Embed Size (px)
Citation preview
Postpartum HemorrhageJEFF YAO
ALI SHAHBAZ
“
”
Investing in maternal health is a wise health and economic policy decision. Women are the sole income-earners in nearly one third of all
households globally. There are spill-over macro-economic benefits from the women whose lives are improved by maternal health
interventions. Many maternal- care interventions are proven to be both effective in reducing maternal death and cost-effective,
especially for high-risk groups.
- WHO MATERNAL HEALTH

In one study,
73%
of such deaths in the US were determined to have been preventable. Underestimation of blood loss contributes greatly to this figure.
Case
A 29 yo G5P4 woman at 39 weeks gestation with preeclampsia delivers vaginally. Her prenatal course has been uncomplicated except for asymptomatic bacteriuria caused by E. coli in the first trimester treated with oral cephalexin. She denies a family history of bleeding diathesis. After the placenta is delivered, there is appreciable vaginal bleeding estimated at 1 L
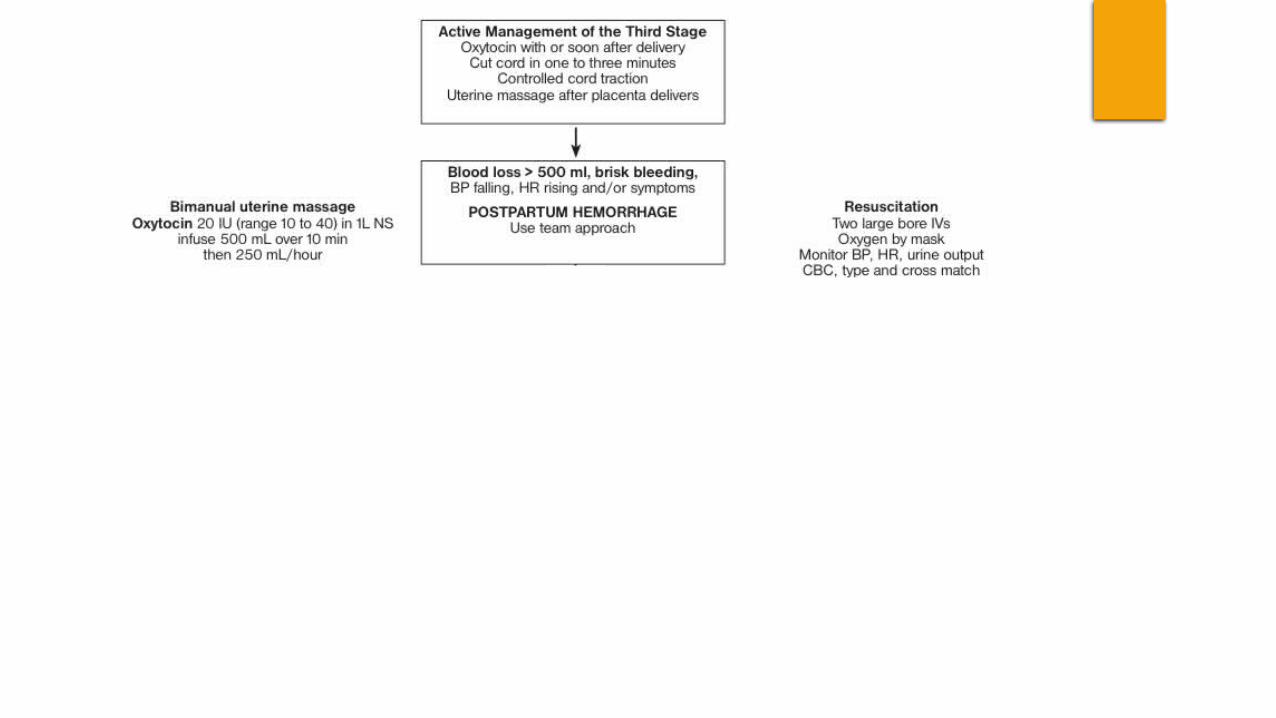
POSTPARTUM HEMMORAGE!!
Define: PPH
Postpartum Hemmorage (PPH)
Blood loss >500mL following vaginal delivery OR >1000mL with C/S
Often underestimated and inaccurate
Clinically: ANY blood loss that can cause hemodynamic instability
If it has the potential to result in hemodynamic instability – TREAT IT!
