISTER, ALTMAN AND ALLISON Annals of Surgery824 LSE,November 1965
tanned collagen was used. These animalsdied of distemper at 12 and 14 days, re-spectively. There was no evidence of em-pyema and fibrous incorporation of theprostheses was complete, suggesting thatappropriate tanning should render thismaterial an effective barrier against leak.
Rectangles of anterior rectus sheath, re-moved from the abdominal wall at thetime of the esophageal substitution, pro-vided a successful outer impermeable layerfor the prostheses. Seventy per cent of theanimals in which this material was usedsurvived beyond 30 days. Two of the fail-ures represented technical errors in ob-taining and suturing the fascial layer. Athird animal died in the fourth postopera-tive week of distemper and showed goodprogress toward auto-anastomosis of theesophageal ends at postmortem examina-tion.A method is described for bridging de-
fects of the esophagus in young puppies.Long-term studies showed adequacy of theesophageal lumen, and growth and de-velopment were supported by normal feed-ing.
References1. Battersby, J. S. and H. King: Esophageal Re-
placement with Plastic Tubes. Arch. Surg.,69:400, 1954.
2. Beall, A. C., Jr., 0. B. Harrington, S. D.Greenberg, G. C. Morris, Jr. and F. C.Usher: Tracheal Replacement with HeavyMarlex Mesh: Circumferential Replacementof the Cervical Trachea. Arch. Surg., 84:390, 1962.
3. Berman, E. F.: The Experimental Replace-ment of Portions of the Esophagus by aPlastic Tube. Ann. Surg., 135:337, 1952.
4. Berman, E. F.: Plastic Prosthesis in Carcinomaof the Esophagus: Surg. Clin. N. Amer.,36:883, 1956.
5. Boyd, T. F.: A Prosthesis for Replacement ofthe Intrathoracic Esophagus. Surg. Forum,13:256, 1962.
6. Braunwald, N. S. and C. A. Hufnagel: Re-construction of the Esophagus with WireMesh Prosthesis. Surgery, 43:600, 1958.
7. Brown, A. L.: Carcinoma of the Esophagus:Use of Rigid Indwelling Esophageal Tube.J. Thor. Surg., 18:493, 1949.
8. Edgerton, M. T.: One-Stage Reconstructionof the Cervical Esophagus or Trachea. Sur-gery, 31:239, 1952.
9. Farrior, R. T.: Primary Reconstruction ofCervical Esophagus. Arch. Otolaryngol., 79:258, 1964.
10. Fryfogle, J. D., G. A. Cyrowski, D. Rothwell,G. Rheault and T. Clark: Replacement ofthe Middle Third of the Esophagus with aSilicone Rubber Prosthesis. Dis. Chest, 43:464, 1963.
11. Gooselaw, J. G. and P. G. Isaacson: PartialIntussusception of Esophagus into a PlasticProsthesis. Surgery, 55:248, 1964.
12. Greening, W. P. and S. S. Ramsay: Cancer ofthe Oesophagus, Palliation by Intubation.Lancet, 2:1122, 1960.
13. Harrington, 0. B., A. C. Beall, Jr., G. C.Morris, Jr. and F. C. Usher: CircumferentialReplacement of the Trachea with MarlexMesh. Amer. Surg., 28:217, 1962.
14. Heimlich, H. J.: Two Palliative Operations forCancer of the Esophagus Using PlasticProstheses. Amer. J. Surg., 103:376, 1962.
15. Hopkins, D. M. and P. E. Bernatz: Experi-mental Replacement of the Cervical Esopha-gus. Arch. Surg., 87:265, 1963.
16. Ingraham, F. D., E. Alexander, Jr. and B. D.Matson: Synthetic Plastic Materials in Sur-gery. New Engl. J. Med., 236:362, 1947.
17. Iske§el, 0. K.: The Use of Free Jejunal Seg-ments in the Reconstruction of Cervical Eso-phageal Defects. Surgery, 51:496, 1962.
18. Kirkpatrick, J. A., S. L. Cresson and G. P.Pilling, IV: The Motor Activity of theEsophagus in Association with EsophagealAtresia and Tracheo-Esophageal Fistula.Amer. J. Roentgenol., 86:884, 1961.
19. Lister, J., R. N. Reynolds and W. A. Allison:A Safe Method of Anesthetizing Puppies forIntra-Thoracic Experimental Surgery. Un-published data.
20. Lyons, A. S., A. R. Beck and L. J. Lester:Esophageal Replacement with Prosthesis.J. Surg. Res., 2:110, 1962.
21. Morfit, H. M. and D. Kramish: Long-TermEnd Results in Bridging Esophageal De-fects in Human Beings with Teflon Pros-theses. Amer. J. Surg., 104:756, 1962.
22. Neuhof, H. and J. M. Ziegler: ExperimentalReconstruction of the Oesophagus by Granu-lation Tubes. Surg. Gynec. & Obstet., 34:767, 1922.
23. O'Connor, T., R. Watson, D. Lepley, Jr. andW. Weisel: Esophageal Prosthesis for Pal-liative Intubation. Arch. Surg., 87:275, 1963.
24. Ravitch, M. M., H. T. Bahnson and T. N. P.Johns: Carcinoma of the Esophagus. J.Thor. Surg., 24:256, 1952.
25. Rob, C. G. and A. H. Bateman: Reconstruc-tion of the Trachea and Cervical Esophagus.Brit. J. Surg., 37:202, 1949.
26. Sheena, K. S., A. J. Ballantyne and J. E.Healey: Replacement of the Cervical Esoph-agus with Marlex Mesh. Surgery, 51:648,1962.
27. Souttar, H. S.: Treatment of Carcinoma ofthe Esophagus. Brit. J. Surg., 15:76, 1927.
28. Symonds, C. J.: The Treatment of MalignantStricture of the Esophagus by Tubage orOral Catheterism. Brit. Med. J., 1:870, 1887.