Embed Size (px)
Citation preview

1
The 36 Week Preemie:
Consequences of Late
Preterm Delivery
Eric Reynolds, MD MPH
Associate Professor of Pediatrics
Division of Neonatology
Kentucky Children’s Hospital
About the handout
This handout includes only the most
important slides from the lecture.
It is not intended to follow the lecture
slide-by-slide
Objectives
Scope of the Problem
National
State-Level
UK
Economic and Medical Consequences of
Late Preterm Delivery
Prematurity Facts
Prematurity is the leading cause of infant mortality in industrialized nations (March of Dimes)
Preterm delivery is increasing
Up 30% since 1981 (US)
11.7% in 199615.1% in 2006 (KY)

2
Scope of ProblemHP
KY US 2010
2004 14.4 12.5 7.6
2005 15.2 12.7
2006 15.1 12.8
2007 15.2 12.7MOD Peristats
In an average week in KY…
174 babies are born preterm
26 are very preterm (<32 weeks)…103 are Late Preterm (34-36)
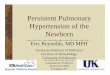
Rising Rate of Prematurity in US:
1997-2007
• National Center for Health Statistics, final natality data.
• Retrieved Feb 24, 2011 from www.marchofdimes.com/peristats.
Percent of Live Births that were Preterm;
(<37 wks) Kentucky, 1997-2007
• National Center for Health Statistics, final natality data.
• Retrieved Feb 24, 2011 from www.marchofdimes.com/peristats.
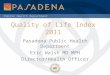
Prematurity by Gestational Age; Kentucky, 2005*
19.760.5
3.92.4
4.9
8.7
<=26
27-28
29-30
31-32
33-34
35-36
*2005 data
**Preterm birth is defined as any live birth occurring <37 completed weeks gestation
Data Source: Kentucky Vital Statistics Files, Live Birth Certificate files, 2005

3
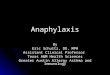
Percent of Live Births that were
Very Preterm (<32 wks) in KY, 1996-2006
• National Center for Health Statistics, final natality data.
• Retrieved Feb 24, 2011 from www.marchofdimes.com/peristats.
Late-Preterm: KY & Nation
• National Center for Health Statistics, final natality data.
• Retrieved Feb 24, 2011 from www.marchofdimes.com/peristats.
Late Preterm % By State (2007)
11
9.29.39.19.9
8.6
9.2
10.5
10.111.4
10
13
11.7
10.1
9
10.7
9.8
9.8
6.5
9.8
Late Prematurity Facts
Late-Preterm infants are:
a majority of NICU admissions
The greatest percentage of NICU patients to receive
respiratory support
the majority of NICU economic costs
often the sickest babies in a NICU
more likely than a full term baby to be rehospitalized in the
first year of life
twice as likely to die in the first year of life as a full term
baby
at risk for long term health issues

4
Definitions
Language used to describe 34-37 week infants
Near Term
Marginally Preterm
Moderately Preterm
Minimally Preterm
Accepted label is now LATE PRETERM
Reflects the fact that these infants have morbidity and
mortality risks more similar to preterm infants than term
infants
Definitions
Gestational ages assigned to Late-Preterm 35-37 34-36 35-36 6/7
Lower limit not defined Nearly all 33 week infants require NICU admission
44-84% of 34 week infants require NICU care
ACOG uses 34 weeks as a critical point for medical decision making for the pregnant woman who is threatening PTL.
Unfortunately, as late as 2006, the IOM still identified terminology as a major hurdle to understanding the problems of prematurity.
Financial Costs
In 2005, the cost of
prematurity in the US
was $26.2 billion. (IOM 2007)
Medical, Educational and Lost
Productivity
In 2004, costs for initial
hospitalization of preterm
infants was $15 billion. Does not include cost of
rehospitalization or long term
problems.
Almost ½ of this goes
to Medicaid.
Medicaid
47.8%
Employer/ Other
Private
46.3%
Other*
3.6%
Uninsured/
Self Pay
2.3%
Financial Costs (KY)
Total NICU charges related to preterm birth was
$204,504,246 for calendar year 2005 with average
charges ranging from $10,919-$88,270 (KY Hospital Discharge Database, 2005)
Total amount paid by KY Medicaid for prematurity
related initial hospitalization stays for calendar year
2005: $7,421,829.49 (KY Medicaid Claims Database, 2005)
Medicaid paid more for the care of babies 35-36 weeks
then it did for babies <26 weeks.
All less than 26 = $1,375,179.58
35-36 weeks = $1,748,349.17