Case
A 29 yo G5P4 woman at 39 weeks gestation with preeclampsia delivers vaginally. Her prenatal course has been uncomplicated except for asymptomatic bacteriuria caused by E. coli in the first trimester treated with oral cephalexin. She denies a family history of bleeding diathesis. After the placenta is delivered, there is appreciable vaginal bleeding estimated at 1 L
Classification of PPH
Early (primary) PPH
Occurs within 24 hours of delivery (most common)
Late (secondary) PPH
24 hours to 6 weeks after delivery (peak incidence at 1-2 weeks postpartum)
Signs and Symptoms of Postpartum Hemorrhage
Signs and Symptoms of Postpartum Hemorrhage
Risk Factors for PPH
Retained Placenta/membranes
Failure to progress during second stage of labour (prolonged labour)
Morbidly adherent placenta
Lacerations
Instrument Delivery
Large for GA newborn
Hypertension and Preeclampsia
Previous PPH
Case
A 29 yo G5P4 woman at 39 weeks gestation with preeclampsia delivers vaginally. Her prenatal course has been uncomplicated except for asymptomatic bacteriuria caused by E. coli in the first trimester treated with oral cephalexin. She denies a family history of bleeding diathesis. After the placenta is delivered, there is appreciable vaginal bleeding estimated at 1 L
