Embed Size (px)
Citation preview
1
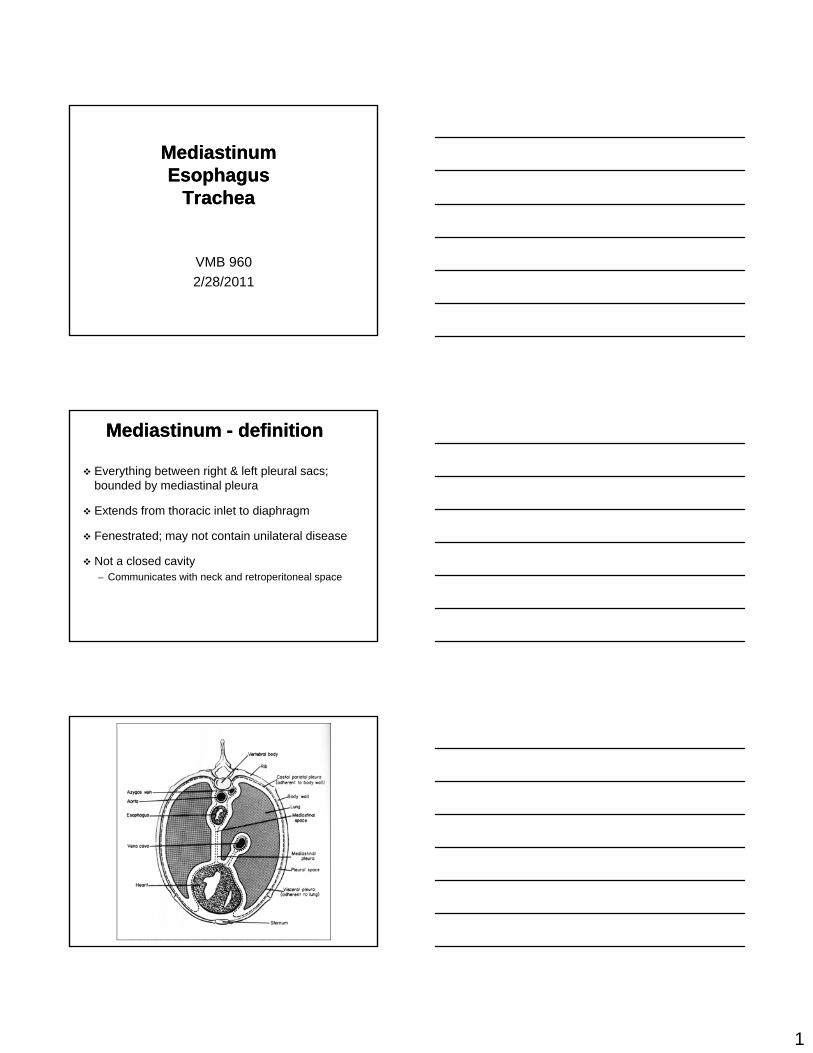
MediastinumMediastinumEsophagus Esophagus
Trachea Trachea
VMB 960
2/28/2011
Mediastinum Mediastinum -- definitiondefinition
Everything between right & left pleural sacs; bounded by mediastinal pleura
Extends from thoracic inlet to diaphragm
Fenestrated; may not contain unilateral disease
Not a closed cavity– Communicates with neck and retroperitoneal space
2
Mediastinal ReflectionsMediastinal Reflections
CranioventralCaudoventralCaval; can’t see
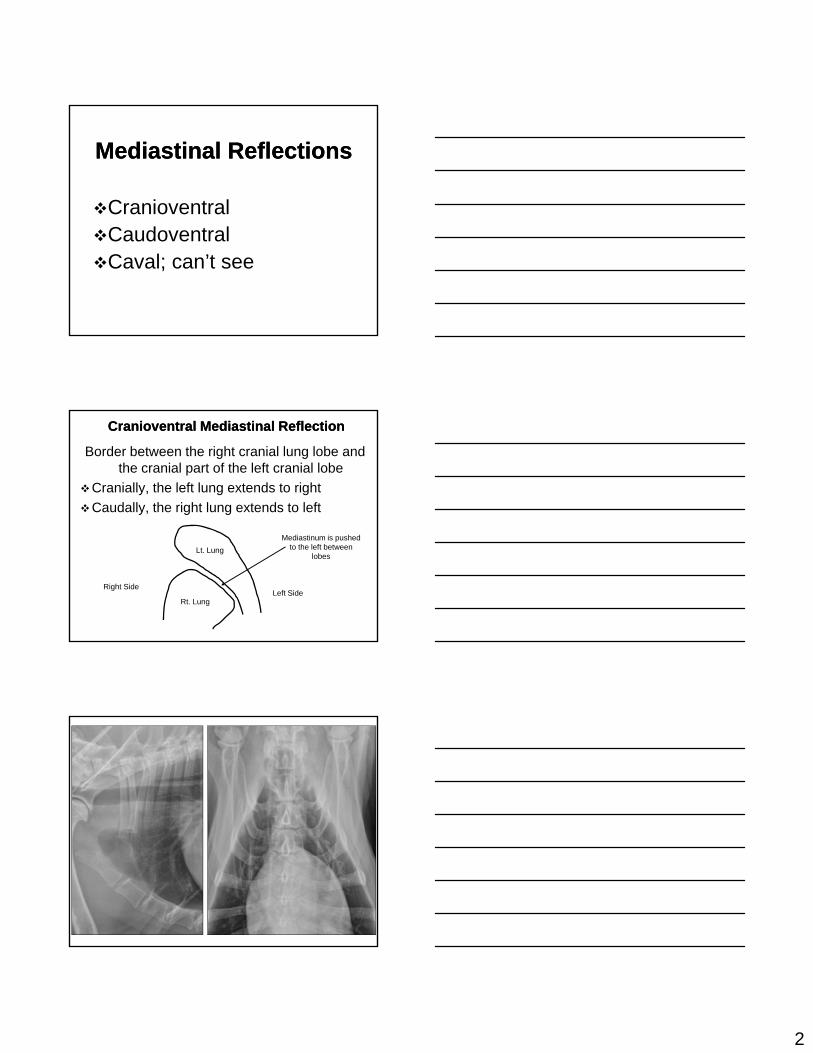
Cranioventral Mediastinal ReflectionCranioventral Mediastinal Reflection
Border between the right cranial lung lobe and the cranial part of the left cranial lobe
Cranially, the left lung extends to right
Caudally, the right lung extends to left
Rt. Lung
Lt. Lung
Left SideRight Side
Mediastinum is pushed to the left between
lobes
3
Mediastinal Organs Mediastinal Organs Normally SeenNormally Seen
Heart
Trachea
Caudal venal cavaCaudal venal cava
Aorta
Thymus (young animals)
Esophagus (sometimes - left lateral)
Mediastinal AbnormalitiesMediastinal Abnormalities
Lymph nodesEsophageal disordersTracheal disorders Thymic massesEctopic thyroid tissueCystsFluid
Things to confuse with Things to confuse with mediastinal lymphomegalymediastinal lymphomegaly
Heart base mass
Mediastinal cyst
Some other mediastinal masses
4
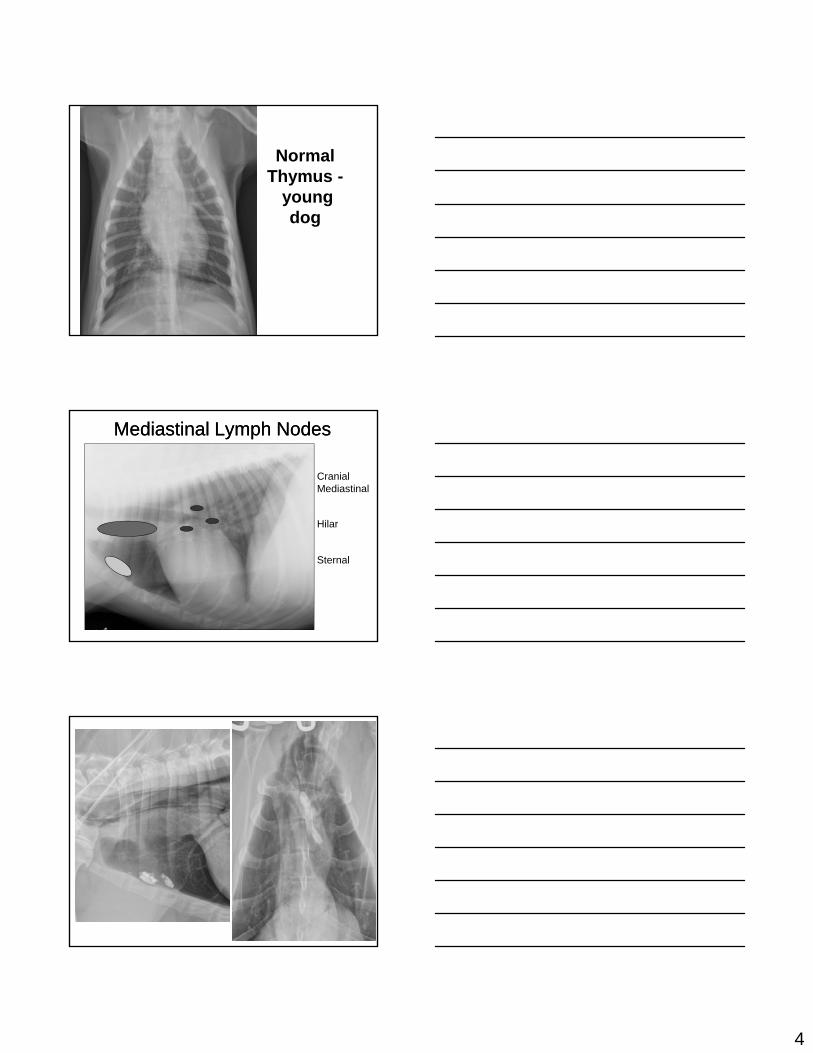
Normal Thymus -
young dogdog
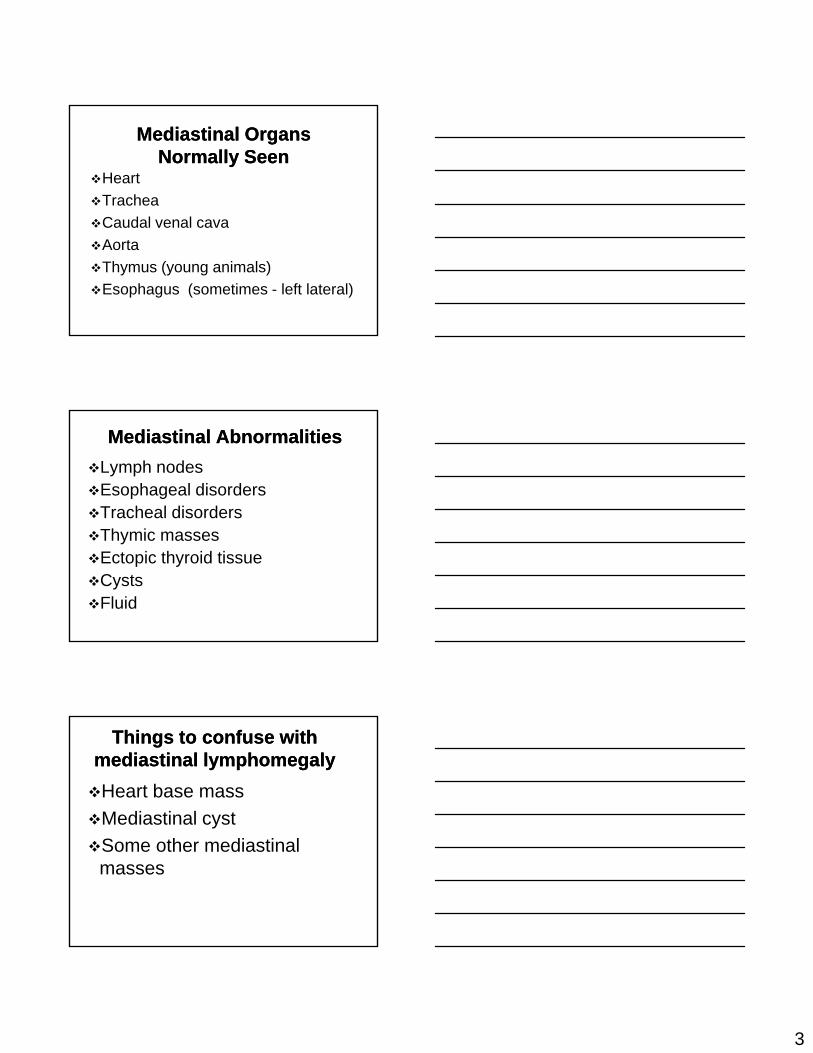
Mediastinal Lymph NodesMediastinal Lymph Nodes
