Embed Size (px)
Citation preview

Nuovi anticoagulanti orali (NOA): dalla farmacologia alla pratica clinica
Caratteristiche farmacologiche e farmacodinamiche
Prof. Alberto CorsiniUniversità degli Studi di Milano

2S1618
Principali caratteristiche farmacocinetiche di warfarin e dei nuovi anticoagulanti orali

Rapid Absorption
A single 150 mg dose in 12 healthy males.
• Rapid absorption (Cmax in up to 2 hours)
• Food delayed Cmax by 2 hours
• Surgery delayed Cmax by 4 hours
Stangier J.: Clin Pharmacokinet 2008:47:285-295


Foods does not affect the pharmacokinetic profile of apixaban
Foods does not affect the pharmacokinetic profile of apixaban
, ◊ Fasted (n = 23); ■ Fed (n = 22
Frost C et al Br J Clin Pharmacol. 2013 Nov;76(5):776-86

6S1618
Summary of absorption, metabolism, and excretion of dabigatran, rivaroxaban, and apixaban
Gong IY and Kim RB Canadian Journal of Cardiology 29 (2013) S24eS33

FDA 2012

P-GP InhibitorsAmiodarone: Dabigatran exposure in healthy subjects was
increased by 60 % in the presence of amiodarone
Verapamil: When dabigatran 150 mg was coadministered with oral verapamil, the Cmax and AUC of dabigatran were
increased,but the magnitude of this change differs, depending on
timing of administration and formulation of verapamil
Clarithromycin: Dabigatan exposure (AUC) in healthy subjects
was increased by about 19 % in the presence of clarithromycin
without any clinical safety concern
Current US labeling for dabigatran with rifampicin a P-GP inducers should be avoided
Pradaxa® – Summary of Product Characteristics

Semin Thromb Hemost. 2015 Mar;41(2):195-207

JA C C VO L . 6 4, 2 0 1 4 Flaker et al.O C T O B E R 1 4 , 2 0 1 4 : 1 5 4 1 – 5 0
Efficacy and Safety of apixaban vs. warfarin in patients with and without amiodarone on Stroke or Systemic Embolism

Adjusted outcomes of rivaroxaban vs warfarin stratified by amiodarone use at baseline
Adjusted outcomes of rivaroxaban vs warfarin stratified by amiodarone use at baseline
Steinberg BA et al. Heart Rhythm 2014;11:925–932)

12S1618
Principali caratteristiche farmacocinetiche di warfarin e dei nuovi anticoagulanti orali

Plasma concentration profiles of rivaroxaban and apixaban in atrial fibrillation patients
Plasma concentration profiles of rivaroxaban and apixaban in atrial fibrillation patients
Gong IY and Kim RB Canadian Journal of Cardiology 29 (2013) S24eS33

NOAC - Differences
l Mechanism of action l Pharmacokineticsl Pharmacodynamicsl Documentation of health benefits and long-term safety

15S1618
Comparative pharmacodynamicsof warfarin and of
NOAs
Desai J et al Gast End 78:227-239 2013
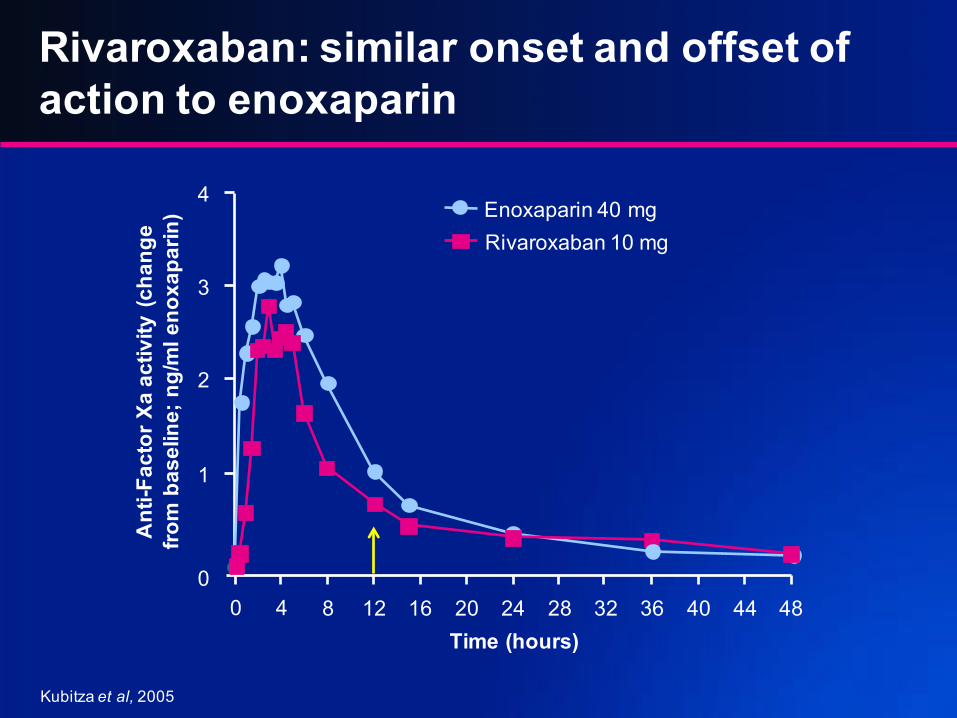
Rivaroxaban: similar onset and offset of action to enoxaparin
Kubitza et al, 2005
0 4 8 12 16 20 24 28 32 36 40 44 48
0
1
2
3
4
Ant
i-Fac
tor X
a ac
tivity
(cha
nge
from
bas
elin
e; n
g/m
l eno
xapa
rin)
Rivaroxaban 10 mg
Enoxaparin 40 mg
Time (hours)

