Embed Size (px)
Citation preview

Presented by: Ivana Oracova, NHS Greater Glasgow and Clyde
Health visitor communication with parents about child obesity concerns atwith parents about child obesity concerns at
the 30 month assessment
Ivana Oracova, Trainee Health PsychologistNHS Greater Glasgow and ClydeNHS Greater Glasgow and Clyde
BackgroundBackground• In 2010, over 20% of 4-5 year olds in Scotland were
overweight or obese – In Glasgow ~ 1 in 25 2.5 year olds will be identified as
b t th 30 th tobese at the 30 month assessment• Prevention and timely management of preschool obesity
important for decreasing risk of obesity and chronicimportant for decreasing risk of obesity and chronic illness later in child’s life
• Health visitors have a unique position to support parents• Health visitors have a unique position to support parents with both prevention and management of child obesity:– yet we know little about their experiences whenyet we know little about their experiences when
communicating with parents about children’s weight (Mikhailovich & Morrison, 2007)
BackgroundBackground• Australia:
Edvardsson et al (2009)o HVs (N=10) - preschool obesity difficult to raise, especially if parents also
overweight: denial, defensiveness and excuses common reactionsLaws et al (2009)( )o HV Survey (N=56) – 22% never or rarely used growth charts - possibly
reflecting a reluctance to raise the issue with parents/lack of confidence?• Sweden: Regber et al (2013)• Sweden: Regber et al (2013)
o HVs (N=15) - BMI charts used inconsistentlyo obesity is sensitive, but parents prefer for their children to be slightly
heavier • UK: Redsell et al (2012)
o HVs (N=30) - talked about their role in advising parents about diet buto HVs (N 30) talked about their role in advising parents about diet but did not formally identify or intervene with larger infants
AimsAims• to describe experiences of health visitors in Scotland when
communicating and raising children's overweight with parents at the 30 month assessment
• to explore whether health visitors experience different communication challenges when raising the issue ofcommunication challenges when raising the issue of children's overweight compared to raising speech and language concernslanguage concerns
MethodsMethods• In depth semi-structured interviews (purposive sampling)
with 19 health visitors (HVs) (18 females)• Data collected between May and September 2016• 8 HVs (42%) interviewed in person, 11 via telephone• 10 HVs (47%) were from the North West, 9 from the North
E t A f GlEast Areas of Glasgow– differences between areas in availability of preschool
weight management interventionsweight management interventions• Average interview length: 44 minutes
Analysis: StagesAnalysis: Stages1. Data collection and initial data analysis
All interviews audio recorded– All interviews audio recorded– cyclical process: initial analysis of the data informed subsequent data
collection - interview schedule slightly modified in light of emerging findings– theoretical sampling: data collected until saturation was reachedtheoretical sampling: data collected until saturation was reached
2. Data preparation – All interviews were transcribed verbatim
» Familiarisation with data to obtain general sense of materialg» All data are currently being imported to QSR N’Vivo 11 software
3. Final data analysis – Thematic content analysis using an interpretative, inductive approachy g
» Analysing and reviewing transcripts, identifying and coding for categories and themes from the data