Cranial Mediastinal
HilarHilar
Sternal
5
6
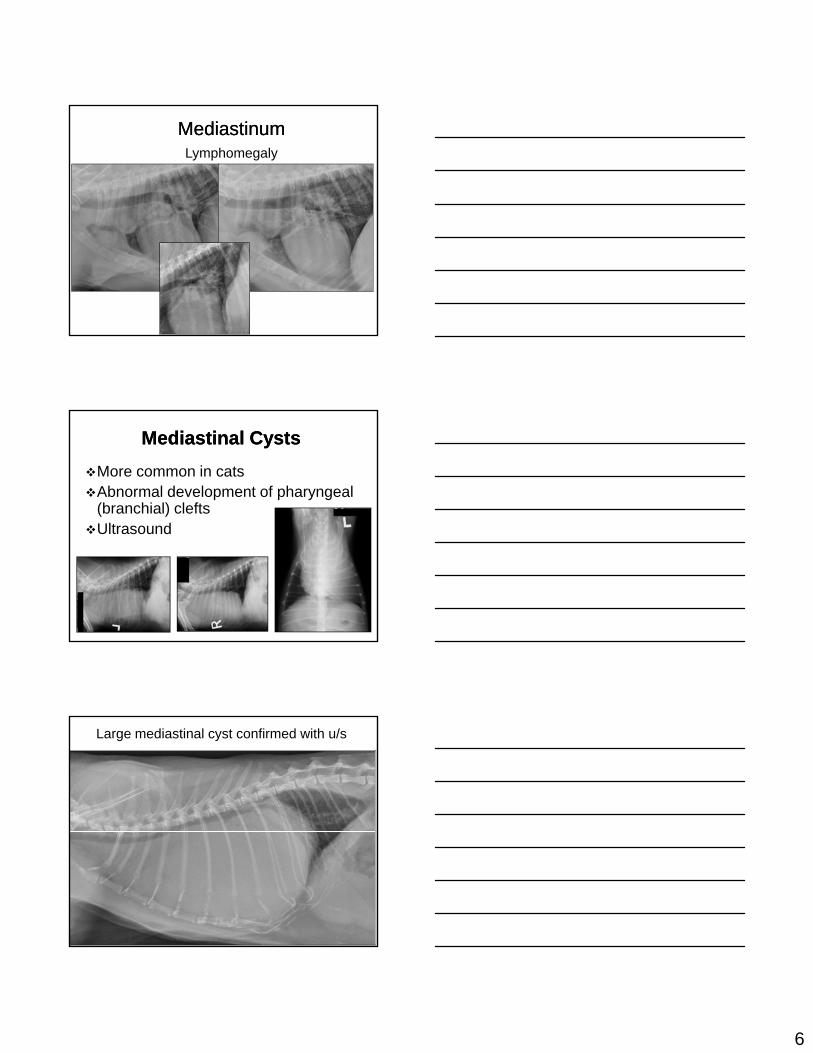
Mediastinum Mediastinum Lymphomegaly
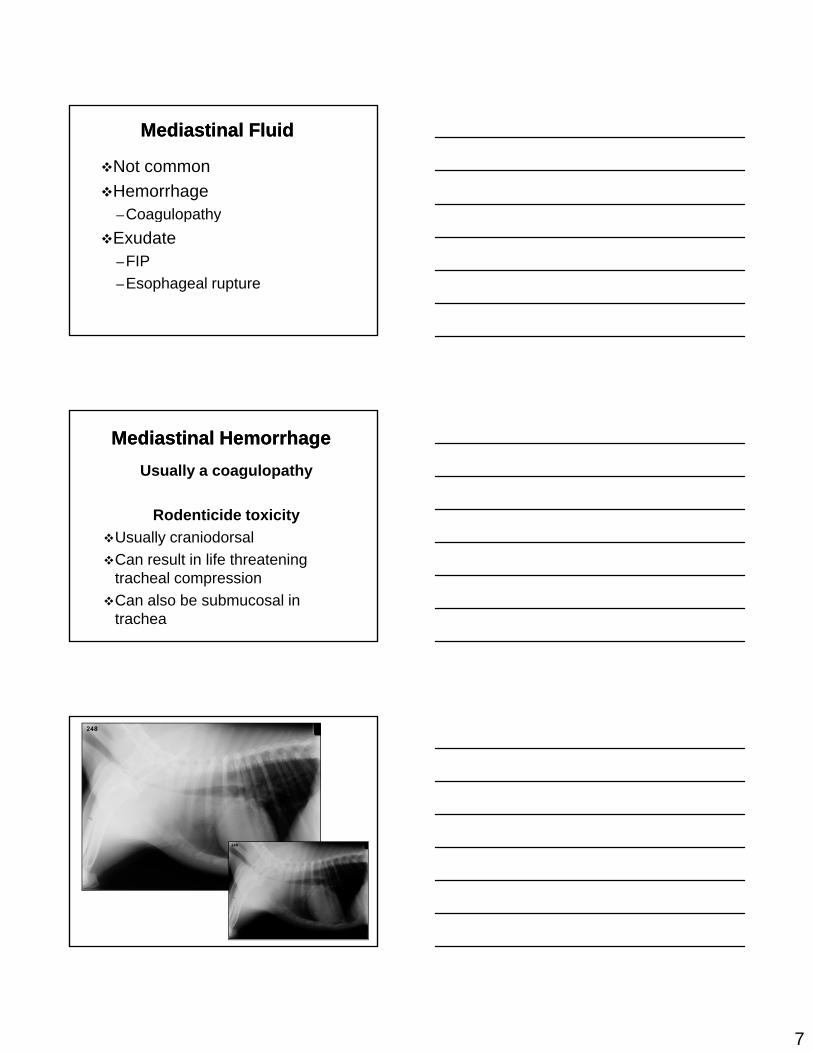
Mediastinal CystsMediastinal Cysts
More common in catsAbnormal development of pharyngeal
(branchial) cleftsUltrasoundUltrasound
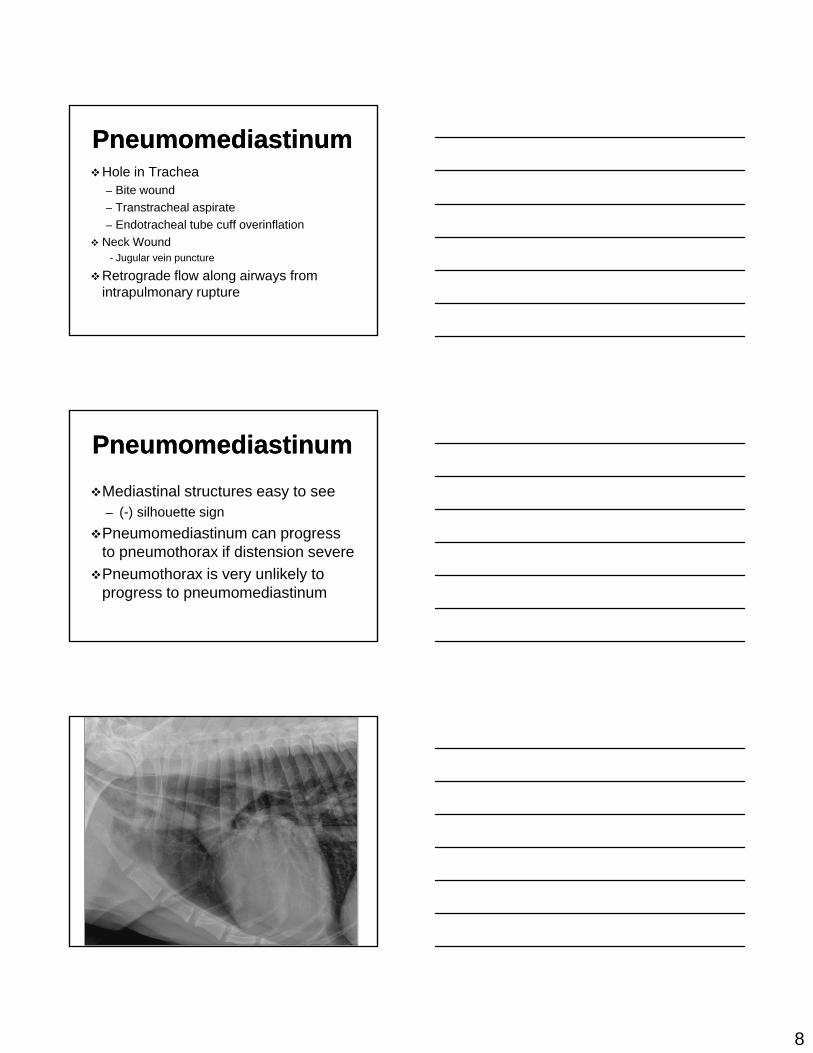
Large mediastinal cyst confirmed with u/s
7
Mediastinal FluidMediastinal Fluid
Not common
Hemorrhage–Coagulopathyg p y
Exudate–FIP
–Esophageal rupture
Mediastinal HemorrhageMediastinal Hemorrhage
Usually a coagulopathy
Rodenticide toxicity
Usually craniodorsal
Can result in life threatening tracheal compression
Can also be submucosal in trachea
8
PneumomediastinumPneumomediastinumHole in Trachea
– Bite wound
– Transtracheal aspirate
E d t h l t b ff i fl ti– Endotracheal tube cuff overinflation
Neck Wound- Jugular vein puncture
Retrograde flow along airways from intrapulmonary rupture
PneumomediastinumPneumomediastinum
Mediastinal structures easy to see – (-) silhouette sign
Pneumomediastinum can progress to pneumothorax if distension severe
Pneumothorax is very unlikely to progress to pneumomediastinum
9
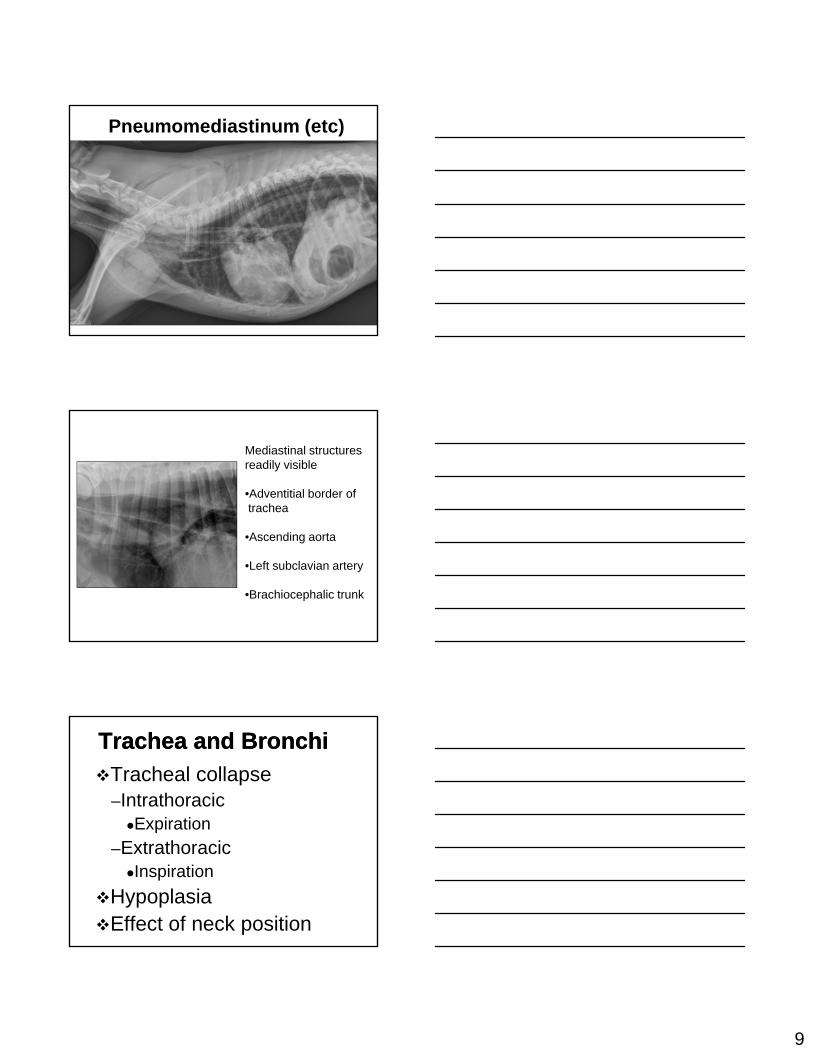
Pneumomediastinum (etc)
Mediastinal structuresreadily visible
•Adventitial border of trachea
•Ascending aorta
•Left subclavian artery
•Brachiocephalic trunk
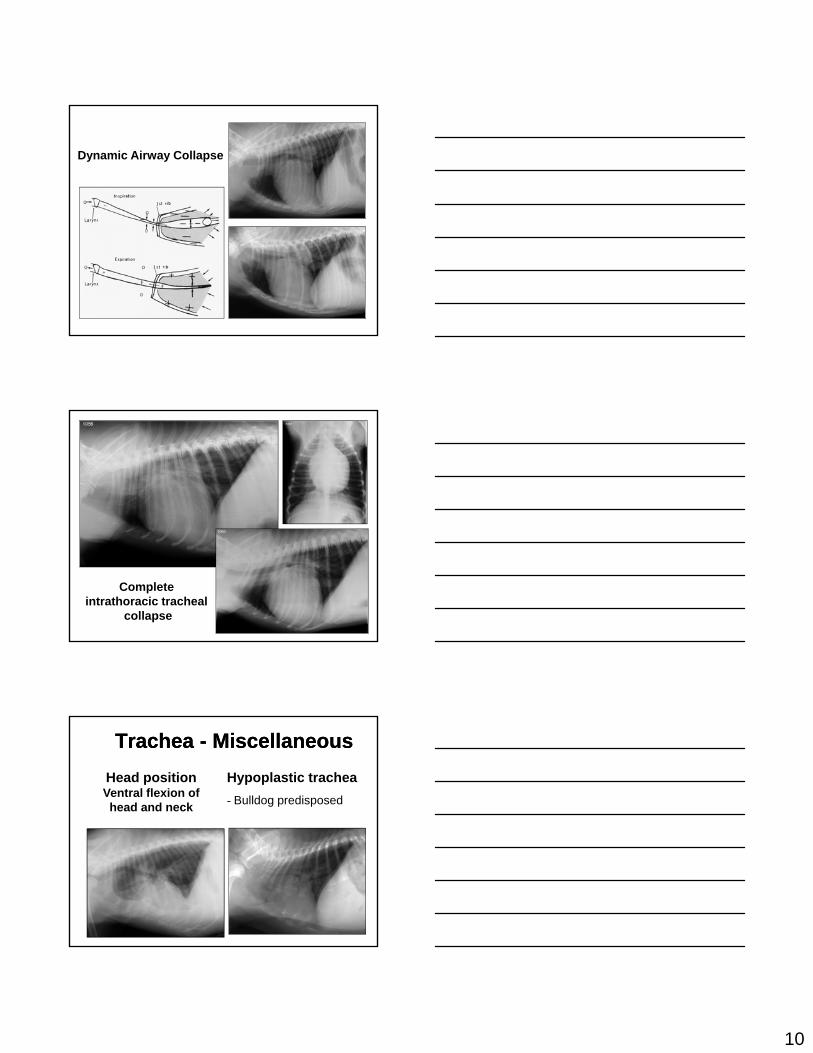
Trachea and BronchiTrachea and Bronchi
Tracheal collapse–IntrathoracicExpirationp
–ExtrathoracicInspiration
HypoplasiaEffect of neck position
