Embed Size (px)
Citation preview
Producer’s Guide toConnectiCare® SOLO
®
Plan Year 2009
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
Table of ContentsII NN TT RR OO DD UU CC TT II OO NNBuilding Your Business with ConnectiCare® SOLO 2Questions? 2Attractive Commissions! 2Doing Business @ www.connecticare.com 2
NN EE WW BB UU SS II NN EE SS SSEligibility Requirements 3Connecticut Residency 3Online Application 3Steps To Apply – New Business (Paper) 3How Can I Expedite The Application Process? 4EFT Instructions and Guidelines 5Tips for Completing Individual Application/Change Form (Paper) 6Application Checklist 7Health Plans Compatible with HSA 8Important Guidelines for New Business 8Rescissions 9Premium Payments 9Dependents 9
CC HH AA NN GG EE SS
Adding Dependents 10Adding Newborns or Adopted Children 10Renewal Process 10Requesting Off-Cycle Plan Changes 10Termination of Coverage 11
UU NN DD EE RR WW RR II TT II NN GG
Medical Underwriting 11Pre-Screening Guidance 12Condition Waivers 12Future Surgery or Procedures 12Declinable Medications 12Declinable Conditions 13Underwriting Risk Criteria 15Height and Weight Table 16FAQs 16
Building Your Business withConnectiCare® SOLOThis guide provides a general overview of our individual
product, ConnectiCare® SOLO, which offers the same personal
service and choice of providers as our group plans.
You’ll find general information on the application process,
eligibility, general underwriting guidelines and commissions.
This guide is not all-inclusive and is subject to change. Also,
for additional details, please see the ConnectiCare SOLO
Member Guidebook.
ConnectiCare SOLO is designed for:
� Self-employed persons
� Recent college graduates
� Part-time employees
� Early retirees
ConnectiCare SOLO is also a solution for other people who:
� are between jobs
� work for employers that don’t offer health insurance
� are not eligible for group coverage
� are dissatisfied with their present plans
Questions?If you have questions about ConnectiCare SOLO, or would like more information, please contact your ConnectiCare Sales Representative or Account Service Representative, or call 1-800-723-2986.
Attractive Commissions!You can build your business with an attractive schedule of
commissions for ConnectiCare SOLO. For details, please see
our Commission & Incentive brochure.
Doing Business @www.connecticare.comSee the online sales tools for ConnectiCare SOLO on the
Producer section of our Web site at www.connecticare.com.
It’s easier than ever to work with ConnectiCare!
� Apply Online
� Get fast quotes for prospective business
� Send full proposals by e-mail or fax
� View and print rate tables
� Check real-time status of applications and make renewal changes
� Manage your book of business in “My Accounts”
� Manage eligibility
� Change a Primary Care Physician
� View/print billing invoices
� Order ID cards
� Secure messaging service
� Update or change an address
� Download policyholder and member rosters
� Download and send forms
� Order materials and brochures
� And much more!
– 2 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY
II NN TT RR OO DD UU CC TT II OO NN �
Eligibility RequirementsIndividuals may apply for ConnectiCare SOLO if they are:
� Legal residents of Connecticut
� Under age 65
� Not enrolled in Medicare
� Single or married; or belong to a civil union/domestic partnership*
Families may apply for coverage for unmarried, dependent
children under age 26.
* Must submit Domestic Partner Verification Form or other satisfactory certification as we determine.
Connecticut ResidencyPlease make sure each family member applying for coverage
meets all of the following eligibility requirements BEFORE
submitting an Individual Application and Individual Health
Statement.
The applicant and dependents must be legal residents of
Connecticut. If residency is questionable, proof of residency
will be required. To demonstrate proof of residency, at least
three of the following items must show the applicant’s name
and current address:
1) Connecticut State Income Tax Return filed within the last 12 months
2) Current Connecticut voter registration card
3) Lease agreement or mortgage document
4) Most recent utility bill
5) Current Connecticut driver’s license
6) Connecticut DMV identification card
7) County or city property tax return filed within the last 12 months.
Online ApplicationNow you are able to offer online application to prospective
ConnectiCare SOLO members, making it even more
convenient to apply for our individual product. We’ve designed
the process to be producer-driven – an individual cannot initiate
online application without being invited to do so by you.
Online application has these advantages:
� It expedites the process because the Individual ApplicationPacket (Parts 1-3) goes directly to our underwriting department.
� It helps to prevent errors on the Individual ApplicationPacket.
� No postage is required.
� It helps us to be more “green” in our business practices. When more people use the Internet, we print fewer formsand conserve paper.
Once you have identified a candidate for online enrollment,
you’ll be able to generate an automatic, pre-formatted e-mail
invitation using a new tool located at “SOLO Quote/Invitation”
on the secure producer section of www.connecticare.com.
Customized with your contact information and whichever plan
option you select, the invitation provides your prospect with
details about the online enrollment process. Plus, you and your
prospect will be able to check online for an updated status of
the application once it’s submitted.
Steps To Apply – New Business(Paper)
APPLICANTS MUST:1) Complete, sign and date the Individual Application/Change Form – PART 1 – no more than 60days prior to the requested effective date. Be sure to:
a. Check the box for the medical plan being selected.
b. Check the boxes for the pharmacy co-pay and pharmacyannual maximum that are being selected (does not apply to HDHP plans).
c. Select a Primary Care Physician (PCP) for each familymember applying for coverage and write the PCP name in the appropriate box. For a complete list of participatingproviders, go to “Find a Doctor” at ww.connecticare.comor see our print directory.
– 3 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
NN EE WW BB UU SS II NN EE SS SS �
2) Accurately and completely answer all questions on the
Individual Health Statement – PART 2 – for each family
member applying for coverage.
If the applicant knowingly provides false informationand/or omits information on the application or healthstatement and such information submitted or omittedmaterially affects the risk assumed by ConnectiCare,ConnectiCare will seek to have the policy rescinded.
3) Complete, sign and date the Underwriting Authorization
Form – PART 3.
4) For applicants under the age of 18, the application must have
a parent/guardian’s signature and date – and the parent/
guardian’s full name must be printed on the application.
5) Applicants do not have to submit their first premium payment
with their application. However, once applicants are approved,
all premiums from the date of approval back to the effective
date are due by the first of the month following the date of their
approval letter. This could mean that applicants could owe us
more than one month of premium and owe the premium
quickly. Also if there is a retro effective date, these members
may get a past due notification. All premiums not received by
the first of the month for the month of coverage are considered
past due. This applies to all premium payment methods –
check, Electric Funds Transfer (EFT) and credit card.