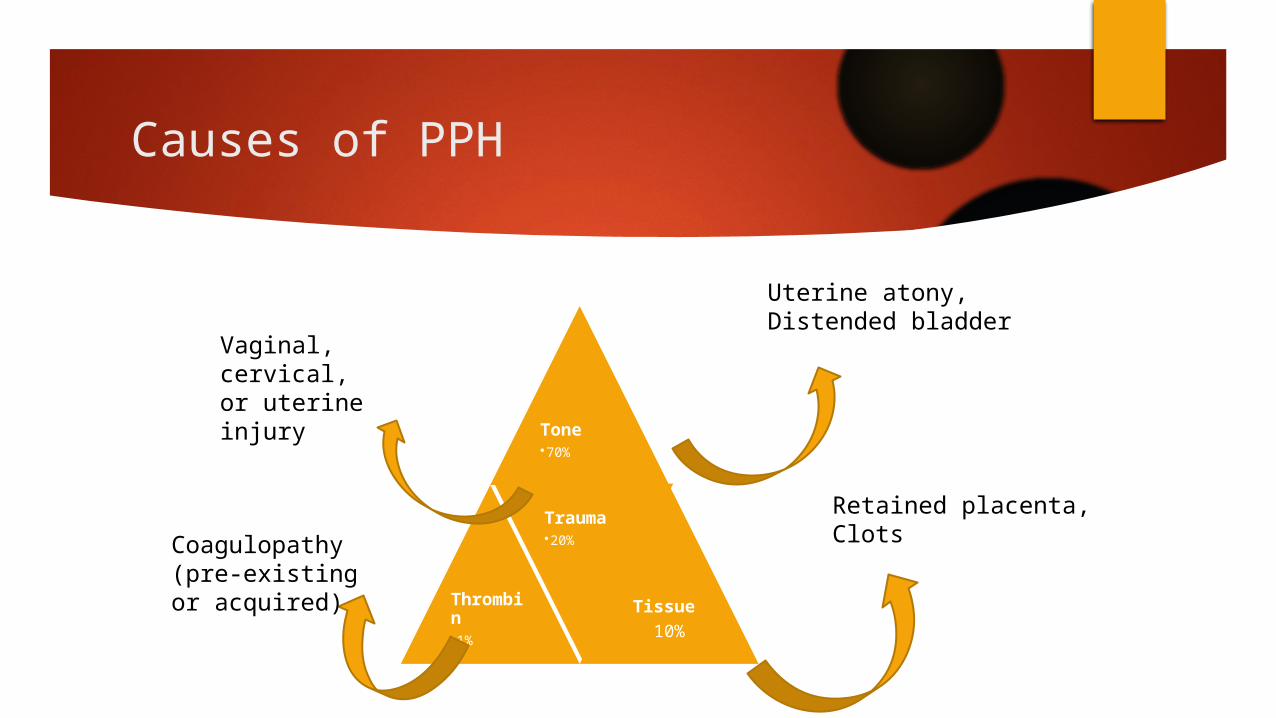
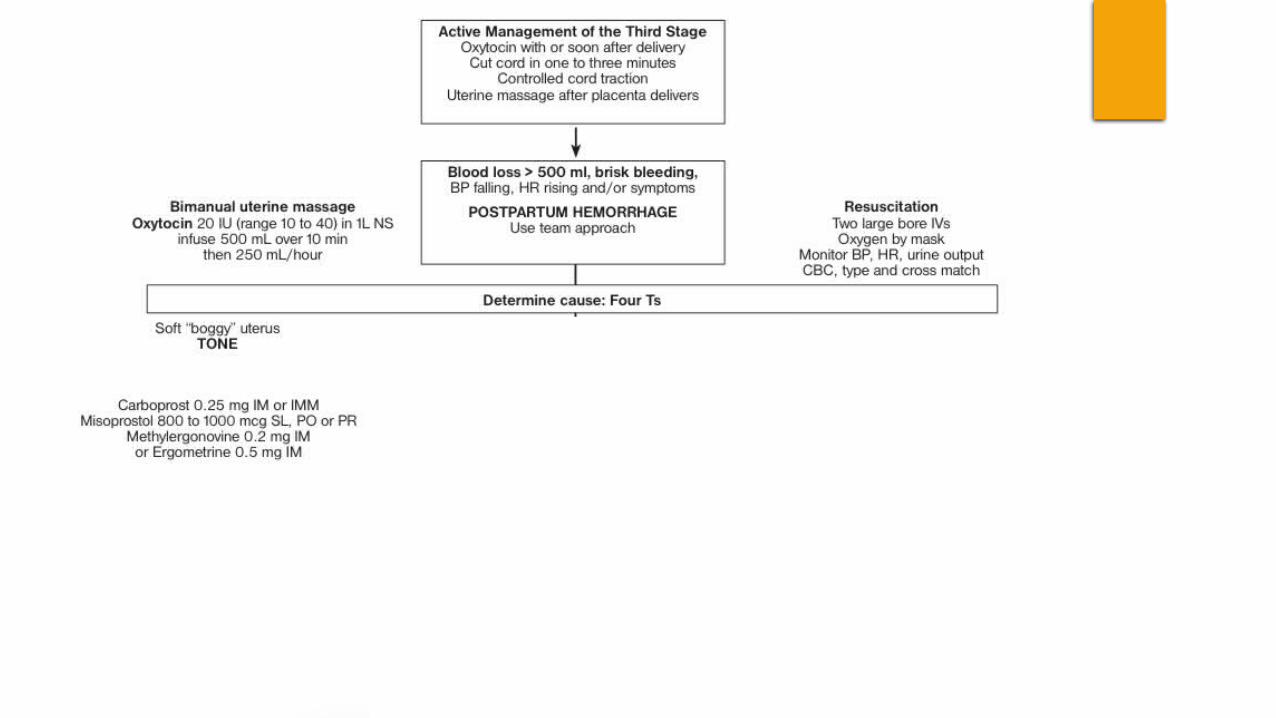
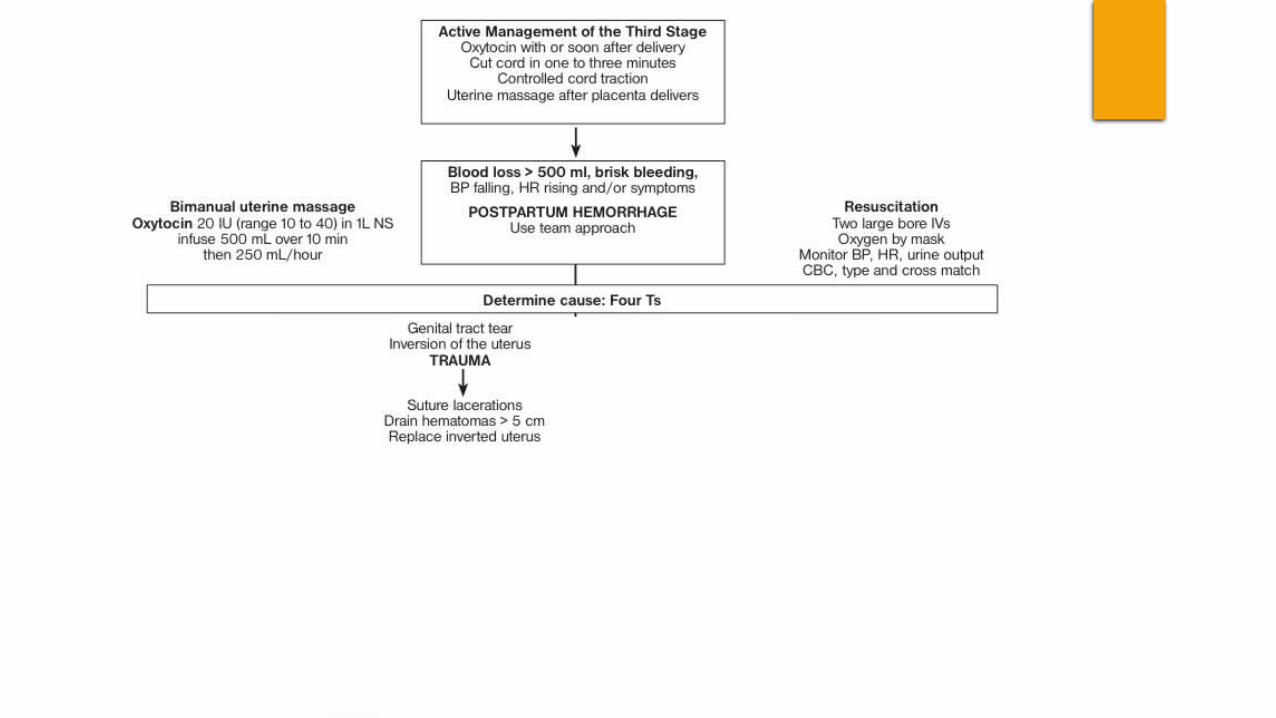
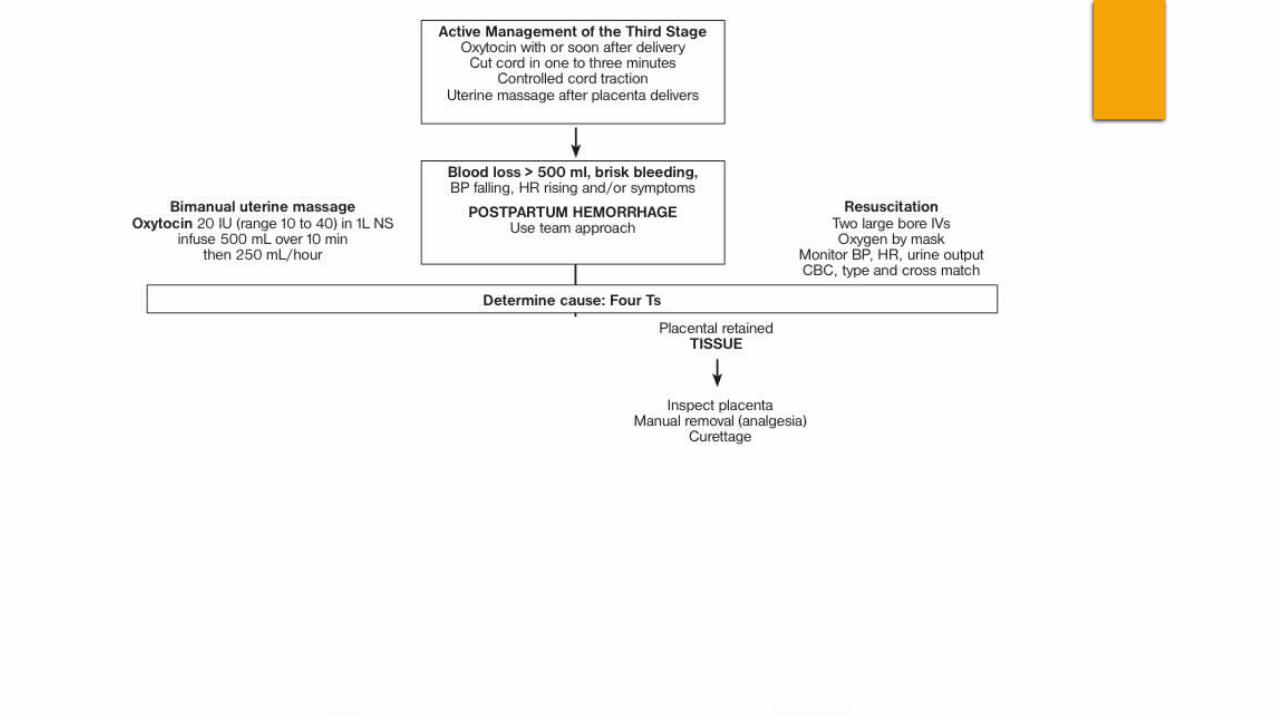
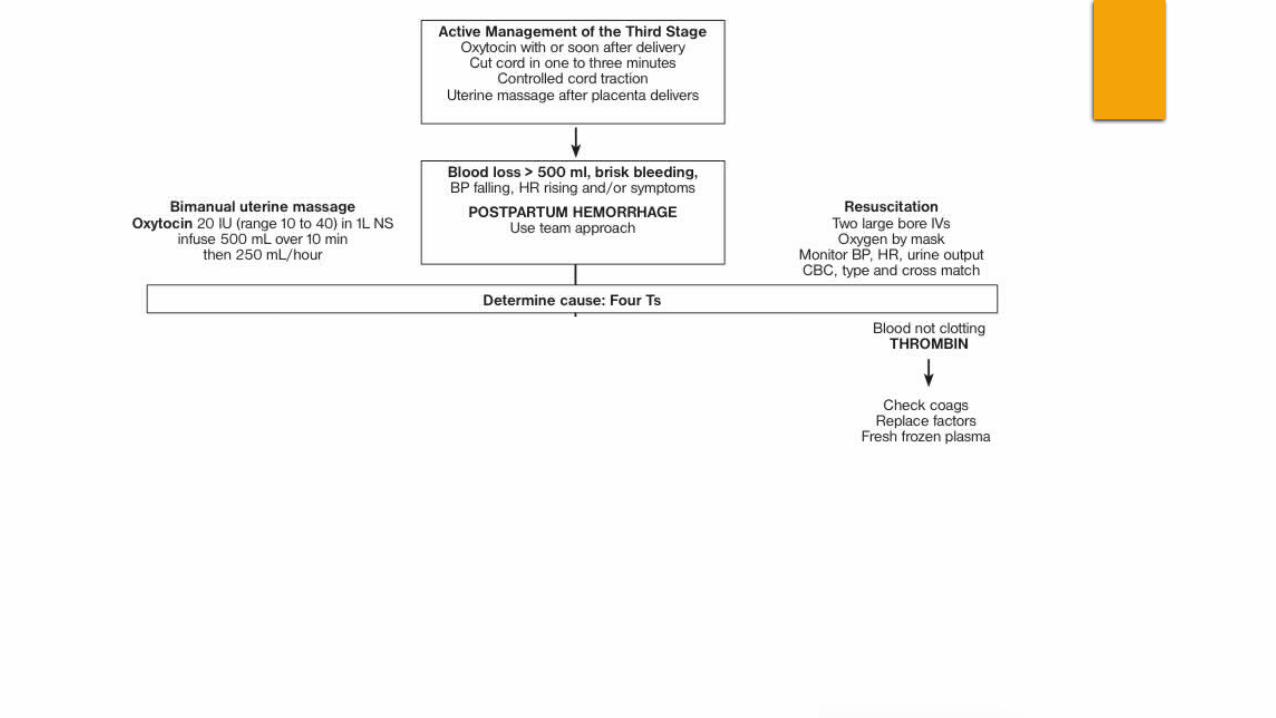
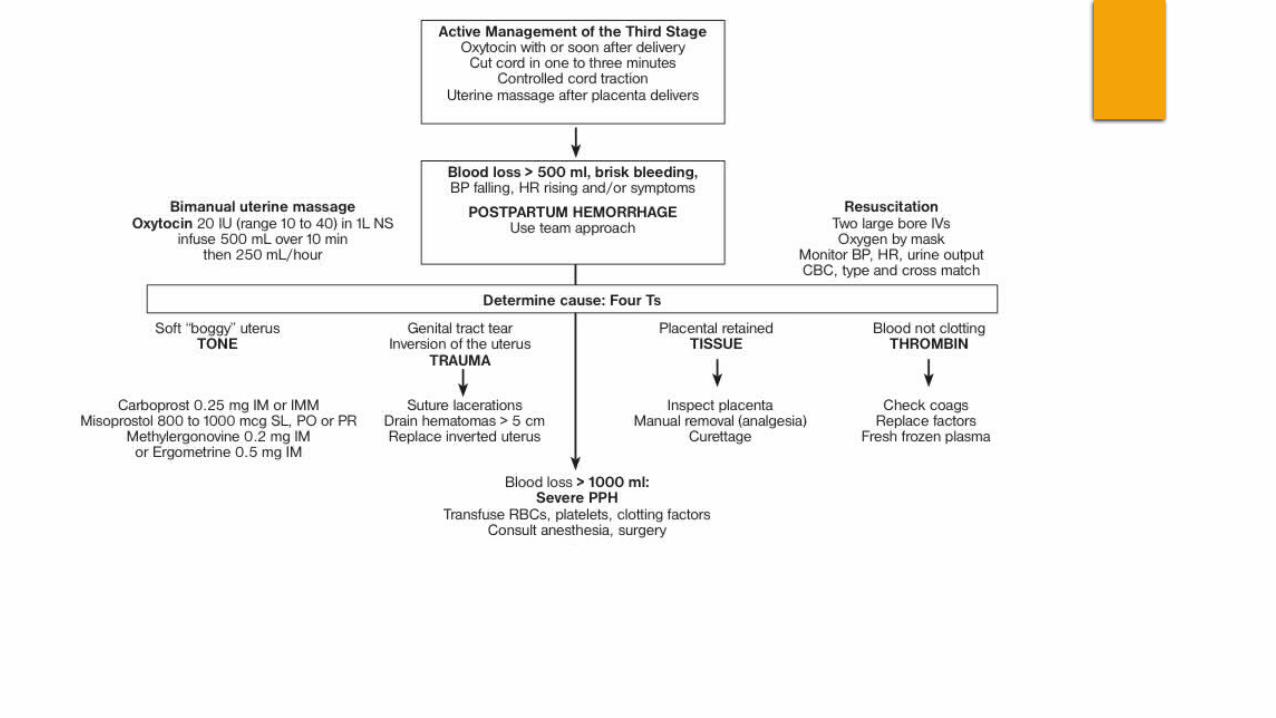
Causes of PPH
Tone•70%
Thrombin•1%
Trauma•20%
Tissue 10%
Uterine atony, Distended bladder
Coagulopathy (pre-existing or acquired)
Vaginal, cervical, or uterine injury
Retained placenta, Clots
TONE : Abnormalities of Uterine Contraction
Over distention of Uterus
Uterine muscle exhaustion
Intra-amniotic infection
Distortion of uterus
Uterine-relaxing medications
Bladder Distention
May prevent uterine contraction