10
Dynamic Airway Collapse
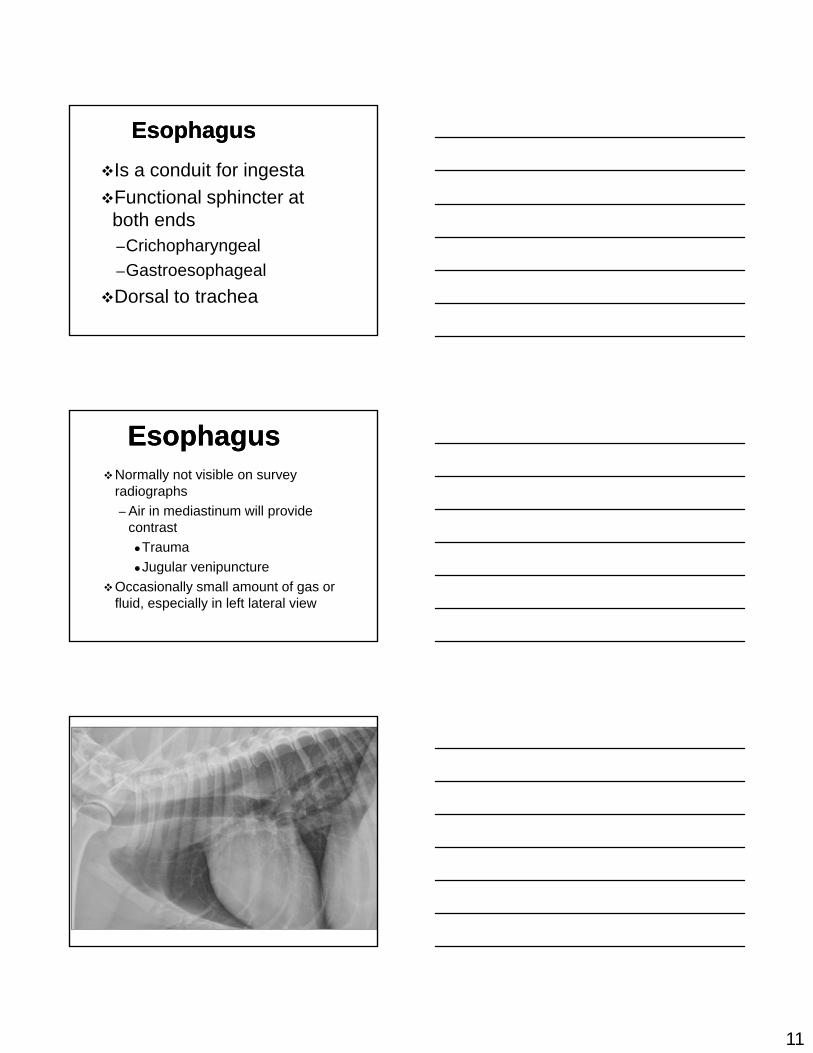
Complete intrathoracic tracheal
collapse
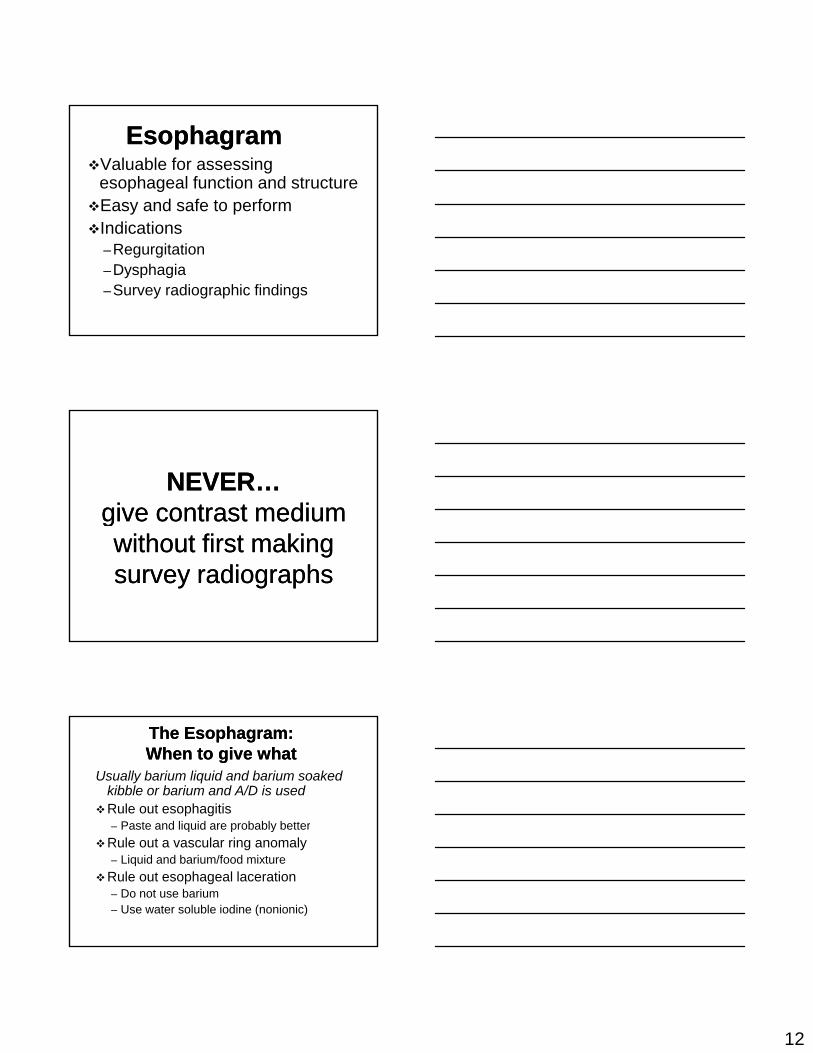
Trachea Trachea -- MiscellaneousMiscellaneous
Head positionVentral flexion of head and neck
Hypoplastic trachea
- Bulldog predisposed
11
EsophagusEsophagus
Is a conduit for ingesta
Functional sphincter at both endsboth ends–Crichopharyngeal
–Gastroesophageal
Dorsal to trachea
EsophagusEsophagusNormally not visible on survey
radiographs
– Air in mediastinum will provide contrastcontrast
Trauma
Jugular venipuncture
Occasionally small amount of gas or fluid, especially in left lateral view
12
EsophagramEsophagramValuable for assessing
esophageal function and structureEasy and safe to performIndications
–Regurgitation–Dysphagia–Survey radiographic findings
NEVER…NEVER…give contrast medium give contrast medium ggwithout first making without first making survey radiographssurvey radiographs
The Esophagram: The Esophagram: When to give whatWhen to give what
Usually barium liquid and barium soaked kibble or barium and A/D is used
Rule out esophagitis – Paste and liquid are probably betterq p y
Rule out a vascular ring anomaly– Liquid and barium/food mixture
Rule out esophageal laceration – Do not use barium – Use water soluble iodine (nonionic)
13
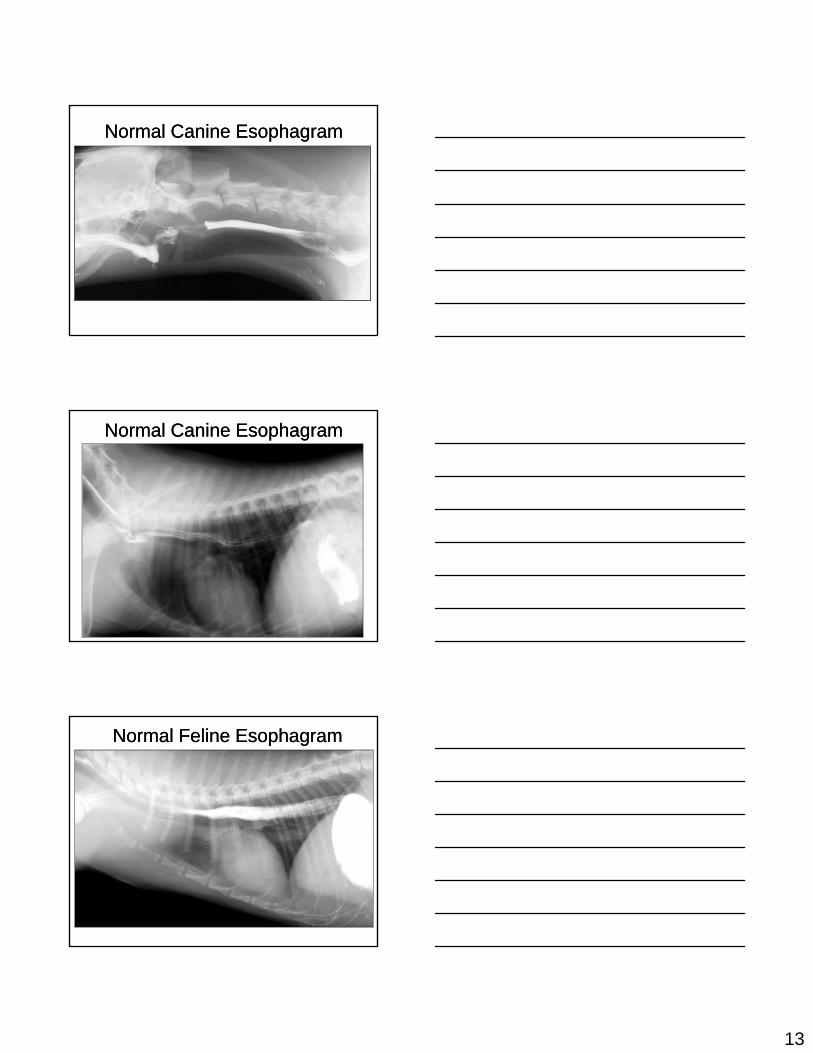
Normal Canine EsophagramNormal Canine Esophagram
Normal Canine EsophagramNormal Canine Esophagram
Normal Feline EsophagramNormal Feline Esophagram
14
