Embed Size (px)
Citation preview

Principle of Vaccinology
Elham Ahmadnezhad MD. MPH. PhD Student of Epidemiology
Farshid fayyaz Jahani MD. MPH. Specialist in Infectious Disease & Tropical Medicine
Tehran University of Medical SciencesTehran University of Medical Sciences
10/10/2011 Vaccinology. 1

Brief History of Lecturers
• Elham & Farshid from Tehran, Iran are couple since 3 years ago
(2008). Farshid graduated from Medical School in Infectious disease
and Tropical medicine’ specialist and Elham now senior student in PhD
of Epidemiology.
• They have common interest in infectious disease epidemiology then
developed some lecturers such as this (Vaccinology).
Hope it’s useful for all target groups.Our Email:
10/10/2011 Vaccinology. 2

OUTLINE
Introduction & Definition
Vaccination policy option
Mass Vaccination
Surveillance System of Vaccination
Vaccine Development
Vaccine Evaluation
Vaccine Safety
Reporting Immunizations
Reliable Web sits
Vaccine Training Course
Review of National Immunization Coverage
10/10/2011 Vaccinology. 3

What is Vaccine
• Dictionary (Dorland 30Dictionary (Dorland 30thth edition 2008) edition 2008)
Attenuated or killed microorganisms or proteins derived from them, administered for
the prevention, treatment, or amelioration of infectious diseases
• WikipediaWikipedia
A vaccine is a biological preparation that improves immunity to a particular disease. A
vaccine typically contains an agent that resembles a disease-causing microorganism, and
is often made from weakened or killed forms of the microbe. The agent stimulates the
body's immune system to recognize the agent as foreign, destroy it, and "remember" it,
so that the immune system can more easily recognize and destroy any of these
microorganisms that it later encounters.
10/10/2011 Vaccinology. 4

What is Vaccinology?
• Vaccinology is the science of developing
vaccines to prevent diseases
10/10/2011 Vaccinology. 5

Vaccines-Historical Perspective• 7th century7th century- Indian Buddhists' drank snake venom to protect against snake bite.
• 10th century10th century- Variolation to prevent smallpox in China and Turkey.
• Early 1700sEarly 1700s- Variolation introduced into England.
• 1760-701760-70- The Jennerian era.
• 1875-19101875-1910- Dawn of Immunological Science.
• 1910-301910-30- Early bacterial vaccines, toxins and toxoids.
• 1930-501930-50- Early viral vaccines: yellow fever and Influenza.
• 1950-19701950-1970- The tissue culture revolution: poliomyelitis, measles, mumps and rubella.
• 1970-19901970-1990- Dawn of the molecular era: hepatitis B, Streptococcus pneumonia, Hemophilus influenza B.
• TodayToday- Glycoconjugate vaccines, rotavirus vaccine, human papilloma virus vaccine and herpes zoster
vaccine.
10/10/2011Vaccinology. 6

Aims of Immunisation Programmes
• To protect those at highest risk (selective immunisation strategy) or• To eradicate, eliminate or control disease (mass immunisation strategy)
Currently, it is estimated that vaccination saves the lives of 3 million3 million children a year
• EradicationEradication Infection (pathogen) has been removed worldwide e.g. smallpox
• EliminationElimination Disease has disappeared from one area but remains elsewhere e.g. polio, measles
• ControlControl Disease no longer constitutes a significant public health problem e.g. neo-natal tetanus
10/10/2011 Vaccinology. 7

Vaccines Achievements1
• With sanitation and nutrition, vaccines are hailed as one of the most
important public health achievements of the 20th century.
• The history of vaccinology lends itself to discussion of its progress in
terms of periods or eras, in which new advances were made.
• Once only targeted against serious childhood diseases, vaccinology has
become a tool for preventing infectious diseases or their complications
and outcomes in all age groups.
• This has seen the number of vaccine-preventable diseases rising to around
26.10/10/2011 Vaccinology. 8

Vaccines Achievements2
• “At the end of the 20th century the US Centers for Disease
Control and Prevention (CDC) cited vaccination as the
number one one public health achievement of that century”
• “The elimination in 1977 of smallpox as a human disease
must rank as oneone of the major achievements of modern
medicine”
10/10/2011 Vaccinology. 9