Tissue: Retained
Retained products
Abnormal placentation
Retained Blood Clots
Trauma of the genital tract
Laceration of cervix, vagina, or perineum
Lacerations from C/S
Uterine Rupture
Uterine inversion
Thrombin: Coagulopathies
Pre-existing States of Coagulopathy
Hemophilia A
Von Willebrand’s Disease
Hx of PPH
Acquired in pregnancy
Idiopathic thrombocytopenic purpura
Thrombocytopenia with preeclampsia
Disseminated intravascular coagulation
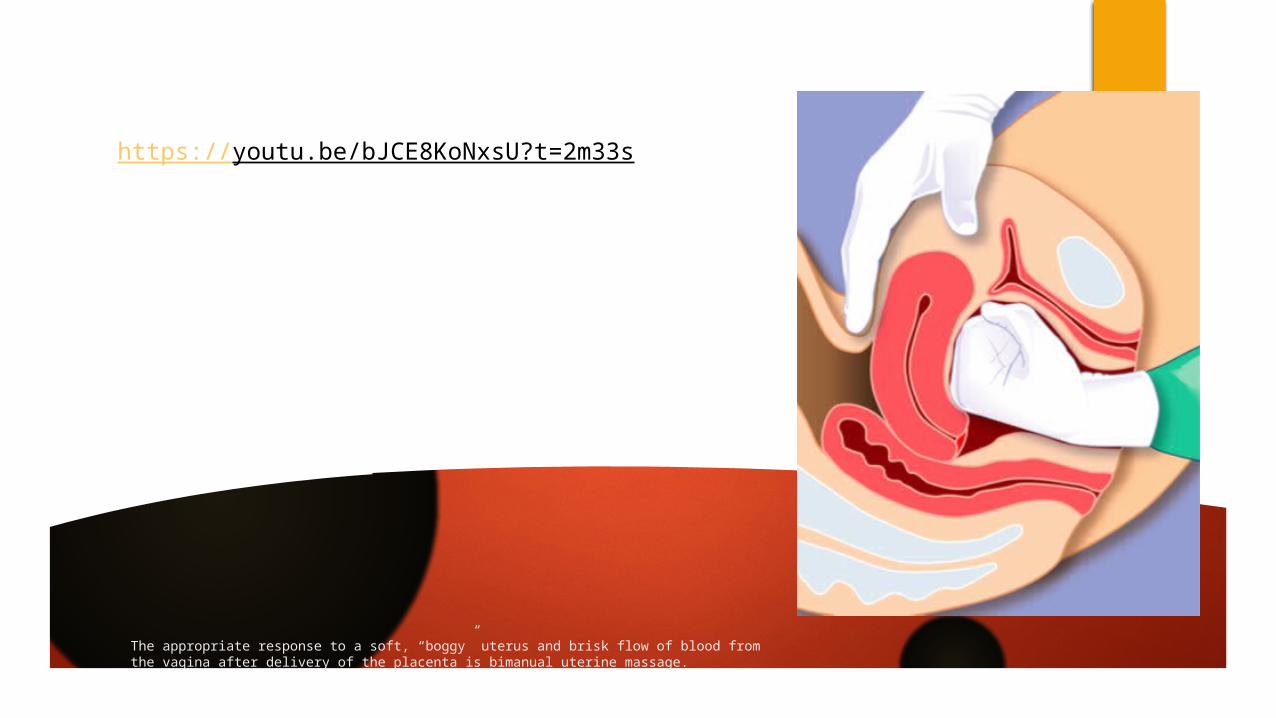
The appropriate response to a soft, “boggy” uterus and brisk flow of blood from the vagina after delivery of the placenta is bimanual uterine massage.