» Data similar in meaning clustered together G th i l f h th f th t t» Gathering examples of each theme from the text
– 20-25% of interviews will be independently coded by second coder
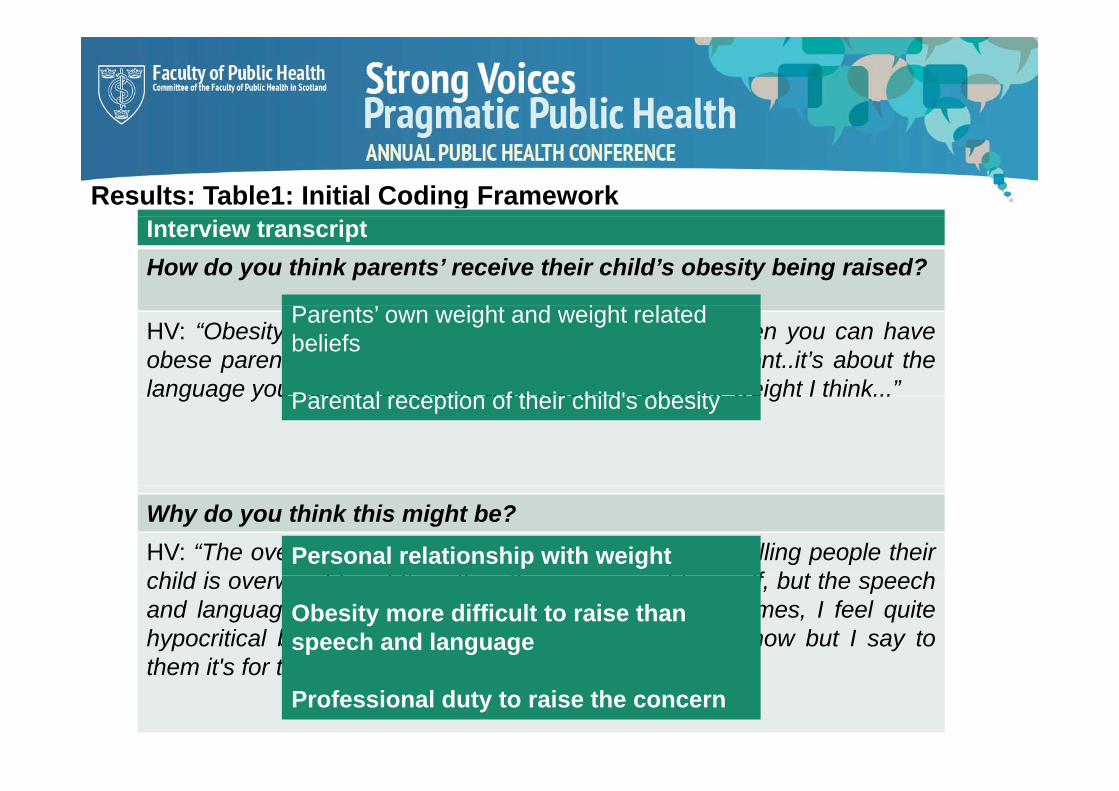
Results: Table1: Initial Coding Framework Interview transcriptHow do you think parents’ receive their child’s obesity being raised?
P ’ i h d i h l dHV: “Obesity is more difficult to raise because quite often you can haveobese parents... I think its about being honest and upfront..it’s about thelanguage you use...everyone is a bit touchy about their weight I think...”
Parents’ own weight and weight related beliefs
P t l ti f th i hild' b itlanguage you use...everyone is a bit touchy about their weight I think...Parental reception of their child's obesity
Why do you think this might be?HV: “The overweight is...a personal thing ... I don’t like telling people theirhild i i ht d I’ itti th i ht lf b t th h
Personal relationship with weightchild is overweight and I’m sitting there overweight myself, but the speechand language I’ve not got a problem with that…Sometimes, I feel quitehypocritical because I'm...I've not done it myself you know but I say tothem it's for their own good
Obesity more difficult to raise than speech and language
them it s for their own goodProfessional duty to raise the concern
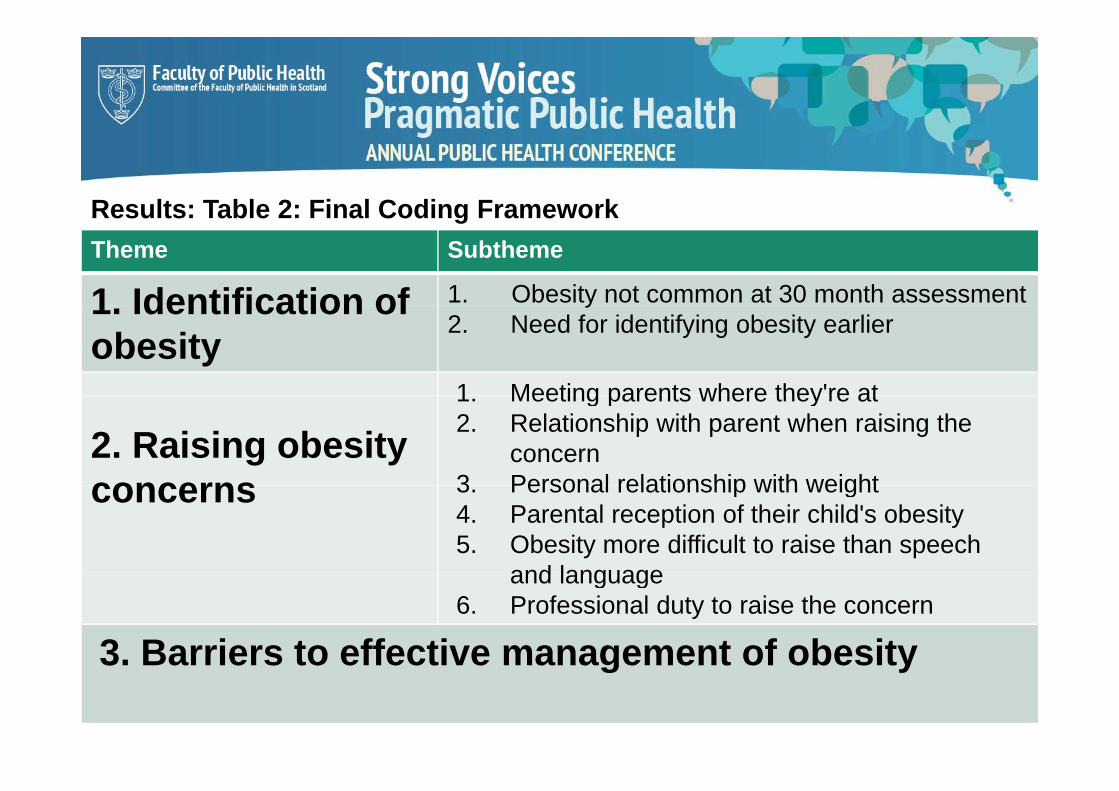
Results: Table 2: Final Coding FrameworkResults: Table 2: Final Coding FrameworkTheme Subtheme
1 Identification of 1. Obesity not common at 30 month assessment1. Identification of obesity
y2. Need for identifying obesity earlier
1 Meeting parents where they're at
2. Raising obesity concerns
1. Meeting parents where they re at2. Relationship with parent when raising the
concern3 Personal relationship with weightconcerns 3. Personal relationship with weight4. Parental reception of their child's obesity5. Obesity more difficult to raise than speech
and languageand language6. Professional duty to raise the concern
3. Barriers to effective management of obesity3. Barriers to effective management of obesity
Theme 1: Identification of obesityTheme 1: Identification of obesity
• HVs talked about the importance of identifying obesity as• HVs talked about the importance of identifying obesity as early as possible and providing parents with information about healthy diet and recommended physical activity y p y ylevels
• Obesity was identified by measuring the child's height and weight and plotting this onto the centile charts, BMI charts were never or rarely used

1 Obesity not common at 30 month assessment1. Obesity not common at 30 month assessment
“...you would think...there would “...you would think...there would be quite a few but
actually...there's probably more
“...majority of children who are overweight are
picked up before 30 y p yon the other end of the
scale...there are more children who are small and skinny and
picked up before 30 months because there
are other concerns in the household impacting that who are small and skinny and
picky eaters rather than the ones who are overweight”
(HV13)
household impacting that child's world and it’s
usually the thing that's i th t hild t b (HV13)causing that child to be
unhealthy...” (HV6)

2 Need for identifying obesity earlier than at 302. Need for identifying obesity earlier than at 30 months
“I wonder if there is a bit of a gap, I think a lot of the problems start when they go off
