Embed Size (px)
Citation preview
Pro: Perioperative anti-TNF Biologics are safe and do not increase
complications associated with surgery.
Pro: Perioperative anti-TNF Biologics are safe and do not increase
complications associated with surgery.
Miguel Regueiro, M.D.Professor of MedicineAssociate Chief for EducationClinical Head and Co-Director, IBD CenterUniversity of Pittsburgh School of Medicine
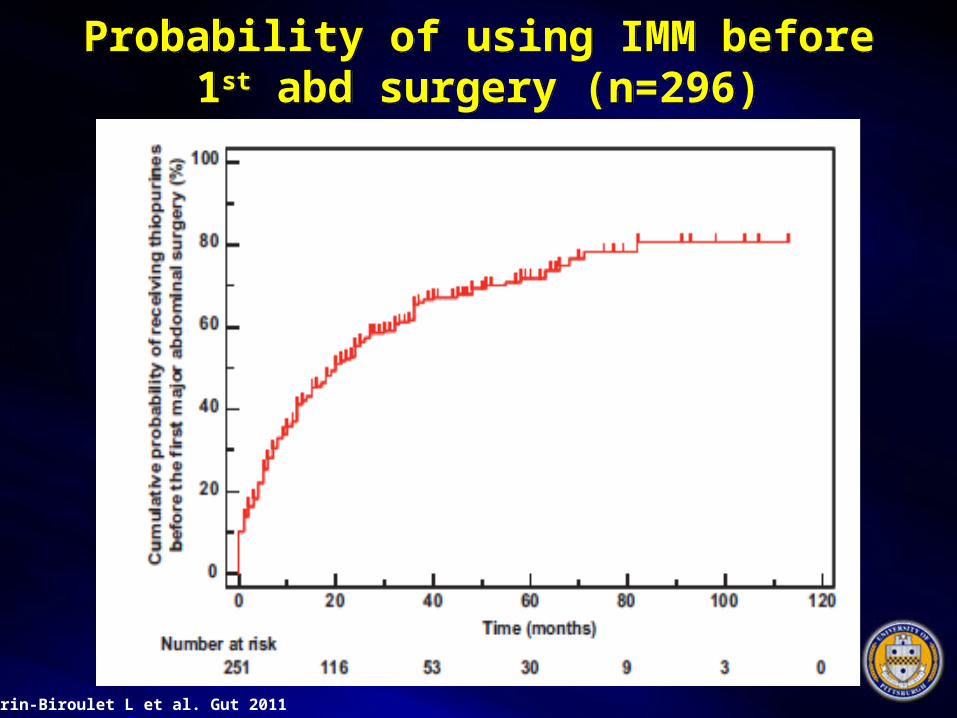
Peyrin-Biroulet L et al. Gut 2011
Probability of using IMM before 1st abd surgery (n=296)
Probability of using IMM before 1st abd surgery (n=296)
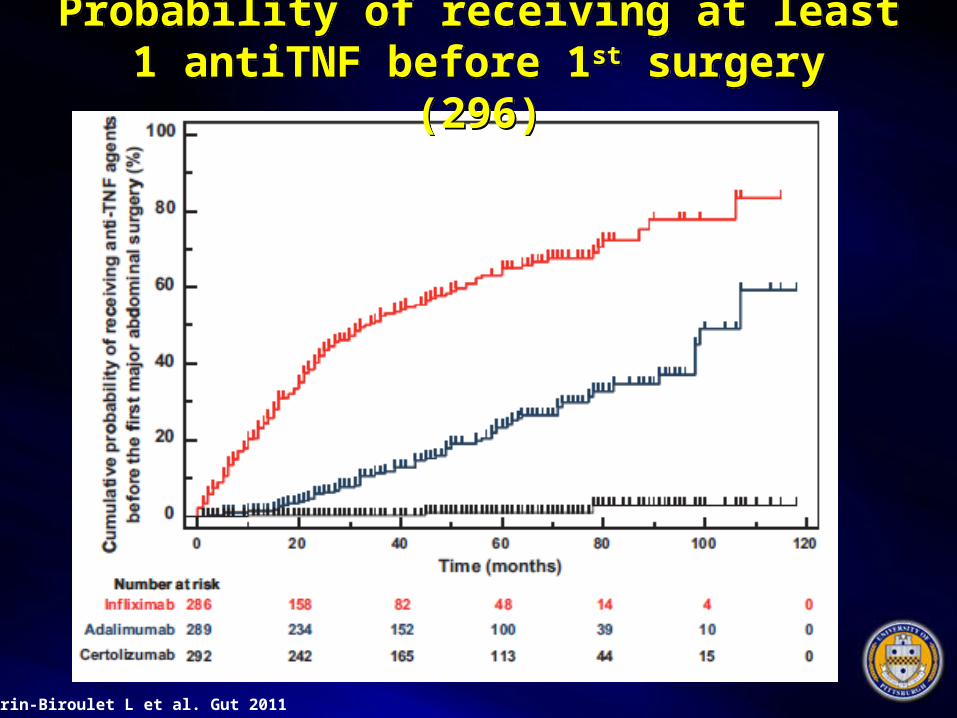
Peyrin-Biroulet L et al. Gut 2011
Probability of receiving at least 1 antiTNF before 1st surgery (296)
Probability of receiving at least 1 antiTNF before 1st surgery (296)
This means that most IBD patients undergoing surgery are taking an
IMM and/or antiTNF
This means that most IBD patients undergoing surgery are taking an
IMM and/or antiTNF
-If it’s an emergent surgery, we don’t have much choice on altering pre-op meds.
-Should the type of operation be altered?
-If the surgery is elective:-Should we alter pre-op meds?
Is starting an antiTNF in the postop setting safe?

Dr Remzi will argue that peri-operative antiTNF is unsafe
Dr Remzi will argue that peri-operative antiTNF is unsafe
As you may know, there’s a bit of a rivalry between Pittsburgh and
Cleveland
Pittsburgh vs ClevelandPittsburgh vs Cleveland

Despite the intercity rivalry, I have the utmost respect for Dr Remzi
and the Cleveland Clinic
Despite the intercity rivalry, I have the utmost respect for Dr Remzi
and the Cleveland Clinic
In reality, our hospitals and cities are quite similar

UPMC and Pittsburgh on a typical summer morning

Cleveland Clinic on that same, bright summer morning

A Tale of Two Cities – a surgeon’s perspective on postop outcome
A Tale of Two Cities – a surgeon’s perspective on postop outcome
• 27 yo CD from Youngstown OH sees Dr Regueiro in Pittsburgh on AZA/ADA
• Develops SBO while in Cleveland and requires emergent surgery w Dr Remzi
• Scenario 1: dc’d 4 days later, “great!” – Dr Remzi – “I am a brilliant surgeon!!”
• Scenario 2: POD 2 develops an anast leak – Dr Remzi – “it’s all because of those poisons Dr Regueiro was giving you!”
