Embed Size (px)
Citation preview

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 1/26
NURUS SA ADAH MOHD FADZIL0616952
AHD 4126:IPD 1Case presentation:UGIB & perinepric abscess

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 2/26
Introduction
Perinephric abscess (PNA) a.k.a perirenal abcess is defined as an abscess(infection) outside therenal capsule .They are rare in comparison to other infections involving the genitourinary tract but they can cause significant morbidity and mortality (Journal International Brazil Urology,2010).
R enal and perinephric abscess formation usually occur in patients with predisposing factors such
as diabetes mellitus, urinary calculi, urinary obstruction and immune compromised patients.Systemic diseases such as DM (46.9%) was much more common than renal or urologic diseasessuch as malignancy (4.1%) or renal stones (10.2%) (Seung Hwan Lee et al.,2010).
U pper gastrointestinal bleeding ( UGIB ) is defined as hemorrhage in the area of upper GI . oftencauses hematemesis (vomiting of blood) or melena (passage of stools rendered black and tarry bythe presence of altered blood) (Manish K Varma,2008) .
GI bleeding is a common complication of duodenal ulcers and can have serious consequences( Alan BR Thomson,2010) .

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 3/26
P reliminary data
Mr W (RN 654381)62/C/maleOccupation : gardenerMarital status : married + 3 childrenFamily background : wife- rubber tapperCaretaker : daughter only available at 7pm
everydayDOR: 22 Sept 2010 : High protein diet
DOA:12 Sept 2010 6.15pm Ward 5C

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 4/26
M edical history
k/c/o:DM (1 year),HPT (10 years),gout
July 2010 : duodenal ulcer& perinephric abcess fromHOSHAS
August : syncopal attack and hemetemesis/melena12 Sept (DOA) : 1. UGIB 2° duodenal ulcer
2. anemia 2° UGIB3. R perinephric abcess

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 5/26
C urrent condition
Melena°/hemetema°Stable & responsive to questionsProblem in memory (day/date)Not accompanied by caretaker but only available at 7pmeveryday
Non-ambulatory RT afraid of pain at PCD drainage site able toeat at semi recumbent position but limited ability to preparefoodPoor appetite RT pain & being selective on certain food RTaltered taste in agingGood dentition & have proper chewing ability

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 6/26
Perinephricabcess
UGIBDU
DM
anemic
Pain
fever Poor oralintake
Candida albicans in immune suppressed and diabetic patients are bacteria found in theabcess (Patterson JE & Andriole VT,1999)
R arely, perinephric abscess may be a presentation of infectious disorders of thegastrointestinal tract. Only two cases GI diorders (ruptured retrocecal appendix &chronic D U ) has been reported( Ching-Tien Kao et al,2002)
Involuntary wtloss
Poor NutritionalStatus
Imm uno-
comp ro m ised