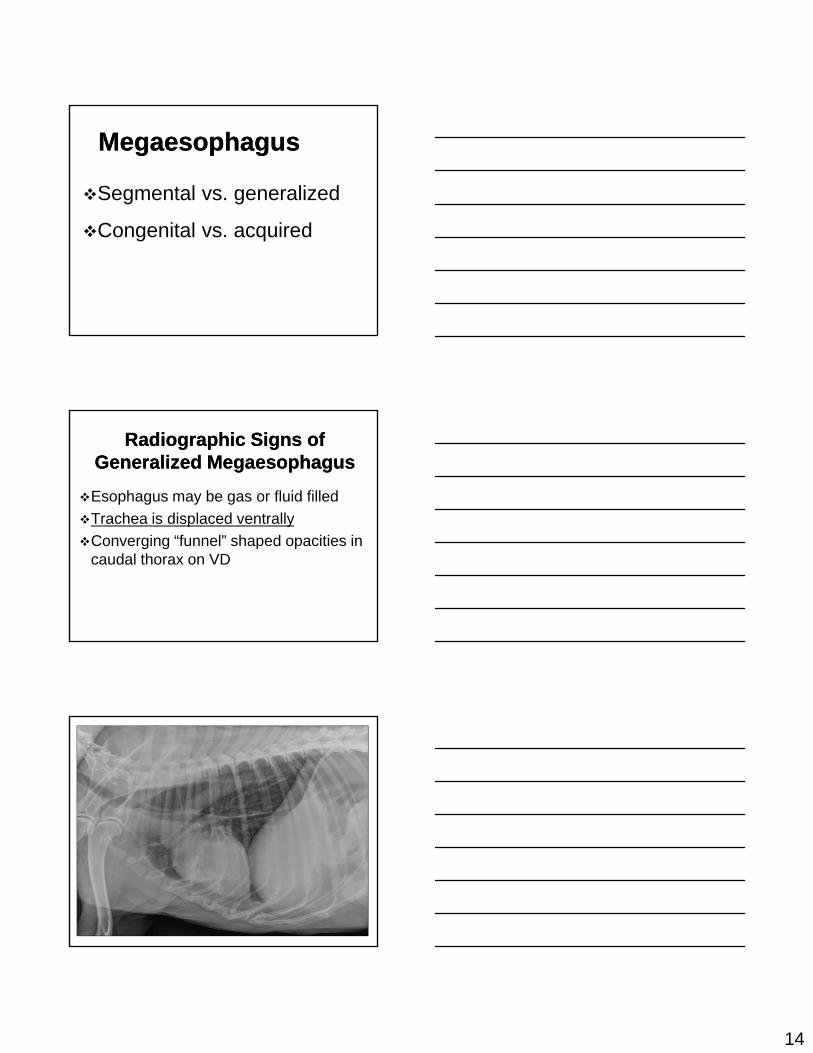
MegaesophagusMegaesophagus
Segmental vs. generalized
Congenital vs. acquired
Radiographic Signs of Radiographic Signs of Generalized MegaesophagusGeneralized Megaesophagus
Esophagus may be gas or fluid filled
Trachea is displaced ventrallyp y
Converging “funnel” shaped opacities in caudal thorax on VD
15
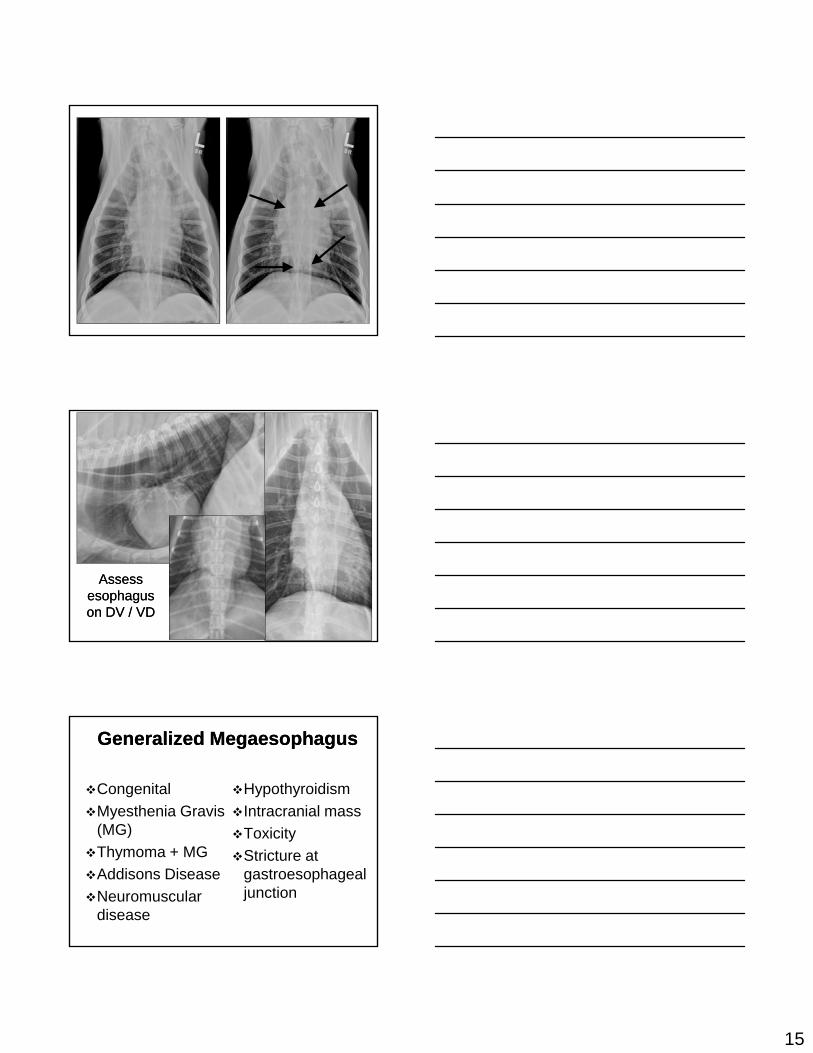
Assess Assess esophagus esophagus on DV / VDon DV / VD
Generalized MegaesophagusGeneralized Megaesophagus
Congenital
Myesthenia Gravis (MG)
Hypothyroidism
Intracranial mass
Toxicity(MG)
Thymoma + MG
Addisons Disease
Neuromuscular disease
Toxicity
Stricture at gastroesophageal junction
16
Radiographic Signs of Radiographic Signs of Segmental MegaesophagusSegmental Megaesophagus
Focal mass effect or gas accumulation
Trachea displaced ventrally ifTrachea displaced ventrally if
abnormality is cranial to heart base
Midline opacity on VD view
Congenital MegaesophagusCongenital Megaesophagus
Segmental–Vascular ring anomaly
R d d t h–Redundant esophagus
Generalized
–"Megaesophagus"
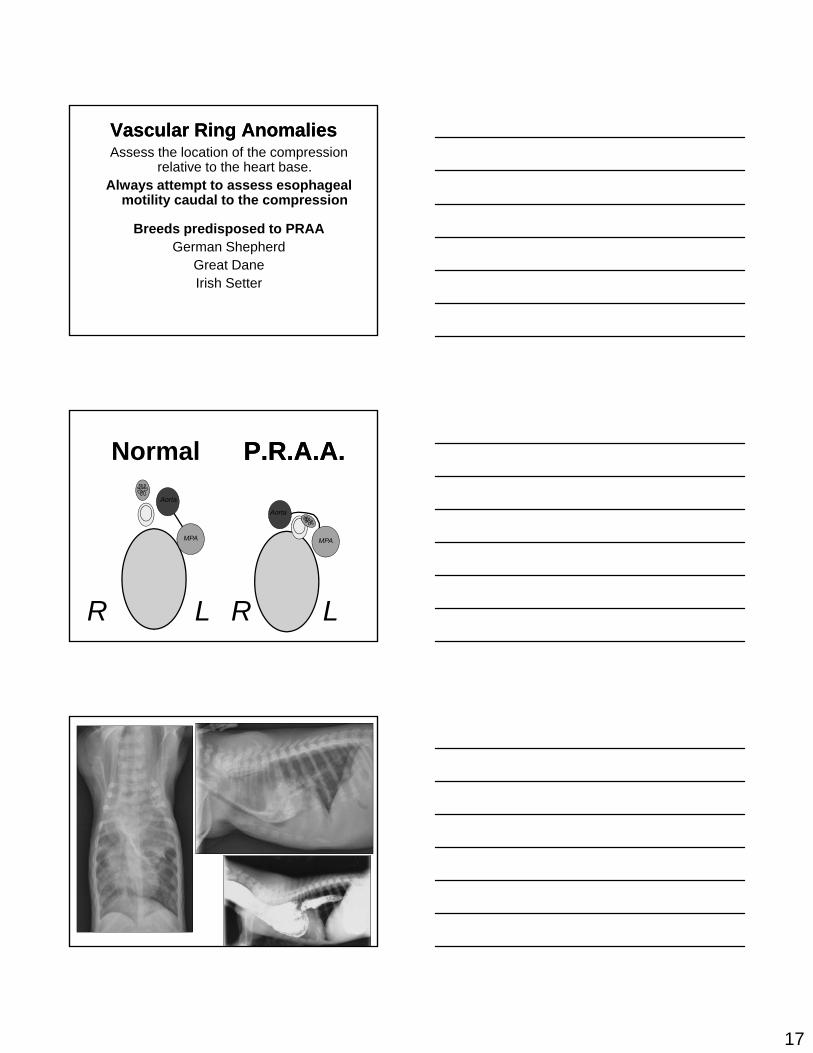
Vascular Ring AnomaliesVascular Ring Anomalies
More common in dogs
Arise from aortic arch or subclavian abnormalities
Patient may also have generalized megaesophagus
17
Vascular Ring AnomaliesVascular Ring AnomaliesAssess the location of the compression
relative to the heart base. Always attempt to assess esophageal
motility caudal to the compression
Breeds predisposed to PRAAGerman Shepherd
Great DaneIrish Setter
P.R.A.A.P.R.A.A.
