Embed Size (px)
DESCRIPTION
Pathologic Diagnosis in Occupational Lung Diseases. Dr.E.Handan Zeren Çukurova University. Occupational lung disease ≠ Pneumoconiosis. Pneumoconiosis = Retention of and pathologic effects from the inhalation of dust particles - PowerPoint PPT Presentation
Citation preview

Pathologic Diagnosis in Occupational Lung Diseases
Dr.E.Handan ZerenÇukurova University

Occupational lung disease ≠ Pneumoconiosis
Pneumoconiosis = Retention of and pathologic effects from the inhalation of dust particles
Many of the diseases named occupational lung disease do not match with this definition

In most cases, the diagnoses is made without tissue examination…. History of the patient Clinical findings Radiologic features Epidemiologic features

Properties of inhaled dust particles… Size (Particles <10μm and more
likely <5μm reach the lung parenchyma)
Fibers, esp. asbest can reach the parenchyma when larger than 10 μm.Width is an important factor
Chemical properties
Mineralogic propertiesall affect the potency of a dust particle to cause lung injury

Pathologic reaction patterns Fibrogenic particles (asbestos,
silica) Nodular fibrosis Intersititial fibrosis Both
Non-Fibrogenic particles (carbon)

Centriacinar emphysema Centriacinar dust macules Mineral dust airway disease Dust-laden macrophages along lymphatic
routes- bronchovascular bundles, pleura, interlobular septa
Noduler fibrosis Diffuse interstitial fibrosis- UIP Massive fibrosis Other reactions- granulomatous reaction,
alveolar proteinosis, hipersensitivity pneumonitis etc.

Hyaline pleural plaques
Pleuritis and pleural fibrosis

Coal Worker’s Pneumoconiosis(CWP) The most significant factor in the
development of CWP is the cumulative exposure to coal dust
Simple CWP- Macules of coal dust and focal emphysema (centriacinar- similar to smoker’s emphysema)

CWP: Different pathologic patterns
Coal nodules
Rheumatoid pneumoconiosis Progressive massive fibrosis

Silicosis
Nodular fibrosis < 10 mm- simple silicosis >1 cm- complicated silicosis
At least a latent period of 20 years Accelerated silicosis- A latent period
of 3-10 years

Dr.Andrew Churg- Van Couver, Canada

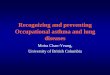
Acute Silicoproteinosis
Same morphology with alveolar proteinosis
Heavy silica inhalation Symptomatic within 3 years, fatal
in most cases

Early Silicosis

Formation of the silicotic nodule


PMF (Progressive massive fibrosis) in silicosis If necrosis is present, TB must be
roled out

Mixed dust pneumoconiosis

İsolated pleural silicosis
ZEREN EH, COLBY TV, ROGGLI VL. SILICA-INDUCED PLEURAL DISEASE: AN UNUSUAL CASE MIMICKING MALIGNANT MESOTHELIOMA. CHEST (1997)112:1436-8

Diseasesassociated with Asbestos exposure Asbestosis Asbestos airway disease Non-neoplastic pleural patologic
conditions Benign asbestos effusion Visseral pleural fibrosis Hyaline pleral plaque
Lung cancer Malignant mesothelioma

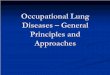
Asbestos bodies
Ghio AJ, Churg A, Roggli VL; Toxicologic Pathology (2004)32:643-649


Asbestosis Heavy exposure, latent period ↓ Pleural involvement- an important
clue Involvement of the lower lobes

Pulmonary Siderosis Deposition of iron and iron oxides following
the exposure- not very uncommon No clinically apparent disease unless mixed
with other fibrogenic dusts Small airway dysfunction and emphysema if
inhaled in large amounts
Asbestosis + Siderosis

Berilliosis-chronic berillium disease Metal working, ceramic, electronic,
computer industry, space industry, dental laboratories using berillium alloys, florescent lamp manufacturing
Multisystemic disease Similar clinic and pathologic features
with sarcoidosis

Hard metal (Cobalt) lung disease As hard as dimond- ideal for ctting
of metal tools Formerly, categorized as “Giant
cell intersititial pneumonia” in Leibow’s classification

Occupational hipersensitivity pneumonia (HP) (extrinsic allergic alveolitis) Organic antigens or simple
inorganic chemical compounds The exposure is obvious in most
cases (e.g: Farmer’s lung); whereas it can be difficult to identify in some others (e.g: Contamination of ventilation system)
Hot-tub disease- Water supplies contaminated by M.Avium

HP
Type 3 (immune complex) ve Type 4 (T-cell mediated, delayed type hypersensitivity ) immune reactions
Acute- 4-6 hours Subacute- days-weeks Chronic- long lasting, low amounts
of antigen exposure. Irreversible respiratory function disability and fibrosis can occur

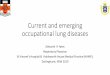
HP-Histology
Chronic bronchiolitis + peribronchiolar interstitial pneumonia
Lyphocytic + histiocytic inflammation, rare eosinophils and plasma cells
Loose granulomas in 2/3 of cases

HP
Fibroblastic plugs filling the alveol lumens (Masson bodies)
In old cases, irreversible changes such as UIP features and end stage lung- difficult to diagnose

Differential diagnosis-HP
Collagen vascular diseases, drug reactions, infections, NSIP
DETAILED CLINICAL INFORMATION + SPECIAL STAINS FOR MICROORGANISMS +IDENTIFICATION OF THE RESPONSIBLE ANTIGEN

Organic dust toxic syndrome Acute, systemic illness following massive
exposure to organic dusts containing microorganisms or their endotoxins
Farmers exposed to grains or moldy hay contaminated with fungi
Not a real immune reaction as it occurs without prior history of sensitization
Intraalveolar space- neutrophils and histiocytes
Acute bronchiolitis

Gases and Fumes
ARDS Chronic bronchitis Necrotizing bronchiolitis Asthma Bronchiectasis Organizing pneumonia

Conclusions
The diagnosis of occupational and environmental diseases is made by combining the clinical, epidemiological, radiologic, and pathologic features with the patient’s occupational and environmental status

In the diagnosis, these questions are important: Is there a clear evidence of exposure to a
known agent that is associated with the findings identified?
How strong is this association and chance of developing the disease?
What is the temporal sequence ofthe exposure, and the onset of the disease?
Can the pathologic findings be explained only by the exposure?
Is the exposure related to a single disease?

THANK YOU…