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 7/26
N utritional Status Assessment
Usual BW is 106 .Loss 30 kg (> 10% of UBW). Indication for high risk of malnutrition.
Date Weight (kg) Height (cm) BMI(kg/m²)
IWR (18.5-24.9)
Wt history(kg)
22/9/10 61.3(unfit- IBW )
165(obtained from
patient)
22.5 50.4-67.8kg 6 y.ago-1063month ago- 76
Current-don t know but keep on loosing
Anthropometry
An unplanned wt loss of 10% or more is a risk factorfor malnutrition (Manual of Clinical Dietetics,5 th edition)
8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 8/26
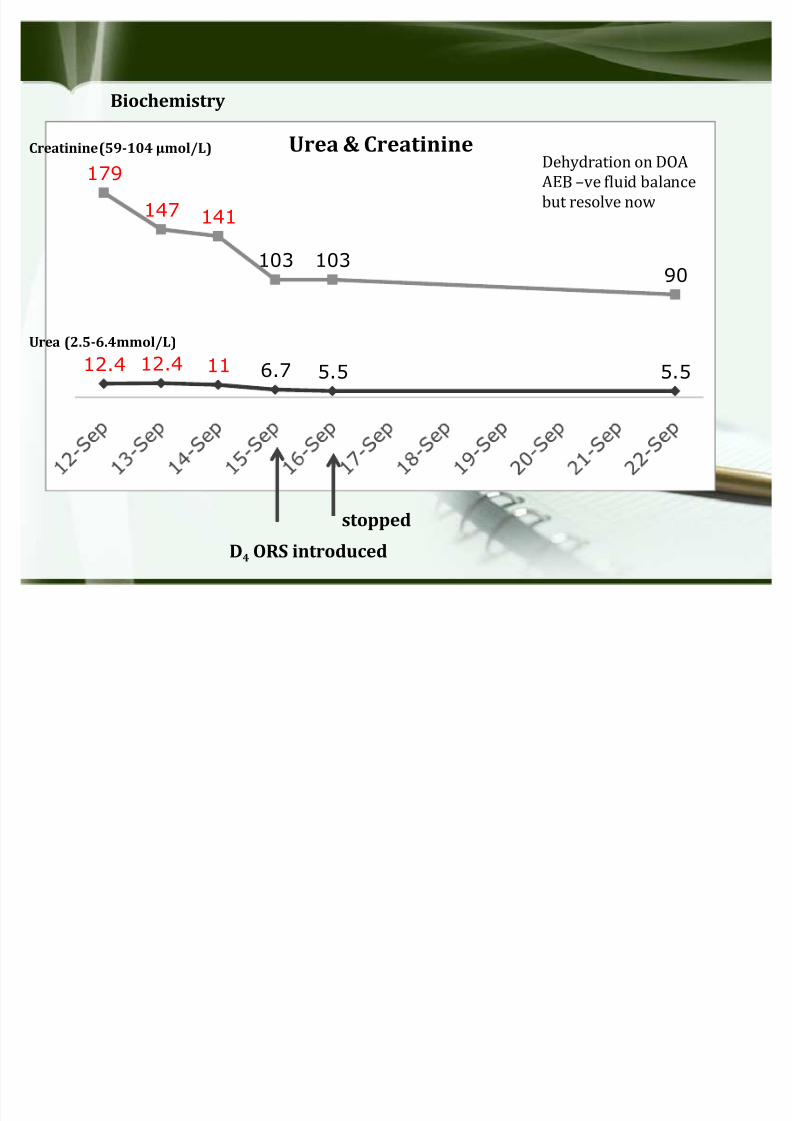
12.4 12.4 11 6.7 5.5 5.5
179
147 141
103 10390
Urea & Creatinine
D4 ORS introduced
Creatinine (59-104 mol/L)
Urea (2.5-6.4mmol/L)
Dehydration on DOAAEB ve fluid balancebut resolve now
Biochemistry
stopped

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 9/26
24
9.4 9.4 9.8 7.4 8.4
42.6
30 30 30 30 30
WBC and Globulin
WBC(4-10X 10 9/L)
Globulin (20-35 gm/L)
IV .Imipenem (anti bact)Infection on DOA(with high T°)but now resolve relatedto mx given

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 10/26
7.38.4 9.5
11.3
8.4 8.3 9.1
H bHb
Hb(13-17g/dL)
2 Platlet Count
T.pentoprazole(antiulcer)Persistent low Hb even undermx(PC& antiulcer) R T anemiccondition+poor intake

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 11/26
17.8 17.8
8.2
3
8.4 8
11.9
10
13
D extrose
Dxt (4-7.8 mmol/L)
Actrapid 2 UActrapid 4 U
Actrapid 3 U
Actrapid stat
Actrapid stopped
Persistently high Dxt evenunder insulin & OAD R Tstress condition

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 12/26
Test (Unit) Normal values* 12/9 Comments
L iver Test function
T.Protein (g/ L ) 66-83 68.2 Normal total
proteinAlbumin (g/ L ) 35-50 25.6 Low albumin
indication of malnutrition AE B wt loss >10% of usual BW +poorintake
T. B ilirubin ( mol/ L ) 0 - 20 19 Normal T. B ilirubin

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 13/26
C linicalVital Signs Normal Values 12/9/10 20/9/10
B P(mmHg) 130/80 120/80 130/80 Normal B P under mx
Temperature (ºC) 37 39 (t.sponging) 37 Fever resolve
I /O Positive balance -110 +550 I mproved into +vebalance
B /O 1x/d (normal to pt) B NO B NO for 8 days Symptom of constipation R T nomotility associated
with disease condition
spo2 100% 98 NP ( R T UGIB ) 99% R A I mproved respiration
Drug (f)
Metformin 500 mg B D OAD
T perindopril 8mg OD anti HPT
T amlodipine 10 mg OD anti HPT
IV imipenem 500 mg B D antibiotic
T pentoprazole 40 mg OD Antireflux/Alleviate ulcer