6) If the EFT option is chosen for premium payment, the appli-
cant should complete and sign the Electronic Funds Transfer
Form – FORM 4. Be sure to include a check marked “void.”
Please see the additional information about Electronic Funds
Transfer (EFT) on the next page.
7) If applicable, complete the Domestic Partner Verification
Form or other satisfactory certfication as we determine.
8) OPTIONAL: Broker Authorization Form – must be
completed and received for ConnectiCare to release to the
broker any information that includes the applicant’s personal
health information.
9) All completed forms must be signed, dated and received at
ConnectiCare by the last day of the month for an effective date
on the 1st of the next month. (i.e. A complete application
received by January 31st would be eligible for a February 1st
effective date. A complete application received on February 1st
would be eligible for a March 1st effective date.)
What if the last day of the month falls on a weekendor a holiday?
Online applications – must be submitted to ConnectiCare by
midnight on the last day of the month, regardless of whether it’s
a weekend or a holiday.
Paper applications – must be received at ConnectiCare by the
last business day before the weekend or holiday.
Forms should be mailed to:
ConnectiCareP.O. Box 4058Farmington, CT 06034-4058
Or, forms may be faxed to 860-678-5274.
Approval for an individual health policy is based on the
applicant meeting the eligibility requirements and underwriting
criteria, and on our review of the Individual Health
Statement(s) and any additional medical and/or pharmacy
information that we request and receive.
To obtain copies of the application forms:
� Go to the producer section of www.connecticare.com,where you can download and print them; or
� Contact your ConnectiCare Sales Representative orAccount Service Representative; or
� Call 1-800-723-2986.
10) Incomplete applications may be returned to the producer.
If that happens, the application will need to be resubmitted
to ConnectiCare with all information filled in and all
questions answered. The effective date will be determined
based on the date that this completed application is received.
How Can I Expedite the Application Process?� Submit the Individual Application Packet (Parts 1-3) using
the online application process rather than the mail. Whenyou use the online application process, the forms go directly toour underwriting department.
� Double-check the forms before you submit them toConnectiCare to make sure that every questions is answeredcompletely and accurately, and that all information is filled in.
� Incomplete applications may be returned to you. If this happens, you will have to resubmit the application, and theeffective date will be determined based on the date that thecompleted application is received.
– 4 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY

EFT Instructions and GuidelinesWhen it comes to Electronic Funds Transfer (EFT)for premium payments, applicants have two optionsfrom which to choose:
1) They can sign-up for EFT along with their initial application.
All they have to do is complete the EFT form and attach a
voided check or statement savings deposit slip with their
application. Applicants should complete and sign the
Electronic Funds Transfer Form – FORM 4. Applicantsshould be sure to include a check marked “Void”. Once
an applicant is approved as a ConnectiCare SOLO member,
all premiums from the date of approval back to the effective
date are due by the first of the month following the date of
the approval letter. This could mean that the individual may
owe us more than one month of premium.
2) The process for new ConnectiCare SOLO applicants is as
follows:
a. ConnectiCare SOLO application is submitted along with
EFT form and application is approved.
b. Effective date of policy and EFT is established.
c. ConnectiCare sends “Pre-Note” file to the bank to
confirm that the bank routing number and checking
account numbers are correct.
d. Member is mailed letter confirming start date of EFT.
Example: If ConnectiCare were to receive an application and
an EFT form on October 28th, and the policy was approved in
November with an effective date of November 1st. The effective
date of the EFT would be November 1st.
Note: For new ConnectiCare SOLO applications, the EFT process is not started or initiated until the policy has been approved.
3) Applicants can wait to sign up for EFT until they are
accepted by and enrolled in ConnectiCare SOLO. All they
need to do is sign the front of the first invoice voucher and
return it with their premium payment. For future payment
drafts, we will use the checking account number that appears
on the check the applicant submits for the initial premium
payment. This way the applicant does not need to submit
a separate form when enrolling in EFT.
4) The process for current policyholders is as follows:
a. Member signs the front of the invoice stub and mails
invoice stub along with premium payment to
ConnectiCare.
b. ConnectiCare sends “Pre-Note” file to the bank to
confirm that the bank routing number and checking
account numbers are correct.
c. Effective date of EFT is established.
d. Member is mailed letter confirming start date of EFT.
Example: If on October 28th ConnectiCare were to receive the
signed invoice stub authorizing EFT, the November invoice
would still be mailed, and the member would have to pay by
check. The effective date of the EFT would not be earlier than
December 1st.
When determining the effective date of EFT, pleasebe aware that ConnectiCare SOLO members stillmay receive their monthly premium invoice in themail for a short period of time. Members will need to continue to pay by check until EFT goes intoeffect. This is because several steps are involved inimplementing EFT.
– 5 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
Monthly EFT Process:� Transactions take place on the 1st of every month unless the
1st falls on a weekend. In that case the money will be drawnon the first banking day of the month.
� Funds will be reflected in ConnectiCare’s system one day later.
� Funds will be reflected on the producer and member Websites two days after money is withdrawn from the account.
� When there is a failed transaction, the following will occur:
– The money is removed from ConnectiCare’s system.
– A letter is mailed to the account holder explaining the returned EFT transaction.
– A $25 fee will be assessed.
– The EFT transaction will be reattempted on the 15th of the current month.
If the transaction also fails on the 15th, the EFT account will
be automatically terminated. A letter will be sent to the account
holder explaining the reason for EFT termination, and that
future payments will need to be made by check. Outstanding
premiums will need to be paid by check before the 10th of the
next month.
Voluntary Termination of EFT:� A written request from the account holder is necessary
for the termination of an EFT account. The account holdershould include the account number along with his or her name on the written request, and fax it to 860-678-5255, ATTN: Billing Department.
Or, written requests may be mailed to:
ConnectiCare, Inc. & AffiliatesAttn: Billing/EFT175 Scott Swamp RoadFarmington, CT 06034-4050
� The request must be received before the 25th of the current month in order to be removed from the following month’s EFT file.
If you have any questions, you may call ConnectiCare’sBilling Department at 1-800-333-1733, Monday throughFriday, 8:00 a.m. – 5:00 p.m., Eastern Time.
Tips for Completing IndividualApplication/Change Form(Paper)
PLEASE MAKE SURE:1) All forms are completed in ink. Incomplete forms may be returned to the producer.