The Ideal Vaccine
• Immunogenic
• Long lasting immunity
• Safe
• Stable in field conditions
• Combined
• Single dose
• Affordable (and accessible) to all
10/10/2011 Vaccinology. 10

Categorization of Current Vaccines
• Live attenuated: Viruses (oral polio, measles, mumps, rubella,
yellow fever), Bacteria (BCG, cholera)- Long lasting immunity, very
fragile (cold chain), mutation to pathogenicity
• Killed Vaccines: Viruses (hep. A, Salk polio) Bacteria (pertussis,
cholera)-intermediate immunity, several doses may be required
• Sub-unit vaccines incl: Toxoids: (tetanus, hep b.,occellular
vaccines), Conjugate polysacaride vaccines linked with suitable
carrier proteins (Hib). Also single or polyvalent vaccines.
10/10/2011 Vaccinology. 11

Viral Vaccines
10/10/2011 Vaccinology. 12

Bacterial Vaccines
10/10/2011 Vaccinology. 13

Target Fungal Vaccines
10/10/2011 Vaccinology. 14

Target Parasitic Disease
• Malaria
• Trypanosomiasis
• Leishmaniasis
• Toxoplasmosis
10/10/2011 Vaccinology. 15

Selective Vaccination
• Vaccine given specifically to those at increased risk of disease:
• High risk groupsHigh risk groups e.g. Pneumococcal vaccine
• Occupational riskOccupational risk e.g. Hepatitis B, influenza
• TravellersTravellers e.g. Yellow fever, rabies, meningitis
• Outbreak controlOutbreak control e.g. Hepatitis A. vaccine, measles
10/10/2011 Vaccinology. 16

Pipelines for Developing Countries
Much needed vaccines for the developingdeveloping world• Malaria• Tuberculosis• HIV• Hookworm• Dengue• Enterotoxigenic Escherichia coli• Shigella
10/10/2011 Vaccinology. 17

More Possibilities• Therapeutic vaccines: Identification of specific tumor
antigens provide immune targets for which immunogenic
vaccines may conceivably be designed. Examples: Leukemia
Breast cancer
Melanoma
Prostate cancer
Colon cancer
• Vaccines against autoimmune diseases
10/10/2011 Vaccinology. 18

Similarities between Vaccines and other Drug
• Vaccines are also medicines
• Potential for adverse effects
• Multiple ingredients
• Potential for interaction with disease and other
medicines
• Also need to comply with standards of safety, efficacy
and quality
10/10/2011 Vaccinology. 19

Vaccination Policy Options
10/10/2011 Vaccinology. 20
Eradication Activities New Vaccine Introduction
Outbreak vs. routine control of epidemic diseases
?
Newer Vaccine Research and Development

Role of disease burden studies in the development and Role of disease burden studies in the development and introduction of new and underutilized vaccinesintroduction of new and underutilized vaccines
Disease-Burden StudiesDisease-Burden Studies
Disease Epidemiology• Geographical distribution• Age groups• Seasonality, risk factors
Vaccine Design
Clinical Evaluation• Study sites• Vaccination schedules & Strategies
Vaccine Utilization• Target groups• Impact• Cost-effectiveness
10/10/2011 Vaccinology. 21

Mass Vaccination
Objective: Objective: Make hosts resistant to infection without
having to experience disease
10/10/2011 Vaccinology. 22

Impact of Mass Vaccination Programmes
• Reduce sizesize of susceptible population
• Reduce numbernumber of cases Reduce risk of infection in population
Reduce contact of susceptible to cases
Lengthening of epidemic cycle -> honeymoon phase
Increase in mean age of infection
10/10/2011 Vaccinology. 23

No Mass Vaccination
10/10/2011 Vaccinology. 24
Each host in contact with infected host becomes infected (with a certain probability)

Mass Vaccination
10/10/2011 Vaccinology. 25
Outbreak attenuated (or averted) by lack of susceptible hosts