Aorta
Aorta
Normal
R R LL
MPA MPA
18
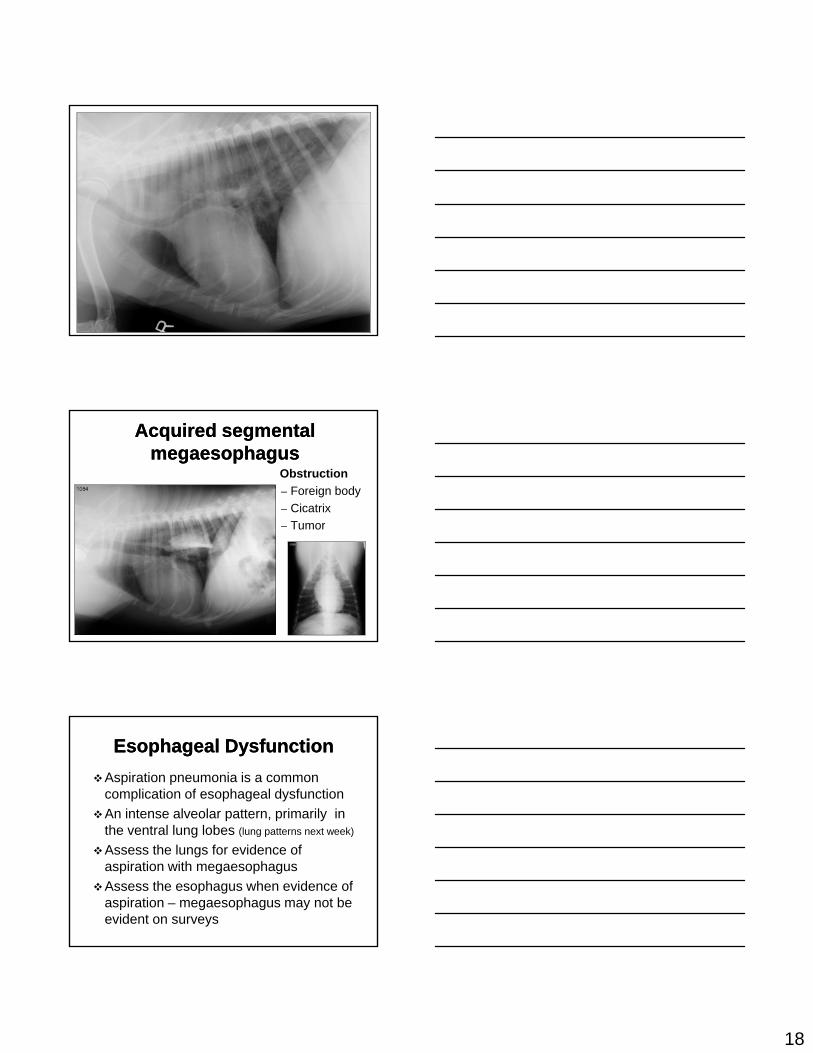
Acquired segmental Acquired segmental megaesophagusmegaesophagus
Obstruction
– Foreign body
– Cicatrix
Tumor– Tumor
Esophageal DysfunctionEsophageal Dysfunction
Aspiration pneumonia is a common complication of esophageal dysfunction
An intense alveolar pattern, primarily in the ventral lung lobes (lung patterns next week)the ventral lung lobes (lung patterns next week)
Assess the lungs for evidence of aspiration with megaesophagus
Assess the esophagus when evidence of aspiration – megaesophagus may not be evident on surveys
19
Swallowing DisordersSwallowing Disorders
Review Fluoroscopy movies- via http://radstudents.ncsu.edu
Folder = fluoroscopy moviesFolder = fluoroscopy movies
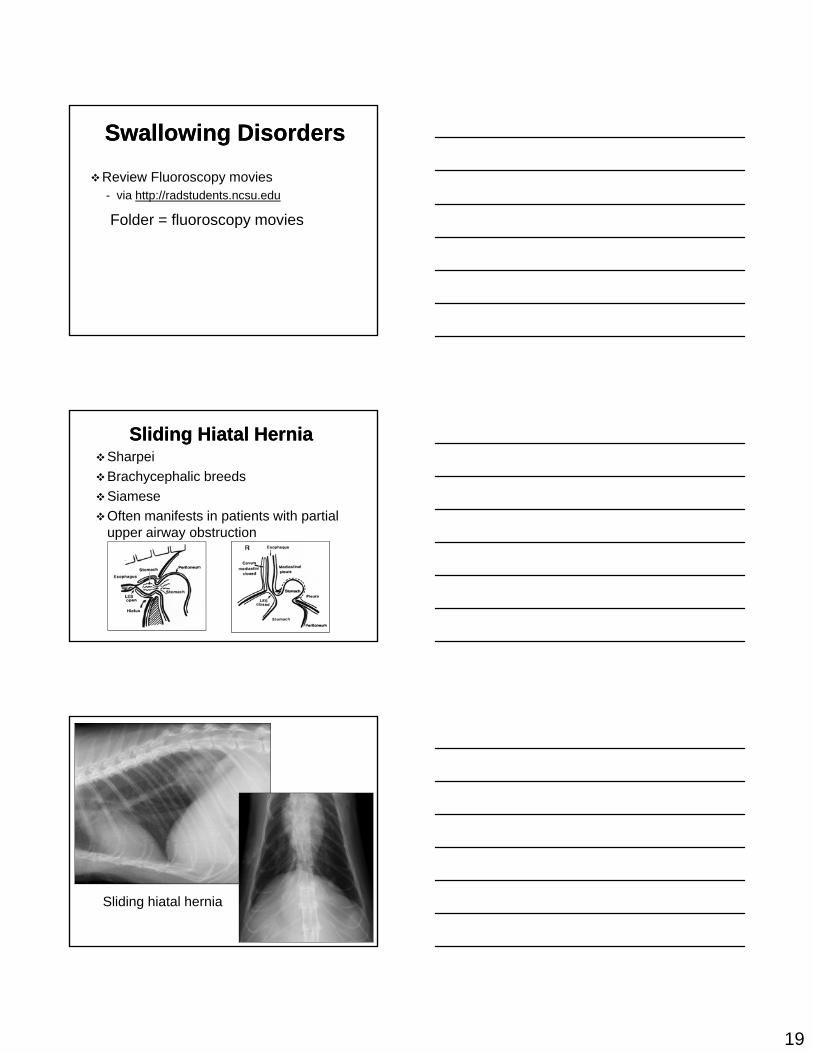
Sliding Hiatal HerniaSliding Hiatal HerniaSharpei
Brachycephalic breeds
Siamese
Often manifests in patients with partial upper airway obstruction
Sliding hiatal hernia
20
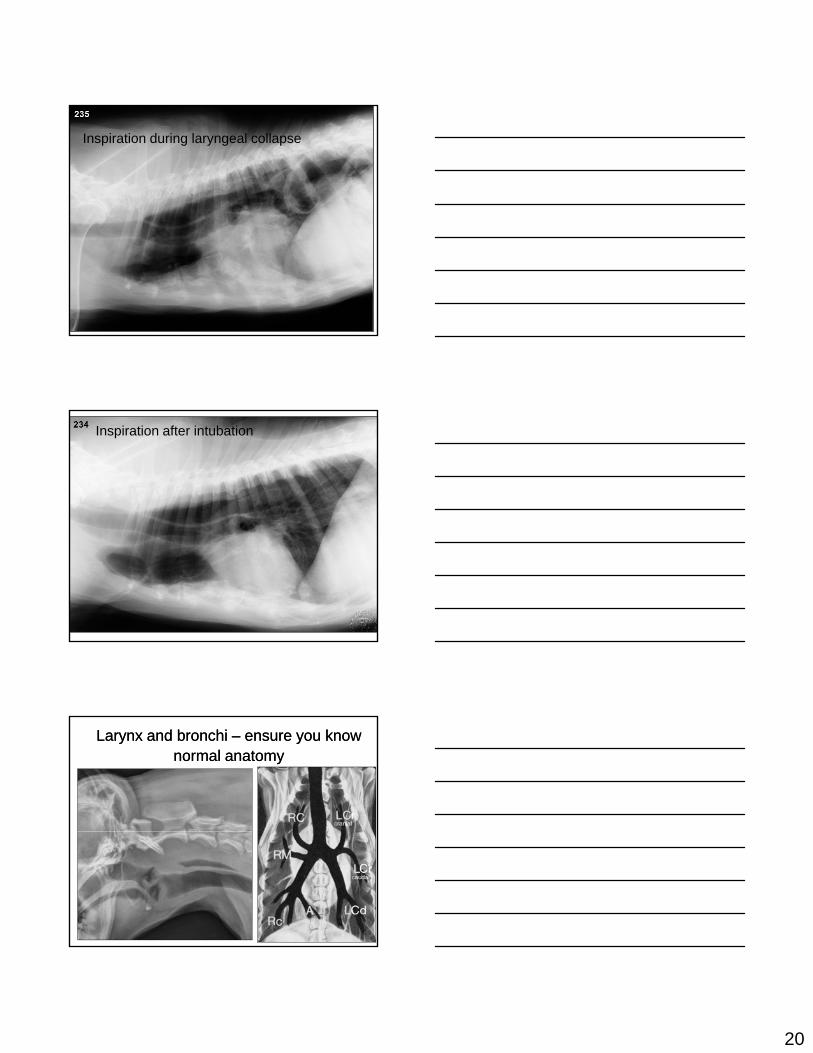
Inspiration during laryngeal collapse
Inspiration after intubation
Larynx and bronchi Larynx and bronchi –– ensure you know ensure you know normal anatomynormal anatomy
1
Mediastinum Mediastinum
Case DiscussionsCase Discussions
3/01/20113/01/2011
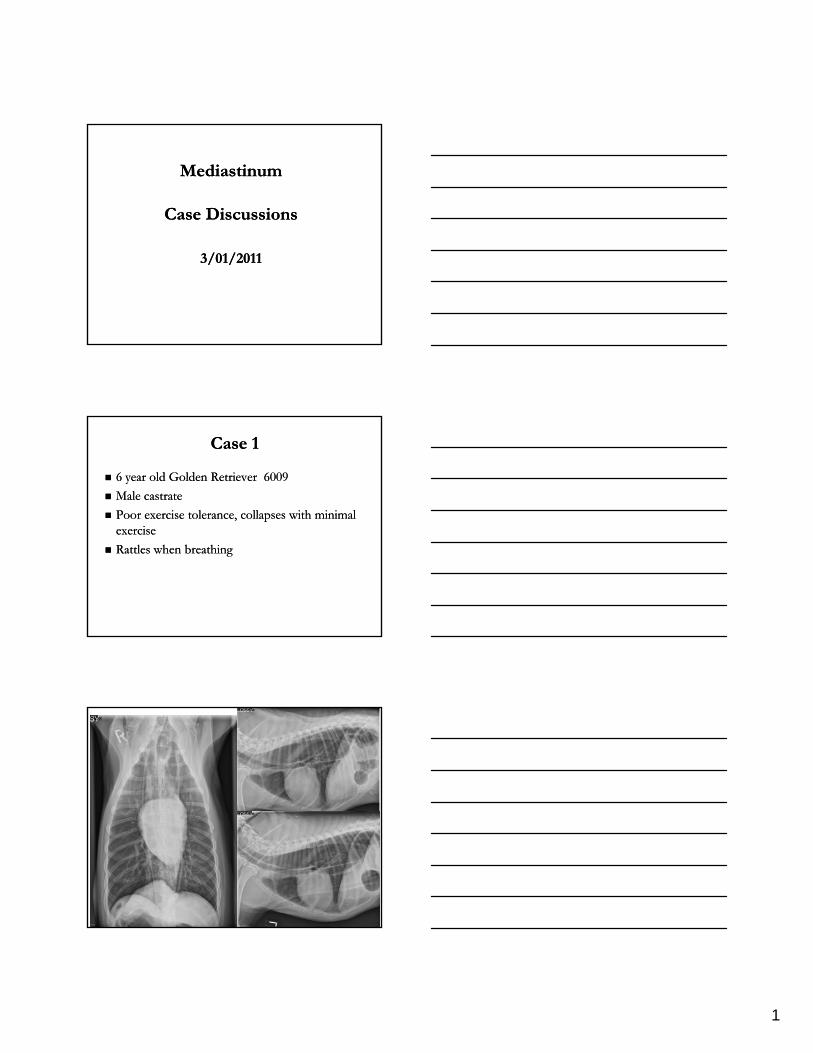
