Embed Size (px)
DESCRIPTION
Preventing Hospital Acquired Infections The Physician’s Role. Shruti Gohil, MD, MPH Susan Huang, MD, MPH Linda Dickey, RN, CIC, MPH Epidemiology & Infection Prevention. Dawn of A New Era: Accountability, Transparency, and Best Practices. - PowerPoint PPT Presentation
Citation preview

Preventing Hospital Acquired Preventing Hospital Acquired InfectionsInfections
The Physician’s RoleThe Physician’s Role
Shruti Gohil, MD, MPHShruti Gohil, MD, MPHSusan Huang, MD, MPHSusan Huang, MD, MPH
Linda Dickey, RN, CIC, MPHLinda Dickey, RN, CIC, MPHEpidemiology & Infection PreventionEpidemiology & Infection Prevention

Dawn of A New Era:Dawn of A New Era:Accountability, Transparency, and Best Accountability, Transparency, and Best PracticesPractices
National concern over National concern over healthcare quality and healthcare quality and patient safetypatient safety
Rising healthcare costsRising healthcare costs
Centers for Medicare and Centers for Medicare and Medicaid Services (CMS) Medicaid Services (CMS) considering financial considering financial penaltiespenalties
– Restricted Restricted reimbursementsreimbursements
– Penalties for HAIsPenalties for HAIs
Delivery System Reform Delivery System Reform Incentive Payments Incentive Payments (DSRIP)(DSRIP)

Healthcare Associated Infections Healthcare Associated Infections (HAIs): (HAIs): A National PriorityA National Priority
Major Morbidity and Major Morbidity and MortalityMortality– 1.7 million HAIs annually1.7 million HAIs annually– 99,000 deaths annually99,000 deaths annually
CostlyCostly– Annual direct medical Annual direct medical
costs: $28.4 - $33.8 costs: $28.4 - $33.8 billion billion (CDC)(CDC)
Average duration of Average duration of inpatient admissions has inpatient admissions has decreased while HAI decreased while HAI frequency has increased*frequency has increased*
*Burke JP. N Engl J Med. 2003 Feb 13;348:651–6.
Stone PW, et al, Am J Infect Control. 2002 May;30(3):145–52.

Types of HAIsTypes of HAIs
Central Line Associated Central Line Associated Bloodstream Infections Bloodstream Infections (CLABSI)(CLABSI)
Catheter Associated Catheter Associated Urinary Tract Infections Urinary Tract Infections (CAUTI)(CAUTI)
Ventilator Associated Ventilator Associated Events (VAE)Events (VAE)
Surgical Site Infections Surgical Site Infections (SSI)(SSI)
C.difficile C.difficile InfectionsInfections

Multidrug Resistant Organisms Multidrug Resistant Organisms (MDROs)(MDROs)
Within 48 hours of admission, patient’s Within 48 hours of admission, patient’s flora changes to match that of the flora changes to match that of the hospitalhospital
Patient risk of HAIs increases with Patient risk of HAIs increases with acquisition of MDROsacquisition of MDROs
Main way to acquire MDROs is viaMain way to acquire MDROs is via Health care worker transmissions Health care worker transmissions EnvironmentEnvironment
A cluster of MDROs is a signal for A cluster of MDROs is a signal for hospital transmission to patientshospital transmission to patients

CRE – Carbapenemase CRE – Carbapenemase Resistant Resistant EnterobactericeaeEnterobactericeae
Most commonly KlebsiellaMost commonly Klebsiella Resistant to most antibacterialsResistant to most antibacterials Mortality rates up to 50%Mortality rates up to 50% Rampant on the East Coast, now spreading to WestRampant on the East Coast, now spreading to West UCI EIP trying to prevent the organism from gaining UCI EIP trying to prevent the organism from gaining
foothold herefoothold here

What is a Cluster?What is a Cluster?
Two or more cases of a relatively uncommon event or disease related in time and/or place greater than expected by chance
MICU – 4 Clusters in 2012, 3 of them VRE last ending December– Now with repeat cluster, Jan /Feb 2013
3T – 5 clusters in 2011, 4 of them VRE– Now with repeat cluster Jan/Feb 2013

Clusters by UnitClusters by Unit2011 thru 20122011 thru 2012

What is Special About What is Special About MICU and 3 Tower?MICU and 3 Tower?
3T sees the highest patient turnover 3T sees the highest patient turnover in patient admissions, discharges, in patient admissions, discharges, and transfersand transfers
MICU accepts a lot of transfers from MICU accepts a lot of transfers from 3T and admits high risk patients from 3T and admits high risk patients from all areas of hospital and communityall areas of hospital and community