Three Scenarios to ConsiderThree Scenarios to Consider
• PRE-operative antiTNF for CROHN’S disease and POST-op complications
• PRE-operative antiTNF for ULCERATIVE COLITIS disease and POST-op complications
• POST-operative antiTNF for CROHN’S disease and POST-op complications
PRE-operative antiTNF for CROHN’S disease and POST-op complications
PRE-operative antiTNF for CROHN’S disease and POST-op complications
What are the data?
9 Crohn’s ds Postop References9 Crohn’s ds Postop References• Tay et al. Surgery 2003• Marchal et al. Aliment Pharmacol Ther 2004
• Colombel et al. Am J Gastroenterol 2004
• Appau et al. J Gastrointest Surg 2008
• Indar et al. World J Surg 2009
• Canedo et al. Colorectal Dis 2011
• Nasir et al. J Gastrointest Surg 2012
• Kasparek et al. Inflamm Bowel Dis 2012
• Kopylov et al. Inflamm Bowel Dis 2012

Tay – Multivariate analysis suggests improved perioperative outcome in CD
pts receiving IMMs before resection
Tay – Multivariate analysis suggests improved perioperative outcome in CD
pts receiving IMMs before resection
• Overall, 11% Postop complications (5.6% on IMM, 25% not on IMM)
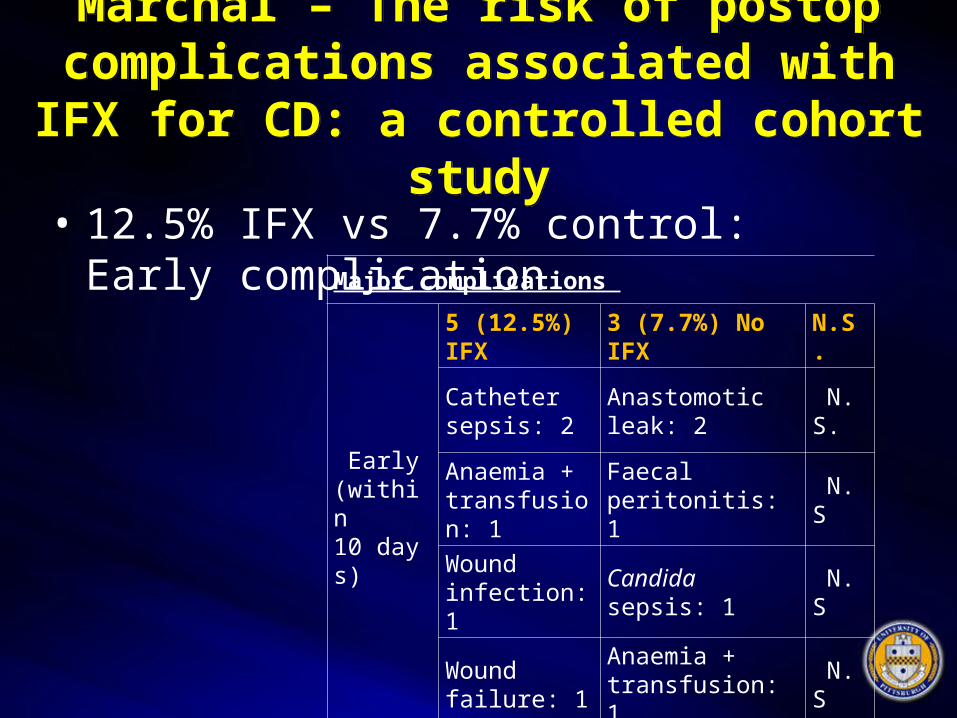
Marchal – The risk of postop complications associated with IFX for
CD: a controlled cohort study
Marchal – The risk of postop complications associated with IFX for
CD: a controlled cohort study
• 12.5% IFX vs 7.7% control: Early complication Major complications
Early (within 10 days)
5 (12.5%) IFX 3 (7.7%) No IFX N.S.
Catheter sepsis: 2
Anastomotic leak: 2
N.S.
Anaemia + transfusion: 1
Faecal peritonitis: 1
N.S
Wound infection: 1
Candida sepsis: 1 N.S
Wound failure: 1
Anaemia + transfusion: 1
N.S
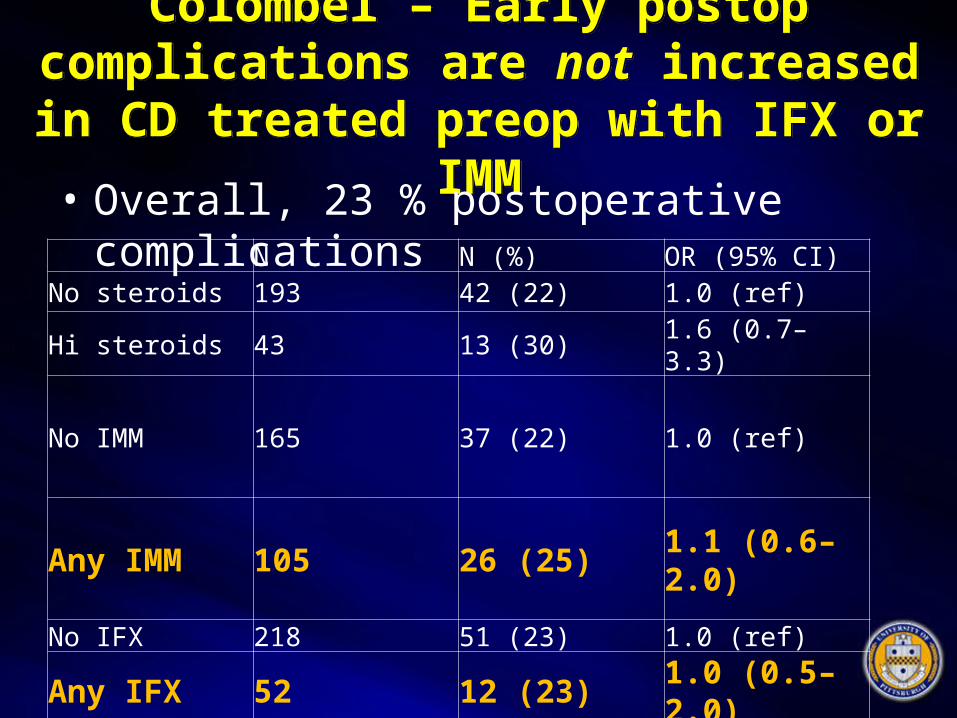
Colombel – Early postop complications are not increased in CD treated preop
with IFX or IMM
Colombel – Early postop complications are not increased in CD treated preop