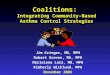
Impact of Mass Immunisation Programme
Annual measles notifications & vaccine coveragePoland 1960-2000
0.0
100.0
200.0
300.0
400.0
500.0
600.0
Year 1964 1969 1974 1979 1984 1989 1994 1999
Year
Cas
es/1
00 0
00
0
10
20
30
40
50
60
70
80
90
100
Imm
un
isation
coverag
e (%)
Vaccination at 12-15 mo Vaccination at 6 years Cases /100 000
10/10/2011 Vaccinology. 26

Surveillance of Vaccine Preventable Disease
• Vaccine uptake
• Vaccine effectiveness
• Serological surveillance
• Adverse events
• Knowledge and attitudes
• Vaccine uptake
• Disease incidence
10/10/2011 Vaccinology. 27

Objectives of SurveillanceVaccine Preventable Diseases
• Pre-implementationPre-implementation
Estimate burden
Decide vaccination strategy
• Post implementationPost implementation Monitor impact and effectiveness
• Nearing eliminationNearing elimination Identify pockets of susceptible
Certification process
10/10/2011 Vaccinology. 28

Disease Incidence• Main sources of dataMain sources of data
Statutory notification
Laboratory reporting
Death registrations
• Other sourcesOther sources
Hospital episodes
Sentinel GP reporting
Paediatric surveillance
10/10/2011 Vaccinology. 29

Measles Case Definitions
• Suspect caseSuspect case Rash and fever
• Probable caseProbable case Rash, fever, and either: cough, coryza or conjunctivitis
• Laboratory confirmedLaboratory confirmed• Saliva/serum IgM positive
10/10/2011 Vaccinology. 30

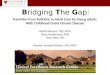
Predictive Value of Notified MeaslesEffect of Change in Incidence
10/10/2011 Vaccinology. 31
1
10
100
1000
10000
100000
1000000
Pre-vaccine Low coverage High coverage Near elimination
Num
ber o
f cas
es
0%
20%
40%
60%
80%
100%
PV+
Non-measles Genuine measles

Surveillance of Vaccine Coverage• Vaccine distributed• Vaccine administered Sampling population assessment e.g. Cluster
Total population assessment (administrative)
Number of doses of vaccine given/used Total (target-)population
10/10/2011 Vaccinology. 32

Use of Administrative Coverage Data
• Usually total population
• Monitor trends over time
• Look for pockets of poor coverage
• Compare with disease epidemiology
• Estimate vaccine effectiveness
10/10/2011 Vaccinology. 33

Steps on Vaccine Development1
• Recognize the diseasedisease as a distinct entity
• Identify etiologicetiologic agent
• Grow agent in laboratorylaboratory
• Establish in animal model animal model for disease
• Identify an immunologic correlate immunologic correlate for immunity to the disease- usually
serum antibody
• InactivateInactivate or attenuateattenuate the agent in the laboratory- or choose antigens
• Prepare candidatecandidate vaccine following GOOD manufacturing Procedures
• Evaluate candidatecandidate vaccine(s) for ability to protect animals
10/10/2011 Vaccinology. 34

Steps on Vaccine Development2
• Prepare protocolprotocol(ss) for human studies
• Apply to MCC for investigational New drug (IND)
approval
• Phase I Phase I human trials- Safety and immugenicity,
dose response
• Phase II Phase II trials- Safety and immugenicity
• Phase III Phase III trials- Efficacy
10/10/2011 Vaccinology. 35

Steps on Vaccine Development3
• Submit Product LicensureLicensure Application MCC approval
• Advisory CommitteesCommittees review and make recommendations
• Marketing Post- Licensure Surveillance for safety and effectiveness
(Phase IVPhase IV)
• Long and ComplicatedComplicated process
Usually takes 1010-1515 years
ManyMany vaccine candidates fail for every success
Costs: $$ 100100- $$ 700700 million per successful vaccine
10/10/2011 Vaccinology. 36

Vaccine Evaluation
Pre-licensingRandomised, Blinded, Controlled Clinical Trials
Vaccine efficacy: Protective Effect under
Idealised Conditions
RCT: controlled experiments, simple interpretation
Post-licensing Observational Studies
Vaccine effectiveness: Protective Effect under
Ordinary Conditions of a public health programme
prone to bias, more complex interpretation
10/10/2011 Vaccinology. 37