Clusters by OrganismClusters by Organism2011 thru 20122011 thru 2012

Genetic Fingerprinting Genetic Fingerprinting
PFGE TestingPFGE Testing Highly specific and sensitiveHighly specific and sensitive Identifies single strains between Identifies single strains between
patients or local environmentspatients or local environments PFGE performed on isolates PFGE performed on isolates
from:from: Patients identified as part of unit Patients identified as part of unit
cluster.cluster. Results will show patterns to be Results will show patterns to be
different vs indistinguishabledifferent vs indistinguishable

MICU Cluster PFGE MICU Cluster PFGE ResultResult

Neighboring RoomsNeighboring Rooms
•Room
24
•Room 26
•Room 25

PFGE InterpretationPFGE Interpretation
Patient 1 VRE present on admissionPatient 1 VRE present on admission 2 days later neighboring patient (Patient 2) 2 days later neighboring patient (Patient 2)
positive with the genetically same organism positive with the genetically same organism – Develops line infection one week laterDevelops line infection one week later– Eventually ExpiresEventually Expires
2 weeks later, Patient 3 becomes positive with 2 weeks later, Patient 3 becomes positive with genetically same organismgenetically same organism
Pattern of VRE positivity in relation to time and Pattern of VRE positivity in relation to time and location best consistent with a combination of location best consistent with a combination of healthcare worker transmission and healthcare worker transmission and environmental transmissionenvironmental transmission

3 Tower PFGE Result3 Tower PFGE Result

Common RoomCommon Room

PFGE InterpretationPFGE Interpretation
Patient 1 - VRE present on admissionPatient 1 - VRE present on admission Resided in 3T B19 for 4 daysResided in 3T B19 for 4 days 5 days AFTER this Patient 1’s departure, the 5 days AFTER this Patient 1’s departure, the
next patient in 3T B19 is admittednext patient in 3T B19 is admitted Another 5 days later, the Patient 2 is Another 5 days later, the Patient 2 is
screened for VRE and is found to have screened for VRE and is found to have genetically same strain as Patient 1 genetically same strain as Patient 1
The pattern of VRE positivity in relation to The pattern of VRE positivity in relation to time and room location are best consistent time and room location are best consistent with with environmental transmissionenvironmental transmission

Prevention StrategiesPrevention Strategies
Hand Hygeine (HH)Hand Hygeine (HH) Personal Protective Equipment (PPE)Personal Protective Equipment (PPE) Isolation PrecautionsIsolation Precautions Bundling procedure kitsBundling procedure kits CLABSI PreventionCLABSI Prevention CAUTI PreventionCAUTI Prevention Surgical Site PreventionSurgical Site Prevention Chlorhexidine Daily BathingChlorhexidine Daily Bathing Environmental CleaningEnvironmental Cleaning Equipment/instrument Disinfection/SterilizationEquipment/instrument Disinfection/Sterilization Injection/Procedure SafetyInjection/Procedure Safety
Highest Yield, Lowest Cost
Intervention for Prevention of ALL
Healthcare Associated Infections


The Data for Hand Hygiene and The Data for Hand Hygiene and Personal Protective Equipment:Personal Protective Equipment:
Reduces acquisition of multidrug resistant Reduces acquisition of multidrug resistant organismsorganisms1,2,3,4,91,2,3,4,9
Reduces transmission of organismsReduces transmission of organisms5,6,105,6,10
– To patientsTo patients– To environmentTo environment
Reduces healthcare associated infectionsReduces healthcare associated infections6,7,8,106,7,8,10
– CLABSI and CAUTI ratesCLABSI and CAUTI rates– C. difficile C. difficile ratesrates– Surgical Site InfectionsSurgical Site Infections
1. Sanderson, PJ et al, J Hosp Infect 1992;21:85-93
2. McFarland, LV et al, NEJM 1989;320:204-10
3. Samore, MH et al, Am J Med;1996;100:32-40
4. Ojajarvi, J , J Hyg 1980;85:193-203.
5. Pittet, D, et al, Lancet ID 2006;6(10):641-652.
6. Pittet, D, et al, Lancet 2000;356:1307-12
7. Larson EL, et al, Behav Med 2000;26:14-22
8. Allegranzi, B et al, J Hosp Infect 2009;73(4):305-315
9. Puzniak, L., et al, Clinical Infectious Diseases 2002, July 1:35
10. Mangini, E., et al, Infection Control and Hosp Epi, Nov 2007;28 :11(1261-66)

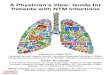
Ubiquitous BacteriaUbiquitous Bacteria

Kramer A. BMC Infectious Diseases 2006;6:130

Joint Commission Joint Commission ExpectationsExpectations
Will conduct direct observationsWill conduct direct observations– Hand HygieneHand Hygiene– Personal Protective Equipment Personal Protective Equipment
Prior citationsPrior citations– Phones used without changing gloves, no Phones used without changing gloves, no
cleaningcleaning– Gowns not worn or worn half onGowns not worn or worn half on– HH lapses observed among staff, medical HH lapses observed among staff, medical
students, and physicians (e.g., Anesthesia)students, and physicians (e.g., Anesthesia)
How are we faring at UCI currently?How are we faring at UCI currently?