https://youtu.be/bJCE8KoNxsU?t=2m33s
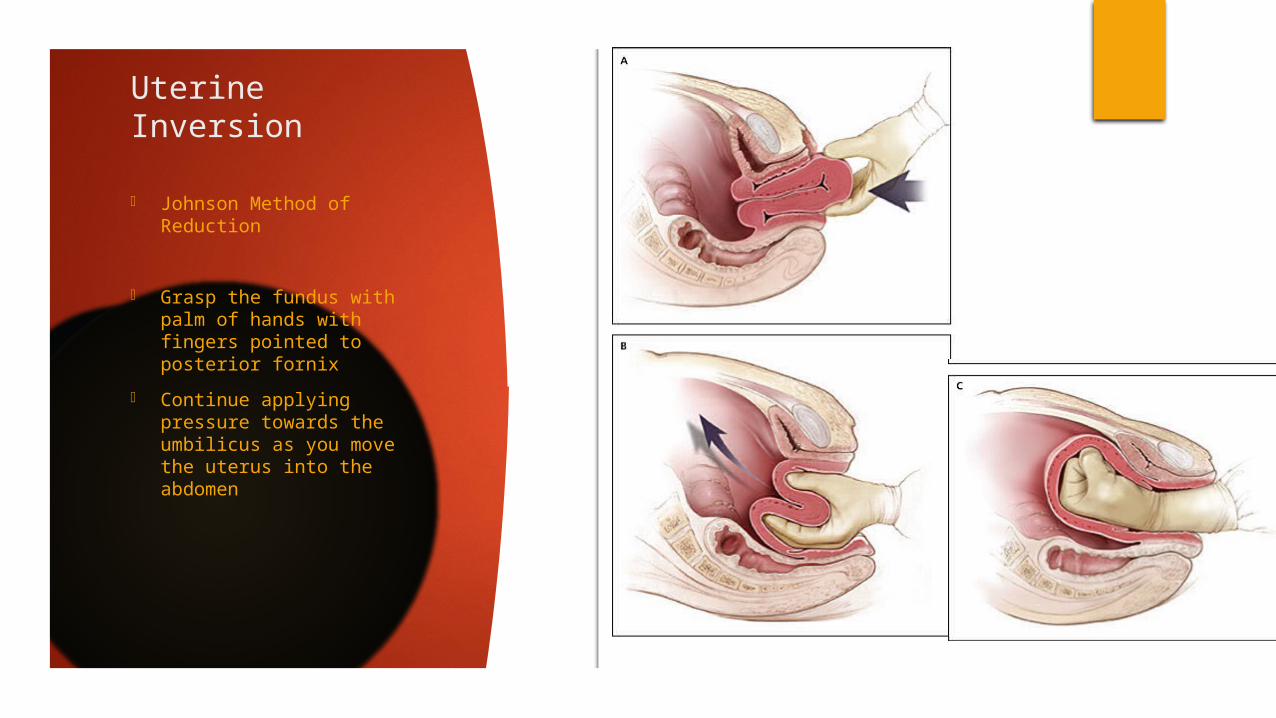
Uterine Inversion
- Johnson Method of Reduction
- Grasp the fundus with palm of hands with fingers pointed to posterior fornix
- Continue applying pressure towards the umbilicus as you move the uterus into the abdomen
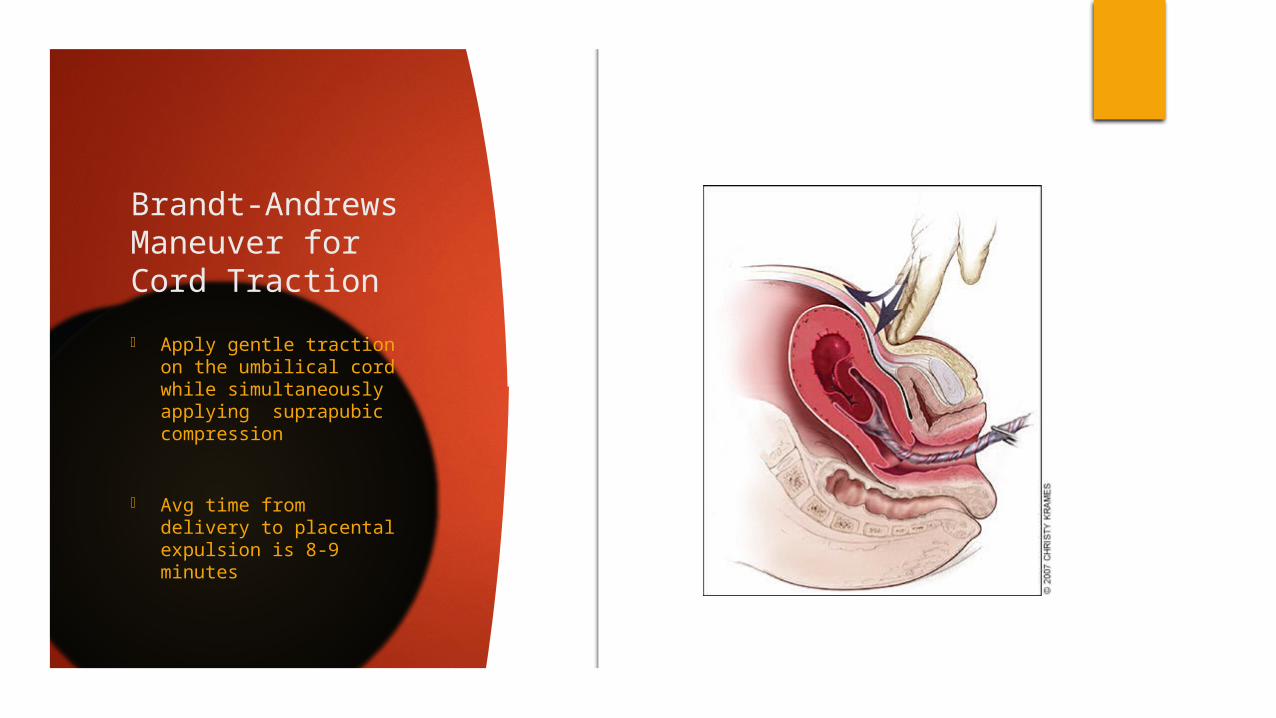
Brandt-Andrews Maneuver for Cord Traction
- Apply gentle traction on the umbilical cord while simultaneously applying suprapubic compression
- Avg time from delivery to placental expulsion is 8-9 minutes
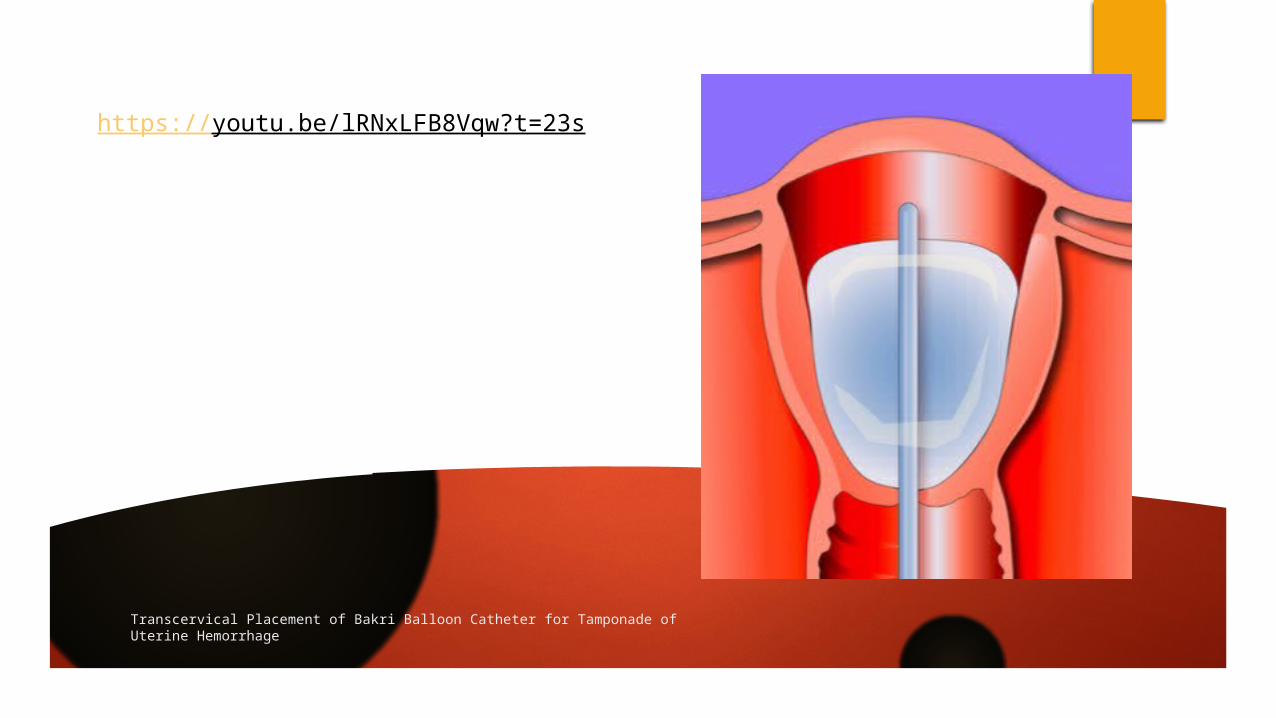
Transcervical Placement of Bakri Balloon Catheter for Tamponade of Uterine Hemorrhage
https://youtu.be/lRNxLFB8Vqw?t=23s