with IFX or IMM• Overall, 23 % postoperative complications
N N (%) OR (95% CI)No steroids 193 42 (22) 1.0 (ref)Hi steroids 43 13 (30) 1.6 (0.7–3.3)
No IMM 165 37 (22) 1.0 (ref)
Any IMM 105 26 (25) 1.1 (0.6–2.0)
No IFX 218 51 (23) 1.0 (ref)
Any IFX 52 12 (23) 1.0 (0.5–2.0)
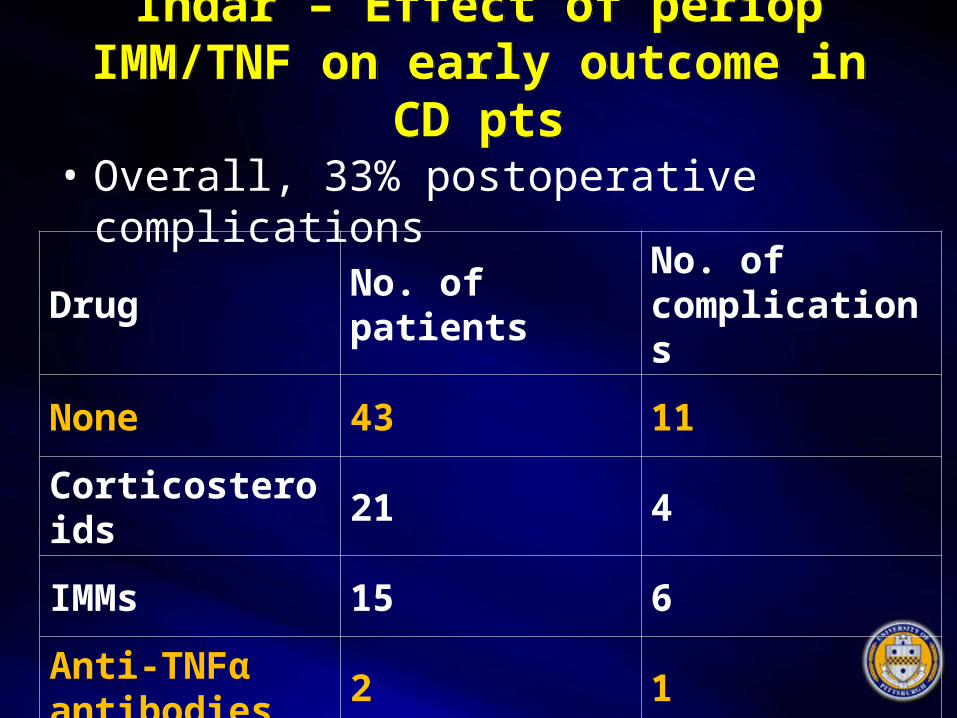
Indar – Effect of periop IMM/TNF on early outcome in CD pts
Indar – Effect of periop IMM/TNF on early outcome in CD pts
• Overall, 33% postoperative complications
Drug No. of patientsNo. of complications
None 43 11
Corticosteroids 21 4
IMMs 15 6
Anti-TNFα antibodies
2 1
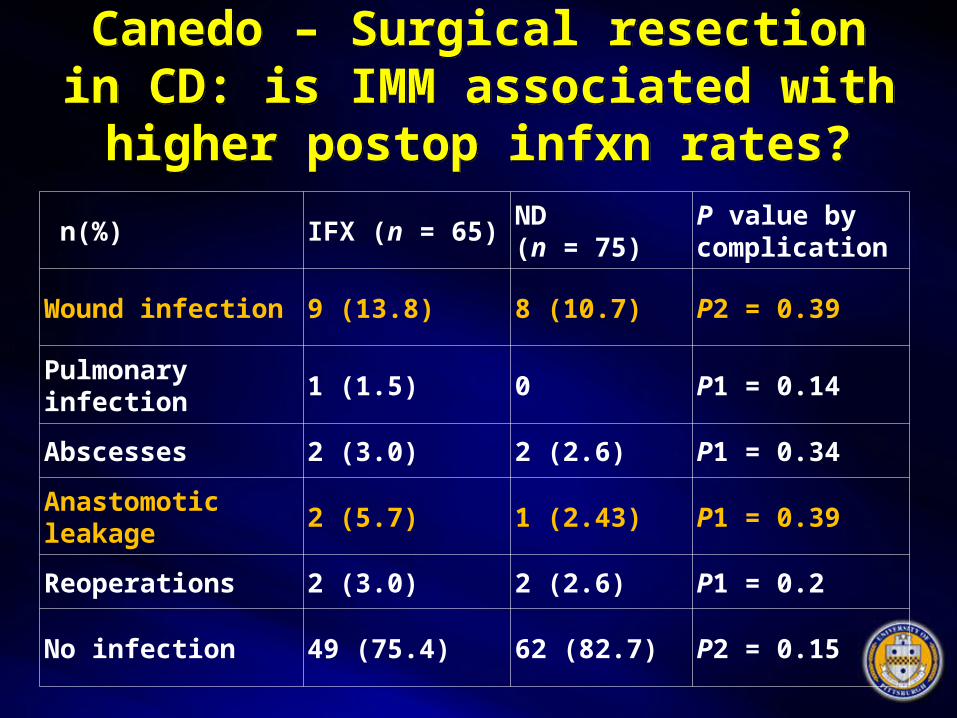
Canedo – Surgical resection in CD: is IMM associated with higher
postop infxn rates?
Canedo – Surgical resection in CD: is IMM associated with higher
postop infxn rates?
n(%) IFX (n = 65) ND (n = 75)P value by complication
Wound infection 9 (13.8) 8 (10.7) P2 = 0.39
Pulmonary infection
1 (1.5) 0 P1 = 0.14
Abscesses 2 (3.0) 2 (2.6) P1 = 0.34
Anastomotic leakage
2 (5.7) 1 (2.43) P1 = 0.39
Reoperations 2 (3.0) 2 (2.6) P1 = 0.2
No infection 49 (75.4) 62 (82.7) P2 = 0.15

Nasir – Periop antiTNF does not increase the early postop complications in CD
Nasir – Periop antiTNF does not increase the early postop complications in CD• Overall, 29% postoperative complications
Abscess/anastomotic leak
N (%) OR (95% CI) OR P value
No anti-TNF 251 5 (1.99) 1.0 (ref)
Anti-TNF 119 4 (3.36) 1.7 (0.5–6.5) 0.43

Kasparek – IFX does not affect postop complication rates in CD
Kasparek – IFX does not affect postop complication rates in CD
• Overall, 59% postoperative complications
Major complications
IFX 16 in 13 patients
No IFX 15 in 12 patients
p1.0
Anastomotic leak 2 (4%) 6 (13%) 0.27
Intraabdominal abscess
3 (6%) 5 (10%) 0.71
Patients requiring reoperation
11 (23%) 10 (21%) 1.0
Postoperative hospital stay (d)
