Embed Size (px)
Citation preview
PROF. C J MBA Thursday, 17th November, 2014
2
“THE CONTROL OF IMPURITIES IN THE QUALITY
CONTROL OF PHARMACEUTICAL DOSAGE FORMS”
1.0 PROTOCOL
Professor Benjamin Chukwuma Ozumba, the Vice
chancellor, UNN
The Deputy Vice chancellors and other Principal officers
of the university
President of the University of Nigeria Alumni Association
and other officers present
Deans of faculty
Directors of institute and Centre
Heads of Department
Distinguished Professors
Past Inaugural lecturers
Heads of Administrative units
Distinguished Academics and Administrators
My Lords, Spiritual and Temporal
Igwes, Chiefs and Elders
Gentlemen of the Press
Lions and lionesses
My students, past, present and future
My patients without whom the content of this lecture
could not have been experienced
Ladies and gentlemen
3
INTRODUCTION It is with great pleasure and immense gratitude to Almighty God, the Creator that I stand before you today to deliver this inaugural lecture. Thanks also go to our Blessed Mother, Queen of Heaven for Her intercessions and protections. In the Faculty of Pharmaceutical Sciences, there are various Departments of which Pharmaceutical & Medicinal Chemistry is one. This aspect of Pharmaceutical Sciences encompasses Pharmaceutical Analysis, Medicinal Chemistry, Phytochemistry, Drug Metabolism and Pharmacokinetics. Thus, Pharmaceutical Analysis, which is my area of specialization, is a branch of Chemistry, which involves the identification, determination, quantitation, purification, separation of the components of a mixture and determination of the structures of drugs. With this definition, the question that
one can easily ask is: What is Drug. A drug is any substance (other than a food or device) intended for use in the diagnosis, cure, relief, treatment or prevention of disease or intended to affect the structure or function of the body. The success of drug therapy therefore is highly dependent among other things on the quality control/assurance of drug during production, type of dosage form and its route of delivery, efficacy and safety of the drug substance. An introduction of these terms is required to facilitate comprehension of this inaugural lecture.
4
QUALITY CONTROL Quality control (QC) refers to the sum of all procedures undertaken to ensure the identity and purity of a particular pharmaceutical. Such procedures may range from the performance of simple chemical tests which determine the identity and screening for the presence of particular pharmaceutical substance to more complicated requirements of pharmacopoeial monographs. It is an important task in the pharmaceutical industry. Quality control not only protects the manufacturer against compensation claims, but also guarantees the patient a safe and effective product. QC measurements include in-process bulk and finished drug product testing, stability testing of the drug formulation, testing of equipment for absence of drug substance and detergent (cleaning validation), microbial testing of drug product etc. Quality control measurements generate a large amount of chemical data that the analysts have to manually transfer the results of the collected data to a spreadsheet application or to a software that provides the capability to transfer, manage and report the QC data automatically and error-free. The software also provides secure data storage and a consistent link between analytical methods, raw data and final results. Therefore, it is easy to show auditors how the results were generated. Established
5
quality standards are published periodically in pharmacopoeias and in some government publications. PHARMACEUTICAL DOSAGE FORMS A pharmaceutical dosage form is the physical form of a dose of a chemical compound used as a drug or medication intended for administration. Pharmaceutical dosage form can be classified into: (1) SOLID TYPE (a) Tablets Tablets are solid dosage forms containing therapeutic substances with or without suitable diluents and may be grouped, according to the method of manufacture, as compressed tablets or molded tablets. Majority of all tablets manufactured are made by compression, and compressed tablets are the most widely used dosage form. Tablets could be buccal tablets intended to be inserted in the buccal pouch; sublingual tablets intended to be inserted beneath the tongue (where the active ingredient is absorbed directly through the oral mucosa); effervescent tablets intended to release carbon dioxide when dissolved in water (contain, in addition to active ingredients, mixtures of acids such as citric acid, tartaric acid and sodium bicarbonate); chewable tablets intended to be chewed and oral tablets intended to be swallowed.
6
(b) Powders and granules Powders are intimate mixtures of dry, finely divided drugs and/or chemicals that may be intended for internal (Oral powders) or external (Topical powders) use. Clinically of importance, when drugs are too bulky to be formed into tablets or capsules of convenient size. Immediately prior to administration, oral powders are mixed in a beverage or apple sauce. Children and those adults who experience difficulty in swallowing tablets or capsules may find powders more acceptable. Bulk oral powders are limited to relatively non-potent drugs such as laxatives, antacids, dietary supplements, and certain analgesics that the patient may safely measure by the teaspoonful or capful. Other bulky powders include douche powders, tooth powders, and dusting powders. Dusting powders are impalpable powders intended for topical application. (c) Capsules Capsules are solid dosage forms in which the drug is
enclosed within either a hard or soft soluble container or
“shell.” The shells are usually formed from gelatin;
however, they also may be made from starch or other
suitable substances. Potent drugs are often mixed with
an inert diluent before being filled into capsules. Hard-
shell capsules typically are filled with powder, beads, or
granules. It may also contain semisolids or liquids
7
however, when encapsulated, one of the sealing
techniques must be employed to prevent leakage.
Furthermore, powder mixtures that tend to liquefy may
be dispensed in hard-shell capsules if an absorbent
such as magnesium carbonate, colloidal silicon dioxide,
or other suitable substance is used. Soft-shell capsules
made from gelatin (sometimes called softgels) or other
suitable material, require large-scale production
methods. The soft gelatin shell is somewhat thicker than
that of hard-shell capsules and may be plasticized by
the addition of a polyol such as sorbitol or glycerin. In
most cases, soft-shell capsules are filled with liquid
contents. Typically, active ingredients are dissolved or
suspended in a liquid vehicle such as vegetable oil;
lower-molecular-weight polyethylene glycols.
(d) Delayed-release tablets or capsules
These are enteric-coated tablets or capsules that are intended to delay the release of drug until the tablet or capsule has passed through the stomach. Such delay is important to alleviate potential problems of drug inactivation or gastric mucosal irritation. (e) Extended-release tablets or capsules These dosage forms are formulated in such manner as to make the contained drug available over an extended period of time following ingestion. Expressions such as “prolonged-action,” “repeat-action,” and “sustained-
8
release” have also been used to describe such dosage forms. (f) Lozenges These are solid preparations that are intended to dissolve or disintegrate slowly in the mouth. They contain one or more drugs, usually in a flavored, sweetened base. Molded lozenges are called pastilles while compressed lozenges are often referred to as troches. They are usually intended for treatment of local irritation or infections of the mouth or throat but may contain active ingredients intended for systemic absorption after swallowing.
(2) SEMI-SOLID TYPE
(a) Creams
Creams are semisolid dosage forms containing one or more drug substances dissolved or dispersed in a suitable base. They are formulated either as water-in-oil or oil-in-water emulsions. However, products consisting of oil-in-water emulsions or aqueous microcrystalline dispersions of long-chain fatty acids or alcohols that are water washable and more cosmetically and aesthetically acceptable are also considered to be creams. (b) Ointments Ointments are semisolid preparations intended for external application to the skin or mucous membranes. Ointment bases recognized for use as vehicles fall into
9
four general categories: the hydrocarbon bases (serve to keep medicaments in prolonged contact with the skin and act as occlusive dressings); the absorption bases (permit the incorporation of aqueous solutions with the formation of a water-in-oil emulsion and also permit the incorporation of additional quantities of aqueous solutions into water-in-oil emulsion); the water-removable bases (are oil-in-water emulsions and medicaments in these bases are more effective than in hydrocarbon bases); and the water-soluble bases (are water-removable bases and, in addition, contain no water-insoluble substances such as petrolatum, anhydrous lanolin, or waxes). Each therapeutic ointment possesses as its base a representative of one of these four general classes. For example petrolatum is mainly used as a base for ophthalmic drugs, while, absorption bases, water-removable bases, and water-soluble bases may be desirable for water-soluble drugs. All must be nonirritating to the eye. (c) Gels Gels (also called jellies) are semisolid systems consisting of either suspensions made up of small inorganic particles or large organic molecules interpenetrated by a liquid. A gel mass of two-phase system consists of a network of small discrete particles (e.g., aluminum hydroxide gel) or relatively large particle size - magma (e.g., Bentonite Magma). Both gels and magmas may be thixotropic, forming semisolids on
10
standing and becoming liquid on agitation. They should be shaken before use to ensure homogeneity and should be labeled to that effect. Single-phase gels consist of organic macromolecules uniformly distributed throughout a liquid in such a manner that no apparent boundaries exist between the dispersed macromolecules and the liquid and may be made from synthetic macromolecules (e.g., Carbomer) or from natural gums (e.g., Tragacanth). The latter preparations are also called mucilages. Although these gels are commonly aqueous, alcohols and oils may be used as the continuous phase. They can be used to administer drugs topically or into body cavities. (d) Pastes Pastes are semisolid dosage forms that contain one or more drug substances intended for topical application. One class is made from a single-phase aqueous gel (e.g., Carboxymethylcellulose Sodium Paste) while the other class, the fatty pastes (e.g., Zinc Oxide Paste), consists of thick, stiff ointments that do not ordinarily flow at body temperature, and therefore serve as protective coatings over the areas to which they are applied. Pastes tend to absorb serous secretions, and are less penetrating and less macerating than ointments, so that they are preferred for acute lesions that have a tendency towards crusting, vesiculation, or oozing. A dental paste is intended for adhesion to the mucous membrane for local effect.