5
Semin Perinatol
Feb 2006;30(1)
April 2006;30(2)
Risk of Chronic Disease
Barker Hypothesis
LBW and increased risk for:
Coronary artery disease
Insulin resistance
Length of Stay
More Late Preterm infants had delayed discharge
term infants.
Not statistically significant, not powered for this outcome
Reasons: Jaundice 8 vs 1
Resp Dist 8 vs 2
Poor Feeding 22 vs 2
Other 12 vs 2
Total 50 vs 7
Wang Pediatrics 2004;114:372-376
Rehospitalization
Late Preterm infants are more likely than a full term baby to be rehospitalized in the first year. 2.4%: >40weeks
3.4%: 38-40weeks
6.3%: 35-37weeks
Reasons Jaundice, Feeding difficulty, Dehydration, others
Male > Female
Mixed results from studies of early discharge
Escobar Semin Perinatol 2006;30(1):28-33 Escobar Pediatrics 1999;104:1-9
Escobar Arch Dis Child 2005;90:125-131 Oddie Arch Dis Child 2005;90:119-124

6
Temp Instability
The Late Preterm infant is more likely than term infants to have temperature instability 10% vs 0% in term (OR infinite)
Wang et al. Pediatrics 2004;114:372-376
Due to Immature epidermis
Higher ratio of surface area to birthweight
More frequent delivery room interventions
If untreated, infant can loose 2-3 C in the first 30 minutes
Hypoglycemia
What’s Normal?
20, 30, 36, 40, 45, 47, 60, 55-100 (mg/dL)
No data on long-term effects of moderate
hypoglycemia (47) on Late Preterm infants
Risk to earlier preterm infants (30.5 + 2.7 weeks) has
been established
Late Preterm more likely to have hypoglycemia
15.6% vs 5.3% (OR 3.3, CI 1.1-12.2)
10-15% in other studies
Lucas Br Med J 1988;297:1304-1308
Wang Pediatrics 2004;114:372-376
Laptook, Jackson Semin Perinatol 2006;30(1):24-27
Poor Feeding
The Late Preterm infant is more likely to
require intravenous infusion
26.7% vs 5.3% (OR 6.48, CI 2.27-22.91)
Reasons:
Hypoglycemia, poor feeding, dehydration
Wang Pediatrics 2004;114:372-376

7
Poor Feeding
The rhythms of suck, swallow and breath are
being integrated into coordinated feeding
from 32-37 weeks.
Most babies have mastered feeding coordination
by 35 weeks,
But some have not
76% of Late Preterm with “poor feeding” had
delayed discharge vs 28.6% of term infants. >48 hours post-vaginal delivery / 96 post c-section
Wang Pediatrics 2004;114:372-376
Post-Discharge Nutrition
Breast is best
Term vs Premie Follow-up formula
Factors affecting nutritional needs
BW <1000 gm*
Discharge Wt <1850 gm*
Serum Prealbumin <10mg/dL*
Growth <2SD or 5th percentile*
Big babies get term formula, Small ones get premie
follow-up formula
BPD*
Osteopenia*
Chronic disease
Limited or decreased intake
*Nutritional Care of High-Risk Newborns, 3rd edition,
Groh-Wargo et al eds. Precept Press, Chicago, 2000
Hyperbilirubinemia
Late Preterm more likely to have jaundice
54.4% vs 37.9% (OR 1.95,
CI 1.04-3.67)
Delayed discharge (1 term vs
8 Late Preterm)Wang Pediatrics 2004;114:372-376
Infants discharged from normal
newborn nursery at <38weeks
have an OR >7 of being
re-admitted for hyperbilirubinemiaMaisels Pediatrics 1998;101:995-998
Hyperbilirubinemia
Subcommittee on Hyperbilirubinemia Pediatrics 2004;114;297-316

