Embed Size (px)
Citation preview
1586 Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil
Practical Approach to the Pathologic Diagnosisof Gastritis
Antonia R. Sepulveda, MD, PhD; Madhavi Patil, MD
● Context.—Most types of gastritis can be diagnosed onhematoxylin-eosin stains. The most common type of chron-ic gastritis is Helicobacter pylori gastritis. Reactive orchemical gastropathy, which is often associated with non-steroidal anti-inflammatory drug use or bile reflux, is com-mon in most practices. The diagnosis of atrophic gastritiscan be challenging if few biopsy samples are available andif the location of the biopsies in the stomach is not known,such as when random biopsies are sampled in one jar. Ifthe biopsy site is not known, immunohistochemical stains,such as a combination of synaptophysin and gastrin, areuseful in establishing the biopsy location.
Objective.—To demonstrate a practical approach toachieving a pathologic diagnosis of gastritis by evaluatinga limited number of features in mucosal biopsies.
Data Source.—In this article, we present several repre-
sentative gastric biopsy cases from a gastrointestinal pa-thology practice to demonstrate the practical applicationof basic histopathologic methods for the diagnosis of gas-tritis.
Conclusions.—Limited ancillary tests are usually re-quired for a diagnosis of gastritis. In some cases, specialstains, such as acid-fast stains, and immunohistochemicalstains, such as for H pylori and viruses, can be useful. Hel-icobacter pylori immunohistochemical stains can particu-larly contribute (1) when moderate to severe, chronic gas-tritis or active gastritis is present but no Helicobacter or-ganisms are identified upon hematoxylin-eosin stain; (2)when extensive intestinal metaplasia is present; and (3) infollow-up biopsies, after antibiotic treatment for H pylori.
(Arch Pathol Lab Med. 2008;132:1586–1593)
Gastritis refers to a group of diseases characterized byinflammation of the gastric mucosa. Histologic ex-
amination of gastric mucosal biopsies is necessary to es-tablish a diagnosis of gastritis. In clinical practice, the roleof the pathologist who evaluates a gastric biopsy for gas-tritis is to find the cause of gastritis because that will pro-vide direct targets toward which therapeutic measures canbe directed. An etiologic classification of gastritis is pre-sented at the end of this section. Comprehensive reviewsof gastritis have been published.1,2,3 The goal of this articleis to present a practical approach to the diagnosis of themost common types of gastritis encountered in a largepractice of gastrointestinal pathology. The reader will bepresented several cases representative of typical forms ofgastritis; for each case, the reader will be promptedthrough a series of questions to examine the histologicfeatures of the mucosa, leading to a pattern of answersand to a final diagnosis.
The first question is aimed at determining whether ornot there are features of chronic or acute (active) gastritis
Accepted for publication January 10, 2008.From the Department of Pathology and Laboratory Medicine, Hos-
pital of the University of Pennsylvania, Philadelphia.The authors have no relevant financial interest in the products or
companies described in this article.Presented in part at the 47th Annual Meeting of the Houston Society
of Clinical Pathologists, Houston, Tex, April 21, 2007.Reprints: Antonia R. Sepulveda, MD, PhD, Department of Pathology
and Laboratory Medicine, University of Pennsylvania, 3400 Spruce St,Founders Six, Philadelphia, PA 19104 (e-mail: [email protected]).
present. If the biopsy shows chronic gastritis, the follow-ing questions should be posed:
1. Are there features of chronic gastritis present? Lym-phocytic and plasmacytic inflammatory reaction indicateschronic gastritis.
2. Are there neutrophils in the mucosa? The presenceof neutrophils indicate active gastritis.
3. Is there Helicobacter?4. Is there glandular atrophy? Is intestinal metaplasia
present?5. What is the topography of lesions (predominantly in
the oxyntic mucosa of the body and fundus, predomi-nantly in antrum, or involving both locations)?
6. Are there special features (such as granulomas, fo-veolar hyperplasia, viral inclusions)?
7. What ancillary studies are indicated, and what arethe results?
TYPES OF CHRONIC GASTRITIS
Infectious Gastritis
Helicobacter pylori infection is the most common cause ofchronic gastritis. Other forms of infectious gastritis includethe following: Helicobacter heilmannii–associated gastritis;granulomatous gastritis associated with gastric infectionsin mycobacteriosis, syphilis, histoplasmosis, mucormyco-sis, South American blastomycosis, anisakiasis or anisak-idosis; chronic gastritis associated with parasitic infec-tions; and viral infections, such as cytomegalovirus andherpesvirus infection.
Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil 1587
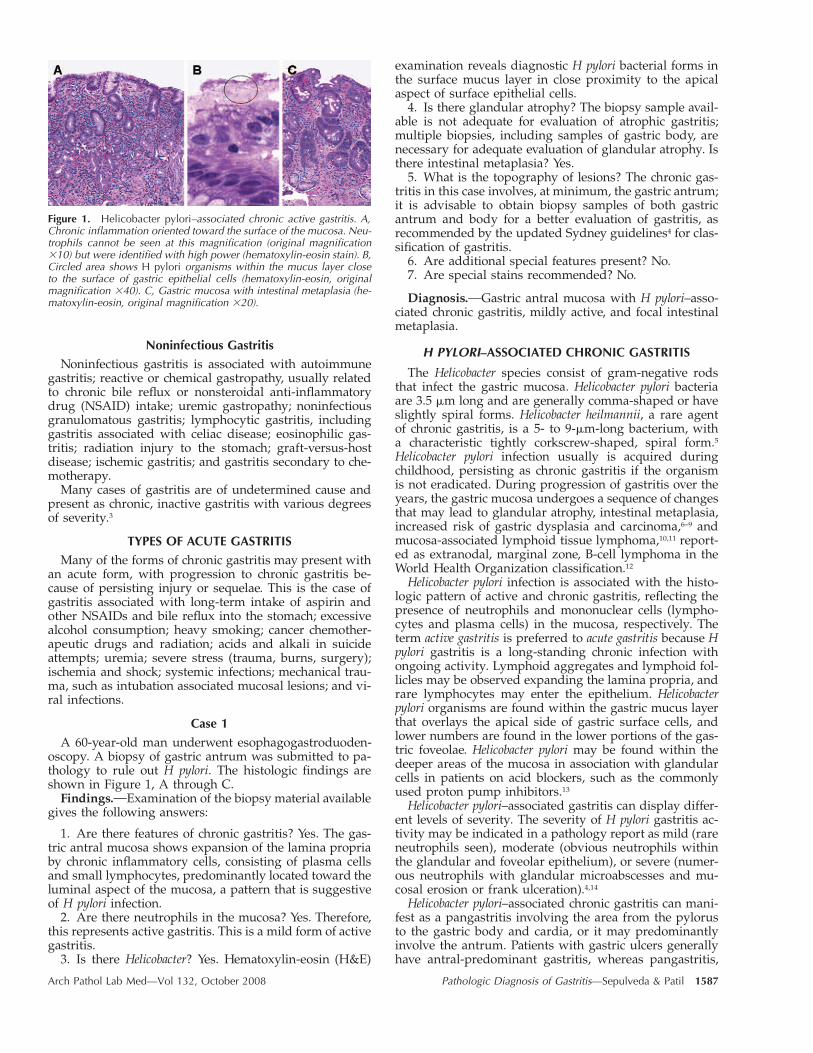
Figure 1. Helicobacter pylori–associated chronic active gastritis. A,Chronic inflammation oriented toward the surface of the mucosa. Neu-trophils cannot be seen at this magnification (original magnification�10) but were identified with high power (hematoxylin-eosin stain). B,Circled area shows H pylori organisms within the mucus layer closeto the surface of gastric epithelial cells (hematoxylin-eosin, originalmagnification �40). C, Gastric mucosa with intestinal metaplasia (he-matoxylin-eosin, original magnification �20).
