Embed Size (px)
Citation preview

Inflammatory Bowel Disease
51© T O U C H B R I E F I N G S 2 0 0 8
a report by
Miguel Regueiro , MD 1 and Mark Lazarev , MD 2
1. Head, Clinical Inflammatory Bowel Disease Program, Division of Gastroenterology, Hepatology, and Nutrition, and Co-Director, Inflammatory Bowel Disease Center,
University of Pittsburgh Medical Center; 2. Fellow, Division of Gastroenterology, Hepatology, and Nutrition, University of Pittsburgh Medical Center
Biologics or Surgery—Which Is Better for the Treatment of Ulcerative Colitis?
Ulcerative colitis (UC) is a disease that has a prevalence of 35–100 per
100,000 people. While UC can often be controlled with 5-aminosalicylic
acid (5-ASA) products and immunomodulators such as azathioprine and
mercaptopurine (6-MP), some patients continue to have active colitis
requiring corticosteroids. Approximately 15% of UC patients will require
hospitalization and treatment with intravenous (IV) steroids at some point
in their lifetime; 25% of these are corticosteroid-refractory and will require
a colectomy. Infliximab has recently emerged as another treatment option
for the induction and maintenance of remission in moderate to severe UC.
Management of Ulcerative Colitis—The Surgical Option
A proctocolectomy is a cure for UC. The surgical options include a
conventional Brooke ileostomy, a continent (Kock pouch) ileostomy, and
an ileal pouch–anal anastomosis (IPAA). The IPAA is the most frequently
performed surgery for UC. A proctocolectomy with IPAA is a cure, but
there are potential lifestyle changes and complications that can occur.
To start, patients need to be educated that bowel habits range from
three to 10 bowel movements per day following IPAA. Usually, this is an
improvement for most patients who undergo surgery for severe colitis.
Patients usually have continence of bowel movements, but incontinence
and seepage, especially nocturnal, may occur in some.
Pouchitis is one of the most common post-surgical complications for
IPAA and is probably related to bacterial stasis in the pouch reservoir. The
main symptoms are diarrhea and abdominal pain. In the largest study, of
1,043 UC patients, the five-year cumulative risk of developing one or
more episodes of pouchitis that required treatment was 36% in patients
without primary sclerosing cholangitis (PSC) and 61% in patients with
PSC.1 Occasionally, pouchitis can become chronic and refractory to
medical therapy.
Another complication of IPAA surgery is decreased fecundity among
female patients. Generally, women with UC have normal fertility levels.
Olsen et al. reported their findings on decreased fecundity in female UC
patients undergoing IPAA. Structured phone interviews concerning
reproductive behavior and waiting times to pregnancy were performed
on 290 female patients with UC.2 Rates of fecundity were the same prior
to diagnosis and before IPAA surgery. However, after surgery the
fecundity ratio (fecundability rate compared with reference population)
dropped to 20% (p<0.0001). This issue needs to be discussed with
female UC patients of child-bearing age who are contemplating surgery.
Of note, patients who undergo permanent or temporary end-ileostomy
do not seem to have decreased fecundability rates.
Rarer complications of IPAA include small-bowel obstruction (20%),
pouch–vaginal fistula (4%), impotence (1.5%), and death (<0.5%).
Overall, the cumulative risk of complications at five years is 68%.3 In
terms of costs, Thompson et al. found increased inpatient and overall
healthcare utilization costs for patients with UC following colectomy.4
Finally, an equal percentage of respondents who had undergone a
colectomy for UC reported that their lives were better before surgery
compared with after surgery.5
Given the Complication Profile of Colectomy for
Ulcerative Colitis, Should Biologic Therapy Be
Considered Before Surgery?
