Embed Size (px)
Citation preview

Nuovi anticoagulanti a confronto:
i risultati dei trials clinici
Walter Ageno Dipartimento di Medicina Clinica e Sperimentale
Università dell’Insubria – Varese
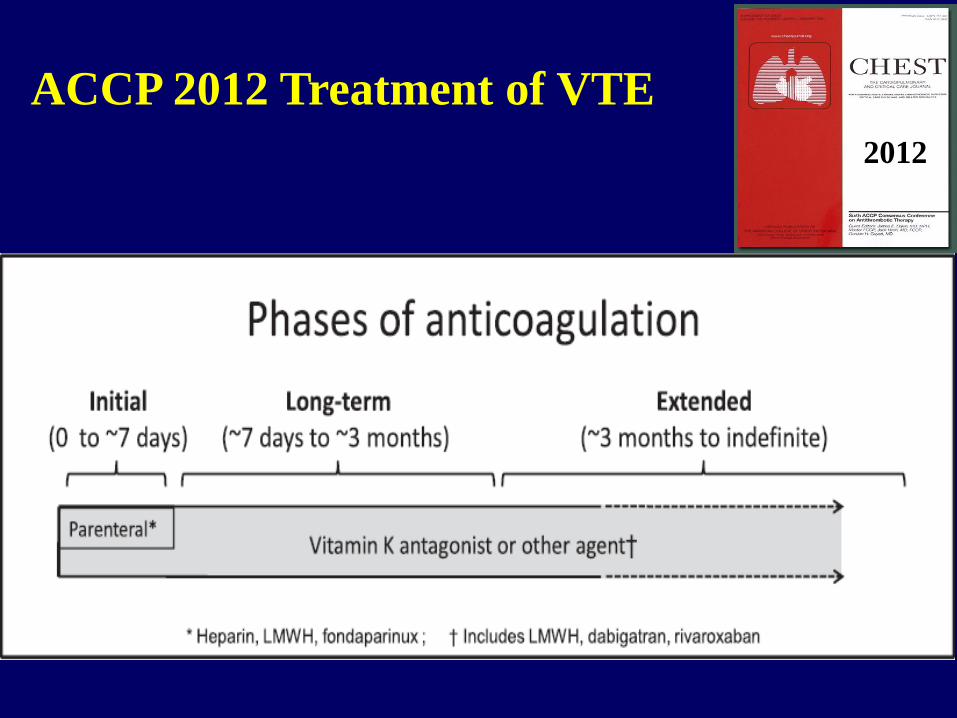
ACCP 2012 Treatment of VTE
2012
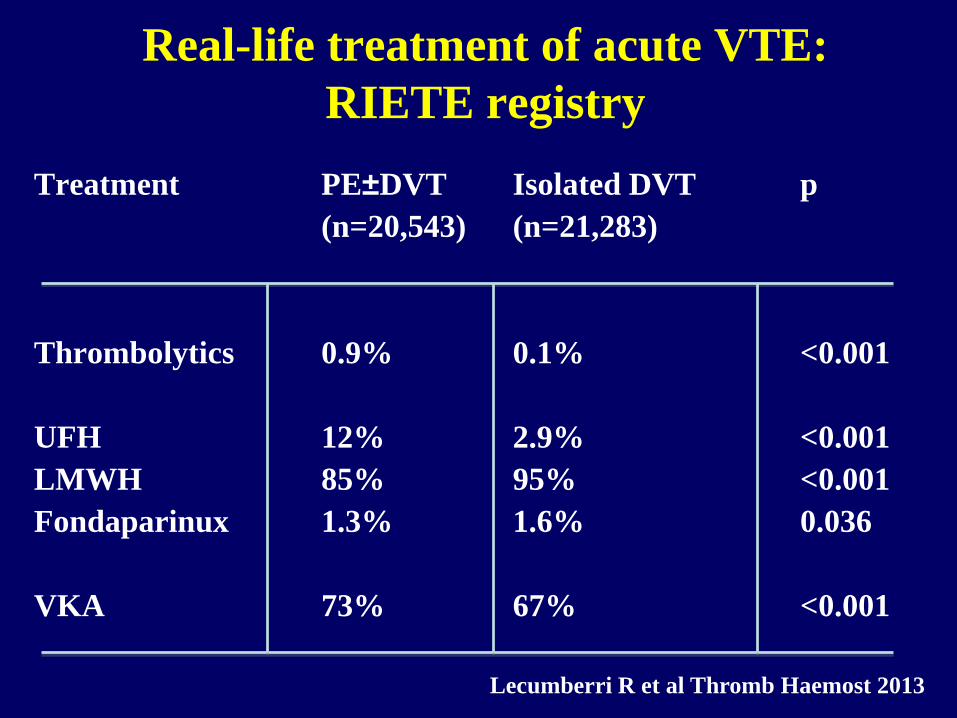
Real-life treatment of acute VTE:
RIETE registry
Treatment PE±DVT Isolated DVT p
(n=20,543) (n=21,283)
Thrombolytics 0.9% 0.1% <0.001
UFH 12% 2.9% <0.001
LMWH 85% 95% <0.001
Fondaparinux 1.3% 1.6% 0.036
VKA 73% 67% <0.001