11
(3) PHARMACEUTICAL INSERTS (a) Suppositories
Suppositories are solid bodies of various weights and shapes, adapted for introduction into the rectal, vaginal, or urethral orifice of the human body. They usually melt, soften, or dissolve at body temperature and may act as a protectant or palliative to the local tissues at the point of introduction or as a carrier of therapeutic agents for systemic or local action. Suppository bases usually employed are cocoa butter, glycerinated gelatin, hydrogenated vegetable oils, mixtures of polyethylene glycols of various molecular weights, and fatty acid esters of polyethylene glycol (surfactants of polyoxyethylenesorbitan fatty acid esters and the polyoxyethylene stearates). (b) Implants (pellets) Implants or pellets are small sterile solid masses
consisting of a highly purified drug (with or without
excipients) made by compression or molding. They are
intended for implantation in the body (usually
subcutaneously) for the purpose of providing continuous
release of the drug over long periods of time. Implants
are administered by means of a suitable special injector
or surgical incision. This dosage form has been useful in
the administration of hormones such as testosterone or
estradiol.
12
(4) LIQUID DOSAGE FORMS (a) Solutions Solutions are liquid preparations that contain one or more chemical substances dissolved in a suitable solvent or mixture of mutually miscible solvents. They are classified according to route of administration, such as “Oral Solutions” and “Topical Solutions,” or by their solute and solvent systems, such as “Spirits,” “Tinctures,” and “Waters.” Solutions intended for parenteral administration are officially entitled “Injections” (i) Oral solutions: They are liquid preparations, intended for oral
administration, and contain one or more substances
with or without flavoring, sweetening, or coloring agents
dissolved in water or cosolvent-water mixtures.
Preparations dispensed as soluble solids or soluble
mixtures of solids, with the intent of dissolving them in a
solvent and administering them orally, are designated
“for Oral Solution”. Those containing high
concentrations of sucrose or other sugars traditionally
have been designated as Syrups. Other additives that
might be present in oral solutions include sorbitol or
glycerin (to inhibit crystallization and to modify solubility,
taste, mouth-feel, and other vehicle properties);
13
antimicrobial agents (to prevent the growth of bacteria,
yeasts, and molds); sweetening agents and thickening
agents (such as the cellulose gums). Viscid sweetened
solutions, containing no sugars but sobitol or
aspartame, are occasionally prepared as vehicles for
administration of drugs to diabetic patients. Oral
solutions, that contain alcohol as a cosolvent, have
been traditionally designated as Elixirs. However, many
others designated as Oral Solutions also contain
significant amounts of alcohol. To be designated as an
Elixir, however, the solution must contain alcohol.
(ii) Topical Solutions: Topical solutions are solutions, usually aqueous but often containing other solvents, such as alcohol and polyols, intended for topical application to the skin, orto the oral mucosal surface. (iii) Otic Solutions: These are solutions, intended for instillation in the outer ear. They are aqueous, or are solutions prepared with glycerin or other solvents and dispersing agents. (iv) Ophthalmic Solutions: Ophthalmic solutions are sterile solutions, essentially
free from foreign particles, suitably compounded and

14
packaged for instillation into the eye. Factors such as
inherent toxicity of the drug itself, isotonicity value, the
need for buffering agents and preservative, sterilization,
and proper packaging are carefully considered while
preparing these dosage forms. Similar considerations
are also made for nasal and otic products.
(v) Irrigations: Irrigations are sterile solutions intended to bathe or flush
open wounds or body cavities and are used topically,
never parenterally.
(vi) Injections:
Injections are preparations intended for parenteral
administration or for constituting or diluting a parenteral
product prior to administration
(b) Supensions
Suspensions are liquid preparations that consist of solid particles dispersed throughout aliquid phase in which the particles are not soluble. Some suspensions are prepared andready for use, while others are prepared as solid mixtures intended for constitution justbefore use with an appropriate vehicle and are designated “for Oral Suspension”. To prevent caking and solidification upon standing with a resulting difficulty in redispersing the suspension upon agitation, suitable ingredients that
15
increase viscosity and the gel stateof the suspension, such as clays, surfactants, polyols, polymers, or sugars, should beadded. Some suspensions are prepared in sterile form and are used as Injectables, as well as for ophthalmic and otic administration. Suspensions should not be injected intravenously or intrathecally. Those intended for any route of administration should contain suitable antimicrobial agents to protect against bacteria, yeast, and mold contamination. Suspensions should always be shaken well before use to ensure uniform distribution of the solid in the vehicle, thereby ensuring uniform and proper dosage.
(i) Ophthalmic suspensions:
Ophthalmic suspensions are sterile liquid preparations
containing solid particles dispersed in a liquid vehicle
intended for application to the eye. Such suspensions
should contain the drug in a micronized form to prevent
irritation and/or scratching of the cornea. Ophthalmic
suspensions should never be dispensed if there is
evidence of caking or aggregation.
(ii) Oral Suspensions: These are liquid preparations containing solid particles dispersed in a liquid vehicle, with suitable flavoring agents, intended for oral administration. Some suspensions labeled as “Milks” or “Magmas” fall into this category.
16
(iii) Topical Suspensions: Topical suspensions are liquid preparations containing solid particles dispersed in a liquid vehicle, intended for application to the skin. Some suspensions labeled as “Lotions” fall into this category. (iv) Otic Suspensions: Otic suspensions are liquid preparations containing micronized particles intended for instillation in the outer ear. (c) Emulsions Emulsions are two-phase systems in which one liquid is dispersed throughout another liquid in the form of small droplets. Where oil is the dispersed phase and an aqueous solution is the continuous phase, the system is designated as an oil-in-water emulsion. Conversely, where water or an aqueous solution is the dispersed phase and oil or oleaginous material is the continuous phase, the system is designated as a water-in-oil emulsion. Emulsions are stabilized by emulsifying agents (surfactants) that prevent coalescence, (the merging of small droplets into larger droplets and, ultimately, into a single separated phase). The surfactants reduce the interfacial tension between the phases, thus increasing the ease of emulsification upon mixing. All emulsions require an antimicrobial agent because the aqueous phase is prone to the growth of
17
microorganisms. Preservatives commonly used in emulsions include methyl-, ethyl-, propyl-, and butyl-parabens, benzoic acid, and quaternary ammonium compounds. (d) Inhalations Inhalations are drugs or solutions or suspensions of one or more drug substances administered by the nasal or oral respiratory route for local or systemic effect. (i) Nebulizers: Nebulizers are used for the administration of inhalation solutions only if they give droplets sufficiently fine and uniform in size so that the mist reaches the bronchioles. Nebulized solutions may be breathed directly from the nebulizer or the nebulizer may be attached to a plastic face mask or intermittent positive pressure breathing (IPPB) machine. Inert gases are used for the nebulization of solutions of drug substances in sterile water for inhalation or in sodium chloride inhalation solution.
(ii) Metered-dose inhalers (MDIs): are propellant-
driven drug suspensions or solutions in liquified gas
propellant with or without a cosolvent and are intended
for delivering metered doses of the drug to the
respiratory tract. It contains multiple doses, often
exceeding several hundred. The most common single-
18
dose volumes delivered are from 25 to 100 µL (also
expressed as mg) per actuation.
(iii) Powders may also be administered by mechanical
devices that require manually produced pressure or a
deep inhalation by the patient.
(iv) Inhalers: Contain inhalants consisting of drugs or combination of drugs, that by virtue of their high vaporpressure, can be carried by an air current into the nasal passage where they exert their effect. (5) DELIVERY SYSTEMS These are dosage forms developed using modern technology that allow for the uniform release or targeting of drugs to the body. (a) Transdermal Systems A transdermal drug delivery system is a formulation or device that when applied to intact skin, are designed to deliver the drug(s) through the skin to the systemic circulation. Such a system typically comprises an outer covering (barrier), a drug reservoir, which may have a rate-controlling membrane, a contact adhesive applied to some or all parts of the system and the system/skin interface, and a protective liner that is removed before applying the system. Transdermal drug delivery system works by diffusion where by the drug diffuses from the drug reservoir, directly or through the rate-controlling
19
membrane and/or contact adhesive if present, and then through the skin into the general circulation. Some of these delivery systems are designed to provide drug delivery at a constant rate, such that a true steady-state blood concentration is achieved and maintained until the system is removed. Once it is removed, blood drug concentration declines at a rate consistent with the pharmacokinetics of the drug. The functional lifetime of the system is defined by the initial amount of drug in the reservoir and the release rate from the reservoir. The first transdermal system for systemic delivery—a three-day patch that delivers scopolamine to treat motion sickness—was approved for use in the United States in 1979. (b) Ocular System The ocular system containing the drug is placed in the lower conjunctival fornix from which the drug diffuses through a membrane at a constant rate. (c) Intrauterine System An intrauterine system is a delivery system intended for
release of drug over a much longer period of time, such
as one year. Typical example is the intrauterine
contraceptive systems.