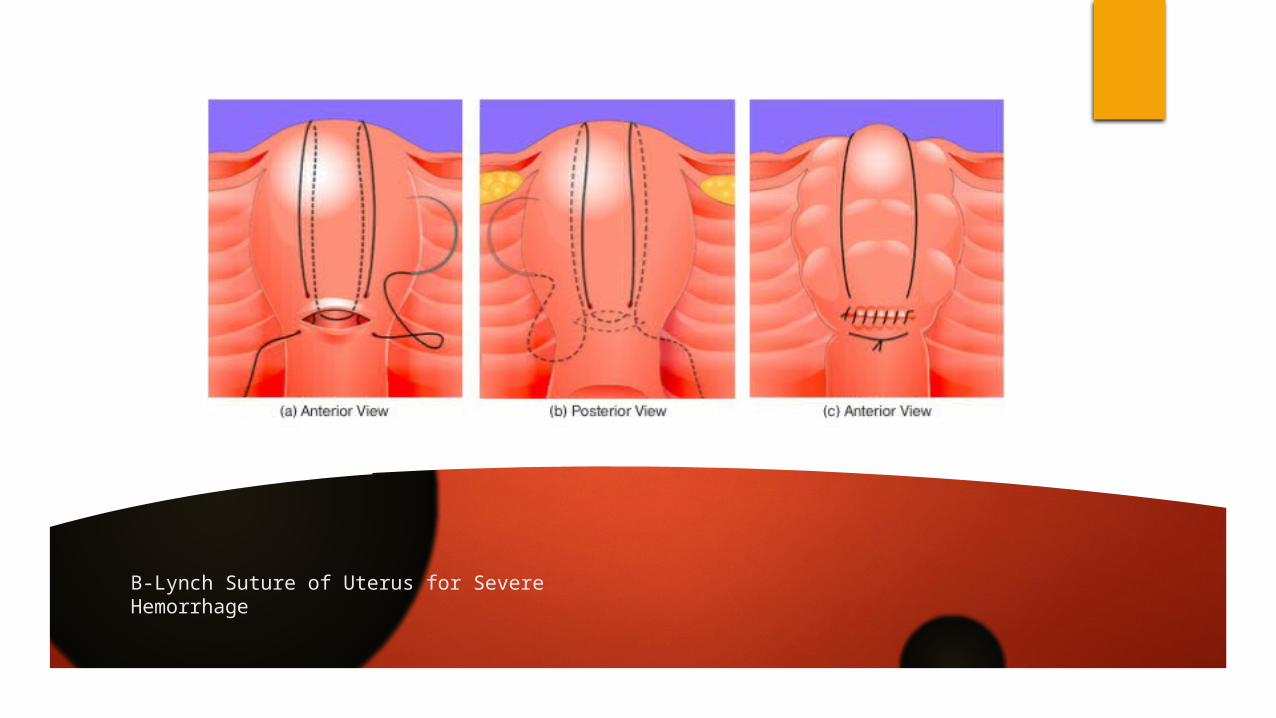
B-Lynch Suture of Uterus for Severe Hemorrhage
SOGC Guideline Recommendations
Active Management of Third Stage of Labour – should be offered and recommended to all women
Oxytocin IM is the preferred medication for prevention of PPH in low-risk vaginal deliveries
An IV bolus of oxytocin can be used for PPH prevention after vaginal birth but not recommended at this time for an elective C/S
Carbetocin can be used for elective C/S and for women delivering vaginally with 1 risk factor to help prevent PPH
Delayed cord clamping by at least 60 seconds is preferred to earlier clamping in premature newborns
Blood loss estimation should be done using clinical markers (signs and symptoms) rather than a visual estimation