Lecumberri R et al Thromb Haemost 2013
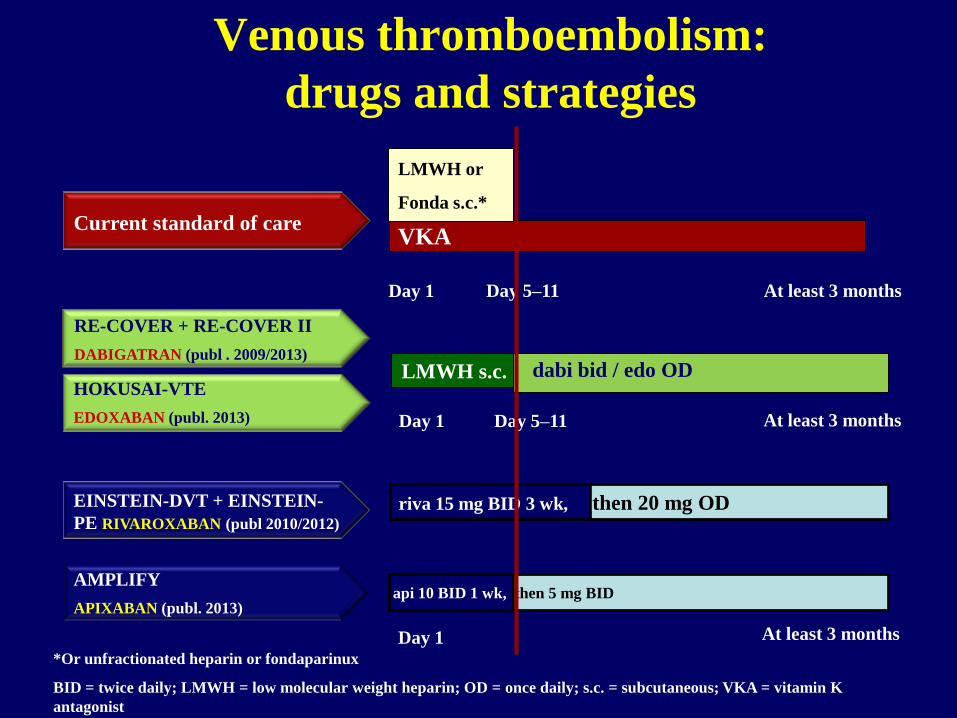
*Or unfractionated heparin or fondaparinux
BID = twice daily; LMWH = low molecular weight heparin; OD = once daily; s.c. = subcutaneous; VKA = vitamin K
antagonist
dabi bid / edo OD
RE-COVER + RE-COVER II
DABIGATRAN (publ . 2009/2013)
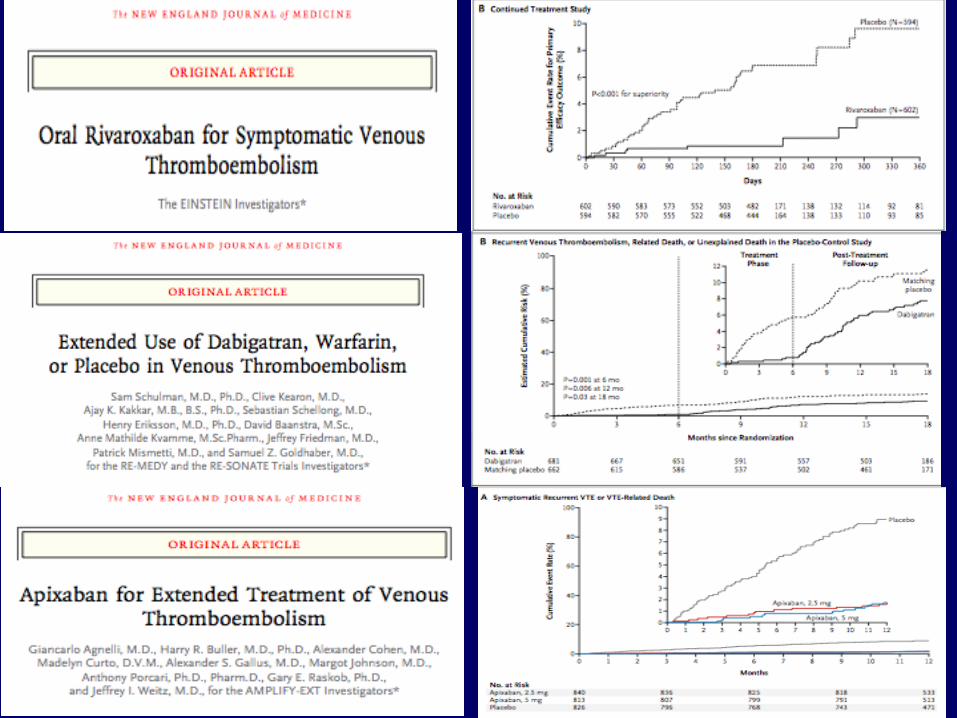
EINSTEIN-DVT + EINSTEIN-
PE RIVAROXABAN (publ 2010/2012)
VKA
AMPLIFY
APIXABAN (publ. 2013)
Day 1
Day 1
Day 1
At least 3 months
At least 3 months
Day 5–11
LMWH s.c.