IMPURITIES An impurity in a drug substance is defined as any component of the drug substance that is not the
20
chemical entity defined as the drug substance and affects the purity of active ingredient or drug substance. Alternatively, an impurity in a drug product is said to be any component of the drug product that is not the chemical entity defined as the drug substance or an excipient in the drug product. Therefore any extraneous material present in the drug substance has to be considered an impurity even if it is totally inert or has superior pharmacological properties. Classification 1. Impurities in drug substances (bulk drugs) Classified into organic impurities; inorganic impurities; organic volatile impurities (residual solvents); enantiomeric impurities and extraneous contaminants. (i) Organic impurities: This type of impurities in bulk drugs are considered to be innocuous by virtue of having no significant undesirable biological activity in the amounts present. These impurities can arise during the manufacturing process and/or storage of the drug substance and can beidentified or unidentified, volatile or nonvolatile. Typical examples are starting materials or intermediates that arise during synthesis (most common impurities); degradation products; reagents, ligands, and catalysts (less commonly impurities). (ii) Inorganic impurities:
21
This type of impurities may also be derived from the manufacturing processes used for bulk drugs. Examples are reagents, ligands, catalysts (rare impurities) and heavy metals(main sources of heavy metals are the water and can easily be avoided using demineralized water and glass-lined reactors). (iii) Organic volatile impurities: Organic volatile impurities relate to residual solvents that may be found in the drug substance. Depending on the possible risk to human health, residual solvents are divided into three classes, namely: class 1 – known or suspected human carcinogens or environmental hazards and should be avoided and examples are benzene (2 ppm limit), carbon tetrachloride (4 ppm limit), pyridine (200 ppm), methylene chloride (600 ppm), toluene (890 ppm), methanol (3000ppm); class 2 – inducers of irreversible toxicity such as neurotoxicity or teratogenicity and examples are acetonitrile (410 ppm), N, N-dimethylformamide (880 ppm), dichloromethane etc.; class 3 – low toxic potential, examples are acetic acid, ethanol, acetone, dimethylsulfoxide (DMSO). (iv) Enantiomeric impurities: These are stereochemistry-related impurities; that is, those compounds that have similar chemical structure but different spatial orientation. (v) Extraneous contaminants:
22
These include chemical and microbiological contaminants. Both may arise because of inadequate cleaning of equipment or facilities or isolation processes. 2. Impurities in pharmaceutical dosage forms A number of impurities can originate during storage or shipment of drug products. Impurities in drug products are classified mostly as degradation products of the drug product; reaction products of the drug product with an excipient and/or immediate container closure system. CONTROL OF IMPURITIES Impurity control in pharmaceutical compounds is necessary and important because it ensures drug quality and safety. Impurities are controlled during drug development and synthesis as well as in drug substances, excipients and drug products. Thus, various methods and techniques have been employed by drug manufacturers in order to ensure that impurities in drug substances or drug products are controlled and comply with official specifications. Such compliance shall be based on qualification of limits for impurities and acceptance criteria for impurities. Qualification of limits for impurities Qualificationis the process of acquiring and evaluating data that establish the biological safety of an individual
23
impurity or a given impurity profile at the level(s) being considered. A pharmaceutical dosage form (drug product) would be considered qualified if the level of any degradation product present in the drug product has been adequately tested in safety and/or clinical studies. Degradation products that are also significant metabolites present in animal and/or human studies are also considered qualified. If a drug product contains two or more drug substances, the limit for any identified impurity applies to the particular drug substance from which it is derived. However, for an unidentified impurity, the limit should normally apply to whichever drug substance leads to the more stringent limit for the impurity, unless it can be clearly demonstrated that the unidentified impurity was derived from a specific drug substance. The limit should take into account the maximum daily dose of each drug substance in the combination product; the content of each drug substance in the combination product, the likely overall patient exposure to the substance and the associated official limit for unidentified impurities. Limits for levels of impurities in an existing drug substance and/or an associated drug product are considered qualified when impurity levels are not more than the limits in an official monograph. Only those impurities designated as qualified in such monographs are subject to the limits specified in the monograph. Such official monographs include United States Pharmacopoeia (USP), British or European Pharmacopoeia (BP or EP), International
24
Conference on Harmonisation (ICH) etc. However, where there is no official monograph one or more of the following criteria are met: levels of impurities are not more than the applicable ICH qualification thresholds; the observed level and the proposed acceptance criterion for the impurity are adequately justified by the scientific literature; appropriate toxicological data are available to demonstrate the safety of the impurity at the proposed levels; the impurity is shown to be a significant metabolite in animal or human studies. (i) Qualification Thresholds: International Conference on Harmonization guidelines recommended that qualification thresholds be based on the maximum daily dose of the drug substance. When these qualification thresholds are exceeded, it is recommended that impurity levels be qualified. Qualification threshold could be lowered when there is evidence that an impurity in certain drug classes or therapeutic classes has previously been associated with adverse reactions in patients. Conversely, when the concern for safety is low a higher threshold for qualifying impurities may be appropriate. The recommended thresholds are presented in Tables 1 and 2 respectively.
25
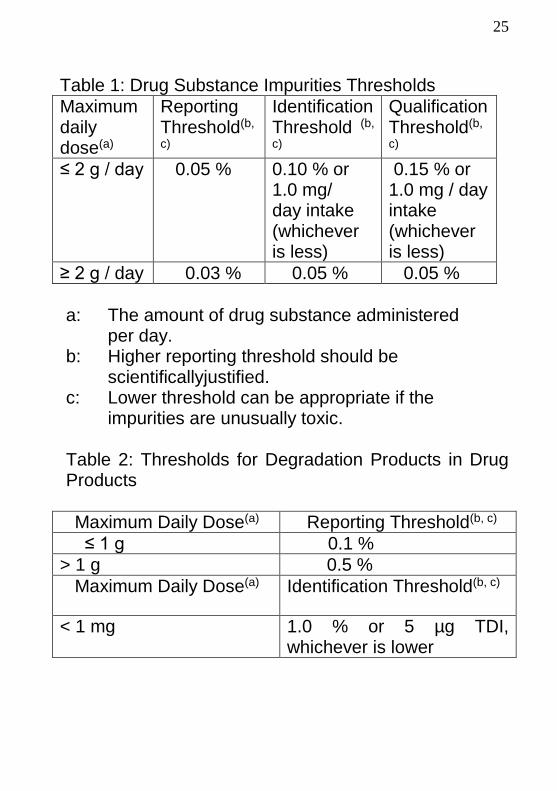
Table 1: Drug Substance Impurities Thresholds
Maximum daily dose(a)
Reporting Threshold(b,
c)
Identification Threshold (b,
c)
Qualification Threshold(b,
c)
≤ 2 g / day 0.05 % 0.10 % or 1.0 mg/ day intake (whichever is less)
0.15 % or 1.0 mg / day intake (whichever is less)
≥ 2 g / day 0.03 % 0.05 % 0.05 %
a: The amount of drug substance administered
per day. b: Higher reporting threshold should be
scientificallyjustified. c: Lower threshold can be appropriate if the
impurities are unusually toxic. Table 2: Thresholds for Degradation Products in Drug Products
Maximum Daily Dose(a) Reporting Threshold(b, c)
≤ 1 g 0.1 %
> 1 g 0.5 %
Maximum Daily Dose(a) Identification Threshold(b, c)
< 1 mg 1.0 % or 5 µg TDI, whichever is lower
26
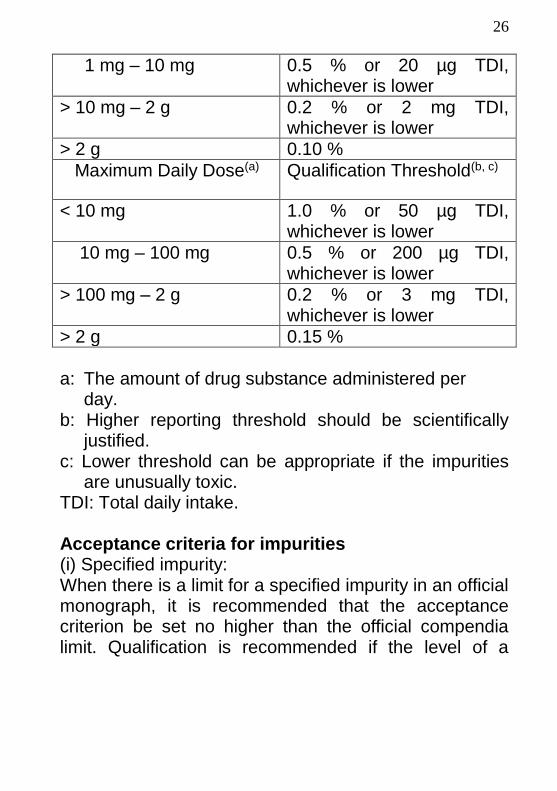
1 mg – 10 mg 0.5 % or 20 µg TDI, whichever is lower
> 10 mg – 2 g 0.2 % or 2 mg TDI, whichever is lower
> 2 g 0.10 %
Maximum Daily Dose(a) Qualification Threshold(b, c)
< 10 mg 1.0 % or 50 µg TDI, whichever is lower
10 mg – 100 mg 0.5 % or 200 µg TDI, whichever is lower
> 100 mg – 2 g 0.2 % or 3 mg TDI, whichever is lower
> 2 g 0.15 %
a: The amount of drug substance administered per
day. b: Higher reporting threshold should be scientifically
justified. c: Lower threshold can be appropriate if the impurities
are unusually toxic. TDI: Total daily intake. Acceptance criteria for impurities (i) Specified impurity: When there is a limit for a specified impurity in an official monograph, it is recommended that the acceptance criterion be set no higher than the official compendia limit. Qualification is recommended if the level of a
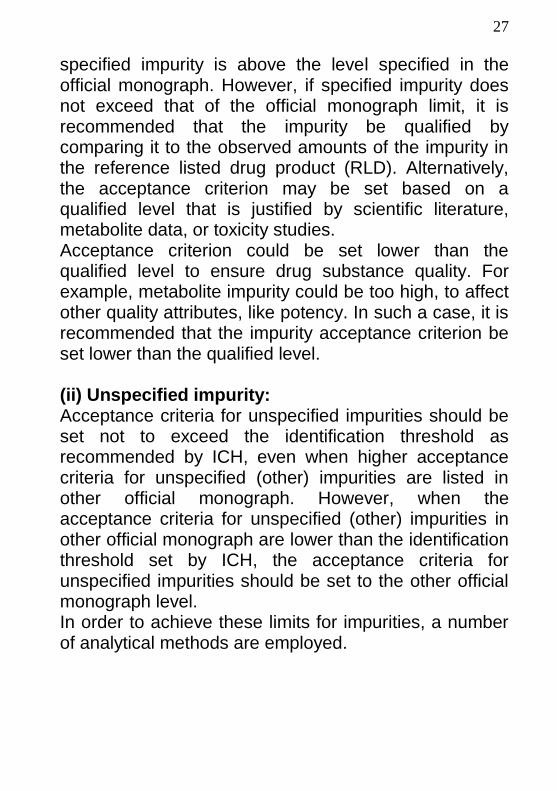
27