Stroke or systemic embolic events by age and sex (A) and major bleeding subgroups (B)
Lancet 2014; 383: 955–62

Andreotti F et akl Eur Heart J. 2015 Dec 7;36(46):3238-49

Clin Pharmacokinet.2015;54(6):651-62
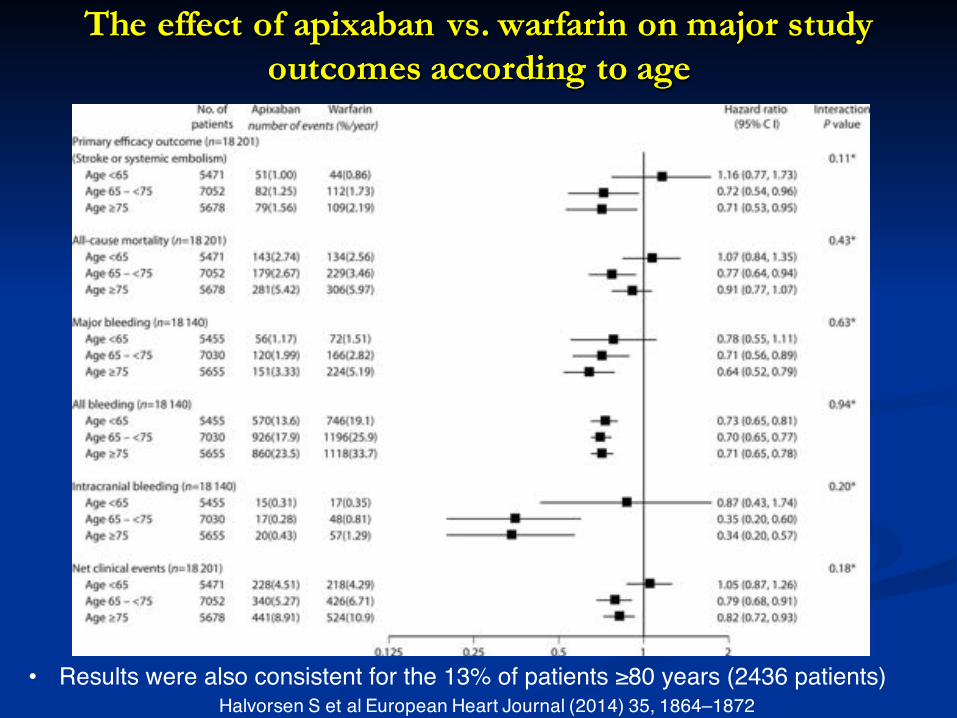
The effect of apixaban vs. warfarin on major study outcomes according to age
The effect of apixaban vs. warfarin on major study outcomes according to age
Halvorsen S et al European Heart Journal (2014) 35, 1864–1872• Results were also consistent for the 13% of patients ≥80 years (2436 patients)

Heidbuchel H et al. Europace. 2015 Oct;17(10):1467-507

Chest. 2016 Jan 18
Major bleeding, difference between the specific medications in patients witheCrCL 50-80 mL/min (A) and eCrCL <50mL/min (B)

