Embed Size (px)
Citation preview
Prescribing for Prescribing for Hypertension Hypertension Case 2BCase 2BBrillantes – del Rosario
GUIDE to GOOD GUIDE to GOOD Prescribing Prescribing Define the Patient’s ProblemSpecify the Therapeutic ObjectiveChoose an appropriate
TreatmentWrite a Prescription and/or Start
treatmentGive Information, Instructions
And WarningsMonitor the Patient
Defining the Patient’s Defining the Patient’s ProblemProblem
General Data & Chief General Data & Chief ComplaintComplaintMr. Paprika, 40/MLiving in ManilaReferred for “high blood”
Defining Patient’s Problem
History of Present IllnessHistory of Present Illness
Good functional capacity until...
1 mo. PTC – At private preemployment consult, BP was 180/90 mmHg. Prescribed unrecalled meds, did not take.
1 day PTC – BP at local clinic was 170/90 mmHg.
Defining Patient’s Problem

Review of SystemsReview of Systems
(-) fever, weight loss, nausea(-) headaches, dizziness, syncope,
seizure(-) BOV, PND(-) exertional dyspnea, orthopnea,
cough(-) palpitations, chest heaviness(-) abdominal pains, vomiting(-) oliguria, dysuria(-) edema, paresis, paresthesias
Defining Patient’s Problem
Past Medical HistoryPast Medical HistoryType 2 diabetes mellitus –
diagnosed July 2008, on metformin 500 mg BID
No Hx of PTB, asthma, allergies, thyroid disorders, gout
Defining Patient’s Problem

Family Medical HistoryFamily Medical HistoryFather – hypertension, suffered
MI at 45 years old, still alive?
Defining Patient’s Problem
Personal & Social HistoryPersonal & Social HistorySales managerMarried, with 2 childrenDenies smoking, alcohol
consumption, illicit drug useNo food preferences
Defining Patient’s Problem
Physical ExaminationPhysical Examination
General | conscious, coherent, not in distress
Vital Signs | BP 180/90, HR 76/min, RR 12/min, T 37.1°C
HEENT| anicteric sclerae, pink conjunctivae, (-) CLAD, JVP = 4 cm at 30 deg, (-) carotid bruits
Chest & Lungs |equal chest expansion, no rales or wheezes
Heart | good S1, AB-PMI at 6th ICS L MCL, normal & regular HR and rhythm, (-) S3 or murmurs
Defining Patient’s Problem

Physical ExaminationPhysical Examination
Abdomen | round, soft, normoactive bowel sounds, (-) tenderness or organomegaly
Extremities | full, equal pulses w/ pink nail beds, no edema
Neurologic|20/20 vision by Snellen chart; on fundoscopy – normal AV ratio, no AV nicking or hemorrhages
Defining Patient’s Problem

Laboratory and Imaging Laboratory and Imaging StudiesStudiesCBC & chemistries | all w/in normal
limitsUrinalysis | USG = 1.020, pH = 6.0, (-)
sugar, +1 proteins, WBC 0-1, RBC 0-1, (-) casts/crystals
EKG | sinus rhythm, normal axis, LVH
CXR PA & Lateral | cardiomegaly, LVH form
Defining Patient’s Problem
Problem ListProblem ListType 2 diabetes mellitusEssential hypertension, grade 3 –
very high added risk
Defining Patient’s Problem

Specify the Therapeutic Specify the Therapeutic ObjectiveObjective
Therapeutic ObjectivesTherapeutic Objectives
1. Control the hypertension. Target BP <130/80 mmHg.
2. Control blood sugar. Target FBS <7.0 mmol/L.
3. Minimize existing target organ damage and prevent development in other organs.
4. Avoid unhealthy lifestyle choices.
Specifying Treatment Objectives
Choose an Appropriate Choose an Appropriate TreatmentTreatment
Antihypertensive DrugsAntihypertensive DrugsACE inhibitorAlpha BlockersARBsBeta bl0ckersCCBsThiazide Diuretics
Choosing the Right Treatment
Mechanisms of ActionsMechanisms of ActionsACE inhibitors
◦Block the conversion of angiotensin I to angiotensin II by inhibiting angiotensin converting enzyme (ACE)
Alpha-blockers◦Lower by by reducing the peripheral
resistanceAngiotensin II antagonists
◦Block type I angiotensin II receptors
Choosing the Right Treatment