specified impurity is above the level specified in the official monograph. However, if specified impurity does not exceed that of the official monograph limit, it is recommended that the impurity be qualified by comparing it to the observed amounts of the impurity in the reference listed drug product (RLD). Alternatively, the acceptance criterion may be set based on a qualified level that is justified by scientific literature, metabolite data, or toxicity studies. Acceptance criterion could be set lower than the qualified level to ensure drug substance quality. For example, metabolite impurity could be too high, to affect other quality attributes, like potency. In such a case, it is recommended that the impurity acceptance criterion be set lower than the qualified level. (ii) Unspecified impurity: Acceptance criteria for unspecified impurities should be set not to exceed the identification threshold as recommended by ICH, even when higher acceptance criteria for unspecified (other) impurities are listed in other official monograph. However, when the acceptance criteria for unspecified (other) impurities in other official monograph are lower than the identification threshold set by ICH, the acceptance criteria for unspecified impurities should be set to the other official monograph level. In order to achieve these limits for impurities, a number of analytical methods are employed.
28
(1)Methods to control impurities arising from starting materials or intermediates during synthesis
Affinity purification- used to control proteineous drugs by retaining them on a column through their affinity to antibodies, enzymes or receptors which have been immobilized on the column. Solvent extraction – the impure compound is dissolved in an organic solvent. For acidic compounds, aqueous sodium hydroxide is added and well mixed. The acid compound reacts with the base to form a salt that is soluble in the aqueous solution. The organic layer that contains the impurities is discarded. The aqueous layer containing the acidic compound is acidified and extracted into a new layer of organic solvent. Solid-phase extraction (SPE) method - uses a solid phase and a liquid phase to isolate the impurity of interest from a solution. It is usually used to clean up a sample before using a chromatographic or other analytical method to quantitate the amount of analyte(s) in the sample.
Recrystallization - a solvent is employed in which the impurity is either completely insoluble or more freely soluble than the drug substance. A saturated solution of drug substance is prepared. The best solvent for recrystallization is that in which the drug substance is
29
poorly soluble at room temperature but soluble at higher temperature. The drug substance then will recrystallize (or precipitate) from the solution upon cooling, while the impurity remains in solution. Chromatography - is an effective and very useful method of separating a drug substance from impurity. The principle is based on how well they are adsorbed on the stationary phase, versus how well they dissolve in the mobile phase. The components with greater affinity for the mobile phase will move faster than those components with greater affinity for the stationary phase, causing the components to separate. There are many chromatographic methods characterized by the nature of the stationary and mobile phases. Among these methods, column chromatography, thin-layer chromatography and paper chromatography are more common ones. Filtration or centrifugation - Filtration is a mechanical method to separate solids from liquids by passing the feed stream through a porous sheet such as a cloth or membrane, which retains the solids and allows the liquid to pass through while centrifugation is a process in which light particles are revolved over high speed with the help of electric motor so that the fine particles which do not settle at bottom would settle down. Applied very often in thin-layer chromatography where the scraped sorbent containing the drug substance is extracted with
30
a suitable solvent, and then followed by filtration or centrifugation. The solvent is removed to collect the desired drug substance.
(2)Methods to control impurities of drug substance (bulk drug) or drug product Such impurities arise from method related; environmental related (exposures to adverse temperatures, light-especially UV light, humidity); ageing; mutual interaction amongst ingredients; degradation (hydrolysis, oxidation, photolytic cleavage, decarboxylation). The methods include: (a) Identification method (i)Reference standard method: Reference standards serve as the basis of evaluation of both process and product performance and are the benchmarks for assessment of drug safety for patient consumption. They are needed, not only for the active ingredients in dosage forms but also for impurities, degradation products, starting materials, process intermediates, and excipients. (ii) Spectroscopic method: Ultraviolet/Visible absorption spectrophotometer (UV/VIS) - used for analysis of a diverse array of compounds containing chromophores. Infrared spectroscopy (IR) - widely used and primarily
31
for the identification and structural analysis of organic materials. The spectra of an unknown, is compared to samples of known materials. In addition to comparison with known compounds, reference charts displaying the absorption wave numbers of chemical groups are used. It is difficult to use for mixtures, and aqueous samples require special cells. Nuclear magnetic resonance spectroscopy (NMR) - is a property of the nucleus of an atom, concerned with what is known as nuclear spin (I). This is equivalent to the nucleus acting like a miniature bar magnet. NMR plays an important role in determining the structure of unknown organic molecules and the study of organic reactions and processes. Mass spectroscopy (MS) - produces charged particles (ions) from the chemical substances that are to, be analyzed. The MS then uses electric and magnetic fields to measure the mass (“weight”) of the charged particles. The magnetic field separates ions according to their momentum (product of mass and velocity), while the electric field separates ions according to their kinetic energy (1/2 mv2). The information in mass spectrum are: exact mass (provides elemental composition); fragmentation (provides structure and fingerprint); isotope abundance (provides presence and number of certain elements).
32
(b) Separation method Separation method is regularly being used for separation of impurities and degradation products. Examples are capillary electrophoresis (CE), chiral separations, gas chromatography (GC); supercritical fluid chromatography (SFC); thin-layer chromatography (TLC); gas chromatography (GC); high performance liquid chromatography (HPLC); high performance thin-layer chromatography (HPTLC). (c) Isolation method Any of the following methods could be employed: solid-phase extraction methods, liquid-liquid extraction methods, accelerated solvent extraction methods, supercritical fluid extraction, column chromatography, flash chromatography, thin-layer chromatography, gas chromatography, high performance liquid chromatography, high performance thin-layer chromatography, capillary electrophoresis, supercritical fluid chromatography. (d) Characterization method For characterization of impurities, different techniques most often used include: atomic emission spectroscopy (AES) - is an important technique for the multi-element analysis of a wide range of materials and atomic or ionic line is used for analysis; infrared spectroscopy; nuclear magnetic resonance spectroscopy; mass spectroscopy; thin-layer chromatography, gas chromatography, high
33
performance liquid chromatography, high performance thin-layer chromatography, capillary electrophoresis, supercritical fluid chromatography. If single method fails to provide the necessary selectivity, orthogonal coupling of chromatographic techniques such as HPLC-TLC and HPLC-CE, or coupling of chromatographic separations with information rich spectroscopic methods such as HPLC-MS or HPLC-NMR may need to be contemplated. HPLC coupled with a diode array UV detector and a mass spectrometer (HPLC-DAD-MS), and such other techniques are almost routinely used. FINANCIAL IMPLICATION Control of impurities is one of many requirements highly regulated Pharmaceutical Manufacturing Companies must compile with, prior to the sale of their drug substances or drug products. The financial implications in the control of impurities will be well understood if we know that the average cost for the determination of only one of such impurities namely organic volatile impurities (OVI) per sample could range from three hundred to five hundred dollars ($300.00-500.00). RESEARCH WORKS Hitherto, the lecture has tried to introduce the title of this inaugural lecture. However, the lecture cannot be concluded without discussing some of the research works carried out by the inaugural lecturer on impurity control. The class of impurities investigated were, the
34
degraded products in drug substances. In this inaugural lecture, only four out of those research works, on drug degradation shall discussed. They were chosen based on their different catalytic processes. (A)Identification of Methyl-biphenyltetrazole as a novel degradation product of irbesartan Irbesartan, 2-n –butyl-4-spirocyclopentane-1-[{(2’-
tetrazol-5-yl)biphenyl-4-yl}methyl]-2-imidazol-5-one is a
potent, long-acting nonapeptide A II receptor antagonist
with a high specificity for the angiotensin type 1 subtype.