Noninfectious GastritisNoninfectious gastritis is associated with autoimmune
gastritis; reactive or chemical gastropathy, usually relatedto chronic bile reflux or nonsteroidal anti-inflammatorydrug (NSAID) intake; uremic gastropathy; noninfectiousgranulomatous gastritis; lymphocytic gastritis, includinggastritis associated with celiac disease; eosinophilic gas-tritis; radiation injury to the stomach; graft-versus-hostdisease; ischemic gastritis; and gastritis secondary to che-motherapy.
Many cases of gastritis are of undetermined cause andpresent as chronic, inactive gastritis with various degreesof severity.3
TYPES OF ACUTE GASTRITISMany of the forms of chronic gastritis may present with
an acute form, with progression to chronic gastritis be-cause of persisting injury or sequelae. This is the case ofgastritis associated with long-term intake of aspirin andother NSAIDs and bile reflux into the stomach; excessivealcohol consumption; heavy smoking; cancer chemother-apeutic drugs and radiation; acids and alkali in suicideattempts; uremia; severe stress (trauma, burns, surgery);ischemia and shock; systemic infections; mechanical trau-ma, such as intubation associated mucosal lesions; and vi-ral infections.
Case 1
A 60-year-old man underwent esophagogastroduoden-oscopy. A biopsy of gastric antrum was submitted to pa-thology to rule out H pylori. The histologic findings areshown in Figure 1, A through C.
Findings. Examination of the biopsy material availablegives the following answers:
1. Are there features of chronic gastritis? Yes. The gas-tric antral mucosa shows expansion of the lamina propriaby chronic inflammatory cells, consisting of plasma cellsand small lymphocytes, predominantly located toward theluminal aspect of the mucosa, a pattern that is suggestiveof H pylori infection.
2. Are there neutrophils in the mucosa? Yes. Therefore,this represents active gastritis. This is a mild form of activegastritis.
3. Is there Helicobacter? Yes. Hematoxylin-eosin (H&E)
examination reveals diagnostic H pylori bacterial forms inthe surface mucus layer in close proximity to the apicalaspect of surface epithelial cells.
4. Is there glandular atrophy? The biopsy sample avail-able is not adequate for evaluation of atrophic gastritis;multiple biopsies, including samples of gastric body, arenecessary for adequate evaluation of glandular atrophy. Isthere intestinal metaplasia? Yes.
5. What is the topography of lesions? The chronic gas-tritis in this case involves, at minimum, the gastric antrum;it is advisable to obtain biopsy samples of both gastricantrum and body for a better evaluation of gastritis, asrecommended by the updated Sydney guidelines4 for clas-sification of gastritis.
6. Are additional special features present? No.7. Are special stains recommended? No.
Diagnosis. Gastric antral mucosa with H pylori–asso-ciated chronic gastritis, mildly active, and focal intestinalmetaplasia.
H PYLORI–ASSOCIATED CHRONIC GASTRITIS
The Helicobacter species consist of gram-negative rodsthat infect the gastric mucosa. Helicobacter pylori bacteriaare 3.5 �m long and are generally comma-shaped or haveslightly spiral forms. Helicobacter heilmannii, a rare agentof chronic gastritis, is a 5- to 9-�m-long bacterium, witha characteristic tightly corkscrew-shaped, spiral form.5Helicobacter pylori infection usually is acquired duringchildhood, persisting as chronic gastritis if the organismis not eradicated. During progression of gastritis over theyears, the gastric mucosa undergoes a sequence of changesthat may lead to glandular atrophy, intestinal metaplasia,increased risk of gastric dysplasia and carcinoma,6–9 andmucosa-associated lymphoid tissue lymphoma,10,11 report-ed as extranodal, marginal zone, B-cell lymphoma in theWorld Health Organization classification.12
Helicobacter pylori infection is associated with the histo-logic pattern of active and chronic gastritis, reflecting thepresence of neutrophils and mononuclear cells (lympho-cytes and plasma cells) in the mucosa, respectively. Theterm active gastritis is preferred to acute gastritis because Hpylori gastritis is a long-standing chronic infection withongoing activity. Lymphoid aggregates and lymphoid fol-licles may be observed expanding the lamina propria, andrare lymphocytes may enter the epithelium. Helicobacterpylori organisms are found within the gastric mucus layerthat overlays the apical side of gastric surface cells, andlower numbers are found in the lower portions of the gas-tric foveolae. Helicobacter pylori may be found within thedeeper areas of the mucosa in association with glandularcells in patients on acid blockers, such as the commonlyused proton pump inhibitors.13
Helicobacter pylori–associated gastritis can display differ-ent levels of severity. The severity of H pylori gastritis ac-tivity may be indicated in a pathology report as mild (rareneutrophils seen), moderate (obvious neutrophils withinthe glandular and foveolar epithelium), or severe (numer-ous neutrophils with glandular microabscesses and mu-cosal erosion or frank ulceration).4,14