Case 1Case 1
6 year old Golden Retriever 60096 year old Golden Retriever 6009
Male castrate Male castrate
Poor exercise tolerance, collapses with minimal Poor exercise tolerance, collapses with minimal iiexercise exercise
Rattles when breathing Rattles when breathing
2
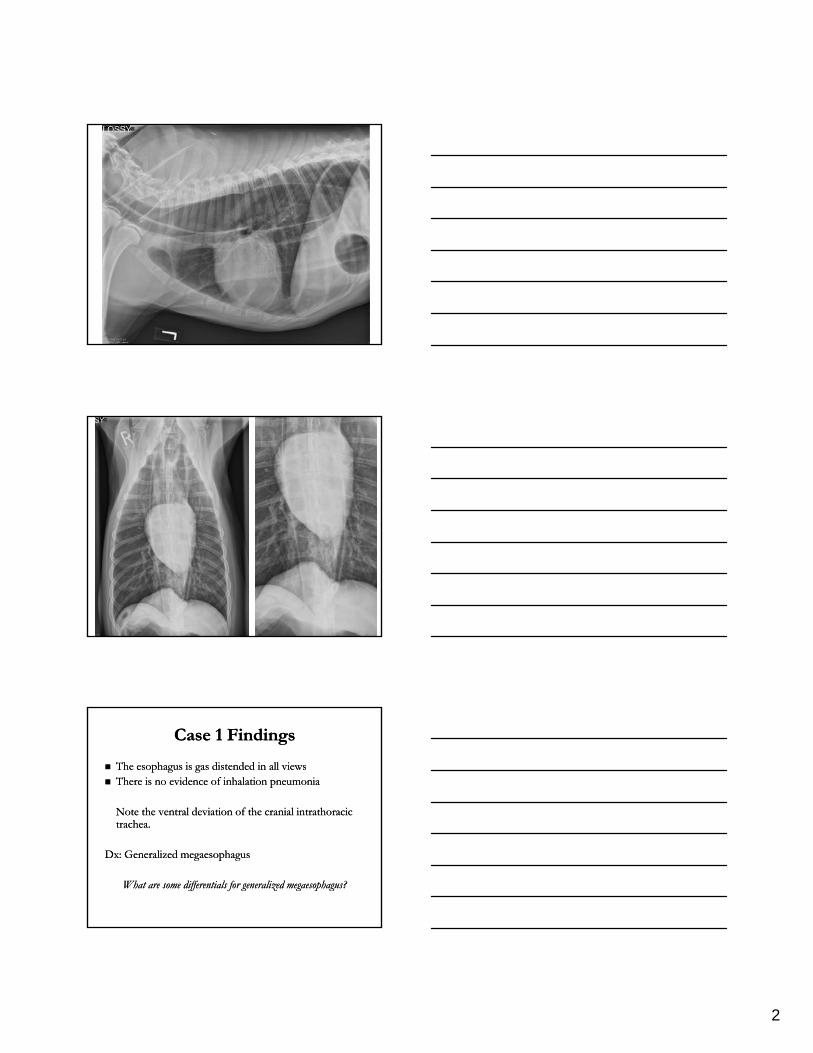
Case 1 Findings Case 1 Findings
The esophagus is gas distended in all views The esophagus is gas distended in all views There is no evidence of inhalation pneumonia There is no evidence of inhalation pneumonia
Note the ventral deviation of the cranial intrathoracic Note the ventral deviation of the cranial intrathoracic trachea.trachea.
Dx: Generalized megaesophagus Dx: Generalized megaesophagus
What are some differentials for generalized megaesophagus?What are some differentials for generalized megaesophagus?
3
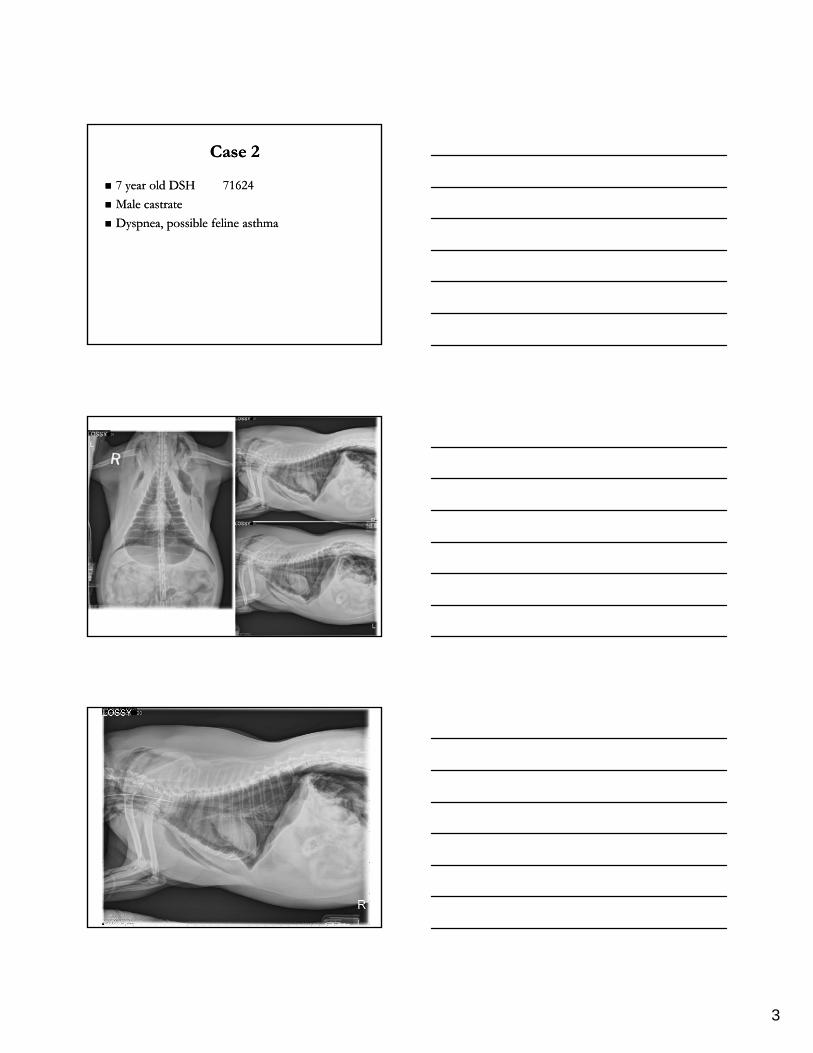
Case 2Case 2
7 year old DSH7 year old DSH 7162471624
Male castrateMale castrate
Dyspnea, possible feline asthmaDyspnea, possible feline asthma
4
5
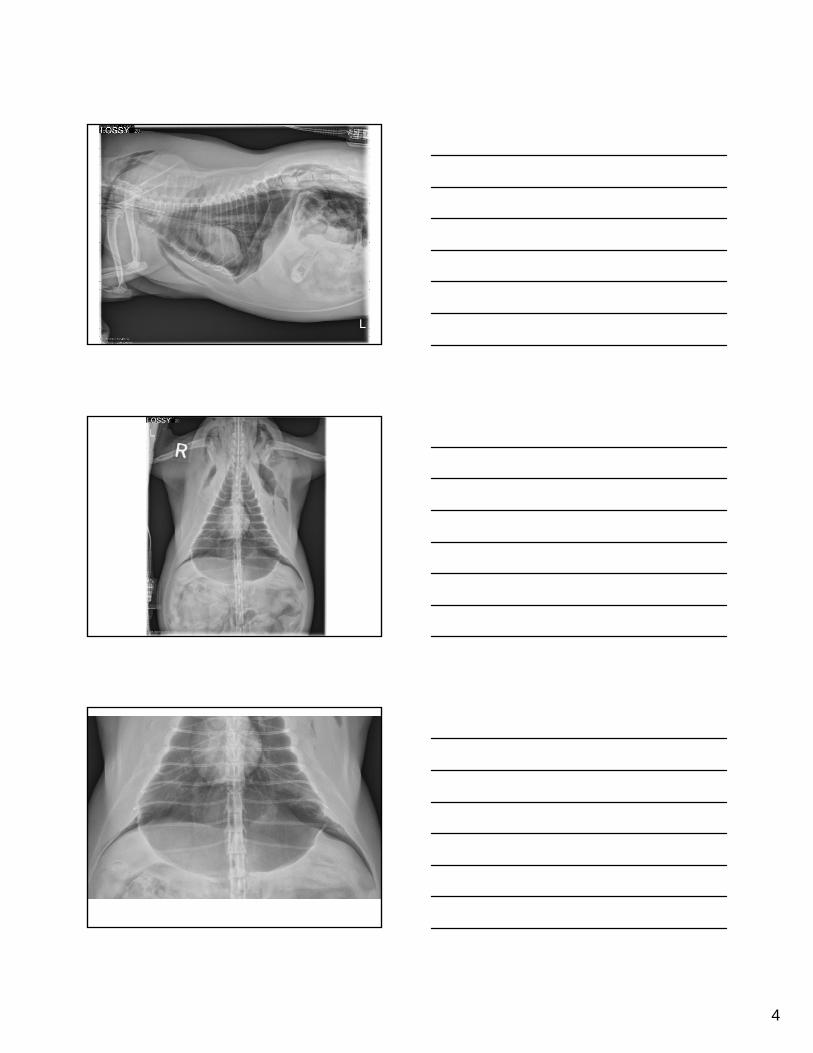
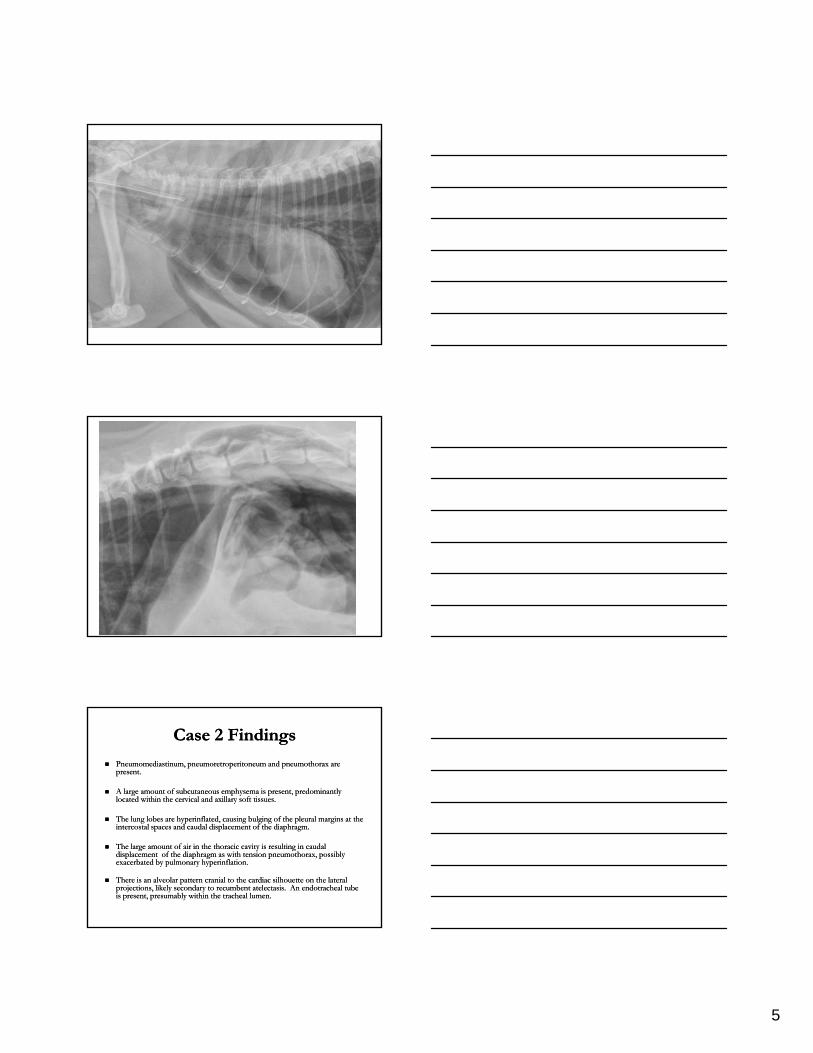
Case 2 Findings Case 2 Findings
Pneumomediastinum, pneumoretroperitoneum and pneumothorax are Pneumomediastinum, pneumoretroperitoneum and pneumothorax are present.present.