2) All questions have been answered completely by the
applicant. Producers may not complete questions on behalf
of the applicant.
3) All changes have been initialed and dated by the primary
applicant. Do not use correction fluid. If the applicantadds information that was missing, he/she must re-sign and
re-date the Individual Application/Change Form and the
Individual Health Statement to verify that the added
information is correct.
4) All applicable forms have been signed and dated by all
applicants who are required to do so. Do not date or signfor the applicant.
5) Proof of legal guardianship (an appointment by the Probate
Court) is included, if applicable.
6) If an EFT option is chosen for future payments, make
sure the EFT form is completed and a voided bank check
is included.
7) The medical plan and pharmacy plan have been selected on
the Individual Application/Change Form.
8) Any questions answered “yes” on the Individual Health
Statement must be explained in detail for each familymember noted. The detailed information should beincluded in the spaces provided under the “HealthHistory” section of the Individual Health Statement.The Application and Health Statement may be sent in a
sealed envelope.
– 6 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY
9) Any attachments to the Individual Application/Change
Form and Individual Health Statement, including medical
information, are signed and dated by the primary applicant
or parent/legal guardian.
10) Agent and agency name for commission payments are
included.
11) The Producer must be licensed in Connecticut and
appointed by ConnectiCare. If you are licensed but not
appointed, please call our Producer, Sales and Customer
Service Line at 1-800-723-2986.
Application Checklist Required before underwriting:
Signed Application with following completed:
� Application Transaction Request Check Box
� Applicant Name
� Applicant Address
� Selection of Plan Choice and Rx rider
� All Dependents’ Names
� All Dependents’ Add/Delete
� All Dependents’ SSNs
� All Dependents’ Sex
� All Dependents’ DOBs
� PCP – Name/Phone Number
� “Other Insurance Box” checked
� “Other Insurance Box” – if yes, insurance section completed
Signature with date of each:
Applicant/Spouse/Domestic Partner and Dependent 18 or older
� Broker Information
� Broker Authorization Form (not required)
Health Statement:
� All questions (#1 - #30) must be answered.
� Specific explanations for any “Yes” answers in the space provided under “Health History.”
� Supplemental Medical Questionnaires completed as appropriate. These should be submitted with the IndividualApplication/Change Form and Individual Health Statementto expedite application processing. To download and print a Supplemental Medical Questionnaire, go to the secure producer section of www.connecticare.com. Click“SOLO/Individual Plans”, then “Forms/Guides” and“Medical Questionnaires”.
Underwriting Authorization Form:
� Signature w/ date of each Applicant/Spouse/ DomesticPartner and Dependent age 18 or older
� All fields complete
Other required documentation (if applicable):
� Domestic Partner Verification Form or other satisfactory certification as we determine
� Disabled Dependent Form
� Election of Electronic Funds Transfer Form
Examples of Material Pend/Missing Information (which may cause unnecessary delay in application process):
� Any information that is missing from Parts 1, 2 or 3 of theApplication Packet, especially current height and weight onthe Individual Health Statement.
� Signature with date of all applicants age 18 or older
� Multiple applications with one check
� Underwriting authorization missing/not signed/not dated
� Questions on the Individual Health Statement that are leftblank or unexplained.
– 7 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
Health Plans Compatible with HSAConnectiCare SOLO has two plan options that are compatible
with Health Savings Accounts (HSAs): HMO Open Access –
High-Deductible Health Plan and Point-of-Service
Open Access – High Deductible Health Plan.
When combined with a High-Deductible Health Plan
(HDHP), a Health Savings Accounts (HSA) can help to lower
medical plan expenses, preserve quality and empower health
care consumers.
We have selected First HSA as our preferred vendor to manage,
administer and service your clients’ HSA accounts.
First HSA also offers producer compensation for each individual
application. This is a one-time payment when the account is
opened. You must be identified as the agent/agency on the
First HSA application to receive compensation from First HSA.
To start the HSA enrollment process for your client is simple:
1) Submit your client’s application for a ConnectiCare SOLO
High-Deductible Health Plan (HDHP) and wait for approval.
2) Determine your client’s method of making HSA
contributions and First HSA service-fee payment. For
detailed instructions, go to the producer section on
www.connecticare.com (click on “SOLO/Individual”
and see “HSA Administration”). Or contact First HSA at
1-888-769-8696.
3) Upon receipt of your client’s acceptance into a ConnectiCare
SOLO HDHP, submit a First HSA application to First HSA.
Note: Do not set up an account until your client’s enrollmentacceptance is confirmed.
4) First HSA will process the HSA application and mail a
“Welcome Packet” to your client.
Important Guidelines for New Business� Effective dates for coverage are the 1st of the month
following underwriting approval.
� Deadline for complete applications is the last day of themonth prior to effective date of coverage.
� If coverage is denied or terminated by ConnectiCare for non-payment, the individual cannot reapply for coverage for 12 months following the requested effective date of thedenial or 12 months from the date of termination.
� ConnectiCare may accept eligible family members for coverage while denying other family members who do notmeet our eligibility or underwriting requirements. (Alsoknown as a “partial denial.”)
� Applicants will be notified in writing of the underwritingdecision. (Producers will receive a copy of the notification.Note: if the underwriting decision is a denial or partialdenial, the reason will not be included in the producer’s copyto protect the privacy of the applicant’s medical information.)
� The applicant is responsible for providing us with completeand accurate information on all forms, and must notify us immediately of any and all changes in health information, name, address and telephone number, and changes in PCP, while the application is pending.
� Underwriting may request directly from the applicant additional health information, if necessary. A medicalrecords request and/or supplemental medical questionnairewill be mailed or e-mailed to the applicant’s home address/e-mail address, with instructions for completion.
� If ConnectiCare requests a supplemental medical questionnaire and/or medical records, it is the applicant’sresponsibility to request/obtain that medical informationfrom their physician and to pay for any costs the physician’soffice may charge to copy and send us those records.
� If additional information is requested and not received by us within 15 days, we will send a follow-up reminder to theapplicant. If the information is not received within 45 daysof the original request, the application will be consideredincomplete and will be withdrawn.
� The applicant will be required to reapply and complete anew application packet.
– 8 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY

RescissionsIn making a determination whether to issue a policy to an
applicant, ConnectiCare will review and rely on the statements
made on the application and health statement. Any material
omission, misrepresentation or misstatements about medical or
pharmacy history, planned treatment or surgeries, weight/height
or other information on the application or health statement
will result in rescission and denial of an otherwise valid claim.