Helicobacter pylori–associated chronic gastritis can mani-fest as a pangastritis involving the area from the pylorusto the gastric body and cardia, or it may predominantlyinvolve the antrum. Patients with gastric ulcers generallyhave antral-predominant gastritis, whereas pangastritis,
1588 Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil
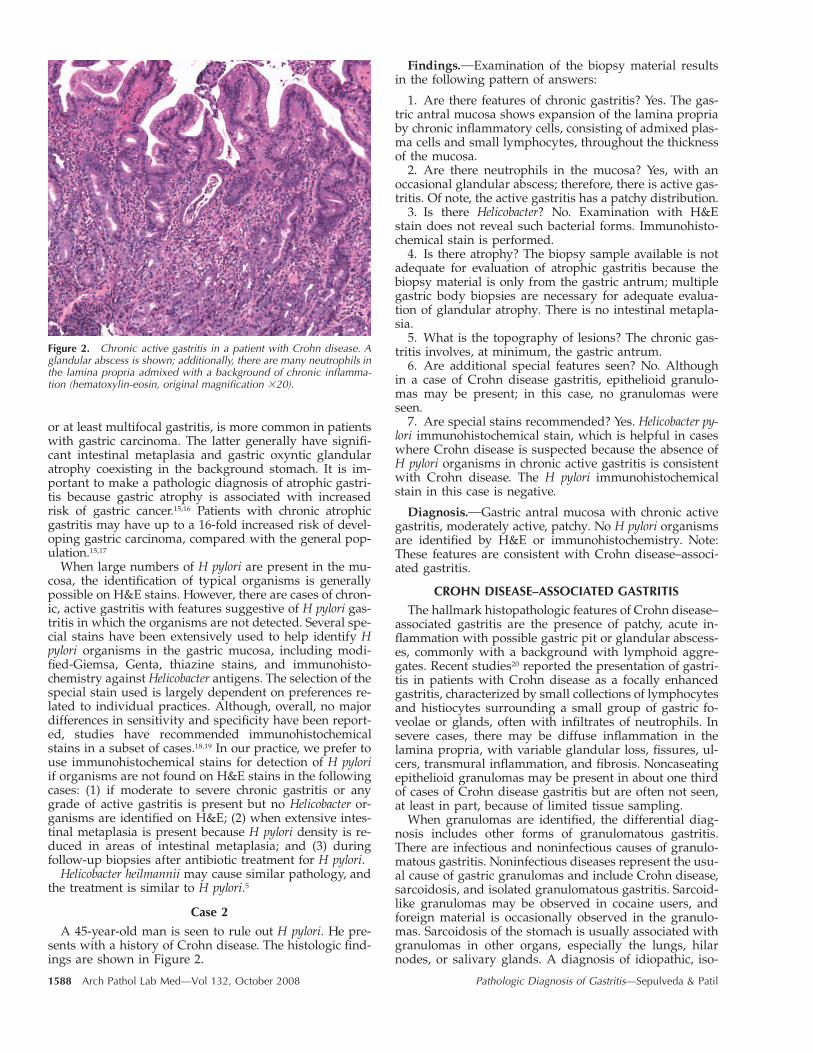
Figure 2. Chronic active gastritis in a patient with Crohn disease. Aglandular abscess is shown; additionally, there are many neutrophils inthe lamina propria admixed with a background of chronic inflamma-tion (hematoxylin-eosin, original magnification �20).
or at least multifocal gastritis, is more common in patientswith gastric carcinoma. The latter generally have signifi-cant intestinal metaplasia and gastric oxyntic glandularatrophy coexisting in the background stomach. It is im-portant to make a pathologic diagnosis of atrophic gastri-tis because gastric atrophy is associated with increasedrisk of gastric cancer.15,16 Patients with chronic atrophicgastritis may have up to a 16-fold increased risk of devel-oping gastric carcinoma, compared with the general pop-ulation.15,17
When large numbers of H pylori are present in the mu-cosa, the identification of typical organisms is generallypossible on H&E stains. However, there are cases of chron-ic, active gastritis with features suggestive of H pylori gas-tritis in which the organisms are not detected. Several spe-cial stains have been extensively used to help identify Hpylori organisms in the gastric mucosa, including modi-fied-Giemsa, Genta, thiazine stains, and immunohisto-chemistry against Helicobacter antigens. The selection of thespecial stain used is largely dependent on preferences re-lated to individual practices. Although, overall, no majordifferences in sensitivity and specificity have been report-ed, studies have recommended immunohistochemicalstains in a subset of cases.18,19 In our practice, we prefer touse immunohistochemical stains for detection of H pyloriif organisms are not found on H&E stains in the followingcases: (1) if moderate to severe chronic gastritis or anygrade of active gastritis is present but no Helicobacter or-ganisms are identified on H&E; (2) when extensive intes-tinal metaplasia is present because H pylori density is re-duced in areas of intestinal metaplasia; and (3) duringfollow-up biopsies after antibiotic treatment for H pylori.
Helicobacter heilmannii may cause similar pathology, andthe treatment is similar to H pylori.5
Case 2
A 45-year-old man is seen to rule out H pylori. He pre-sents with a history of Crohn disease. The histologic find-ings are shown in Figure 2.
Findings. Examination of the biopsy material resultsin the following pattern of answers:
1. Are there features of chronic gastritis? Yes. The gas-tric antral mucosa shows expansion of the lamina propriaby chronic inflammatory cells, consisting of admixed plas-ma cells and small lymphocytes, throughout the thicknessof the mucosa.
2. Are there neutrophils in the mucosa? Yes, with anoccasional glandular abscess; therefore, there is active gas-tritis. Of note, the active gastritis has a patchy distribution.
3. Is there Helicobacter? No. Examination with H&Estain does not reveal such bacterial forms. Immunohisto-chemical stain is performed.
4. Is there atrophy? The biopsy sample available is notadequate for evaluation of atrophic gastritis because thebiopsy material is only from the gastric antrum; multiplegastric body biopsies are necessary for adequate evalua-tion of glandular atrophy. There is no intestinal metapla-sia.
5. What is the topography of lesions? The chronic gas-tritis involves, at minimum, the gastric antrum.
6. Are additional special features seen? No. Althoughin a case of Crohn disease gastritis, epithelioid granulo-mas may be present; in this case, no granulomas wereseen.
7. Are special stains recommended? Yes. Helicobacter py-lori immunohistochemical stain, which is helpful in caseswhere Crohn disease is suspected because the absence ofH pylori organisms in chronic active gastritis is consistentwith Crohn disease. The H pylori immunohistochemicalstain in this case is negative.
Diagnosis. Gastric antral mucosa with chronic activegastritis, moderately active, patchy. No H pylori organismsare identified by H&E or immunohistochemistry. Note:These features are consistent with Crohn disease–associ-ated gastritis.
CROHN DISEASE–ASSOCIATED GASTRITISThe hallmark histopathologic features of Crohn disease–
associated gastritis are the presence of patchy, acute in-flammation with possible gastric pit or glandular abscess-es, commonly with a background with lymphoid aggre-gates. Recent studies20 reported the presentation of gastri-tis in patients with Crohn disease as a focally enhancedgastritis, characterized by small collections of lymphocytesand histiocytes surrounding a small group of gastric fo-veolae or glands, often with infiltrates of neutrophils. Insevere cases, there may be diffuse inflammation in thelamina propria, with variable glandular loss, fissures, ul-cers, transmural inflammation, and fibrosis. Noncaseatingepithelioid granulomas may be present in about one thirdof cases of Crohn disease gastritis but are often not seen,at least in part, because of limited tissue sampling.