Efficacy, Effectiveness, Impact and Herd Immunity
•Efficacy is the direct protection to a vaccinated individual as estimated from clinical trial
•Effectiveness is an estimate of the direct protection in a field study post licensure.
•Herd Immunity is an indirect effect of vaccination due to reduced disease transmission.
•Impact is the population level effect of a vaccination programme. This will depend on
many factors such as vaccine coverage, herd immunity and effectiveness.
10/10/2011 Vaccinology. 38

Basic Calculation of VE % reduction in attack rate of disease in vaccinated (ARV)
compared to unvaccinated (ARU) individuals
VE (%) = (ARU-ARV) X 100 ARU
Where
and
Consequently, VE = 1-RR (preventive fraction)
10/10/2011 Vaccinology. 39
ARU
ARU1
ARV
ARURR

0,9 – 0,2
0,9 VE = = 78%
Vaccinated
IV = 2/10 = 0,2
IU = 9/10 = 0,9
Unvaccinated
Basic Calculation of VE
10/10/2011 Vaccinology. 40

Methods to Assess VE• Pre-licensure:
Randomised control trial (RCT)
• Post-licensure:
Observational/Field investigation • Screening method
• Cohort study
• Household contact study
• Case-control study10/10/2011 Vaccinology. 41

Observational study: Screening Method
• Used with Routine Surveillance Data Take population vaccine coverage (PPVPPV)
Compare with coverage in cases (PCVPCV)
VE = 1 - PCV x (1-PPV) (1-PCV) x PPV
10/10/2011 Vaccinology. 42

Observational study: Screening Method
10/10/2011 Vaccinology. 43
Relationship between VE, PPV and PCV
0
0.2
0.4
0.6
0.8
1
0.5 0.6 0.7 0.8 0.9 1
Proportion of population vaccinated
Pro
po
rtio
n o
f ca
ses
vacc
inat
ed
VE=60%
VE=80%VE=90%
VE=95%

Potential Pitfalls....
• Case definition;
• Vaccine history;
• Case ascertainment;
• Comparability of vaccinated/unvaccinated groups.
10/10/2011 Vaccinology. 44

Methodological Issues: Case Definition1
• Lower specificity: Case definition based only on clinical
criteria may result in false-positive diagnoses
ARV > ARU
VE (%) = (ARU-ARV) X 100 ARU
artificial reduction in VE
10/10/2011 Vaccinology. 45

Methodological Issues: Case Definition2
Changes in MUMPSMUMPS vaccine effectivenessCase definition
Diagnosis by school nurseARV 18% (12/67) 89 ARU 28% (77/272) 25% (68/272)VE 37% 52%
Kim Farley et al 1985 AJE
10/10/2011 Vaccinology. 46

Changes in MUMPSMUMPS vaccine effectivenessCase definition
Diagnosis by school nurse Parotitis > 2 daysARV 18% (12/67) 12% (8/67)ARU 28% (77/272) 25% (68/272)VE 37% 52%
Kim Farley et al 1985 AJE
10/10/2011 Vaccinology. 47
Methodological Issues: Case Definition2

Methodological issues: Vaccine History Ascertainment
• Avoid misclassification of vaccination status
• Equal effort to confirm vaccination status
amongst cases and non-cases Vaccination histories should be documented using GP, clinic,
hand-held or computer records
Persons with missing vaccination records should be excluded
10/10/2011 Vaccinology. 48

Vaccine effectiveness: Post licensure monitoring of VE
Post-licensure: maintenance of VE • Problems in vaccine delivery
Cold chain failure, schedule violation, n° of doses, vaccine strain substitution
• Epidemiological factors
Pathogen changes
• Methodological bias
Selection bias, confounding, chance effects
• Low protective efficacy
Bad batch, different target population, alternative patterns of use, vaccine
strain used
10/10/2011 Vaccinology. 49

Summary of VE• Multiple sources of data are valuablevaluable to
evaluate vaccine programmes
• Source of data and case definitions change
with stagestage of vaccination programme
• Monitoring VE is integral
• VE can be carefully estimated from routineroutine
data
10/10/2011 Vaccinology. 50