In addition, such omissions, misrepresentations or misstatements
may result in rescission of the policy back to the policy effective
date, and the client would be responsible for reimbursing
ConnectiCare for any paid claims. The premium paid and
collected at the point of rescission would be credited toward the
claims paid by ConnectiCare. This could result in either a refund
owed to the client, or claim payments owed by the client.
Premium PaymentsThe monthly premium payment is due on the 1st of every
month. If premium is not received around the 15th of
the month, a past due notification will be mailed to the
accountholder. Monthly premium payments can be made
by choosing one of the following options:
� Electronic funds transfer (EFT) – members can automatically enroll in EFT with the invoice stub when making a monthly premium payment.
� Online credit card payment.
� Personal check/money order.
In-force premium payments should be mailed to:
ConnectiCare, Inc. & AffiliatesP.O. Box 30726Hartford, CT 06150
For answers to your ConnectiCare SOLO billing questions,
please call 1-800-333-1733.
Note: ConnectiCare SOLO is an individual plan and is notoffered to groups. ConnectiCare SOLO is medically underwrittenand policyholders are required to pay the monthly premiums within the grace period or their policies may be terminated.
DependentsDependents are defined as the spouse/partner and children of
the applicant. Children are defined as a natural child, adopted
child, stepchild, or other child for whom the applicant or
applicant’s spouse has been appointed legal guardian by a
Probate Court. “Child” also includes the insured’s mentally or
physically handicapped, unmarried child – if the disability
began before age 26 and while the child still was eligible for
dependent coverage – and as a result of the disability, the child
is unable to support himself/herself. In the case of a natural
child or stepchild, the child is not required to live with the
applicant. However, in the case of “other child” (i.e., foster
child, grandchild), the child is required to live with the
applicant in a “natural parent/child setting”. Please submit
legal guardianship documentation with the Individual
Application/Change Form anytime the dependent falls into
the “other child” category.
ELIGIBLE CHILDREN MUST ALSO BE:� Unmarried
� Under age 26
� Not able to support himself/herself due to mental or physical handicap that began before age 26 and while thechild was still eligible for dependent converage. Verificationof Dependent Disability Form must be submitted andapproved.
– 9 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
Adding DependentsAn Individual Application/Change Form and Individual
Health Statement must be completed to add dependents to a
ConnectiCare SOLO policy. The application is subject to
medical underwriting, except in the case of newborn or adopted
children if added within the first 31 days of eligibility, or if
there is no change in premium based on the added newborn or
adopted dependent. The effective date for additional dependents
is determined in the same manner as effective dates for
applicants – except for an additional newborn or adopted child.
Adding Newborns or Adopted ChildrenThe insured’s newborn natural child receives coverage for the
first 31 days after birth. The adopted child receives coverage for
the first 31 days from the date of placement with the insured.
Coverage for the newborn or adopted child will end at the
earlier of the termination of the insured’s coverage or the end
of this 31-day period, unless the insured has notified us of the
newborn or adopted child and has paid us any additional
premium, if applicable.
The policyholder must complete an Individual Application and
pay any additional premium within 31 days of birth or legal
placement of the child. Otherwise, the newborn’s or adopted
child’s coverage ends on the 32nd day. If the newborn natural
child or adopted child is not added to the plan within the
31-day period, the dependent will be subject to the complete
medical underwriting process and must meet all enrollment and
underwriting requirements. If approved, coverage will become
effective on the first of the month following approval.
Renewal ProcessAll ConnectiCare SOLO policies renew with a common renewal
date. Written notification is sent directly to the policyholder’s
home address in advance of the renewal date. (Please be sure to
report address changes to us in a timely manner so your clients
will receive this notification.)
You will have online access to your clients’ renewal information.
You’ll also receive a packet in the mail containing a list of all
your clients’ renewal information. Please review your renewals
carefully. If no changes are requested, the policy will
automatically renew.
Note: Additional rate increases may be incurred due to changes in a policyholder’s age-band status.
Requesting Off-Cycle Plan ChangesTo receive prompt, accurate review of your request for an off-
cycle plan change for ConnectiCare SOLO, you should:
� Have your client complete the Individual Application/Change Form (Part 1) and the Underwriting Authorization Form (Part 3);
� Fax both forms to our Intake Department at 860-678-5274.
Our Underwriting Department will review the request and
respond with a decision within two business days. Notification
will be mailed to the policyholder, with a copy mailed to you,
stating that the request has been approved, denied or is pending.
(A request will be “pending” if we have asked the policyholder
for medical records, or if we have sent the policyholder a ques-
tionnaire.) The notification will include a copy of the Individual
Application/Change Form requesting the plan change.
Off-cycle plan change requests that are approved become effec-
tive the first of the month following Underwriting approval.
If the off-cycle plan change request is denied, the notification to
your client will state the reason for denial. In such cases, your
client’s current plan will remain in force.
Important: Retroactive effective dates are not allowed, nor are deductible credits. A new deductible period beginswith the effective date of change. Off-cycle plan changes are limited to one per calendar year.
– 10 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY
CC HH AA NN GG EE SS �

Medical UnderwritingOur underwriting department reviews the available medical
history and current health information of applicants and their
dependents to determine underwriting risk in accordance with
ConnectiCare’s guidelines. ConnectiCare will make the final
decision on the acceptance of any insurable risk. All information
discovered during the underwriting process will be used,
including, but not limited to, the health questions on the
Individual Application/Change Form and Individual Health
Statement, claim history, medical and pharmacy records, and
any additional information that may be requested.
1) ConnectiCare reserves the right to accept or deny requested
coverage, based on the information on the Individual Health
Statement provided by the applicant and/or their dependent(s),
and any other information obtained by us or provided to us.
2) An Individual Health Statement must be completed by the
applicant, including all dependents requesting coverage.
3) Underwriting may request additional information related to
specific conditions directly from the applicant and/or any
dependents. A medical records request and/or a supplemental
medical questionnaire will be mailed or e-mailed to the
applicant’s and/or dependent’s home address/e-mail address,
with instructions for completion.
4) In an attempt for underwriting to make a fair and accurate
determination on the current health status of a prospective
member who has not been to a provider for any reason,
including a physical exam, he/she will be required to have
a medical professional complete a series of questions for
underwriting review. These questions include the following:
a. Height/weight in office
b. Blood pressure in office
c. Documentation of any abnormal lab values in the last 5 years
d. A list of any symptoms the member has been experiencing
– 11 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
Termination of CoverageCANCELING DEPENDENTSTo cancel dependent coverage, an Individual Application/
Change Form (or other written request) must be completed.