13 [5–41] 12 [5–54] 0.64
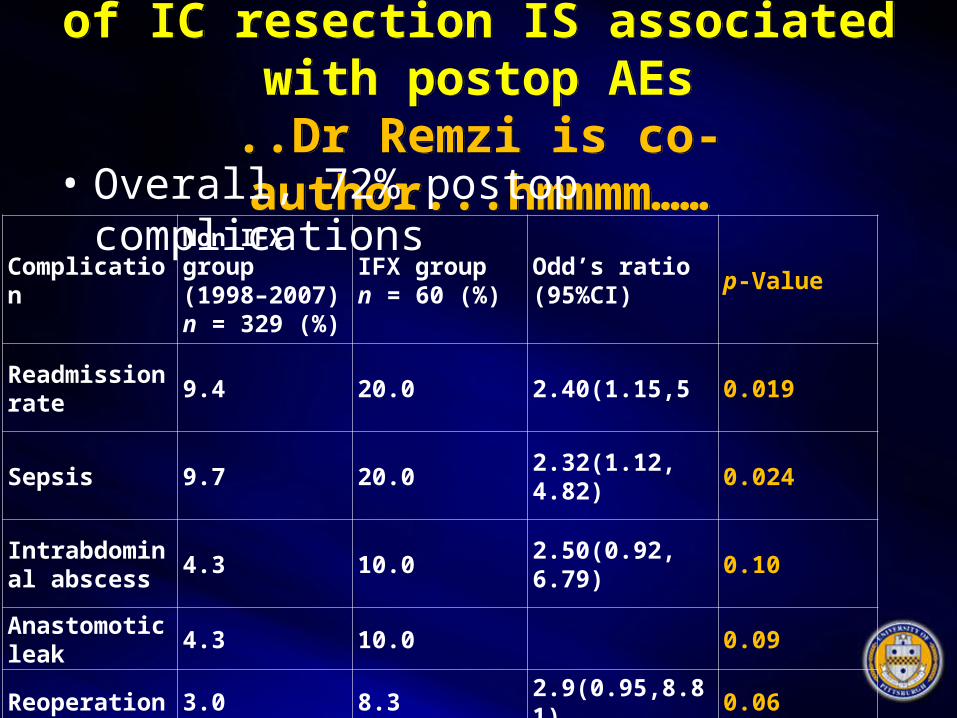
Appau – Use of IFX within 3 mos of IC resection IS associated with postop AEs
..Dr Remzi is co-author...hmmmm……
Appau – Use of IFX within 3 mos of IC resection IS associated with postop AEs
..Dr Remzi is co-author...hmmmm……• Overall, 72% postop complications
ComplicationNon IFX group (1998–2007) n = 329 (%)
IFX group n = 60 (%)
Odd’s ratio (95%CI)
p-Value
Readmission rate
9.4 20.0 2.40(1.15,5 0.019
Sepsis 9.7 20.0 2.32(1.12, 4.82) 0.024
Intrabdominal abscess
4.3 10.0 2.50(0.92, 6.79) 0.10
Anastomotic leak
4.3 10.0 0.09
Reoperation 3.0 8.3 2.9(0.95,8.81) 0.06

Kopylov – AntiTNF and Postop complications in CD: Systematic
Review and Meta-analysis
Kopylov – AntiTNF and Postop complications in CD: Systematic
Review and Meta-analysis
- OR 1.7 (CI, .93-3.19) postop complications
- Number Needed to Harm = 20
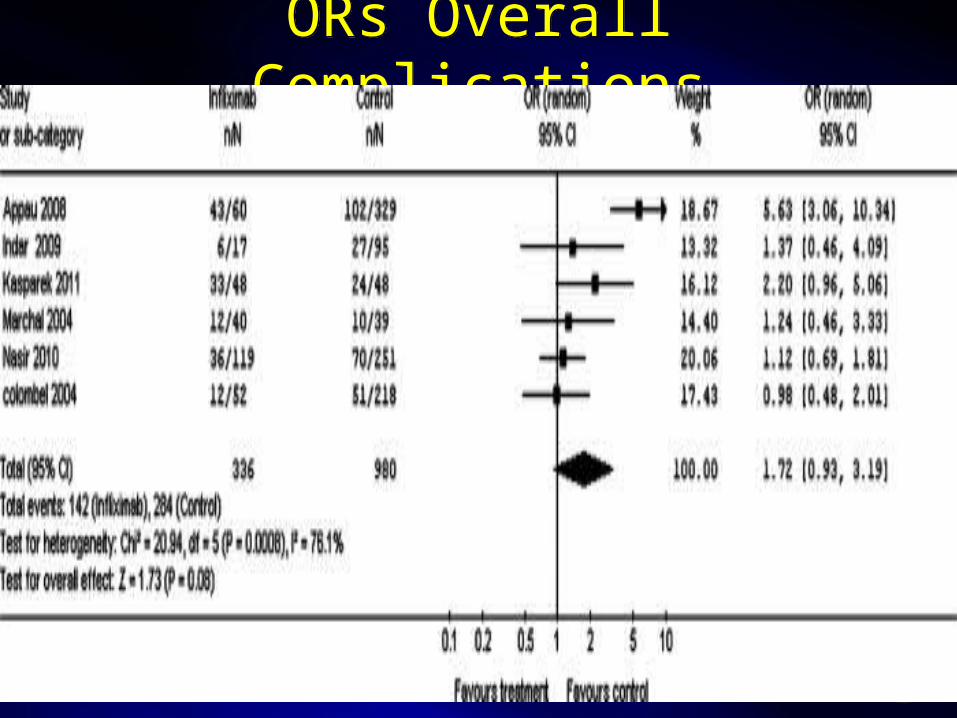
ORs Overall ComplicationsORs Overall Complications
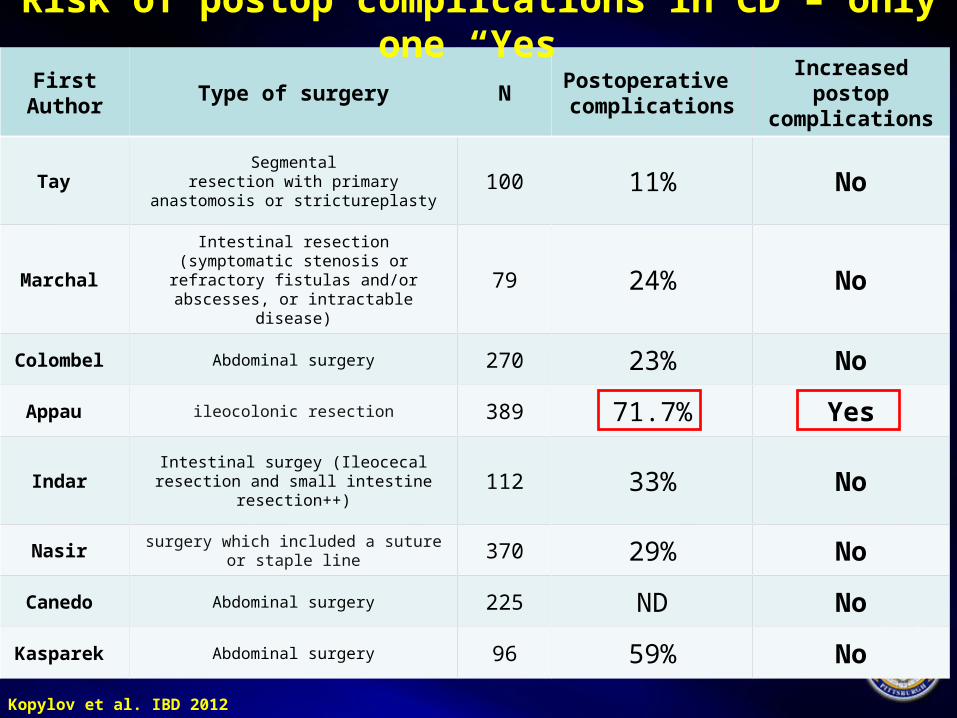
First Author
Type of surgery NPostoperative complications
Increased postop complications
Tay Segmental
resection with primary anastomosis or strictureplasty
100 11% No
Marchal Intestinal resection (symptomatic stenosis or
refractory fistulas and/orabscesses, or intractable disease)
79 24% No
Colombel Abdominal surgery 270 23% No
Appau ileocolonic resection 389 71.7% Yes
Indar Intestinal surgey (Ileocecal resection and small
intestine resection++) 112 33% No
Nasir surgery which included a suture or staple line 370 29% No
Canedo Abdominal surgery 225 ND No
Kasparek Abdominal surgery 96 59% No
Kopylov et al. IBD 2012
Risk of postop complications in CD – only one “Yes”
PRE-operative antiTNF for ULCERATIVE COLITIS disease
and POST-op complications
PRE-operative antiTNF for ULCERATIVE COLITIS disease
and POST-op complications
What’s the data?