Infliximab has been shown to be effective for moderate to severe UC. In
ACT-1 and ACT-2, Rutgeerts et al. performed a placebo-controlled
double-blind randomized trial on 364 patients who received infliximab
5mg/kg, infliximab 10mg/kg, or placebo.6 Outcome measures were
clinical response (defined as at least a three-point and 30% decrease in
the Mayo score) at eight and 30 weeks. At eight weeks, 69% of patients
in the 5mg/kg arm had a clinical response compared with 37% for
placebo controls. At 30 weeks, the response rate was 52% for the
infliximab group compared with 30% for controls (p=0.002). There was
no statistically significant difference between the 5mg/kg and 10mg/kg
arms for both time-points. Additionally, concomitant immunomodulator
Miguel Regueiro, MD, is an Associate Professor of Medicine atthe University of Pittsburgh School of Medicine, Head of theClinical Inflammatory Bowel Disease Program in the Division ofGastroenterology, Hepatology, and Nutrition, and Co-Director ofthe Inflammatory Bowel Disease Center at the University ofPittsburgh Medical Center. He is also the Associate Chief forEducation and Director of the Gastroenterology, Hepatology,and Nutrition Fellowship Training Program at the University ofPittsburgh. Dr Regueiro’s main clinical and research interest is
inflammatory bowel disease (IBD), with a focus on Crohn’s disease and ulcerative colitis. He is theprincipal investigator for several multicenter international research trials and conducts clinicalresearch that defines the natural course and phenotypes of IBD. He is a member of severalprofessional and scientific societies, including the American Gastroenterological Association(AGA), the American College of Gastroenterology (ACG), and the Crohn’s Colitis Foundation ofAmerica (CCFA). He has received multiple honors, including the Clinical Investigator TrainingAward from Beth Israel Hospital-Harvard/Massachussetts Institute of Technology (MIT) HealthSciences, the 2002 CCFA Physician of the Year, and the 2003 National Research Excellence inGastrointestinal Disease Award. In addition, Dr Regueiro has been an invited lecturer and keynotespeaker for national and international seminars and has published many articles, reviews, andabstracts in gastroenterology journals. He received his BA from the University of Pennsylvania andhis MD from Hahnemann University, before completing his internal medicine internship andresidency and clinical and research fellowship training in gastroenterology at Harvard MedicalSchool’s Beth Israel Hospital.
regueiro.qxp 15/4/08 11:07 Page 51
Inflammatory Bowel Disease
52 U S G A S T R O E N T E R O L O G Y
or 5-ASA use did not change the outcomes of response or remission in
the subgroup analysis. In a post hoc analysis of ACT-1 and ACT-2, there
was a 43% risk reduction in colectomy rate at 54 weeks in patients who
received infliximab compared with those who received placebo.7 Also,
health-related quality of life in the same study group was found to be