Mechanism of ActionMechanism of ActionBeta-blockers
◦Competitive antagonists of the effects of catecholamines at beta-adrenergic receptor sites
Thiazide Diuretics◦Blocks renal tubular reabsorption of
Na leading to urinary Na loss
Choosing the Right Treatment
Mechanism of ActionMechanism of ActionCalcium Antagonists
◦Inhibit the cellular influx of Ca which is responsible for maintenance of the plateau phase of the action potential
◦The cells they affect are typically the vascular smooth muscle, myocardial cells and cells within the SA and AV nodes
◦They dilate coronary and peripheral arteries with little or no effect on venous tone, have a-ve inotropic action, reduce HR and slow AV conduction
Choosing the Right Treatment
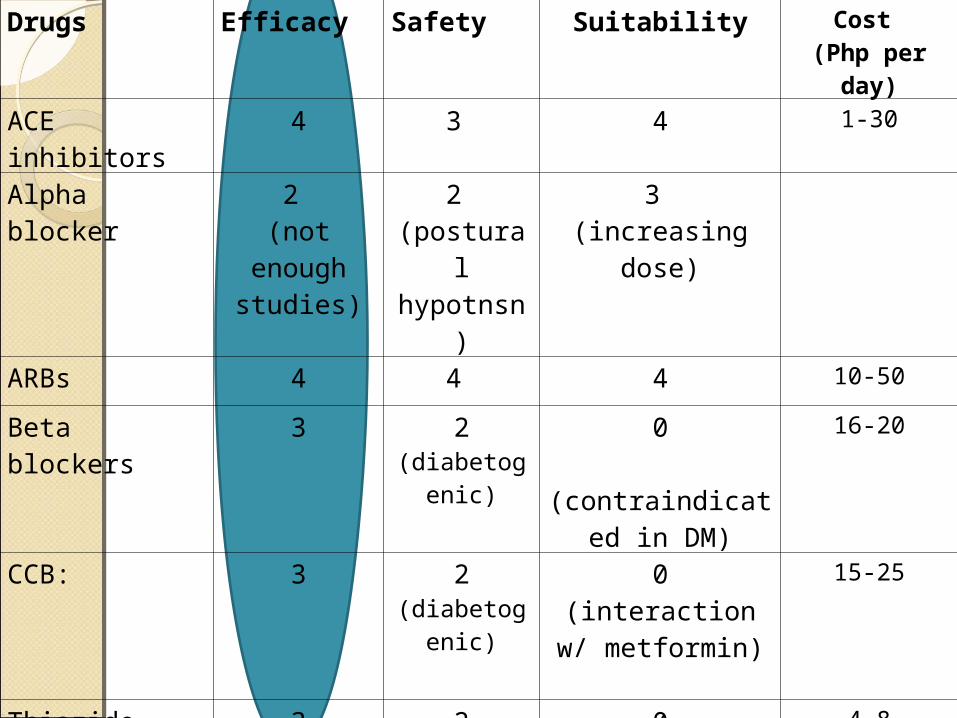