When granulomas are identified, the differential diag-nosis includes other forms of granulomatous gastritis.There are infectious and noninfectious causes of granulo-matous gastritis. Noninfectious diseases represent the usu-al cause of gastric granulomas and include Crohn disease,sarcoidosis, and isolated granulomatous gastritis. Sarcoid-like granulomas may be observed in cocaine users, andforeign material is occasionally observed in the granulo-mas. Sarcoidosis of the stomach is usually associated withgranulomas in other organs, especially the lungs, hilarnodes, or salivary glands. A diagnosis of idiopathic, iso-
Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil 1589
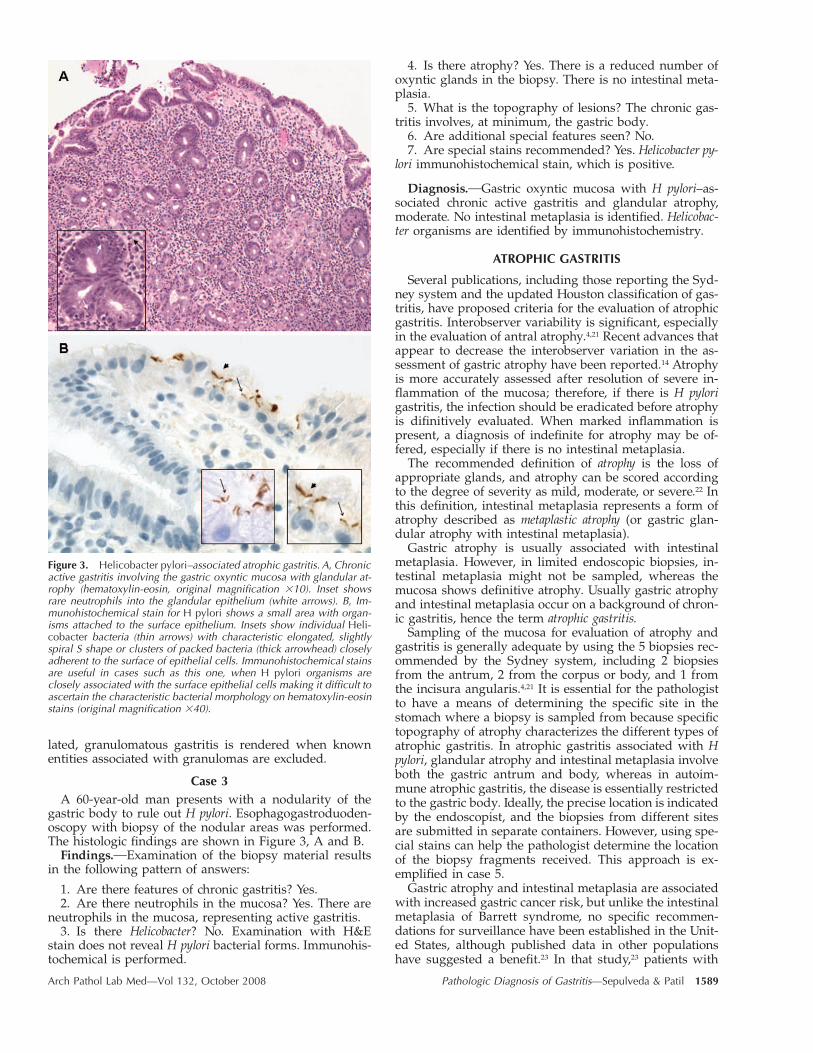
Figure 3. Helicobacter pylori–associated atrophic gastritis. A, Chronicactive gastritis involving the gastric oxyntic mucosa with glandular at-rophy (hematoxylin-eosin, original magnification �10). Inset showsrare neutrophils into the glandular epithelium (white arrows). B, Im-munohistochemical stain for H pylori shows a small area with organ-isms attached to the surface epithelium. Insets show individual Heli-cobacter bacteria (thin arrows) with characteristic elongated, slightlyspiral S shape or clusters of packed bacteria (thick arrowhead) closelyadherent to the surface of epithelial cells. Immunohistochemical stainsare useful in cases such as this one, when H pylori organisms areclosely associated with the surface epithelial cells making it difficult toascertain the characteristic bacterial morphology on hematoxylin-eosinstains (original magnification �40).
lated, granulomatous gastritis is rendered when knownentities associated with granulomas are excluded.
Case 3A 60-year-old man presents with a nodularity of the
gastric body to rule out H pylori. Esophagogastroduoden-oscopy with biopsy of the nodular areas was performed.The histologic findings are shown in Figure 3, A and B.
Findings. Examination of the biopsy material resultsin the following pattern of answers:
1. Are there features of chronic gastritis? Yes.2. Are there neutrophils in the mucosa? Yes. There are
neutrophils in the mucosa, representing active gastritis.3. Is there Helicobacter? No. Examination with H&E
stain does not reveal H pylori bacterial forms. Immunohis-tochemical is performed.
4. Is there atrophy? Yes. There is a reduced number ofoxyntic glands in the biopsy. There is no intestinal meta-plasia.
5. What is the topography of lesions? The chronic gas-tritis involves, at minimum, the gastric body.
6. Are additional special features seen? No.7. Are special stains recommended? Yes. Helicobacter py-
lori immunohistochemical stain, which is positive.
Diagnosis. Gastric oxyntic mucosa with H pylori–as-sociated chronic active gastritis and glandular atrophy,moderate. No intestinal metaplasia is identified. Helicobac-ter organisms are identified by immunohistochemistry.
ATROPHIC GASTRITIS
Several publications, including those reporting the Syd-ney system and the updated Houston classification of gas-tritis, have proposed criteria for the evaluation of atrophicgastritis. Interobserver variability is significant, especiallyin the evaluation of antral atrophy.4,21 Recent advances thatappear to decrease the interobserver variation in the as-sessment of gastric atrophy have been reported.14 Atrophyis more accurately assessed after resolution of severe in-flammation of the mucosa; therefore, if there is H pylorigastritis, the infection should be eradicated before atrophyis difinitively evaluated. When marked inflammation ispresent, a diagnosis of indefinite for atrophy may be of-fered, especially if there is no intestinal metaplasia.
The recommended definition of atrophy is the loss ofappropriate glands, and atrophy can be scored accordingto the degree of severity as mild, moderate, or severe.22 Inthis definition, intestinal metaplasia represents a form ofatrophy described as metaplastic atrophy (or gastric glan-dular atrophy with intestinal metaplasia).
Gastric atrophy is usually associated with intestinalmetaplasia. However, in limited endoscopic biopsies, in-testinal metaplasia might not be sampled, whereas themucosa shows definitive atrophy. Usually gastric atrophyand intestinal metaplasia occur on a background of chron-ic gastritis, hence the term atrophic gastritis.
Sampling of the mucosa for evaluation of atrophy andgastritis is generally adequate by using the 5 biopsies rec-ommended by the Sydney system, including 2 biopsiesfrom the antrum, 2 from the corpus or body, and 1 fromthe incisura angularis.4,21 It is essential for the pathologistto have a means of determining the specific site in thestomach where a biopsy is sampled from because specifictopography of atrophy characterizes the different types ofatrophic gastritis. In atrophic gastritis associated with Hpylori, glandular atrophy and intestinal metaplasia involveboth the gastric antrum and body, whereas in autoim-mune atrophic gastritis, the disease is essentially restrictedto the gastric body. Ideally, the precise location is indicatedby the endoscopist, and the biopsies from different sitesare submitted in separate containers. However, using spe-cial stains can help the pathologist determine the locationof the biopsy fragments received. This approach is ex-emplified in case 5.