significantly improved after one year.8
Patients in ACT-1 and ACT-2 were treated on an outpatient basis.
Infliximab’s success is less pronounced in the inpatient setting,
particularly among patients with steroid-refractory disease. In a
randomized double-blind trial, Jarnerot et al. examined 45 patients with
severe to moderately severe UC who were hospitalized and placed on
high-dose IV corticosteroids.9 If they satisfied the criteria for fulminant
colitis at day three, or if they were found to meet criteria for severe to
moderately severe disease (by the Seo index) at day five to seven, they
were then randomized to receive a single 4–5mg/kg infusion of
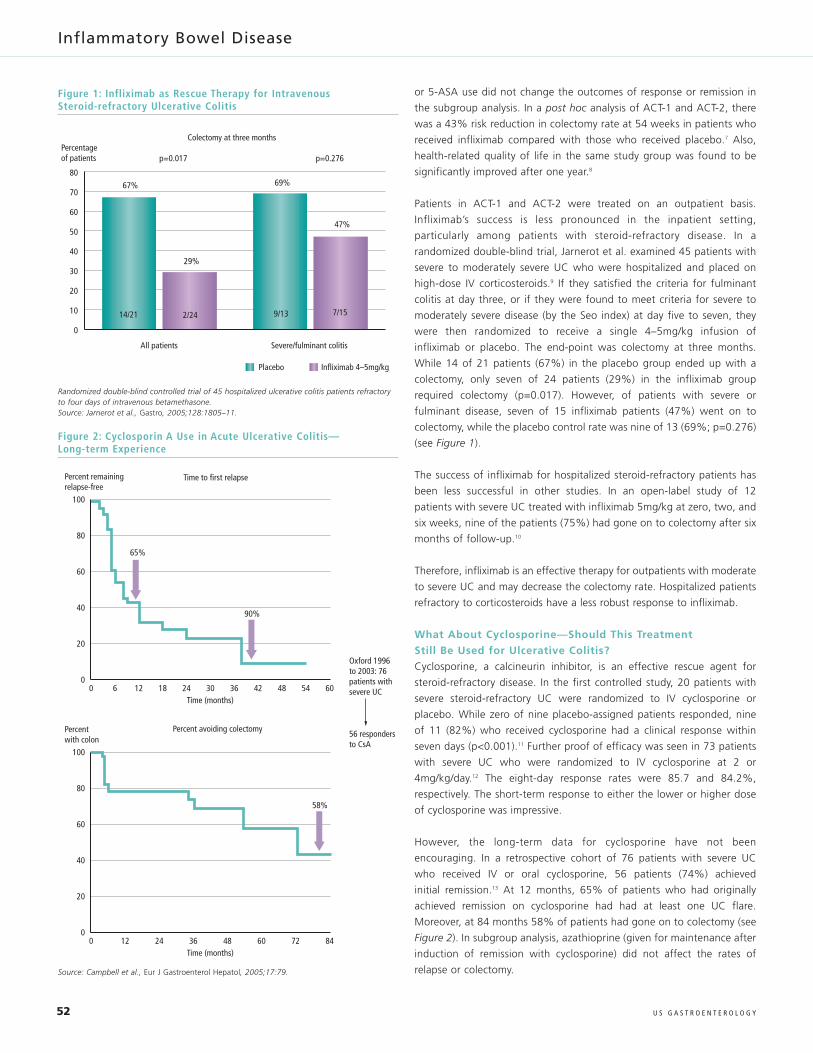
infliximab or placebo. The end-point was colectomy at three months.
While 14 of 21 patients (67%) in the placebo group ended up with a
colectomy, only seven of 24 patients (29%) in the infliximab group
required colectomy (p=0.017). However, of patients with severe or
fulminant disease, seven of 15 infliximab patients (47%) went on to
colectomy, while the placebo control rate was nine of 13 (69%; p=0.276)
(see Figure 1).
The success of infliximab for hospitalized steroid-refractory patients has
been less successful in other studies. In an open-label study of 12
patients with severe UC treated with infliximab 5mg/kg at zero, two, and
six weeks, nine of the patients (75%) had gone on to colectomy after six
months of follow-up.10
Therefore, infliximab is an effective therapy for outpatients with moderate
to severe UC and may decrease the colectomy rate. Hospitalized patients
refractory to corticosteroids have a less robust response to infliximab.
What About Cyclosporine—Should This Treatment
Still Be Used for Ulcerative Colitis?
Cyclosporine, a calcineurin inhibitor, is an effective rescue agent for
steroid-refractory disease. In the first controlled study, 20 patients with
severe steroid-refractory UC were randomized to IV cyclosporine or
placebo. While zero of nine placebo-assigned patients responded, nine
of 11 (82%) who received cyclosporine had a clinical response within
seven days (p<0.001).11 Further proof of efficacy was seen in 73 patients
with severe UC who were randomized to IV cyclosporine at 2 or
4mg/kg/day.12 The eight-day response rates were 85.7 and 84.2%,
respectively. The short-term response to either the lower or higher dose
of cyclosporine was impressive.
However, the long-term data for cyclosporine have not been
encouraging. In a retrospective cohort of 76 patients with severe UC
who received IV or oral cyclosporine, 56 patients (74%) achieved
initial remission.13 At 12 months, 65% of patients who had originally
achieved remission on cyclosporine had had at least one UC flare.
Moreover, at 84 months 58% of patients had gone on to colectomy (see
Figure 2). In subgroup analysis, azathioprine (given for maintenance after
induction of remission with cyclosporine) did not affect the rates of
relapse or colectomy.