A large amount of subcutaneous emphysema is present, predominantly A large amount of subcutaneous emphysema is present, predominantly located within the cervical and axillarylocated within the cervical and axillary soft tissues.soft tissues.
Th l l b h i fl t d i b l i f th l l i t thTh l l b h i fl t d i b l i f th l l i t th The lung lobes are hyperinflated, causing bulging of the pleural margins at the The lung lobes are hyperinflated, causing bulging of the pleural margins at the intercostal spaces and caudal displacement of the diaphragm.intercostal spaces and caudal displacement of the diaphragm.
The large amount of air in the thoracic cavity is resulting in caudal The large amount of air in the thoracic cavity is resulting in caudal displacement of the diaphragm as with tension pneumothorax, possibly displacement of the diaphragm as with tension pneumothorax, possibly exacerbated by pulmonary hyperinflation.exacerbated by pulmonary hyperinflation.
There is an alveolar pattern cranial to the cardiac silhouette on the lateral There is an alveolar pattern cranial to the cardiac silhouette on the lateral projections, likely secondary to recumbent atelectasis.projections, likely secondary to recumbent atelectasis. An endotracheal tube An endotracheal tube is present, presumably within the tracheal lumen.is present, presumably within the tracheal lumen.
6
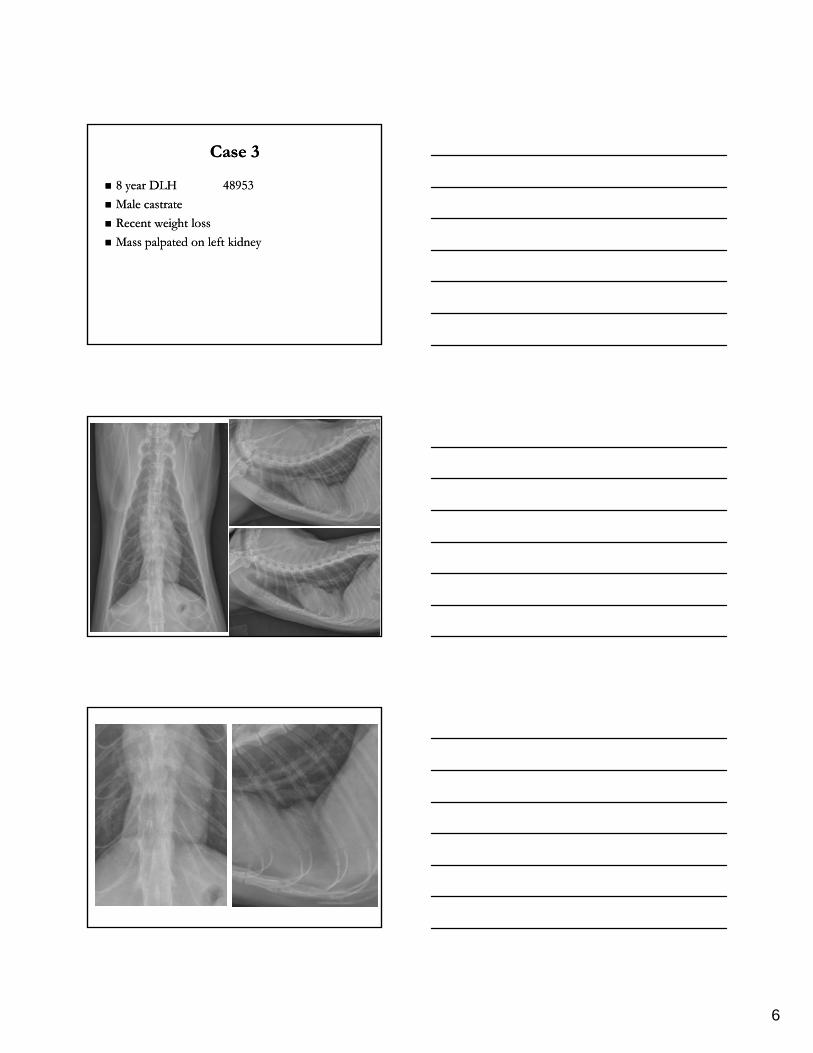
Case 3Case 3
8 year DLH8 year DLH 4895348953
Male castrate Male castrate
Recent weight lossRecent weight loss
Mass palpated on left kidney Mass palpated on left kidney
7
Case 3 FindingsCase 3 Findings
There is an increase in soft tissue opacity caudal There is an increase in soft tissue opacity caudal to the cardiac silhouette that silhouettes with to the cardiac silhouette that silhouettes with both the diaphragm and the heart. There is poor both the diaphragm and the heart. There is poor distinction of the diaphragm at this level. distinction of the diaphragm at this level.
These findings are consistent with a peritoneal These findings are consistent with a peritoneal pericardial diaphragmatic hernia. pericardial diaphragmatic hernia.
How would you confirm this diagnosis?How would you confirm this diagnosis?
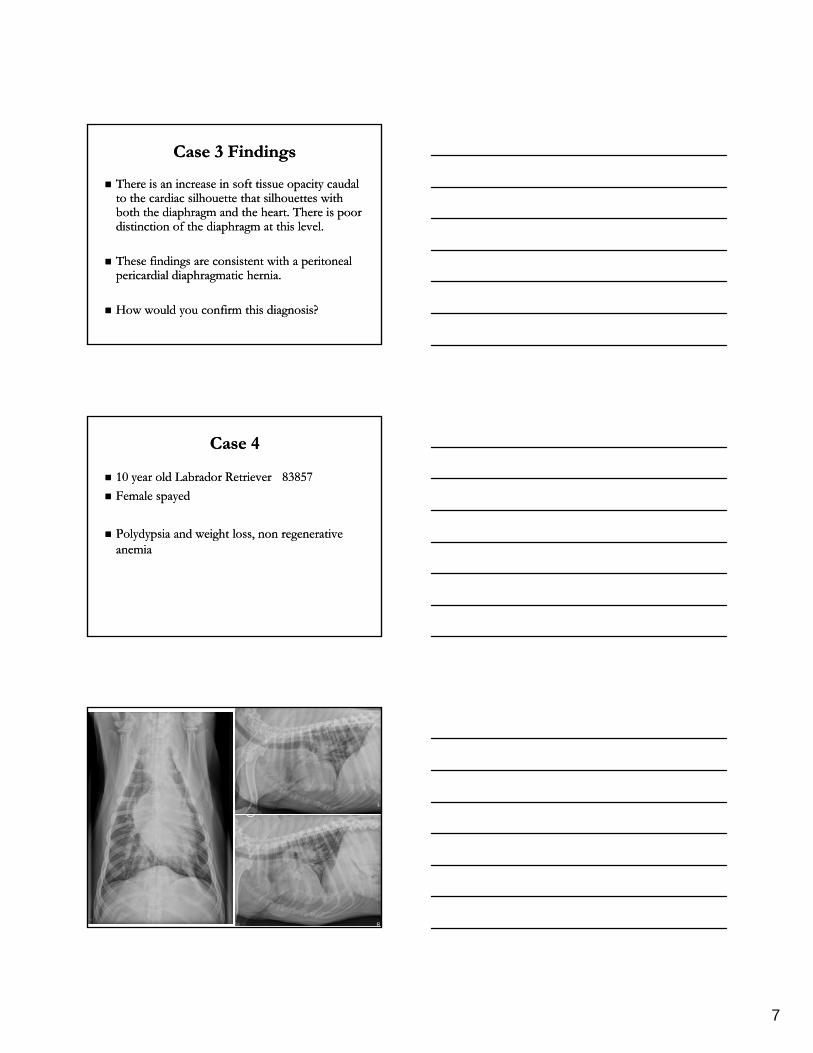
Case 4Case 4
10 year old Labrador Retriever 10 year old Labrador Retriever 8385783857
Female spayed Female spayed
Polydypsia and weight loss, non regenerative Polydypsia and weight loss, non regenerative anemia anemia
8
9
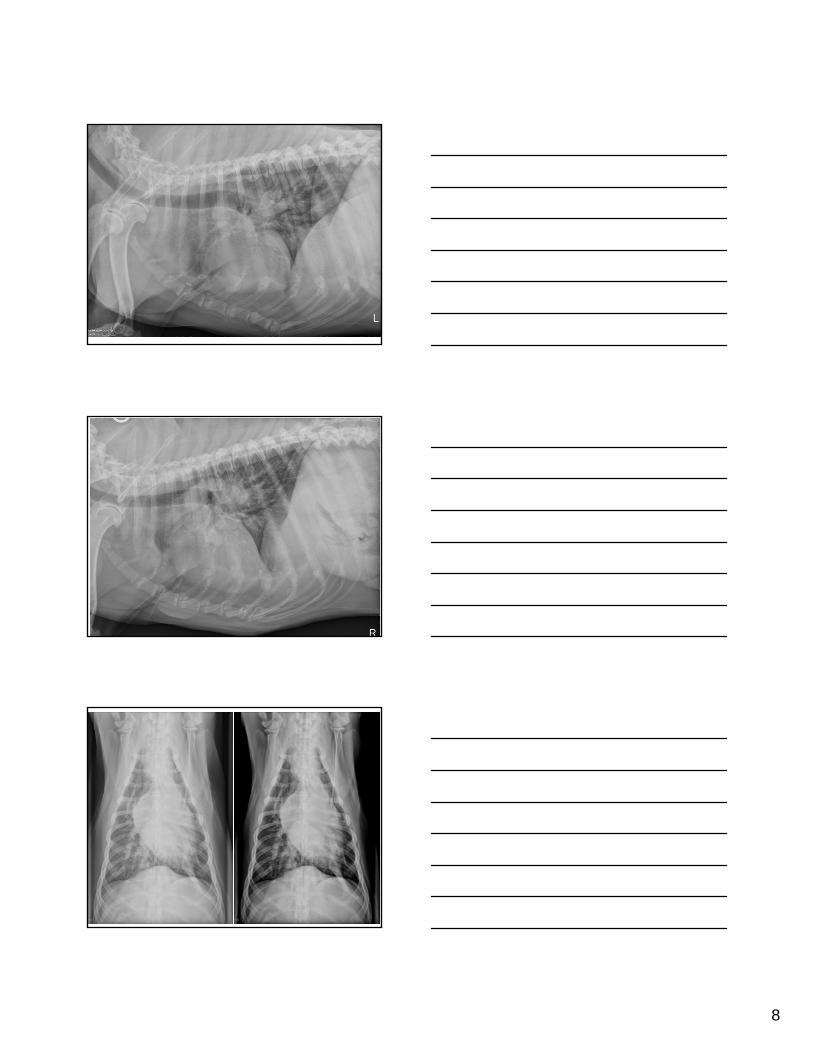
Case 4 FindingsCase 4 Findings The trachea is dorsally displaced cranial to the heart by an ill The trachea is dorsally displaced cranial to the heart by an ill
defined soft tissue mass. defined soft tissue mass.