Non-payment of premium is NOT considered a cancellation request.
If the policyholder wishes to cancel a dependent from the
policy, he or she will need to provide written notification within
30 days of the termination date. If a spouse/partner is to be
removed from a policy due to divorce or legal separation,
legal documentation must be attached to the Individual
Application/Change Form, and the Individual Application/
Change Form must be signed by the policyholder.
ConnectiCare will not process requests to make termination
effective retroactively.
CANCELING A POLICYIf a member wishes to terminate his or her policy, he or she
will need to provide written notification 30 days before the
identified termination date. The member must submit this
signed notification and include the date requested for termina-
tion of the policy.
Non-payment of premium is NOT considered a cancella-tion request. Cancellation requests should be sent to:
Mailing Address: ConnectiCare, Inc. & Affiliates175 Scott Swamp RoadP.O. Box 4058Farmington, CT 06034-4058
E-mail Address: [email protected] Number: 860-678-5255
ConnectiCare will not process requests to make a termination effective retroactively.
5) Dependents requesting coverage after the policyholder’s
effective date of coverage are required to complete an
Individual Application/Change Form, Individual Health
Statement and Underwriting Authorization Form, except
adopted children or newborn children added within 31 days.
6) Anytime we received a request to remove an existing
ConnectiCare SOLO member from his or her current policy
and issue the individual a new ConnectiCare SOLO policy,
medical underwriting will be required. Rationale: Since the
member is applying for coverage under a new policy, the
application is subject to the same underwriting requirements
as any other new application.
In the event of a policyholder’s death or divorce, or if the
policyholder becomes eligible for Medicare, then the
dependent can be moved to policyholder status without
medical underwriting.
Note: An Individual Application/Change Form is required to move the dependent to policyholder status.
7) If additional information is requested and not received by us within 15 days, we will send a follow-up reminder to theapplicant. If the information is not received within 45 days of the original request, the application will be considered incomplete and will be withdrawn. Also, the original effectivedate will become void. The application will need to be resubmitted to ConnectiCare with all information filled in and all questions answered – along with the additional information that was requested previously. A new effective datewill then be determined based on the date that this completedapplication is received.
Pre-Screening GuidanceConnectiCare SOLO’s pre-screening guidance allows producers
to obtain a preliminary response from our underwriting
department to questions regarding medical eligibility for
ConnectiCare SOLO prospects.
Note: Information that ConnectiCare provides during this pre-screening process is not a guarantee of coverage or eligibility,and is not intended to be the source for underwriting decisions.ConnectiCare reserves the right to request additional information or to decline coverage. ConnectiCare’s final decisionwill be based on enrollment requirements, a review of the completed application and medical underwriting.
� All requests for pre-screening guidance must be submittedusing the “Request for Pre-Screening Guidance” form, which may be downloaded from the secure producer site at www.connecticare.com. The form should be sent to theunderwriting department by fax 860-678-5204 or e-mail: [email protected].
� The form will ask for all medical history, including: condition/diagnosis; onset date; details (symptoms, treatment, tests, results); medications (name, dose, frequency); date last treated; and current status.
Underwriting will respond by fax or e-mail within 48 hours of
receiving the request for pre-screening guidance. This response is
not the final decision regarding acceptance for coverage.
A final decision will be based upon a completed application
which includes the health statement and any additional
information provided to underwriting.
Remember: To obtain a final decision on coverage, you must
follow the “Steps To Apply” on page 3.
Condition WaiversCondition waivers are not offered.
Future Surgery or ProceduresApplicants who are advised to have – or have scheduled – future
surgery, tests, or procedures are subject to further review.
Pertinent details should be provided on the Individual Health
Statement.
– 12 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY
UU NN DD EE RR WW RR II TT II NN GG �
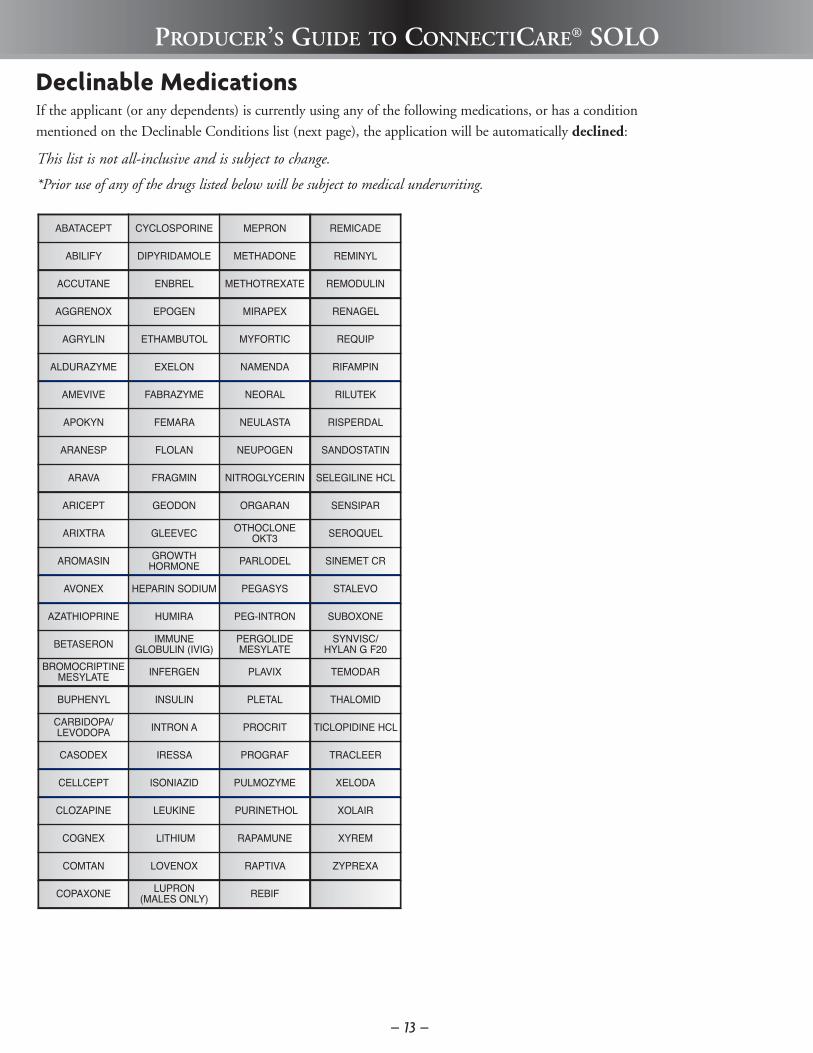
Declinable MedicationsIf the applicant (or any dependents) is currently using any of the following medications, or has a condition
mentioned on the Declinable Conditions list (next page), the application will be automatically declined:
This list is not all-inclusive and is subject to change.