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 14/26
D ietary (hospital)
M eal time Food items Amt E (k C al) C HO (g) P (g) Fat (g)
BF (8am) Roti +kaya 2 pcs 157.5 37.5 4 6
+sweet coffee (1tbspsugar)
1cup 60 15 - -
L(12pm) White rice ½ exc 37.5 7.5 1 0.25
fish +vegetable soup 1exc 125 - 7 11
papaya 1 slice 60 15 - -
AT(4pm) Roti +kaya 2 pcs 157.5 37.5 4 6
Plain water 1 glass - - - -
Total 112.5 17 23.25
Total (kCal) 727.25 450 68 209.25
% 62 9.3 28.7
8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 15/26
Nutrition Diagnosis
FFQ: no refine sugar /high salt routine but query on why food served hassugar (drinks/kaya). Alcohol °smoke°
No outside food takenPlain water 1.5 L /day taken
Poor appetite½ exc rice during lunch< ½ recommended energy meet by total oral intake
Selective towards H BV protein- Able to finish fish but not chicken since it isclaimed to be lembik . Prefer ayam kampungCan tolerate milk powder & egg.Adequate Fiber (vege& fruit) R T pt s preferenceFaulty believe- cannot take egg to prevent puss & did not take dinner sinceafraid of high blood glucose
Inadequate energy & protein intake R T decreasing appetite AE B Energy intake of 727.25 kcal/d & Protein intake of 17 g/d, less than requirement (energy req~1800(30 kcal/kg BW ) kcal/d & protein req ~67.4 g/d)

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 16/26
Medical Nutrition Therapy

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 17/26
Estimation of energy requirement
Harris-Benedict BEE= 66.47 + 13.75 (Wt) + 5 (Ht) 6.76 ( Age)= 66.47 + 13.75 (61.3) + 5 (165) 6.76 (62)
TEE = BEE x AF x IF AF= 1.1 (confine to bed) IF= 1.2 (mild stress RT high Dxt)
= 1315 x 1.1 x 1.2= 1736 kCal
Quick Method= 30 kCal/kg x IBW= 30 kCal/kg x 61.3 kg= 1839 kCal
RNIMale 60-65 y old= 2010 kcal/d
To plan for 1800 kCal/day menu
Estimation of protein requirement = 1.1-1.2 g/kg x IBW (mild stress RT low alb, poor appetite & drainage procedure)= 1.1-1.2 g/kg x 61.3 kg= 67.4 -73.6g/day
RNI=59 g/d
Intervention

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 18/26
Objective
To provide adequate energy & protein and preserve lean bodymassTo improve macronutrients and micronutrient biochemabnormalities (Dxt)To encourage better quality of life (BO) to promote bowelmotility
PrincipleBy providing high calorie high protein diet and top up withnourishing fluid with:E=1800 kcal/d protein:67.4- 73.6g/d (1.1-1.2g/kgBW)
fluid=1.8L/d (1kcal/ml)
8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 19/26
Implementation1. Encourage orally as much as pt tolerated to meet Energy recommendation by
promoting small & frequent feeding
2. Correct on faulty believeHigh BG RT stress condition prolonged fasting (skip dinner) that lead torebounce hyperglycemiaPuss RT improper hygiene that lead to infection. Egg white is ok to take not yellowcoz yellow have sulphur(worsen the puss)
3. Explain on high protein dietNeed to increase H BV protein intake for early recovery+ boost immunity againstinfection
Encourage to finish fish/chicken(if fish is not possible)/egg provided (ratah lauk)Discuss with cook to provide fish only
4. Discuss regarding LSDD diet to pt and cooksuppose pt should not get kaya bun. Pt must report if order is not correct
5. G lucerna SR as oral supplement according to nurse shift (3 shifts/d).High protein,high calhave fiber for bowel openSR of glucose to alleviate stress induced hyperglycemia
6. Compliment good attitude & motivate changes
Cont current fluid intake for good hydration status & forBO
Motivate movement when there is no pain for bowel motility

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 20/26

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 21/26
M enu planningFULL HO S P ITAL M eal Energy C HO P Fat
BF ± 2pcs White B read + 1 nos egg + 2 tsp margerineL ± 4exc White rice+ 1 exc fried fish + 1exc fruitAT-2pcs White B read + 1 nos egg + 2 tsp margerine
D-4 exc White rice+ 1 exc fried fish + 1 exc fruit
215531215
531
307530
75
111511
15
151915
19Glucerna SR± 2 ½ scp (x3*/d) 278 36 13.5 9.8
Total : 1770 246 65.5 77.8
H ALF HO S P ITAL M eal Energy C HO P Fat
BF ±2pcs White B read + 1 nos egg + 2 tsp margerineL ±2 exc White rice+ ½ exc fried fish + 1exc fruitAT-2pcs White B read + 1 nos egg + 2 tsp margerineD- 2 exc White rice+ ½ exc fried fish + 1 exc fruit
215363215363
30453045
117.5117.5
15171517
Glucerna SR± 6 scps (x3*/d) 666 86.4 32.4 23.4
Total : 1822 236.4 69.4 87.4
LITTLE HO S P ITAL M eal Energy C HO P Fat
BF ±1pcs White B read + ½ nos egg + 2 tsp margerineL ±1 exc White rice+ ½ exc fried fish + 1exc fruitAT-1pcs White B read + ½ nos egg + 2 tsp margerineD- 1 exc White rice+ ½ exc fried fish + 1 exc fruit
185.5291185.5291
15301530
5.55.55.55.5
11.516.511.516.5
Glucerna SR± 6 scps (x4/d) 888 115.2 43.2 31.2
Total : 1841 205.2 65.2 87.4