baby foods, because they go from taking jars of baby food to eating a sausage
roll with not very much in between I don'troll with not very much in between. I don t know if obesity would be better addressed earlier, before parents get into habits and
ti ” (HV13)routines...” (HV13)
Theme 2: Raising obesity concernsTheme 2: Raising obesity concerns
• Raising obesity concerns to parents is a sensitive topic• Raising obesity concerns to parents is a sensitive topic– needs to be discussed appropriately
• Centile charts - a helpful visual tool– a good 'way in' to raise the concern and an opportunity to ask about a good ay o a se e co ce a d a oppo u y o as abou
diet and activity levels
• Confidence to raise the subject rated to be 7 or higher– However, having years of experience important to navigate these
conversations successfullyconversations successfully
1. Meeting parents at where they are1. Meeting parents at where they are • Use softer/strengths based approach - look at each family in
isolationisolation• Assess parents’ recognition of the issue• Avoid medicalising• Avoid medicalising
“...most parents are quite offended when you broach the subject with th d d d t d bit f d i d th d d
“if you have the parents behind you you can take the back seat
them and you do need to do a bit of dancing around the gardens and soothe and calm the waters with them...(HV11)
if you have the parents behind you, you can take the back seat and give family time to offload and let it sink in, it’s about the containment you need to do in the beginning...how you would
h it d 't d d th bj t b t th lapproach it doesn't depend on the subject but on the people you're talking to...” (HV6)

2. Relationship with parents when raising obesity2. Relationship with parents when raising obesity concerns
“...the anxiety is the relationship, it's a very sensitive topic for parents...If you ask me how it makes me feel, it feels a bit unpleasant and its anxiety provoking, not majorly...but from a professional perspective this can impact your relationship with the family and they can avoid your appointments... (HV5)
“I think that’s a relationship with the parent, I am confident to raise the b t ti f h th i t i th tconcern, but your perception of how they are going to receive that you
need to be careful... if you haven’t got a relationship you have to be mindful of setting the scene ...“ (HV7)
“...when you are new on the case load you haven’t had time to build a relationship and a lot of people that I am meeting at 30 months, they haven’t met me before ” (HV3)haven t met me before... (HV3)
3. Personal relationship with weight3. Personal relationship with weight
“Th i ht i l “I am not a size 10 myself“The overweight is a personal thing because I don’t like telling people their child is overweight
I am not a size 10 myself so I am very conscious that
you've got to also look h lth t i thi d i ”and I’m sitting there
overweight myself... I feel quite hypocritical because I've
healthy to give this advice…” (HV7)
q ypnot done it myself but I say to them it's for their own good ”(HV6)
.”..we know ourselves that weight is a big issue for usgood... (HV6) weight is a big issue for us as well and it does feel quite personal to have weight commented on ” (HV13)commented on... (HV13)commented on... (HV13)
4 Views on parental reception of their child's4. Views on parental reception of their child s obesity“.. parents are in denial, they think it's just ‘puppy fat’ and they'll grow out of it, they just don't see it as an issue ” (HV12)issue… (HV12)