UC Postop ReferencesUC Postop References• Selvasekar et al J Am Coll Surg 2007• Schluender et al Dis Colon Rectum 2007• Mor et al Dis Colon Rectum 2008• Ferrante et al Inflamm Bowel Dis 2009• Norgard et Aliment Pharmacol Ther 2012• Yang et al Aliment Pharmacol Ther 2010
UC and CD Studies combined:• Kunitake et al J Gastrointest Surg 2008• Waterman et al Gut 2012
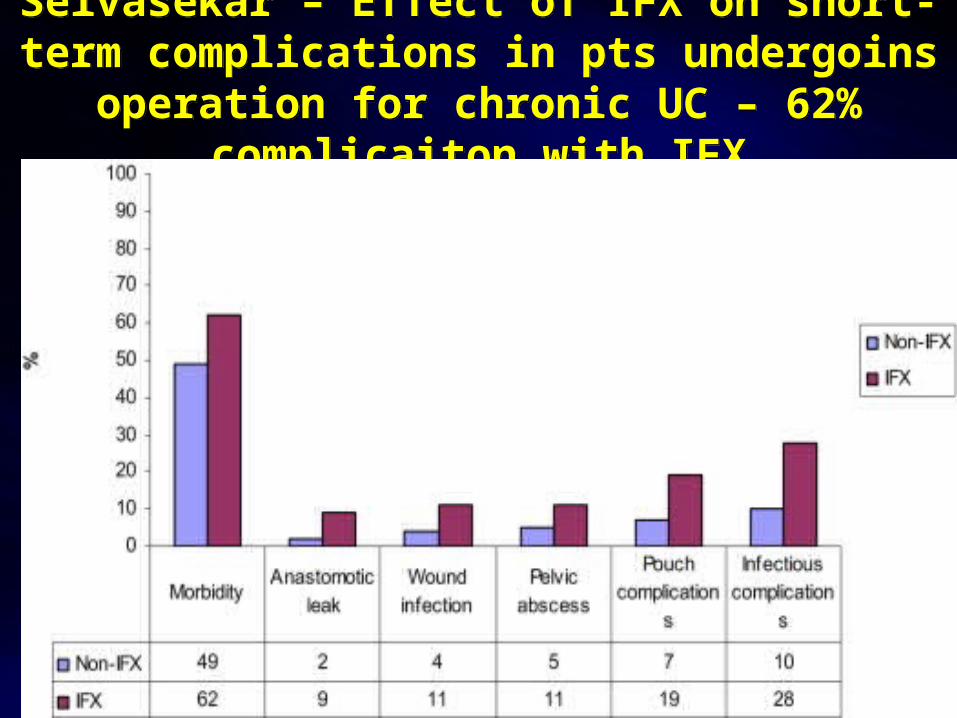
Selvasekar – Effect of IFX on short-term complications in pts undergoins operation for
chronic UC – 62% complicaiton with IFX
Selvasekar – Effect of IFX on short-term complications in pts undergoins operation for
chronic UC – 62% complicaiton with IFX
Mor – IFX in UC is associated with an increased risk of postop complications
after restorative proctocolectomy
Mor – IFX in UC is associated with an increased risk of postop complications
after restorative proctocolectomy
• OR early complication IFX 3.54 (P = 0.004; 95% CI1.51-8.31).
• OR sepsis IFX 13.8 (P = 0.011; 95% CI, 1.82-105)
• OR late complication IFX 2.19 times (P = 0.08; 95% CI, 0.91-5.28)
Norgard – Pre-op use of antiTNF and the risk of postop complications in pts with
UC – a nationwide cohort study
Norgard – Pre-op use of antiTNF and the risk of postop complications in pts with
UC – a nationwide cohort study
• 1226 UC pts – 199 IFX
• Most underwent ileostomy (not IPAA)
• OR reoperation 1.07 (95% CI: 0.71-1.59)
• OR anastomosis leakage 0.52 (95% CI: 0.06-4.11) respectively
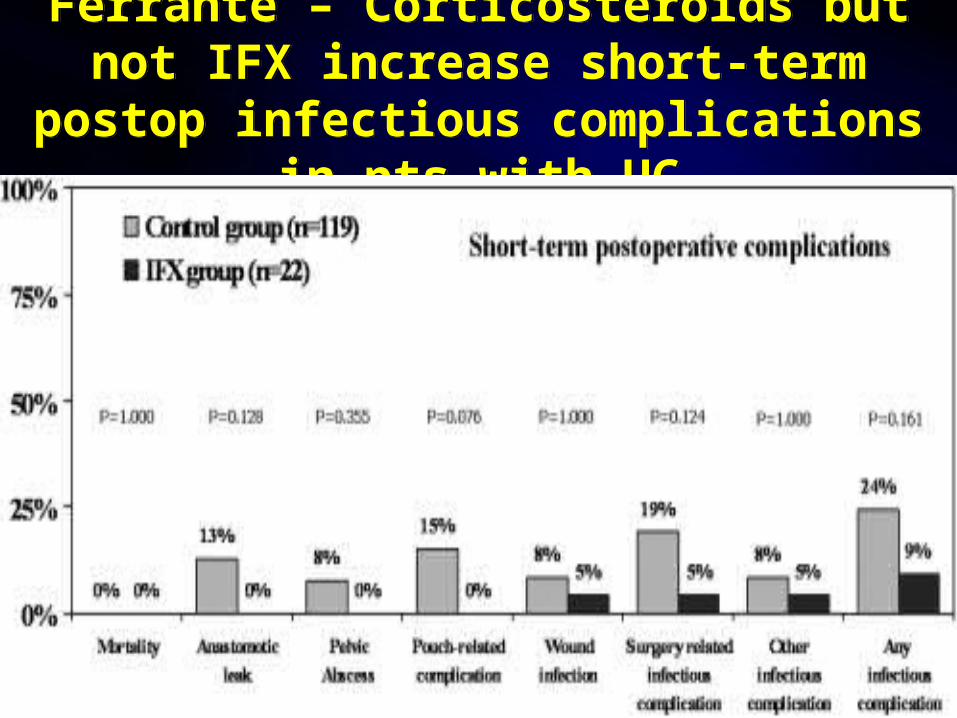
Ferrante – Corticosteroids but not IFX increase short-term postop infectious