Gastric atrophy and intestinal metaplasia are associatedwith increased gastric cancer risk, but unlike the intestinalmetaplasia of Barrett syndrome, no specific recommen-dations for surveillance have been established in the Unit-ed States, although published data in other populationshave suggested a benefit.23 In that study,23 patients with
1590 Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil
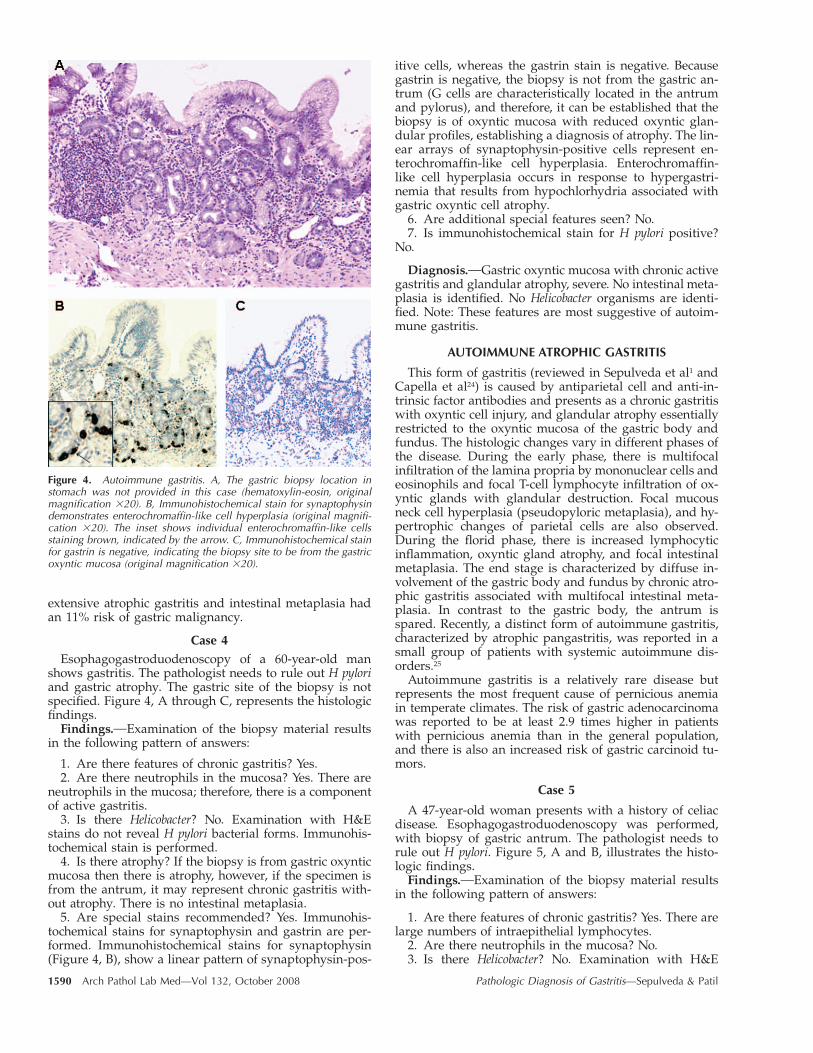
Figure 4. Autoimmune gastritis. A, The gastric biopsy location instomach was not provided in this case (hematoxylin-eosin, originalmagnification �20). B, Immunohistochemical stain for synaptophysindemonstrates enterochromaffin-like cell hyperplasia (original magnifi-cation �20). The inset shows individual enterochromaffin-like cellsstaining brown, indicated by the arrow. C, Immunohistochemical stainfor gastrin is negative, indicating the biopsy site to be from the gastricoxyntic mucosa (original magnification �20).
extensive atrophic gastritis and intestinal metaplasia hadan 11% risk of gastric malignancy.
Case 4Esophagogastroduodenoscopy of a 60-year-old man
shows gastritis. The pathologist needs to rule out H pyloriand gastric atrophy. The gastric site of the biopsy is notspecified. Figure 4, A through C, represents the histologicfindings.
Findings. Examination of the biopsy material resultsin the following pattern of answers:
1. Are there features of chronic gastritis? Yes.2. Are there neutrophils in the mucosa? Yes. There are
neutrophils in the mucosa; therefore, there is a componentof active gastritis.
3. Is there Helicobacter? No. Examination with H&Estains do not reveal H pylori bacterial forms. Immunohis-tochemical stain is performed.
4. Is there atrophy? If the biopsy is from gastric oxynticmucosa then there is atrophy, however, if the specimen isfrom the antrum, it may represent chronic gastritis with-out atrophy. There is no intestinal metaplasia.
5. Are special stains recommended? Yes. Immunohis-tochemical stains for synaptophysin and gastrin are per-formed. Immunohistochemical stains for synaptophysin(Figure 4, B), show a linear pattern of synaptophysin-pos-
itive cells, whereas the gastrin stain is negative. Becausegastrin is negative, the biopsy is not from the gastric an-trum (G cells are characteristically located in the antrumand pylorus), and therefore, it can be established that thebiopsy is of oxyntic mucosa with reduced oxyntic glan-dular profiles, establishing a diagnosis of atrophy. The lin-ear arrays of synaptophysin-positive cells represent en-terochromaffin-like cell hyperplasia. Enterochromaffin-like cell hyperplasia occurs in response to hypergastri-nemia that results from hypochlorhydria associated withgastric oxyntic cell atrophy.
6. Are additional special features seen? No.7. Is immunohistochemical stain for H pylori positive?
No.
Diagnosis. Gastric oxyntic mucosa with chronic activegastritis and glandular atrophy, severe. No intestinal meta-plasia is identified. No Helicobacter organisms are identi-fied. Note: These features are most suggestive of autoim-mune gastritis.
AUTOIMMUNE ATROPHIC GASTRITIS
This form of gastritis (reviewed in Sepulveda et al1 andCapella et al24) is caused by antiparietal cell and anti-in-trinsic factor antibodies and presents as a chronic gastritiswith oxyntic cell injury, and glandular atrophy essentiallyrestricted to the oxyntic mucosa of the gastric body andfundus. The histologic changes vary in different phases ofthe disease. During the early phase, there is multifocalinfiltration of the lamina propria by mononuclear cells andeosinophils and focal T-cell lymphocyte infiltration of ox-yntic glands with glandular destruction. Focal mucousneck cell hyperplasia (pseudopyloric metaplasia), and hy-pertrophic changes of parietal cells are also observed.During the florid phase, there is increased lymphocyticinflammation, oxyntic gland atrophy, and focal intestinalmetaplasia. The end stage is characterized by diffuse in-volvement of the gastric body and fundus by chronic atro-phic gastritis associated with multifocal intestinal meta-plasia. In contrast to the gastric body, the antrum isspared. Recently, a distinct form of autoimmune gastritis,characterized by atrophic pangastritis, was reported in asmall group of patients with systemic autoimmune dis-orders.25
Autoimmune gastritis is a relatively rare disease butrepresents the most frequent cause of pernicious anemiain temperate climates. The risk of gastric adenocarcinomawas reported to be at least 2.9 times higher in patientswith pernicious anemia than in the general population,and there is also an increased risk of gastric carcinoid tu-mors.