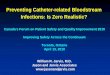
Hand Hygiene Adherence at Hand Hygiene Adherence at UCIUCI
MD staff consistently MD staff consistently below goalbelow goal– Nursing Staff >90% Nursing Staff >90%
compliancecompliance
Chronic problemChronic problem
2012

Personal Protective Personal Protective Equipment Equipment Adherence at UCIAdherence at UCI
Attending MD compliance Attending MD compliance 60%60%– Nadir 20% in one quarterNadir 20% in one quarter
Medical student Medical student compliance previously only compliance previously only 25% now improving25% now improving
2012

Most common infractions:Most common infractions:– No use of PPENo use of PPE– PPE half on, half offPPE half on, half off
Other issues:Other issues:– Use of phone or pager Use of phone or pager
while in precautionswhile in precautions
2012
Personal Protective Personal Protective Equipment Equipment Adherence at UCIAdherence at UCI

Call to Action:Call to Action: Culture Culture ChangeChange
Pattern of chronic underperformance Pattern of chronic underperformance by MDs requires a new approachby MDs requires a new approach
Responsibility for HH/PPE is not that of Responsibility for HH/PPE is not that of the Hospital, Infection Prevention, the Hospital, Infection Prevention, CMS, or Joint CommissionCMS, or Joint CommissionIt is a contract between each MD and the It is a contract between each MD and the patientpatient

MD ChampionsMD Champions

How to be a ChampionHow to be a Champion
““Doctor, I noticed you didn’t wash your Doctor, I noticed you didn’t wash your hands”hands”a) “Thanks for caring to let me know”a) “Thanks for caring to let me know”b) “I just did, but I’ll do it again - thank you”b) “I just did, but I’ll do it again - thank you”c) “Thanks for the reminder. I’ll do it right c) “Thanks for the reminder. I’ll do it right
now.”now.”
Keeping others accountable..Keeping others accountable..a)a)Remind students Remind students b)b)Remind one anotherRemind one anotherc)c)““Everybody wash and gown up”Everybody wash and gown up”d) “Remember… d) “Remember… C. diff C. diff – soap and water”– soap and water”

Clean Your ThingsClean Your Things
StethoscopesStethoscopes– After every useAfter every use– Alcohol or CaviwipesAlcohol or Caviwipes– Contact precaution roomsContact precaution rooms
White CoatsWhite Coats– Wash frequentlyWash frequently– Visibly cleanVisibly clean
Items You Use on PatientsItems You Use on Patients– Site Right, GlucometerSite Right, Glucometer
High touch (pagers, phones)High touch (pagers, phones)– Wipe at least dailyWipe at least daily
Use gloves

Case: Anesthesia and OR Hand Case: Anesthesia and OR Hand HygieneHygiene
Problem: CMS Citation for HH non-Problem: CMS Citation for HH non-adherence in ORadherence in OR
Solution:Solution:– Patient Safety Vice Chair, Shermeen Patient Safety Vice Chair, Shermeen
Vakharia, MD identified issues specific to Vakharia, MD identified issues specific to workflow/tasksworkflow/tasks
– Implemented intervention: Sprixx Implemented intervention: Sprixx personal hand sanitizerpersonal hand sanitizer
Observed HH efforts still under wayObserved HH efforts still under way– So far, Attending Anesthesiologist HH So far, Attending Anesthesiologist HH
improved from improved from 50% to 70% 50% to 70% in one monthin one month

Case: Medicine Resident Action Case: Medicine Resident Action PlanPlan
Problem: Hand Hygiene among residents low Solution:
– Medicine Residency Director, Lloyd Rucker devised plan that highlights accountability and daily reminders
Morning huddle - Case Manager will remind team daily about the importance of HH/PPE
Hand washing officer of the day selected for each medicine ward team– Observe team during rounds, remind everyone to
comply

Culture Change: Call to Culture Change: Call to ActionAction
Ideas?Ideas?
We can and must do better!We can and must do better!