At least 3 months
Current standard of care
LMWH or
Fonda s.c.*
HOKUSAI-VTE
EDOXABAN (publ. 2013)
Day 5–11
riva 15 mg BID 3 wk, then 20 mg OD
api 10 BID 1 wk, then 5 mg BID
Venous thromboembolism:
drugs and strategies
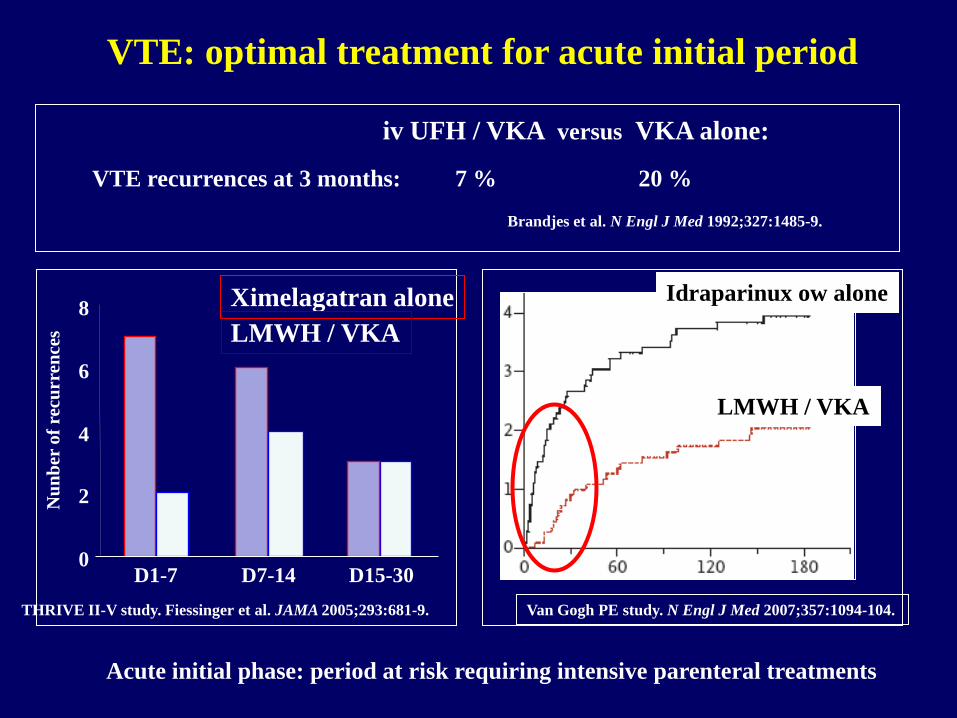
iv UFH / VKA versus VKA alone:
VTE: optimal treatment for acute initial period
Brandjes et al. N Engl J Med 1992;327:1485-9.
VTE recurrences at 3 months: 7 % 20 %
0
2
4
6
8
D1-7 D7-14 D15-30
Ximelagatran alone
LMWH / VKA
Nu
nb
er o
f re
curr
ence
s
THRIVE II-V study. Fiessinger et al. JAMA 2005;293:681-9.
HR = 2.09 [ 1.2 – 3.6 ]
Van Gogh PE study. N Engl J Med 2007;357:1094-104.
Idraparinux ow alone
LMWH / VKA
Acute initial phase: period at risk requiring intensive parenteral treatments
0
0,5
1
1,5
2
2,5
3
3,5
4
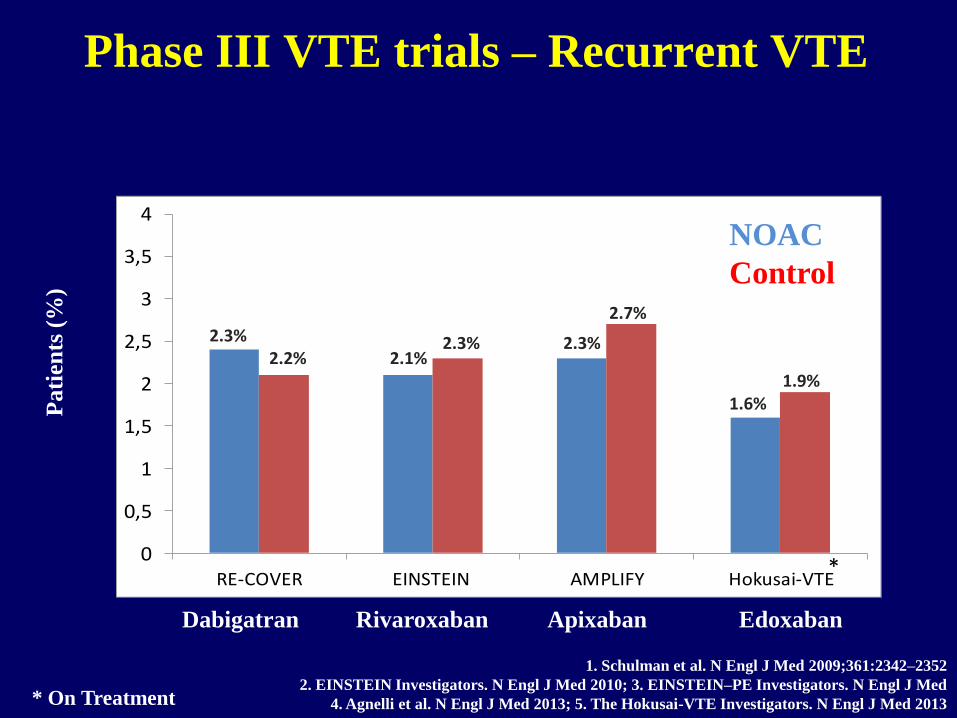
RE-COVER EINSTEIN AMPLIFY Hokusai-VTE
Pati
ents
(%
) Phase III VTE trials – Recurrent VTE
1.6% 1.9%
2.3% 2.2% 2.1%
2.3% 2.3%
2.7%
1. Schulman et al. N Engl J Med 2009;361:2342–2352