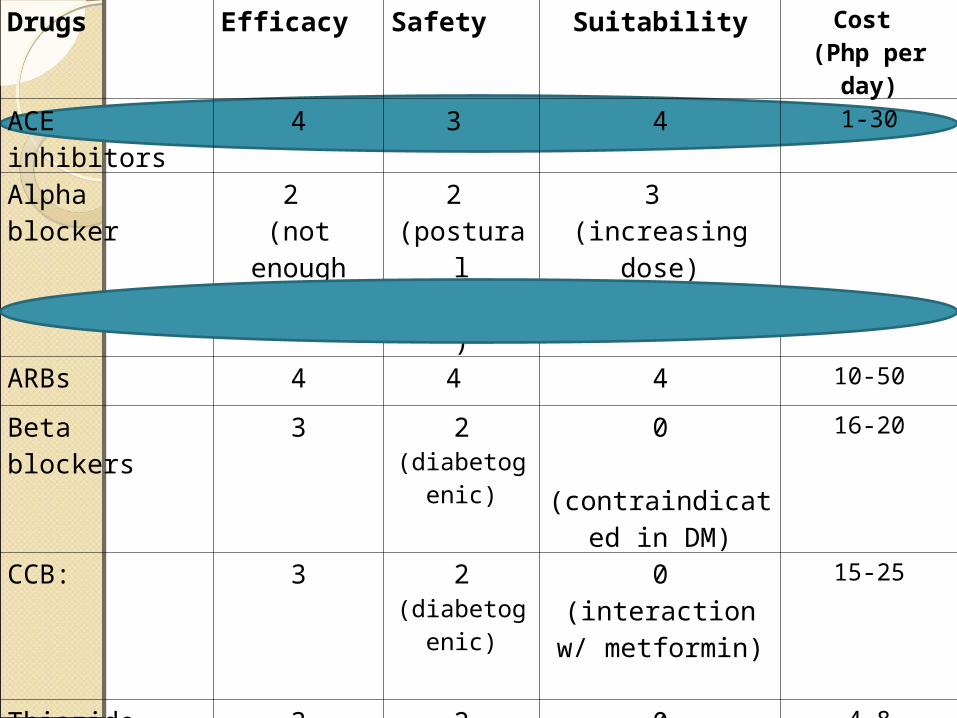
Drugs Efficacy Safety Suitability Cost (Php per day)
ACE inhibitors 4 3 4 1-30
Alpha blocker 2 (not enough
studies)
2 (postural
hypotnsn)
3 (increasing dose)
ARBs 4 4 4 10-50
Beta blockers 3 2 (diabetogenic)
0(contraindicated in
DM)
16-20
CCB: 3 2 (diabetogenic)
0(interaction w/
metformin)
15-25
Thiazide Diuretics 3 2 (diabetogenic)
0(contraindicated in
DM)
4-8
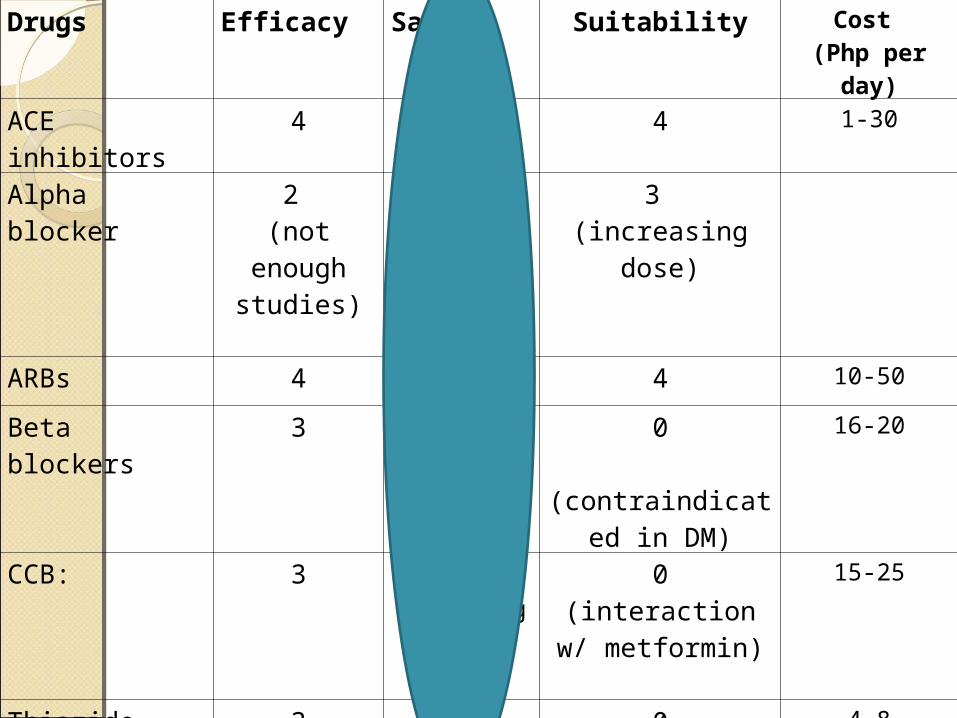
Drugs Efficacy Safety Suitability Cost (Php per day)
ACE inhibitors 4 3 4 1-30
Alpha blocker 2 (not enough
studies)
2 (postural
hypotnsn)
3 (increasing dose)
ARBs 4 4 4 10-50
Beta blockers 3 2 (diabetogenic)
0(contraindicated in
DM)
16-20
CCB: 3 2 (diabetogenic)
0(interaction w/
metformin)
15-25
Thiazide Diuretics 3 2 (diabetogenic)
0(contraindicated in
DM)
4-8