*Prior use of any of the drugs listed below will be subject to medical underwriting.
– 13 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
ABATACEPT CYCLOSPORINE MEPRON REMICADE
ABILIFY DIPYRIDAMOLE METHADONE REMINYL
ACCUTANE ENBREL METHOTREXATE REMODULIN
AGGRENOX EPOGEN MIRAPEX RENAGEL
AGRYLIN ETHAMBUTOL MYFORTIC REQUIP
ALDURAZYME EXELON NAMENDA RIFAMPIN
AMEVIVE FABRAZYME NEORAL RILUTEK
APOKYN FEMARA NEULASTA RISPERDAL
ARANESP FLOLAN NEUPOGEN SANDOSTATIN
ARAVA FRAGMIN NITROGLYCERIN SELEGILINE HCL
ARICEPT GEODON ORGARAN SENSIPAR
ARIXTRA GLEEVEC OTHOCLONEOKT3 SEROQUEL
AROMASIN GROWTH HORMONE PARLODEL SINEMET CR
AVONEX HEPARIN SODIUM PEGASYS STALEVO
AZATHIOPRINE HUMIRA PEG-INTRON SUBOXONE
BETASERON IMMUNE GLOBULIN (IVIG)
PERGOLIDEMESYLATE
SYNVISC/HYLAN G F20
BROMOCRIPTINEMESYLATE INFERGEN PLAVIX TEMODAR
BUPHENYL INSULIN PLETAL THALOMID
CARBIDOPA/LEVODOPA INTRON A PROCRIT TICLOPIDINE HCL
CASODEX IRESSA PROGRAF TRACLEER
CELLCEPT ISONIAZID PULMOZYME XELODA
CLOZAPINE LEUKINE PURINETHOL XOLAIR
COGNEX LITHIUM RAPAMUNE XYREM
COMTAN LOVENOX RAPTIVA ZYPREXA
COPAXONE LUPRON(MALES ONLY) REBIF
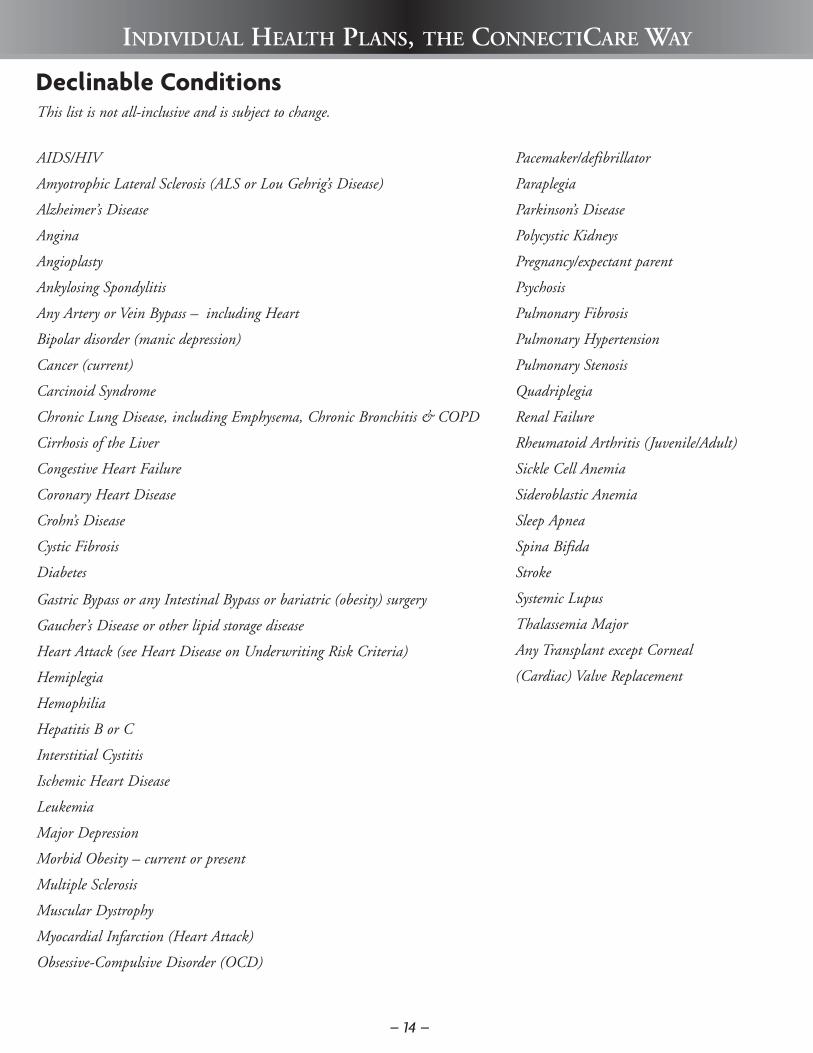
Declinable ConditionsThis list is not all-inclusive and is subject to change.