2. EINSTEIN Investigators. N Engl J Med 2010; 3. EINSTEIN–PE Investigators. N Engl J Med
4. Agnelli et al. N Engl J Med 2013; 5. The Hokusai-VTE Investigators. N Engl J Med 2013
*
* On Treatment
NOAC
Control
Dabigatran Rivaroxaban Apixaban Edoxaban
0
0,5
1
1,5
2
2,5
3
3,5
4
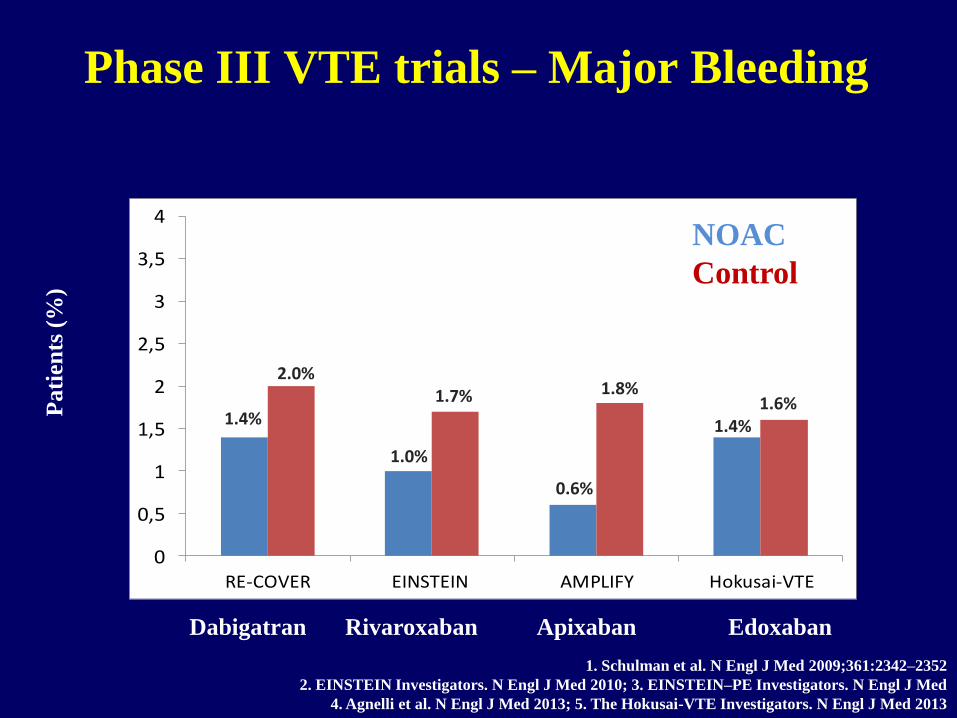
RE-COVER EINSTEIN AMPLIFY Hokusai-VTE
Pati
ents
(%
) Phase III VTE trials – Major Bleeding
1.4% 1.6%
1.4%
2.0%
1.0%
1.7%
0.6%
1.8%
1. Schulman et al. N Engl J Med 2009;361:2342–2352
2. EINSTEIN Investigators. N Engl J Med 2010; 3. EINSTEIN–PE Investigators. N Engl J Med
4. Agnelli et al. N Engl J Med 2013; 5. The Hokusai-VTE Investigators. N Engl J Med 2013
NOAC
Control
Dabigatran Rivaroxaban Apixaban Edoxaban
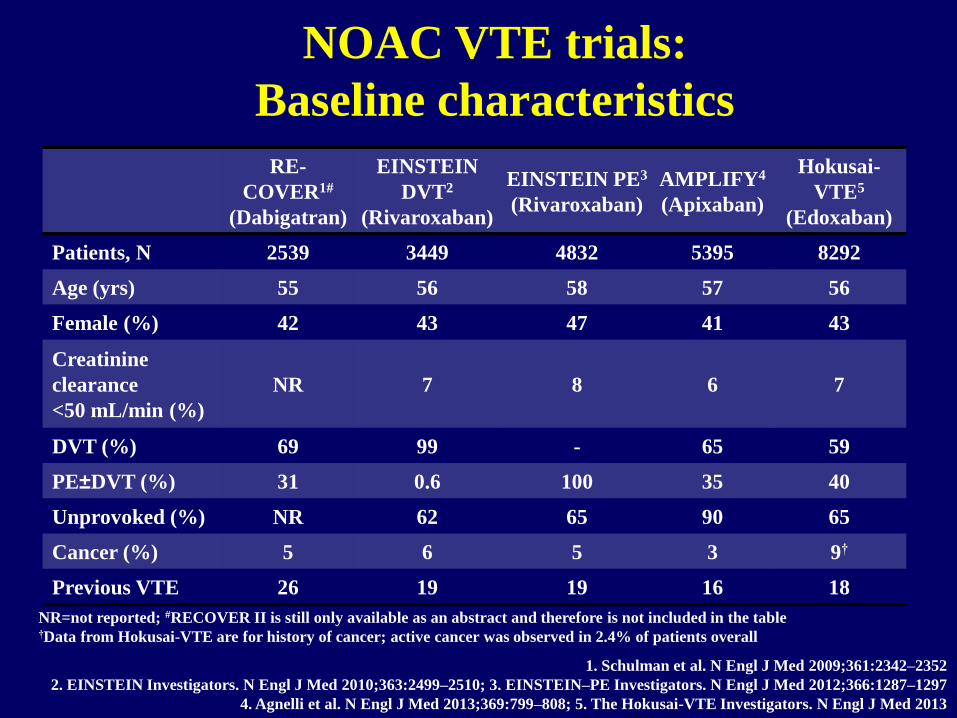
RE-
COVER1#
(Dabigatran)
EINSTEIN
DVT2
(Rivaroxaban)
EINSTEIN PE3
(Rivaroxaban)
AMPLIFY4
(Apixaban)
Hokusai-
VTE5
(Edoxaban)
Patients, N 2539 3449 4832 5395 8292
Age (yrs) 55 56 58 57 56