Clinically, it is used in the treatment of hypertension,
diabetic neuropathy and heart failure. The hydrolytic
degradation of irbesartan was hydroxide ion catalyzed.
The degradation was observed to follow apparent first-
order rate kinetics. The isolation and separation of
irbesartan from its major degraded product was
achieved by high performance liquid chromatography.
Figure 1 illustrates the composition of HPLC system.
35
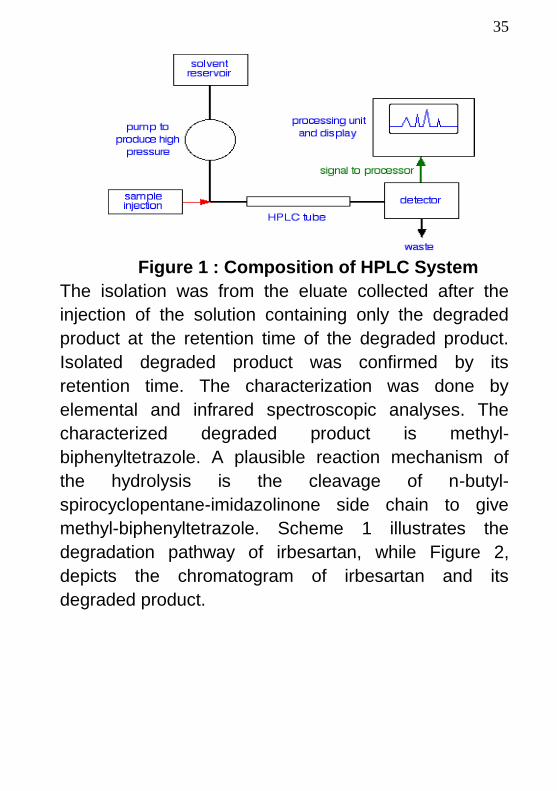
Figure 1 : Composition of HPLC System
The isolation was from the eluate collected after the
injection of the solution containing only the degraded
product at the retention time of the degraded product.
Isolated degraded product was confirmed by its
retention time. The characterization was done by
elemental and infrared spectroscopic analyses. The
characterized degraded product is methyl-
biphenyltetrazole. A plausible reaction mechanism of
the hydrolysis is the cleavage of n-butyl-
spirocyclopentane-imidazolinone side chain to give
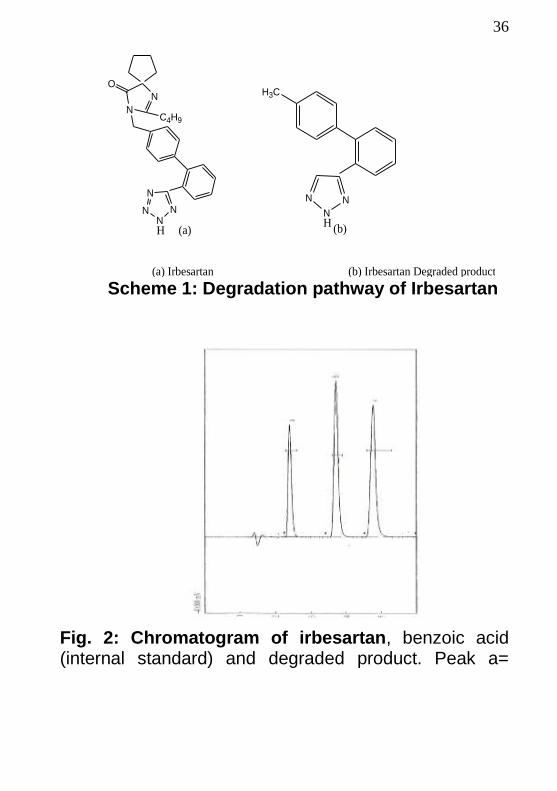
methyl-biphenyltetrazole. Scheme 1 illustrates the
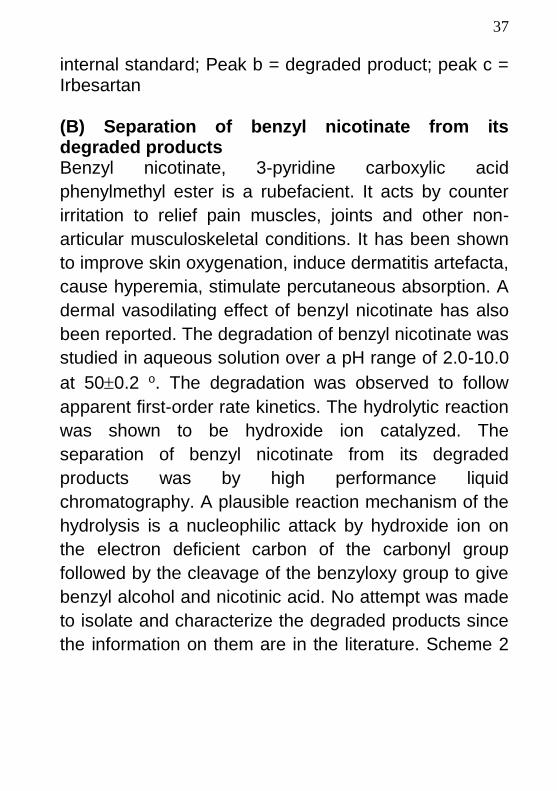
degradation pathway of irbesartan, while Figure 2,
depicts the chromatogram of irbesartan and its
degraded product.
36
N
NC4H9
N
N
NN
O
H (a)
NN
N
H3C
(b)
(a) Irbesartan (b) Irbesartan Degraded product
H
Scheme 1: Degradation pathway of Irbesartan
Fig. 2: Chromatogram of irbesartan, benzoic acid (internal standard) and degraded product. Peak a=
37
internal standard; Peak b = degraded product; peak c = Irbesartan (B) Separation of benzyl nicotinate from its degraded products Benzyl nicotinate, 3-pyridine carboxylic acid
phenylmethyl ester is a rubefacient. It acts by counter
irritation to relief pain muscles, joints and other non-
articular musculoskeletal conditions. It has been shown
to improve skin oxygenation, induce dermatitis artefacta,
cause hyperemia, stimulate percutaneous absorption. A
dermal vasodilating effect of benzyl nicotinate has also
been reported. The degradation of benzyl nicotinate was
studied in aqueous solution over a pH range of 2.0-10.0
at 500.2 o. The degradation was observed to follow
apparent first-order rate kinetics. The hydrolytic reaction
was shown to be hydroxide ion catalyzed. The
separation of benzyl nicotinate from its degraded
products was by high performance liquid
chromatography. A plausible reaction mechanism of the
hydrolysis is a nucleophilic attack by hydroxide ion on
the electron deficient carbon of the carbonyl group
followed by the cleavage of the benzyloxy group to give
benzyl alcohol and nicotinic acid. No attempt was made
to isolate and characterize the degraded products since
the information on them are in the literature. Scheme 2
38
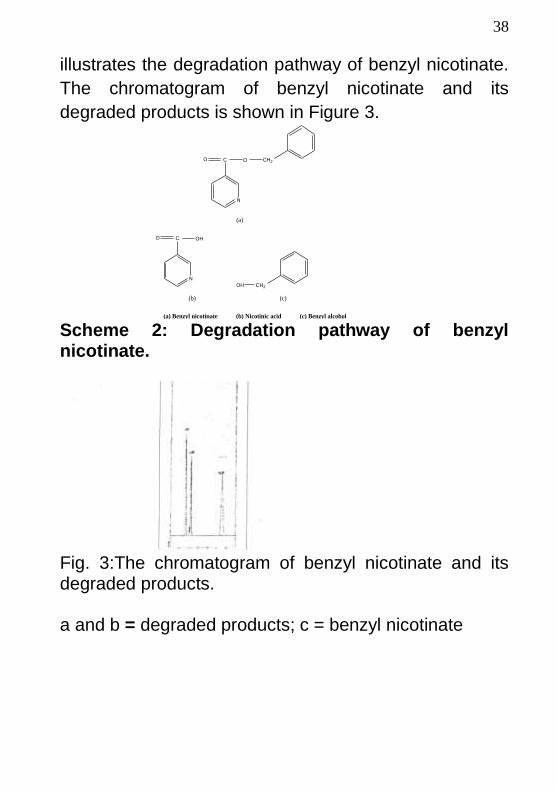
illustrates the degradation pathway of benzyl nicotinate.
The chromatogram of benzyl nicotinate and its
degraded products is shown in Figure 3.
N
CO O CH2
(a)
N
CO OH
(b)
OH CH2
(c)
(a) Benzyl nicotinate (b) Nicotinic acid (c) Benzyl alcohol Scheme 2: Degradation pathway of benzyl nicotinate.