8
Sepsis/Sepsis Work-ups
Late Preterm infants more likely to undergo
sepsis evaluation
36.7% vs 12.6% (OR 3.97, CI 1.82-9.21)
More likely to be treated with 7 day course
of antibiotics
No difference in actual culture proven sepsis
Wang Pediatrics 2004;114:372-376
Length of Stay (Days)
64
71
32
49
12
37
8
24 21
54
0
10
20
30
40
50
60
70
80
<28
weeks
28-32 33-36 >36 Total
Not Infected
Infected
Abdu A, et al. (Abstract) J Invest Med. 2009;57(1):387.
Structural Neurologic
Complications
86/1011 (9%) had a report of a neurological complication: IVH, grades I-II 29
HIE/prolonged seizures 30
Other 7
Coma 6
IVH, grades III-IV 6
Brain atrophy 4
Intracranial infarct 2
Brain death 2
Clark RH J Perinatol 2005;25:251-257

9
Two-Year Follow-up
Late Preterm Infants Have Worse 24-Month
Neurodevelopmental Outcomes Than Term Infants
Studied 7500 (6300 term and 1200 late preterm)
Bayley exams at 24 months
Late preterm infants:
had lower MDI (85 vs. 89) and PDI (88 vs. 92) (p<0.0001).
were more likely to have severe or mild mental or
psychomotor delay.
were more likely to have MDI <70 (but not PDI)
Lower MDI was associated with modifiable social
factors. GA was largest contributor to lower PDI.Woythaler et al, Pediatrics 2011;127:e622-e629
Respiratory Failure
Late Preterm more likely to have
respiratory distress
28.9% vs 4.2%
(OR 9.14, CI 2.9-37.8)
Wang Pediatrics 2004;114:372-376
Primary Diagnosis
437, 43.3%
33, 3.3%
32, 3.2%
31, 3.1%
24, 2.4%
98, 9.7%84, 8.3%
72, 7.1%
41, 4.1%
63, 6.2%
40, 4.0%
24, 2.4%14, 1.4% 11, 1.1%
6, 0.6%
RDS
MAS
Pneumonia / sepsis
Surgical support
Major GI anomaly
Primary Dx unknown
TTN
Heart disease
PPHN
HIE
CDH left-sided
Aspiration syndrome
Lung hypoplasia - not CDH
Major neuro anomaly
CDH right-sided
Clark RH 2006

10
TTN
Delayed Transition
Usually benign respiratory condition that does not usually require mechanical ventilation
About 4% of pulmonary diagnoses in Clark’s study
“Malignant” TTN syndrome(Keszler‘92)
Predilection for PPHN following elective c-section
Clark J Perinatol 2005 Apr;25(4):251-7
Respiratory Distress Syndrome
Incidence is inversely related to GA
Surfactant deficiency or dysfunction, epithelial injury, and vascular protein leak
Primary problem is loss of FRC and deflation stability
Most common pulmonary diagnosis in patients >34 weeks
Safe lung recruitment is essential to the prevention of acute lung injury
Clark J Perinatol 2005 Apr;25(4):251-7
Pneumonia
Associated chorioamnionitis
Most common is GBS
Difficult to distinguish from RDS
Can be associated with shock
Acute lung injury and inflammation inhibit surfactant function
Clark RH 2006
PPHN
Suprasystemic
pulmonary vascular
resistance causes right
to left shunting
at the FO and/or PDA
CXR - clear
Very wide swings in
PaO2
1-4% of live births
Actual incidence is
difficult to ascertain
Clark RH 2006