Female (%) 42 43 47 41 43
Creatinine
clearance
<50 mL/min (%)
NR 7 8 6 7
DVT (%) 69 99 - 65 59
PE±DVT (%) 31 0.6 100 35 40
Unprovoked (%) NR 62 65 90 65
Cancer (%) 5 6 5 3 9†
Previous VTE 26 19 19 16 18
NOAC VTE trials:
Baseline characteristics
NR=not reported; #RECOVER II is still only available as an abstract and therefore is not included in the table †Data from Hokusai-VTE are for history of cancer; active cancer was observed in 2.4% of patients overall
1. Schulman et al. N Engl J Med 2009;361:2342–2352
2. EINSTEIN Investigators. N Engl J Med 2010;363:2499–2510; 3. EINSTEIN–PE Investigators. N Engl J Med 2012;366:1287–1297
4. Agnelli et al. N Engl J Med 2013;369:799–808; 5. The Hokusai-VTE Investigators. N Engl J Med 2013
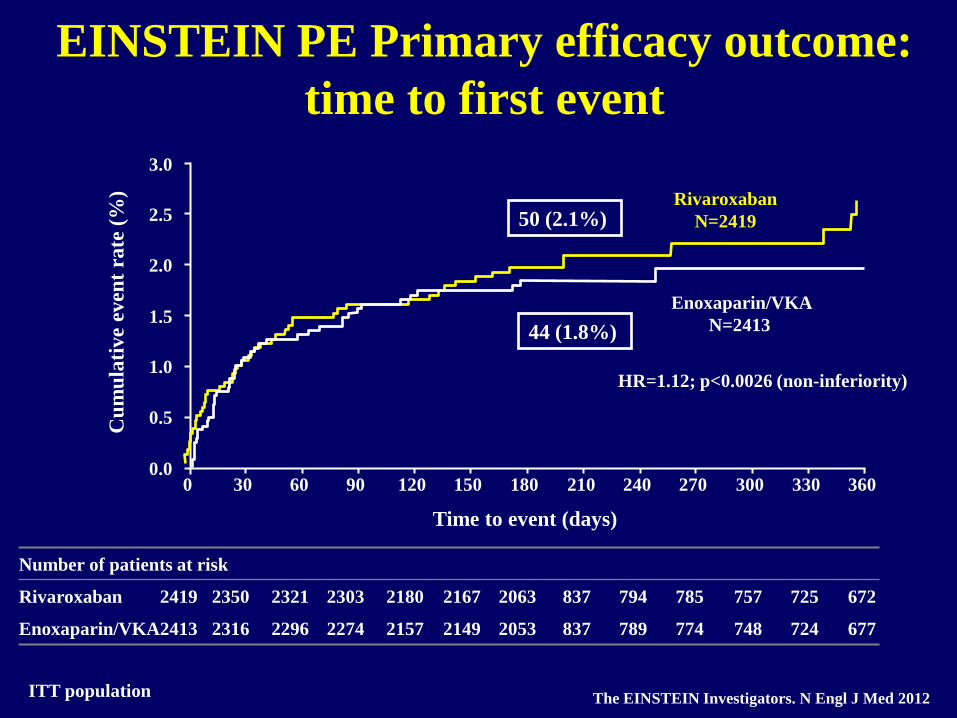
EINSTEIN PE Primary efficacy outcome:
time to first event
ITT population
3.0
2.5
2.0
1.5
1.0
0.0
0.5
0 30 60 90 120 150 180 210 240 270 300 330 360
Number of patients at risk
Rivaroxaban 2419 2350 2321 2303 2180 2167 2063 837 794 785 757 725 672