Fig. 3:The chromatogram of benzyl nicotinate and its degraded products. a and b = degraded products; c = benzyl nicotinate
39
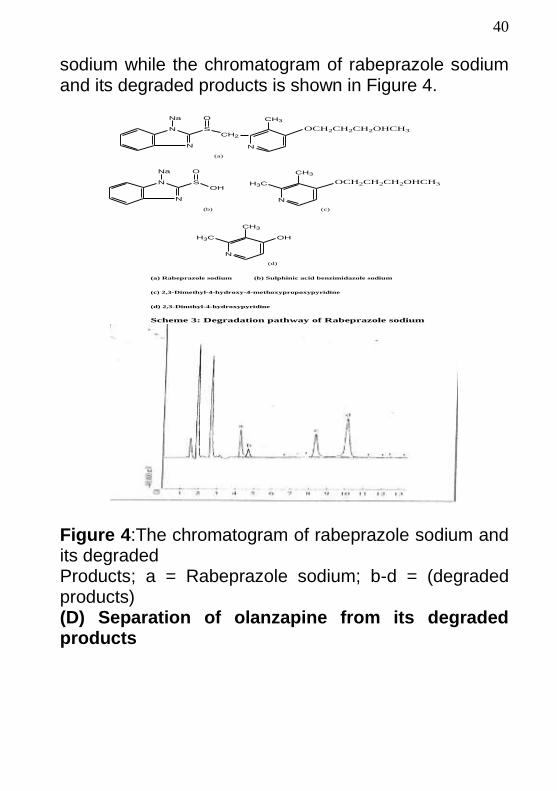
(C) Separation of rabeprazole sodium from its degraded products Rabeprazole sodium, {[(4-(3-methoxypropoxy)-3-methyl-2-pyridinyl]-methyl)-sulfinyl}-1H-benzimidazole sodium is a substituted benzimidazole proton pump inhibitor. Clinically, it is administered as delayed-release enteric coated tablets for the treatment of gastroesophageal reflux disease, duodenal ulcers and pathological hypersecretory conditions, including Zollinger-Ellison syndrome. Rabeprazole acts by blocking irreversibly the hydrogen-potassium adenosine triphosphate enzyme system (the K+/H+-ATPase – the proton pump) of the gastric parietal cell. It has been shown to be a more rapid inhibitor of proton pump when compared to other proton pump inhibitors such as omeprazole, lansoprazole or pantaprazole. The degradation reaction rate followed first-order kinetics. The breakdown of rabeprazole sodium was observed to be water and hydrogen ion catalyzed. The separation of rabeprazole sodium from its degraded products was by high performance liquid chromatography. The probable reaction mechanism of the hydrolysis is the cleavage of methyl-sulfinyl bond to give 2,3-Dimethyl-4-methoxypropoxy pyridine and sulphinic acid derivative of benzimidazole sodium, followed by subsequent cleavage of the 4-methoxypropoxy group to give 2,3-Dimethyl-4-hydroxyl pyridine. In this study, the degraded products were not isolated and characterized. Scheme 3 illustrates the degradation pathway of rabeprazole
40
sodium while the chromatogram of rabeprazole sodium and its degraded products is shown in Figure 4.
N
N
Na
SCH2
N
CH3
OCH2CH2CH2OHCH3
O
(a)
N
N
Na
SOH
N
CH3
OCH2CH2CH2OHCH3
O
(b)
H3C
(c)
N
CH3
OHH3C
(d)
(a) Rabeprazole sodium (b) Sulphinic acid benzimidazole sodium
(c) 2,3-Dimethyl-4-hydroxy-4-methoxypropoxypyridine
(d) 2,3-Dimthyl-4-hydroxypyridine
Scheme 3: Degradation pathway of Rabeprazole sodium
Figure 4:The chromatogram of rabeprazole sodium and its degraded Products; a = Rabeprazole sodium; b-d = (degraded products) (D) Separation of olanzapine from its degraded products
41
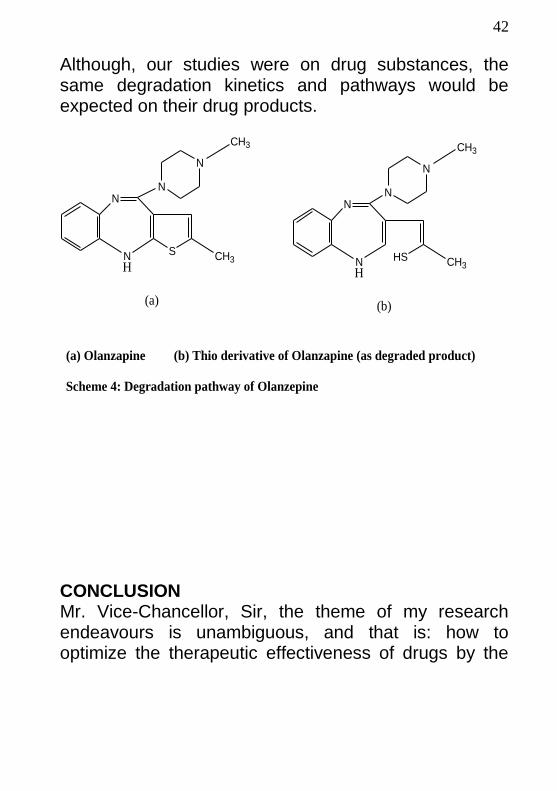
Olanzapine, 2-methyl-4-(4-methyl-1-piperazinyl)-10H-thieno [2,3-b][1,5]benzodiazepine is a second generation antipsychotic agent (so-called atypical antipsychotics) and belongs to the class of thienobenzodiazepine. Clinically, the drug is used in the management of schizophrenia and for the treatment of moderate to severe mania associated with bipolar disorder. It acts by antagonizing serotonin (5-HT2), muscarinic, histamine (H1) and adrenergic (α1) receptors as well as dopamine (D1/D2) receptors. The degradation reaction rates followed first-order kinetics with respect to olanzapine. The hydrolytic reaction was observed to be hydrogen and hydroxide ion – catalyzed. The separation of olanzapine from its degraded products was by thin-layer chromatographic and spectroscopic methods. The probable mechanism of reaction of acid-catalyzed degradation involves protonation of the sulphur atom of the thieno moiety, followed by the rupture of the C-S bond adjacent to diazepine ring. For base-catalyzed degradation, the mechanism could involve proton transfer from the secondary amine in the benzodiazepine ring to the sulfur atom, followed by electron delocalization and subsequent cleavage of the C-S bond. The study, made no attempt to determine and ioslate the degradation products and specific degradation pathways for olanzapine, however, the TLC analysis and absorbance spectra show the degraded product to be more polar than olanzapine. Scheme 4 illustrates the degradation pathway of olanzapine.
42
Although, our studies were on drug substances, the same degradation kinetics and pathways would be expected on their drug products.
N
S
N
N
NH
CH3
CH3
(a)
N
HS
N
N
NH
CH3
CH3
(b)
(a) Olanzapine (b) Thio derivative of Olanzapine (as degraded product)
Scheme 4: Degradation pathway of Olanzepine
CONCLUSION Mr. Vice-Chancellor, Sir, the theme of my research endeavours is unambiguous, and that is: how to optimize the therapeutic effectiveness of drugs by the
43
control of degradants (impurities) in drug products. The lecture therefore has attempted to show (a) what pharmaceutical quality control entails (b) types of pharmaceutical dosage forms (c) types of impurities in pharmaceutical products and various analytical techniques to control them (d) drug degradants as impurities (e) regulatory requirements for such impurity control. Another objective of the inaugural lecture is to bring to limelight the magnanimity of highly regulated Pharmaceutical Manufacturing Companies to people of the world vis-`a-vis the costs of their drug products. This magnanimity could be appreciated considering that the cost of testing a sample for residual solvents is in the range of three hundred to five hundred dollars ($300.00-500.00). This test is one out of many tests to be performed in an attempt to be in compliance with Federal Regulatory Agencies. Mr. Vice-Chancellor, Sir, I joined the services of this great University (1984) as a Graduate Assistant after my B.Pharm degree in 1982 from the University of Ife, Ile-Ife. I left for United States of America (1993) on a postdoctoral fellowship shortly after obtaining my Ph.D in 1990. I rejoined the University in 2007 and became a Professor in 2009. The inaugural lecturer has made some contributions, not only to knowledge through my publications, but also through successful supervision of a handful of graduate students. Currently, I am supervising three (3) Ph.D students working on projects that would generate data for optimal drug effectiveness.