– 14 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY
AIDS/HIV
Amyotrophic Lateral Sclerosis (ALS or Lou Gehrig’s Disease)
Alzheimer’s Disease
Angina
Angioplasty
Ankylosing Spondylitis
Any Artery or Vein Bypass – including Heart
Bipolar disorder (manic depression)
Cancer (current)
Carcinoid Syndrome
Chronic Lung Disease, including Emphysema, Chronic Bronchitis & COPD
Cirrhosis of the Liver
Congestive Heart Failure
Coronary Heart Disease
Crohn’s Disease
Cystic Fibrosis
Diabetes
Gastric Bypass or any Intestinal Bypass or bariatric (obesity) surgery
Gaucher’s Disease or other lipid storage disease
Heart Attack (see Heart Disease on Underwriting Risk Criteria)
Hemiplegia
Hemophilia
Hepatitis B or C
Interstitial Cystitis
Ischemic Heart Disease
Leukemia
Major Depression
Morbid Obesity – current or present
Multiple Sclerosis
Muscular Dystrophy
Myocardial Infarction (Heart Attack)
Obsessive-Compulsive Disorder (OCD)
Pacemaker/defibrillator
Paraplegia
Parkinson’s Disease
Polycystic Kidneys
Pregnancy/expectant parent
Psychosis
Pulmonary Fibrosis
Pulmonary Hypertension
Pulmonary Stenosis
Quadriplegia
Renal Failure
Rheumatoid Arthritis (Juvenile/Adult)
Sickle Cell Anemia
Sideroblastic Anemia
Sleep Apnea
Spina Bifida
Stroke
Systemic Lupus
Thalassemia Major
Any Transplant except Corneal
(Cardiac) Valve Replacement
– 15 –
PRODUCER’S GUIDE TO CONNECTICARE® SOLO
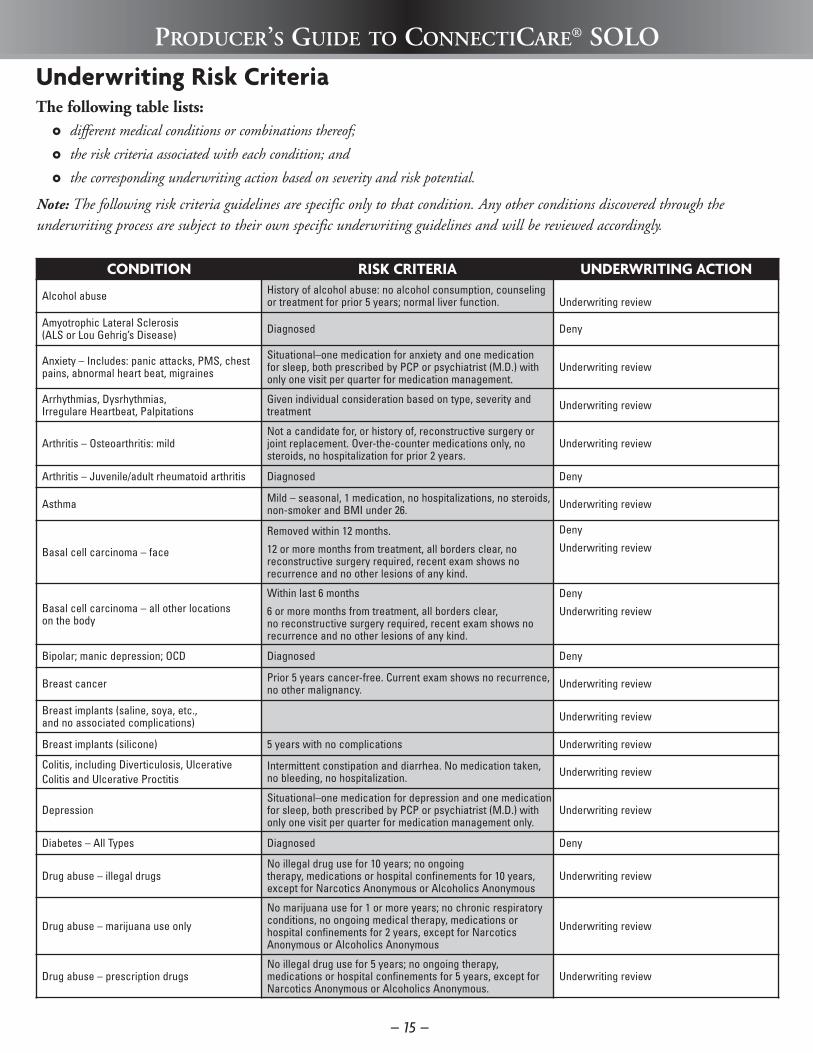
CONDITION RISK CRITERIA UNDERWRITING ACTION
Alcohol abuse History of alcohol abuse: no alcohol consumption, counselingor treatment for prior 5 years; normal liver function. Underwriting review
Amyotrophic Lateral Sclerosis(ALS or Lou Gehrig’s Disease) Diagnosed Deny
Anxiety – Includes: panic attacks, PMS, chestpains, abnormal heart beat, migraines
Situational–one medication for anxiety and one medication for sleep, both prescribed by PCP or psychiatrist (M.D.) withonly one visit per quarter for medication management.
Underwriting review
Arrhythmias, Dysrhythmias,Irregulare Heartbeat, Palpitations
Given individual consideration based on type, severity andtreatment Underwriting review
Arthritis – Osteoarthritis: mildNot a candidate for, or history of, reconstructive surgery orjoint replacement. Over-the-counter medications only, nosteroids, no hospitalization for prior 2 years.
Underwriting review
Arthritis – Juvenile/adult rheumatoid arthritis Diagnosed Deny
Asthma Mild – seasonal, 1 medication, no hospitalizations, no steroids,non-smoker and BMI under 26. Underwriting review
Basal cell carcinoma – face
Removed within 12 months.
12 or more months from treatment, all borders clear, no reconstructive surgery required, recent exam shows no recurrence and no other lesions of any kind.
Deny
Underwriting review
Basal cell carcinoma – all other locations on the body
Within last 6 months
6 or more months from treatment, all borders clear, no reconstructive surgery required, recent exam shows norecurrence and no other lesions of any kind.
Deny
Underwriting review
Bipolar; manic depression; OCD Diagnosed Deny
Breast cancer Prior 5 years cancer-free. Current exam shows no recurrence,no other malignancy. Underwriting review
Breast implants (saline, soya, etc., and no associated complications) Underwriting review
Breast implants (silicone) 5 years with no complications Underwriting review
Colitis, including Diverticulosis, UlcerativeColitis and Ulcerative Proctitis
Intermittent constipation and diarrhea. No medication taken,no bleeding, no hospitalization. Underwriting review
DepressionSituational–one medication for depression and one medicationfor sleep, both prescribed by PCP or psychiatrist (M.D.) withonly one visit per quarter for medication management only.
Underwriting review
Diabetes – All Types Diagnosed Deny
Drug abuse – illegal drugsNo illegal drug use for 10 years; no ongoing therapy, medications or hospital confinements for 10 years,except for Narcotics Anonymous or Alcoholics Anonymous
Underwriting review
Drug abuse – marijuana use only
No marijuana use for 1 or more years; no chronic respiratoryconditions, no ongoing medical therapy, medications or hospital confinements for 2 years, except for NarcoticsAnonymous or Alcoholics Anonymous
Underwriting review
Drug abuse – prescription drugsNo illegal drug use for 5 years; no ongoing therapy, medications or hospital confinements for 5 years, except forNarcotics Anonymous or Alcoholics Anonymous.