Heidbuchel H et al. Europace. 2015 Oct;17(10):1467-507
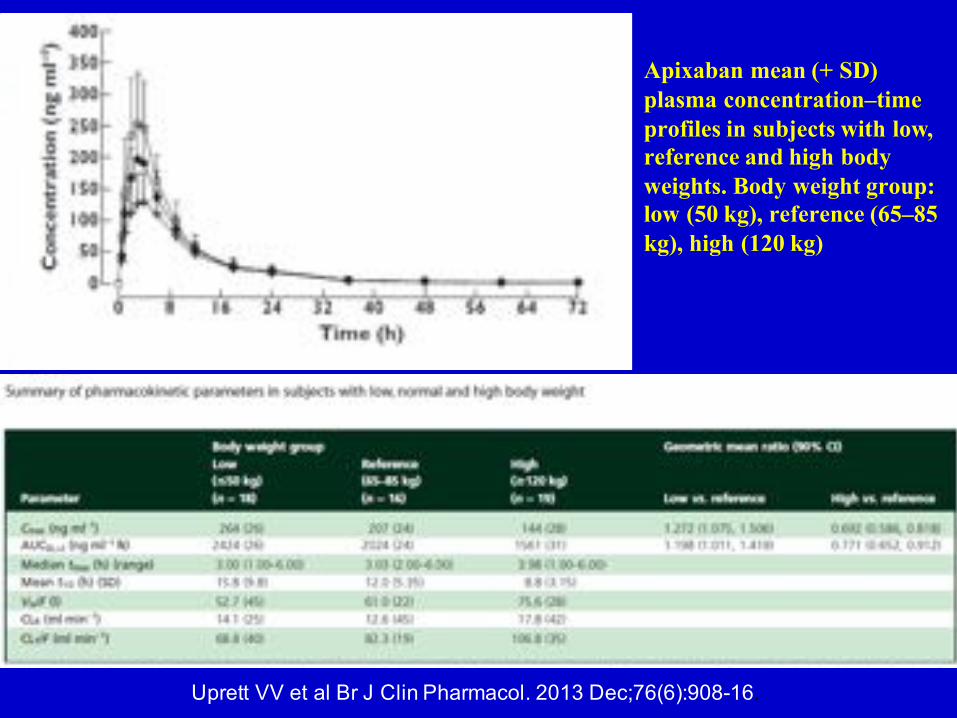
Apixaban mean (+ SD) plasma concentration–time profiles in subjects with low, reference and high body weights. Body weight group: low (50 kg), reference (65–85 kg), high (120 kg)
Uprett VV et al Br J Clin Pharmacol. 2013 Dec;76(6):908-16.

Risultati di efficacia e sicurezza dei NAOA: ictus o eventi embolici sistemici; B: sanguinamenti maggiori
Risultati di efficacia e sicurezza dei NAOA: ictus o eventi embolici sistemici; B: sanguinamenti maggiori
Lancet 2014; 383: 955–62

Bleeding rates of newer anticoagulants
DeWald TA, Becker RCJ Thromb Thrombolysis. 2014 Feb;37(2):217-33

Reilly PA et al. J Am Coll Cardiol 2014;63:321–8
Major Bleeding Event and Ischemic Stroke/SEE Vs Trough Plasma Concentration of Dabigatran


with rivaroxaban or apixabanPlasma concentration over time at steady state after treatment with rivaroxaban or apixaban
Clinical Pharmacology: Advances and Applications 2014:6 179–187
Inset: Individual plasma concentration–time profiles

Anti-FXa activity over time at steady state on day 4 of treatment with rivaroxaban or apixaban
Clinical Pharmacology: Advances and Applications 2014:6 179–187
Inset: Individual plasma concentration–time profiles

Distribution of CV values calculated from DOAC concentrations in treated patients at trough and peak

Testa S et al Thrombosis Research 137 (2016) 178–183

Once-daily vs. twice-daily dosing: difference between intake and predicted biological impact in general
Once-daily vs. twice-daily dosing: difference between intake and predicted biological impact in general
Europace.2015 Feb 17. pii: euu311.