44
In the area of administration and service since 2007, I had served a 3-year term as Head of Department of Pharmaceutical and Medicinal Chemistry and currently serving as the Head of the same Department. As I am an academic mentor to some people now, I also was mentored. I wish to especially acknowledge Prof. P. I. Akubue, who made it possible for me to be where I am today in the field of academics. Sir, I sincerely thank you for your love and support and ask Almighty God to continue to bless you and the family. My next gratitude goes to Prof. O. K. Udela who offered me the opportunity of being a staff of the Faculty of Pharmaceutical Sciences, University of Nigeria, Nsukka. I owe unalloyed gratitude to Prof. C. N. Aguwa for his love and for recognizing my potentials and giving me the opportunity to rejoin the Faculty in 2007. Sir, I sincerely thank you and may the Almighty God continue to bless you and the family. I am deeply indebted to Prof. A. Kar and Dr. (Mrs.) A. Singh for their academic contributions in my academic life. I thank in a very special way the immediate past vice-chancellor of this university, Prof. BathoOkolo for his fairness in professorial appraisals. Likewise, I immensely thank Prof. S. I. Ofefule, for his courage and fairness in Faculty staff appraisals. My special gratitude goes to Professors Onyejekwe (Uncle D), Onyekegbu and Osadebe all of Faculty of Engineering for their love and support. To my respected colleagues in the Department, I express my special thanks for your support. They include:
45
Prof. (Mrs.) P. O. Osadebe- a special friend, a mother and one who hardly says no to requests. G. C. Ebi- a difficult academic to deal with.Dr. (Mrs.) N. J. Nwodo- a very close friend, a mother and one who is always available to help. Dr. W. O. Obonga- a respectful and friendly colleague. Dr. E. O. Omeje- a very close family friend. This is an academic that I lack words to describe his administrative assistance to me, and the Department. A tireless one who would very happily execute all assignments.Dr.Omeje, I cannot thank you enough but I ask Almighty God to bless you and the family. Dr. M. Agbo- an out-spoken academic. Pharm. P. Uzor- thoughtful and hard-working academic Pharm. C. O. Nnadi- quiet and hard-working academic. Dr. (Mrs.) U. Odoh- though a very senior academic, she was listed last because shecurrently belongs to Department of Pharmacognosy and Environmental Medicine. A special friend, a mother, one who is always available to, assist people. I thank in a special way the non-academic staff of the Department, especially Pharm. Justus Nwaoga (a very close friend), Mrs. Rose Anyaoha (humble and
46
respectful), Mrs.UzomaObioma (hard-working and efficient administrative staff) and Mike Ugwoke (hard-working and efficient laboratory staff) for their support. I appreciate in a special way, the current Dean of the Faculty, Prof. E. Ibezim, the immediate past Dean, Prof. V. C. Okore and the Faculty Officer, Mrs.A. Nwodo. My special appreciations also go to all my colleagues in the Faculty as well as other staff and students of the Faculty. In a special way, I thank Engr. Sir. J. C. Anochie and Commandery 585, Trans-Ekulu, Enugu for their support. To the following, I express my immense gratitude: Prof. P. E. Chigbu. Dr. C. A. Nwakanma, Dr. J. K. Egbebike, Dr.AloyEzeabisili, Prof. F. O. Okafor, Prof. E. Oguejiofor, Prof. V. O. Ekechukwu, Prof. E. Ezeani, Prof. F. C. Chilaka, Prof. L. Anike, Prof. L. Ezeogu, Dr. Mike Egbebike, Arc. J. J. Emejulu, Arc. Chris. Okeke, Dr.E. Agwagom, Sir Bonny Nweke, Sir Obi Amadi, Barr. B. N. Chima, Dr.NworjiUgo, Prof. O. Njoku, Prof. T. Okonkwo, NduOkonkwo, Dr. (Mrs.) I. Echezona, Dr. Phil. Eze, Prof. (Mrs.) Okafor, Prof. P. Okoha, Prof. A. Falodun, Prof. C. Nwafia, Prof.Oparaji, Dr. T. Onyekaba, Pharm. I. Ugbene, Engr. H. Ejiofor, Rev.Fr.(Dr.) C. Okpalike, Rev. P. Umeh, Assoc. Prof. I. Uzochukwu, Assoc. Prof. F.B. Okoye, Mrs. P. Ejimofor, Mrs. V. Soto.
47
To my brothers and sisters (whom I love dearly), cousins (especially Chief W. Osieneme and family; Mrs. Agnes Obidiwe and family), uncles and aunts, I sincerely thank you for your love and support. Finally, to my beautiful wife and son, I especially thank you for your love, support and understanding. Mr. Vice-Chancellor, Sir, distinguished ladies and gentlemen, I thank you all for your attention. May Almighty God bless and take all of you home safely.
REFERENCES
Ahuja S, Scypinski S (2001) Handbook of Modern
Pharmaceutical Analysis, Academic Press, New York,
p.298.
Ahuja S (1992) Trace and Ultra trace Analysis by HPLC,
John Wiley, New York, p.84.
48
Allen LV, Popovich NG, Ansel AC (2010) Ansel’s
Pharmaceutical Dosage forms and Drug Delivery, 9th
edition, John Wiley New York.
Farmer S, Anderson P, Burns P, Velagalef R (2002)
Forced degradation of ibuprofen in bulk and tablet.
Pharm Tech 28: 42.
Gillis JC, Markham A (1997) Review of pharmacology
and clinical efficacy of irbesartan.Drugs 54: 885.
Gorog S (2006) The importance and challenges of
impurity profiling in Modern Pharmaceutical Analysis.
Trends in Analytical Chemistry, p.755
International Conference on Harmonization (2000)
Guidance on impurities in new drug substances. Federal
Register Q3A(R) 65(140): 45085.
International Conference on Harmonization (2000)
Guidance on impurities in new drug products. Federal
Register Q3B(R) 65(139): 44791.
International Conference on Harmonization (1997)
Impurities Q3C- Guidelines for residual solvents.
Federal Register 62(247): 67377.
49
International Conference on Harmonization (1999)
Specifications, Q6A: Test procedures and acceptance
criteria for new drug substances and new drug products.
Chemical Substances 65(146): 67488.
Joachim E (1998). The use of hyphenated LC-MS
technique for characterization of impurity profiles during
drug development. J Pharm Biomed Anal 18: 707
Katzung GB (2007) Antipsychotic agents and
lithium.Basic and Clinical Pharmacology, 10th edition,
McGraw Hill, New York, p.435.
Mbah CJ (2012) Identification of Methyl-
biphenyltetrazole as a novel degradation product of
irbesartan. J Chromatogr Separation Tech 3: 6.
Mbah CJ (2011) Olanzapine degradation kinetics in
aqueous solution. Die Pharmazie 66: 168.
Mbah CJ (2010) Degradation kinetics of benzyl
nicotinate in aqueous solution. Indian J Pharm Sci 72:
40.
Mbah CJ (2007) Kinetics of decomposition of
rabeprazole sodium in aqueous solution determined by
50
high performance liquid chromatography. Die
Pharmazie 62: 112.
Mbah CJ (2004) Kinetics of decomposition of irbesartan
in aqueous solution determined by high performance
liquid chromatography. Die Pharmazie 59: 920-922.
Pharmacoppeial Forum (2013) Pharmaceutical dosage
forms. 29(5): 1629.
Prakash A, Faulds D (1998) Pharmacology and clinical
efficacy of rabeprazole. Drugs 55: 261-267.
Waber B (2001) A review of irbesartan in
antihypertensive therapy; comparison with
antihypertensive agents. Current Ther Res 62: 505-523.
William MP, Paunder R (1999) The pharmacology of
rabeprazole. Aliment PharmacolTher 13: 3-10.
51
INAUGURAL LECTURES
OF THE UNIVERSITY OF NIGERIA, NSUKKA
1. Prof. K. Nzimir o – 1976
Title: the Crisis in the Social Sciences: The
Nigerian Situation
2. Prof. Chika Okonjo – 1976
Title: Economic Science, Imperialism and Nigerian
Development.
3. Prof. K. S. Hegde, Vet. Medicine – 1977
Title:
4. Prof. D. I. Nwoga – 1977
52
Title: Visions Alternatives: Literary Studies in a
Transitional Culture.
5. Prof. J. A. Umeh – 1977
Title: Land Policies and Compulsory Acquisition of
Private Land for Public Purposes in Nigeria.
6. Prof. D. C. Nwafo – 1984
Title: The Surgeon as an Academic
7. Prof. G. E. K. Ofomata – 1985
Title: Soil Erosion in Nigeria: The views of a
Geomorphologist.
8. Prof. E. U. Odigboh – 1985
Title: Mechanization of cassava production and
processing: A Decade of Design and Development.
9. Prof. R. O. Ohuche – 1986
Title: Discovering what Learners have attained in
Mathematics.
10. Prof. S. C. Ohaegbulam – 1986
Title: Brain surgery: A luxury in a Developing Country
like Nigeria.
11. Prof. I. C. Ononogbu – 1998
Title: Lipids: Your Friend or Foe.
12. Prof. V. E. Harbor-Peters – 2001
53
Title: Unmasking some Aversive Aspects of Schools
Mathematics and Strategies for averting them.
13. Prof. P. O. Esedebe – 2003
Title: Reflections on History, Nation Building and the
University of Nigeria.
14. Prof. E. P. Nwabueze – 2005
Title: In the Spirit of Thespis: The Theatre Arts and
National Integration.
15. Prof. I. U. Obi – 2006
Title: What have I done as an Agricutlural Scientist?
(Achievements, Problems and Solution Proposals).
16. Prof. P. A. Nwachukwu – 2006
Title: A Journey through the Uncharted Terrain of Igbo
Linguistics.
17. Rev. Fr. Prof. A. N. Akwanya – 2007
Title: English Language learning in Nigeria: In search of
an enabling principle.
18. Prof. T. UzodinmaNwala – 2007
Title: The OtontiNduka Mandate: From Tradition to
Modernity.
19. Prof. J. A. Ibemesi – June 2007
Title: From studies in Polymers and Vegetable oils to
Sanitization of the Academic System.
54
20. Prof. Obi U. Njoku – June 2007
Title: Lipid Biochemistry: Providing New Insights in our
Environment.
21. Prof. Humphrey Assisi Asobie – July 2007
Title: Re-inventing the Study of International Relations:
From State and State Power to Man and Social Forces.
22. Prof.AloyEmekaAghaji – July 2007
Title: Prostate Cancer: Coping with the Monster in a
Third World Setting.