complications in pts with UC
Ferrante – Corticosteroids but not IFX increase short-term postop infectious
complications in pts with UC
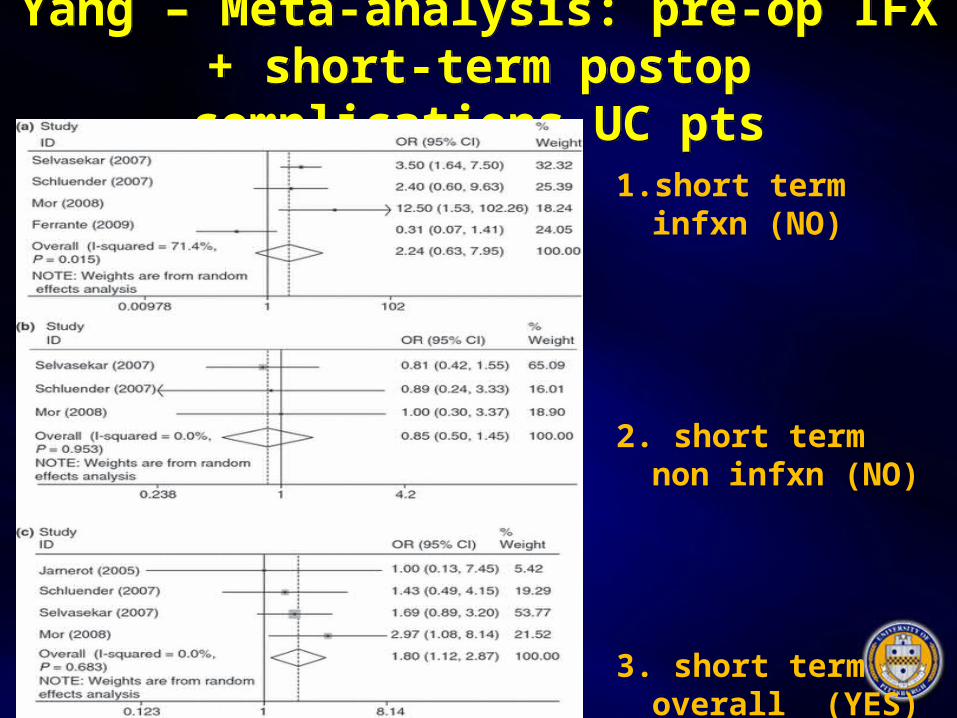
Yang – Meta-analysis: pre-op IFX + short-term postop complications UC pts
Yang – Meta-analysis: pre-op IFX + short-term postop complications UC pts
1. short term infxn (NO)
2. short term non infxn (NO)
3. short term overall (YES)

Periop antiTNF UC studiesPeriop antiTNF UC studiesAuthor Type of
SurgeryN Postoperative
ComplicationsIncreased Postop Complications
Selvasekar IPAA 30147 IFX
62% Yes
Schluender IPAA 13417 IFX
28%37%IFX v 27%
No
Mor IPAA 52385 IFX
OR IFX 3.5 totalOR IFX 13.8 infxn
Yes
Ferrante IPAA 14122 IFX
22% overallSteroids/1 step J
No
Norgard Most Ileostmy
1226199 IFX
OR IFX 0.5 No
Yang Most IPAA
5 studies OR IFX 1.8 Yes

Is starting POST-op antiTNF within 1 mos of CD surgery safe?
Is starting POST-op antiTNF within 1 mos of CD surgery safe?
Postoperative infliximab is not associated with an increase in adverse
events in Crohn's disease.
Regueiro M, El-Hachem S, Kip K, et al. Dig Dis Sci. 2011 Dec;56(12):3610-5.
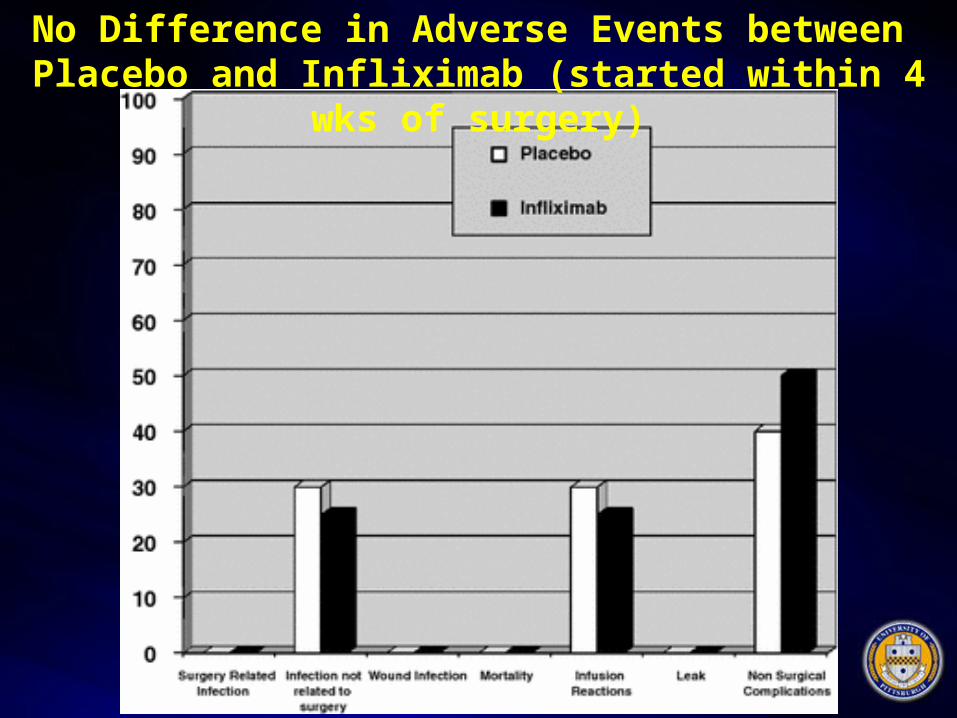
No Difference in Adverse Events between Placebo and Infliximab (started within 4 wks of surgery)
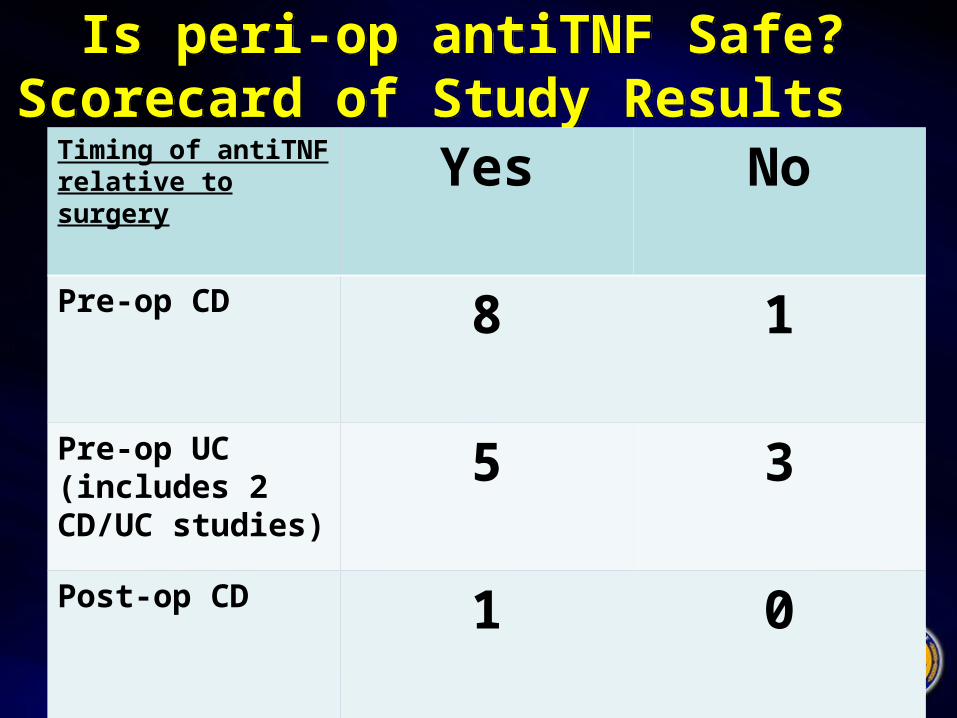
Is peri-op antiTNF Safe? Scorecard of Study Results
Is peri-op antiTNF Safe? Scorecard of Study Results
Timing of antiTNF relative to surgery Yes No
Pre-op CD 8 1
Pre-op UC (includes 2 CD/UC studies)
5 3
Post-op CD 1 0
What I do in practice?What I do in practice?