Figure 1: Infliximab as Rescue Therapy for Intravenous Steroid-refractory Ulcerative Colitis
0
All patients
Colectomy at three months
p=0.017
67%
29%
69%
47%
Percentageof patients p=0.276
Placebo Infliximab 4–5mg/kg
Severe/fulminant colitis
10
20
30
40
50
60
70
80
14/21 2/24 9/13 7/15
Randomized double-blind controlled trial of 45 hospitalized ulcerative colitis patients refractoryto four days of intravenous betamethasone.Source: Jarnerot et al., Gastro, 2005;128:1805–11.
Figure 2: Cyclosporin A Use in Acute Ulcerative Colitis—Long-term Experience
00
65%
90%
6 12 18 24 30Time (months)
36 42 48 54 60
20
40
60
80
100
Percent remainingrelapse-free
Time to first relapse
00
58%
12 24 36 48 60Time (months)
72 84
20
40
60
80
100
Percent with colon
Oxford 1996to 2003: 76patients withsevere UC
56 respondersto CsA
Percent avoiding colectomy
Source: Campbell et al., Eur J Gastroenterol Hepatol, 2005;17:79.
regueiro.qxp 15/4/08 11:08 Page 52

Biologics or Surgery—Which Is Better for the Treatment of Ulcerative Colitis?
53U S G A S T R O E N T E R O L O G Y
Therefore, cyclosporine is an effective rescue therapy for hospitalized UC
patients refractory to steroids, but this effect is short-lived and the long-
term results are disappointing. Additionally, cyclosporine is not without
risks and serious adverse events, such as seizures, renal failure, and
opportunistic infection, have been reported.
Is Tacrolimus an Alternative Option?
Tacrolimus, like cyclosporine, works by inhibition of interleukin (IL)-2
synthesis and release. Its role in refractory UC is not as well studied. In a
study of moderate to severe steroid-refractory UC, 60 patients were
randomized to high-trough FK concentrations, low-trough, or placebo.14
After two weeks, 13 of 19 patients (68.4%) in the high-trough
(10–15ng/ml) groups had a partial response—defined as a four-point or
greater drop in disease activity index (DAI)—compared with a placebo
response of only two of 20 (10%; p<0.001). Mucosal healing was also
achieved in 78.9% of the high-trough group. Notably, patients in the
low-trough (5–10ng/ml) group did not have a clinically significant
response. Also, patients in this study were felt to be less severe, being
‘refractory’ to <30mg oral doses of prednisone. In a longer open study of
IV or oral tacrolimus, patients were followed for a mean of 16 months.15
Thirteen of 38 patients (34%) with refractory UC went into complete
remission at one month, while the two-year colectomy rate was 50%.
In general, the jury on tacrolimus in severe UC is still out. Its short-term
efficacy may be similar to that of cyclosporine, with potentially less
toxicity; however, long-term data are lacking. The inflammatory bowel
disease (IBD) community has been slow to embrace this option.
Are There Any New Medications Available?
At present, there are no new medications available. Visilizumab, a
humanized anti-CD3 monoclonal antibody, initially showed promise;16
however, it was not found to be more effective than placebo in a
phase III trial. Basiliximab and daclizumab, both monoclonal antibodies
blocking the IL-2 receptor alpha-chain (CD25) on activated T cells, have
both had mixed results, and neither drug is available.17,18 MLN02, a
monocolonal antibody that blocks α4β7 integrin, has shown efficacy in
a phase II study of patients with active UC,19 and is currently being tested
in a phase III trial.
Putting the Evidence-based Data into Perspective—
When to Operate and When to Treat with Medication
There are clear situations in which saving the colon is either not possible
or not worth the expense. Colectomy is therefore favored in the
following scenarios: toxic megacolon; severe colitis with growth
retardation (children) failing medical management; dysplasia or neoplasm
(can also include patients with numerous pseudopolyps where dyplasia
screening is not practical); long-standing (>10 years) UC requiring
multiple courses of corticosteroids, or failing 5-ASAs, immuno-
modulators, and infliximab; and inpatients refractory to IV corticosteroids
and cyclosporine.