Let’s GO An Example
10/10/2011 Vaccinology. 51

A Randomized, Controlled Experiment
• 400,000 elementary school students
participated in the experiment.
• 200,000 chosen at random from 400.000 in
the treatment group got the vaccine.
• The remaining 200,000 in the control group
did not get the vaccine.
10/10/2011 Vaccinology. 52

A Randomized, Controlled Double-Blind Experiment
• The 200,000 children in the control got a fake
vaccination called a placebo.
• The children and their parents were not told if
they got the real vaccine or not.
• Even the doctors and nurses didn’t know; only
the statisticians knew
10/10/2011 Vaccinology. 53

Experimental Results
Looks promising but is it significant?
10/10/2011 Vaccinology. 54
Size Rate
Treatment 200,000 28
Control 200,000 71
Total 400,000 99

Analysis: The Devil’s Advocate
• Let’s play the devil’s advocate. Let’s assume
the vaccine has no effect.
• Then the 99 cases of polio were split into the
two groups purely at random.
• Is it very likely only 25 fall in the treatment
group?
10/10/2011 Vaccinology. 55

A Probability Model
• Put 400,000 balls in an urn with 99 black and the rest white.
• Draw 200,000 (for the treatment group) and count the
number of black balls.
• What is the chance of a split as extreme or more extreme
than 28 in the treatment group and 71 in the control group.
• About one in a billion
10/10/2011 Vaccinology. 56

Calculating Probabilities• A statistician relies on the theory of probability to
calculate probabilities.
• The number of black balls X in the treatment group
follows the hypergeometric distribution.
•
10/10/2011 Vaccinology. 57
99 399901
200000
400000
200000x x

Conclusion: Get vaccinated!
• We must reject the hypothesis that the treatment has no
effect; otherwise we must believe we are incredibly
unlucky.
• We can therefore recommend mass vaccination.
• We also note a vaccination does not prevent polio. Your
best protection is to get vaccinated and encourage
everyone to be vaccinated.
10/10/2011 Vaccinology. 58

Vaccine Safety
10/10/2011 Vaccinology. 59

Today’s Agenda
• The Good
The benefits of vaccination
Ongoing safety monitoring
• The Bad
Vaccines “rocky” past
Acceptable risk?
• And the Ugly
Wealth of misinformation
Vaccine refusal
10/10/2011 Vaccinology. 60

Vaccines Work
JAMA 2007 298(18)2156-2163MMWR August 22, 2008 903-913
10/10/2011 Vaccinology. 61

Pre-licensure Safety Monitoring1
10/10/2011 Vaccinology. 62

Pre-licensure Safety Monitoring2
• Vaccine Adverse Event Reporting System (VAERS)
Limitations
• Vaccine Safety Datalink (VSD)
Established in 1990 by CDC and 8 HMOs
Database on 8.8 million lives
10/10/2011 Vaccinology. 63

Safety Monitoring -Who looks at all that data?
Institute of Medicine (IOM)• Part of the National Academy of Science• Non-profit, non-governmental organization, volunteer• Provide the CDC, NIH and congress on data interpretation on matters of
bio-medical science• IOM Vaccine Safety Reports – The “Gold Standard” in vaccine safety
analysis MMR and Autism (2001) Thimerosal and Neurodevelopmental Disorders (2001) Multiple Immunizations and Immune Dysfunction (2002) HepB Vaccine and Demyelinating Neurological Disorders (2002) SV40 Contamination of Polio Vaccine and Cancer (2002) Influenza vaccines and Neurological Complications (2003) Vaccines and Autism (2004)
10/10/2011 Vaccinology. 64

The Bad
• The Cutter IPV incident (1955)
• Vaccine associated paralytic polio
• Swine flu vaccine and GBS (1976-7)
10/10/2011 Vaccinology. 65

The Cutter Incident
• 1950s Jonas Salk pioneering work with IPV
• 5 companies stepped forward to manufacture IPV
after licensure
• Cutter (the smallest) made a bad batch 100,000 children injected with live virus
70,000 got mild polio
200 were permanently paralyzed
10 died
10/10/2011 Vaccinology. 66