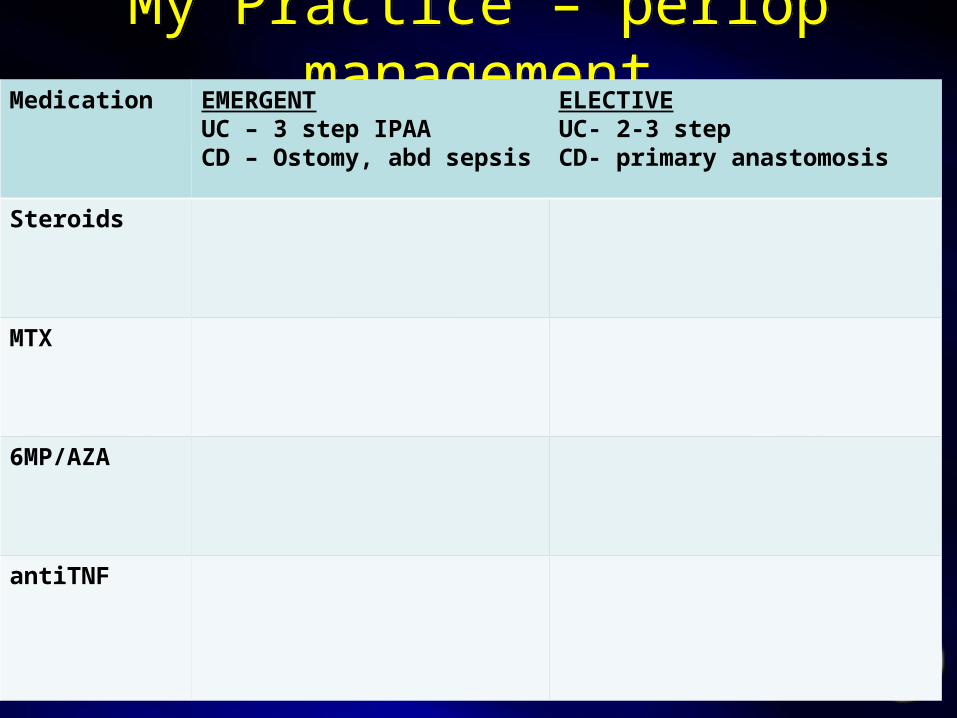
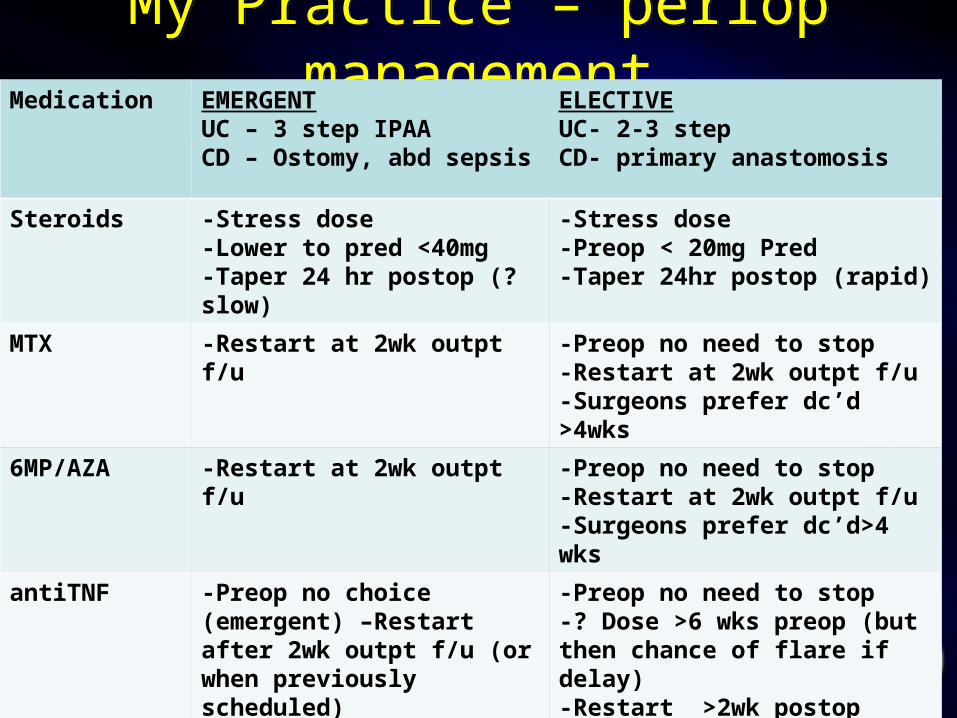
My Practice – periop managementMy Practice – periop managementMedication EMERGENT
UC – 3 step IPAA CD – Ostomy, abd sepsis
ELECTIVEUC- 2-3 stepCD- primary anastomosis
Steroids
MTX
6MP/AZA
antiTNF
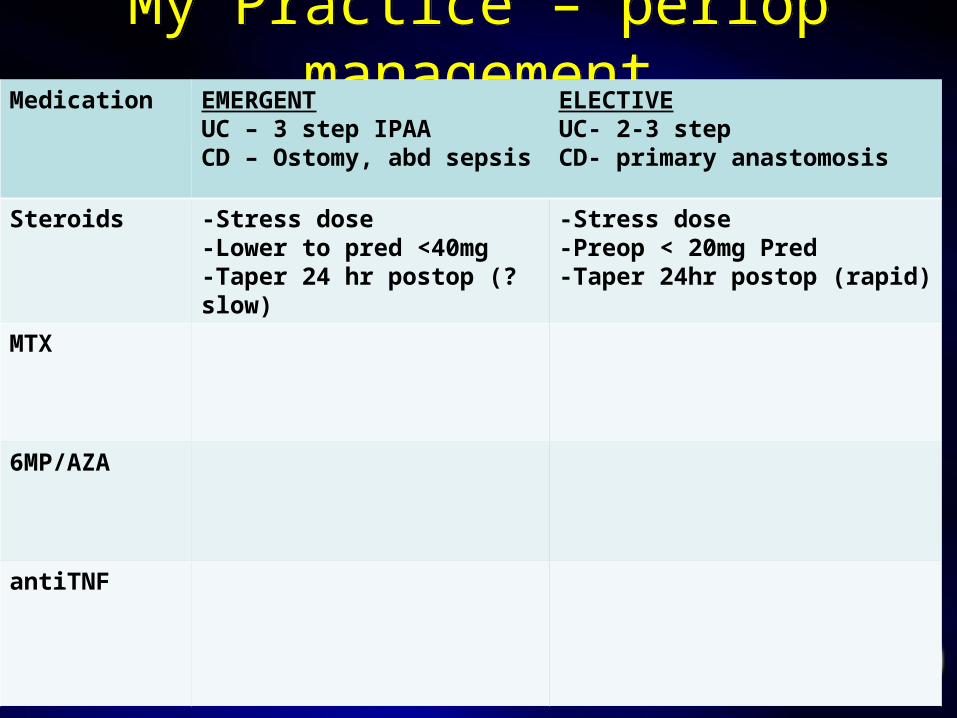
My Practice – periop managementMy Practice – periop managementMedication EMERGENT
UC – 3 step IPAA CD – Ostomy, abd sepsis
ELECTIVEUC- 2-3 stepCD- primary anastomosis
Steroids -Stress dose -Lower to pred <40mg-Taper 24 hr postop (?slow)
-Stress dose -Preop < 20mg Pred -Taper 24hr postop (rapid)
MTX
6MP/AZA
antiTNF
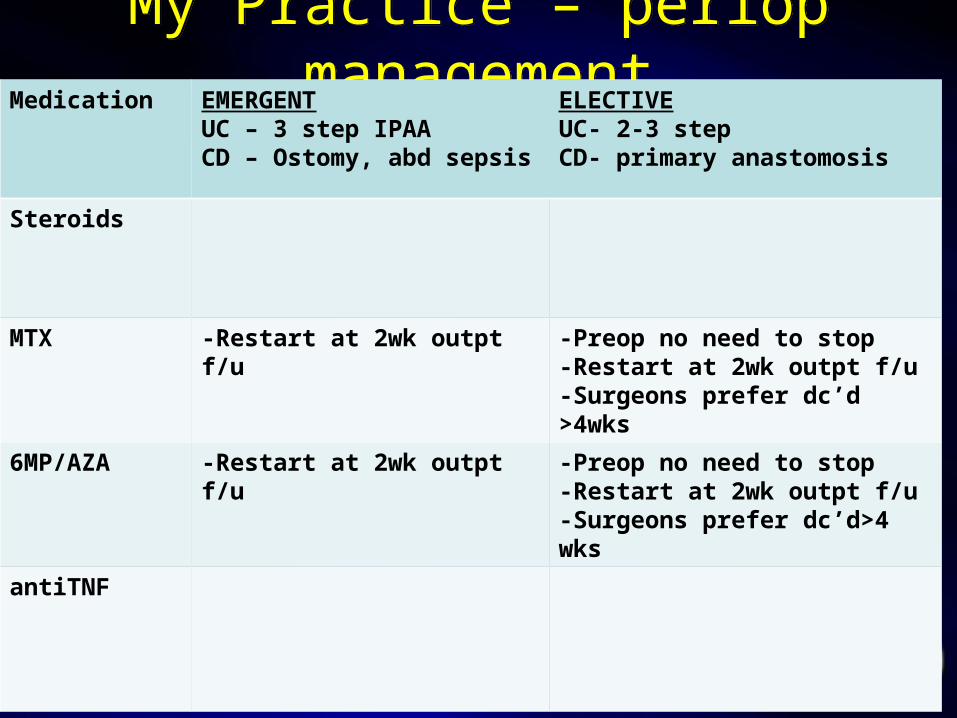
My Practice – periop managementMy Practice – periop managementMedication EMERGENT
UC – 3 step IPAA CD – Ostomy, abd sepsis
ELECTIVEUC- 2-3 stepCD- primary anastomosis
Steroids
MTX -Restart at 2wk outpt f/u -Preop no need to stop-Restart at 2wk outpt f/u-Surgeons prefer dc’d >4wks
6MP/AZA -Restart at 2wk outpt f/u -Preop no need to stop-Restart at 2wk outpt f/u-Surgeons prefer dc’d>4 wks
antiTNF

My Practice – periop managementMy Practice – periop managementMedication EMERGENT
UC – 3 step IPAA CD – Ostomy, abd sepsis
ELECTIVEUC- 2-3 stepCD- primary anastomosis
Steroids
MTX
6MP/AZA
antiTNF -Preop no choice (emergent) –Restart after 2wk outpt f/u (or when previously scheduled)
-Preop no need to stop-? Dose >6 wks preop (but then chance of flare if delay)-Restart >2wk postop
My Practice – periop managementMy Practice – periop managementMedication EMERGENT
UC – 3 step IPAA CD – Ostomy, abd sepsis