There is a soft tissue mass dorsal to the cranial sternebrae. There is a soft tissue mass dorsal to the cranial sternebrae.
The principal bronchi are displaced laterally and ventrally.The principal bronchi are displaced laterally and ventrally.
Findings are consistent with enlargement of the sternal, cranial Findings are consistent with enlargement of the sternal, cranial mediastinal and tracheobronchial lymph nodes. mediastinal and tracheobronchial lymph nodes.
The pulmonary parenchyma and cardiovascular structures are The pulmonary parenchyma and cardiovascular structures are within normal limits. within normal limits.
What are some differentials for thoracic lymphomegaly?What are some differentials for thoracic lymphomegaly?
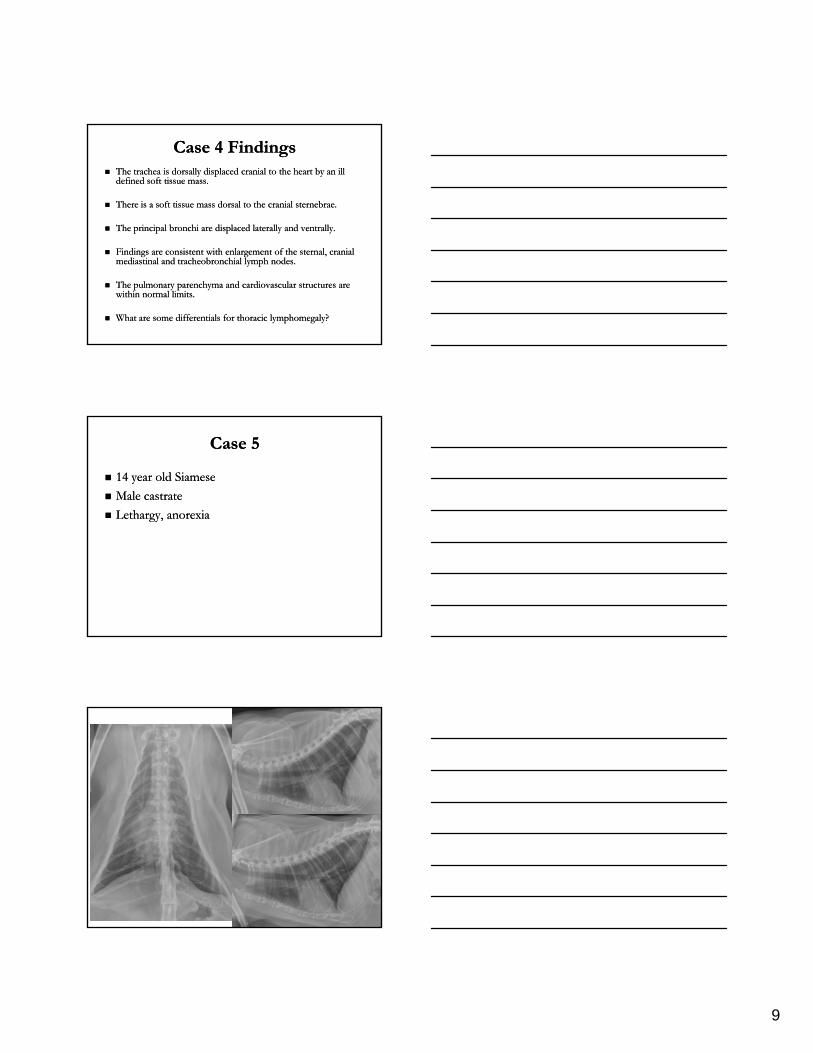
Case 5Case 5
14 year old Siamese 14 year old Siamese
Male castrateMale castrate
Lethargy, anorexia Lethargy, anorexia
10
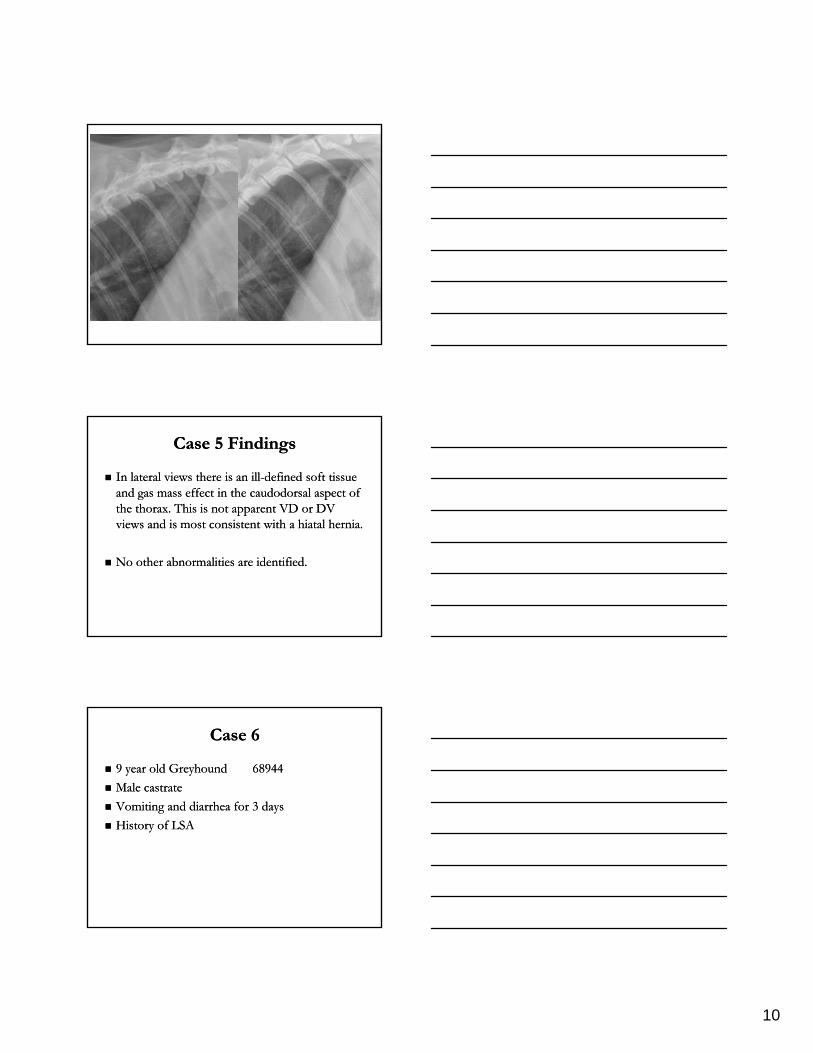
Case 5 Findings Case 5 Findings
In lateral views there is an illIn lateral views there is an ill--defined soft tissue defined soft tissue and gas mass effect in the caudodorsal aspect of and gas mass effect in the caudodorsal aspect of the thorax. This is not apparent VD or DV the thorax. This is not apparent VD or DV views and is most consistent with a hiatal herniaviews and is most consistent with a hiatal herniaviews and is most consistent with a hiatal hernia. views and is most consistent with a hiatal hernia.
No other abnormalities are identified.No other abnormalities are identified.
Case 6 Case 6
9 year old Greyhound 9 year old Greyhound 6894468944
Male castrateMale castrate
Vomiting and diarrhea for 3 days Vomiting and diarrhea for 3 days
History of LSAHistory of LSA
11
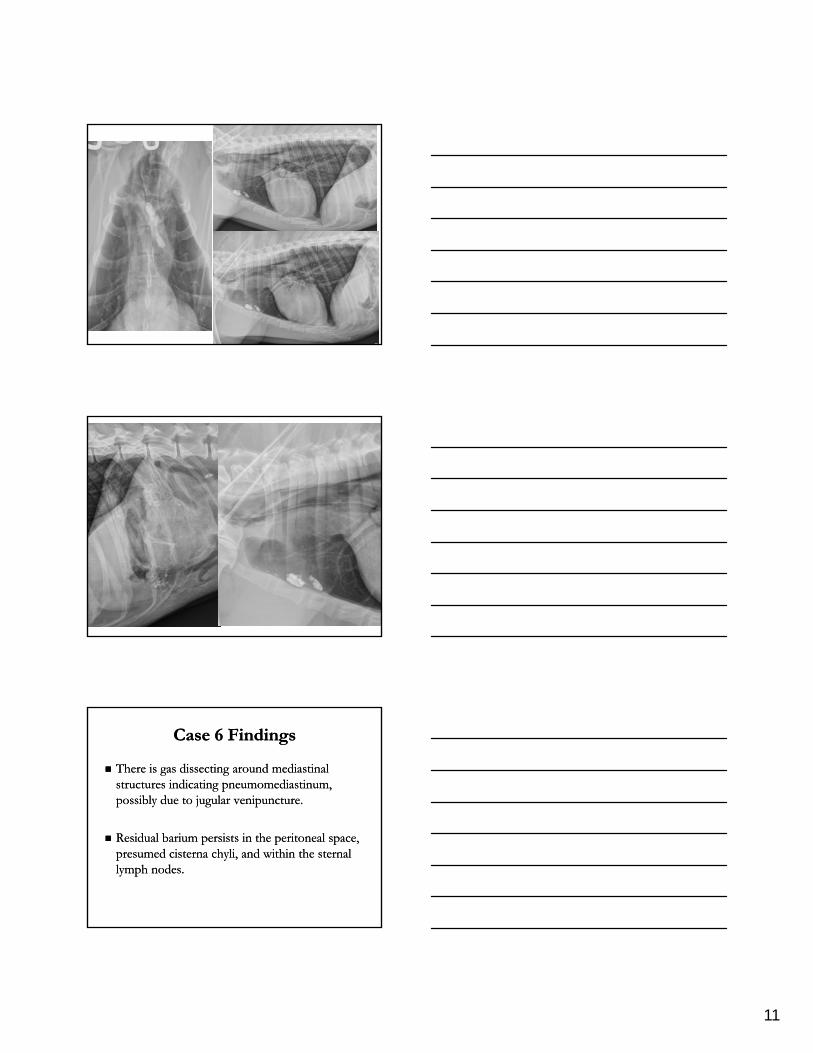
Case 6 Findings Case 6 Findings
There is gas dissecting around mediastinal There is gas dissecting around mediastinal structures indicating pneumomediastinum, structures indicating pneumomediastinum, possibly due to jugular venipuncture. possibly due to jugular venipuncture.
Residual barium persists in the peritoneal space, Residual barium persists in the peritoneal space, presumed cisterna chyli, and within the sternal presumed cisterna chyli, and within the sternal lymph nodes. lymph nodes.