Enoxaparin/VKA 2413 2316 2296 2274 2157 2149 2053 837 789 774 748 724 677
Cu
mu
lati
ve
even
t ra
te (
%)
Time to event (days)
Rivaroxaban
N=2419
Enoxaparin/VKA
N=2413
HR=1.12; p<0.0026 (non-inferiority)
The EINSTEIN Investigators. N Engl J Med 2012
44 (1.8%)
50 (2.1%)
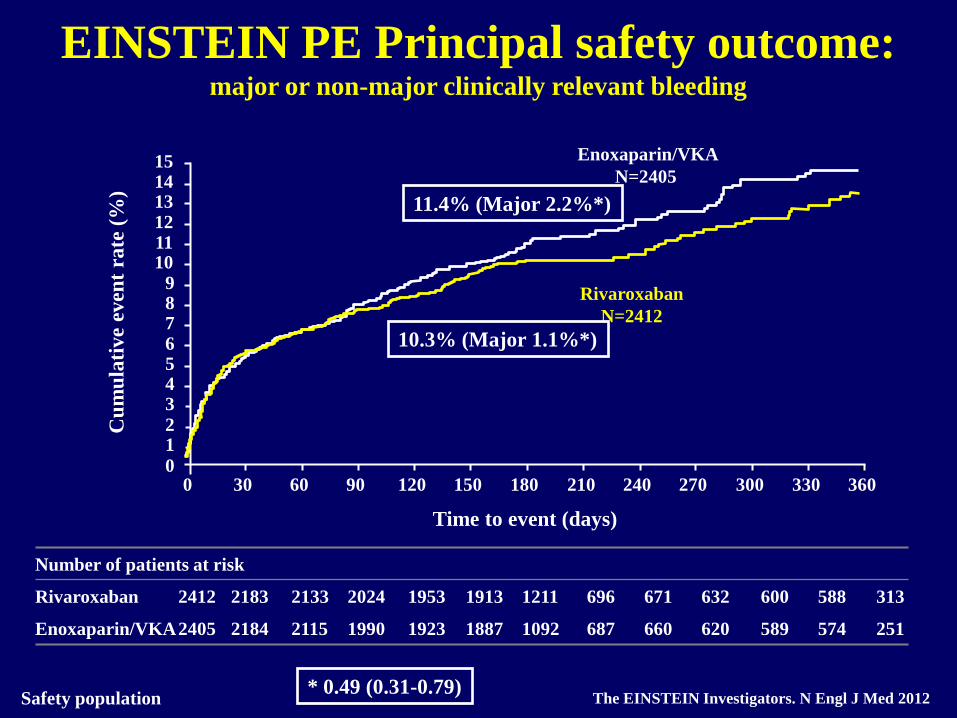
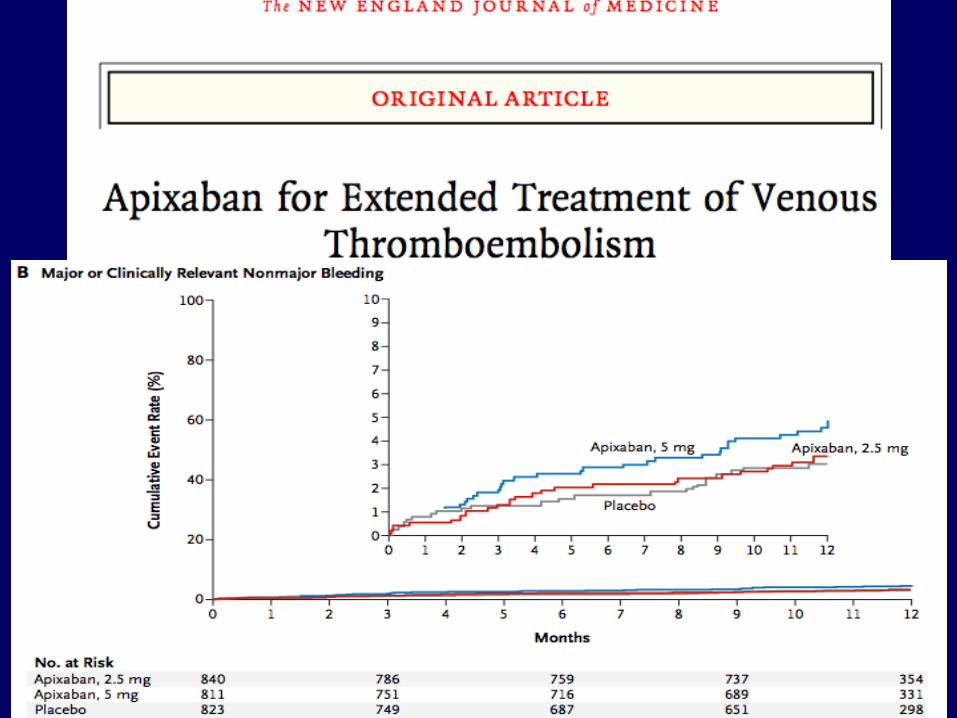
EINSTEIN PE Principal safety outcome: major or non-major clinically relevant bleeding
Safety population
0 30 60 90 120 150 180 210 240 270 300 330 360
15 14
10
13 12 11
9 8 7 6 5 4 3 2 1
0
Number of patients at risk
Rivaroxaban 2412 2183 2133 2024 1953 1913 1211 696 671 632 600 588 313
Enoxaparin/VKA 2405 2184 2115 1990 1923 1887 1092 687 660 620 589 574 251
Cu
mu
lati
ve
even
t ra
te (
%)
Time to event (days)
Rivaroxaban
N=2412
Enoxaparin/VKA
N=2405
The EINSTEIN Investigators. N Engl J Med 2012
11.4% (Major 2.2%*)
10.3% (Major 1.1%*)
* 0.49 (0.31-0.79)
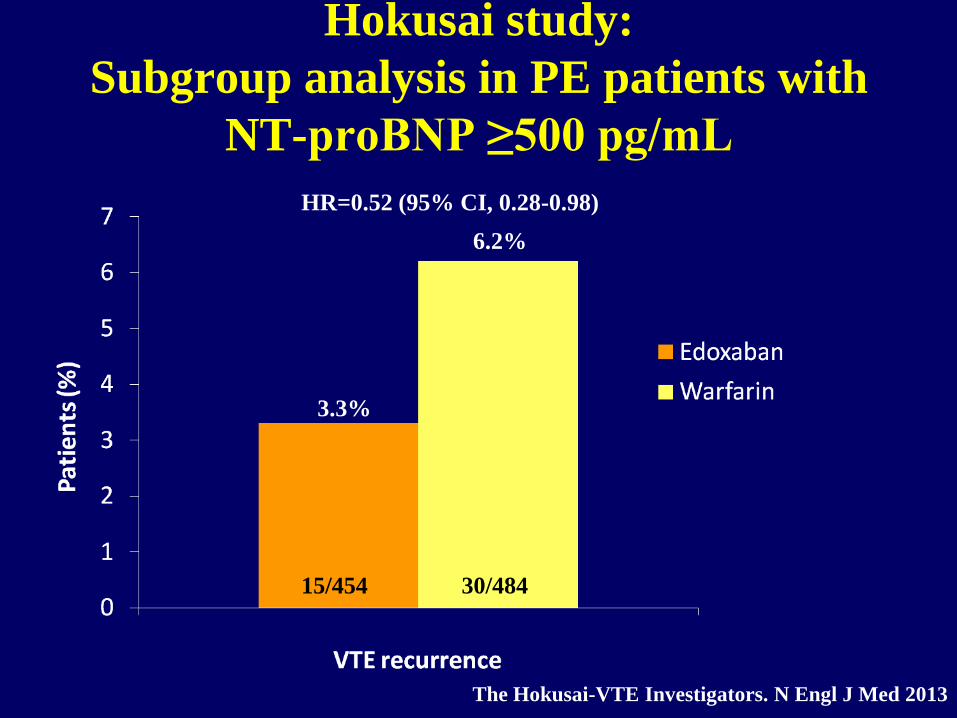