Drugs Efficacy Safety Suitability Cost (Php per day)
ACE inhibitors 4 3 4 1-30
Alpha blocker 2 (not enough
studies)
2 (postural
hypotnsn)
3 (increasing dose)
ARBs 4 4 4 10-50
Beta blockers 3 2 (diabetogenic)
0(contraindicated in
DM)
16-20
CCB: 3 2 (diabetogenic)
0(interaction w/
metformin)
15-25
Thiazide Diuretics 3 2 (diabetogenic)
0(contraindicated in
DM)
4-8

Drugs Efficacy Safety Suitability Cost (Php per day)
ACE inhibitors 4 3 4 1-30
Alpha blocker 2 (not enough
studies)
2 (postural
hypotnsn)
3 (increasing dose)
ARBs 4 4 4 10-50
Beta blockers 3 2 (diabetogenic)
0(contraindicated in
DM)
16-20
CCB: 3 2 (diabetogenic)
0(interaction w/
metformin)
15-25
Thiazide Diuretics 3 2 (diabetogenic)
0(contraindicated in
DM)
4-8
Drugs Efficacy Safety Suitability Cost (Php per day)
ACE inhibitors 4 3 4 1-30
Alpha blocker 2 (not enough
studies)
2 (postural
hypotnsn)
3 (increasing dose)
ARBs 4 4 4 10-50
Beta blockers 3 2 (diabetogenic)
0(contraindicated in
DM)
16-20
CCB: 3 2 (diabetogenic)
0(interaction w/
metformin)
15-25
Thiazide Diuretics 3 2 (diabetogenic)
0(contraindicated in
DM)
4-8