There are situations where infliximab or cyclosporine is preferred to
colectomy. In our practice, outpatients with moderate to severe UC who
are failing on or intolerant to 5-ASAs/immunomodulators are started on
infliximab. Hospitalized UC patients refractory to three to five days of IV
corticosteroids present a treatment dilemma. We would consider those
who have never been on immunomodulator therapy for cyclosporine as a
bridge to immunomodulators. If they have received and failed—or cannot
tolerate—immunomodulators, we would not recommend cyclosporine.
Generally, the majority of physicians and patients seem to prefer
infliximab to cyclosporine for severe steroid-refractory UC. If this course
is taken, the patient must understand that there is a 40–75% chance
that infliximab may not work and a colectomy will be required.
Whether the risk of colectomy and IPAA is higher in the setting of
infliximab has not been settled, but most would agree that performing a
two- or three-stage (rather than one-stage) pouch surgery is prudent. It
has been our experience that those steroid-refractory patients not
responding to the week zero and week two doses of infliximab are
unlikely to respond to additional doses and should undergo colectomy.
Until there is a medical cure for UC, several unanswered questions
remain: Are the risks and complications of colectomy higher or lower
than biologic therapy? Is the patient’s quality of life better after
colectomy or biologic therapy? Is the long-term outcome better
with colectomy or biologic therapy? ■
1. Penna C, Dozois R, Tremaine W, et al., Pouchitis after ileal pouch-anal anastomosis for ulcerative colitis occurs with increasedfrequency in patients with associated primary sclerosingcholangitis, Gut, 1996:38(2):234–9.
2. Olsen KO, Juul S, Berndtsson I, et al., Ulcerative colitis: femalefecundity before diagnosis, during disease, and after surgerycompared with a population sample, Gastroenterology,2002;122(1):15–19.
3. Akram S, Ingle SB, Dhillon S, et al., Incidence of post-surgicalcomplications among ulcerative colitis (UC) patients (Pts): Apopulation-based study, Am J Gastroenterol, 2007;102(S2):S480.
4. Thompson HC, Meissner B, Rahman MI, et al., Increasedhealthcare utilization following colectomy in ulcerative colitis,Am J Gastroenterol, 2007;102(S2):S435.
5. Thompson HC, Eisenberg D, Bala M, Rahman MI, Patient reportedquality of life following surgery in ulcerative colitis, Am JGastroenterol, 2007;102(S2):S436.
6. Rutgeerts P, Sandborn WJ, Feagan BG, et al., Infliximab forinduction and maintenance therapy for ulcerative colitis, N Engl JMed, 2005;353(23):2462–76.
7. Sandborn WJ, Rutgeerts P, Feagan BG, et al., Infliximab reducescolectomy in patients with moderate-to-severe ulcerative colitis:
Analysis from ACT I and ACT2, Am J Gastroenterol, 2007;102(S2):S479.
8. Feagan BG, Reinisch W, Rutgeerts P, et al., The effects of infliximabtherapy on health-related quality of life in ulcerative colitispatients, Am J Gastroenterol, 2007;102(4):794–802.
9. Jarnerot G, Hertervig E, Friis-Liby I, et al., Infliximab as rescuetherapy in severe to moderately severe ulcerative colitis: arandomized, placebo-controlled study, Gastroenterology,2005;128(7):1805–11.
10. Regueiro M, Curtis J, Plevy S, Infliximab for hospitalized patientswith severe ulcerative colitis, J Clin Gastroenterol, 2006;40(6):476–81.
11. Lichtiger S, Present DH, Kornbluth A, et al., Cyclosporine in severeulcerative colitis refractory to steroid therapy, N Engl J Med,1994;330(26):1841–5.
12. Van Assche G, D’Haens G, Noman M, et al., Randomized, double-blind comparison of 4 mg/kg versus 2mg/kg intravenouscyclosporine in severe ulcerative colitis, Gastroenterology,2003;125(4):1025–31.
13. Campbell S, Travis S, Jewell D, Ciclosporin use in acute ulcerativecolitis: a long-term experience, Eur J Gastroenterol Hepatol,2005;17(1):79–84.