Case 5
A 47-year-old woman presents with a history of celiacdisease. Esophagogastroduodenoscopy was performed,with biopsy of gastric antrum. The pathologist needs torule out H pylori. Figure 5, A and B, illustrates the histo-logic findings.
Findings. Examination of the biopsy material resultsin the following pattern of answers:
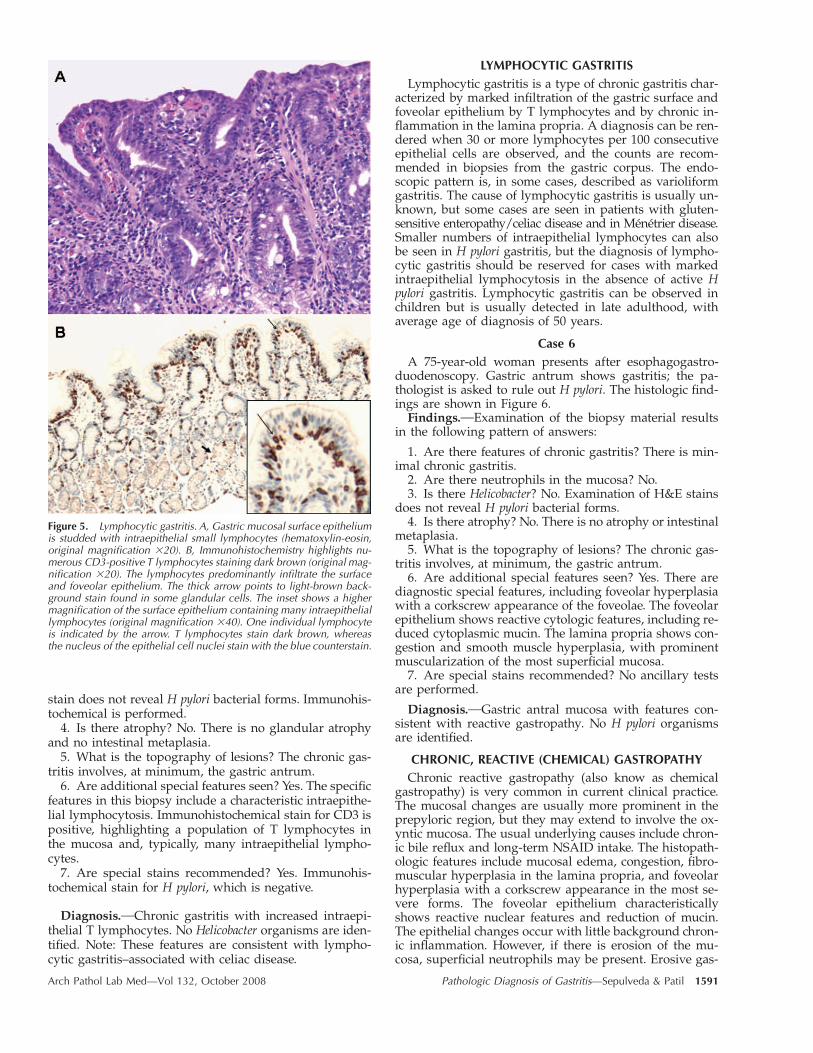
1. Are there features of chronic gastritis? Yes. There arelarge numbers of intraepithelial lymphocytes.
2. Are there neutrophils in the mucosa? No.3. Is there Helicobacter? No. Examination with H&E
Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil 1591
Figure 5. Lymphocytic gastritis. A, Gastric mucosal surface epitheliumis studded with intraepithelial small lymphocytes (hematoxylin-eosin,original magnification �20). B, Immunohistochemistry highlights nu-merous CD3-positive T lymphocytes staining dark brown (original mag-nification �20). The lymphocytes predominantly infiltrate the surfaceand foveolar epithelium. The thick arrow points to light-brown back-ground stain found in some glandular cells. The inset shows a highermagnification of the surface epithelium containing many intraepitheliallymphocytes (original magnification �40). One individual lymphocyteis indicated by the arrow. T lymphocytes stain dark brown, whereasthe nucleus of the epithelial cell nuclei stain with the blue counterstain.
stain does not reveal H pylori bacterial forms. Immunohis-tochemical is performed.
4. Is there atrophy? No. There is no glandular atrophyand no intestinal metaplasia.
5. What is the topography of lesions? The chronic gas-tritis involves, at minimum, the gastric antrum.
6. Are additional special features seen? Yes. The specificfeatures in this biopsy include a characteristic intraepithe-lial lymphocytosis. Immunohistochemical stain for CD3 ispositive, highlighting a population of T lymphocytes inthe mucosa and, typically, many intraepithelial lympho-cytes.
7. Are special stains recommended? Yes. Immunohis-tochemical stain for H pylori, which is negative.
Diagnosis. Chronic gastritis with increased intraepi-thelial T lymphocytes. No Helicobacter organisms are iden-tified. Note: These features are consistent with lympho-cytic gastritis–associated with celiac disease.
LYMPHOCYTIC GASTRITISLymphocytic gastritis is a type of chronic gastritis char-
acterized by marked infiltration of the gastric surface andfoveolar epithelium by T lymphocytes and by chronic in-flammation in the lamina propria. A diagnosis can be ren-dered when 30 or more lymphocytes per 100 consecutiveepithelial cells are observed, and the counts are recom-mended in biopsies from the gastric corpus. The endo-scopic pattern is, in some cases, described as varioliformgastritis. The cause of lymphocytic gastritis is usually un-known, but some cases are seen in patients with gluten-sensitive enteropathy/celiac disease and in Menetrier disease.Smaller numbers of intraepithelial lymphocytes can alsobe seen in H pylori gastritis, but the diagnosis of lympho-cytic gastritis should be reserved for cases with markedintraepithelial lymphocytosis in the absence of active Hpylori gastritis. Lymphocytic gastritis can be observed inchildren but is usually detected in late adulthood, withaverage age of diagnosis of 50 years.
Case 6A 75-year-old woman presents after esophagogastro-
duodenoscopy. Gastric antrum shows gastritis; the pa-thologist is asked to rule out H pylori. The histologic find-ings are shown in Figure 6.
Findings. Examination of the biopsy material resultsin the following pattern of answers:
1. Are there features of chronic gastritis? There is min-imal chronic gastritis.
2. Are there neutrophils in the mucosa? No.3. Is there Helicobacter? No. Examination of H&E stains
does not reveal H pylori bacterial forms.4. Is there atrophy? No. There is no atrophy or intestinal
metaplasia.5. What is the topography of lesions? The chronic gas-
tritis involves, at minimum, the gastric antrum.6. Are additional special features seen? Yes. There are
diagnostic special features, including foveolar hyperplasiawith a corkscrew appearance of the foveolae. The foveolarepithelium shows reactive cytologic features, including re-duced cytoplasmic mucin. The lamina propria shows con-gestion and smooth muscle hyperplasia, with prominentmuscularization of the most superficial mucosa.