23. Prof. Eunice A. C. Okeke – August 2007
Title: Making Science Education Accessible to All.
24. Prof.Chibuike U. Uche – August 2007
Title: The future of the Past in Banking
25. Prof.Ossie O. Enekwe – September 2007
Title: Beyond Entertainment: A Reflection on Drama and
Theatre.
26. Prof.OnyechiObidoa – September 2007
Title: Life Does Not Depend On The Liver: Some
Retrospectives, Perspectives, And Relevance in
Xenobiosis, Chemoprevention And Capacity Building.
27. Prof.OkechukwuIbeanu – 2008
Title: Affluence and Affliction: The Niger Delta as a
Critique of Political Science in Nigeria.
55
28. Prof. Damian UgwutikiriOpata – 2008
Title: Delay and Justice in the Lore and Literature of
Igbo Extraction.
29. Rev. Fr. Prof.ElobuikeMalachyNwabuisi – 2008
Title: Education for What?
30. Prof. Michael C. Madukwe – 2008
Title: Practice Without Policy: The Nigerian Agricultural
Extension Service.
31. Prof. Anthony N. Eke – 2008
Title: Delay And Control In Differential Equations:
Apogee of Development.
32. Prof. Joe SonneChinyereMbagwu – 2008
Title: From Paradox To Reality: Unfolding the
Discipline of Soil Physics in Soil Science.
33. Prof.InnoUzomaNwadike – 2008
Title: Igbo Studies: From the Plantation of West Indies to
the Forest lands of West Africa, 1766 – 2008.
34. Prof. Benjamin ChukwumaOzumba – 2008
Title: Improving Maternal Health in Developing
Countries: The Nigerian Experience.
35. Prof. Henrietta NkechiEne-Obong – 2008
56
Title: Nutrition Science and Practice: Emerging Issues
and Problems in Food Consumption, Diet Quality and
Health.
36. Prof.AmaraucheChukwu – 2008
Title: Using Neglected Local Raw Materials In
Developing High Level International Health Manpower.
37. Prof. Samuel OgbonnaEnibe – 2008
Title: Engineering Systems Analysis and Optimization.
38. Prof. Michael IfeanyiUguru – 2008
Title: Crop Genetics and Food Security.
39. Prof. Alex I. Ikeme (KSM) – 2008
Title: Poly-Functional Egg: How can it be Replaced?
40. Prof.Chukwuma C. Soludo – 2008
Title: Financial Globalization and Domestic Monetary
Policy: Whither the Economics of the 21st Century.
41. Prof. Josephine IfeyinwaOkafor (Mrs) – 2008
Title: Fungal Diseases: A Serious Threat to Human
existence in recent Times.
42. Prof. C. C. Agu – 2008
Title: Understanding the ABC of the Financial System.
43. Prof. Polycarp E. Chigbu – 2009
57
Title: Semi-Latin Squares and Related “Objects”:
Statistics and Combinatorics Aspects.
44. Prof. Reuben U. Okafor – 2009
Title: 4-circle Base Triangular Model in Ageing and
Death Education.
45. Prof. Francisca NnekaOkeke – 2009
Title: Geomagnetic Research in Physics: The Journey So
Far.
46. Prof. Clara Ikekeonwu – 2009
Title: Language and Gender in Nigeria: Perception,
Pattern and Prospects.
47. Prof. Fabian C. Okafor – 2009
Title: The Varied Roles of Snails (Gastropod Molluscs)
in the Dynamics of Human Existence.
48. Prof.DenchrisNnabuikeOnah – 2009
Title: The Elegance and Success of Trypanosomes as
Parasites: Immunological Perspective.
49. Prof. Grace ChibikoOfforma – 2009
Title: Curriculum across Languages.
50. Prof. Doris UkanwamakaEgonu – 2010
Title: Illiteracy in a Century-Old Education System: The
Challenge of Adult Education in Nigeria.
51. Prof.UchennaMariestellaNzewi – 2010
58
Title: It’s all in the Brain: Of Gender and Achievement
in Science and Technology Education.
52. Prof. Beatrice A. Okeke-Oti – 2010
Title: They have Dignity and Worth and Therefore Need
Restoration.
53. Prof. Ernest Onwasigwe – 2010
Title: Paediatric Ophthalmology: Past, Present and
Future.
54. Prof. Chika Onwasigwe – 2010
Title: Disease Transition in Sub-Saharan Africa: The
Case of Non-Communicable Diseases in Nigeria.
55. Prof. Rich EnujiokeUmeh – 2010
Title: River Blindness: An Insight into Community
Directed Management of Endemic Diseases.
56. Prof. Eric C. Eboh – 2011
Title: Agricultural Economy of Nigeria: Paradoxes and
Crossroads of Multimodal Nature.
57. Prof. George O. S. Amadi – 2011
Title: Political Jaywalking and Legal Jiggery-Pokery in
the Governance of Nigeria: Wherein Lies the Rule of
Law?
58. Prof. Ola Oloidi – 2011
Title: The Rejected Stone: Visual Arts In An Artistically
Uninformed Nigerian Society.
59
59. Prof. Felicia N. Monye (Mrs) – 2011
Title: The Consumer and Consumer Protection in
Nigeria: Struggles, Burdens and Hopes.
60. Prof.GoddyChubaOkoye – 2011
Title: Enhancing Healthy Human Life Through
Bioengineering and Rehabilitation Medicine.
61. Prof. James C. Ogbonna – 2011
Title: Biotechnology and the Future of Human
Existence.
62. Prof.Ngozi M. Nnam – 2011
Title: Adequate Nutrition for Good Health: Is Our
Environment Nutrition Friendly?
63. Prof. Joseph C. Okeibunor – 2011
Title: Health Services for the Poor by the Poor: Lessons
for Addressing the Diverse Social Problems in Nigeria.
64. Prof.Okwesili Fred C. Nwodo- 2012
Title: From Water Beyond Wine to Longevity.
65. Prof. Fab ObetaOnah- 2012
Title: Engaging the Challenges of Human Resource
Management in Public Organisations in Nigeria.
66. Prof. Emmanuel OnyebuchiEzeani- 2012
60
Title: Delivering the Goods: Repositioning Local
Governments in Nigeria to Achieve the Millenium
Development Goals (MDGs).
67. Prof.MalachyIkechukwuOkwueze - 2012
Title: Religion: Indeed the ‘Opium’ of Life?
68. Prof. Emmanuel ChinedumIbezim- 2012
Title: Exploring the Exciting World of the Wonder
Agents called Drugs.
69. Prof. Patience Ogoamaka Osadebe-2012
Title: From the Lab. Bench Through the Gardens to the
Apothecary: Journey So Far.
70. Prof.Ifeoma Maureen Ezeonu – 2012
Title: People vs Bacteria: Bacteria Innocent Until
Proven Guilty.
71. Prof. Chika Njideka Oguonu-2012
Title: Fiscal Management And Grassroots Development:
Issues And Concerns In The Nigerian Context.
72. Prof. Gabriella I. Nwaozuzu -2013
Title: The Babelist Theory of Meaning.
73. Prof.Basden Jones C. Onwubere – 2013
Title: High Blood Pressure - The Silent Killer On The
Prowl: Combating The Albatross.
74. Prof.ObinaOnwujekwe – 2013
61
Title: Moving Nigeria From Low Coverage to Universal
health Coverage: Health System Challenges, Equity and
the Evidence.
75. Prof. David N. Ezeh -2013
Title: Science Without Women: A Paradox.
76. Prof. Elizabeth UgonwaAnyakoha - 2013
Title: Advancing A Framework For Showcasing Family
Concerns: Challenging The Challenges.
77. Prof. Micah OkwuchukwuOsilike – 2013
Title: Fixed Point Theory and Applications:
Contributions from Behind Closed Doors.
78. Prof. Augustine A. Ubachukwu – 2014
Title: Physics in Life and the end of all Things.
79. Engr. Prof. Daniel Oraeguna N. Obikwelu -2014
Title: Metallic Materials: Challenges in the 21st Century
Nigeria and Didactic Lessons from the 18th Century
Industrial Revolution.
80. Prof. (Mrs.) Catherine IkodiyaOreh – 2014
Title:Igbo Cultural Widowhood Practices: Reflections
On Inadvertent Weapons of Retrogression in Community
Development.
81. Prof. Charles LivinusAnijaAsadu– 2014
Title:The Soil We Do Not Know.
62
82. Prof. Basil ChukwuemekaEzeanolue - 2014
Title: Hear the Voice
83. Prof. Ifeoma Pamela Enemo – 2014
Title: Dangerous Families In Nigerian Law: A National
Albatross?
84. Prof. Christopher OkekeTagboUgwu– 2014
Title: The Demise of the African God/s: Fallacy or
Reality
85. Prof. Bernard ObialoMgbenka - 2014
Title: Clariid Catfish Aquaculture: a Panacea for Quality
Animal Protein Security
86. Prof. Benjamin Sunday ChudiUzochukwu
Title: Accelerating the Achievements of Health-Related
Millennium Development Goals: Social Determinants of
Health approach and Mainstreaming Health in All
Policies
87. Venerable Prof. Samuel Obiajulu Ike
Title: The Matter of the Heart
88. Prof. ChimdiMemnofuChuka-Okosa
Title: Beyond Vision