11
Air Leaks
Includes:
Pneumothorax
Pneumopericardium
Pneumomediastinum
PIE
Assymptomatic PTX in
1% of routine x-rays
Association with MAS
Decreased incidence in
surfactant treated
patients
Meconium Aspiration Syndrome
10–15% of deliveries have MSAF
Only 1/20 develop MAS
9.7% of pulmonary diagnosis in Clark’s study
Historically, the most common indication for ECMO
Pathophysiology: “check valve” obstruction, air trapping, PPHN, andsurfactant inactivation
Clark RH 2006
Clark J Perinatol 2005 Apr;25(4):251-7
Congenital Diaphgragmatic Hernia
Incidence 1:4000 births
Left side most common
Severe PPHN is common
Mortality approximately 40–50% even with ECMO support
Not specific to Late Preterm infants, but carries higher mortality in this group
Chronic Lung Disease
10% develop chronic lung disease
16% on ventilators at 30 days or discharge
77 / 945 (8%) of survivors discharged on O2
Most common pulmonary diagnosis leading to
CLD is RDS
Clark RH J Perinatol 2005;25:251-257

12
Late Preterm and RSV
Preterm infants are at increased risk for severe
RSV disease.
Interrupted lung development
34 week infant at 52% of the lung volume of a term infant.
Decreased maternally-transmitted antibody levels
32-35 week infants have mean serum IgG levels 43%
lower than that of term infants.
Welsman LE. Pediatr Infect Dis J. 2003;22(2 suppl):S33-S39
Colin A. Pediatrics 2010;126:115-128
Lanston C. Am Rev Respir 1984;129:607-613
Yeung CY. Lancet. 1968;1(7553):1167-1170
Rare Complications
Apnea and Bradycardia Not found in term babies, only rarely in late preterm
Necrotizing Enterocolitis (NEC) Associated with other markers of compromised perfusion
Cerebral Palsy Associated with chorioamnionitis (11% attributable risk)
Increased risk for SIDS
Neonatal Death
Wang Pediatrics 2004;114:372-376
Solutions are not easy!
Some babies are going to be preterm
PTL with advanced dilation
34 week mom with proteinuria, hypertension, headache and
abdominal pain.
Balancing the risk of prolonging a high-risk pregnancy to
32-36 weeks versus neonatal cost and complications
For some babies mortality/morbidity may or may not be
less if the pregnancy is continued to term
Culture of litigation and practice of defensive medicine
C-section on Demand
Power of Education and
Commitment
Labor Induction Process Improvement: A patient
Quality-of-Care InitiativeJM Fisch et al. Obstetrics & Gynecology 2009;113(4):797-803
Over a 4 year period:
Decreased overall inductions from 24.9% to 16.6%
Decreased elective inductions from 9.1% to 6.4%
Decreased elective inductions before 39 weeks from
11.8% to 4.3%
Decreased frequency of C-section among
nulliparous women from 34.5% to 13.8%
Pitt

13
Power of Education and
Commitment
Decreasing Elective Deliveries Before 39
Weeks of Gestation in an Integrated Health
Care SystemBT Oshiro et al. Obstetrics & Gynecology 2009;113(4):804-811
Elective delivery before 39 weeks decreased from
28% to 10% in 6 months.
Intermountain Health
Conclusions
Late Preterm infants represent a large portion of what
we do in the NICU.
Late Preterm infants have morbidity and mortality
statistics more similar to preterm infants than term
babies.
“Even with appropriate size and favorable Apgar scores [Late-
Preterm] infants have significantly more documented medical
problems when compared to term babies”.
Despite recent modest improvements, late preterm
infants are a major public health problem in Kentucky
and the US.
Good News
Preterm Birth Rate Drops Three Percent
Fewer Babies Face Health Risks of an Early Birth
WHITE PLAINS, N.Y., APRIL 6, 2010- The nation's preterm birth
rate dropped for the second consecutive year.
The preterm birth rate dropped to 12.3 percent, according to the
report, "Births: Preliminary Data for 2008," which was released
today by the National Center for Heath Statistics. That's down from
the 2007 preliminary rate of 12.7 percent. The declines follow a
more than 20 percent increase in the preterm birth rate between
1990 and 2006.
The March of Dimes says 79 percent of the decline in the preterm
birth rate occurred among late preterm babies.
http://www.marchofdimes.com/peristats/whatsnew.aspx?id=39&dv=wn
Acknowledgments
Susan DeGraff
MOD
Peristats
http://www.marchofdimes.com/peristats
Healthy Babies are Worth the Wait
http://www.prematurityprevention.org