Hokusai study:
Subgroup analysis in PE patients with
NT-proBNP ≥500 pg/mL
15/454 30/484
HR=0.52 (95% CI, 0.28-0.98)
3.3%
6.2%
The Hokusai-VTE Investigators. N Engl J Med 2013
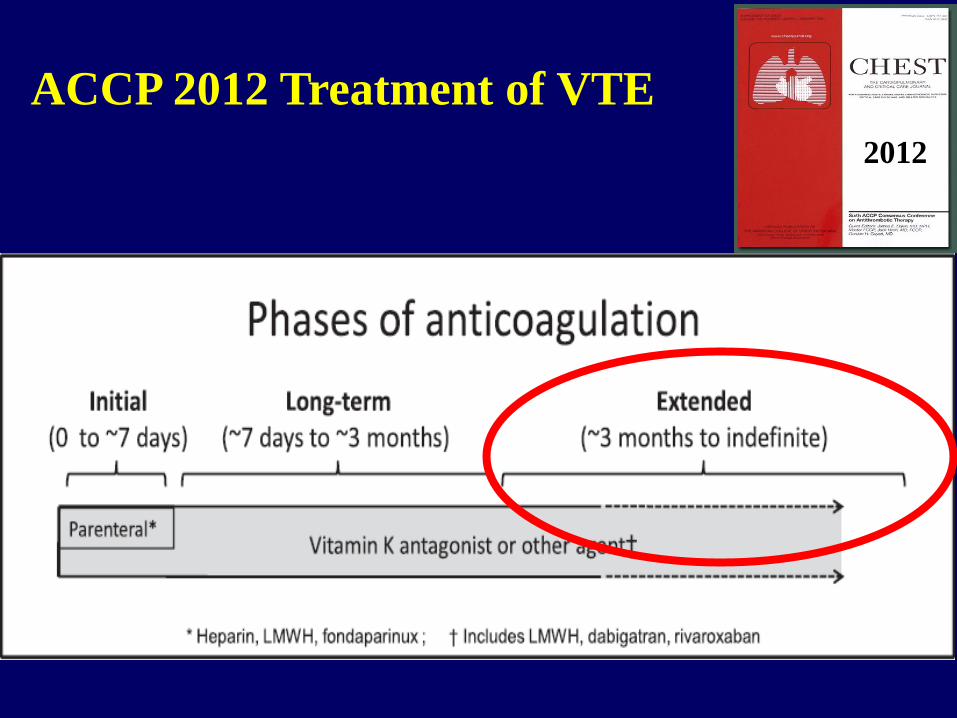
ACCP 2012 Treatment of VTE
2012
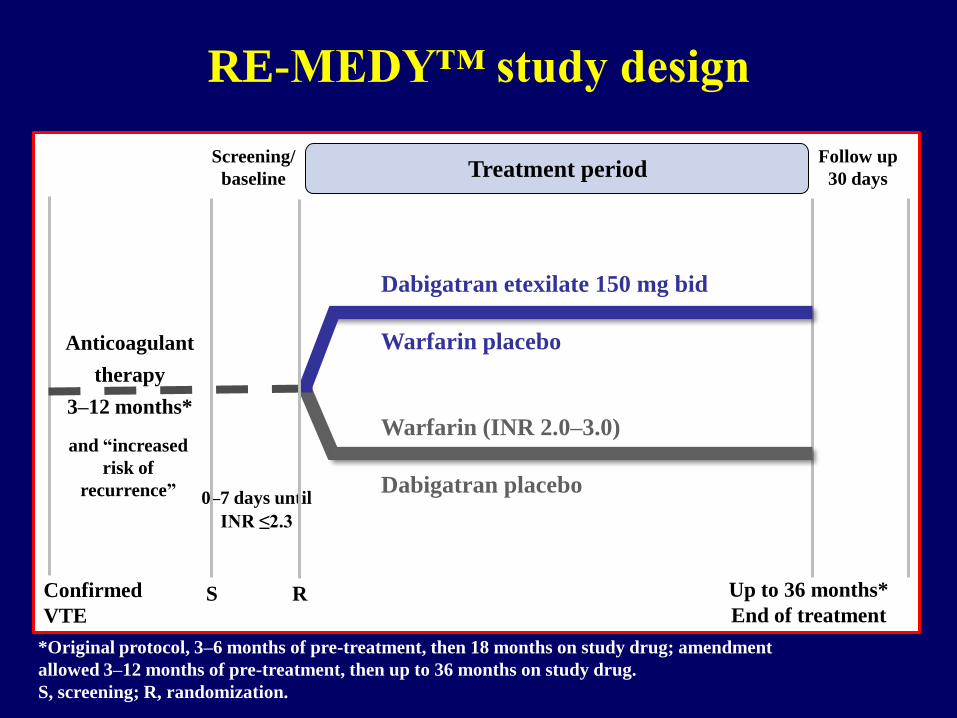
RE-MEDY™ study design
S, screening; R, randomization.
*Original protocol, 3–6 months of pre-treatment, then 18 months on study drug; amendment
allowed 3–12 months of pre-treatment, then up to 36 months on study drug.
Confirmed
VTE
Anticoagulant
therapy
3–12 months*
S R
0–7 days until
INR ≤2.3
Screening/
baseline
Dabigatran etexilate 150 mg bid
Warfarin placebo
Warfarin (INR 2.0–3.0)
Dabigatran placebo
Up to 36 months*
End of treatment
Follow up
30 days Treatment period
and “increased
risk of
recurrence”
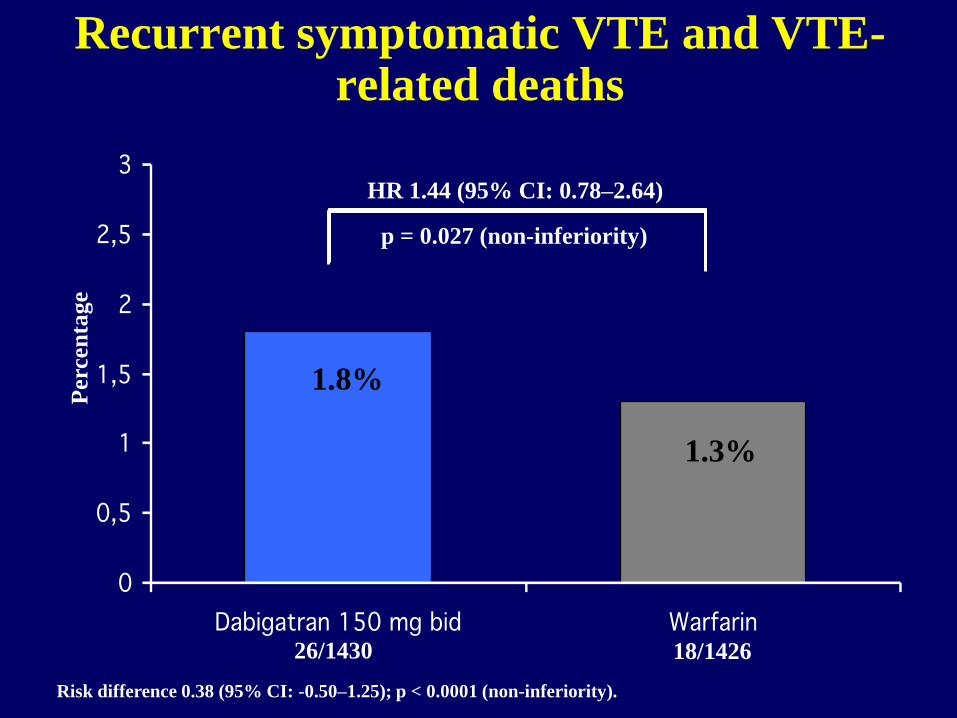
26/1430
Recurrent symptomatic VTE and VTE-related deaths
1.8%
1.3%
Risk difference 0.38 (95% CI: -0.50–1.25); p < 0.0001 (non-inferiority).