ELECTIVEUC- 2-3 stepCD- primary anastomosis
Steroids -Stress dose -Lower to pred <40mg-Taper 24 hr postop (?slow)
-Stress dose -Preop < 20mg Pred -Taper 24hr postop (rapid)
MTX -Restart at 2wk outpt f/u -Preop no need to stop-Restart at 2wk outpt f/u-Surgeons prefer dc’d >4wks
6MP/AZA -Restart at 2wk outpt f/u -Preop no need to stop-Restart at 2wk outpt f/u-Surgeons prefer dc’d>4 wks
antiTNF -Preop no choice (emergent) –Restart after 2wk outpt f/u (or when previously scheduled)
-Preop no need to stop-? Dose >6 wks preop (but then chance of flare if delay)-Restart >2wk postop
Summary Periop antiTNFSummary Periop antiTNF
• CD: antiTNF is not associated with increased risk when used in the perioperative period
• UC: severity of ds is most associated with complications rather than antiTNF– 3 step IPAA being done anyway
• Practically speaking: surgery should NOT be delayed because a patient is on antiTNF
With that, I give you Dr Remzi







![Coupling discrete elements and micropolar continuum ...civil.colorado.edu/~regueiro/publications/...[Regueiro and Yan, 2010] that retains an “open window” compu tationally on the](https://img.pdfslide.us/doc/110x75/611236c163470671bf355222/coupling-discrete-elements-and-micropolar-continuum-civil-regueiropublications.jpg)


![Overload relay - grupoimex.com térmicos.pdfTNF –20° TNF TNF –5° 750 4000 12000 1650 TNF +5° TNF +15° a b c d R [ ] i [°C] 5 47 16.5 4.7 86 60 112 Technical overview Bimetal](https://img.pdfslide.us/doc/110x75/60065006b9ae12444231e63f/overload-relay-trmicospdf-tnf-a20-tnf-tnf-a5-750-4000-12000-1650-tnf.jpg)


