P-DrugP-DrugACE INHIBITORSARBs
Choosing the Right Treatment

ACE InhibitorsACE InhibitorsCaptoprilEnalaprilLisonopril
Choosing the Right Treatment
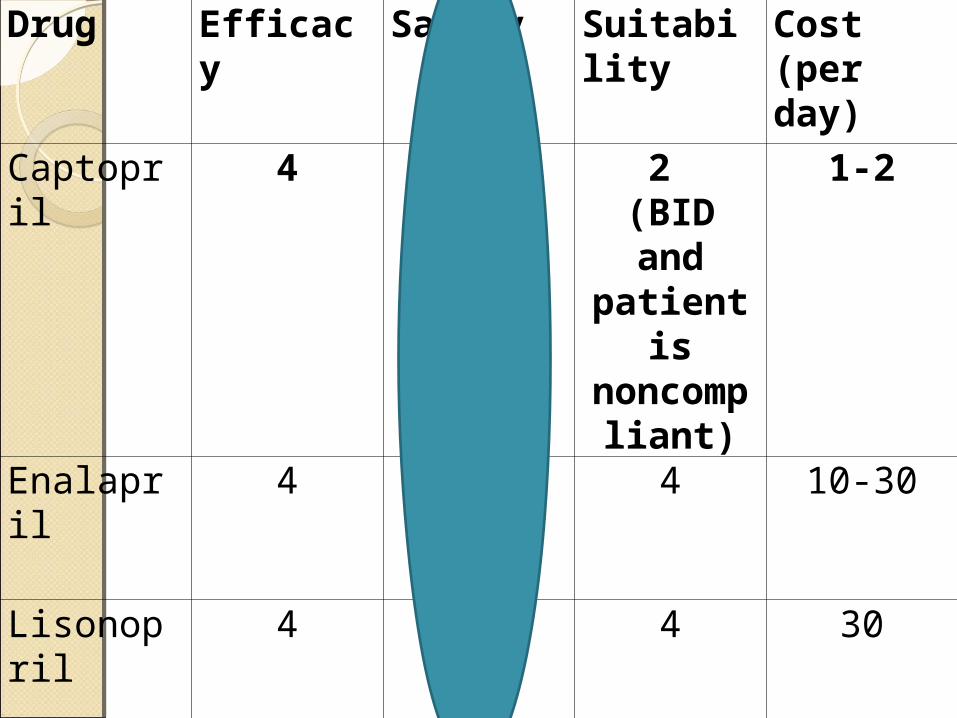
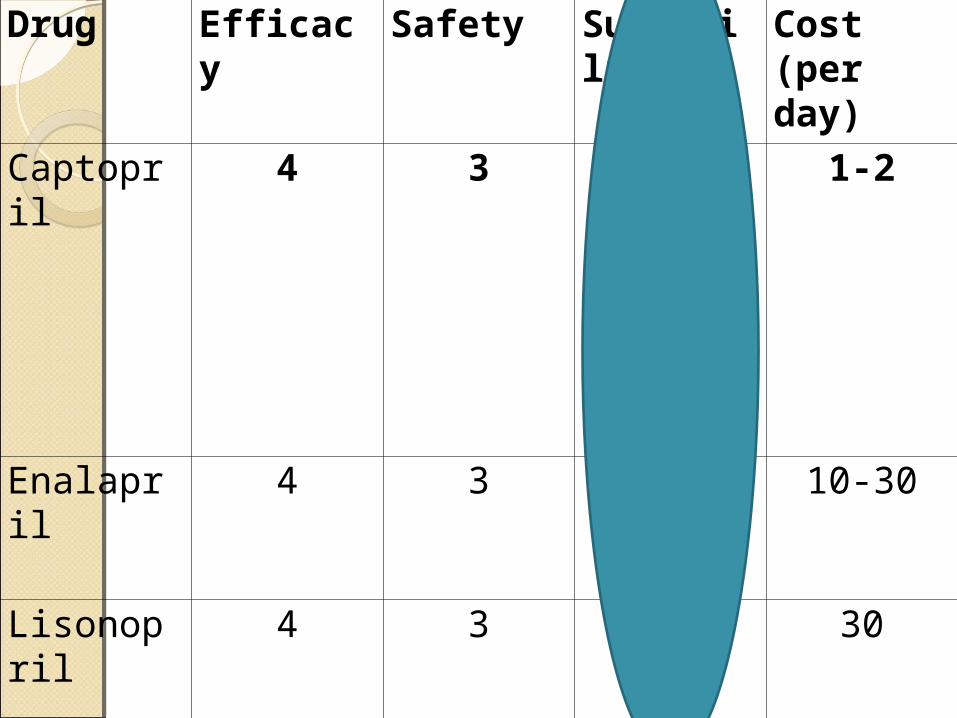
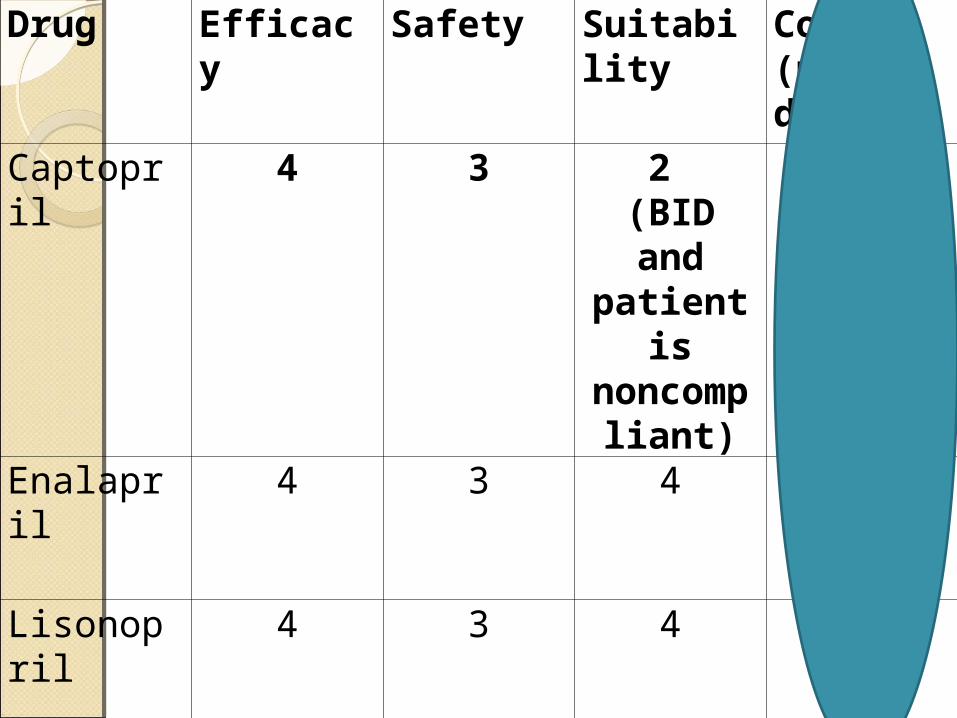
Drug Efficacy Safety Suitability Cost (per day)
Captopril 4 3 2 (BID and patient is
noncompliant)
1-2
Enalapril 4 3 4 10-30
Lisonopril 4 3 4 30
Drug Efficacy Safety Suitability Cost (per day)
Captopril 4 3 2 (BID and patient is
noncompliant)
1-2
Enalapril 4 3 4 10-30
Lisonopril 4 3 4 30
Drug Efficacy Safety Suitability Cost (per day)
Captopril 4 3 2 (BID and patient is
noncompliant)
1-2
Enalapril 4 3 4 10-30
Lisonopril 4 3 4 30