Vaccine-Associated Paralytic Polio(VAPP)
• OPV is a live attenuated virus
• 1 out of 2.4 million doses VAPP
• 1997 a IPV/OPV schedule
• 2000 an all IPV schedule recommended
10/10/2011 Vaccinology. 67

“Swine Flu” vaccine of 1976-1977
• Increased risk of Guillain-Barré syndrome (GBS)
• Risk period was 6-8 weeks after vaccine and most
>25 yrs of age
• Incident of 1 per 100,000
• Above the background rate of 0.87 per million
persons in a 6 week period
10/10/2011 Vaccinology. 68

“Acceptable” Risk?• Local side effects
Swelling, redness
• Systemic side effects
Fever, pain, allergic reaction
• MMR and Thrombocytopenia
• MMR(V) and febrile seizures
• Adolescent vaccines and syncope
• Guillain-Barré and MCV4
10/10/2011 Vaccinology. 69

MMR & Thrombocytopenia
• Yes
• 1 in 40,000 at 12-23 months
• Less common than after natural disease
Journal of Autoimmunity 2001 16: 309-18
10/10/2011 Vaccinology. 70

MMR(V) & Febrile Seizures
• 10% develop fever after 1st MMR dose
• Febrile Seizure Risk
4 cases / 10,000 doses MMR + V
9 cases / 10,000 doses MMRV
MMWR 2008 57: 258-60
10/10/2011 Vaccinology. 71

Syncope and Adolescent Vaccines
MMWR May 2, 2008 / 57(17);457-460
10/10/2011 Vaccinology. 72

Guillain-Barré Syndrome and MCV4
• MCV4 (Menactra®) licensed in Jan 2005
• Sept 2005 alert by FDA/CDC:
2.5 million doses
5 cases of GBS in month following vaccine (VAERS data)
10/10/2011 Vaccinology. 73

and the Ugly
• Wealth of misinformation
MMR and Autism
Mercury poisoning
Vaccines overwhelming the immune system
• Vaccine refusal
10/10/2011 Vaccinology. 74

ReportingReporting ImmunizationImmunization RequirementsRequirements
• Documenting administration of vaccine
• Documenting record of immunization
10/10/2011 Vaccinology. 75

Reporting immunization requirements: Documenting administration of vaccine Content
• Name and address of vaccine
• Medicare number
• Date of birth and gender
• Date of administration
• Name and lot number of vaccine
• Name of immunizer
• Other data as required
10/10/2011 Vaccinology. 7676

Reporting immunization requirements: Documenting administration of vaccine Content-Lot Number
3 lot numbers on packaging:
On antigen carton
On adjuvant carton
On shoe box
Document lot numberDocument lot numberon shoe box.on shoe box.
10/10/2011 Vaccinology. 7777

Immunization Practice Standards
• Vaccine management
• Informed consent
• Administration of vaccine
• Documentation
• Anaphylaxis management
• Reporting of adverse events
10/10/2011 Vaccinology. 78

Immunization practice standards: Vaccine management-Storage and handling of vaccine
• Cold chain system
• Control procedure/mechanism/equipmentVaccine fridge
Dialer and data logger
Vaccine coolers
Cold and warm marks or minimum-maximum
thermometers
• Cold chain breach79

Immunization practice standards Informed consent
• Parental consent required for individuals
• less than 16 years old
• Risk vs. benefits (of receiving vaccine or not)
• General info about vaccine and potential side effects
• Ensure info is well understood
• Allow opportunities for questions
• Assess health with screening questions
• Document informed consent
10/10/2011 Vaccinology. 80

Immunization practice standards Informed consent
Screening Questions (Screening Questions (ExamplesExamples))
• Is unwell today?
• Has history of severe life-threatening allergy to
Eggs
Previous dose of the vaccine; or
Any of its components
• Past history of Guillain Barre Syndrome
• Has disease or treatment lowering immunity
• Has severe bleeding disorder
10/10/2011 Vaccinology. 81

Immunization practice standardsAdministration of vaccine
IntramuscularIntramuscular injection injection
IM in vastus lateralis (Birth to 18 months)
IM in deltoid(18 mths and over)
10/10/2011 Vaccinology. 82Source : http://www.health.gov.nl.ca/health/publications/immunization/S4/