Uterine tamponade is effective to temporarily control active PPH from uterine atony not responding to medical therapy
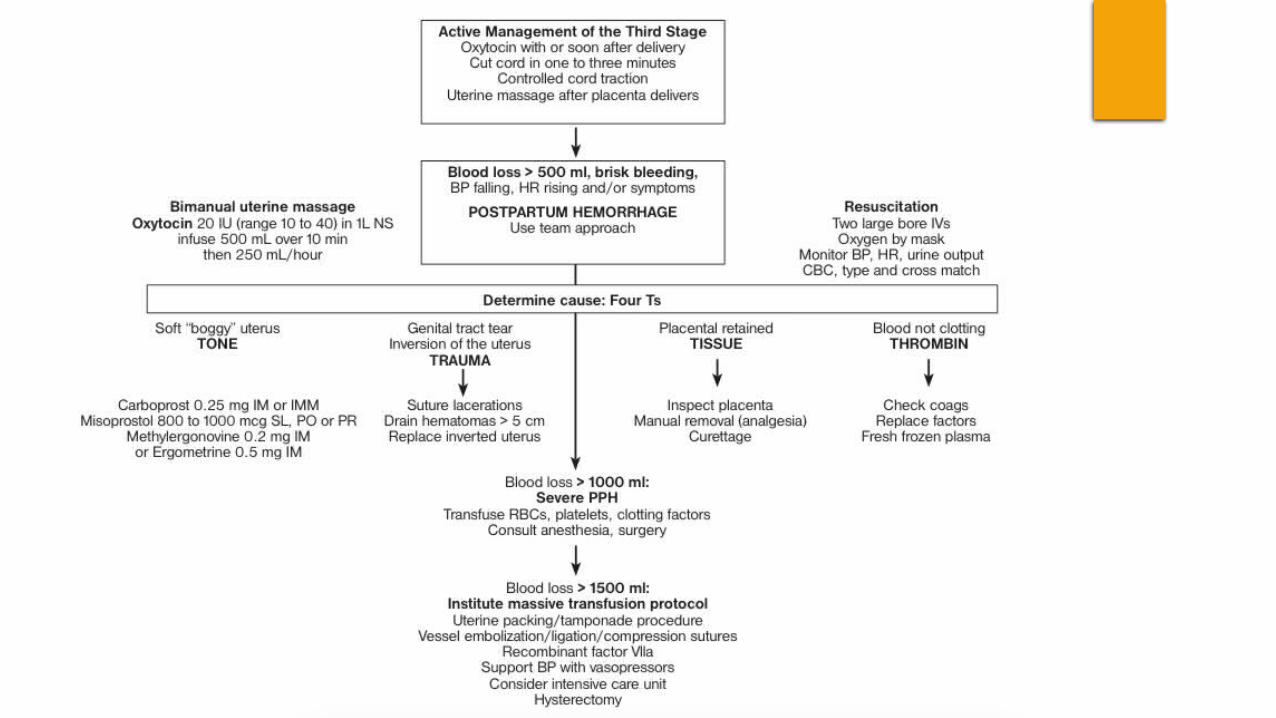
Surgical techniques should be used for intractable PPH unresponsive to medical therapy
SUMMARY [ALMOST DONE!]
Postpartum hemorrhage is unpredictable and can occur in women with no risk factors.
AMTSL includes oxytocin after delivery of the fetal anterior shoulder and controlled cord traction with the Brandt maneuver.
Uterine massage after delivery of the placenta is a reasonable approach and is included in some AMTSL protocols
Delayed cord clamping (one to three minutes after delivery) may be considered





