14. Ogata H, Matsui T, Nakamura M, et al., A randomized dose findingstudy of oral tacrolimus (FK506) therapy in refractory ulcerativecolitis, Gut, 2006;55(9):1255–62.
15. Fellermann K, Tanko Z, Herrlinger KR, et al., Response of refractorycolitis to intravenous or oral tacrolimus (FK506), Inflam Bowel Dis,2002;8(5):317–24.
16. Plevy S, Salzberg B, Van Assche G, et al., A phase I study ofvisilizumab, a humanized anti-CD3 monoclonal antibody, in severesteroid-refractory ulcerative colitis, Gastroenterology, 2007;133(5):1414–22.
17. Creed TJ, Probert CS, Norman MN, et al.; BASBUCINVESTIGATORS, Basiliximab for the treatment of steroid-resistantulcerative colitis: further experience in moderate and severedisease, Aliment Pharmacol Ther, 2006;23(10):1435–42.
18. Van Assche G, Sandborn WJ, Feagan BG, et al., Daclizumab, ahumanized monoclonal antibody to the interleukin 2 receptor(CD25), for the treatment of moderately to severely activeulcerative colitis: a randomized, double blind, placebo controlled,dose ranging trial, Gut, 2006;55(11):1568–74.
19. Feagan BG, Greenberg GR, Wild G, et al., Treatment of ulcerativecolitis with a humanized antibody to the a4b7intergrin, N Engl JMed, 2005:352(24):2499–2507.
regueiro.qxp 15/4/08 11:08 Page 53

The Society of Gastroenterology Nurses and Associates, Inc.—The ‘Gold Standard’ of the Gastroenterology Nursing Profession
In 1969 Marna L Schirmer, a registered nurse (RN), was assisting
gastroenterologists with procedures at Mount Sinai Hospital Medical Center
in New York. Determined to expand her knowledge and keep abreast of the
latest technologies and techniques, Schirmer attended educational meetings
of the professional association for gastrointestinal (GI) physicians: the
American Society for Gastrointestinal Endoscopy (ASGE). Seeing a number of
other nurses in attendance, Schirmer realized the time was right for an
organization dedicated to the gastroenterology and endoscopy nursing
profession. It is due to Schirmer’s concerted efforts that the Society of
Gastroenterology Nurses and Associates, Inc. (SGNA) was formed and held its
first annual meeting in 1974.
In three decades, the SGNA has grown from fewer than 100 to more than
8,000 members, 88% of whom are licensed practicing nurses (LPNs), 5% of
whom are technicians, and 7% of whom are affiliates, including vendors,
managers, and consultants. These nursing professionals and associates
share diagnostic techniques, collaborate on research projects, develop
educational curricula for other professionals, and further their own learning
in the field. Their collective efforts help to advance the safe and effective
practice of gastroenterology and endoscopy nursing.
SGNA is the only national association for GI nursing and sets high standards
for the profession through the position statements it publishes. Viewed as
the ‘gold standard’ in the industry, the SGNA’s position statements cover
topics such as the role of GI RNs in the management of patients undergoing
sedated procedures, the performance of GI manometry studies and
provocative testing, the role of the nurse/associate in the placement of the
percutaneous endoscopic gastrostomy (PEG) tube, role delineation of
assistive personnel, and role delineation of the advanced practice nurse in
gastroenterology/hepatology and endoscopy. A complete list of SGNA
position statements can be found at www.sgna.org
Joining the SGNA helps GI nurses enhance their professional growth and
prepare for the future. With 62 regional societies, members can become
active in SGNA close to home. The regional societies host meetings,
conferences, and special programs, giving members the opportunity to earn
continuing education contact hours while networking with like-minded
peers. In addition to regional societies, members benefit from the
opportunity to take part in 17 electronic special interest groups
(e-SIGs). The e-SIGs allow members to share experiences within a
sub-specialty and, because interaction is online, members have the luxury of
participating when it is most convenient for them. Members of
e-SIGs receive online access to new and archived newsletters, the e-SIG
discussion forum, and the opportunity to meet in person each year at the
SGNA Annual Course. Belonging to an e-SIG offers excellent networking
possibilities, in addition to the opportunity to stay at the cutting edge of new
technologies, standards, and practices. The current SGNA e-SIGs are: advanced
practice, ambulatory GI practice, associates, capsule endoscopy, endoscopic
ultrasound, endoscopic retrograde cholangiopancreatography (ERCP),
hepatology, laboratory management, legislative, LPNs/licensed vocational
nurses (LVNs), manometry, nurse endoscopist, pediatric, pulmonary, research,
university and VA (Veterans Affairs medical centers) nurses.