ImmunizationImmunization practice standards practice standardsAdministration of vaccine
Post-vaccinationPost-vaccination
• Check
For bruising, redness, swelling
Client for any adverse event
• Instruct client
To wait 15 minutes
Of possible side effects and what to do
To call if adverse event in next 4 weeks
Need for a second dose
10/10/2011 Vaccinology. 83

Immunization practice standards Documentation
• Consent form: Pandemic H1N1 Influenza
Immunization
• Client immunization record
• Adverse event following immunization
• CSDS – as directed
10/10/2011 Vaccinology. 84

Immunization practice standards Anaphylaxis management
• Assess and manage ABCs
• Call for help
• Administer epinephrine
• Call 115
• Repeat dose as needed
• Document and share clinical info
10/10/2011 Vaccinology. 85

8610/10/2011 Vaccinology. 86
Immunization practice standards Immunization practice standards ReportingReporting AEFI - AEFI -
CurrentCurrent surveillance process
• AEFI form to be completed by PH or physician
• Form submitted to RMOH
• PH enters data in CSDS and sends form to CDC
Unit
• CDC Unit faxes form to PHAC
• Refer to NB Immmunization Handbook
Immunizers: inform clients to call PH if severe or unusual reactions in the 4 weeks following
vaccination.

8710/10/2011 Vaccinology. 87
Immunization practice standards Immunization practice standards ReportingReporting AEFI - AEFI -Enhanced severe AEFI surveillance
• AEFI form to be completed by physician
• May be completed by PH when reported to PH first
• Form submitted to RMOH
• PH enters data entered in CSDS and sends form to CDC Unit
• Refer to GNB website for reporting process, case definition and form
http://www.gnb.ca/0053/h1n1/audience_professionals-e.asp

8810/10/2011 Vaccinology. 88
Immunization practice standards Immunization practice standards ReportingReporting AEFI - AEFI -
Enhanced severe AEFI surveillance
Weekly active AEFI reporting
• Internal medicine specialist and neurologists will submit weekly count
of cases meeting case definition of 8 conditions along with DOB and
name to CDC Unit via special email address.
• CDC Unit will send the information to MOH.
• Timely data to be used be regional PH to ensure complete reporting of
AEFI.

• Used injection material
Handling
Disposal
Sharp containers
Where to place
When to replace
How to dispose of
• Needle stick injury – refer to RHA policy
• Use of personal protective equipment and infection control measures
10/10/2011 Vaccinology. 89
Immunization practice standards Immunization practice standards Occupational health issues

Reliable web sites
10/10/2011 Vaccinology. 90

CDC Vaccines and ImmunizationContact Information
• Telephone 800.CDC.INFO
• Email [email protected]
• Website www.cdc.gov/vaccines• Vaccine Safety www.cdc.gov/od/science/iso
10/10/2011 Vaccinology. 91

10/10/2011 Vaccinology. 92

Promote Epidemiology Training & Research
• WHO Advanced Training Course on Immunology, Vaccinology,
and Biotechnology Applied to Infectious Diseases
• Liaison with epidemiology training programmers
INCLEN, FETP, EPIET
• WHO Collaborating Centers
10/10/2011 Vaccinology. 93

References
• Geoffrey A. Weinberg and Peter G. Szilagyi. Vaccine Epidemiology: Efficacy, Effectiveness ,and the Translational Research Roadmap.
The Journal of Infectious Diseases 2010; 201 (11): 1607 -1610
• European Program for Intervention Epidemiology Training. Principle of Vaccinology. 2008
• EPI coverage survey, WHO. Available at: http://www.who.int/immunization_monitoring/routine/EPI_coverage_survey.pdf. Access
date: 10.10.2011
• Geert Leroux-Roels, Paolo Bonanni, Terapong Tantawichien,Fred Zepp. Understanding Modern Vaccines: Perspectives in Vaccinology
Vaccine development. Volume1/ Issue1/ 115-150
• Thomas D. Szucs. Health economic research on vaccinations and immunization practices—an intro uctory primer. Vaccine 23 (2005):
2095–2103
• NB Immunization Handbook, sections IV-III, IV-IV
10/10/2011 Vaccinology. 94