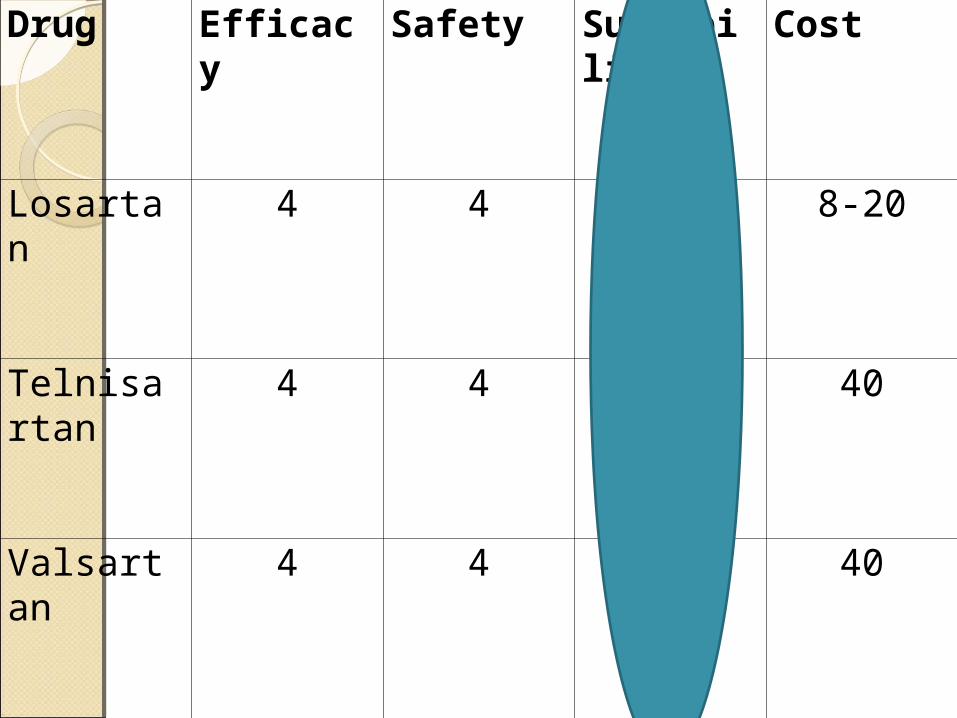
Angiotensin Receptor Angiotensin Receptor BlockersBlockersLosartanTelnisartanValsartan
Choosing the Right Treatment