Major gastrointestinal bleedingMajor gastrointestinal bleeding
Gomez-Outes A et al Thrombosis. 2013;2013:640723
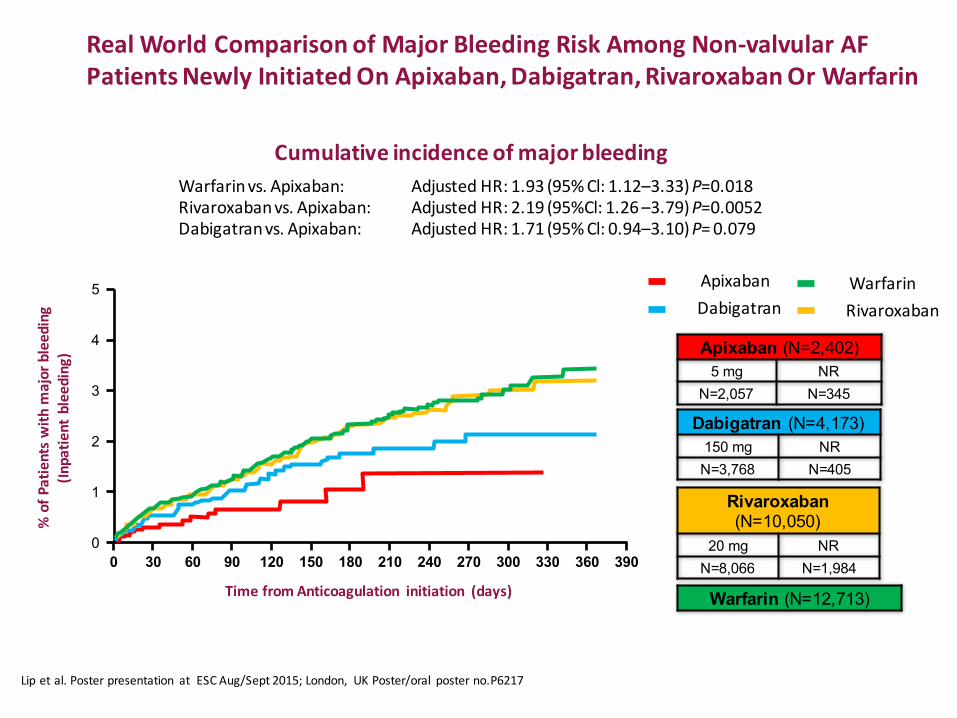
Warfarinvs.Apixaban: AdjustedHR:1.93(95%Cl:1.12–3.33)P=0.018Rivaroxabanvs.Apixaban:AdjustedHR:2.19(95%Cl:1.26–3.79)P=0.0052Dabigatranvs.Apixaban: AdjustedHR:1.71(95%Cl:0.94–3.10)P=0.079
Cumulativeincidenceofmajorbleeding
%ofP
atientsw
ithm
ajorbleeding
(Inpatie
ntbleeding)
TimefromAnticoagulation initiation (days)
0
0
1
2
3
4
5
30 60 90 120 150 180 210 240 270 300 330 360 390
WarfarinApixabanDabigatran Rivaroxaban
Dabigatran (N=4,173)
150 mg NR
N=3,768 N=405
Rivaroxaban (N=10,050)
20 mg NR
N=8,066 N=1,984
Apixaban (N=2,402)
5 mg NR
N=2,057 N=345
Warfarin (N=12,713)
Lipetal.Posterpresentation atESCAug/Sept2015;London, UKPoster/oral posterno.P6217
RealWorldComparisonofMajorBleedingRiskAmongNon-valvularAFPatientsNewlyInitiatedOnApixaban,Dabigatran,RivaroxabanOrWarfarin

DiscontinuationratesofNOACsinrealworld
Panetal. Presented attheESCCongress2014.Abstract #5112.
**Analysiscontrolled forother variablesincluding age,gender, onsetofembolic orprimaryischemicstroke, dyspepsiaorstomachdiscomfort, congestiveheartfailure, coronaryarterydisease,diabetes,hypertension, renaldisease,myocardialinfarction, historyofTIAorstrokeandhistoryofbleeding.
* Effectsizeisversusapixabanwhichactsasareferencecategory.
Retrospectivecohort studyNVAFpatientsnewlyprescribedaNOACornewlyprescribedwarfarinwithoutknee/hipreplacementsurgeriesinthetimeperiodofJan1– Dec31,2013
DiscontinuationratesofOACs
Dabigatranvs. apixaban*: HR**=1.581 (CI:1.451–1.721),P<0.0001Rivaroxabanvs. apixaban*: HR**=1.125(CI:1.121–1.317),P<0.0001Warfarinvs. apixaban*: HR**=1.638 (CI:1.514–1.772),P<0.0001
70
60
50
40
30
20
10
0
0 30 60 90 120 150 180 210 240 270 300 320 360 380Timefromanticoagulantinitiation(days)
%ofp
atientsw
ithdiscontin
uatio
n
Apixaban (n=2956)
Dabigatran (n=4495)
Rivaroxaban (n=12080)
Warfarin (n=14340)

Ip GYH and Lane DA J A C C V O L . 6 6 , N O. 2 1 , 2 0 1 5





