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 22/26
Monitoring

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 23/26
B iochemical
28
30
Albumin progression
8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 24/26
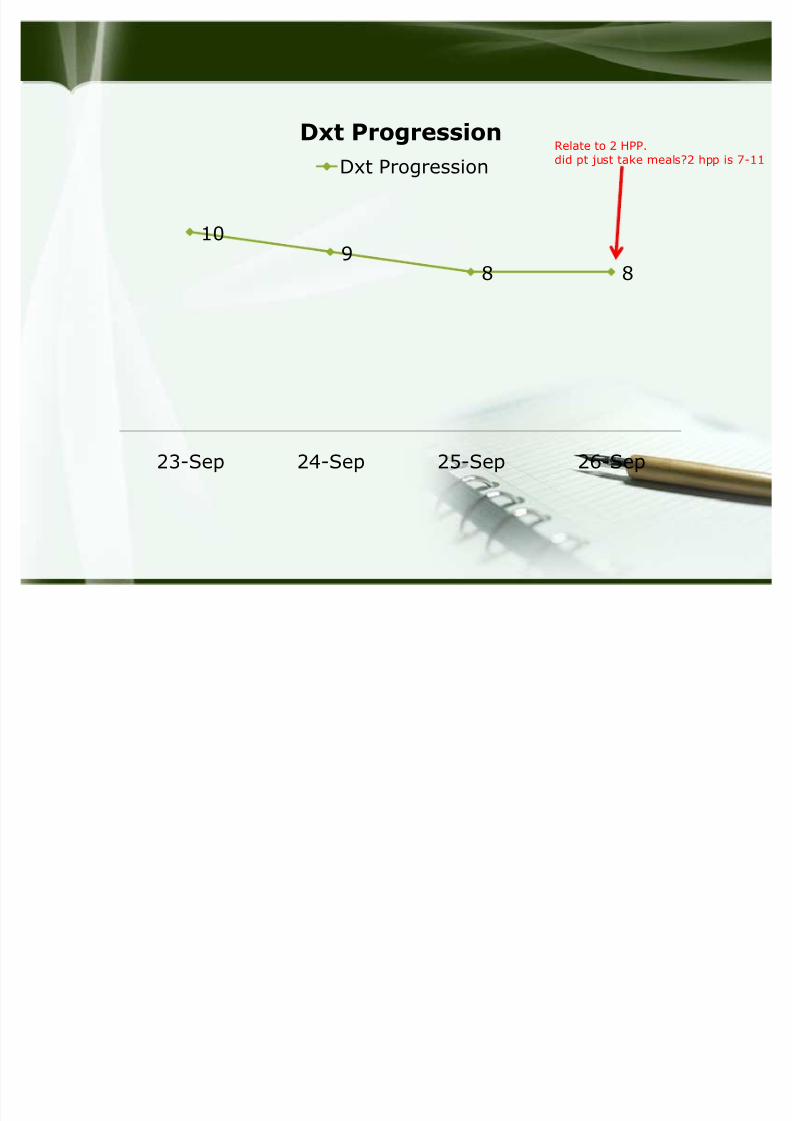
109
8 8
23-Sep 24-Sep 25-Sep 26-Sep
Dxt
Progression
Dxt ProgressionRelate to 2 HPP.did pt just take meals?2 hpp is 7-11

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 25/26
D ietary
Able to finish half of hospital diet Tolerate supplementation providedPt is taking dinner servedImproved appetite
Meal on 23 sep-5 oct 2010 Energy
C HO PFat
BF ±1pcs White B read + 1 nos egg + 2 tsp margerineL ±2 exc White rice+ 1 exc fried fish + 1exc fruitAT-1pcs White B read + 1 nos egg + 2 tsp margerineD- 2 exc White rice+ ½ exc fried chicken + 1 exc fruit
239377239381
15451515
1111117.5
15171519
Glucerna SR± 6 scps (x3*/d) 666 86.4 32.4 23.4
Total : 1902 176 73 89.4

8/8/2019 present ipd
http://slidepdf.com/reader/full/present-ipd 26/26