Drug Efficacy Safety Suitability Cost
Losartan 4 4 4 8-20
Telnisartan 4 4 4 40
Valsartan 4 4 4 40

Drug Efficacy Safety Suitability Cost
Losartan 4 4 4 8-20
Telnisartan 4 4 4 40
Valsartan 4 4 4 40
Drug Efficacy Safety Suitability Cost
Losartan 4 4 4 8-20
Telnisartan 4 4 4 40
Valsartan 4 4 4 40

Drug Efficacy Safety Suitability Cost
Losartan 4 4 4 8-20
Telnisartan 4 4 4 40
Valsartan 4 4 4 40
Write a PrescriptionWrite a PrescriptionStart TreatmentStart Treatment
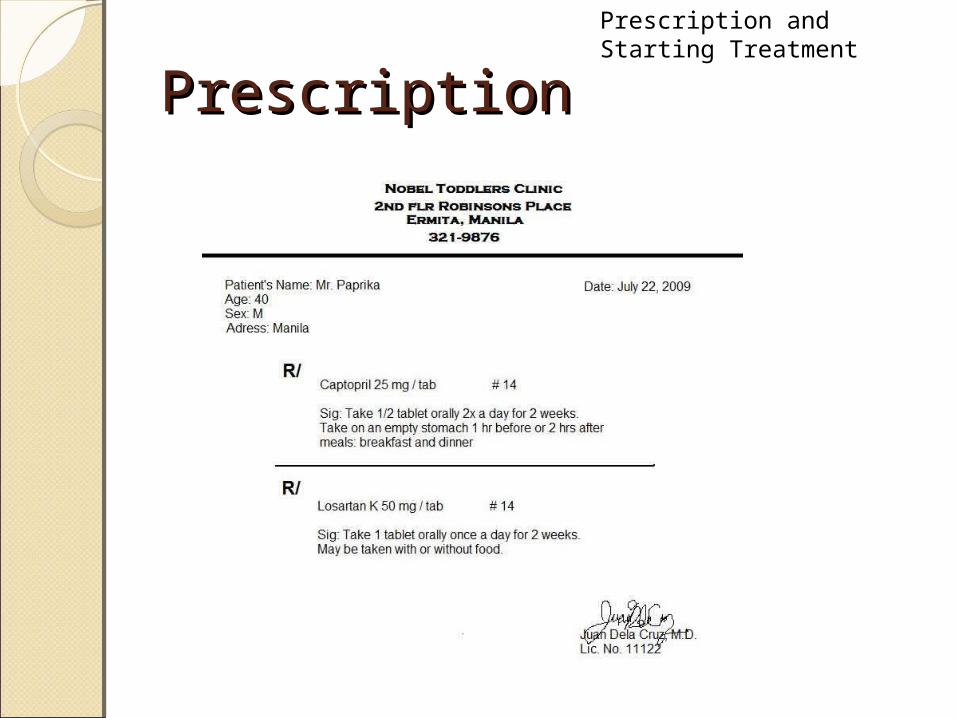
PrescriptionPrescriptionPrescription and Starting Treatment