HR 1.44 (95% CI: 0.78–2.64)
18/1426
Perc
en
tage
p = 0.027 (non-inferiority)
0
0,5
1
1,5
2
2,5
3
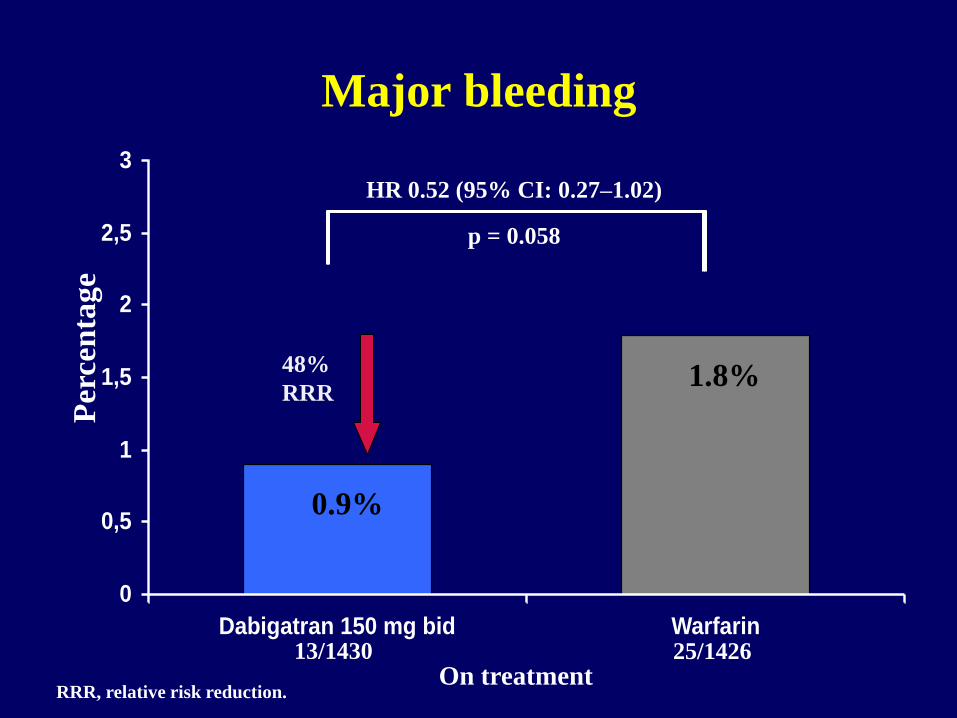
Dabigatran 150 mg bid Warfarin13/1430
Major bleeding
0.9%
1.8%
HR 0.52 (95% CI: 0.27–1.02)
25/1426
Per
cen
tage
p = 0.058
On treatment
48%
RRR
RRR, relative risk reduction.
Eleggibilità da piano terapeutico
per Xarelto
• Prevenzione della TVP recidivante e dell’EP
dopo TVP PROSSIMALE acuta nell’adulto
• Diagnosi confermata mediante ecografia
ARTI INFERIORI nelle 48 ore precedenti
• Oppure
• Terapia con EBPM o ENF o fondaparinux
• Insufficienza grave (clearance creatinina < 30
mL/min-15 mL/min per alcuni farmaci?)
• Insufficienza epatica moderata-grave (Child-Pugh
B-C); epatite acuta
• Terapia con farmaci non associabili (es.
antiretrovirali)
• Gravidanza e allattamento
• Neoplasia attiva con indicazione a EBPM a lungo
termine
• Concomitante EP con instabilità emodinamica
Pazienti non candidabili ai nuovi
anticoagulanti orali
I nuovi anticoagulanti nella terapia del
TEV: conclusioni
• Studi di fase III 27.100 pazienti con TVP ed EP dimostrano efficacia comparabile al trattamento standard e sicurezza complessivamente superiore
• Non vi sono segnali di differenze nei vari sottogruppi, soprattutto di pazienti più fragili
• I vantaggi pratici sono indiscutibili
• Siamo in attesa di dati da studi osservazionali/fase IV (Xalia)
I nuovi anticoagulanti nella terapia del
TEV: conclusioni 2
• E’ fondamentale la selezione dei pazienti idonei per ciascun trattamento
• E’ fondamentale un’adeguata istruzione dei pazienti
• E’ fondamentale un adeguato follow-up
• Aree incerte:
• Embolia polmonare con disfunzione ventricolare dx
• Neoplasia attiva (vs EBPM)
• Sedi inusuali





