7. Are special stains recommended? No ancillary testsare performed.
Diagnosis. Gastric antral mucosa with features con-sistent with reactive gastropathy. No H pylori organismsare identified.
CHRONIC, REACTIVE (CHEMICAL) GASTROPATHYChronic reactive gastropathy (also know as chemical
gastropathy) is very common in current clinical practice.The mucosal changes are usually more prominent in theprepyloric region, but they may extend to involve the ox-yntic mucosa. The usual underlying causes include chron-ic bile reflux and long-term NSAID intake. The histopath-ologic features include mucosal edema, congestion, fibro-muscular hyperplasia in the lamina propria, and foveolarhyperplasia with a corkscrew appearance in the most se-vere forms. The foveolar epithelium characteristicallyshows reactive nuclear features and reduction of mucin.The epithelial changes occur with little background chron-ic inflammation. However, if there is erosion of the mu-cosa, superficial neutrophils may be present. Erosive gas-
1592 Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil
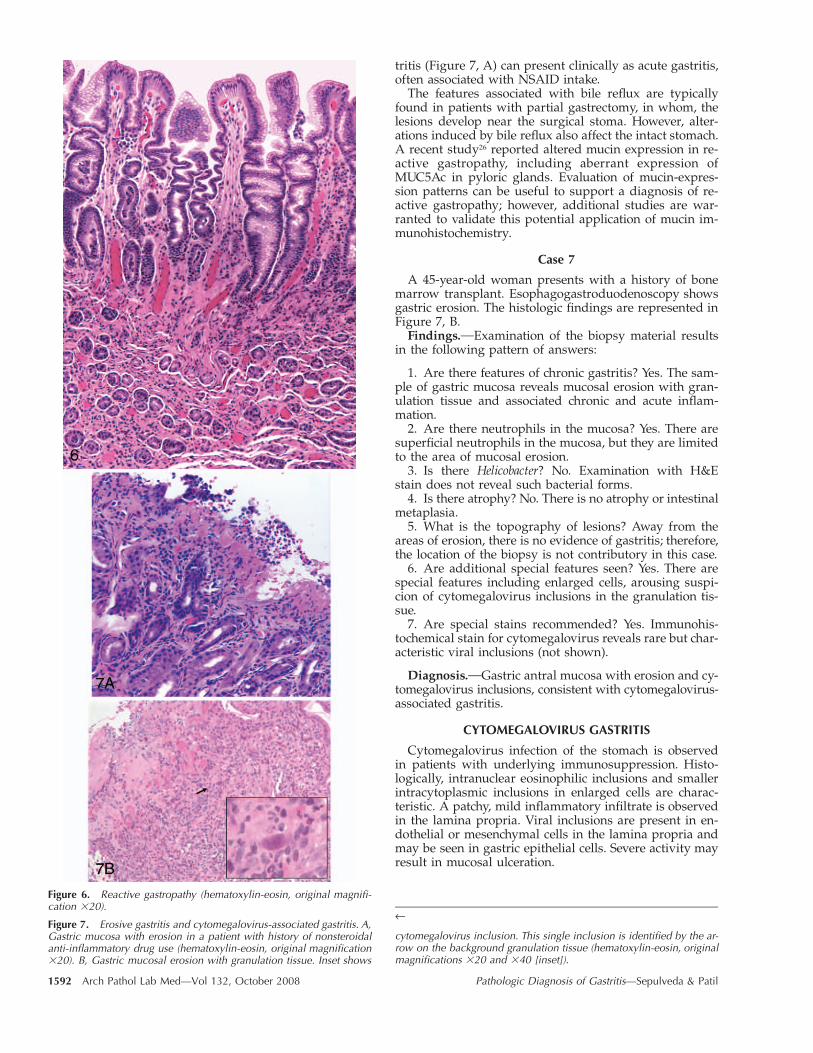
Figure 6. Reactive gastropathy (hematoxylin-eosin, original magnifi-cation �20).
Figure 7. Erosive gastritis and cytomegalovirus-associated gastritis. A,Gastric mucosa with erosion in a patient with history of nonsteroidalanti-inflammatory drug use (hematoxylin-eosin, original magnification�20). B, Gastric mucosal erosion with granulation tissue. Inset shows
←
cytomegalovirus inclusion. This single inclusion is identified by the ar-row on the background granulation tissue (hematoxylin-eosin, originalmagnifications �20 and �40 [inset]).
tritis (Figure 7, A) can present clinically as acute gastritis,often associated with NSAID intake.
The features associated with bile reflux are typicallyfound in patients with partial gastrectomy, in whom, thelesions develop near the surgical stoma. However, alter-ations induced by bile reflux also affect the intact stomach.A recent study26 reported altered mucin expression in re-active gastropathy, including aberrant expression ofMUC5Ac in pyloric glands. Evaluation of mucin-expres-sion patterns can be useful to support a diagnosis of re-active gastropathy; however, additional studies are war-ranted to validate this potential application of mucin im-munohistochemistry.
Case 7
A 45-year-old woman presents with a history of bonemarrow transplant. Esophagogastroduodenoscopy showsgastric erosion. The histologic findings are represented inFigure 7, B.
Findings. Examination of the biopsy material resultsin the following pattern of answers:
1. Are there features of chronic gastritis? Yes. The sam-ple of gastric mucosa reveals mucosal erosion with gran-ulation tissue and associated chronic and acute inflam-mation.
2. Are there neutrophils in the mucosa? Yes. There aresuperficial neutrophils in the mucosa, but they are limitedto the area of mucosal erosion.
3. Is there Helicobacter? No. Examination with H&Estain does not reveal such bacterial forms.
4. Is there atrophy? No. There is no atrophy or intestinalmetaplasia.
5. What is the topography of lesions? Away from theareas of erosion, there is no evidence of gastritis; therefore,the location of the biopsy is not contributory in this case.
6. Are additional special features seen? Yes. There arespecial features including enlarged cells, arousing suspi-cion of cytomegalovirus inclusions in the granulation tis-sue.
7. Are special stains recommended? Yes. Immunohis-tochemical stain for cytomegalovirus reveals rare but char-acteristic viral inclusions (not shown).
Diagnosis. Gastric antral mucosa with erosion and cy-tomegalovirus inclusions, consistent with cytomegalovirus-associated gastritis.
CYTOMEGALOVIRUS GASTRITIS
Cytomegalovirus infection of the stomach is observedin patients with underlying immunosuppression. Histo-logically, intranuclear eosinophilic inclusions and smallerintracytoplasmic inclusions in enlarged cells are charac-teristic. A patchy, mild inflammatory infiltrate is observedin the lamina propria. Viral inclusions are present in en-dothelial or mesenchymal cells in the lamina propria andmay be seen in gastric epithelial cells. Severe activity mayresult in mucosal ulceration.