“[it] may be taken as criticism of not looking after their child properly so they can become quite defensivechild properly, so they can become quite defensive... ‘oh he's big boned’, ‘he doesn't eat very much’...” (HV13)( )(HV13)
“ most parents know if their child is overweight and need to hear it from someone else ” (HV7)and need to hear it from someone else... (HV7)
4 Views on parental reception of their child's4. Views on parental reception of their child s obesity• When asked about any differences in parental reception of obesity versus speech and language concernsversus speech and language concerns....
“.... it is overweight that parents see much more as a failure, because they think they have control over what their child eats, [but not] whether their child speaks, it is something that they perceive they have done...”(HV11)y p y ( )
“... they want their children to be speaking... they are more inclinedto tell you there is a problem with speech and language than obesityand I think it’s all to do with peoples’ perceptions ... because there’sp p p palways been a stigma put to people being overweight...” (HV9)
5 Obesity more difficult to raise than speech5. Obesity more difficult to raise than speech problems
“Obesity is very “Obesity is very personal..I am less
confident with it than
““Obesity is always a bit more difficult to raise because quite often you “I am much more confident with it than
speech because I feel like I am
criticising the
because qu te o te youcan have obese parents... It’s about being honest and upfront
I am much more confident raising speech and lang age
(HV13)
criticising the child's
appearance...”(HV13)
honest and upfront... about the language you use...everyone is a bit touchy about their
language [concerns]because (HV13)(HV13)touchy about their
weight...” (HV8)parents really want their children to talk...” (HV5)

6. Professional duty to raise obesity concerns6. Professional duty to raise obesity concerns“This [raising of obesity] “This [raising of obesity] created a barrier in my“ you have to be discreet but created a barrier in my
relationship with the parent, but it's never t i t b i d
..you have to be discreet but there comes a time and place where you have to be honest abo t it there's too m ch not going to be raised,
its a duty that I have as such...” (HV5)
about it... there's too much going on tip toes and we don't want to offend anybody [but] there's more harm to the child if we don't do something...” (HV12)
“If mum and dad are sitting there “If mum and dad are sitting there and they are enormous, you’re having to touch on them ashaving to touch on them as well...[but] you still have to get the point over, you wouldn’t want to not say anything ”want to not say anything... (HV4)
Theme 3: Barriers to effective management of gobesity
“It i f t ti“We are quite time“I don't think I am a specialist in that, I can identify at early t b t I thi k h th
“It is frustrating that we have interventions, but don't have
“We are quite time restricted so it’s difficult but ...we get support so Istages ..but I think when they
are quite obese they need further help...so I would feel
don't have capacity to deal with people in timely
get support ...so I think we can
manage it to a certain degree butconfident up to a certain
degree...but ...further than that a specialist could be
timely fashion...and if we don't start straight away it takes
certain degree but we get to a point where we need
advice andpmuch more in depth with it...”