The society’s website (www.sgna.org) features a wealth of information and
resources tailored to the interests and needs of GI nurses and associates.
Members can search the membership directory and resource guide, which
provides a complete listing of members and their practice affiliations. This is
the only national directory of nurses and associates involved in
gastroenterology and endoscopy nursing. As an exclusive service to
members, all professional resources and practice reference materials are
available at a discount of 50% or more. The website features an
employment network that highlights employment opportunities in GI
nursing settings across the country and the ability to post résumés for
employers to view.
Gastroenterology Nursing is the SGNA’s acclaimed journal, which contains
reports from the front-line of nursing. Peer-reviewed articles, editorial, and
case reports help nurses to improve the quality of patient care and stay up-
to-date with new procedures and therapies, pharmacology, SGNA
guidelines, and more. Published six times a year, Gastroenterology Nursing
is one of the many benefits of membership and offers resource and product
reviews, as well as continuing education opportunities. Members also
receive a subscription to SGNA News, a monthly print publication that
includes course information, meeting dates, and leadership and board
updates. Past issues of SGNA News are archived online for future reference.
For late-breaking news and updates that need to be communicated quickly,
SGNA provides e-Scope, a monthly electronic newsletter delivered directly
to members via e-mail.
SGNA’s Annual Course is the premier educational and networking event for
GI nurses and associates and draws delegates from around the world. The
2008 course will be held in Salt Lake City, Utah on May 16–21, and will
offer attendees the opportunity to earn up to 42 contact hours. The
Annual Course is designed to provide the kind of continuing education
members need and want—whether they are new to the field or seasoned
‘veterans.’ Optional pre-course sessions are available on May 16–18, with
concurrent and general sessions being held May on 18–21. Education is
provided in the following topic areas: advanced practice, ambulatory/
office, associate/technician, experienced nurse, management, pediatric,
pulmonary, and research.
Experienced GI nurses may choose to obtain national certification in the
specialty by satisfying specific practice requirements and successfully
completing a written examination based on the extensive role delineation
research study, which defines areas of practice and sets the blueprint for the
exam. The test is administered by the American Board of Certification for
Gastroenterology Nurses (ABCGN), which is an independent non-
governmental agency established in 1986. Certified RNs earn the certified
gastroenterology registered nurse (CGRN) diploma and LPNs/LVNs earn the
certified gastroenterology nurse (CGN) credential. The certification
recognizes professional achievements and promotes excellence in the
specialty. The major goal of the program is to establish a high standard of
competency among healthcare professionals employed in gastroenterology
and endoscopy nursing. More information about the ABCGN and the
certification exam can be found at www.abcgn.org ■
54 © T O U C H B R I E F I N G S 2 0 0 8
Association Focus
SGNA_book.qxp 11/4/08 03:15 Page 54
SGNA | Your Gateway to Opportunity36th Annual Course | May 15 –20, 2009 | St. Louis, Missouri
Visit www.sgna.org for themost up-to-date information.
T H E P R E M I E R E V E N T F O R G I A N D E N D O S C O P Y N U R S E S A N D P R O F E S S I O N A L S
SGNA_ad.qxp 7/4/08 04:39 Page 55












![Coupling discrete elements and micropolar continuum ...civil.colorado.edu/~regueiro/publications/...[Regueiro and Yan, 2010] that retains an “open window” compu tationally on the](https://img.pdfslide.us/doc/110x75/611236c163470671bf355222/coupling-discrete-elements-and-micropolar-continuum-civil-regueiropublications.jpg)
