Arch Pathol Lab Med—Vol 132, October 2008 Pathologic Diagnosis of Gastritis—Sepulveda & Patil 1593
COMMENT
Most types of gastritis can be diagnosed with H&Estains. To reach a determination of etiology and a specificdiagnostic entity, a limited list of questions can be usedto evaluate the histopathology of gastric biopsies, whichcan lead to a pattern of answers that corresponds to aspecific diagnosis of the most common types of gastritis.Although not ideal, the diagnosis of gastritis can bereached from limited biopsy material, even when the lo-cation of the biopsy is not indicated. If the biopsy site isnot known, immunohistochemical stains for synaptophy-sin and gastrin can help determine the biopsy location,permitting a specific diagnosis of atrophic gastritis type.Helicobacter pylori immunohistochemical stains can be par-ticularly useful when moderate to severe chronic gastritisor any active gastritis is present but no Helicobacter organ-isms are identified on H&E stains, when extensive intes-tinal metaplasia is present, and to evaluate follow-up bi-opsies after antibiotic treatment for H pylori.
At the end of the day, there are a number of cases witha diagnosis of chronic inactive gastritis, generally mild, forwhich a specific etiology cannot be determined by histo-pathologic examination alone. This may be accounted forby limited tissue sampling, nonspecific focal, mild, chronicinactive gastritis associated with various systemic disor-ders, or as yet uncharacterized forms of gastritis.
References1. Sepulveda AR, Dore MP, Bazzoli F. Chronic gastritis. Available at: http://
www.emedicine.com. Accessed November 27, 2007.2. Srivastava A, Lauwers GY. Pathology of non-infective gastritis. Histopathol-
ogy. 2007;50:15–29.3. McKenna BJ, Appelman HD. Primer: histopathology for the clinician—how
to interpret biopsy information for gastritis. Nat Clin Pract Gastroenterol Hepatol.2006;3:165–171.
4. Dixon MF, Genta RM, Yardley JH, Correa P, the participants in the Inter-national Workshop on the Histopathology of Gastritis, Houston 1994. Classifi-cation and grading of gastritis: the updated Sydney System. Am J Surg Pathol.1996;20:1161–1181.
5. Singhal AV, Sepulveda AR. Helicobacter heilmannii gastritis: a case studywith review of literature. Am J Surg Pathol. 2005;29:1537–1539.
6. Sipponen P, Kekki M, Haapakoski J, Ihamaki T, Siurala M. Gastric cancerrisk in chronic atrophic gastritis: statistical calculations of cross-sectional data. IntJ Cancer. 1985;35:173–177.
7. Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infectionand the development of gastric cancer. N Engl J Med. 2001;345:784–789.
8. Asaka M, Sugiyama T, Nobuta A. et al. Atrophic gastritis and intestinal meta-plasia in Japan: results of a large multicenter study: Helicobacter. 2001;6:294–299.
9. Correa P, Haenszel W, Cuello C, Tannenbaum S, Archer M. A model forgastric cancer epidemiology. Lancet. 1975;2:58–60.
10. Parsonnet J, Hansen S, Rodriguez L, et al. Helicobacter pylori infectionand gastric lymphoma. N Engl J Med. 1994;330:1267–1271.
11. Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, Isaacson PG. Helicobacterpylori–associated gastritis and primary B-cell gastric lymphoma. Lancet. 1991;338:1175–1176.
12. Jaffe ES, Harris NL, Stein H, Vardiman JW. Pathology and Genetics of Tu-mours of Hematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2001.World Health Organization Classification of Tumours; vol 3.
13. Tagkalidis P, Royce S, Macrae F, Bhathal P. Selective colonization by Hel-icobacter pylori of the deep gastric glands and intracellular canaliculi of parietalcells in the setting of chronic proton pump inhibitor use. Eur J GastroenterolHepatol. 2002;14:453–456.
14. Rugge M, Genta RM. Staging and grading of chronic gastritis. Hum Pathol.2005;36:228–233.
15. Huang JQ, Sridhar S, Chen Y, Hunt RH. Meta-analysis of the relationshipbetween Helicobacter pylori seropositivity and gastric cancer. Gastroenterology.1998;114:1169–1179.
16. Correa P, Houghton J. Carcinogenesis of Helicobacter pylori. Gastroenter-ology. 2007;133:659–72.
17. Sepulveda AR, Coelho LG. Helicobacter pylori and gastric malignancies.Helicobacter. 2002;7(suppl 1):37–42.
18. Jonkers D, Stobberingh E, de Bruine A, Arends JW, Stockbrugger R. Eval-uation of immunohistochemistry for the detection of Helicobacter pylori in gastricmucosal biopsies. J Infect. 1997;35:149–154.
19. Toulaymat M, Marconi S, Garb J, Otis C, Nash S. Endoscopic biopsy pa-thology of Helicobacter pylori gastritis: comparison of bacterial detection by im-munohistochemistry and Genta stain. Arch Pathol Lab Med. 1999;123:778–781.
20. Xin W, Greenson JK. The clinical significance of focally enhanced gastritis.Am J Surg Pathol. 2004;28:1347–1351.
21. Price A. The Sydney System: histological division. J Gastroenterol Hepatol.1991;6:209–222.
22. Rugge M, Correa P, Dixon MF. et al. Gastric mucosal atrophy: interob-server consistency using new criteria for classification and grading. Aliment Phar-macol Ther. 2002;16:1249–1259.
23. Whiting JL, Sigurdsson A, Rowlands DC, Hallissey MT, Fielding JW. Thelong term results of endoscopic surveillance of premalignant gastric lesions. Gut.2002;50:378–381.
24. Capella R, Fiocca C, Cornaggia M. Autoimmune gastritis. In: Graham DY,Genta RM, Dixon MF, eds. Gastritis. Philadelphia, Pa: Lippincott Williams; 1999:79–96.
25. Jevremovic D, Torbenson M, Murray JA, Burgart LJ, Abraham SC. Atrophicautoimmune pangastritis: a distinctive form of antral and fundic gastritis associ-ated with systemic autoimmune disease. Am J Surg Pathol. 2006;30:1412–1419.
26. Mino-Kenudson M, Tomita S, Lauwers GY. Mucin expression in reactivegastropathy: an immunohistochemical analysis. Arch Pathol Lab Med. 2007;131:86–90.
Archives of Pathology & Laboratory Medicine and Archives of Ophthalmology will publish a jointtheme issue on ophthalmic pathology in August 2009. Articles on diagnostic procedures, path-ologic mechanistic pathways, and translational research in retinoblastoma, melanoma, lympho-ma, orbital, and adnexal tumors in ophthalmic pathology will have the best chance for consid-eration in this theme issue. Manuscripts must be submitted no later than February 1, 2009 forconsideration in the joint theme issue. All submissions will undergo our usual peer review process.
Important: When submitting a manuscript for this theme issue, be certain to mention this inboth the cover letter and the Comment section within the AllenTrack submission system.
To view our Instructions for Authors, visit
http://arpa.allenpress.com/pdf/instructions�for�authors.pdf