Giving of Information, Giving of Information, Instructions and WarningsInstructions and Warnings
Effects of the drug:◦Why the drug is needed: “Mr. Paprika,
you have to take these drugs because these will control your high blood pressure.”
◦Which symptoms will disappear and which will not: “BP will be lowered and should last for about 24 hours.”
◦What will happen if the drug is taken incorrectly or not at all: “ The hypertension will persist and can result to further organ damage and other complications.”
Infos, Instructions, Warnings

Side effects:◦Which side effects may occur:
“Captopril may cause persistent dry cough, dizziness, fatigue, headache, abdominal pain, and skin reactions. Losartan may cause dizziness, runny nose, sore throat and back pain.”
◦What action to take: “Inform the doctor/me.”
Infos, Instructions, Warnings
Instructions◦How the drug should be taken; when it
should be taken; how long the treatment should continue– “For Captopril, you have to take ½ tablet orally twice a day. It should be taken on an empty stomach 1 hour before or 2 hours after meals: breakfast and dinner. For Losartan, you have to take 1 tablet orally once a day with or without food. Continue the treatment for 2 weeks”.
◦How the drug should be stored: “Store the drugs at room temperature”
◦What to do with left-over drugs: “Finish all the drugs and none should be left”
Infos, Instructions, Warnings
Warnings:◦When the drug should not be taken:
“As much as possible, do not drink any alcoholic drink as this may interact with the drugs.”
◦Why the drug should be taken regularly: “You have to take the drugs correctly and regularly for it to have an effect on your BP and prevent further serious complications.”
Infos, Instructions, Warnings

Future Consultations:◦When to come back (or not): “You have to
come back after two weeks for evaluation.”◦In what circumstances to come earlier: “
You can come back earlier if you experience side effects of the drugs or other new symptoms.”
◦What information the doctor will need at the next appointment: “Please have your BP taken regularly (at least twice a day), record it in a logbook and when you come back, bring the log of your BP from the start of treatment.”
Infos, Instructions, Warnings

Everything clear?◦Ask the patient whether everything
is understood◦Ask the patient to repeat the most
important information◦Ask whether the patient has any
more questions
Infos, Instructions, Warnings

Non-Pharmacologic Non-Pharmacologic Treatment StrategiesTreatment Strategies1. Lifestyle Measures
a) Smoking/Alcohol/Illicit Drugs• Positive reinforcement• Passive smoking
b) Diet• Sodium Restriction• Glycaemic Control• Other Dietary Changes
c) Physical Exercise2. Family Education
Infos, Instructions, Warnings
Monitoring of TreatmentMonitoring of Treatment
MonitoringMonitoring
Passive Monitoring◦Encourage Mr. Paprika to invest in a
good BP apparatus and educate his family members or neighbors on proper usage.
◦Inform patient that his his BP should be monitored regularly In the morning and afternoon
Monitoring

MonitoringMonitoring
Active Monitoring◦Advise Mr. Paprika to return for consult
after 2 weeks If a control in BP is evident at the 2 week
checkup continue the treatment If BP control is not evident at the 2 week
checkup adjust the treatment If any of the side effects (ACEi-induced cough)
is bothering the patient adjust treatment accordingly
Monitoring





