(HV12)
away it takes away the cloud...” (HV13)
advice and support from
another team...” (HV3)( )
Theme 3: Barriers to effective management of
“I haven't used any obesity
Theme 3: Barriers to effective management of obesity
“We get confused because services come
and go we have to
I haven t used any obesity interventions but on paper it
[MEND] seems a good and go...we have to
check with each other because there have
b h
intervention...what you have is ...people are looking for quick fixes....but with any been so many changes
and we all feel a bit overwhelmed about what
quick fixes....but with any intervention that asks
parents to commit, t t k t you do and when..”
(HV14)parents are not keen to
engage...” (HV11)
ImplicationsImplications• Prevalence of childhood overweight and obesity estimated to affect
60 illi hild b 2020 (d O i t l 2010)60 million children by 2020 (de Onis et al, 2010)• Supporting HVs and parents with skills for behaviour change
important for prevention of child obesityimportant for prevention of child obesity
Current challenges:Current challenges:• Obesity not common for HVs? (e.g. Isma et al., 2013)• HV guidance focus on other priorities – need for guidelines to place g p g p
stronger emphasis on preschool obesity• Debunking the ‘puppy fat’ myth –support HVs to educate parents
th t ‘P f t’ h lif l h lththat ‘Puppy fat’ can have lifelong health consequences• Reducing stigma of obesity an ongoing challenge for us all
ReferencesReferences• Miklahoilovich, K., & Morrison, P. (2007). Discussing childhood overweight and obesity
with parents: a health communication dilemma. Journal of Child health care, 11, 311.K Ed d D Hö t A R i i i b t hild ’ i ht M t l• K, Edvardsson D, Hörnsten A. Raising issues about children’s overweight - Maternal and child health nurses’ experiences. J Adv Nurs.2009;65(12):2542–51.
• R. Laws, K. J. Campbell, P. van der Pligt, K. Ball, J. Lynch, G. Russell, R. Taylor, et al,Obesity prevention in early life: an opportunity to better support the role of MaternalObesity prevention in early life: an opportunity to better support the role of Maternaland Child Health Nurses in Australia, BMC Nursing, 2015, 14, 1
• Regber S, Mårild S, Johansson Hanse J. Barriers to and facilitators of nurseparentinteraction intended to promote healthy weight gain and prevent childhood obesity atSwedish child health centers. BMC Nursing. 2013;12:27.
• Redsell SA, Swift JA, Nathan D, Siriwardena AN, Atkinson P, Glazebrook C. UK healthvisitors’ role in identifying and intervening with infants at risk of developing obesity.Maternal Child Nutri 2013;9(3):396–408Maternal Child Nutri. 2013;9(3):396–408
• de Onis M, Blössner M, Borghi E: Global prevalence and trends of overweight andobesity among preschool children. Am J Clin Nutr. 2010, 92: 1257-1264.10.3945/ajcn.2010.29786.
• Isma GE, Bramhagen AC, Ahlstrom G, Östman M, Dykes AK. Obstacles to theprevention of overweight and obesity in the context of child health care in Sweden.BMC Family Practice. 2013;14:143.





