Underwriting review
Underwriting Risk CriteriaThe following table lists: � different medical conditions or combinations thereof;
� the risk criteria associated with each condition; and
� the corresponding underwriting action based on severity and risk potential.
Note: The following risk criteria guidelines are specific only to that condition. Any other conditions discovered through the underwriting process are subject to their own specific underwriting guidelines and will be reviewed accordingly.
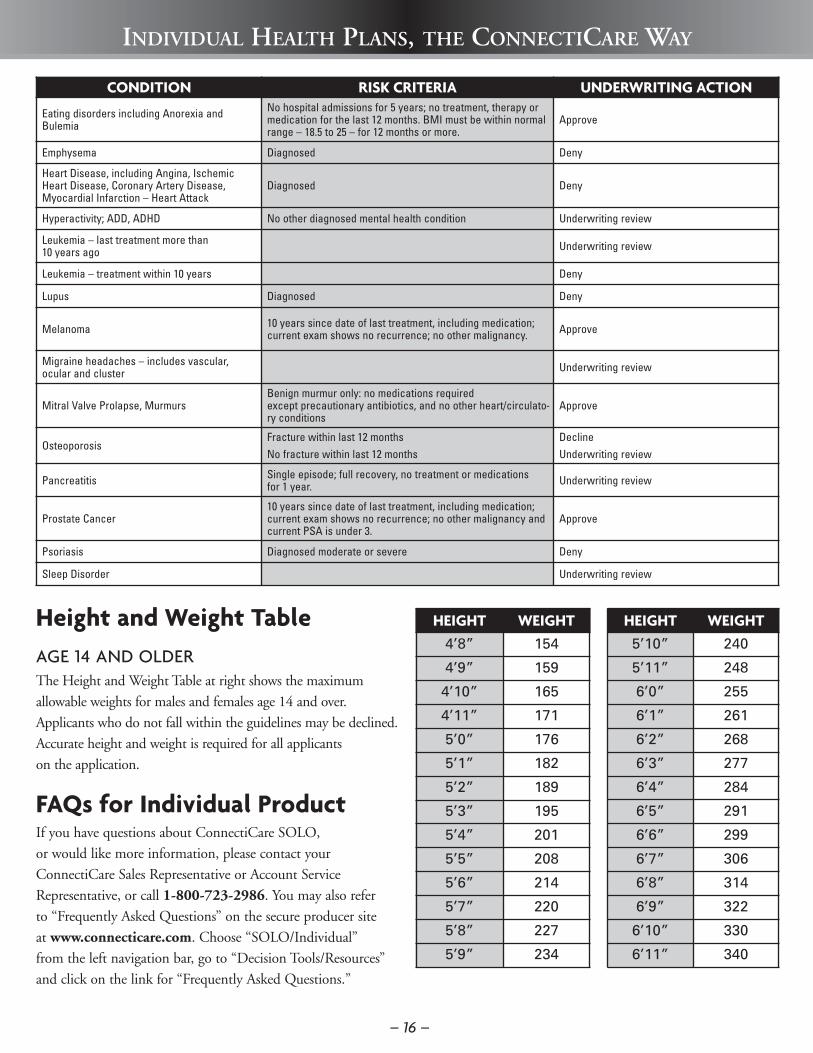
Height and Weight TableAGE 14 AND OLDERThe Height and Weight Table at right shows the maximum
allowable weights for males and females age 14 and over.
Applicants who do not fall within the guidelines may be declined.
Accurate height and weight is required for all applicants
on the application.
FAQs for Individual ProductIf you have questions about ConnectiCare SOLO,
or would like more information, please contact your
ConnectiCare Sales Representative or Account Service
Representative, or call 1-800-723-2986. You may also refer
to “Frequently Asked Questions” on the secure producer site
at www.connecticare.com. Choose “SOLO/Individual”
from the left navigation bar, go to “Decision Tools/Resources”
and click on the link for “Frequently Asked Questions.”
– 16 –
INDIVIDUAL HEALTH PLANS, THE CONNECTICARE WAY
CONDITION RISK CRITERIA UNDERWRITING ACTION
Eating disorders including Anorexia andBulemia
No hospital admissions for 5 years; no treatment, therapy ormedication for the last 12 months. BMI must be within normalrange – 18.5 to 25 – for 12 months or more.
Approve
Emphysema Diagnosed Deny
Heart Disease, including Angina, IschemicHeart Disease, Coronary Artery Disease,Myocardial Infarction – Heart Attack
Diagnosed Deny
Hyperactivity; ADD, ADHD No other diagnosed mental health condition Underwriting review
Leukemia – last treatment more than 10 years ago Underwriting review
Leukemia – treatment within 10 years Deny
Lupus Diagnosed Deny
Melanoma 10 years since date of last treatment, including medication;current exam shows no recurrence; no other malignancy. Approve
Migraine headaches – includes vascular, ocular and cluster Underwriting review
Mitral Valve Prolapse, MurmursBenign murmur only: no medications required except precautionary antibiotics, and no other heart/circulato-ry conditions
Approve
OsteoporosisFracture within last 12 monthsNo fracture within last 12 months
DeclineUnderwriting review
Pancreatitis Single episode; full recovery, no treatment or medications for 1 year. Underwriting review
Prostate Cancer10 years since date of last treatment, including medication;current exam shows no recurrence; no other malignancy andcurrent PSA is under 3.
Approve
Psoriasis Diagnosed moderate or severe Deny
Sleep Disorder Underwriting review
HEIGHT WEIGHT4’8” 154
4’9” 159
4’10” 165
4’11” 171
5’0” 176
5’1” 182
5’2” 189
5’3” 195
5’4” 201
5’5” 208
5’6” 214
5’7” 220
5’8” 227
5’9” 234
HEIGHT WEIGHT5’10” 240
5’11” 248
6’0” 255
6’1” 261
6’2” 268
6’3” 277
6’4” 284
6’5” 291
6’6” 299
6’7” 306
6’8” 314
6’9” 322
6’10” 330
6’11” 340
ConnectiCare, Inc. & Affiliates175 Scott Swamp RoadFarmington, CT 06034
HMO coverage is underwritten by ConnectiCare, Inc.; POS coverage is underwritten by ConnectiCare Insurance Company, Inc. This plan is issued on an individual basis and is regulated as an individual health insurance plan. This plan is not available to employer groups. SOLO PG 0409
www.connecticare.com/solo
Questions?If you have questions about ConnectiCare SOLO, or would like moreinformation, please contact your ConnectiCare Sales Representative orAccount Service Representative, or call 1-800-723-2986.